Embed Size (px)
Citation preview
4/15/2013
1
CPT 2013 Update
Stuart Shanker, M.D., F.A.A.P.
Disclosure
I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME activity
I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.
Goals
Learn 2013 CPT Updates
Reinforce Basics
Apply Scenarios
Review Kancare
4/15/2013
2
Agenda
Update CPT
Review Guidelines
Apply Routine Cases
Discuss Newborn Coding
Review KanCare – Medicaid
2013 Update
Almost all code descriptors and instructions have been revised to include the term “qualified health care professional” (QHCP) when the word “physician” is included.
New codes have been added for transitional care services, complex care coordination, allergy ingestion challenges, interfacilitytransport of critical patients 24 months of age or less, polysomnography for children less than 6 years of age.
2013 Update
Revisions of codes have been made in the neonatal and pediatric critical care sections, Influenza codes have been revised, cardiology section has been revised, infusion and IV therapy codes revised and vision screening (99174) has been revised.
4/15/2013
3
2013 Update
Psychiatry section codes have been deleted (90804 – 09) and new codes have replaced them which include psychotherapy with E and M services (90833, 90836, 90838) and (90832,90834, 90837) without E and M services.
2013 Update
Definitions of New patients include no services of a QHCP of the Exact same specialty and subspecialty within the same group practice for the past three years.
Established patients have received services from a QHCP of the Exact same specialty and subspecialty within the same group practice within the past three years.
2013 Update
Observation or Inpatient Care Services on the same date:
99234 – Detailed or Comprehensive Hxand Exam; MDM straighforward or low complexity; 40 minutes spent on the floor99235 – Comprehensive Hx and Exam;MDM moderate complexity; 50 minutes 99236 – Comprehensive Hx and Exam;MDM moderate complexity; 55 minutes
4/15/2013
4
2013 Update
99444 – Online Medical Evaluation by a physician to an established patient or guardian not originating from a related E/M service provided within the previous seven days, using the Internet or similar electronic communications network.
2013 Update Pediatric Critical Care Transport:
99466-67 Face to Face care during the interfacility transport of a critical patient 24 months of age or younger; 30 minutes or greater.
99485 Non Face to Face Supervision by a “Control physician” (the physician directing transport services of a critical patient 24 months of age or less) including 2 way communication with the specialized transport team before transport, at the referring facility and during the transport; first 30 minutes.
2013 Update
Pediatric Critical Care Transport:99486 Non Face to Face Supervision by a
“Control physician” (the physician directing transport services of a critical patient 24 months of age or less) including 2 way communication with the specialized transport team before transport, at the referring facility and during the transport; each additional 30 minutes.
4/15/2013
5
2013 Update
Pediatric Critical Care Transport:99485-86 do not include pre-transport
communication between the control physician and the referring facility before or following patient transport.
May not use these codes if 99466-67 are used for the transport as these include the non-face to face time component.
2013 Update
Newborn Care Services:Neonatal Intensive Care Services and Neonatal Critical Care Services use the same definitions for creating the codes. (Pediatric Critical Care does also)
These codes 99468-69 are used once per day. (Initial and Subsequent)
May be used with additional codes for delivery attendance (99464) or resuscitation (99465) or Intubation (31500).
2013 Update
Critical care for those less than 6 years of age who are taken care of initially at one institution and transferred to another institution on the same date by different physicians in different groups:
The referring physician should use the series of 99291-92 (time based critical care) and the receiving physician should use initial day of care codes (99468,99471,99475).
4/15/2013
6
2013 Update
When a newborn receives normal newborn care (99460–62) by one group and becomes critically ill the same day, if the same group provides the critical care as well, use the normal care code as above and use the initial critical care code (99468) modified by 25.
If the patient has already received intensive care services or hospital care services and then needs critical care by the same group, only the critical care codes may be used.
2013 Update
Intensive Neonatal Care is for those Not Critically Ill but needing intensive cardiac and respiratory monitoring, continuous and/or frequent vital sign monitoring, heat maintenance, enteral and/or parenteral nutritional adjustments, lab and oxygen monitoring, and constant observation by the health care team under the direct supervision of the physician or QHCP. (99477-80)
2013 Update
Intensive Neonatal Care codes are assigned by initial day and subsequent days and by weight categories of very low birth weight (< 1500 gms), low birth weight (1500-2500 gms), and normal weight (2501-5000 gms).
Delivery attendance (99464), resuscitation (99465) or intubation (31500) may be used with the initial code of 99477. 99477 must then be modified with a 25.
4/15/2013
7
2013 Update
Neonatal Critical care and Neonatal Intensive care codes have a list of additional procedures and codes which are bundled in the care provided for the neonate, i.e., respiratory care, oxymetry, IV fluid management, umbilical catheterizations, etc. (See the list).
2013 Update
When a neonate or infant is transferred after the initial day within the same facility to the care of another physician in a different group, both physicians may report subsequent hospital care services (99231-33). Or the receiving physician may also use the subsequent normal newborn care codes (99462).
2013 Update
When a neonate or infant becomes critically ill on a day when initial or subsequent intensive care codes were reported by one physician and is transferred to critical care by a different group, the transferring physician may use either the intensive care code for the day or may use time based critical care codes (99291-92) for the time spent providing the care. The receiving physician uses Critical care codes.
4/15/2013
8
2013 Update
When a neonate or infant becomes critically ill on a day when intensive care codes have been performed and the same group takes care of the critical care services, the group should only use the neonatal or pediatric critical care codes for their services (99468-99476).
2013 Update
Complex Chronic Care Coordination Services99487 - first hour of care with no face to
face visit, per calendar month99488 – first hour of care with one face to
face visit, per calendar month99489 – each additional 30 minutes
Coordination of care by physician or QHCP for management and coordination of services to those at home, in a domiciliary home or assisted living.
2013 Update
Transitional Care Management Services99495 – Communication with the patient
and/or caregiver within 2 business days of discharge from an inpatient hospital.
MDM of at least moderate complexityFace to face within 14 calendar days of
dischargeBegins on the date of discharge and
continues for 29 days
4/15/2013
9
2013 Update
Transitional Care Management Services99496 – Communication with the patient
and/or caregiver within 2 business days of discharge from an inpatient hospital stay.
MDM of high complexityFace to face visit within 7 calendar days
of discharge
2013 Update
Immunizations:90701 DTP is deleted90718 Td is deleted
The influenza vaccine series of 90653, 90672, 90685, 90686, 90687, 90688 are new codes for products that are to be used in the future (Quadrivalent vaccines) and should be reviewed for your use in the office/clinic when they become available.
2013 Update Psychiatry and Psychotherapy has been
extensively revised.
90862 has been deleted and replaced with both E/M codes and psychotherapy codes with and without evaluation and management services. (99304 – 99337; 99341 -99350)
90863 Pharmacologic management including prescription and review of medication, when performed with psychotherapy services. Use in addition to the code for the primary procedure.
4/15/2013
10
2013 Update Allergy and Clinical Immunology
This section has been extensively revised and new codes have been added. Ingestion Challenge testing code 95075 has been deleted and replaced with 95076 and 95079. These are for the first 120 minutes of the challenges and for every 60 minutes thereafter.
Many codes are no longer being paid by Medicare and this may affect Medicaid and other insurers.
2013 Update Neurology and Neuromuscular Procedures
Sleep Medicine services are now divided into those of any age with 1-3 parameters of sleep (95808) and those 6 years and older with 4 parameters of sleep (95810) and those 6 years and older with 4 parameters with CPAP or BiPAP (95811).
95782 for those less than 6 years of age with 4 parameters and 95783 for those less than 6 years and with CPAP or BiPAP.
2013 Update
Visual testing added:99174 for Instrument-based ocular
photoscreening with interpretation and report.
4/15/2013
11
2013 Update
ICD-9-CM is in effect until October 1, 2014.
There are no new codes in the last year or until ICD-10-CM will begin.
Evaluation and Management Guidelines
Five sets: CPT; CMS in 1995, 1997; PATH; Incident to billing.
The CPT guidelines are in the 2013 CPT book. These are basic but give an appreciation of the way to use the system.
CMS is separate from CPT guidelines and more descriptive/restrictive.
Evaluation and Management Guidelines
The 1995 guidelines were the first attempt to set up more rigorous documentation that physicians need to complete in order to use specific codes.
The 1997 guidelines further refined the 1995 ones by making primarily the physical exam components more specific and by defining the number of elements to complete to satisfy documentation.
4/15/2013
12
Evaluation and Management Guidelines
PATH stands for Physicians at Teaching Hospitals.
These essentially follow the other guidelines but add the supervision of student and resident physicians in both hospitals and outpatient settings in evaluating which codes to use.
The Medicare Part B “Supervising Physicians in Teaching Settings” is the de facto national standard from which this is derived.
Evaluation and Management Guidelines
The definitions, payment, documentation scenarios, billing procedures, use of diagnostic tests, high risk procedures, psychiatry, time based codes, exceptions and the rest of the criteria for the use of these codes is available at the CMS website in the Carriers Manual Part 3.
Evaluation and Management Guidelines
“Incident to” billing means “services incident to the service of a physician or other professional permitted by statute to bill for services… when those services meet all the requirements applicable to the benefit.”
Incident-to billing is state specific as well as Medicare, Medicaid, and CMS defined.
The QHCP bills under the NPI of the physician.
4/15/2013
13
Evaluation and Management Guidelines
This set of guidelines is also sited in the CMS website under “Incident to” billing.
In some states an QHCP is able to bill independently. This is not “incident to” billing. They are paid on a different schedule which is usually 85% of the physician’s.
Evaluation and Management Guidelines
The process is to improve documentation.
The medical record is set up to be a chronologic document of care provided by multiple people through separate events or historical items related to the individual’s health.
It should reduce the hassles of claim processing and may serve as a legal document to verify care provided.
Evaluation and Management Guidelines
The record should be complete and legible. The documentation should follow a pattern or
template and include seven different areas with specific components completed.
If not documented, the rational for ordering a diagnostic or ancillary service must be easily inferred.
Past and present diagnoses should be accessible in the record as well as appropriate health risk factors and assessments.
4/15/2013
14
Evaluation and Management Guidelines
The patient’s progress, response to and changes in treatment and revision of diagnosis should be documented.
All of these general guidelines should be reported through the use of the CPT and ICD-9-CM systems when billing.
A reviewer should be able to identify the patient’s status through the documentation and correlate it to the billing.
Evaluation and Management Guidelines
In order to do the last step efficiently, insurance companies and the government have developed systems to process your claims.
These are called “Claims analysis software”. This software uses a specific set of quality
and quantity items to analyze your claim. If you fit the analysis, the claim goes through. If not, the claim is further reviewed by asking for more data.
Evaluation and Management Guidelines
That data is then manually reviewed and consideration is given to its influence on the original code used.
After that evaluation, your total pattern of coding is identified and reviewed to see whether you follow the standardized curve (bell curve) or not.
High level coders (up-coding) are compared to standard coders and are monitored.
4/15/2013
15
Evaluation and Management Guidelines
Low level coders (under-coding) are not further monitored but create more profit for the insurer or savings for the government.
The problem obviously is to get it correct to begin with and then avoid the hassles.
All of this process is kept up to date through the National Correct Coding Initiatives (NCCI) which gives input to the use of specific codes. Think of the NCCI edit that we are now going through with 90460-61.
Evaluation and Management Guidelines
NCCI edits were developed by CMS for Medicare but are now used by most insurers and Medicaid.
Examples include doing two procedures which cannot possibly be done at the same session. Having an initial and subsequent service reported on the same date of service. Gender-specific codes are also included
Evaluation and Management Guidelines
NCCI edits may be overridden by a modifier but have to be on their list.
Example is 25 modifier for immunizations given during preventative or problem oriented visits.
www.cms.hhs.gov/NationalCorrectCodInitEd
4/15/2013
16
Evaluation and Management Guidelines
Sometimes you may want to have an additional review when your patient mix shows a more complex group than the usual.
The problem is that many physicians think they take care of sicker patients but when the data is reviewed, they don’t.
This is then a red flag to the insurer to review and ask for additional data on that physician’s claims to get him/her back in line.
Evaluation and Management Guidelines
Routine audits are standard and required by insurers.
HEDIS audits are an example which everyone goes through.
Claims audits by insurers or the government may be infrequent but are usually a sign that your practice is unusual. Not good or bad but different than the standard. Their job is to find out why.
Evaluation / Management Codes
There are 20 categories of E/M codes.
How many do you use routinely?
What type of practice do you have?
Is there an opportunity to expand your E/M category usage?
Do you want to limit your codes to be more restrictive in the type of patients you see?
4/15/2013
17
Evaluation / Management Codes
Office or other outpatient services
Hospital observation services
Hospital inpatient services
Consultations
Emergency Department services
Critical Care services
Nursing facility services
Evaluation / Management Codes
Domiciliary, rest home or custodial care
Home care
Prolonged physician services
Case management
Care plan oversight
Preventative medicine
Non-face-to-face physician services
Evaluation / Management Codes
Special E/M services
Newborn care
Inpatient neonatal intensive care
Pediatric and neonatal critical care
Other E/M services
4/15/2013
18
Evaluation / Management Codes
The E/M code used is not dependent on the diagnosis code used.
The code used should be reported based on the services provided and documented in the medical record.
Evaluation / Management Codes
All E/M codes have seven components which are divided into Key components, Contributory factors and Explicit components.
Evaluation / Management Codes
The Key ones are: 1. History2. Physical Examination3. Medical Decision Making
The Contributory ones are: 4. Counseling5. Coordination of Care6. Nature of the Presenting Problem
The Explicit component is: 7. Time
4/15/2013
19
Evaluation / Management Codes
History has four elements:1. Chief Complaint2. History of the present illness3. Review of Systems4. Past, family and social history
Evaluation / Management Codes
Chief ComplaintThe reason for the encounter. May be a quote of the patient’s or parent’s words.
Evaluation / Management Codes
History of the present illnessUsually need at least three elements which should describe the illness from the onset of the problem or from the last patient encounter to the present.
It has to be pertinent to the CC.
Have a choice of eight elements to help describe this component which must be obtained and documented by the physician.
4/15/2013
20
Evaluation / Management Codes
Elements of the HPI:1. Location – anatomic site of symptom2. Duration of symptom3. Timing of occurrence, number of signs
or frequency of symptoms4. Quality of sign or symptoms5. Severity – Acuteness or intensity6. Context situation in which sign occurs7. Modifying factors8. Associated signs and symptoms
Evaluation / Management Codes
Review of Systems is a series of questions to better define the CC and help establish a diagnosis and plan.
It has up to thirteen components in the inventory of systems.
Both positive and negative responses must be documented.
Evaluation / Management Codes
Components of the ROS:1. Constitutional (fever, weight loss, etc.)2. Eyes3. Ears, nose, mouth, throat4. Cardiovascular5. Gastrointestinal6. Genitourinary7. Musculoskeletal8. Integumentary (skin and or breast)
4/15/2013
21
Evaluation / Management Codes
Components of the ROS cont.:9. Neurologic10. Psychiatric11. Endocrine12. Hematologic / lymphatic 13. Allergic / immunologic
Evaluation / Management Codes
Although it may seem like there is a crossover of information obtained from the HPI and the ROS, this data is not usable in each section simultaneously. It should be in one or the other section.
Evaluation / Management Codes
Past, Family and Social history as related to the CC. Usually need two of the three areas covered but for a comprehensive history will need all three covered.
4/15/2013
22
Evaluation / Management Codes
Past History as related to medical and surgical history for the CC. May Include:
1. Illnesses and/or hospitalizations2. Injuries3. Surgeries4. Current meds5. Allergies6. Immunizations7. Age appropriate feeding history/dietary
status
Evaluation / Management Codes
PFSH cont.:8. Pregnancy history9. Birth history (weight , APGAR, etc)10. Developmental history11. Sexual history
Evaluation / Management Codes
Family History includes:1. Health status or cause of death of
family members2. Specific diseases of family members
that may place the patient at risk or has to do with the CC.
3. Hereditary disorders in the family
4/15/2013
23
Evaluation / Management Codes
Social History includes an age appropriate review of activities as they relate to the CC
1. Review of living arrangements2. Use of drugs, alcohol, or tobacco by the
patient or caregiver3. Childcare arrangements4. Education level5. Domestic violence and/or child abuse
Evaluation / Management Codes
The history obtained then falls into one of four levels:
1. Problem Focused2. Expanded Problem Focused3. Detailed Problem Focused4. Comprehensive
Evaluation / Management Codes
The Physical exam is the next area to be documented, reviewed, and given a specific level.
The PE is divided into seven body areas and eleven organ systems.
There are four levels of physical exam defined in the same way as the history. (Problem focused, Expanded, Detailed, and Comprehensive)
4/15/2013
24
Evaluation / Management Codes
Body areas:1. Head, including the face2. Neck3. Chest, including breasts and axilla4. Abdomen5. Genitalia, groin, buttocks6. Back7. Each extremity
Evaluation / Management Codes
Organ systems:1. Eyes2. Ears, nose, mouth, throat3. Cardiovascular4. Respiratory5. Gastrointestinal
6. Genitourinary (female and male)7. Musculoskeletal8.Skin
Evaluation / Management Codes
Organ systems cont.:9. Neurologic10. Psychiatric11. Hematologic, lymphatic, and
immunologic
4/15/2013
25
Evaluation / Management Codes
The differences in the 1995 versus the 1997 physical exam are in the details.
Example: 1995 exam of the abdomen is one element if the abdominal exam is marked. The 1997 exam includes the specific elements of the abdominal exam with the liver, spleen and hernias being evaluated and counting for three elements of an examination.
Evaluation / Management Codes
The problem of doing a full PE on each patient is that the parts of the exam that count relate to the CC.
If you come in with a CC of abdominal pain and the examination includes the ENMT body area, then they won’t count for the complexity of the visit unless you show why it relates in your documentation. (Strep with abdominal pain)
Evaluation / Management Codes
Generally the physicians within a group should all document the same way. If there is a difference, this should be documented in a set of written policies for your practice which can be referred to in case of an audit. (Three doctors use the 1997 guidelines and one uses the 1995)
As a general rule, the 1995 guidelines favor the general pediatrician while the 1997 favors the specialist exam.
4/15/2013
26
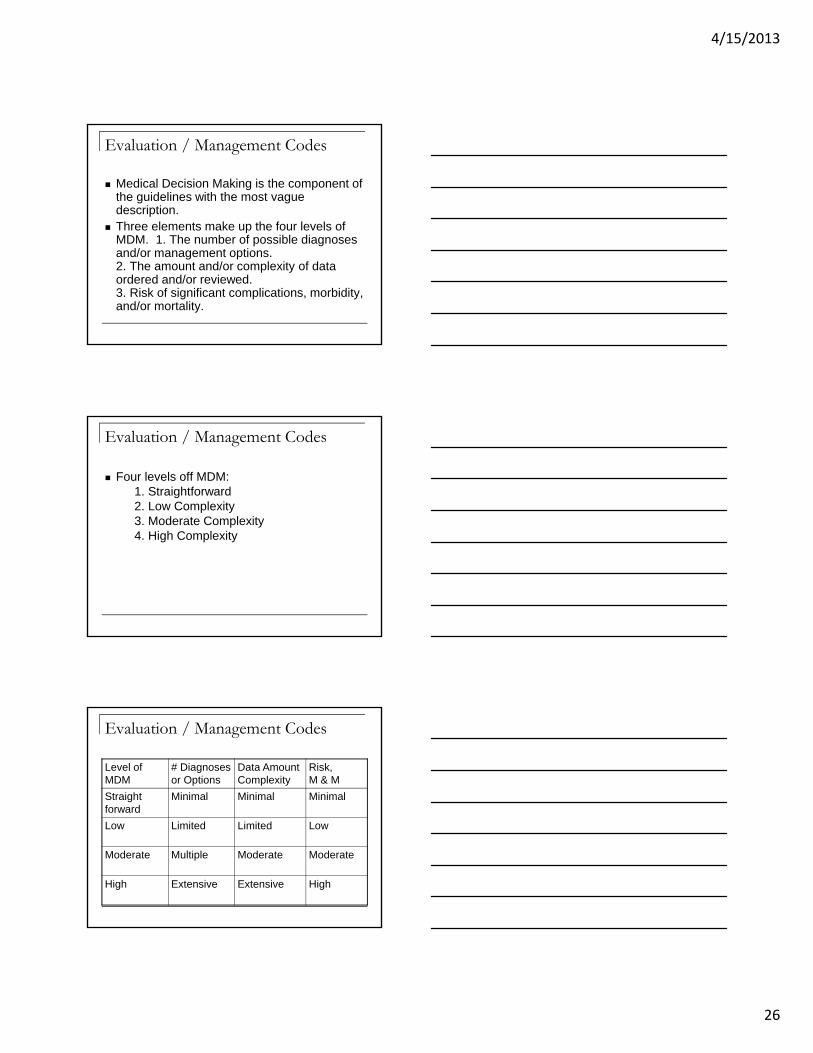
Evaluation / Management Codes
Medical Decision Making is the component of the guidelines with the most vague description.
Three elements make up the four levels of MDM. 1. The number of possible diagnoses and/or management options.2. The amount and/or complexity of data ordered and/or reviewed.3. Risk of significant complications, morbidity, and/or mortality.
Evaluation / Management Codes
Four levels off MDM:1. Straightforward2. Low Complexity3. Moderate Complexity4. High Complexity
Evaluation / Management Codes
Level of MDM
# Diagnoses or Options
Data Amount Complexity
Risk, M & M
Straight forward
Minimal Minimal Minimal
Low Limited Limited Low
Moderate Multiple Moderate Moderate
High Extensive Extensive High
4/15/2013
27
Evaluation / Management Codes
The Risk is evaluated by:1. The presenting problem (self limited,
acute, chronic and the number of them).
2. Diagnostic procedure(s) ordered3. Management options
A list is shown at the CMS website and on page 30 of the book, Coding for Pediatrics, 2013.
Evaluation / Management Codes
This area has many caveats that people have tried to assign and been denied.
Example is that a drug prescription constitutes moderate level MDM. It does not by itself because the level has to be met by fulfilling two of the three components.
Management options are supported with documentation of the problems addressed, patient’s progress and response to treatment and the plan of care.
Evaluation / Management Codes
Time is the last area to evaluate in the process of E/M coding.
It can only be used as the controlling factor when counseling, coordination of care, or both account for more than 50% of the physician face-to-face time with a patient.
Otherwise use the other factors we have already discussed.
4/15/2013
28
Evaluation / Management Codes
Guidelines include:1. The time spent must be face to face.2. Floor/unit time in the hospital includes
the time at the patient’s bedside, time spent counseling the family/patient, time spent on the floor writing notes, and time spent coordinating care with the nurses or other team members.
Evaluation / Management Codes
Guidelines cont.:3. Time spent in counseling may be with
the patient, family, and/or those responsible for the patient.
4. Counseling refers to activities which are not procedures and include discussions about a condition and/or its management.
5.Time on a date does not have to be continuous.
Evaluation / Management Codes
Guidelines cont.:6. Only providers with an NPI may submit
for time related codes.7. Report the code with the time closest to
the actual time spent, eg, if you spent 35 minutes on an office visit, use code 99215 as it has 40 minutes as its time specified.
8. The chosen code has to have a time assigned to it.
4/15/2013
29
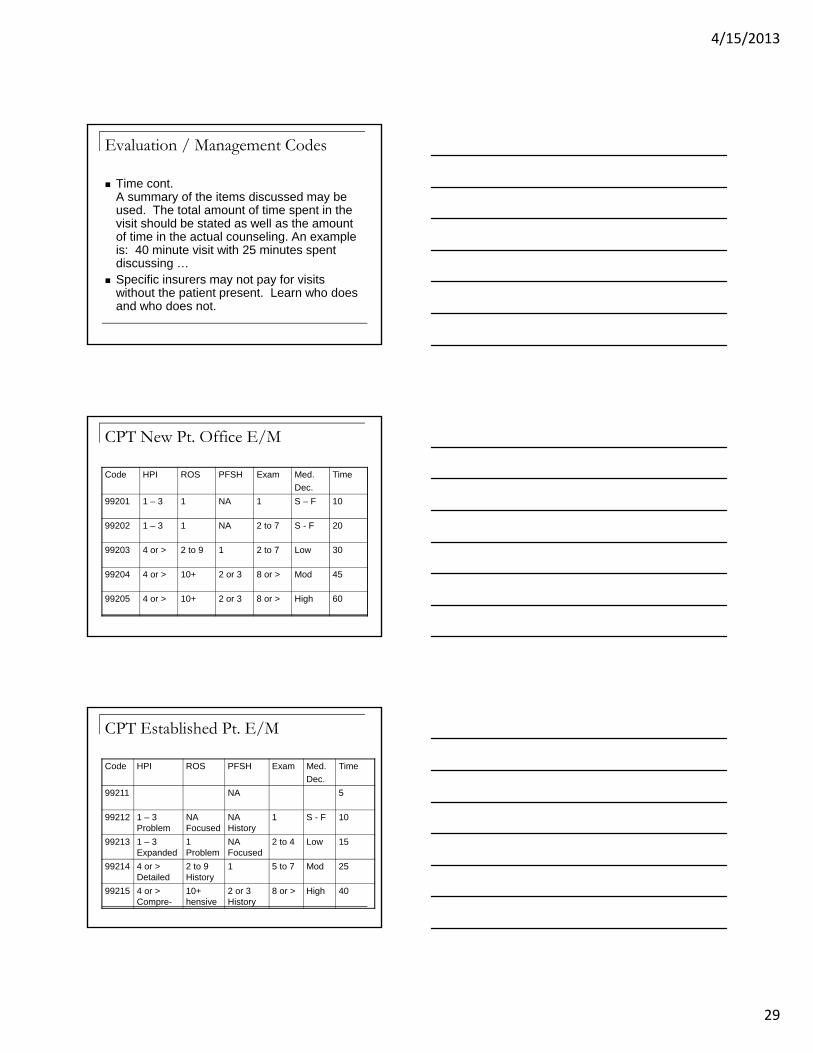
Evaluation / Management Codes
Time cont.A summary of the items discussed may be used. The total amount of time spent in the visit should be stated as well as the amount of time in the actual counseling. An example is: 40 minute visit with 25 minutes spent discussing …
Specific insurers may not pay for visits without the patient present. Learn who does and who does not.
CPT New Pt. Office E/M
Code HPI ROS PFSH Exam Med.
Dec.
Time
99201 1 – 3 1 NA 1 S – F 10
99202 1 – 3 1 NA 2 to 7 S - F 20
99203 4 or > 2 to 9 1 2 to 7 Low 30
99204 4 or > 10+ 2 or 3 8 or > Mod 45
99205 4 or > 10+ 2 or 3 8 or > High 60
CPT Established Pt. E/M
Code HPI ROS PFSH Exam Med.
Dec.
Time
99211 NA 5
99212 1 – 3 Problem
NA Focused
NA History
1 S - F 10
99213 1 – 3 Expanded
1 Problem
NA Focused
2 to 4 Low 15
99214 4 or > Detailed
2 to 9 History
1 5 to 7 Mod 25
99215 4 or > Compre-
10+ hensive
2 or 3 History
8 or > High 40
4/15/2013
30
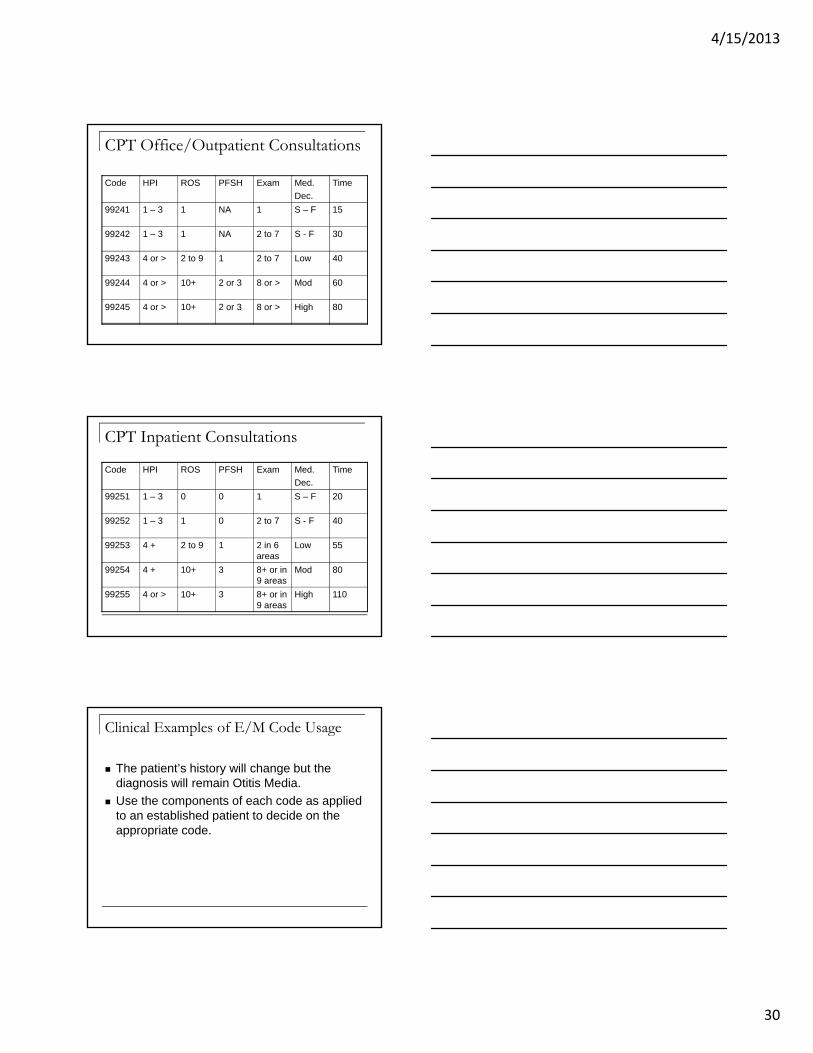
CPT Office/Outpatient Consultations
Code HPI ROS PFSH Exam Med.
Dec.
Time
99241 1 – 3 1 NA 1 S – F 15
99242 1 – 3 1 NA 2 to 7 S - F 30
99243 4 or > 2 to 9 1 2 to 7 Low 40
99244 4 or > 10+ 2 or 3 8 or > Mod 60
99245 4 or > 10+ 2 or 3 8 or > High 80
CPT Inpatient Consultations
Code HPI ROS PFSH Exam Med.
Dec.
Time
99251 1 – 3 0 0 1 S – F 20
99252 1 – 3 1 0 2 to 7 S - F 40
99253 4 + 2 to 9 1 2 in 6 areas
Low 55
99254 4 + 10+ 3 8+ or in 9 areas
Mod 80
99255 4 or > 10+ 3 8+ or in 9 areas
High 110
Clinical Examples of E/M Code Usage
The patient’s history will change but the diagnosis will remain Otitis Media.
Use the components of each code as applied to an established patient to decide on the appropriate code.
4/15/2013
31
Clinical Examples of E/M Code Usage
Nursing evaluation of a follow-up on a previous otitis media with a tympanogram (92567) and/or audiogram (92551).
Code ?
Clinical Examples of E/M Code Usage
Nursing evaluation of a follow-up on a previous otitis media with a tympanogram (92567) and/or audiogram (92551).
99211
Clinical Examples of E/M Code Usage
F/U otitis media with primary exam limited to the ears. History problem focused; PE problem focused; MDM straightforward
Code ?
4/15/2013
32
Clinical Examples of E/M Code Usage
F/U otitis media with primary exam limited to the ears. History problem focused; PE problem focused; MDM straightforward
99212
Clinical Examples of E/M Code Usage
2 yr. old with pinkeye and URI recently. History expanded problem focused; PE expanded problem focused; MDM moderate low complexity.
Code ?
Clinical Examples of E/M Code Usage
2 yr. old with pinkeye and URI recently. History expanded problem focused; PE expanded problem focused; MDM moderate low complexity.
99213
4/15/2013
33
Clinical Examples of E/M Code Usage
Infant with suspected third AOM within 2-3 months with fever and cough. History detailed; PE detailed; MDM moderate complexity.
Code ?
Clinical Examples of E/M Code Usage
Infant with suspected third AOM within 2-3 months with fever and cough. History detailed; PE detailed; MDM moderate complexity.
99214
Clinical Examples of E/M Code Usage
3 month old with fever, vomiting, irritability. History comprehensive; PE comprehensive; MDM high complexity and time spent as 40 minutes.
Code ?
4/15/2013
34
Clinical Examples of E/M Code Usage
3 month old with fever, vomiting, irritability. History comprehensive; PE comprehensive; MDM high complexity and time spent as 40 minutes.
99215
Clinical Examples of E/M Code Usage
The following are Asthma diagnoses for the continuum of E/M codes.
Given the following case histories what CPT code would you assign to each case ?
Clinical Examples of E/M Code Usage
8 year old with known unstable asthma is having an acute exacerbation; already receiving inhaled albuterol and inhaled steroids by MDI. History is detailed; PE is detailed; MDM is moderate
Code ?
4/15/2013
35
Clinical Examples of E/M Code Usage
8 year old with known unstable asthma is having an acute exacerbation; already receiving inhaled albuterol and inhaled steroids by MDI. History is detailed; PE is detailed; MDM is moderate
99214
Clinical Examples of E/M Code Usage
Follow-up visit for a 9 year old with stable asthma who is in good health. History is problem focused; PE is problem focused; MDM is straightforward.
Code ?
Clinical Examples of E/M Code Usage
Follow-up visit for a 9 year old with stable asthma who is in good health. History is problem focused; PE is problem focused; MDM is straightforward.
99212
4/15/2013
36
Clinical Examples of E/M Code Usage
Follow-up visit for child with stable chronic asthma using an steroid MDI and beta agonist as needed. History is expanded problem focused; PE is expanded problem focused; MDM is low complexity.
Code ?
Clinical Examples of E/M Code Usage
Follow-up visit for child with stable chronic asthma using an steroid MDI and beta agonist as needed. History is expanded problem focused; PE is expanded problem focused; MDM is low complexity.
99213
Clinical Examples of E/M Code Usage
1 year old known to have recurrent wheezing following an RSV infection. Is having increasingly frequent attacks over the last two months. CXR shows new infiltrates. Sweat test from last week is positive. History is comprehensive; PE is comprehensive; MDM is high complexity.
Code ?
4/15/2013
37
Clinical Examples of E/M Code Usage
1 year old known to have recurrent wheezing following an RSV infection. Is having increasingly frequent attacks over the last two months. CXR shows new infiltrates. Sweat test from last week is positive. History is comprehensive; PE is comprehensive; MDM is high complexity.
99215
Clinical Examples of E/M Code Usage
Nurse reviews inhaler technique (94664) and obtains PEF’s for a 10 year old patient. She discusses disease management with the mother and teaches the patient home monitoring.
Code ?
Clinical Examples of E/M Code Usage
Nurse reviews inhaler technique (94664) and obtains PEF’s for a 10 year old patient. She discusses disease management with the mother and teaches the patient home monitoring.
99211 (plus the 94664 already in the history).
4/15/2013
38
Clinical Examples of E/M Code Usage
A clinical scenario can be created for every type of illness or problem that you see.
What code do you use when the history obtained, the PE done or the MDM doesn’t fit into the nice components as listed in the charts ?
Established office visit; History problem focused; PE detailed; MDM expanded problem focused.
Clinical Examples of E/M Code Usage
Audits reveal that the least amount of information obtained in any one section guides the code to be used for the visit.
In the example, the lowest code, 99212, is used. This creates a lot of confusion for people who
feel that they spent a lot of time with the patient. The solution is to use time as the factor to figure
out your code. (If > 50% of the visit is spent counseling).
Newborn Codes
Newborns should be coded one of four ways depending on their status.
Normal newbornsHospitalized newbornsIntensive care newbornsCritical care newborns
4/15/2013
39
Normal Newborns
99460 Normal Newborn Admission, hospital or birthing center
99461 Normal Newborn, initial care other than in a hospital or birthing center
99462 Subsequent hospital daily care of the normal newborn
99463 24 hour care of the hospital or birthing center normal newborn
99238 Discharge day care of the hospitalized newborn
Hospital care of the Admitted newborn with a problem 99221 Low complexity Admission of the
hospitalized newborn
99222 Moderate complexity of the hospitalized newborn
99223 High complexity of the hospitalized newborn
Daily hospital care of a hospitalized newborn with a problem 99231 Low complexity daily care of a
hospitalized newborn
99232 Moderate complexity daily care of a hospitalized newborn
99233 High complexity daily care of a hospitalized newborn
Procedure codes may be added to these daily charges.
4/15/2013
40
Intensive care of the Hospitalized Newborn 99477 Initial hospital care of the E/M of the neonate,
28 days of age or younger, who requires intensive observation, frequent interventions, and other intensive care services
This set of codes is inclusive of the following vascular procedures: 36000 Peripheral vessel cath; 36140,36620 other arterial catheters; 36510 UVC; 36555 Central vessel cath; 36400,36405,36406 Vascular access procedures; 36420, 36600 Vascular punctures; 36660 UAC
Intensive care of the Hospitalized Newborn It includes airway and ventilation
management codes: 31500 Endotracheal intubation; 94002-04 Vent. management; 94375 bedside pulmonary function testing; 94610 Surfactant administration; 94660 CPAP
94760-62 ABG’s
36430. 36440 Tx of blood components
43752 OG or NG tube placement
Intensive care of the Hospitalized Newborn 51100 Suprapubic Tap 51701,51702 Bladder Catheterization 62270 Lumbar Puncture
99291-92 Critical care codes by time
4/15/2013
41
Intensive care of the Hospitalized Newborn
99291-92 Can be used: 1. in the outpatient setting, 2. if the physician is at the
referring hospital setting3. if they are a second physician
of a different specialty who is not reporting a per-day neonatal critical care code
Intensive care of the Hospitalized Newborn 99478 Subsequent intensive care, per day,
for the E/M of the infant < 1500 grams
99479 Subsequent intensive care, per day, for the E/M of the infant 1500 – 2500 grams
99480 Subsequent intensive care, per day, for the E/M of the infant 2500 – 5000 grams
Critical Care of the Hospitalized Newborn
99468 Initial inpatient neonatal critical care
99469 Subsequent inpatient neonatal critical care, per day for the E/M of the critically ill neonate, 28 days of age or less
99471 Initial critical care of inpatient 29 days to 24 months of age
99472 Subsequent inpatient critical care, per day for the E/M of the critically ill neonate, 29 days of age to 24 months of age
4/15/2013
42
KanCare
Medicaid HMO program for the state of Kansas
Administered through three carriers:Amerigroup: www.amerigroup.comSunflower State: www.sunflowerstatehealth.comUnited Community: www.uhccommunityplan.com
Each has their own set of rules but they are built from the KMAP system.
KanCare
AmeriGroup and United follow the NCCI edits but Sunflower State uses the McKesson X10 edits.
This is why there are some differences in the coding requirements between the individual companies.
It is very important to go to their websites and review their updates and get educated on their systems.
KanCare
The EPSDT program in Kansas is called KAN Be Healthy.
Each of the insurance administrations use this system in providing preventative care to their patients.
There are multiple methods to code for preventative care. These are outlined in the KAN Be Healthy Billing Bulletin on the KMAP website.
4/15/2013
43
KanCare
A key change in KBH billing from the 6/11 Update is to use the EP modifier on preventative care codes (99381-85 or 99391-95) or on office visit codes (99202-05 or 99213-15). These must use a “V” ICD-9-CM diagnosis code to be reimbursed and have the KBH become updated.
Three billing options are given as examples.
For those billing without the EP modifier, reimbursement is less.
KanCare
In addition to modifying the well care codes with an EP, in order to have the 90460 – 61 get paid by AmeriGroup, and United use -25 as well. (And 90471-72)
Sunflower will pay for 90460 when modified with -25 but will not pay for 90461 even when modified.
Keep monitoring these as the companies will have pressure put on them by users of the system.
KanCare
KBH uses the AAP periodicity schedule for preventative visits.
KBH provides a form for providers to fill out and requires the form be completed for all EPSDT visits.
Documentation is a key in audits and is compared to the codes which have been billed.
Audits may be educational or punitive.
4/15/2013
44
KanCare
The Billing Bulletin has updates that are done quarterly through the KAN BE Healthy Provider Manual at the KMAP website: www.kmap-state-ks.us/Public/Bulletins/BulletinSearch
The majority of the changes which have occurred this year were in the 01.2013 update. The updates from multiple previous quarters are listed in the most recent update. (The dates of those are marked as “Issued 3/10” or “Updated 06/11”).
KanCare
As this reference is continuously being revised, it is imperative for you to keep up to date with it or be behind in the changes and as a result potentially needing to revise, re-submit billings and therefore delay payments.
Check this weekly as there are new revisions that are helpful to you and may explain why a claim has been paid at a certain rate or not been paid as expected.
KanCare
In order to be up to date with the reimbursement schedule, one needs to go to the KMAP website and log in. After going through their steps you can get the updated schedule by going to the “Pediatric Fee Schedule” and click on it to download the most current one. (Usually updated monthly but doesn’t change much.)
4/15/2013
45
Questions and Problems
References
CPT 2013
Coding for Pediatrics 2013, 18th edition
AAP.org
CMS.gov