Embed Size (px)
Citation preview

Page 1 of 3
Case report
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Augustatou CG, Glynos CL, Cokkinos P, Papaparaskevas J. Culture-negative endocarditis due to Mycoplasma pneumonia. OA Case Reports 2013 Feb 28;2(2):12.
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to c
once
ption
and
des
ign,
man
uscr
ipt p
repa
ratio
n, re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
Ana
esth
etic
s &
Criti
cal C
are
Culture-negative endocarditis due to Mycoplasma pneumoniae
CG Augustatou1*, CL Glynos2, P Cokkinos3, J Papaparaskevas4
AbstractIntroductionWe report a case of culture-negative endocarditis due to Myc-oplasma pn-eumoniae.Case reportA 50-year-old woman was admitted for heart failure in our intensive car-e unit. Transoesophageal echocardi-ography revealed severe mitral reg-urgitation due to a flail posterior le-aflet with ruptured chordae tendine-ae and an 8-mm vegetation. The pat-ient received 10 days of combined a-ntibiotic therapy before undergoing successful mitral valve replacement. This is the second reported case of M. pneumoniae endocarditis in an i-mmunocompetent patient, suggesti-ng that this pathogen should be con-sidered as a cause of endocarditis with negative blood cultures.ConclusionExperience with the treatment of Mycoplasma endocarditis is too lim-ited to make any recommendations.
IntroductionCardiovascular infections caused by mycoplasmas have rarely been de-scribed and are associated with high
mortality. However, this pathology has been suggested since 1978. Di-agnosis is difficult to make, as these bacteria are not observed on Gram-stained smears and are difficult to cultivate1.
Several studies have suggested that broad range PCR analysis target-ing the 16S rDNA sequence in cardiac valve tissue specimens is a promising tool for aetiologic diagnosis of endo-carditis but with some limitations1.
We report the second case of cul-ture-negative endocarditis due to Mycoplasma pneumoniae in an im-munocompetent patient.
Case ReportA 50-year-old woman who was an active smoker and had a history of chronic obstructive pulmonary disease (COPD) was admitted to the intensive care unit of our hospital withcardiac failure. Ten days before her admission, she had been hospi-talized in the Respiratory depart-ment of another hospital because of insistent non-productive cough and progressively increasing dyspnoea. She had no previous history of car-diovascular disease and did not have domestic animals or birds.
On physical examination, she was afebrile, in sinus tachycardia (120 bpm) and with a blood pressure of 90/50 mm Hg. Cardiac ausculta-tion revealed a moderate (4/6 in in-tensity) pansystolic apical murmur. Lung auscultation revealed bilateral basal crepitations. Her chest X-ray showed diffuse airspace opacifica-tion, small bilateral effusions and car-diac enlargement. Transoesophageal echocardiography was performed to reveal a hyperdynamic left ventricle and severe mitral regurgitation with
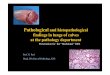
rupture of the chordae tendineae and a flail posterior leaflet (Figure 1). On top of the ruptured chordae tendine-ae, an 8-mm vegetation was ob-served. The patient’s white blood cell count was 1.37 × 103/ml, haemoglo-bin concentration was 13.7g/100 ml, erythrocyte sedimentation rate was 92 mm/h and C-reactive protein level was 11.3mg/L. A progressive eleva-tion of liver enzymes was observed [from normal values on admission to lactate dehydrogenase (LDH) 587, aspartate aminotransferase (AST)
* Corresponding Author Email: [email protected] Anaesthesiology Department and Intensive
Care Unit, Municipal Hospital of Athens, Athens 11522, Greece
2 George P. Livanos and Marianthi Simou Laboratories, Evangelismos Hospital, 1st Department of Pulmonary and Critical Care, University of Athens, Athens, 10675, Greece; Laboratory of Molecular Pharmacology, Department of Pharmacy, University of Patras, Patras, Greece
3 2nd Cardiology Department, Onassis Cardiac Surgery Center, 356 Syngrou Avenue, Athens 17674, Greece
4 Departmentof Microbiology, Medical School, National and Kapodistrian University of Athens, Athens 11527, Greece
Figure 1: Transoesophageal echo-cardiography: Prolapse of the posterior mitral leaflet (P2-P3). Rupture of chordae tendineae (flail leaflet). A mobile 8-mm vegetation is also visible.

Page 2 of 3
Case report
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Augustatou CG, Glynos CL, Cokkinos P, Papaparaskevas J. Culture-negative endocarditis due to Mycoplasma pneumonia. OA Case Reports 2013 Feb 28;2(2):12.
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to c
once
ption
and
des
ign,
man
uscr
ipt p
repa
ratio
n, re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
238 and alanine aminotransferase (ALT)94 IU eleven days later].
Three sets of blood cultures, each consisting of an aerobic and an an-aerobic bottle (Bactec 9000, Becton Dickinson and Co, Franklin Lakes, NJ, USA), were taken before antibi-otic administration; the cultures re-mained negative after an incubation period of 7 days. Sputum and urine specimens taken for culture also test-ed negative. Blood serological tests (ELISA method) for Legionella pneu-monophila, Chlamydia pneumoniae, Brucella spp., Coxiella burnetii, Bar-tonella spp., Influenza virus A and B, respiratory syncytial virus and As-pergillus spp., performed on admis-sion, were negative.
Τhe serum samples for IgM and IgG antibodies to M. pneumoniae were positive. The IgG and IgM titres were 14.1 and 17.6 IU/ml, respec-tively (normal range for IgG and IgM: <9 = negative, >11 = positive). During the observation period of one month, the values were 14 and 20.7 lU/ml, respectively.
After cultures and serological tests were performed, a diagnosis of en-docarditisdue to M. pneumoniae was confirmed, and intravenous antibi-otic treatment with linezolid (600 mg/12h), ceftriaxone (2g/12h), gen-tamycin (80 mg/8h) and azithromy-cin (500 mg/12h) was initiated. Ten days after the initiation of antibiotic therapy, the patient underwent mi-tral valve replacement. Aerobic and anaerobic cultures of the excised mi-tral valve tissue tested negative.
DNA was extracted from the valve tissue using the QIAamp DNA Mini kit (Qiagen, Hilden, Germany), accord-ing to the manufacturer’s instruc-tions. Two PCR assays were used for detection of the causative agent: a previously described M. pneumoniae species-specific semi-nested PCR as-say and a broad-range 16S rRNA PCR assay1–5 (but with negative results).
The prosthetic mitral valve was functioning normally on follow-up echocardiography. The patient was
discharged on her 12th postoperative day, and she remains well one year later.
DiscussionEndocarditis due to M. pneumo-niae has been very rarely described and is associated with high mortal-ity. Among the published reports on blood culture-negative endocarditis with underlying valvular abnormali-ties, congenital heart disease, or pros-thetic valves, we found only 7 reports of Mycoplasma endocarditis1,6–11, and M. hominis was the causative agent in most of these; M. pneumo-niae endocarditis was described in only one, a 21-year-old patient with rheumatic aortic valve disease11. We present the second case of an im-munocompetent patient with blood culture-negative endocarditis due to M. pneumoniae.
Our diagnosis was based on the combination of transoesophageal echocardiographic findings and the results of serologic testing. A possi-ble source of bacteraemia could be the colonization of the respiratory system after an atypical pneumonia (the patient was a smoker with a his-tory of COPD).
The results of PCR analysis of the mitral valve tissue were negative. Possible reasons for this could be a low bacterial tissue load or a delay inperforming the PCR. As stated ear-lier, Mycoplasma endocarditis is a rare entity and has been described in studies based on the 16S rDNA analy-sis of cardiac valve specimens in only two cases1.
In our patient, the diagnosis and adjusted therapy for Mycoplasma en-docarditis was based on compatible clinical features and serologic chang-es appropriate for a recent M. pneu-moniae infection. It is important to exclude the diagnosis of Mycoplasma endocarditis, even in the absence of pneumonia, because the evolution of the disease may be fatal and requires specific antibiotic therapy, compris-ing β-lactams and aminoglycosides,
which are usually used in the treat-ment of bacterial endocarditis and are not effective8,12.
ConclusionExperience with the treatment of My-coplasma endocarditis is too limited to make any recommendations. In our case, and throughout the post-operative course, newer macrolides were the treatment of choice. Fortu-nately, the patient received appro-priate treatment and survived to full recovery.
ConsentWritten informed consent was obtained from the patient for publi-cation of this case report and accom-panying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
References1. Fenollar F, Gauduchon V, Casalta J-P, Lepidi H, Vandenesch F, Raoult D. My-coplasma endocarditis: two case re-ports and a review. Clin Infect Dis. 2004 Feb;38(3):e21–4.2. Goldenberger D, Kunzli A, Vogt P, Zbin-den R, Altwegg M. Molecular diagnosis of bacterial endocarditis by broad-range PCR amplification and direct sequenc-ing. J Clin Microbiol. 1997 Nov;35(11): 2733–9.3. Gauduchon V, Chalabreysse L, Etienne J, Celard M, Benito Y, Lepidi H, et al. Mo-lecular diagnosis of infective endocar-ditis by PCR amplification and direct sequencing of DNA from valve tissue. J Clin Microbiol. 2003 Feb; 41(2):763–6.4. Grijalva M, Horvath R, Dendis M, Erny J, Benedik J. Molecular diagnosis of culture negative infective endocarditis: clinical validation in a group of surgically treated patients. Heart. 2003 Mar;89(3):263–8.5. La Scola B, Michel G, Raoult D. Use of amplification and sequencing of the 16S rRNA gene to diagnose Mycoplasma pneumoniae osteomyelitis in a patient with hypogammaglobulinemia. Clin In-fect Dis. 1997 Jun;24(6):1161–3.6. Hidalgo-Tenorio C, Pasquau J, López-Checa S, López-Ruz MA. Endocarditis due to Mycoplasma hominis. Enferm In-fecc Microbiol Clin. 2006 Aug–Sep;24(7): 470–1.

Page 3 of 3
Case report
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Augustatou CG, Glynos CL, Cokkinos P, Papaparaskevas J. Culture-negative endocarditis due to Mycoplasma pneumonia. OA Case Reports 2013 Feb 28;2(2):12.
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to c
once
ption
and
des
ign,
man
uscr
ipt p
repa
ratio
n, re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
by Mycoplasma hominis. Am J Med. 1989 Jun;86(6 Pt 2):819–21. 11. Popat K, Barnardo D, Webb-Peploe M. Mycoplasma pneumoniae endocarditis.Br Heart J. 1980 Jun;44(1):111–2. 12. Le T, Bayer A. Combination antibiotic therapy for infective endocarditis. Clin Infect Dis. 2003 Mar;36(5):615–21.
hominis. Eur J Clin Microbiol Infect Dis. 2000 Aug;19(8):638–40.9. Morimoto S. Endocarditis and myo-carditis caused by Mycoplasma. Ryoiki-betsu Shokogun Shirizu. 1999;(24 pt 2): 244–8. 10. Cohen JI, Sloss LJ, Kundsin R, Golightly L. Prosthetic valve endocarditis caused
7. Dominguez SR, Littlehorn C, Nyquist AC. Mycoplasma hominis endocardi-tis in a child with a complex congenital heart defect. Pediatr Infect Dis J. 2006 Sep;25(9):851–2. 8. Blasco M, Torres L, Marco M, Moles B, Villuendas M, Garcia Moya J. Prosthetic valve endocarditis caused by Mycoplasma




![Mycoplasma hominis Septic Arthritis of the Hip … … · pus cells (white blood cell [WBC] ... and a positive and negative predictive value of 96 ... Mycoplasma hominis Septic Arthritis](https://img.pdfslide.net/doc/110x75/5b02ebcb7f8b9a65618ffba3/mycoplasma-hominis-septic-arthritis-of-the-hip-pus-cells-white-blood-cell.jpg)