Embed Size (px)
Citation preview
CTG & partogram
Done by : Areej AL-Hadidi
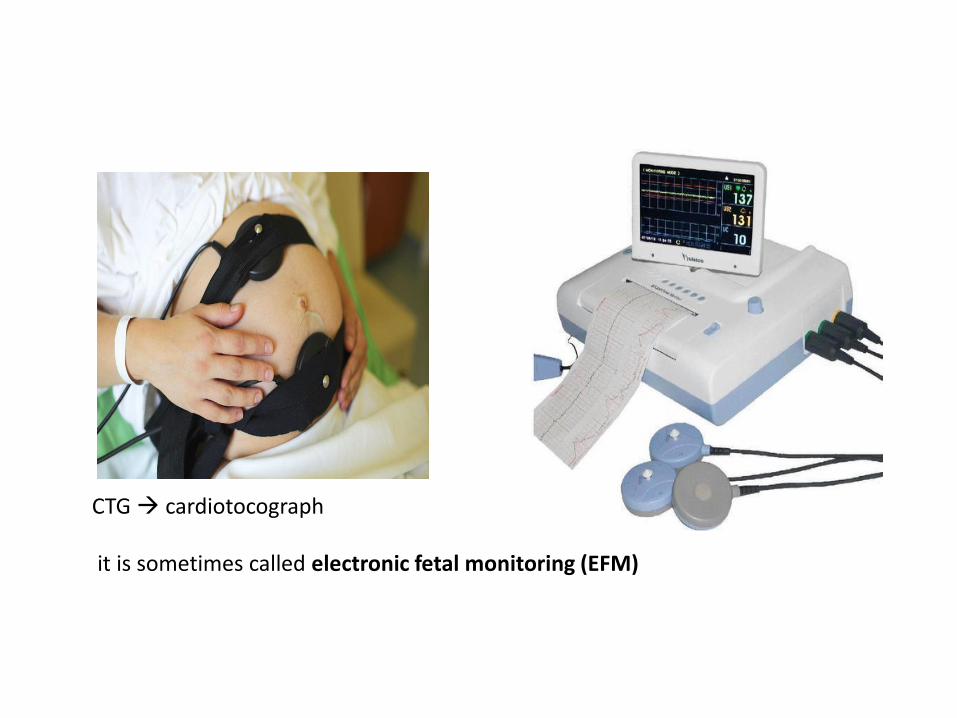
CTG cardiotocograph it is sometimes called electronic fetal monitoring (EFM)
• The cardiotocograph (CTG) is a continuous tracing of the fetal heart rate used to assess fetal wellbeing, together with an assessment of uterine activity.
• The CTG recording is obtained with the pregnant woman positioned comfortably in a left lateral or semi-recumbent position to avoid compression of the maternal vena cava.
• Two external transducers are placed on the mother’s abdomen, each attached with a belt.
• One transducer is a pressure-sensitive contraction tocodynometer (stretch gauge) that measures the pressure required to flatten a section of the abdominal wall. This correlates with the internal uterine pressure and indicates if there is any uterine activity (contractions). We put it against the fundus
• The second transducer uses ultrasound and the Doppler effect to detect motion of the fetal heart, and measures the interval between successive beats, thereby allowing a continuous assessment of fetal heart rate. We divide the fetus into 3 thirds and we put it against the nearest 1/3 to the head
• Recordings are then made for at least 30 minutes with the output from
the CTG machine producing two ‘lines’ traced onto a running piece of paper, one a tracing of fetal heart rate and a second a tracing of uterine activity.
• The mother may be given a button to press to record any fetal movements
that she has felt. • In addition, the CTG machine may record fetal movements detected via
the tocodynometer.
• Fetal cardiac behaviour is regulated through the autonomic nervous system and by vasomotor, chemoceptor and baroreceptor mechanisms.
• It depends on sympathetic and parasympathetic interactions
• Pathological events, such as fetal hypoxia, modify these signals and hence cardiac response including variation in heart rate patterns, which can be detected and recorded in the CTG
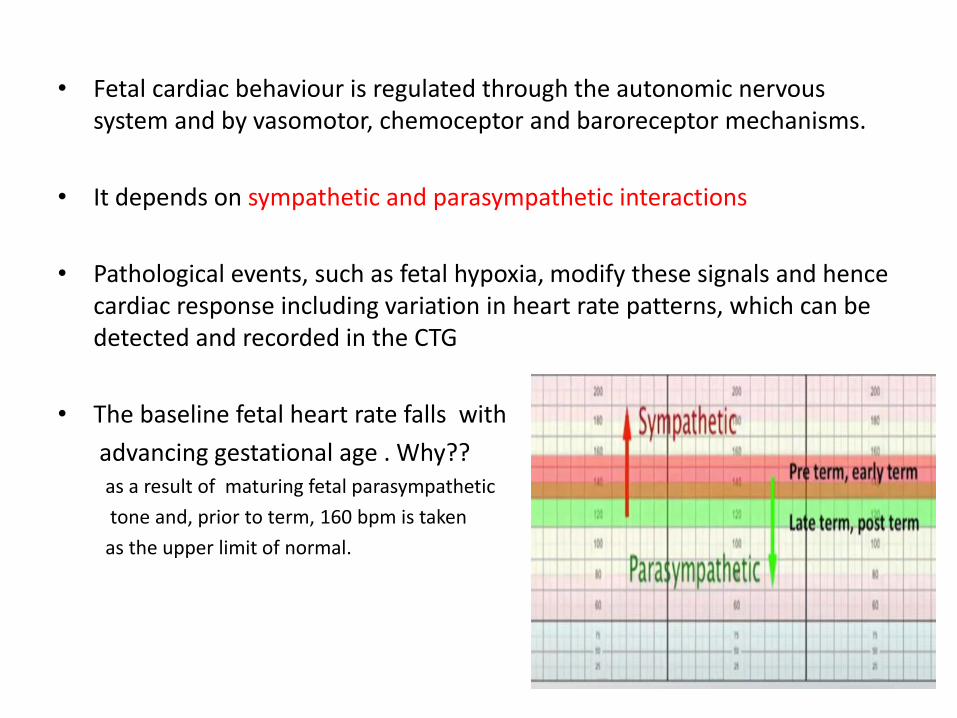
• The baseline fetal heart rate falls with
advancing gestational age . Why?? as a result of maturing fetal parasympathetic
tone and, prior to term, 160 bpm is taken
as the upper limit of normal.
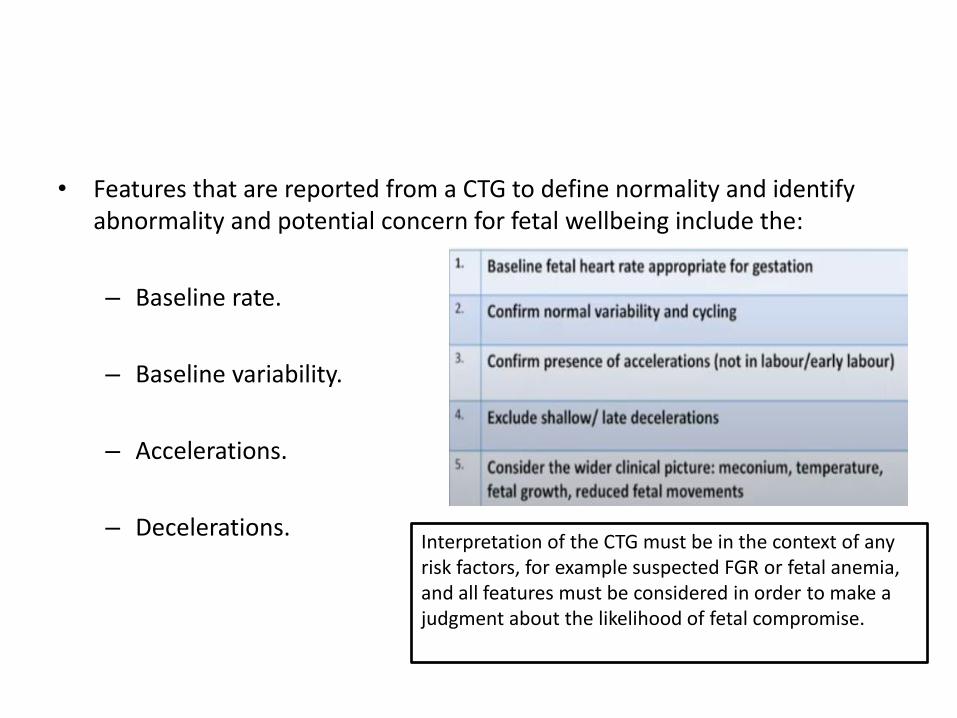
• Features that are reported from a CTG to define normality and identify abnormality and potential concern for fetal wellbeing include the:
– Baseline rate.
– Baseline variability.
– Accelerations.
– Decelerations.
Interpretation of the CTG must be in the context of any risk factors, for example suspected FGR or fetal anemia, and all features must be considered in order to make a judgment about the likelihood of fetal compromise.
Baseline fetal heart rate:
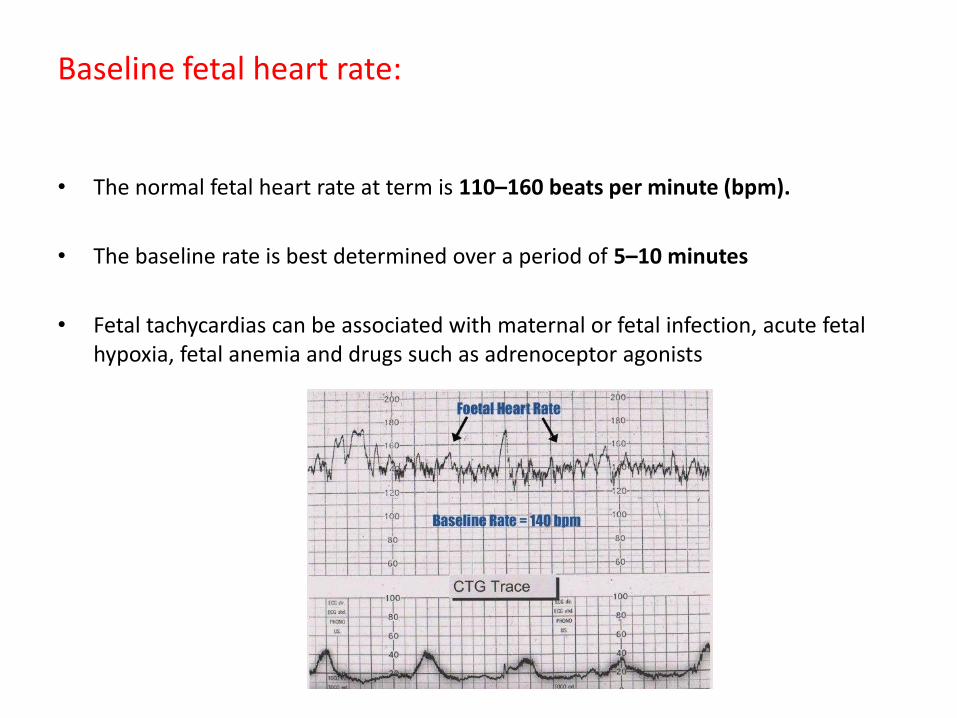
• The normal fetal heart rate at term is 110–160 beats per minute (bpm).
• The baseline rate is best determined over a period of 5–10 minutes
• Fetal tachycardias can be associated with maternal or fetal infection, acute fetal hypoxia, fetal anemia and drugs such as adrenoceptor agonists
Baseline variability:
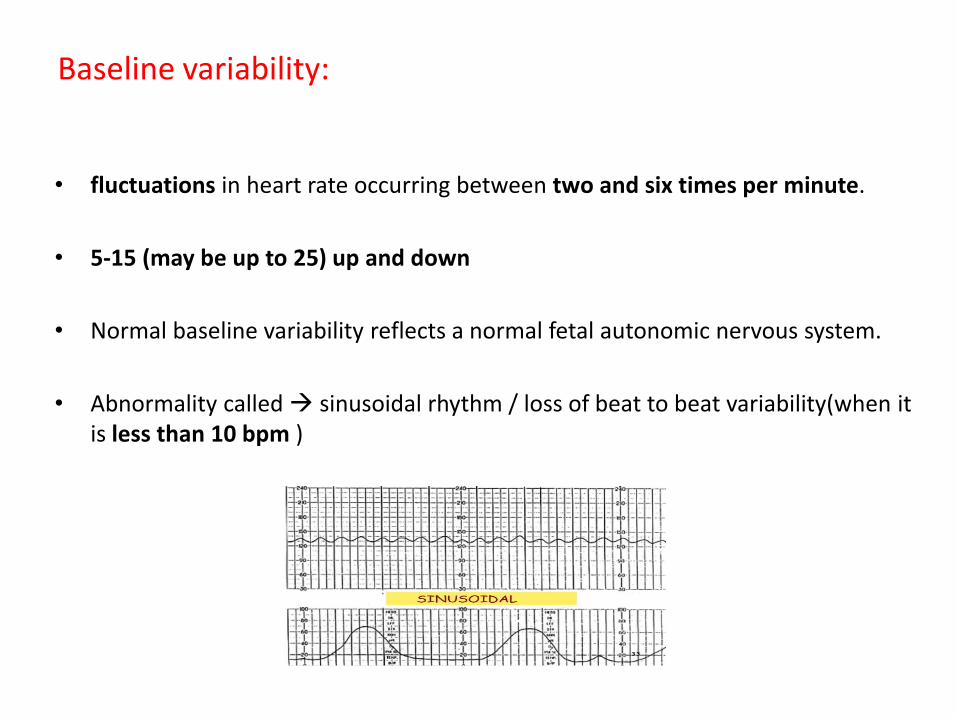
• fluctuations in heart rate occurring between two and six times per minute.
• 5-15 (may be up to 25) up and down
• Normal baseline variability reflects a normal fetal autonomic nervous system.
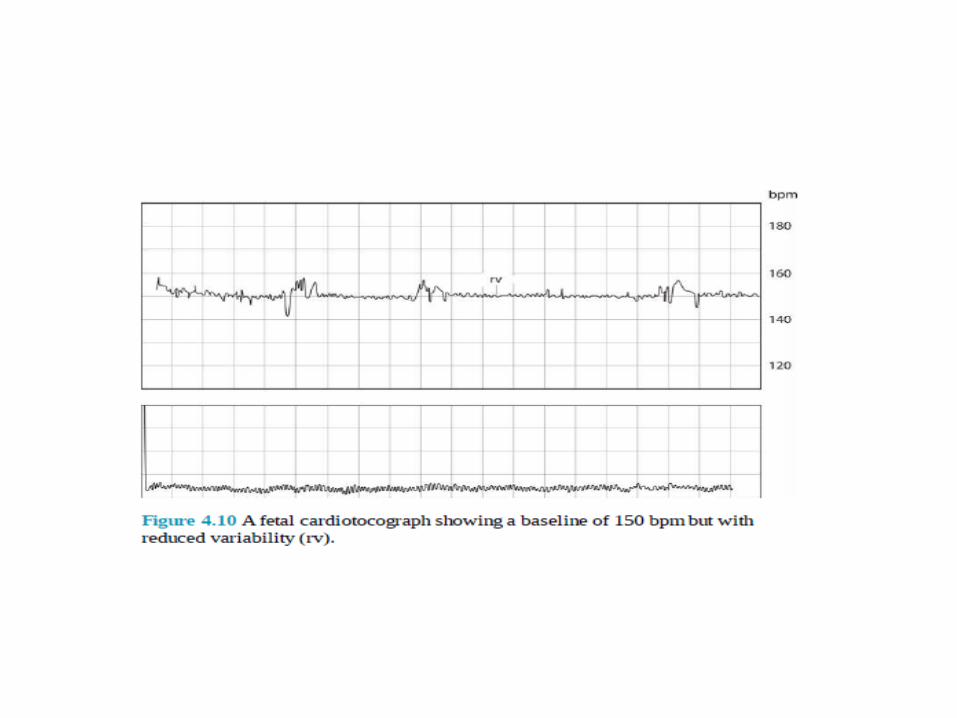
• Abnormality called sinusoidal rhythm / loss of beat to beat variability(when it is less than 10 bpm )
Cont,,
• baseline variability is modified by :
– fetal sleep states and activity
– gestational age
– hypoxia
– fetal infection
– Fetal distress
– Fetal anemia
– drugs suppressing the fetal central nervous system, such as opioids, and hypnotics (all of which reduce baseline variability).
• It is the first thing to be affected
As fetuses display deep sleep cycles of 90 minutes at a time, baseline variability may be normally reduced for this length of time, but should be preceded and followed by a period of normal baseline variability on the CTG trace. (babies should wake up when we move them)
During sleep HR will decrease as well , so reduced variability with high baseline is always a sign of concern
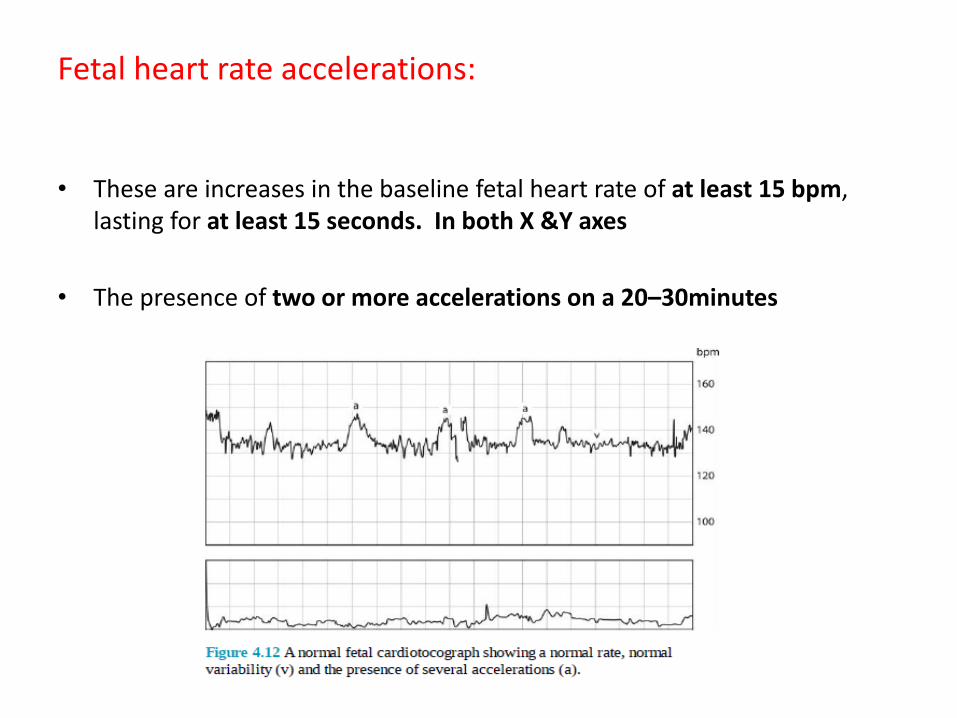
Fetal heart rate accelerations:
• These are increases in the baseline fetal heart rate of at least 15 bpm, lasting for at least 15 seconds. In both X &Y axes
• The presence of two or more accelerations on a 20–30minutes
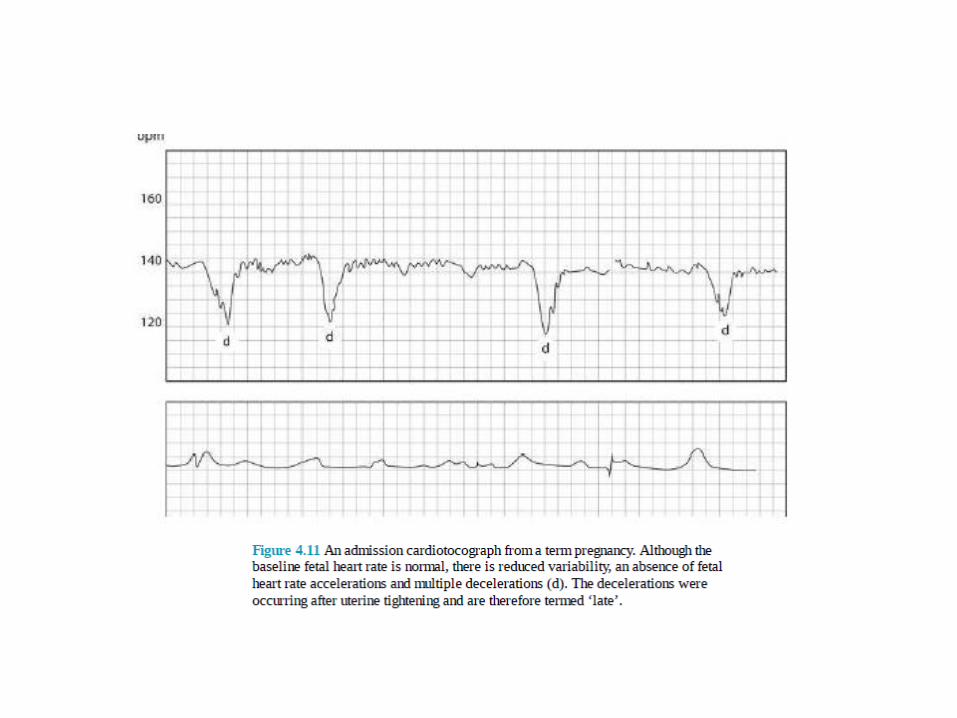
Fetal heart rate decelerations:
• These are transient reductions in fetal heart rate of 15 bpm or more, lasting for more than 15 seconds.
• Decelerations can be indicative of fetal hypoxia or umbilical cord compression.
• There is a higher chance of fetal hypoxia being present if there are additional abnormal features such as reduced variability or baseline tachycardia
Cont ,,
• Early / type I / mirror image decelerations
– They occur as a result of contractions and head compression
– Benign but if persists >60 minutes (reassess) , >90 minutes (no adequate time to recover)
– Reassure the mother
• delayed/ late/ type II:
– fetal distress
• variable
– Contractions are different in relation ,size or duration
– Cord compression
– Just change the position of the mother

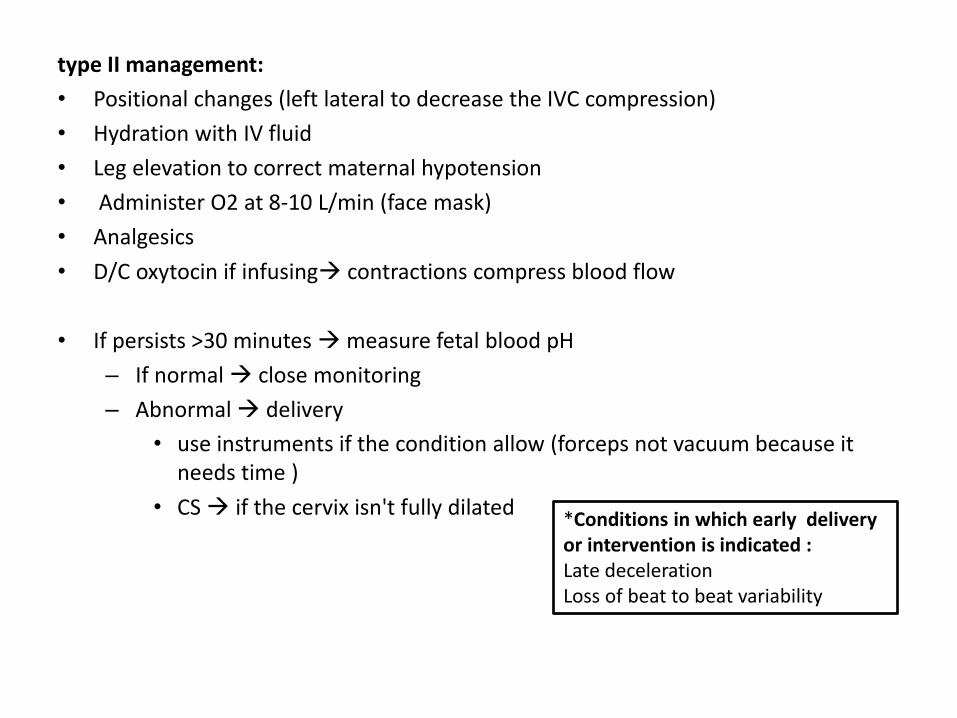
type II management:
• Positional changes (left lateral to decrease the IVC compression)
• Hydration with IV fluid
• Leg elevation to correct maternal hypotension
• Administer O2 at 8-10 L/min (face mask)
• Analgesics
• D/C oxytocin if infusing contractions compress blood flow
• If persists >30 minutes measure fetal blood pH
– If normal close monitoring
– Abnormal delivery
• use instruments if the condition allow (forceps not vacuum because it needs time )
• CS if the cervix isn't fully dilated
*Conditions in which early delivery or intervention is indicated : Late deceleration Loss of beat to beat variability
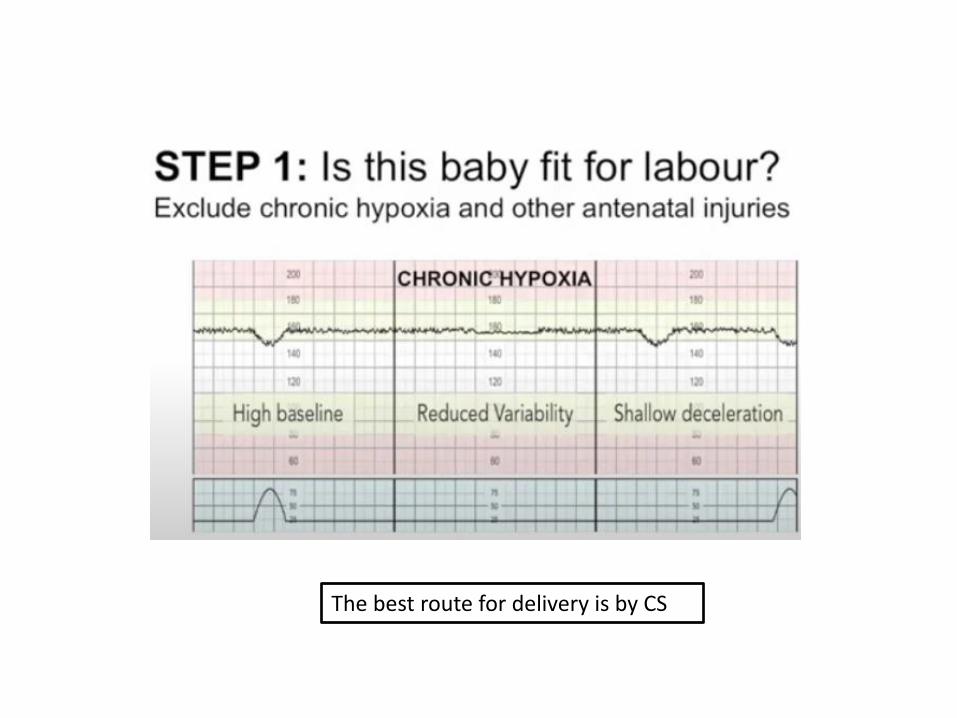
The best route for delivery is by CS
Dr C BRAVADO
• DR: define risks (Hx& PE)
• C: contractions (3-5 in 10 minutes ,each one last for 40-60 seconds)
• B RA :baseline rate
• V: variability – Moderate variability: normal (5-15) – <5 reduced – Marked variability : indication of hypoxia (we can’t determine a baseline zig zag )
• A: accelerations
• D : decelerations
• O: overall assessment
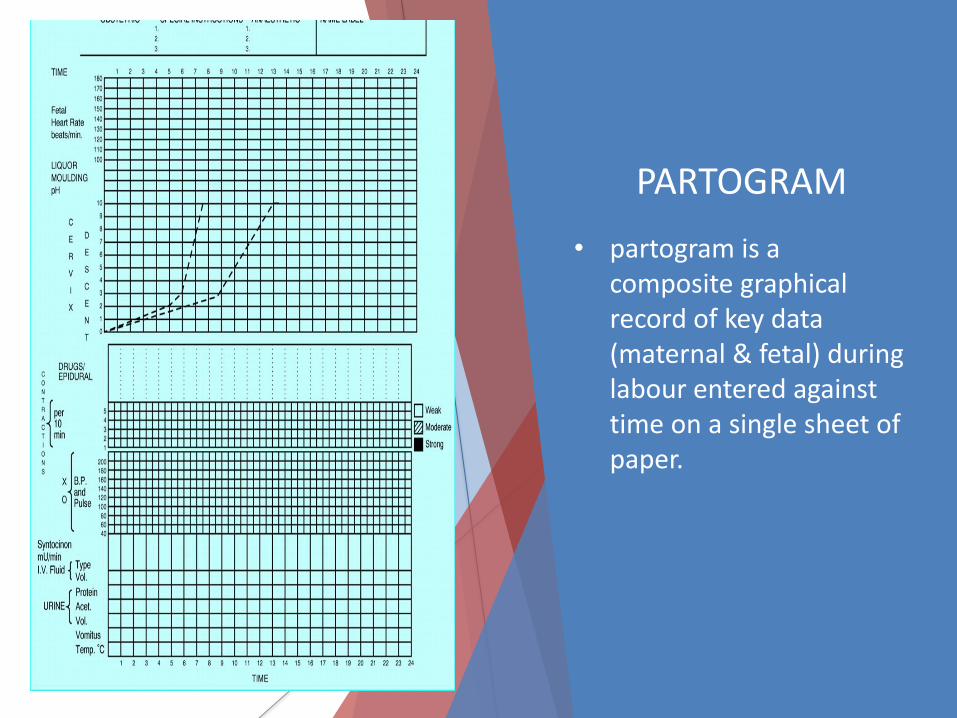
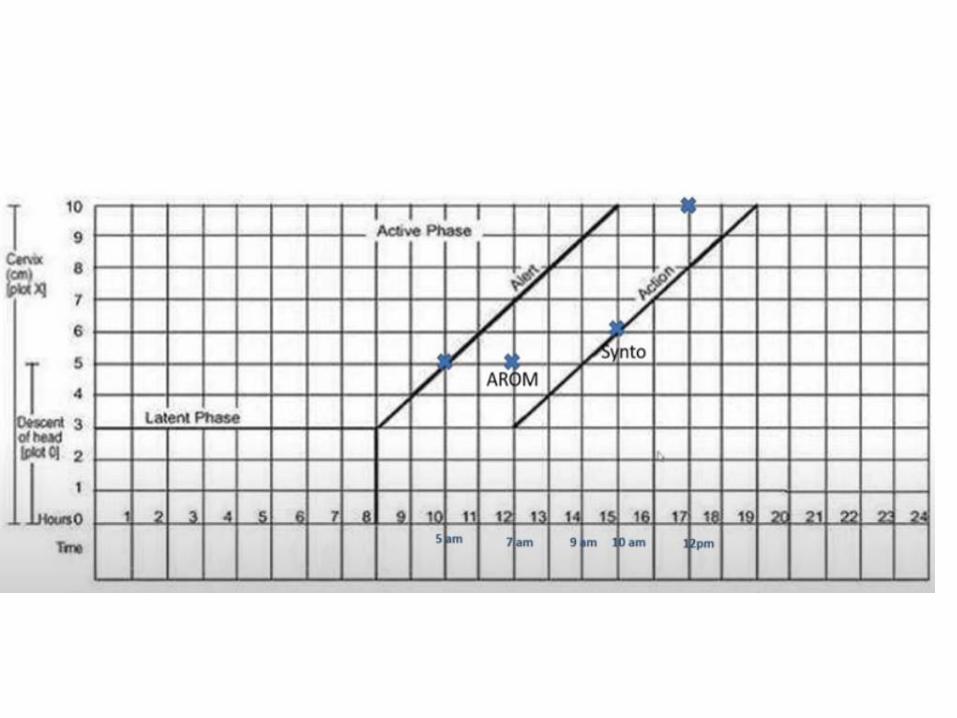
PARTOGRAM
• partogram is a composite graphical record of key data (maternal & fetal) during labour entered against time on a single sheet of paper.
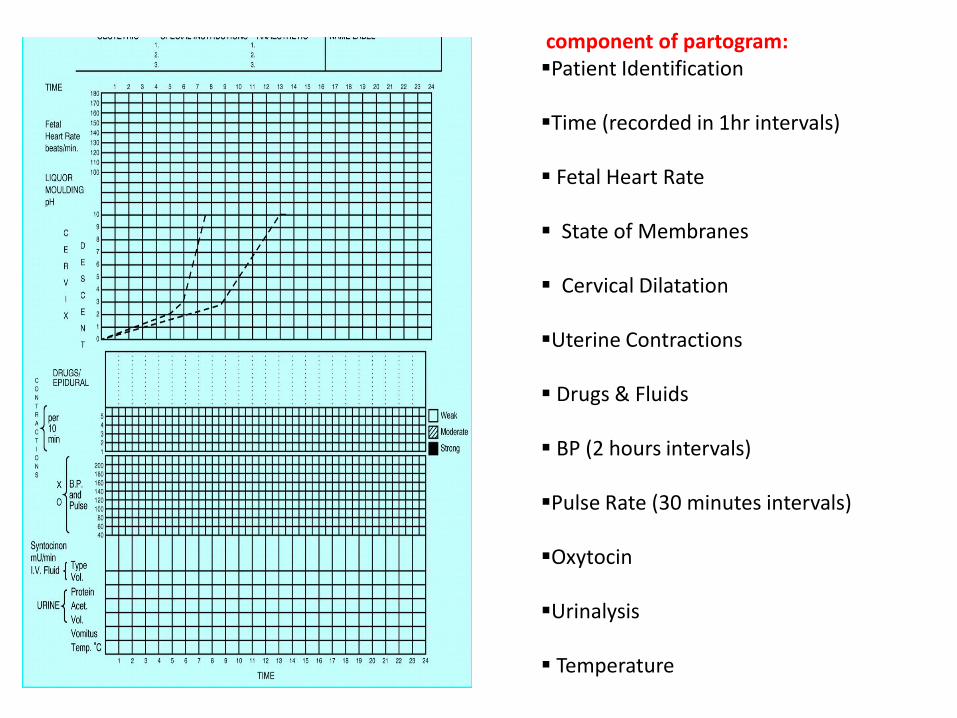
component of partogram: Patient Identification
Time (recorded in 1hr intervals)
Fetal Heart Rate
State of Membranes
Cervical Dilatation
Uterine Contractions
Drugs & Fluids
BP (2 hours intervals)
Pulse Rate (30 minutes intervals)
Oxytocin
Urinalysis
Temperature
Cont,,
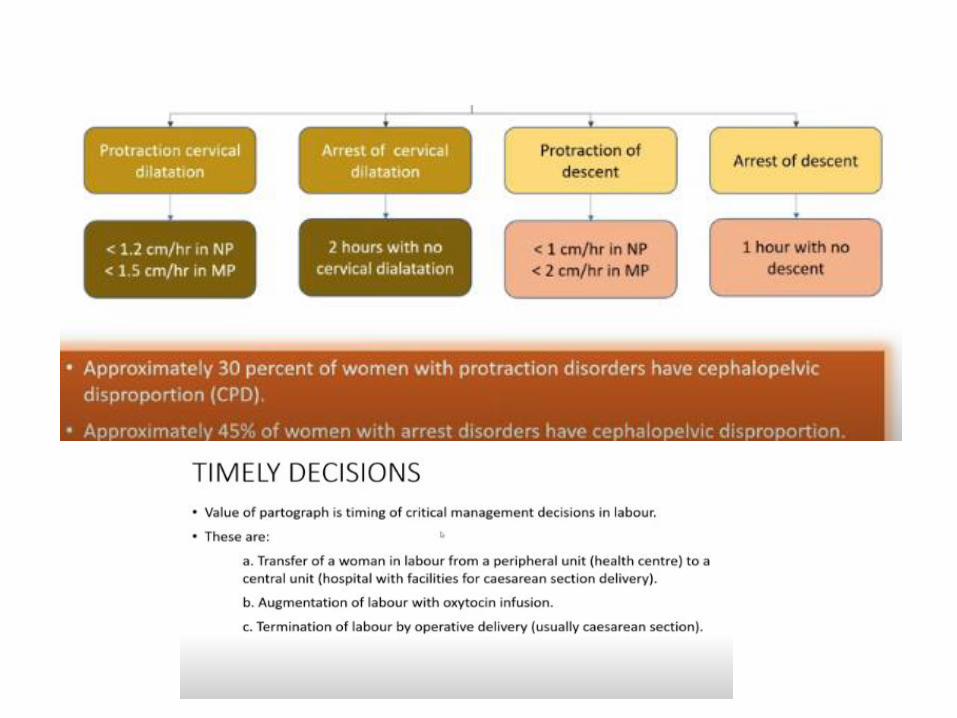
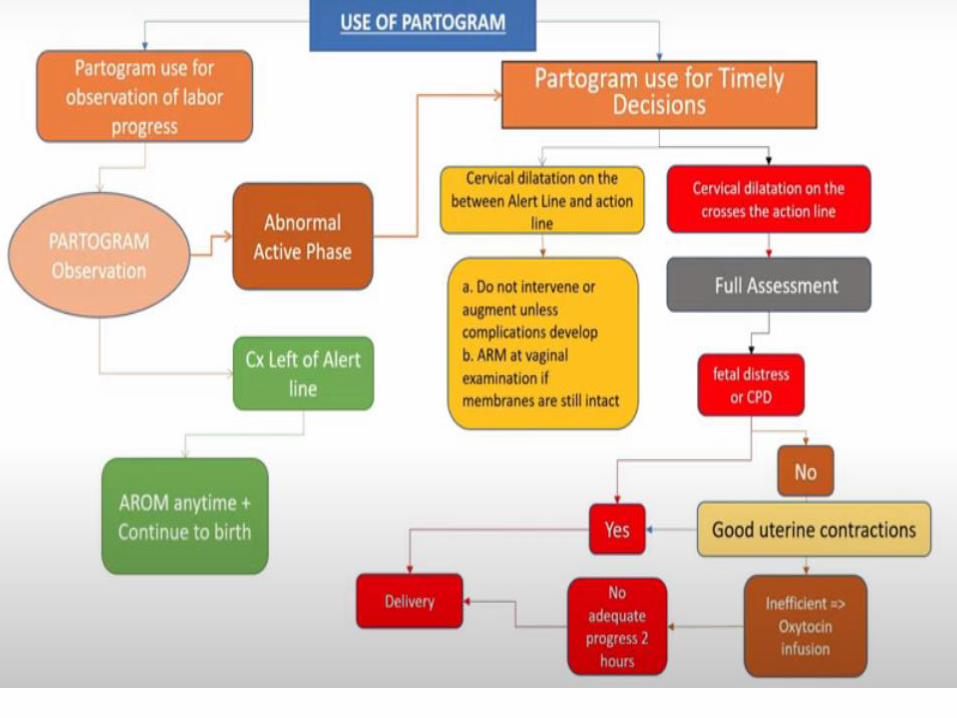
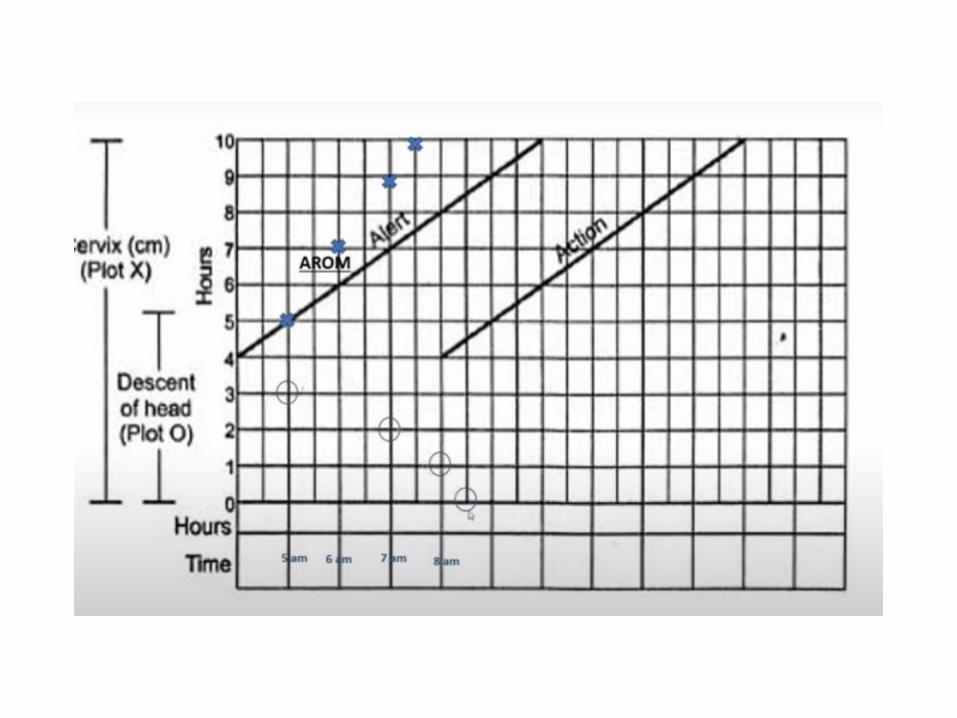
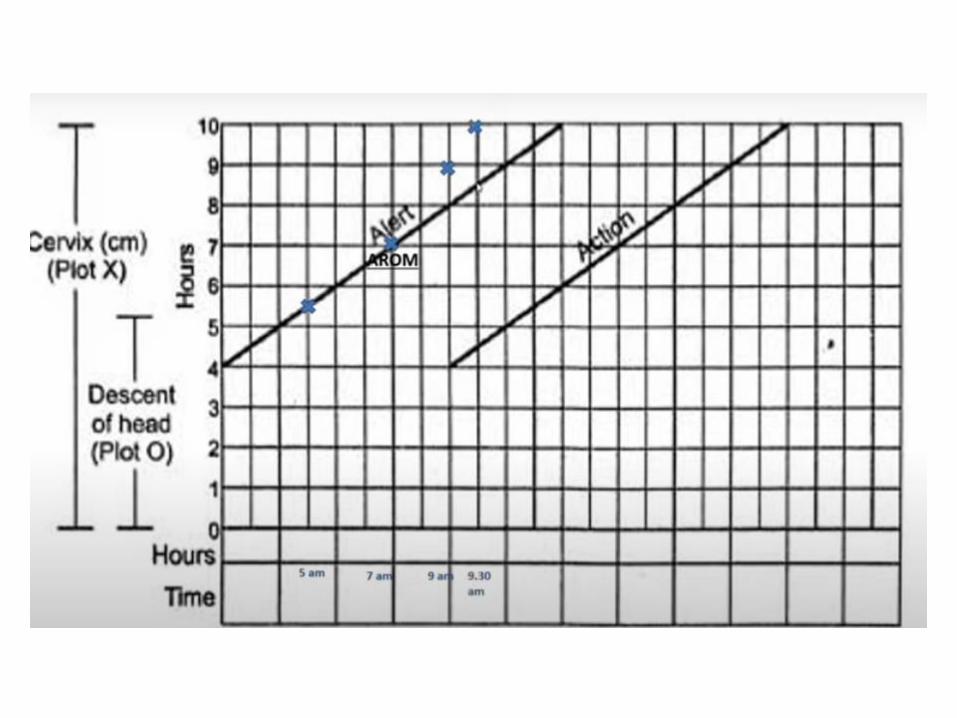
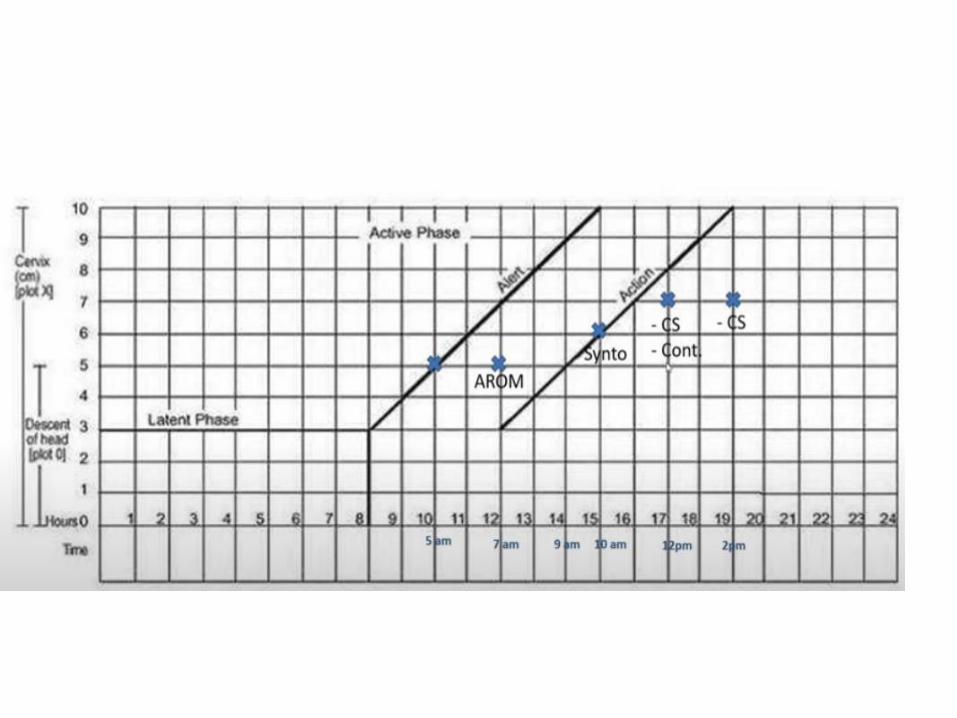
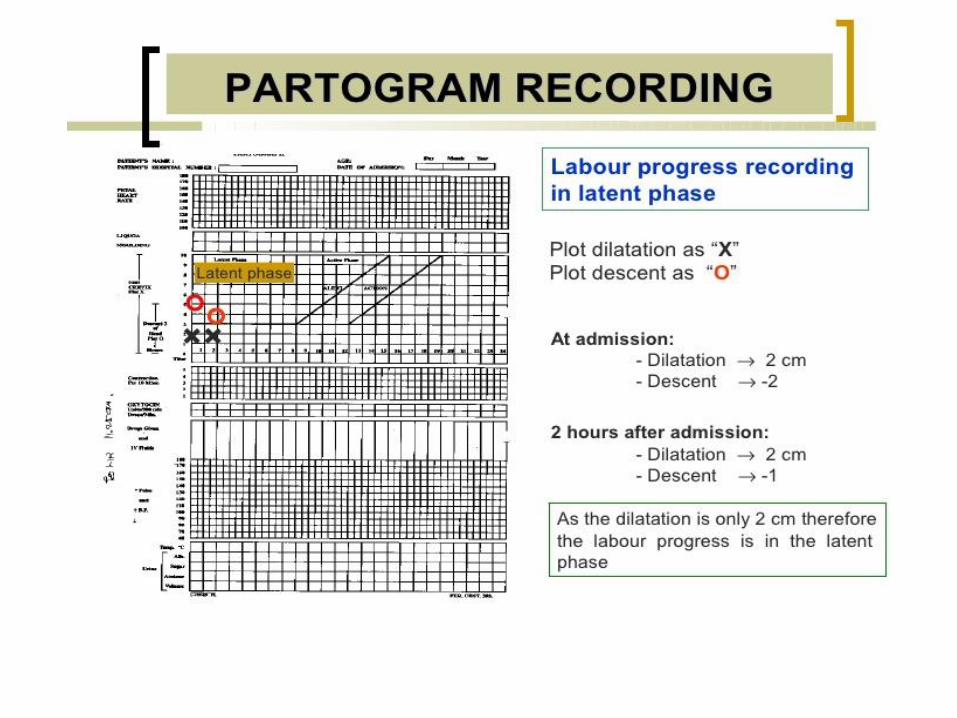
• The Alert line starts at 4 cm of cervical dilatation and it travels diagonally upwards to the point of expected full dilatation (10 cm) at the rate of 1 cm per hour.
• The action line is located 4 hours to the right of the alert line.
• As slope is to the left side of the alert line everything is ok
• Cervical dilatation represents the active phase
• Descent represents the second stage
• It is used for:
1.record observations
2.plan and adjust management guidelines
3. indicate the appropriate timing of certain interventions can be incorporated
• We remove the latent phase in the modified one . Why??
– Latent phase is difficult to diagnose and assign its start which lead to early admission and intervention
– Prolonged latent stage is relatively infrequent and doesn’t usually associated with poor perinatal outcomes