-
8/3/2019 CT ANATOMY Temporal Bone
1/22
1873D CT of the Temporal Bone: Anatomy and Pathology
The temporal bone includes many small struc-
tures within a very compact region, some
measuring well under 1 mm. Their multi-
spatial orientation makes it dicult to conceptualize
the intricate three-dimensional (3D) relationship o
these structures based on conventional two-dimen-
sional (2D) imaging. The purpose o this study is to
demonstrate the role played by 3D CT to better un-
derstand the complex anatomy o the temporal bone.
In addition, select pathological cases are eatured to
highlight the role played by 3D CT to urther charac-
terize disease entities not ully evaluated by conven-tional
two-dimensional imaging.
Introduction
Conventional two-dimensional imaging in the axial
and coronal planes is routinely used to display the
anatomy and pathology o the temporal bone. Al-
though the trained head and neck radiologist may
easily interpret such studies, the general radiologist
may nd it dicult when it comes to interpretation
o such scans. Also, there is a long learning curve
when one starts to interpret temporal bone studies.
It is the inherent multi-spatial orientation o several
small structures within a compact region that makes
the anatomy o the temporal bone so complex. How-
ever, we believe that 3D reconstructions o the tem-
poral bone can help one better understand temporal
bone anatomy. Such volume-rendered 3D images
can be sectioned in any plane and rotated in space
to better conceptualize the underlying anatomy. The
purpose o this article is thereore to demonstrate the
role played by 3D CT to simpliy the complex anat-omy o the
temporal bone. In addition, using select
pathological cases, we demonstrate the role played
by 3D CT in urther characterizing disease entities
not well evaluated by conventional 2D imaging. We
will rst discuss the technique essential toward ob-
taining good 3D CT images beore proceeding with
the actual anatomy and pathology o the temporal
bone, since the quality o reconstruction depends on
optimal raw data.
Girish M. Fatterpekar, MD
Amish Doshi, MD
Bradley N. Delman, MD
Department of Radiology
Mount Sinai Medical Center
New York, NY
Corresponding author:
Girish Fatterpekar, MD
Department of Radiology
Mount Sinai Medical Center
One Gustave L. Levy Place
New York, NY 10029
Email: [email protected]
Phone: (212) 241-1497
3D CT of the Temporal Bone: Anatomy and Pathology
Abstract
-
8/3/2019 CT ANATOMY Temporal Bone
2/22
188 SECTION 4 Advanced CT and MR Imaging Throughout the Body
Technique
To obtain good 3D reconstructions, it is absolutely
essential to obtain the thinnest possible overlapping
slices. We obtained our temporal bone scans using
0.75 mm collimation with a 0.75 mm slice thickness
at 120 kVp, 200 mAs, a pitch o 0.8, and a 15 cm eld
o view with a matrix size o 512 x 512. The initial
data sets were then reconstructed at 0.1 mm inter-
vals. Each scan was obtained on a 16-slice spiral CT
scanner (Somatom Sensation 16; Siemens Medical
Solutions, Malvern, Pennsylvania). While obtaining
3D reconstructions, it is important to remember that
any amount o gantry tilt results in distortion o the
reconstructed 3D image. All studies were thereore
obtained with the neck fexed such that the inra-or-
bito-meatal line was parallel to the scanning plane
when obtaining images in the axial plane. A zero de-
gree gantry tilt when obtaining such images ensuredno distortion
o the post-processed 3D images. Vol-
ume-rendered 3D images were generated rom the
original 2D data with dierent sot tissue and bone
algorithms using the TeraRecon Aquarius Worksta-
tion v3.3 (TeraRecon, Inc. San Mateo, Caliornia).
These post-processed images were subsequently
rotated in space and sectioned in various planes us-
ing the built-in cut-plane tool allowing optimal 3D
display o the individual structures o the temporal
bone. A direct 2D to 3D correlate o the raw data set
in axial and coronal planes was also obtained to high-
light the role played by 3D CT to evaluate the tem-
poral bone. Additionally, the study also demonstrates
the role played by 3D CT to provide inormation that
is complementary to conventional 2D imaging, when
evaluating pathology o the temporal bone.
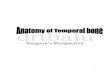
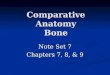
Normal Temporal Bone Anatomy
The temporal bone essentially consists o the exter-
nal ear including the pinna and the external auditory
canal, the middle ear including the ossicles, and theinner ear
comprising largely o the cochlea, vestibule
and the semicircular canals (Figure 1).
Figure 1: Volume-rendered 3D CT image o the auditory
system. EAC: External auditory canal. The box in the
bottom right corner o each fgure represents the
orientation o the reconstructed image in a three-
dimensional plane. Thus, A denotes anterior, P: posterior,
R: right side, L: let, H: head end, and F: the oot end
-
8/3/2019 CT ANATOMY Temporal Bone
3/22
1893D CT of the Temporal Bone: Anatomy and Pathology
Middle Ear
The middle ear, or tympanic cavity, helps to transmit
sound waves rom the external auditory canal to the
inner ear via the contained ossicles, namely, the mal-
leus, the incus, and the stapes.
The malleus, shaped like a hammer, has acets on the
posterior surace o the head that provide or articu-
lation with the body o the incus (Figure 2). The neck
o the malleus lies inerior to the head and provides
attachment to the tensor tympani. The long process,
or manubrium, o the malleus provides attachment at
its tip to the tympanic membrane (Figure 2).
The incus, shaped like a premolar tooth, has acets
on the anterior surace o its body that articulate with
the head o the malleus (Figure 3). Two divergingprocesses, the
short process directed posterolaterally
and the long process directed ineriorly, arise rom
the body o the incus. The long process o the incus
lies posterior and parallel to the manubrium o the
malleus (Figure 4). It bends medially to end in a
rounded projection, the lenticular process, which ar-
ticulates with the head o the stapes (Figure 3).
The stapes, shaped like a stirrup, has a head that ar-
ticulates with the lenticular process o the incus (Fig-
ure 5). The neck o the stapes lies inerior to the head
and provides attachment to the stapedius muscle.
Two diverging processes known as the crura arise
rom the neck. They are connected at their inerior
ends by the ootplate (Figure 5). The ootplate sits on
the oval window allowing or transmission o sound
waves to the inner ear (Figure 6).
Figure 2: Volume-rendered 3D CT image o the malleus. Figure 3:
Volume-rendered 3D CT image o the incus.
-
8/3/2019 CT ANATOMY Temporal Bone
4/22
190 SECTION 4 Advanced CT and MR Imaging Throughout the Body
Figure 4: Volume-rendered 3D CT image o the malleusand incus
illustrating that the long process o the
incus lies parallel and posterior to the manubrium
o the malleus.
Figure 5: Volume-rendered 3D CT image o the stapes.
Figure 6: A) (Let image) Volume-rendered 3D CT image shows the
relative positions o the malleus, incus, oval window
and the inner ear. B) (Right image) Widening the window level
reveals the stapes sitting on the oval window, thereby
allowing transmission o sound waves to the inner ear.
Figure 6A Figure 6B
-
8/3/2019 CT ANATOMY Temporal Bone
5/22
1913D CT of the Temporal Bone: Anatomy and Pathology
Inner Ear
The inner ear, primarily responsible or balance and
hearing, consists o the cochlea, vestibule, and the
semicircular canals (Figure 7).
The cochlea, shaped like a conical snail shell, winds
around its central axis or slightly more than 2
turns as it spirals toward the apex, known as cupola
(Figure 8). A ne bony partition called the osseous
spiral lamina divides the bony canal o the cochlea
into an upper passage, the scala vestibuli, and a low-
er passage, the scala tympani (Figure 9).
The vestibule is continuous anteriorly with the co-
chlea and posteriorly with the semicircular canals
(Figure 7). It contains the utricle and the saccule,parts o the
membranous labyrinth that are primarily
concerned with balance.
The three semicircular canals, superior, posterior,
and lateral are nearly orthogonal to each other. This
conguration helps in detection o angular accelera-
tion in any o the three dimensions. Each o the ca-
nals makes about two thirds o a circle. O the three
semicircular canals, the superior and posterior semi-
circular canals join to orm a common limb, called
the common crus (Figure 10).
Figure 7: Volume-rendered 3D CT image o
the inner ear.
Figure 8: Volume-rendered 3D CT image
o the cochlea.
Figure 9: Volume-rendered 3D CT image o the cochlea,
having dissected open the overlying bony wall o the
cochlea to expose the osseous spiral lamina.
Figure 10: Volume-rendered 3D CT image o the
semicircular canals.
-
8/3/2019 CT ANATOMY Temporal Bone
6/22
192 SECTION 4 Advanced CT and MR Imaging Throughout the Body
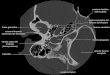
Osseous Canals of the Facial and
Vestibulocochlear Nerves
The internal auditory canal (IAC) contains the acial
and the vestibulocochlear nerves. At the lateral end
o the IAC, known as the undus, the acial nerve
lies anterosuperior, the cochlear nerve anteroine-
rior, and the superior and inerior vestibular nerves
posterosuperior and posteroinerior respectively. As
they exit the IAC, each o these nerves lies within its
own bony canal. Using 3D CT, it is possible to view
the individual canals or these nerves (Figure 11 and
12). With careul manual dissection o the overlying
structures, it is also possible to ollow the winding
course o the acial nerve housed within its own bony
canal as it traverses the temporal bone (Figure 13).
Having exhibited the individual structures o the
temporal bone, we now display serial 3D imageso the temporal
bone in both the axial and coronal
planes, comparing each reconstructed 3D image to
its corresponding 2D image (Figure 14 and 15). We
believe that once the three-dimensional congura-
tion o the individual structure is understood and the
various components o the temporal bone have been
examined as a composite, interpreting serial images
in the axial and coronal planes becomes a lot easier.
Two-dimensional images represent these various
structures as lines and circles o varying dimensions.
Using corresponding 3D CT images o varying thick-
nesses helps to improve the perception and assess-
ment o the temporal bone (Figure 14 and 15).
Figure 11: Volume-rendered 3D CT image o the
temporal bone revealing the dissected (cut) frst
portion o the acial nerve canal and the canal or the
superior vestibular nerve.
Figure 12: Volume-rendered 3D CT image othe temporal bone
showing the canal or the
cochlear nerve.
Figure 13: Volume-rendered 3D CT image o the canalor the acial
nerve as it traverses the temporal bone. The
acial nerve exits the anterosuperior aspect o the internal
auditory canal as the labyrinthine segment housed within
its own bony channel, the allopian canal. It then makes
a hairpin turn (the anterior genu) and courses as the
tympanic segment along the medial wall o the tympanic
cavity below the lateral semicircular canal. At the
posterior genu, it makes another turn and heads vertically
down as the mastoid segment to exit the temporal bone
at the stylomastoid oramen. The canal or the chorda
tympani, a branch o the mastoid segment o the acial
nerve, is also present.
-
8/3/2019 CT ANATOMY Temporal Bone
7/22
1933D CT of the Temporal Bone: Anatomy and Pathology
Temporal Bone Pathology
Having demonstrated the capability o 3D CT to
depict the normal anatomy o the temporal bone,
we now highlight its role in evaluating temporal
bone pathology.
Figure 14A
Figure 14B
-
8/3/2019 CT ANATOMY Temporal Bone
8/22
194 SECTION 4 Advanced CT and MR Imaging Throughout the Body
Figure 14C
Figure 14D
Figure 14E
-
8/3/2019 CT ANATOMY Temporal Bone
9/22
1953D CT of the Temporal Bone: Anatomy and Pathology
Figure 14F
Figure 14G
Figure 14H
-
8/3/2019 CT ANATOMY Temporal Bone
10/22
196 SECTION 4 Advanced CT and MR Imaging Throughout the Body
Figure 14I
Figure 14K
Figure 14J
-
8/3/2019 CT ANATOMY Temporal Bone
11/22
1973D CT of the Temporal Bone: Anatomy and Pathology
Figure 14L
Figure 14M
Figure 14N
-
8/3/2019 CT ANATOMY Temporal Bone
12/22
198 SECTION 4 Advanced CT and MR Imaging Throughout the Body
Figure 14O
Figure 14P
Figure 14: (A P) From inerior to superior, serial 2D and
corresponding 3D images o the
temporal bone in axial plane.
sp: styloid process, sm: stylomastoid oramen, ns: nerve to
stapedius, ms: mastoid segment
o the acial nerve, ct: chorda tympani, c aqueduct: cochlear
aqueduct, V aqueduct: vestibular
aqueduct, PSCC: posterior semicircular canal, pg: posterior
genu, LSCC: lateral semicircular
canal, CN: cochlear nerve, IV: Inerior vestibular nerve, IAC:
internal auditory canal, ts: tympanic
segment o the acial nerve, SV: superior vestibular nerve, c:
allopian canal o the acial nerve,
ag: anterior genu, SSCC: superior semicircular canal.
-
8/3/2019 CT ANATOMY Temporal Bone
13/22
1993D CT of the Temporal Bone: Anatomy and Pathology
Figure 15A
Figure 15B
Figure 15C
-
8/3/2019 CT ANATOMY Temporal Bone
14/22
200 SECTION 4 Advanced CT and MR Imaging Throughout the Body
Figure 15D
Figure 15E
Figure 15F
-
8/3/2019 CT ANATOMY Temporal Bone
15/22
2013D CT of the Temporal Bone: Anatomy and Pathology
Figure 15G
Figure 15H
Figure 15I
-
8/3/2019 CT ANATOMY Temporal Bone
16/22
202 SECTION 4 Advanced CT and MR Imaging Throughout the Body
Figure 15J
Figure 15K
Figure 15L
-
8/3/2019 CT ANATOMY Temporal Bone
17/22
2033D CT of the Temporal Bone: Anatomy and Pathology
Figure 15M
Figure 15N
Figure 15O
Figure 15: (A O) From anterior to posterior, serial 2D and
corresponding 3D coronal plane
images o the temporal bone.
ag: anterior genu, ts: tympanic segment o the acial nerve, c:
allopian canal o the acial
nerve, CN: cochlear nerve, SV: superior vestibular nerve, SSCC:
superior semicircular canal,
IAC: internal auditory canal, LSCC: lateral semicircular canal,
ms: mastoid segment o the
acial nerve, c aqueduct: cochlear aqueduct, sm: stylomastoid
oramen, PSCC: posterior
semicircular canal, V aqueduct: vestibular aqueduct.
-
8/3/2019 CT ANATOMY Temporal Bone
18/22
-
8/3/2019 CT ANATOMY Temporal Bone
19/22
2053D CT of the Temporal Bone: Anatomy and Pathology
Illustrated Case 2
Dysplastic semicircular canals
The illustrated case is o a 25-year-old male with
bilateral sensorineural hearing loss. The dysplastic
lateral semicircular canal is easily recognized with
2D imaging. However, the recognition o the absent
common crus is made possible only rom the 3D ren-
derings o the inner ear (Figure 17). Such additional
inormation gained helps us better understand the
embryology o the temporal bone.
Figure 17: 25-year-old male with bilateral sensorineural hearing
loss. (A) (Let images) 2D and 3D axial
CT images reveal enlarged, dysplastic lateral semicircular
canals bilaterally (curved arrow). (B) (Right
images) 2D coronal CT images show segments o the posterior and
superior semicircular canals
(arrow). Corresponding 3D coronal CT images (thickened to 3 mm
reconstructions) reveal an abnormal
orientation o the posterior (arrow) and superior semicircular
canal (curved arrow) with a suggestion oabsent common crus (hatched
arrow). (C) (Below) 3D CT reconstructions demonstrate the
dysplastic
lateral semicircular canals. The common crura are not seen
bilaterally. Though an abnormal orientation o
the posterior and superior semicircular canals was noted on the
axial and coronal 2D scans, the absent
common crura could only be identifed on the 3D CT
reconstructions.
-
8/3/2019 CT ANATOMY Temporal Bone
20/22
206 SECTION 4 Advanced CT and MR Imaging Throughout the Body
Illustrated Case 3
Acoustic neuroma
The illustrated case is o a 53-year-old emale with
known right acoustic neuroma. The ballooning o
the internal auditory canal easily establishes the di-
agnosis o acoustic neuroma on 2D imaging. The
presence o normal-sized bony neural canals at the
undus o the IAC establishes the acoustic neuroma
to be purely intracanalicular. This inormation could
be obtained only with the aid o the reconstructed 3D
images (Figure 18).
Figure 18: 53-year-old emale with known right acoustic neuroma.
(A) (Let) 2D and 3D axial CT
images reveal a widened right internal auditory canal consistent
with the provided diagnosis oright acoustic neuroma.
(B) (Below) 3D CT reconstructions clearly show the individual
neural canals at the lateral end
(undus) o the IAC. There is no discrepancy in the size o these
neural canals on comparison o
the two sides. This suggests that the acoustic neuroma is purely
intracanalicular and does not
extend through the bony neural canals. This inormation could not
be obtained based on the
2D data set alone.
-
8/3/2019 CT ANATOMY Temporal Bone
21/22
2073D CT of the Temporal Bone: Anatomy and Pathology
Illustrated Case 4
Cholesteatoma
The illustrated case is o an 88-year-old male with
cholesteatoma. The diagnosis o cholesteatoma is
easily established with conventional 2D imaging.
However, the extent o the erosive process involving
the basal turn o the cochlea and the round window
was made only ater a review o the reconstructed 3D
images (Figure 19).
Figure 19: 88-year-old male with cholesteatoma. (A) (Let) 2D and
3D axial CT images expose
a sot tissue mass in the let tympanic cavity causing erosion o
the malleus and incus (arrow).The stapes is not seen in the 2D
images but can be seen on the 3 mm thick reconstructed 3D
CT (curved arrow). There appears to be erosion into the basal
turn o the cochlea (hatched
arrow). (B) (Below) 3D CT reconstructions disclose absence o a
portion o the basal turn o
cochlea, likely rom the erosive process o the cholesteatoma.
Also, visualization o the other
inner ear structures shows that the erosive process extends into
the round and oval windows.
This was not readily identifed when the 2D data set was
initially interpreted.
-
8/3/2019 CT ANATOMY Temporal Bone
22/22
Conclusion
This article illustrates the role played by 3D CT in
evaluating anatomy and pathology o the temporal
bone. Though there is a learning curve when one
starts using the TeraRecon Aquarius Workstation, we
have ound the sotware to be extremely user-riend-
ly. Once one becomes amiliar with the various keys,
the time to generate such 3D images averages about
15 minutes per temporal bone study. We also eel that
the superior resolution capability o the TeraRecon
sotware has greatly enhanced the generation o these
3D reconstructions. The authors strongly believe that
such volume-rendered 3D reconstructions allow bet-
ter understanding o the temporal bone anatomy.
Also, the complementary inormation gained while
evaluating temporal bone pathology aids greatly in
the evaluation o various disease entities. Such in-
ormation allows or better pre-surgical planning andalso aids in
our understanding o the embryology o
the temporal bone.
References
1. Som, PM, Curtin, HD, eds. Head and Neck Imaging. 4th
Edition.
St. Louis, MO: Mosby-Year Book, Inc, 2002.
2. Swartz, H, Harnsberger, HR. Imaging o the Temporal Bone.
3rd
Edition. New York, NY: Thieme Medical Publishers, Inc, 1998.
3. Zeier, B, Sabini P, Sonne J. Congenital absence o the
oval
window: radiologic diagnosis and associated anomalies. Am J
Neuroradiol 21(2): 322-327, 2000.
4. Maee MF, Kumar A, Yannias DA, et al. CT o the middle ear
in evaluation o cholesteatoma and other sot tissue masses.
Radiology 148: 465-472, 1983.
5. Jun BC, Song SW, Cho JE, Park CS, Lee DH, Chang KH, Yeo
SW. Three-dimensional reconstruction based on images rom
spiral high-resolution compute tomography o the temporal
bone:
anatomy and clinical application. J Laryngol Otol. 119(9):
693-
698, 2005.
6. Stone JA, Mukherji SK, Jewett BS, Carrasco VN, Castillo M.
CT
evaluation o prosthetic ossicular reconstruction procedures:
what
the otologist needs to know. Radiographics 20(3): 593-605,
2000.
7. Satar, Bulent; Mukherji, Suresh K.; Telian, Steven A.
Congenital
Aplasia o the Semicircular Canals. Otology &
Neurotology.
24(3):437-446, 2003.