Embed Size (px)
Citation preview

Paciente de 84 años de edad, conantecedentes de fibrilación auricular cró-nica en tratamiento con acenocumarol(anticoagulante oral, antagonista dela vitamina K), que acude a urgenciascon clínica de fatiga, dificultad respira-toria, expectoración abundante conocasionales trazas hemáticas e inflama-ción del área preauricular derecha de24 horas de evolución.
A la exploración física, se objetiva uncuadro de parotiditis derecha y unhematoma submucoso en trígono retro-molar, pilares faríngeos y paladar blan-do derechos con desplazamiento de laúvula hacia la izquierda. A la depresiónlingual se observa que el hematomadesciende a modo de «sábana» por elespacio retrofaríngeo en su parte dere-cha. En la analítica existe un aumentode la urea (89 mg/dl) y de la creatinina(1,4 mg/dl) y unas pruebas de coagu-lación muy alteradas con tiempos inde-tectables. La radiografía cervical late-ral muestra la siguiente imagen: (Fig.1).
An 84 year old patient, witha history of chronic atrial fib-rillation undergoing treat-ment with acenocoumarol(oral anticoagulant, vitaminK antagonist), presented tothe emergency services withclinical fatigue, breathing dif-ficulties, much expectoration,with occasional traces ofblood and inflammation inthe right preauricular areawhich she had been experi-encing for 24 hours.On physical examination,parotiditis on the right sidewas noted and a submucos-al hematoma on the retro-molar trigone, pharyngeal pil-lars and soft palate on rightside with uvula displacementtowards the left side. On flat-tening the tongue, it isobserved that the hematomadescends like a “sheet” downthe retropharyngeal space onthe right side. Tests showedan increase in urea (89mg/dl) and creatinine (1,4mg/dl) and coagulation tests
were abnormal with undetectable times*. The lateral cervi-cal radiography showed this image: (Fig. 1)
Página del Residente
Rev Esp Cirug Oral y Maxilofac 2004;26:259-262
¿Cuál sería su diagnóstico y actitudterapéutica?What would the diagnosis be and the therapeutic approach?
Figura 1. Rx cervical lateral de la paciente.Figure 1. Lateral cervical X-ray of the patient.
CO 26/4 22/9/04 16:50 Página 259

Discusión
La radiografía cervical lateral presenta un espacio prevertebralde inusuales dimensiones, lo que hace sospechar, junto con la clí-nica y exploración, que la paciente presenta un importante hema-toma retrofaríngeo.
Con este diagnóstico se consulta con el Servicio de Hematolo-gía antes de realizar cualquier maniobra exploratoria adicional (naso-fibroscopia) y se decide administrar factor VII recombinante paraintentar normalizar la coagulación. Pasada media hora, la tasa deprotrombina es del 15%, pero dado el estado de urgencia de lapaciente, se decide intentar su intubación electiva, no sin antesadministrar más factor VII por recomendación del Servicio de Hema-tología. Con cierta dificultad, se consigue la intubación orotraque-al. La paciente es trasladada a la UCI donde permanece bajo seda-ción y se controla de modo definitivo la coagulación. Posteriormentese le realiza TAC cervical observándose importante hematoma quese extiende desde nasofaringe a porción alta de hipofaringe (Figs.2 y 3), reafirmando la necesidad de continuar con la intubación,aunque por indicación de la UCI se decide realizar traqueotomía,manteniéndola hasta la total resolución del episodio (controladopor TAC).
El hematoma retrofaríngeo es una rara entidad de repercusiónfatal, dada su evolución rápida hacia la obstrucción de la vía aérea.Atendiendo a su etiología pueden describirse varios factores: infec-ciones, traumatismos cervicales, traumatismos de grandes vasoscervicales, movimientos violentos cervicales, iatrogenia (cateteriza-ción cardíaca o angiografías cerebrales), hemorragia por adenomade paratiroides, ingestión de cuerpo extraño, hemofilia A, abuso deácido acetilsalicílico o como el caso que nos ocupa terapia antico-
The lateral cervical radiography showed a prevertebralspace of unusual dimensions, which led to the suspicion that,together with the tests and the examination, that the patientpresented a considerable retropharyngeal hematoma.
With this diagnosis, and before any further examinationis carried out (nasofibroscope), the Hematology Service isconsulted and a decision is made to administer recombinantfactor VII in an attempt to normalise coagulation. After halfan hour, the level of prothrombin is 15%, but given the crit-ical state of the patient, a decision is made to attempt elec-tive intubation, but not before administering more factor VIIfollowing the recommendation of the Hematology Service.With a certain degree of difficulty orotracheal intubation isachieved. The patient is taken to intensive care where she iskept under sedation and coagulation is closely controlled.Following this a CT scan of cervical spine is made, and a con-siderable hematoma is observed which descends from thenasopharynx to the uppermost portion of the hypophar-ynx (Figs. 2 and 3), confirming the need to continue withintubation although, following the recommendation of theIntensive Care Unit, a tracheotomy is performed and main-tained until the complete resolution of the case (with CT con-trol).
Retropharyngeal hematoma is very rare but it can havefatal repercussions given how quickly the airway becomesobstructed. With regard to its etiology various factors canbe described: infections, cervical trauma, trauma of largecervical vessels, violent cervical movements, iatrogenic com-plications (cardiac catheterisation or celebral angiography),haemorrhages because of parathyroid adenoma, ingestionof a foreign body, haemophilia A, acetylsalicylic acid abuseor, as in our case, anticoagulant therapy. To be more pre-cise, a case like this may appear in 2-4% of anticoagulatedpatients.1
Clinical presentation may include cervical pain, dys-phagia, dyspnea or muffled voice. Capps et al. describe aclinical triad of subcutaneous reddening of anterior neck andsuperior thorax, tracheal and oesophageal compression andventral displacement of trachea.1 It is common for patientsto be underdiagnosed in the early stages, as at first there
Hematoma retrofaríngeo
Retropharyngeal hematoma
A. Riaño Argüelles1, M.Á. Bada García2, R. Martino Gorbea2, A. Etayo Pérez1, J.L. Castiella Iribas2, R. Palomero Rodríguez3
Página del Residente
Rev Esp Cirug Oral y Maxilofac 2004;26:259-262
1 Médico Interno Residente2 Médico Adjunto3 Jefe de ServicioServicio de Cirugía Oral y MaxilofacialHospital Virgen del Camino. Pamplona
Correspondencia:Ana Riaño Argüelles Plaza Rafael Alberti nº9, 1ºC 31010 Barañain (Navarra)
CO 26/4 22/9/04 16:50 Página 260

Rev Esp Cirug Oral y Maxilofac 2004;26 261A. Riaño Argüelles y cols.
is a little discomfort in theupper airways, and this canbe confused with a simplecase of pharyngitis. It is 12 to48 hours later that alarmingsymptoms of airway com-promise occur, and urgentintubation is required or a tra-cheotomy so as to guaranteepermeability. This prolongedperiod of time is due to thepeculiar structure of theretropharyngeal space, as thesurrounding muscles do notoffer resistance to hematomainduced space expansion. This space is situated betweenthe pharynx and the spine.The posterior aspect of theretropharyngeal space ismade up of the prevertebralfascia, anatomically describedas an unfolding with an ante-rior lamina called «fasciaalar» and another posteriorlamina that is the preverte-bral fascia, with a virtualspace called the «dangerspace». It extends from thebase of the skull to the pos-terior mediastinum and it islimited laterally by the fusionof both laminas by the trans-verse apophysis of the adja-cent vertebral bodies. Infec-tions of the retropharyngealspace can spread to the dan-ger space, and from hereprogress to the posteriormediastinum with serious lifethreatening risk.Hematoma prognosis is goodif diagnosed and treatedquickly. It has been demon-
strated that patients with retropharyngeal hematoma sec-ondary to coagulation problems (haemophilia, hemorrhag-ic diathesis, anticoagulant therapy, ...) develop the hematomamore silently and that intubation or a tracheotomy, oncethe diagnosis has been reached, is more difficult.1
Bulging of the posterior wall of the pharynx is a sign ofa hematoma in an advanced stage, as described by Fieldand DeSaussure.
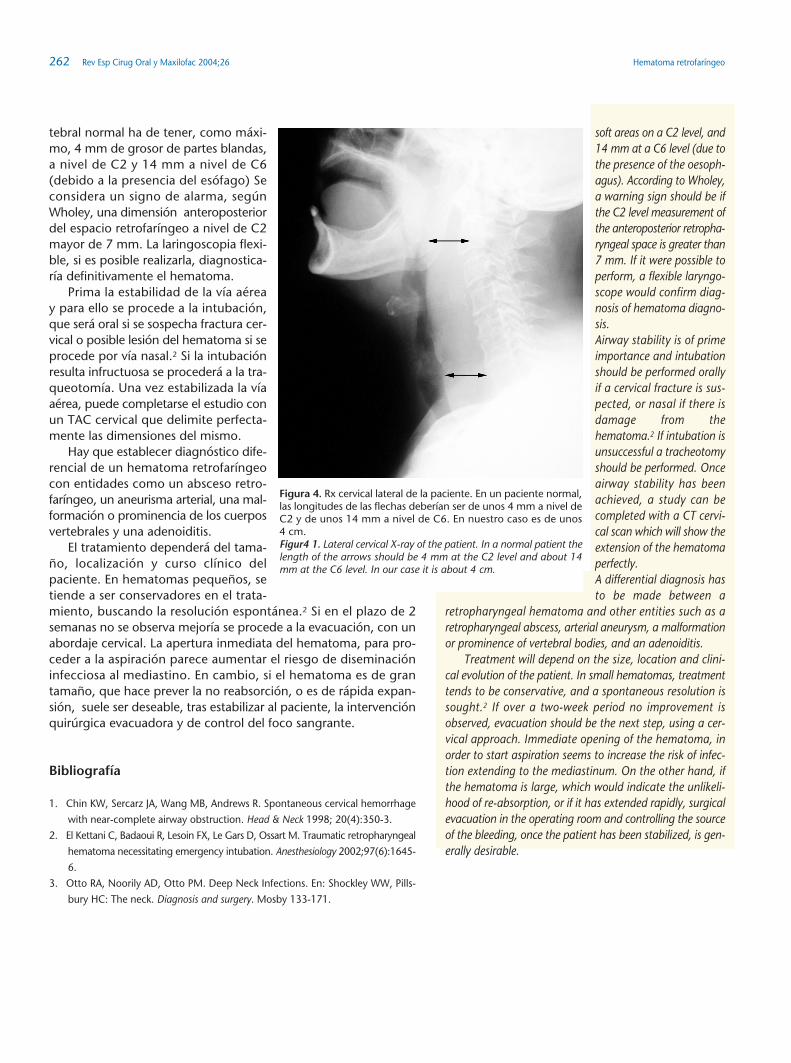
As an additional test, the lateral cervical radiography(Fig. 4) provides fundamental information. A normal pre-vertebral space should have 4mm maximum thickness of
agulante. En concreto, episodios comoel descrito, pueden aparecer en el 2%-4% de los pacientes anticoagulados.1
Clínicamente puede manifestarsepor dolor cervical, disfagia, disnea o vozgangosa. Capps et al. describen la tria-da clínica de enrojecimiento subcutá-neo en cuello anterior y tórax superior,compresión traqueal y esofágica y des-plazamiento ventral traqueal.1 Suele sercomún, que los pacientes resulten infra-diagnosticados en su fase temprana,pues al principio suelen producir levesmolestias de vías altas, pudiendo con-fundirse con una simple faringitis. Esentre las 12-48 h cuando comienzan lossíntomas alarmantes de compromiso devía aérea que requieren intubaciónurgente o traqueotomía para garanti-zar la permeabilidad. Este periodo detiempo tan dilatado es debido a la par-ticularidad de conformación del espa-cio retrofaríngeo, ya que los músculosque lo delimitan no ofrecen resisten-cia a la expansión del espacio por unhematoma.
Este espacio está situado entre lafaringe y la columna vertebral. La caraposterior del espacio retrofaríngeo estáconstituida por la fascia prevertebral,anatómicamente se describe un des-doblamiento de la misma, en un veloanterior denominado «fascia alar» y enotro posterior que es la fascia preverte-bral en si misma, delimitando entreambas un espacio virtual llamado «espa-cio peligroso». Se extiende desde la basedel cráneo hasta el mediastino poste-rior y a los lados queda delimitado porla fusión de ambos velos a nivel de lasapófisis transversas de los cuerpos ver-tebrales sucesivos. Infecciones del espa-cio retrofaríngeo pueden diseminarsehacia el espacio peligroso, y de aquí pro-gresar hacia mediastino posterior con un riesgo vital muy alto.3
El pronóstico del hematoma es bueno si se diagnostica y tratarápidamente. Está demostrado que pacientes con hematoma retro-faríngeo secundario a problemas de coagulación (hemofilia, diáte-sis hemorrágicas, terapia anticoagulante, etc.) desarrollan de unaforma más silente el hematoma y es más dificultoso, cuando sealcanza el diagnóstico, la intubación o la traqueotomía.1 Es signode hematoma en estadio avanzado el abombamiento de la paredposterior de la faringe, descrita por Field y DeSaussure.
Como prueba complementaria, la radiografía lateral cervical (Fig.4) proporciona una información fundamental. Un espacio prever-
Figura 2 y 3. TAC dos días después de la intubación. Se ve el tuboorotraqueal como único paso de la vía aérea.Figures 2 and 3 . CT scan two days after intubation. The orotra-cheal tybe is visible.
CO 26/4 22/9/04 16:50 Página 261
Hematoma retrofaríngeo262 Rev Esp Cirug Oral y Maxilofac 2004;26
tebral normal ha de tener, como máxi-mo, 4 mm de grosor de partes blandas,a nivel de C2 y 14 mm a nivel de C6(debido a la presencia del esófago) Seconsidera un signo de alarma, segúnWholey, una dimensión anteroposteriordel espacio retrofaríngeo a nivel de C2mayor de 7 mm. La laringoscopia flexi-ble, si es posible realizarla, diagnostica-ría definitivamente el hematoma.
Prima la estabilidad de la vía aéreay para ello se procede a la intubación,que será oral si se sospecha fractura cer-vical o posible lesión del hematoma si seprocede por vía nasal.2 Si la intubaciónresulta infructuosa se procederá a la tra-queotomía. Una vez estabilizada la víaaérea, puede completarse el estudio conun TAC cervical que delimite perfecta-mente las dimensiones del mismo.
Hay que establecer diagnóstico dife-rencial de un hematoma retrofaríngeocon entidades como un absceso retro-faríngeo, un aneurisma arterial, una mal-formación o prominencia de los cuerposvertebrales y una adenoiditis.
El tratamiento dependerá del tama-ño, localización y curso clínico delpaciente. En hematomas pequeños, setiende a ser conservadores en el trata-miento, buscando la resolución espontánea.2 Si en el plazo de 2semanas no se observa mejoría se procede a la evacuación, con unabordaje cervical. La apertura inmediata del hematoma, para pro-ceder a la aspiración parece aumentar el riesgo de diseminacióninfecciosa al mediastino. En cambio, si el hematoma es de grantamaño, que hace prever la no reabsorción, o es de rápida expan-sión, suele ser deseable, tras estabilizar al paciente, la intervenciónquirúrgica evacuadora y de control del foco sangrante.
Bibliografía
1. Chin KW, Sercarz JA, Wang MB, Andrews R. Spontaneous cervical hemorrhage
with near-complete airway obstruction. Head & Neck 1998; 20(4):350-3.
2. El Kettani C, Badaoui R, Lesoin FX, Le Gars D, Ossart M. Traumatic retropharyngeal
hematoma necessitating emergency intubation. Anesthesiology 2002;97(6):1645-
6.
3. Otto RA, Noorily AD, Otto PM. Deep Neck Infections. En: Shockley WW, Pills-
bury HC: The neck. Diagnosis and surgery. Mosby 133-171.
soft areas on a C2 level, and14 mm at a C6 level (due tothe presence of the oesoph-agus). According to Wholey,a warning sign should be ifthe C2 level measurement ofthe anteroposterior retropha-ryngeal space is greater than7 mm. If it were possible toperform, a flexible laryngo-scope would confirm diag-nosis of hematoma diagno-sis.Airway stability is of primeimportance and intubationshould be performed orallyif a cervical fracture is sus-pected, or nasal if there isdamage from thehematoma.2 If intubation isunsuccessful a tracheotomyshould be performed. Onceairway stability has beenachieved, a study can becompleted with a CT cervi-cal scan which will show theextension of the hematomaperfectly.A differential diagnosis hasto be made between a
retropharyngeal hematoma and other entities such as aretropharyngeal abscess, arterial aneurysm, a malformationor prominence of vertebral bodies, and an adenoiditis.
Treatment will depend on the size, location and clini-cal evolution of the patient. In small hematomas, treatmenttends to be conservative, and a spontaneous resolution issought.2 If over a two-week period no improvement isobserved, evacuation should be the next step, using a cer-vical approach. Immediate opening of the hematoma, inorder to start aspiration seems to increase the risk of infec-tion extending to the mediastinum. On the other hand, ifthe hematoma is large, which would indicate the unlikeli-hood of re-absorption, or if it has extended rapidly, surgicalevacuation in the operating room and controlling the sourceof the bleeding, once the patient has been stabilized, is gen-erally desirable.
Figura 4. Rx cervical lateral de la paciente. En un paciente normal,las longitudes de las flechas deberían ser de unos 4 mm a nivel deC2 y de unos 14 mm a nivel de C6. En nuestro caso es de unos4 cm.Figur4 1. Lateral cervical X-ray of the patient. In a normal patient thelength of the arrows should be 4 mm at the C2 level and about 14mm at the C6 level. In our case it is about 4 cm.
CO 26/4 22/9/04 16:50 Página 262

















![e]/Lu+uf gu/kflnsf, ;'v]{t · ko{6sLo :ynx¿sf] ljj/0f qm=;+= ko{6sLo :ynx¿sf] gfd j8f g+= s}lkmot! Uf+ufdfnf, b]ptL aHo}, b'uf{ dlGb/, lzj dlGb/, sflnsf dlGb/!@ wfld{s tyf ko{6lso](https://img.pdfslide.net/doc/110x75/60214045588b6704b01041b2/eluuf-gukflnsf-vt-ko6slo-ynxsf-ljj0f-qm-ko6slo-ynxsf-gfd.jpg)









![04-1251-4492-9-ED CATÁLOGO DE LAS ESPECIES DE ...ve.scielo.org/pdf/saber/v26n4/art05.pdf395 ––––––– 2014 2014 9HUVLyQ¿QDO DJRVWR 6DEHU 8QLYHUVLGDGGH2ULHQWH 9HQH]XHOD](https://img.pdfslide.net/doc/110x75/60ff9e1d1cda4e304218ed15/04-1251-4492-9-ed-catlogo-de-las-especies-de-ve-395-aaaaaaa.jpg)

