Embed Size (px)
DESCRIPTION
Cultural Competence Seminar. Teresa M. Nesman, Ph.D. November 30, 2012 Department of Child and Family Studies College of Behavioral and Community Sciences, USF. What Is Culture?. Culture definitions are developed for different purposes, emphasizing different aspects of life. - PowerPoint PPT Presentation
Citation preview

Cultural Competence Seminar
Teresa M. Nesman, Ph.D.November 30, 2012
Department of Child and Family StudiesCollege of Behavioral and Community Sciences, USF

Culture definitions are developed for different purposes, emphasizing different aspects of life.
What Is Culture?
(Kao, Hsu, & Clark, 2004)

◦ Traits, abilities, and habits that signify membership in a society Volksgeist or the "spirit of the folk” - cultural traits
are shaped by ancestral history & physical environment; include language, literature, religion, the arts, customs, & folklore (Herder, 1769)
“Complex whole”- includes knowledge, belief, art, morals, law, custom, & any other capabilities & habits acquired by man as a member of society" (Tylor, 1958 [1871])
What is Culture?

◦ Shared behavior, lifestyle, and meanings: “Customs, beliefs, values, knowledge, and skills that
guide a people’s behavior along shared paths” (Linton, 1947)
“Means by which a local population maintains itself in an ecosystem” (Rappaport, 1968 [1980])
“Pattern of meanings embodied in symbols…by means of which men communicate, perpetuate, & develop their knowledge about and attitudes toward life" (Geertz 1973)
What is Culture?

Culture is general and specific Culture is shared Culture is learned Culture is symbolic Culture is adaptive and mal-adaptive Culture is integrated Culture is dynamic
Attributes of Culture

Everyone “has” culture
Why Focus on Culture?

Sense of self Group membership- individualism vs.
collectivism Communication & language Relationships View of time Values & norms Beliefs & attitudes Mental processes & learning styles Work styles & practices Dress & appearance Food & eating habits Art & aesthetics
Stately & Clark, 2003
Dimensions of Culture

Culture is often invisible to people until they find themselves in cross-cultural situations◦ Since one is born into a culture, one experiences
that culture as always already there, part of the world that one sees, not as a way of seeing the world (Steeves & Kahn, 1995, p. 183).
Why Focus on Culture?


Culture influences most, if not all aspects of human social interactions
Why Focus on Culture?

(Cross, Bazron, Dennis, & Isaacs, 1989)
SelfActualization
Culture and Human Needs
Esteem and Identity
Love and Belonging
Safety and Security
Physiologic (e.g., Food, Water)
Culture:The way we go about meeting our
needs
Maslow’s Hierarchy Of Human Needs

Culture influences health behaviors and expectations.
Why Focus on Culture?

Typical week’s groceries in Germany : $500.07

Typical week’s groceries in China : $155.06

Typical week’s groceries in Chad : $1.62

Life trajectories and health status are impacted by culture:◦ Lifestyles◦ Help-seeking behaviors◦ Values/beliefs/norms of families & individuals◦ Values/beliefs/norms of service systems
Culture and Health

Lack of cultural compatibility between health care organizations and clients reduces access to appropriate services and can result in: ◦ Misdiagnoses (Fabrega, Ulrich, & Mezzich, 1993;
Kilgus, Pumariega, & Cuffe, 1995; Malgady & Constantino, 1998; U.S. DHHS, 2001; Yeh et al., 2002)
◦ Mistrust and low utilization of services (Snowden, 1998; Takeuchi, Sue, & Yeh, 1995; Theriot, Segal, & Cowsert, 2003; U.S. DHHS, 2001)
Culture and Help-Seeking
(Hernandez & Nesman, et al., 2006)

Understanding Cultural Influences in Yourself and Others

What was in your “back yard” when you were a child?
What did your kitchen look like? What was in it? Who spent most time in it?
What were common foods you ate? When & where did you eat?
How did you learn to read? Who helped you? What was a common saying related to health,
hygiene, or well-being? What did your parent(s)/caregivers do when you
were sick with a cold?
Activity: Childhood Memories

Cultural Competence: What is it and Why is It Important?

Culturally Diverse ContextsIndividual In context of FAMILY
CULTURALLYDIVERSEENVIRONMENT
In context of

Process of becoming adapted to a new culture, either within the natural culture or among strangers, at home or in a foreign land.
Process of learning to adjust.
Involves re-orientation of thinking, feeling, and communicating.
Acculturation

The force that moves a culture learner across a continuum from a state of no understanding of, or even hostility to, a new culture to a near total understanding.Moving from mono-culturism to bi- or multi-culturism.
Cross Cultural Competence

What seems to be right, logical, sensible, important, or obvious to a person in one culture may seem wrong, irrational, silly, unimportant, or confusing to someone in another culture.
Differences between cultures are too often perceived
as threatening or bothersome and are described in negative terms.
Most people take their own language for granted until they encounter another language.
Cross-Cultural Interactions

Understanding another culture requires personal experience
and time spent interacting with members of that cultural group.
Stereotyping is most likely to occur in the absence of frequent contact with people from other cultures.
Understanding another culture is a continuous and not a discrete process.
Culture is negotiated whenever two or more groups come in contact.
Cross-Cultural Interactions

“The acquisition of awareness, knowledge and skills needed to function effectively in a pluralistic democratic society (e.g., ability to communicate, interact, negotiate, and intervene on behalf of clients from diverse backgrounds)” (Stately & Clark, 2003)
“The ability of individuals and systems to respond respectfullyand effectively to people of all cultures, races, ethnicbackgrounds, sexual orientations, and faiths or religions in amanner that recognizes, affirms, and values the work of theindividuals, families, tribes, and communities and protects thedignity of each.” (Child Welfare League of America, 2002)
(Cross-)Cultural Competence

Individual level- engage in actions or create conditions that maximize the optimal development of clients and client systems
Organizational and societal level- develop theories, practices, policies, and organizational structures that are responsive to all groups
Levels of Action in Cultural Competence
(Stately & Clark, 2003)

Cultural Destructiveness
Cultural Incapacity
Cultural Blindness Cultural Pre-Competence
Cultural Competence
Advanced Cultural Competence
Cultural Competence Continuum
(Cross, Bazron, Dennis, & Isaacs, 1989)

Cultural destructiveness: assumes one race or culture is superior to another, e.g. social or medical experiments without knowledge or consent
Cultural incapacity: unconscious bias, paternalistic posture, may support segregation, disproportionately applies resources
Cultural Competence Continuum- 1
(Cross, Bazron, Dennis, & Isaacs, 1989)

Cultural blindness: believes ethnicity or race makes no difference, views self as unbiased yet is ethnocentric in service delivery, views minorities as culturally deprived, encourages assimilation
Cultural pre-competence: commitment to civil rights, realizes weaknesses and makes attempts to improve, hires staff that match the service population but may be only token efforts
Cultural Competence Continuum- 2
(Cross, Bazron, Dennis, & Isaacs, 1989)

Basic cultural competence: accepts and respects difference, continuously self-assesses, adapts service models, seeks advise and input from minority communities and includes informal supports
Advanced cultural competence: holds culture in high esteem, seeks to add to knowledge base, advocates continuously for cultural competence across service systems
Cultural Competence Continuum- 3
(Cross, Bazron, Dennis, & Isaacs, 1989)

ALERT
Model
for
Service
Providers
Accept: Accept the family’s beliefs, values,& practices, even if you don’t agree
Learn: Learn about the culture of thecommunity and the individualfamilies you serve; ask questionsrather than assuming you know
Explain: Explain to families why you needinformation, why time &appointments are important, & howtheir child will benefit
Respect: Respect the family’s cultural ideas,beliefs, values & practices. Findculturally appropriate ways to showrespect
Train: Support & elicit the participation offamilies in the education & trainingof providers

Multi-Cultural Panel Discussion on Help-Seeking Behavior

How does the family talk about illness? What questions are asked of a person who doesn’t feel well?
Who in the family decides what to do for a sick family member?
Where or who does the family go to for help outside the home? What kind of help is sought?
What kind of service provider is most often contacted? What do family members believe about the help they will
get at a medical facility? Where do they go in emergencies? How do families talk about insurance, financial, or legal
status? How do families address any literacy or linguistic
challenges?
Questions: Help-Seeking

What are the most difficult barriers to accessing medical services for someone from your background?
What is the worst situation you’ve ever seen that limited access to services for someone from your background?
What is the best situation you’ve seen that facilitated access to services for someone from your background?
Questions: Experiences with Accessing Services

Increasing Access to Services for Culturally Diverse Families: Organizational Cultural Competence

“A set of congruent behaviors, attitudes, and policies that come together in an agency that enables employees to work effectively in cross-cultural situations.” (Cross, Bazron, Dennis, & Isaacs, 1989)
“A culturally competent program possesses the skills and abilities to work effectively with diverse populations. This is demonstrated by serving particular subgroups of the larger population in a way that understands, is relevant to and respects the unique features, cultural beliefs, language and lifestyles within these populations” (Amherst H. Wilder Foundation, 2002)
Organizational Cultural Competence

Cultural/Linguistic characteristics of a
community’s population(s)
Infrastructure Domain/
Functions
Direct Service Domain/Functions
Degr
ee o
f com
patib
ility
defin
es le
vel o
f or
gani
zatio
nal/s
yste
mic
cultu
ral c
ompe
tenc
e
Outcomes: Reducing mental
health disparities
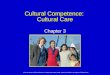
Compatibility
Definition: Within a framework of addressing mental health disparities in a community, the level of a human service organization’s/system’s cultural competence can be described as the degree of compatibility and adaptability between the cultural/linguistic characteristics of a community’s population AND the way the organization’s combined policies and structures/processes work together to impede and/or facilitate access, availability and utilization of needed services/supports (Hernandez,& Nesman, 2006).
Increasing Accessibility of Mental Health Services to Culturally/Linguistically Diverse Populations
Community Context
Hernandez, M., & Nesman, T. (2006).
Organization’s/System’s

Cultural View of Health History Language Characteristics Resource Characteristics Strength Characteristics Needs Characteristics
Knowledge/Awareness of Organizational and Community Characteristics
An organization’s/system’s
combined policies, structures and
processes
Cultural/Linguistic characteristics of a
community’s population(s)
Compatibility
Hernandez, M., & Nesman, T. (2006).

Infrastructure Domain
Direct Service Domain
• Organizational Values• Policies/Procedures/
Governance• Planning/Monitoring/
Evaluation• Communication• Human Resources
Development• Community &
Consumer Participation
• Facilitation of a Broad Service Array
• Organizational Infrastructure/ Supports- language, technology, etc.
AccessThe ability to
enter, navigate, and exit
appropriate services and
supports
AvailabilityServices and
supports exist in sufficient range and capacity to meet the needs of the population
UtilizationAppropriate
rates of use of needed mental health services
Compatibility between the infrastructure and
direct service functions of an organization
Compatible Organizational Strategies
Hernandez, M., & Nesman, T. (2006).

• Specific behaviors, knowledge, attitudes, policies, and procedures that demonstrate: Acceptance, respect, regard, flexibility, knowledge about culture
and ethnicity• Working effectively when faced with cultural differences including:
Responding effectively, linguistic competence, improving access to and quality of care for underserved
• Congruence across system components/levels: Policies and procedures that enable effective work in
cross/multi-cultural situations at all organizational levels• Self-assessment and quality assurance• On-going development of knowledge, resources, and service
models: Knowledge and skills to use appropriate assessment and
treatment methods
Key Aspects of Organizational Cultural Competence
(Cross, Bazron, Dennis, & Isaacs, 1989)

Organizational Cultural Competence: Assessment of Progress

Awareness of one’s own and others’ culture (beliefs, values, assumptions), and one’s own prejudices & stereotypes
Knowledge about and sensitivity to diverse clients being served (e.g., epidemiology, social context, resources, etc.)
Developing appropriate service strategies and techniques (e.g. cross-cultural communication skills, openness, flexibility & adaptability, knowing when interpretation is needed, etc.)
Individual Competencies
(Seeleman, Suurmond, & Stronks, 2009; Stately & Clark, 2003; Suh, 2004; )

Acknowledgement of culture◦Observable behaviors & attitudes demonstrate
acceptance, respect, regard, flexibility, & knowledge about communities served.
◦Policies, procedures, & documents demonstrate acceptance, respect, regard, flexibility, & knowledge about communities served.
Ongoing assessment◦Ongoing self-assessment of cross-cultural
relations◦Ongoing quality assurance
Organizational Competencies
(Cross, Bazron, Dennis, & Isaacs, 1989; Harper, Hernandez, Nesman, Mowery, Worthington, & Isaacs, 2006)

Responsiveness to cross-cultural dynamics◦ Organization recognizes and responds effectively
to cross-cultural issues that impact access to care◦ Linguistic adaptations meet client needs◦ Organization facilitates equal access to and
utilization of quality care Cultural knowledge development
◦ Ongoing development of knowledge about characteristics of communities served
◦ Ongoing assessment of organizational compatibility with the communities served
Organizational Competencies Detail- 2
(Cross, Bazron, Dennis, & Isaacs, 1989; Harper, Hernandez, Nesman, et al., 2006)

Adaptation for compatibility◦ Adaptations are made to policies and procedures to
increase compatibility with community characteristics
◦ Input and feedback is regularly sought from community members & clients
◦ Infrastructure supports the delivery of compatible & effective direct services
◦ Outcomes are meaningful to providers, families, & community members (quality of life, satisfaction with services, treatment effectiveness, costs effectiveness, etc.)
Organizational Competencies Detail- 3
(Cross, Bazron, Dennis, & Isaacs, 1989; Harper, Hernandez, Nesman, et al., 2006)

Cautions Avoid stereotyping- culture is not static, and varies by
individuals and families, it’s not a single variable, it’s a dynamic process
Attention to culture may be interpreted as intrusive or singling out as “different” (i.e., not normal, an outsider)
Cultural assumptions may hinder practical understanding (e.g., access may be hindered by work hours rather than cultural beliefs)
Medical terms can stigmatize- use culturally appropriate explanations & terms, ask “What do you call this problem?”
Don’t assume that health goals are the same, ask “What matters most to you?”
(Kleinman & Benson, 2006)

Cultural Competence Outcomes More effective, holistic care for diverse patients Improved quality of life of patients Increased health care satisfaction Improved perception of health care providers Better adherence to prescribed treatments Personal & professional growth of health care providers Improved quality of care Improved provider-patient rapport Treatment effectiveness Cost effectiveness (increased adherence, reduced
emergency care) Reduced disparities in health outcomes for diverse groups
(Suh, 2004)

Linking Refugee Children to Services in the Community

What cross-cultural issues are identified? How has the organization developed
knowledge about the population? How has the organization facilitated access
to services? How does the organization determine its
effectiveness in serving the population?
Questions

Using a Cultural Competence Assessment Tool

Individual Level AssessmentCognitive Domain___ Cultural awareness- appreciation and sensitivity to
values, beliefs, lifeways, practices, & problem-solving strategies of clients
___ Cultural knowledge- learning about other cultures’ worldview, languages, & social contexts through cultural immersion or extensive training
Affective Domain___ Cultural sensitivity- intentional and affective
perception of cultural diversity and respect for cultural differences
(Suh, 2004)

Individual Level AssessmentBehavioral Domain___ Ability to conduct cultural and physical
assessments & communicate cross-culturally to learn patients’ cultural beliefs, values, and practices & determine proper interventions
Environmental Domain___ Cultural encounter experience with patients of
different cultural backgrounds, either in cultural immersion or international programs
(Suh, 2004)

Organizational Values_____ Cultural competence is incorporated into
the organization’s mission statement_____ Staff is familiar with and understands
cultural competence in the organization_____ Organizational leadership and staff say
cultural competence is important
Cultural Competence Assessment Domains 1

Policies, Procedures, & Governance_____ Policies and procedures include cultural and
linguistic competence._____ Policies and procedures in the principal
language of the client._____ Administrators, the board of directors, and
committees support culturally competent practices.
_____ Proportional representation of diverse group members at all levels.
Cultural Competence Assessment Domains 2

Planning, Monitoring, & Evaluation_____ Baseline information on cultural groups is collected_____ Ongoing awareness of cultural group characteristics_____ Cultural competence plan is updated annually._____ Cultural competence planning involves staff and
clients._____ Systematic collection of information about groups
served and staff demographics._____ Monitoring of access to and quality of services for all
groups served._____ Programs fit the cultural and historical aspects of
communities and staff
Cultural Competence Assessment Domains 3

Communication_____ Leadership communicates with staff about cultural
competence._____ Community feedback is solicited and responded
to. _____ Organization décor and written materials
communicate a culture-affirming message. _____ Staff able to communicate effectively in ways that
are easily understood by diverse audiences._____Targeted outreach activities to communicate health
care information in appropriate languages & literacy levels.
Cultural Competence Assessment Domain 4

Human Resource Development_____ Diverse staff recruited with knowledge of
community served. _____ Diverse staff retained and promoted equitably._____ Staff knowledgeable about federal and state
statutes and regulations for cultural and linguistic competence.
_____ Staff evaluated on cultural and linguistic competence for promotion.
_____ Bilingual interpreters assessed for ability to accurately translate in health settings.
Cultural Competence Assessment Domains 5

Community and Consumer Participation_____ Organizational leadership and staff collaborate
with clients and community members in developing culturally competent services.
_____ Staff participates in cultural functions and community education activities.
_____ The organization purchases goods and services from community-based and minority businesses.
_____The organization values the opinions of clients, & solicits feedback.
_____Staff involved in community advocacy for social issues.
Cultural Competence Assessment Domains 6

Facilitation of a Broad Service Array_____Services are appropriate for community
culture & incorporate strengths in all aspects of care.
_____ Services are accessible, facilitate’ use, & provide for continuity of care.
_____ Facilitates obtaining health education materials & other resources in appropriate languages.
Cultural Competence Assessment Domains 7

Organizational Resources_____Database systems, set up to support planning,
monitoring, and evaluating services for diverse clients, including tracking disparities.
_____Financial resources support cultural competence, such as diversity training or compensation for bilingual capacity.
_____Communication resources support cultural and linguistic competence through appropriate technologies and staffing (e.g., interpreters, etc.).
_____ Culturally/linguistically appropriate educational media, forms, literature, and service directories.
Cultural Competence Assessment Domains 8

Data Sources Mission statement, other documents Website & other media Outreach activities Attendance records for meetings Meeting minutes Participant evaluation/satisfaction surveys Personnel files Clinical records; case records MIS data Opinion surveys Participant observation (journal) Interviews with staff; administrators; community members

A developmental process: Cultural competence is a goal toward which professionals, agencies, and systems can strive; it can be learned & improved
A continuum: Responses to cultural difference move back & forth along the continuum, varying for individuals, groups, points in time, & contexts
An ongoing process: It is active, developmental, iterative, and aspirational rather than achieved
PROCESS OF CULTURAL COMPETENCE

Resourceshttp://rtckids.fmhi.usf.edu/rtcpubs/CulturalCompetence/porch/default.cfm
http://rtckids.fmhi.usf.edu/rtcpubs/CulturalCompetence/services/default.cfm
http://rtckids.fmhi.usf.edu/rtcpubs/CulturalCompetence/protocol/default.cfm

Betancourt, J.R., & Green, A.R. (2010). Linking cultural competence training to improved health outcomes: Perspectives from the field. Academic Medicine, 85, 4: 583-585.
Callejas, L.M., Hernandez, M., Nesman, T., and Mowery, D. (2010). Creating a front porch in systems of care: Improving access to behavioral health services for diverse children and families. Evaluation and Program Planning 33,1:32-35.
Cross, T., Bazron, B., Dennis, K., & Isaacs, M. (1989). Toward a culturally competent system of care: A monograph on effective services for minority children who are severely emotionally disturbed. Washington, DC: National Technical Assistance Center for Children’s Mental Health.
Harper, M., Hernandez, M., Nesman, T., Mowery, D., and Worthington, J., Isaacs, M. (Eds.) (2006). Organizational Cultural Competence Assessment: A Review of Assessment Protocols (Making Children’s Mental Health Services Successful series, FMHI pub. No. 240-2). Tampa, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute, Research & Training Center for Children’s Mental Health. Available: http://rtckids.fmhi.usf.edu/rtcpubs/CulturalCompetence/protocol/default.cfm
Hernandez, M., Nesman, T., Isaacs, M., Callejas, L. M., & Mowery, D. (Eds.). (2006). Examining the research base supporting culturally competent children’s mental health services. Tampa, FL: USF, Louis de la
Parte Florida Mental Health Institute, Research & Training Center for Children’s Mental Health.
Hernandez, M., Nesman, T., Mowery, D., Acevedo-Polakovich, I. D., and Callejas, L. M. (2009). Cultural competence: A review and conceptual model for psychiatric and mental health services. Psychiatric Services, 60, 8:1046-1050.
Kleinman, A., & Benson, P. (2006). Anthropology in the clinic: The problem of cultural competency and how to fix it. PLOS Medicine 3, 10: 1673-1676.
Seeleman, C., Suurmond, J., & Stronks, K. (2009). Cultural competence: A conceptual framework for teaching and learning. Medical Education 43: 229-237.
Siegel, C., Davis-Chambers, E., Haugland, G., Bank, R., Aponte, C., & McCombs, H. (2000). Performance measures of cultural competency in mental health organizations. Administration and Policy in Mental Health 28, 2:91-106.
Stately, A.L., & Clark, R.L. (2003). AIDS Project Los Angeles & United American Indian Involvement, Inc.
Suh, E.E. (2004). The model of cultural competence through an evolutionary concept analysis. Journal of Transcultural Nursing 15: 93-102.
U.S. Department of Health and Human Services [DHHS]. (1999). Mental health: A report of the Surgeon General. Rockville, MD: Author.
World Health Organization. (2001). The World Health Report 2001. Mental Health: New Understanding, New Hope. France. http://www.who.int/entity/whr/2001/en/whr01_en.pdf
References