Embed Size (px)
Citation preview

Critical review
Page 1 of 8
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Stevic R, Dodic M. Ultrasonography of tendon abnormalities. OA Musculoskeletal Medicine 2013 Jun 01;1(2):12.
Ultrasonography of tendon abnormalities
R Stevic1,2*, M Dodic3
AbstractIntroductionTendon abnormalities are common musculoskeletal disorders. Accu-rate and timely diagnosis of tendon abnormalities is essential to ensure proper treatment and to prevent tendon disability. The purpose of this critical article is to describe the sono-graphic characteristic of different tendon abnormalities.Material and methodsA retrospective review of ultra-sonography images of patients with different tendon abnormalities was conducted and the results of analysis were compared with the published literature data.ResultsThe study included 149 patients (105 male patients, 44 female patients), with average age of 47.4 ± 16, with 157 affected tendons. The most affected tendon in our patients was supraspinatus tendon, followed by Achilles tendon and patellar ligament. Dominant patho-logic finding was tendinosis in 83 cases, with chronic tendinosis to be more frequent. Partial-thickness tear was detected in 35 cases, the most common occurred in supraspi-natus tendon. Full-thickness tear was revealed in 11 patients, with Achilles tendon being the most common. Tenosynovitis was diagnosed in 18 cases. In 8 of 13 cases, tenosynovitis of long head of the biceps tendon
was associated with abnormalities of the supraspinatus tendon. In five cases, tenosynovitis of wrist and hand tendons was detected. Tendon tumour was detected in 10 patients, seven ganglion cysts and three giant cell tumours of tendon sheath. Results of our study are similar to those in the published literature data.DiscussionMusculoskeletal sonography is well suited for evaluating tendons. In most cases, its accuracy is at least equivalent to that of magnetic reso-nance imaging for imaging tendon abnormalities. But the advantages of sonography, such as accessibility, low cost, dynamic capability and needle guidance make it as a first-line imaging technique in tendons evalu-ation. Although operator dependence is an often quoted disadvantage of sonography, experienced musculo-skeletal radiologists can perform effective tendon evaluation and quickly detect the abnormality.ConclusionUltrasound is an efficient and accu-rate imaging method for evaluation of tendon abnormalities. Like magnetic resonance imaging, ultrasonography is a technique that affords anatomic images in multiple planes and that may provide information about tissue characterisation.
IntroductionTendons are frequently affected by a wide range of inflammatory, degen-erative and traumatic processes. The spectrum of pathologic changes includes tendinosis, tenosynovitis and partial or complete tear. Ultrasonog-raphy (US) is a reliable, non-invasive, widely available and inexpensive imaging modality of choice for tendon examination. It combines direct multiplanar, tomographic evalua-tion of the tendons with dynamic
investigation of their movement and provides both an anatomic and a functional assessment. Experienced musculoskeletal radiologists can easily diagnose most basic lesions as a tendon sheath widening, peritend-initis, calcific and/or degenerative changes and tendon tears. Accurate and timely diagnosis of musculo-skeletal tendon abnormalities, espe-cially injuries is critical to ensure proper treatment and thus, minimise possible tendon disability1,2.
This critical review examines the US appearance of normal tendon anatomy, as well as the US appearances of different presentations of tendon injuries and non-traumatic conditions.
Material and methodsWe conducted a retrospective review of US images of patients, with different tendon abnormalities and compared the results of analysis with the published literature data.
ResultsThis study included 149 patients, including 105 male patients and 44 female patients, with average of 47.4 ± 16 years with 157 affected tendons. One half of the patients were aged between 45 years and 65 years. The most affected tendon in our patients was the supraspinatus tendon, followed by Achilles tendon and patellar ligament. Dominant pathologic finding was tendinosis in 83 cases, with chronic tendi-nosis to be the more frequent ones. Partial-thickness tear was detected in 35 cases, most frequently on the supraspinatus tendon. Full-thickness tear was revealed in 11 patients, with Achilles tendon being the most common. Tenosynovitis was diag-nosed in 18 cases, including 13 cases of long head of biceps tendon and five cases of wrist tendons (three cases
* Corresponding authorEmails: [email protected], [email protected] Faculty of Medicine, University of Belgrade,
Dr Subotica 8, 11000 Belgrade, Serbia2 Center of Radiology and Magnetic Resonance
Imaging, Clinical Centre of Serbia, Pasterova 2, 11000 Belgrade, Serbia
3 Radiology Practice, Rige od Fere 22, 11000 Belgrade, Serbia
Dia
gnosi
s
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Stevic R, Dodic M. Ultrasonography of tendon abnormalities. OA Musculoskeletal Medicine 2013 Jun 01;1(2):12.
Critical review
Page 2 of 8
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
on flexor and two cases on extensor tendons). In 8 of the 13 cases, teno-synovitis of long head of biceps tendon was associated with abnor-
malities of supraspinatus tendon. In 10 patients, tendon tumour was detected, including seven ganglion cysts and three giant cell tumours of
tendon sheath (Table 1). Results of our study are similar to those in the published literature data.
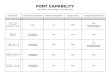
DiscussionUltrasonography appearance of nor-mal tendonsFor adequate diagnostic evaluation, shape, contour and echo texture of tendon, must be carefully analysed. Sonographic appearance of tendons has the basis in their anatomy. Tendons are strong bundles of parallel, dominantly type I collagen fibres, and this internal architecture is clearly visualised on conventional examination, when the ultrasound beam is perpendicular to the tendon. Tendon echogenicity decreases artificially, if the angle between tendon and ultrasound beam is higher or lower than 90° (anisot-ropy). On longitudinal scans, normal tendons appear as tightly packed echoic structures with fine parallel internal linear echoes (fibrillar pattern) separated by fine anechoic lines2,3. Tendon contour is regular and sharply defined (Figure 1A). On
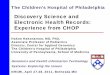
Table 1 The frequency of pathologic fi ndings of tendons.
Tendon Acute tendinosis
Chronic tendinosis
Tenosynoviti s Complete tear
Parti al tear
Ganglion GCTTS* Total
Supraspinatus 5 33 0 5 21 64
Achilles tendon 5 6 0 5 6 22
Patellar ligament 9 6 0 0 2 17
Quadriceps tendon 4 6 0 1 3 14
LHBT** 0 1 13 0 0 14
Common extensor 4 0 0 0 0 0 4
Adductor magnus 4 0 0 0 0 0 4
Wrist 0 0 5 0 0 4 9
Ankle 0 0 0 0 0 2 2 4
Knee 0 0 0 0 0 1 1 2
Others*** 0 0 0 0 3 0 0 3
Total 31 52 18 11 35 7 3 157
* GCTTS, giant cell tumour of tendon sheath.** LHBT, long head of biceps tendon.*** Soleus, peroneus longus and tibialis posterior tendon.
Figure 1A: Normal sonograms of the Achilles tendon in a 24-year-old man. Longitudinal sonogram shows normal fibrillar pattern (arrows), calcaneal insertion (C) and minor anisotropy (arrowhead).

Critical review
Page 3 of 8
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Stevic R, Dodic M. Ultrasonography of tendon abnormalities. OA Musculoskeletal Medicine 2013 Jun 01;1(2):12.
transverse scans, tendons appear as oval-to-round structures character-ised by tightly packed echoic dots, with a homogeneous distribution
(Figure 1B). A thin anechoic layer, of synovial fluid surrounding tendons, with synovial sheath, can be visual-ised with very-high-frequency trans-
ducers (13–20 MHz). Sonographic confirmation of the presence of tendon abnormality should always be obtained by comparing longi-tudinal and transverse scans. This is the best way to avoid pitfalls and artefacts because of incorrect angu-lation between the ultrasound beam and the tendon. Tendons should be examined with the patient at rest and during active and/or passive motion. Colour Doppler and power Doppler capability of sonography can give important information about hyper-aemia that can be associated with inflammation and solid tumours1,4,5.
Ultrasound appearances of tendon abnormalitiesTendinosisGenerally, the most common patho-logic conditions affecting the tendons are tendinopathies and the frequency of these conditions depends on investigated groups. The sportsmen experience acute tendinosis and tendon tears more frequent than others. In the general population, tendinopathies are caused by repeti-tive microtrauma and age-related changes. While tendinosis refers to the structural changes of degen-eration seen histologically or with imaging, tendinopathy is a clinical term describing tendon pain and swelling3,4,6,7. Ultrasound appearance of tendinosis depends on extensity and the time between injury and sonographic evaluation. In acute tendinosis, initially, tendon is thick-ened, with normal contour and echo structure. As the process progresses, the fibrillar pattern is lost and tendon becomes hypoechoic, with further swelling (Figure 2). Discrete focal hypoechoic areas may repre-sent small partial tears, which may not extend to the tendon surface. But if a defect is present on the tendon surface, dynamic evaluation (i.e., during movement) should be performed to rule out partial tear5,7,8. Increased Doppler flow can point to hyperaemia that can be associated with tendinopathy2,9. The presence
Figure 1B: Transverse sonogram shows normal echogenic tendon (arrows) and Kager’s fat pad (K).
Figure 2: Acute Achilles tendinosis. (A) Longitudinal sonogram of a patient, who has achillodynia shows fusiform enlargement of the central tendon. The tendon is hypoechoic, inhomogeneous throughout most of its course. (B) Altered morphology of the tendon in short axis.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Stevic R, Dodic M. Ultrasonography of tendon abnormalities. OA Musculoskeletal Medicine 2013 Jun 01;1(2):12.
Critical review
Page 4 of 8
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
of neovascularity in the degenerated tendon has been suggested as a cause of pain, but Zanetti et al. showed that this sign has no role in outcome prediction10.
In our patients, the most common tendon affected by acute tendinosis was the patellar tendon followed by Achilles tendon, common extensor tendon of elbow and quadriceps
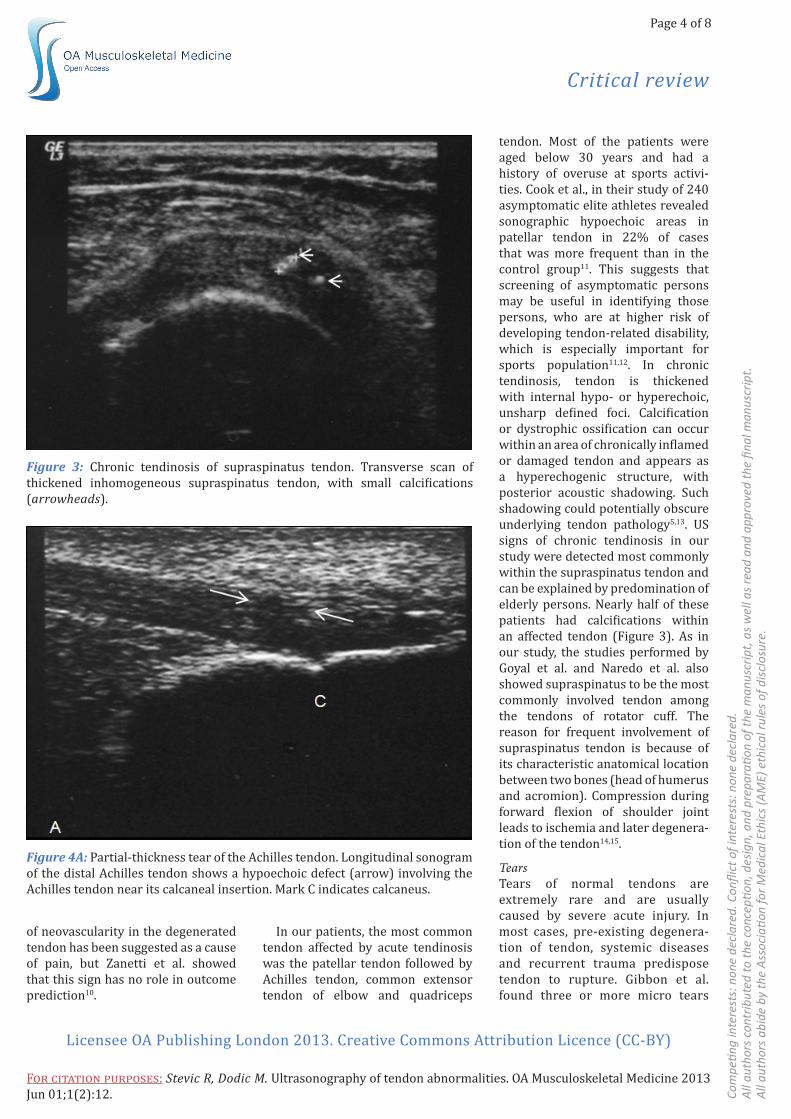
tendon. Most of the patients were aged below 30 years and had a history of overuse at sports activi-ties. Cook et al., in their study of 240 asymptomatic elite athletes revealed sonographic hypoechoic areas in patellar tendon in 22% of cases that was more frequent than in the control group11. This suggests that screening of asymptomatic persons may be useful in identifying those persons, who are at higher risk of developing tendon-related disability, which is especially important for sports population11,12. In chronic tendinosis, tendon is thickened with internal hypo- or hyperechoic, unsharp defined foci. Calcification or dystrophic ossification can occur within an area of chronically inflamed or damaged tendon and appears as a hyperechogenic structure, with posterior acoustic shadowing. Such shadowing could potentially obscure underlying tendon pathology5,13. US signs of chronic tendinosis in our study were detected most commonly within the supraspinatus tendon and can be explained by predomination of elderly persons. Nearly half of these patients had calcifications within an affected tendon (Figure 3). As in our study, the studies performed by Goyal et al. and Naredo et al. also showed supraspinatus to be the most commonly involved tendon among the tendons of rotator cuff. The reason for frequent involvement of supraspinatus tendon is because of its characteristic anatomical location between two bones (head of humerus and acromion). Compression during forward flexion of shoulder joint leads to ischemia and later degenera-tion of the tendon14,15.
TearsTears of normal tendons are extremely rare and are usually caused by severe acute injury. In most cases, pre-existing degenera-tion of tendon, systemic diseases and recurrent trauma predispose tendon to rupture. Gibbon et al. found three or more micro tears
Figure 3: Chronic tendinosis of supraspinatus tendon. Transverse scan of thickened inhomogeneous supraspinatus tendon, with small calcifications (arrowheads).
Figure 4A: Partial-thickness tear of the Achilles tendon. Longitudinal sonogram of the distal Achilles tendon shows a hypoechoic defect (arrow) involving the Achilles tendon near its calcaneal insertion. Mark C indicates calcaneus.
Critical review
Page 5 of 8
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Stevic R, Dodic M. Ultrasonography of tendon abnormalities. OA Musculoskeletal Medicine 2013 Jun 01;1(2):12.
in athletes with partial-thickness Achilles tendon tears, compared to normal tendons or tendons without partial-thickness tear4,16. When the clinical finding is suspect to tendon tear, imaging examination is neces-sary to confirm clinical diagnosis and to distinguish partial from complete tear. In partial tear, tendon
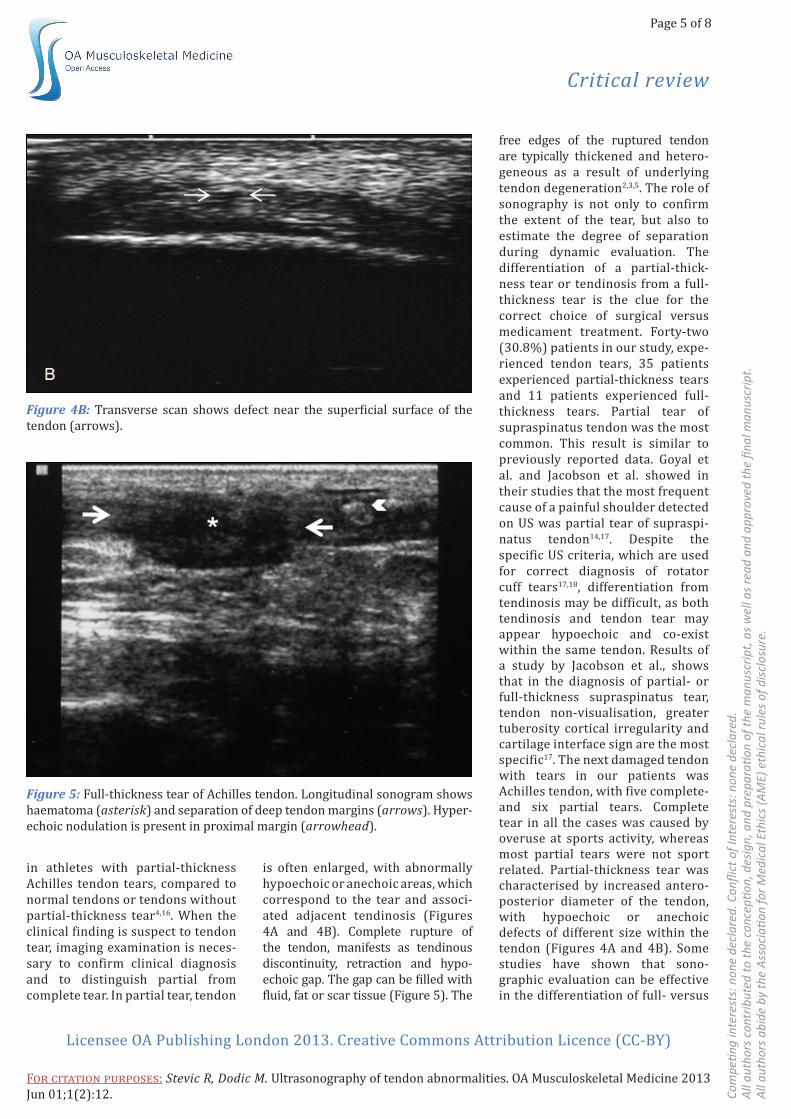
is often enlarged, with abnormally hypoechoic or anechoic areas, which correspond to the tear and associ-ated adjacent tendinosis (Figures 4A and 4B). Complete rupture of the tendon, manifests as tendinous discontinuity, retraction and hypo-echoic gap. The gap can be filled with fluid, fat or scar tissue (Figure 5). The
free edges of the ruptured tendon are typically thickened and hetero-geneous as a result of underlying tendon degeneration2,3,5. The role of sonography is not only to confirm the extent of the tear, but also to estimate the degree of separation during dynamic evaluation. The differentiation of a partial-thick-ness tear or tendinosis from a full-thickness tear is the clue for the correct choice of surgical versus medicament treatment. Forty-two (30.8%) patients in our study, expe-rienced tendon tears, 35 patients experienced partial-thickness tears and 11 patients experienced full-thickness tears. Partial tear of supraspinatus tendon was the most common. This result is similar to previously reported data. Goyal et al. and Jacobson et al. showed in their studies that the most frequent cause of a painful shoulder detected on US was partial tear of supraspi-natus tendon14,17. Despite the specific US criteria, which are used for correct diagnosis of rotator cuff tears17,18, differentiation from tendinosis may be difficult, as both tendinosis and tendon tear may appear hypoechoic and co-exist within the same tendon. Results of a study by Jacobson et al., shows that in the diagnosis of partial- or full-thickness supraspinatus tear, tendon non-visualisation, greater tuberosity cortical irregularity and cartilage interface sign are the most specific17. The next damaged tendon with tears in our patients was Achilles tendon, with five complete- and six partial tears. Complete tear in all the cases was caused by overuse at sports activity, whereas most partial tears were not sport related. Partial-thickness tear was characterised by increased antero-posterior diameter of the tendon, with hypoechoic or anechoic defects of different size within the tendon (Figures 4A and 4B). Some studies have shown that sono-graphic evaluation can be effective in the differentiation of full- versus
Figure 4B: Transverse scan shows defect near the superficial surface of the tendon (arrows).
Figure 5: Full-thickness tear of Achilles tendon. Longitudinal sonogram shows haematoma (asterisk) and separation of deep tendon margins (arrows). Hyper-echoic nodulation is present in proximal margin (arrowhead).
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Stevic R, Dodic M. Ultrasonography of tendon abnormalities. OA Musculoskeletal Medicine 2013 Jun 01;1(2):12.
Critical review
Page 6 of 8
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
partial-thickness tears or tendi-nosis, with an accuracy of 92%19. Kälebo et al. reported an accuracy of 95% in the use of sonography in the detection of partial-thickness tears
of the Achilles tendon20. On other hand, some studies that included surgery (Aström et al.) showed that findings from neither sonography nor magnetic resonance imaging
(MRI) could be used to accurately distinguish partial-thickness tears from tendinosis21.
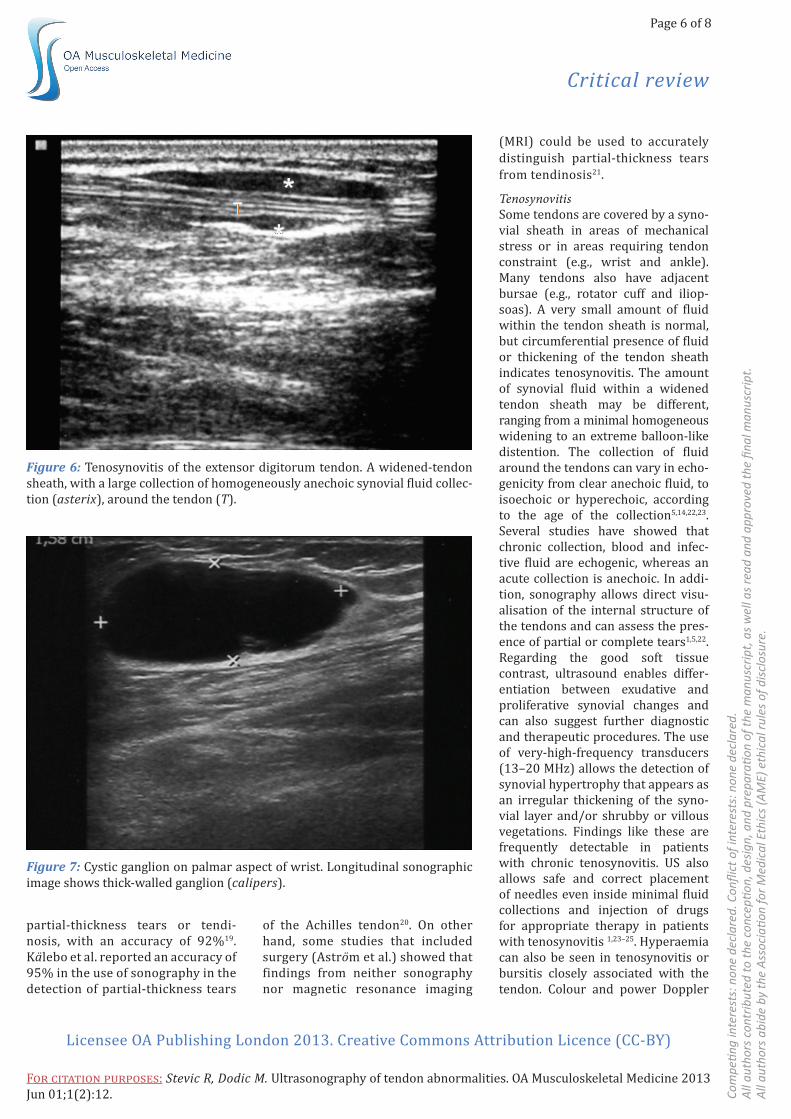
Tenosynovitis Some tendons are covered by a syno-vial sheath in areas of mechanical stress or in areas requiring tendon constraint (e.g., wrist and ankle). Many tendons also have adjacent bursae (e.g., rotator cuff and iliop-soas). A very small amount of fluid within the tendon sheath is normal, but circumferential presence of fluid or thickening of the tendon sheath indicates tenosynovitis. The amount of synovial fluid within a widened tendon sheath may be different, ranging from a minimal homogeneous widening to an extreme balloon-like distention. The collection of fluid around the tendons can vary in echo-genicity from clear anechoic fluid, to isoechoic or hyperechoic, according to the age of the collection5,14,22,23. Several studies have showed that chronic collection, blood and infec-tive fluid are echogenic, whereas an acute collection is anechoic. In addi-tion, sonography allows direct visu-alisation of the internal structure of the tendons and can assess the pres-ence of partial or complete tears1,5,22. Regarding the good soft tissue contrast, ultrasound enables differ-entiation between exudative and proliferative synovial changes and can also suggest further diagnostic and therapeutic procedures. The use of very-high-frequency transducers (13–20 MHz) allows the detection of synovial hypertrophy that appears as an irregular thickening of the syno-vial layer and/or shrubby or villous vegetations. Findings like these are frequently detectable in patients with chronic tenosynovitis. US also allows safe and correct placement of needles even inside minimal fluid collections and injection of drugs for appropriate therapy in patients with tenosynovitis 1,23–25. Hyperaemia can also be seen in tenosynovitis or bursitis closely associated with the tendon. Colour and power Doppler
Figure 6: Tenosynovitis of the extensor digitorum tendon. A widened-tendon sheath, with a large collection of homogeneously anechoic synovial fluid collec-tion (asterix), around the tendon (T).
Figure 7: Cystic ganglion on palmar aspect of wrist. Longitudinal sonographic image shows thick-walled ganglion (calipers).

Critical review
Page 7 of 8
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Stevic R, Dodic M. Ultrasonography of tendon abnormalities. OA Musculoskeletal Medicine 2013 Jun 01;1(2):12.
US help to differentiate active from inactive joint processes5,22,24. US is more sensitive than MRI in the detec-tion of synovitis and tenosynovitis1,2. Sonographic finding of tenosynovitis was detected in 18 of our patients, in 13 biceps tendons and in five wrist and hand tendons (Figure 6). As in other studies, our results showed that tendon bicep tenosynovitis was frequently associated with pathology of supraspinatus tendon (in eight of the 13 cases)14,15. Five patients, with tenosynovitis of wrist and hand tendons, were aged below 30 years and tenosynovitis was associated with overuse in all cases in contrast to other studies, where arthritis was the most common cause23,24.
Other lesions-ganglion cysts and giant cell tumours of the tendon sheathGanglion cysts are benign ‘tumour-like’ masses that arise from the muci-nous degeneration of collagenous structures. These lesions typically contain a viscous, gelatinous fluid that is surrounded by a wall composed of a dense, fibrous connective tissue. They are caused by chronic irrita-
tion, repetitive injury and ischemia. Ganglion cysts have been reported in most joints throughout the body, commonly about the wrist and ankle26,27. Ganglia on sonography usually appear as hypoechoic or anechoic, well-bordered masses usually located near a joint or a tendon sheath (Figure 7). They typically show posterior acoustic enhancement, but small ganglionic cysts, however, may show little or no enhancement. Other variable sono-graphic features of ganglion cysts include the presence of lobulations, defined margins, internal echoes and septations27,28. The majority of ganglia are completely avascular on colour Doppler sonography, but complex cystic ganglia can have demonstrable colour Doppler flow, likely due to superimposed inflammation. In our patients, ganglia were diagnosed most commonly at wrist as in others studies27,28. The differential diagnosis of a ganglionic cyst includes anechoic or hypoechoic masses. In addition to the diagnosis of ganglia, sonography is helpful when needle aspiration
is warranted. Sonography can also guide accurate intracystic steroid injection24,25.
Giant cell tumour of the tendon sheath is also known as localised nodular tenosynovitis. Pathologi-cally, giant cell tumours are identical to pigmented villonodular synovitis. They are the most common in the hand, exceeded only by ganglion cysts in that location. The second most frequent site of occurrence is the ankle-foot complex. In diag-nosing a giant cell tumour of the tendon sheath, US can show the tumour’s site, size and echogenicity, contact of the tumour with the tendon sheath, bone erosion and internal vascularity26,29. Differentia-tion from a ganglion is very important, because giant cell tumour can only be treated with resection, although ganglionic cysts can be treated with both resection and needle punc-ture, with steroid injection. The studies by Middleton et al. and Wang et al. showed that all the giant cell tumours of the tendon sheath in the hand and wrist appeared as a homogeneous, hypoechoic or hyper-echoic, well-delineated solid mass in close contact with a tendon whereas ganglionic cysts appear anechoic, cystic26,29,30. The borders of the lesion are clear, but the extensively growing lesions may have close contact with the adjacent tendon sheath and joint capsule. In our study, an irregular mass surrounding peroneal tendons was revealed in one case (Figure 8). In most cases, giant cell tumours of the tendon sheath are hypervas-cular lesions and colour Doppler sonography detects variable internal flow signals. Even if the sonographic appearance of a giant cell tumour of the tendon sheath is not diagnostic, it is strongly suggestive. Sonog-raphy has been proposed as the first method to assess a giant cell tumour of the tendon sheath29.
ConclusionUltrasound is an efficient and accu-rate imaging method for evaluation
Figure 8: Giant cell tumour of tendon sheath. Transverse sonogram of peroneal tendons show giant cell tumour with a hypoechoic mass (arrows) surrounding peroneal tendons (asterix).

Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Stevic R, Dodic M. Ultrasonography of tendon abnormalities. OA Musculoskeletal Medicine 2013 Jun 01;1(2):12.
Critical review
Page 8 of 8
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
of tendon abnormalities. Like MRI, US is also a technique that affords anatomic images in multiple planes and may provide information about tissue characterisation. Artefacts and pitfalls should always be considered, because they can be misinterpreted as areas of altered tendon echogenicity due to anatomic lesions. As in other studies, our experience indicates that US should be considered as a part of the clinical examination in patients with suspected tendon lesions. Basic lesions that can be easily diagnosed are follows: tendon sheath widening, peritendinitis, calcific and/or degen-erative changes and tendon tears. In addition, colour Doppler and power Doppler sonography can give impor-tant information about hyperaemia that can be associated with inflam-mation and solid tumours. US can also be used to monitor response to systemic and local treatments. Comparative studies between US and other imaging techniques (MRI, arthrography and arthroscopy) have confirmed the reliability of US and the good sensitivity : specificity ratio.
Abbreviations listMRI, magnetic resonance imaging; US, ultrasonography.
References1. Grassi W, Filippucci E, Farina A, Cervini C. Sonographic imaging of tendons. Arthritis Rheum. 2000 May;43(5):969–76.2. Lee KS. Musculoskeletal sonography of the tendon. J Ultrasound Med. 2012 Dec;31(12):1879–84.3. Fornage BD, Rifkin MD. Ultrasound examination of tendons. Radiol Clin North Am. 1988 Jan;26(1):87–107.4. Chang A, Miller TT. Imaging of tendons. Sports Health 2009 Jul;1(4):293–300.5. Robinson P. Sonography of common tendon injuries. AJR Am J Roentgenol. 2009 Sep;193(3): 607–18.6. Tan SC, Chan O. Achilles and patellar tendinopathy: current understanding of pathophysiology and management. Disa-bility Rehabil. 2008;30(20–22):1608–15.7. Khan KM, Bonar F, Desmond PM, Cook JL, Young DA, Visentini PJ, et al. Patellar tendinosis (jumper’s knee): find-ings at histopathological examination, US, and MR imaging. Victorian Institute
of Sport Tendon Study Group. Radiology. 1996 Sep;200(3):821–7.8. Carr JC, Hanly S, Griffin J, Gibney R. Sonography of the patellar tendon and adjacent structures in pediatric and adult patients. AJR Am J Roentgenol. 2001 Jun;176(6):1535–9.9. Cook JL, Malliaras P, De Luca J, Ptasznik R, Morris M. Vascularity and pain in the patellar tendon of adult jumping athletes: a 5 month longitudinal study. Br J Sports Med. 2005 Jul;39(7):458–61.10. Zanetti M, Metzdorf A, Kundert H-P, Zollinger H, Vienne P, Seifert B, et al. Achilles tendons: clinical relevance of neovascularization diagnosed with power Doppler US. Radiology. 2003 May;227(2):556–60.11. Cook JL, Khan KM, Harcourt PR, Kiss ZS, Fehrmann MW, Griffiths L, et al. Patellar tendon ultrasonography in asymptomatic active athletes reveals hypoechoic regions: a study of 320 tendons. Victorian Institute of Sport Tendon Study Group. Clin J Sport Med. 1998 Apr;8(2):73–7.12. Fredberg U, Bolvig L. Significance of ultrasonographically detected asymp-tomatic tendinosis in the patellar and achilles tendons of elite soccer players: a longitudinal study. Am J Sports Med. 2002 Jul–Aug;30(4):488–91.13. Gibbon WW, Cooper JR, Radcliffe GS. Distribution of sonographically detected tendon abnormalities in patients with a clinical diagnosis of chronic Achilles tendinosis. J Clin Ultrasound. 2000 Feb;28(2):61–6.14. Goyal P, Hemal U, Kumar R. High reso-lution sonographic evaluation of painful shoulder. I J Radiol. 2010;12(1).15. Naredo E, Iagnocco A, Valesini G, Uson J, Beneyto P, Crespo M. Ultrasonographic study of painful shoulder. Ann Rheum Dis. 2003 Oct;62(10):1026–7.16. Gibbon WW, Cooper JR, Radcliffe GS. Sonographic incidence of tendon micro-tears in athletes with chronic Achilles tendinosis. Br J Sports Med. 1999 Apr;33(2):129–30.17. Jacobson JA, Lancaster S, Prasad A, van Holsbeeck MT, Craig JG, Kolowich P. Full-thickness and partial-thickness supraspinatus tendon tears: value of US signs in diagnosis. Radiology. 2004 Jan;230(1):234–42.18. Moosikasuwan JB, Miller TT, Burke BJ. Rotator cuff tears: clinical, radiographic, and US findings. Radiographics. 2005 Nov–Dec;25(6):1591–607.19. Hartgerink P, Fessell DP, Jacobson JA, van Holsbeeck MT. Full-versus
partial-thickness Achilles tendon tears: sonographic accuracy and characterization in 26 cases with surgical correlation. Radi-ology. 2001 Aug;220(2):406–12.20. Kälebo P, Allenmark C, Peterson L, Swärd L. Diagnostic value of ultrasonog-raphy in partial ruptures of the Achilles tendon. Am J Sports Med. 1992 Jul–Aug;20(4):378–81.21. Aström M, Gentz CF, Nilsson P, Rausing A, Sjöberg S, Westlin N. Imaging in chronic achilles tendinopathy: a comparison of ultrasonography, magnetic resonance imaging and surgical findings in 27 histologically verified cases. Skel-etal Radiol. 1996 Oct;25(7):615–20.22. Lin J, Jacobson JA, Fessell DP, Weadock WJ, Hayes CW. An illustrated tutorial of musculoskeletal sonography: part 2, upper extremity. AJR Am J Roentgenol. 2000 Oct;175(4):1071–9.23. Kharat A, Kharat K, Singh A. Biceps tendon tenosynovitis: a sonologic marker of shoulder joint derangement. Ind J Radiol Imag. 2006 Nov;16(4):633–6.24. Hmamouchi I, Bahiri R, Srifi N, Aktaou S, Abouqal R, Hajjaj-Hassouni N. A comparison of ultrasound and clinical examination in the detection of flexor tenosynovitis in early arthritis. BMC Musculoskelet Disord. 2011 May;12:91.25. Ho CF, Chiou HJ, Chou YH, Chang CY. Peritendinous lesions: the role of high-resolution ultrasonography. Clin Imaging. 2003 Jul–Aug;27(4):239–50.26. Bianchi S, Della Santa D, Glauser T, Beaulieu JY, van Aaken J. Sonography of masses of the wrist and hand. AJR Am J Roentgenol. 2008 Dec;191(6):1767–75.27. Wang G, Jacobson JA, Feng FY, Girish G, Caoili EM, Bradnon C. Sonog-raphy of wrist ganglion cysts: variable and noncystic appearances. J Ultrasound Med. 2007 Oct;26(10):1323–8.28. Teefey SA, Dahiya N, Middleton WD, Gelberman RH, Boyer MI. Ganglia of the hand and wrist: a sonographic analysis. AJR Am J Roentgenol. 2008 Sep;191(3):716–20.29. Middleton WD, Patel V, Teefey SA, Boyer MI. Giant cell tumors of the tendon sheath: analysis of sonographic findings. AJR Am J Roentgenol. 2004 Aug;183(2):337–9.30. Wang Y, Tang J, Luo Y. The value of sonography in diagnosing giant cell tumors of the tendon sheath. J Ultrasound Med. 2007 Oct;26(10):1333–40.