Embed Size (px)
Citation preview

C
BOG
AUestwbiainwsnaatJ
Opbs2icfdi
cdcT
GUPCB
n7
A
©
RESEARCH
urrent Research
eyond Energy Balance: There Is More tobesity than Kilocalories
EORGE A. BRAY, MD; CATHERINE M. CHAMPAGNE, PhD, RD, FADA
tavsmails
BTacHtfioriwtcdwtto
tbteifoiky(lecTssciir
BSTRACTsing an epidemiologic model of the interactions between
nvironmental agents and human hosts to explain obe-ity, we explored food, medications, physical inactivity,oxins, and viruses as environmental agents that interactith a genetically programmed host to disturb energyalance and cause obesity. Large portion sizes, high fatntakes, easy access to calorically sweetened beverages,nd lack of any need to be physically active all play a rolen the toxic environment that leads to obesity. The ge-etic and physiologic responses of a host determinehether or not this toxic environment will produce obe-
ity. Reversing the current trends of obesity requires aew look at the limits of the energy balance concept, andbetter understanding of how environmental factors
cutely and chronically change the responses of suscep-ible hosts.Am Diet Assoc. 2005;105:S17-S23.
besity is a chronic, relapsing, stigmatized, neuro-chemical disease that is increasing in prevalence(1,2). During the early part of the 20th century the
revalence of obesity rose slowly, but around 1980 itegan to rise more rapidly. Children are affected by obe-ity, with the prevalence rising from 5% in 1960 to 15% in000 (2). Associated with this rise in obesity rates was anncrease in the prevalence of type 2 diabetes mellitus inhildren and adolescents (3). This presages a dire futureor these children as complications of blindness, heartisease, renal failure, and amputation disable them dur-ng the next 20 years or so.
Obesity increases health risk and the cost of healthare (4). Diabetes mellitus, gall bladder disease, heartisease, hypertension, osteoarthritis, and several types ofancer are all increased in persons with overweight.hese risks can be reversed by modest weight loss. To
. A. Bray is a Boyd professor in the Louisiana Stateniversity System and is a professor of medicine at theennington Biomedical Research Center and C. M.hampagne is a professor of nutrition at the Penningtoniomedical Research Center, Baton Rouge, LA.Address correspondence to: George A. Bray, MD, Pen-
ington Center, 6400 Perkins Rd, Baton Rouge, LA0808. E-mail: [email protected] © 2005 by the American Dietetic
ssociation.0002-8223/05/10505-1003$30.00/0
odoi: 10.1016/j.jada.2005.02.018
2005 by the American Dietetic Association
ackle the hazards of obesity for children, adolescents,nd adults, we need to adopt effective strategies for pre-ention and, where prevention fails, for treatment of obe-ity. Many children and adults with overweight are trau-atized by the stigma of obesity. Children may be teased
t school and labeled “fatty.” Adults experience prejudicen social and economic situations. Measures of quality ofife show that persons with obesity score lower on manycales and that weight loss improves their quality of life.
EYOND ENERGY BALANCEhere is no doubt that obesity results from energy imbal-nce, and that we can predict the magnitude of weighthange over time if we know the net energy balance.owever, it is what the energy balance concept does not
ell us that is most important in dealing with obesity. Therst law of thermodynamics, which describes the conceptf energy balance, does not tell us anything about theegulation of food intake or the way in which genes arenvolved in this process. It does not help us to understandhy men and women distribute fat in different places on
heir bodies, or to understand how fat distributionhanges with age. The first law also doesn’t help us un-erstand why some drugs produce weight gain and otherseight loss, or why weight loss stops after a period of
reatment with diet or medication (5). Understandinghese mechanisms will allow us to tackle the epidemic ofbesity.Another problem with the concept of energy balance is
hat we are never in energy balance. To study energyalance, we housed healthy men in small rooms (respira-ion calorimeters) where we manipulated food intake andxercise to get as close as possible to zero energy balance;e, when energy intake equals energy expenditure. Inact, we rarely got closer than 50 kcal/day, or about 2.5%ut of an intake of 2,000 kcal/day. The values for energymbalance in these healthy men ranged from 50 to 150cal/day. Had these differences been maintained for 1ear, these men would be expected to gain about 2.5 kg5.5 lb) at the smaller error and 7.5 kg (16.5 lb) at thearger error. To keep from gaining weight we must correctnergy intake or energy expenditure every few days toounterbalance the error that occurred on previous days.hese corrective responses around a weight of relativetability make it look like there is weight regulation. Forome persons, the oscillations around this balance pointan keep weight stable for many years. For others, theres a slow upward drift in this regulatory point and weights gained gradually. Persons fortunate enough to haveobust corrective responses can maintain a stable weight
ver many years. If their weight is not stable, two otherSupplement to the Journal of the AMERICAN DIETETIC ASSOCIATION S17

siTaostc
iMSgMtwi
ot(peAflatwtls
tfhpfwUwlw
towiwot
ETodeotar
FAAtfnotetccoMa
p2idsiammsgaot
rcatsdsis
Fpswt
S
trategies are available. One is conscious control, exhib-ted in some persons by a pattern of restrained eating.he second and perhaps best way to maintain weight overlong period is not counting kilocalories, but weighing
neself regularly at the same time of day on an accuratecale, and then decreasing food intake or increasing ac-ivity if weight has been gained. This can allow one toorrect weight gain before it gets out of hand.
The consequences of energy imbalance are graphicallyllustrated in the movie by Morgan Spurlock, Supersize
e (2004, Hart Sharp Video, Roadside Attractions, andamuel Goldwyn Films), in which the documentarianained 25 lb in 1 month by eating all of his meals atcDonald’s restaurants, and supersizing the portions if
he clerk asked. Because we are never in energy balance,e need to view energy balance as an ideal—not a real-
stic goal to be obtained by counting kilocalories.From the perspective of energy balance, the solution to
besity should be simple: Eat less and exercise more. Theruth of this advice was shown by Kinsell and colleagues6) for overweight persons in a metabolic ward who wererovided with all of their food. During the course of sev-ral months, patients ate diets providing 1,200 kcal/day.fter an initial rapid weight loss due to rebalancing bodyuids, subsequent weight loss was linear and was notffected by wide variations in macronutrient content ofhe diet. More recent studies using foods that were taggedith a nonradioactive isotope (carbon-13) showed that
he better the adherence to a diet, the greater the weightoss (7). Thus, it is adherence to diets, not diets them-elves, that makes the difference (8).Another limitation to the concept of energy balance as
he cause of obesity is the implication that if one is gettingatter, it is one’s own fault. One need only to control his orer energy intake and energy expenditure to control theroblem. This implies that we should blame our childrenor their obesity. This seems grossly unfair. If obesityere easily controlled by moderating energy intake, theS military would not discharge up to 5,000 men andomen yearly for failing to meet its weight standards. If
oss of livelihood is not sufficient motivation to loseeight, then the problem must be more complex.The cure of obesity in leptin-deficient human beings
reated with leptin shows a genetic basis for one type ofbesity, and that obesity is more than simply lack ofillpower (9). Although simple in theory, applying the
deas of energy balance and counting kilocalories to bodyeight control has proven unsuccessful. More than 95%f persons using diet, behavior, and lifestyle approacheso lose weight regained it in less than 5 years (10).
NVIRONMENTAL AGENTShe current epidemic can be viewed from the perspectivef an epidemiologic model, shown in Figure 1. Food,rugs, viruses, toxins, and low physical activity are thenvironmental agents that facilitate the development ofbesity. One or more of these factors acting on a suscep-ible host can produce obesity. Using this model, we canpproach the problem by manipulating either the envi-
onment or the host. w18 May 2005 Suppl 1 Volume 105 Number 5
oods the spokesperson for the Grocery Manufacturers ofmerica said in the movie Supersize Me, “The food indus-
ry is part of the problem.” Several components of ourood supply may be important in determining whether orot obesity develops. The first of these is the portion sizef packages and servings. There is convincing evidencehat when larger portion sizes are provided, more food isaten (11). Portion sizes have dramatically increased inhe past 40 years (12) and now need reduction. Calori-ally sweetened beverages that contain 10% high-fructoseorn syrup (HFCS), available in containers of 12, 20, or 32z, provide 150, 250, or 400 kcal if it is all consumed.any foods list the kilocalories per serving, but the pack-
ge often contains more than one serving.Patterns of food consumption have changed during the
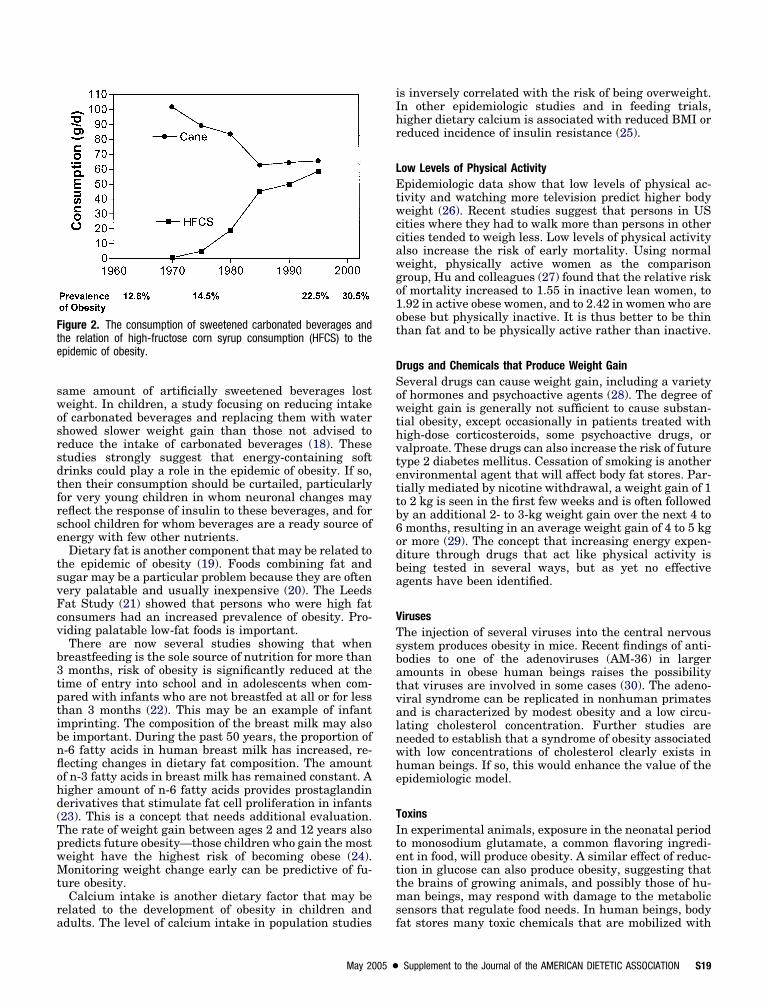
ast 30 years (13). The most striking change from 1970 to000 was in the rising consumption of HFCS (14). HFCSs now used as the caloric sweetener in almost all softrinks as well as in reconstituted juice drinks and manyolid foods. The rise in HFCS consumption occurred dur-ng the same time interval as the rapid rise in the prev-lence of obesity (2,14). On one hand, this relationshipay be strictly coincidental. But, on the other hand, itay not (Figure 2). Fructose is sweeter than glucose, or
ucrose, a molecule that is a combination of fructose andlucose. In addition, HFCS is a solution of both fructosend glucose as separate molecules, and thus it differs insmotic properties from a solution with the same concen-ration of sucrose.
The intake of calorically sweetened beverages can beelated to the epidemic of obesity (14-17). Ludwig andolleagues (15) reported that the intake of soft drinks waspredictor of initial body mass index (BMI) in children in
he Planet Health Study. They also showed that higheroft drink consumption predicted an increase in BMIuring nearly 2 years of follow-up, those with the highestoft drink consumption at baseline having the highestncrease in BMI. A Danish study (16) showed that per-ons consuming calorically sweetened beverages over 10
igure 1. Epidemiologic model of obesity. In this model, the agent thatroduces obesity is food or food-related products. If food is in limitedupply, obesity does not develop. The food that is ingested interactsith the host. In a susceptible host, the toxic effects of food produce
he disease of obesity.
eeks gained weight, whereas subjects drinking the
swosrsdtfrse
tsvFcv
b3tptibnflohd(TpwMt
ra
iIhr
LEtwccawgo1ot
DSowthvtettb6odba
VTsbatvalnwhe
TItettms
Fte
ame amount of artificially sweetened beverages losteight. In children, a study focusing on reducing intakef carbonated beverages and replacing them with waterhowed slower weight gain than those not advised toeduce the intake of carbonated beverages (18). Thesetudies strongly suggest that energy-containing softrinks could play a role in the epidemic of obesity. If so,hen their consumption should be curtailed, particularlyor very young children in whom neuronal changes mayeflect the response of insulin to these beverages, and forchool children for whom beverages are a ready source ofnergy with few other nutrients.Dietary fat is another component that may be related to
he epidemic of obesity (19). Foods combining fat andugar may be a particular problem because they are oftenery palatable and usually inexpensive (20). The Leedsat Study (21) showed that persons who were high fatonsumers had an increased prevalence of obesity. Pro-iding palatable low-fat foods is important.There are now several studies showing that when
reastfeeding is the sole source of nutrition for more thanmonths, risk of obesity is significantly reduced at the
ime of entry into school and in adolescents when com-ared with infants who are not breastfed at all or for lesshan 3 months (22). This may be an example of infantmprinting. The composition of the breast milk may alsoe important. During the past 50 years, the proportion of-6 fatty acids in human breast milk has increased, re-ecting changes in dietary fat composition. The amountf n-3 fatty acids in breast milk has remained constant. Aigher amount of n-6 fatty acids provides prostaglandinerivatives that stimulate fat cell proliferation in infants23). This is a concept that needs additional evaluation.he rate of weight gain between ages 2 and 12 years alsoredicts future obesity—those children who gain the mosteight have the highest risk of becoming obese (24).onitoring weight change early can be predictive of fu-
ure obesity.Calcium intake is another dietary factor that may be
elated to the development of obesity in children and
igure 2. The consumption of sweetened carbonated beverages andhe relation of high-fructose corn syrup consumption (HFCS) to thepidemic of obesity.
dults. The level of calcium intake in population studies f
May 2005 ●
s inversely correlated with the risk of being overweight.n other epidemiologic studies and in feeding trials,igher dietary calcium is associated with reduced BMI oreduced incidence of insulin resistance (25).
ow Levels of Physical Activitypidemiologic data show that low levels of physical ac-
ivity and watching more television predict higher bodyeight (26). Recent studies suggest that persons in US
ities where they had to walk more than persons in otherities tended to weigh less. Low levels of physical activitylso increase the risk of early mortality. Using normaleight, physically active women as the comparisonroup, Hu and colleagues (27) found that the relative riskf mortality increased to 1.55 in inactive lean women, to.92 in active obese women, and to 2.42 in women who arebese but physically inactive. It is thus better to be thinhan fat and to be physically active rather than inactive.
rugs and Chemicals that Produce Weight Gaineveral drugs can cause weight gain, including a varietyf hormones and psychoactive agents (28). The degree ofeight gain is generally not sufficient to cause substan-
ial obesity, except occasionally in patients treated withigh-dose corticosteroids, some psychoactive drugs, oralproate. These drugs can also increase the risk of futureype 2 diabetes mellitus. Cessation of smoking is anothernvironmental agent that will affect body fat stores. Par-ially mediated by nicotine withdrawal, a weight gain of 1o 2 kg is seen in the first few weeks and is often followedy an additional 2- to 3-kg weight gain over the next 4 tomonths, resulting in an average weight gain of 4 to 5 kg
r more (29). The concept that increasing energy expen-iture through drugs that act like physical activity iseing tested in several ways, but as yet no effectivegents have been identified.
iruseshe injection of several viruses into the central nervousystem produces obesity in mice. Recent findings of anti-odies to one of the adenoviruses (AM-36) in largermounts in obese human beings raises the possibilityhat viruses are involved in some cases (30). The adeno-iral syndrome can be replicated in nonhuman primatesnd is characterized by modest obesity and a low circu-ating cholesterol concentration. Further studies areeeded to establish that a syndrome of obesity associatedith low concentrations of cholesterol clearly exists inuman beings. If so, this would enhance the value of thepidemiologic model.
oxinsn experimental animals, exposure in the neonatal periodo monosodium glutamate, a common flavoring ingredi-nt in food, will produce obesity. A similar effect of reduc-ion in glucose can also produce obesity, suggesting thathe brains of growing animals, and possibly those of hu-an beings, may respond with damage to the metabolic
ensors that regulate food needs. In human beings, body
at stores many toxic chemicals that are mobilized withSupplement to the Journal of the AMERICAN DIETETIC ASSOCIATION S19

wccalae
TGSfEkr1afwfiiiactlibtd
ISlefcepwwnat(htsdl
PTmphh(t
sPtfoL(
imvt
slmtapcttrgOc
bmauvom
gbrtlsv
itiqtPrwgf
S
eight loss. The metabolic rate can be reduced by organo-hlorine molecules (31), and prolonged exposure to manyhlorinated chemicals in our environment has conceiv-bly affected metabolic pathways and energy metabo-ism. Food additives are another class of chemicals thatre widely distributed and may be involved in the currentpidemic of obesity.
HE HOSTenetic Factorsignificant insight into the causes of obesity has come
rom the cloning of genes that produce obesity in animals.xtensive molecular and reverse genetic studies (mousenockouts) have also helped establish critical pathwaysegulating body fat and food intake. Leptin, identified in994, is an important hormone produced in adipose tissuend secreted into the blood relative to the amount of bodyat (32). Leptin-deficient persons are massively obese andhen leptin is administered, food intake falls and body
at is mobilized until body weight is nearly normalized,ndicating that important metabolic-genetic pathways ex-st that can control body fat. Similar deficiencies in foodntake have been found with genetic changes in themino acid sequence of a key regulator of food intakealled the melanocortin-4 receptor (33). When this recep-or is inactive, food intake is nearly as high as wheneptin is deficient, but when partially preserved, the foodntake is only modestly above control levels (34). Theseasic biological insights tell us that body fat has impor-ant regulation that is largely, if not completely, indepen-ent of will power.
ntrauterine Imprintingeveral intrauterine events may lead to obesity later in
ife, probably due to fetal imprinting as a result of earlyxposure that affects brain plasticity. The Dutch winteramine of 1945 showed that starvation of infants in uteroould affect long-term postnatal weight status. Anotherxample is the infants of mothers who smoked duringregnancy, who have an increased risk of becoming over-eight during their first 3 decades of life when comparedith infants of mothers who did not smoke during preg-ancy (35). Similarly, infants of mothers with diabetesre at higher risk of developing obesity than infants borno mothers who did not have diabetes during pregnancy36). Infants who are small for their gestational age are atigher risk of developing central adiposity and diabeteshan normal-weight infants (24). Finally, experimentaltudies teach us that exposure to high levels of insulinuring the period of brain plasticity can lead to obesityater in life.
hysiologic Controlo maintain a stable body weight over time, the bodyust correct daily errors in energy balance. A number of
hysiologic factors are known to disturb this correction. Aigh rate of carbohydrate oxidation, as measured by aigh respiratory quotient predicts future weight gain37). One explanation is that when carbohydrate oxida-
ion is higher than carbohydrate intake, carbohydrate t20 May 2005 Suppl 1 Volume 105 Number 5
tores are depleted and we must eat to replace them.ersons with obesity who have lost weight are less effec-ive in increasing fat oxidation in the presence of a high-at meal than normal-weight persons, and this may bene reason why they are so susceptible to weight regain.ow metabolic rate may also predict future weight gain
38).Physical activity gradually declines with age, account-
ng for some increase in body fat. Recent studies suggestoderate exercise is beneficial in reducing risk of cardio-
ascular disease (39) and type 2 diabetes, and in facili-ating the oxidation of fat in the diet (40).
Fat cells in our body serve two major functions. Theytore and release fatty acids ingested from food or fromiver or fat cells and they secrete many important hor-
ones and chemicals. The discovery of leptin catapultedhe fat cell into the arena of endocrine cells (41). Inddition to leptin, the fat cell secretes a variety of othereptides (lipoprotein lipase, adipsin [complement D],omplement C, adiponectin, tumor necrosis factor-�, in-erleukin-6, plasminogen activator inhibitor-1, angio-ensinogen, bradykinin, and resistin). The fat cell alsoeleases other metabolites such as lactate, fatty acids,lycerol, and prostacyclin formed from arachidonic acid.ur understanding of fat cells as important endocrine
ells continues to expand.
To maintain a stable body weight overtime, the body must correct daily errors
in energy balance.
Production of cortisol from inactive cortisone in fat cellsy the enzyme 11-�-hydroxysteroid dehydrogenase type 1ay be important in determining the quantity of visceral
dipose tissue (42). Changes in this enzyme may contrib-te to the risk for menopausal women of developing moreisceral fat. High levels of this enzyme keep the quantityf cortisol in visceral fat high, providing a fertile environ-ent for developing new fat cells.Information about hunger and satiety comes from the
astrointestinal tract where several peptides signal theody to stop or start eating. Ghrelin (43) has receivedecent attention because, in contrast to other gastrointes-inal hormones, it stimulates food intake. Levels of ghre-in are low in obesity, except in those with Prader-Williyndrome, suggesting that it may play a role in the de-elopment of hyperphagia seen in these persons.The brain is a receiver, transducer, and transmitter of
nformation about hunger and satiety. Several neuro-ransmitter systems are involved in regulation of foodntake (44). Receptors for serotonin modulate both theuantity of food eaten and macronutrient selection andheir loss through genetic targeting produces obesity.eptide neurotransmitters also play a very importantole in the regulation of feeding. Sleep deprivation is oneay to enhance the release of peptides that produce hun-er (45). In young men allowed to sleep only 4 hours/nightor 2 days, leptin decreased and ghrelin increased relative
o the pattern seen with 10 hours of sleep on each of two
nr
ODATtaNregtodiwbt
lpmdust
dtmmtkeml
dfiaepbe
bRfsr
awpt
CWFaimthdttpblaabmvas
FOiwodmgaitcadnpidafasfbr
Tm3C
R
ights. Thus, our epidemic of obesity may reflect oneesponse to less sleep.
BESITY IS A CHRONIC, RELAPSING, NEUROCHEMICALISEASE PRODUCED BY THE INTERACTION OF ENVIRONMENTND HOSThe epidemic of obesity occurs on a genetic backgroundhat has not changed significantly in the past 100 yearsnd certainly not since the epidemic began 20 years ago.onetheless, it is clear that genetic factors play a critical
ole in the susceptibility of becoming obese in a “toxicnvironment” (46). One analogy is that genes load theun and a permissive or toxic environment pulls therigger. Modification of environmental factors acting onur ancient genes must be the strategy to prevent theisease. To believe that this can be done by a person alones to miss the argument of how environmental factors,ith major emphasis on the imprinting of the plasticrain of a growing child or adolescent, have acted onhese genes to produce the current epidemic.
We argue that the first law of thermodynamics hasulled us into the uncomfortable place of believing thatersons, through willpower, increased food choices, orore places to exercise, can overcome the current epi-
emic of obesity. Cognitive approaches relying on individ-al commitment and resolve have been unsuccessful intemming obesity in the past, and nothing suggests thathey will be more successful in the future.
At least three preventive strategies areavailable to deal with the epidemic:
education, regulation, and modificationof the food supply.
We also argue that it is what the first law of thermo-ynamics does not tell us that is important. In this con-ext, it is the unconscious host systems on which environ-ental factors operate to produce obesity. If the vendingachines that now provide kickbacks to schools con-
ained beverages with no added sugar or HFCS, availableilocalories would be reduced. We have argued that thexposure of young children to HFCS may produce detri-ental imprinting of the brain, making obesity more
ikely and more difficult to control.At least three preventive strategies are available to
eal with the epidemic: education, regulation, and modi-cation of the food supply. Education in school curriculabout good nutrition and healthful weight would be ben-ficial in helping all children learn how to select appro-riate foods and could be included in schools, with schoolreakfast and lunch programs designed to match theseducational messages.It is unwise to rely on educational strategies alone
ecause they have not prevented the epidemic of obesity.egulation is a second strategy. Regulating an improved
ood label is one good idea. Regulations on appropriateerving sizes might be part of the information provided byestaurants when requested.
Modification in some components of the food system is
May 2005 ●
third and most important strategy. Because the energye eat comes from food, we need to modify this system torovide smaller portions and less energy density if we areo succeed in combating the epidemic of obesity.
ONCLUSIONShere do dietetics professionals fit into this picture?
irst, educated dietetic professionals need to be keenlyware of the complexity of the obesity problem. A dietet-cs professional obviously cannot alter a person’s genetic
akeup, but he or she is able to address the environmen-al aspects that serve to exacerbate the situation. Simplyanding out diet sheets is not enough and should beiscouraged. Helping a patient with obesity requires at-ention to overall diet history, current eating habits, ac-ivity patterns, and behavioral obstacles that either causeroblems or prevent change. While quick weight loss maye a patient’s immediate desire, the need for permanentifestyle changes should be the primary objective. Tips forddressing this have been outlined previously by Braynd Champagne (47). Finally, dietetics professionals cane instruments of change by appealing to policymakers toodify environmental conditions, such as the school
ending machines. We can think of no better profession-ls to craft this effective message to both lawmakers andchool officials alike.
UTURE DIRECTIONSur lives are constrained by the laws of nature— grav-
ty, momentum, and thermodynamics. The strategiese employ to deal with the influence of these laws onur lives include education, regulation, and productesign. Deaths resulting from the effects of the laws ofomentum produced by automobile accidents provide a
limpse into the strategies we could use to minimizeccidents just as the law of energy balance providesdeas about how we might minimize obesity. Althoughhe laws of momentum or the laws of thermodynamicsannot be changed, their ability to produce automobileccidents and obesity can be mitigated. This can beone through better education about driving and aboututritional needs to prevent obesity. This can be com-lemented by regulations that, in the case of cars,nclude requiring seat belts, airbags, and other safetyevices. In the case of obesity, it includes limitingccess to large portion sizes and high– energy-densityoods and having an environment in which physicalctivity is more difficult to avoid. Finally, product de-ign can make cars safer, and modifying the types ofoods that are available can provide strategies to com-at the obesity epidemic by redesigning the food envi-onment.
his research was supported in part by the US Depart-ent of Agriculture CSREES Special Grant No. 2003-
4323-14010 to the Pennington Biomedical Researchenter.
eferences1. Bray GA. Obesity is a chronic, relapsing neurochem-
ical disease. Int J Obes Relat Metab Disord. 2004;28:
34-38.Supplement to the Journal of the AMERICAN DIETETIC ASSOCIATION S21
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
S
2. Flegal KM, Carroll MD, Ogden CL, Johnson CL.Prevalence and trends in obesity among US adults,1999-2000. JAMA. 2002;288:1723-1727.
3. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prev-alence and trends in overweight among US children andadolescents, 1999-2000. JAMA. 2002;288:1728-1732.
4. Klein S, Burke LE, Bray GA, Blair S, Allison DB,Pi-Sunyer X, Hong Y, Eckel RH. Clinical implicationsof obesity with specific focus on cardiovascular dis-ease: A statement for professionals from the Ameri-can Heart Association Council on Nutrition, PhysicalActivity and Metabolism endorsed by the AmericanCollege of Cardiology Foundation. Circulation. 2004;110:2952-2967.
5. Bray GA, Greenway FL. Current and potential drugsfor treatment for obesity. Endocr Rev. 1999;20:805-875.
6. Kinsell LW, Gunning B, Michaels GD, Richardson J,Cox SE, Lemon C. Calories do count. Metabolism.1964;13:195-204.
7. Lyon XH, Di Vetta V, Milon H, Jequier E, Schutz Y.Compliance to dietary advice directed towards in-creasing the carbohydrate to fat ratio of the everydaydiet. Int J Obes Relat Metab Disord. 1995;19:260-269.
8. Dansinger ML, Gleason JA, Griffith JL, Selker HP,Schaefer EJ. Comparison of the Atkins, Ornish,Weight Watchers, and Zone diets for weight loss andheart disease risk reduction: A randomized trial.JAMA. 2005;293:43-53.
9. Licinio J, Caglayan S, Ozata M, Yildiz BO, deMiranda PB, O’Kirwan F, Whitby R, Liang L, CohenP, Bhasin S, Krauss RM, Veldhuis JD, Wagner AJ,DePaoli AM, McCann SM, Wong ML. Phenotypic ef-fects of leptin replacement on morbid obesity, diabe-tes mellitus, hypogonadism, and behavior in leptin-deficient adults. Proc Natl Acad Sci USA. 2004;101:4531-4536.
0. Weighing the Options: Criteria for EvaluatingWeight-Management Programs. Washington, DC:Institute of Medicine National Academy Press;1995.
1. Diliberti N, Bordi PL, Conklin MT, Roe LS, Rolls BJ.Increased portion size leads to increased energy in-take in a restaurant meal. Obes Res. 2004;12:562-568.
2. Nielsen SJ, Popkin BM. Patterns and trends in foodportion sizes, 1977-1998. JAMA. 2003;289:450-453.
3. Putnam J, Allshouse JE. Food Consumption, Pricesand Expenditures, 1970-97. Washington, DC: USDept of Agriculture Economic Research Service;1999.
4. Bray GA, Nielsen SJ, Popkin BM. Consumption ofhigh-fructose corn syrup in beverages may play a rolein the epidemic of obesity. Am J Clin Nutr. 2004;79:537-543.
5. Ludwig DS, Peterson KE, Gortmaker SL. Relationbetween consumption of sugar-sweetened drinks andchildhood obesity: A prospective, observational anal-ysis. Lancet. 2001;357:505-508.
6. Raben A, Agerholm-Larsen L, Flint A, Holst JJ, AstrupA. Meals with similar energy densities but rich in pro-tein, fat, carbohydrate, or alcohol have different effects
on energy expenditure and substrate metabolism but 322 May 2005 Suppl 1 Volume 105 Number 5
not on appetite and energy intake. Am J Clin Nutr.2003;77:91-100.
7. Schulze MB, Manson JE, Ludwig DS, Colditz GA,Stampfer MJ, Willet WC, Hu FB. Sugar-sweetenedbeverages, weight gain, and incidence of type 2 dia-betes in young and middle-aged women. JAMA. 2004;292:927-934.
8. James J, Thomas P, Cavan D, Kerr D. Preventingchildhood obesity by reducing consumption of carbon-ated drinks: Cluster randomised controlled trial.BMJ. 2004;328:1237.
9. Bray GA, Popkin BM. Dietary fat intake does affectobesity! Am J Clin Nutr. 1998;68:1157-1173.
0. Drewnowski A, Specter SE. Poverty and obesity: Therole of energy density and energy costs. Am J ClinNutr. 2004;79:6-16.
1. Blundell JE, MacDiarmid JI. Fat as a risk factor foroverconsumption: Satiation, satiety, and patterns ofeating. J Am Diet Assoc. 1997;97(suppl):S63-S69.
2. von Kries R, Koletzko B, Sauerwald T, von Mutius E,Barnert D, Grunert V, von Voss H. Breast feedingand obesity: Cross sectional study. BMJ. 1999;319:147-150.
3. Ailhaud G, Guesnet P. Fatty acid composition of fatsis an early determinant of childhood obesity: A shortreview and an opinion. Obes Rev. 2004;5:21-26.
4. Bhargava SK, Sachdev HS, Fall CH, Osmond C, Lak-shmy R, Barker DJ, Biswas SK, Ramji S, Prabhaka-ran D, Reddy KS. Relation of serial changes in child-hood body-mass index to impaired glucose tolerancein young adulthood. N Engl J Med. 2004;350:865-875.
5. Pereira MA, Jacobs DR Jr, Van Horn L, Slattery ML,Kartashov AI, Ludwig DS. Dairy consumption, obe-sity, and the insulin resistance syndrome in youngadults: The CARDIA Study. JAMA. 2002;287:2081-2089.
6. Hancox RJ, Milne BJ, Poulton R. Association be-tween child and adolescent television viewing andadult health: A longitudinal birth cohort study. Lan-cet. 2004;364:257-262.
7. Hu FB, Willett WC, Li T, Stampfer MJ, Colditz GA,Manson JE. Adiposity as compared with physical ac-tivity in predicting mortality among women. N EnglJ Med. 2004;351:2694-2703.
8. Allison DB, Mentore JL, Heo M, Chandler LP, Cap-pelleri JC, Infante MC, Weiden PJ. Antipsychotic-induced weight gain: A comprehensive research syn-thesis. Am J Psychiatry. 1999;156:1686-1696.
9. O’Hara P, Connett JE, Lee WW, Nides M, Murray R,Wise R. Early and late weight gain following smokingcessation in the Lung Health Study. Am J Epidemiol.1998;148:821-830.
0. Dhurandhar NV, Israel BA, Kolesar JM, MayhewGF, Cook ME, Atkinson RL. Increased adiposity inanimals due to a human virus. Int J Obes RelatMetab Disord. 2000;24:989-996.
1. Tremblay A, Pelletier C, Doucet E, Imbeault P.Thermogenesis and weight loss in obese individu-als: A primary association with organochlorine pol-lution. Int J Obes Relat Metab Disord. 2004;28:936-939.
2. Zhang Y, Proenca R, Maffei M, Barone M, Leopold L,
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
Friedman JM. Positional cloning of the mouse obesegene and its human homologue. Nature. 1994;372:425-432.
3. Farooqi IS, Keogh JM, Yeo GS, Lank EJ, CheethamT, O’Rahilly S. Clinical spectrum of obesity and mu-tations in the melanocortin 4 receptor gene. N EnglJ Med. 2003;348:1085-1095.
4. Farooqi IS, Yeo GS, O’Rahilly S. Binge eating as aphenotype of melanocortin 4 receptor gene muta-tions. N Engl J Med. 2003;349:606-609.
5. Toschke AM, Ehlin AG, von Kries R, Ekbom A, Mont-gomery SM. Maternal smoking during pregnancy andappetite control in offspring. J Perinat Med. 2003;31:251-256.
6. Dabelea D, Pettitt DJ, Hanson RL, Imperatore G,Bennett PH, Knowler WC. Birth weight, type 2diabetes, and insulin resistance in Pima Indianchildren and young adults. Diabetes Care. 1999;22:944-950.
7. Zurlo F, Lillioja S, Esposito-Del Puente A, NyombaBL, Raz I, Saad MF, Swinburn BA, Knowler WC,Bogardus C, Ravussin E. Low ratio of fat to carbohy-drate oxidation as predictor of weight gain: Study of24-h RQ. Am J Physiol. 1990;259:E650-E657.
8. Astrup A, Gotzsche PC, van de Werken K, RanneriesC, Toubro S, Raben A, Buemann B. Meta-analysis ofresting metabolic rate in formerly obese subjects.Am J Clin Nutr. 1999;69:1117-1122.
9. Blair SN, LaMonte MJ, Nichaman MZ. The evolutionof physical activity recommendations: How much is
enough? Am J Clin Nutr. 2004;79:913S-920S.May 2005 ●
0. Smith SR, de Jonge L, Zachwieja JJ, Roy H, NguyenT, Rood J, Windhauser M, Volaufova J, Bray GA.Concurrent physical activity increases fat oxidationduring the shift to a high-fat diet. Am J Clin Nutr.2000;72:131-138.
1. Spiegelman BM, Flier JS. Obesity and the regulationof energy balance. Cell. 2001;104:531-543.
2. Hochberg Z, Friedberg M, Yaniv L, Bader T, TiosanoD. Hypothalamic regulation of adiposity: The role of11beta-hydroxysteroid dehydrogenase type 1. HormMetab Res. 2004;36:365-369.
3. Cummings DE, Shannon MH. Roles for ghrelin in theregulation of appetite and body weight. Arch Surg.2003;138:389-396.
4. Cowley MA, Cone RD, Enriori P, Louiselle I, Wil-liams SM, Evans AE. Electrophysiological actions ofperipheral hormones on melanocortin neurons. AnnN Y Acad Sci. 2003;994:175-186.
5. Spiegel K, Tasali E, Penev P, Van Cauter E. Briefcommunication: Sleep curtailment in healthyyoung men is associated with decreased leptinlevels, elevated ghrelin levels, and increased hun-ger and appetite. Ann Intern Med. 2004;141:846-850.
6. Snyder EE, Walts B, Perusse L, Chagnon YC, Weis-nagel SJ, Rankinen T, Bouchard C. The human obe-sity gene map: The 2003 update. Obes Res. 2004;12:369-439.
7. Bray GA, Champagne CM. Obesity and the metabolicsyndrome: Implications for dietetics practitioners.
J Am Diet Assoc. 2004;104:86-89.Supplement to the Journal of the AMERICAN DIETETIC ASSOCIATION S23
C
IiX
Opi(ieaUi
eamcTpcwTr
ctetiwite
p
XlNpeP
MMAE
A
S
RESEARCH
ommentary
mproving Health Outcomes: Future Directionsn the Field
AVIER PI-SUNYER, MD, MPH; P. M. KRIS-ETHERTON, PhD, RD
etsi
imfponbmo
dnchganese
ataipagp
ccPvdpg
hbtsstS
besity has been steadily increasing in the UnitedStates for the past 3 decades. At present almost 65%of the population is overweight or obese, with the
revalence higher for minority populations. Obesity nows present in 31% of the population and overweight in 34%1). Approximately 1% of the adult population is movingnto the obese category (body mass index [BMI]�30) ev-ry year. A similar increase is being seen among childrennd adolescents (2). This pattern is not confined to thenited States, but is also occurring throughout the world,
n both developed and less developed countries (3).Obesity is associated with several risk factors and dis-
ases. These include insulin resistance, glucose intoler-nce, type 2 diabetes mellitus, hypertension, dyslipide-ia, coronary heart disease, stroke, heart failure, and
ertain kinds of cancer, as well as earlier mortality (4).his has led to increasing costs. Obesity has been re-orted to be responsible for 5.5% to 7.8% of all health careosts (5), to lead to a loss of productivity by days lost fromork, and to cause a great number of disabilities (6).hese disabilities are expensive both financially and withespect to quality of life.
The change in weight of the US population has oc-urred without changes in the gene pool, suggesting thathe root cause of the epidemic is change in lifestyle andnvironment rather than a biological genetic change inhe population. This does not imply that genes are notmportant. Between 30% and 40% of the variance ofeight is genetic (7). There is clearly a gene-environment
nteraction, with some individuals being more sensitivehan others to the “toxic” environment we now experi-nce.The environmental determinants of weight gain in the
opulation are diet and physical activity. Individuals are
. Pi-Sunyer is director, Obesity Research Center, Co-umbia University, St Luke’s-Roosevelt Hospital Center,ew York, NY. P. M. Kris-Etherton is a distinguishedrofessor of nutrition, Department of Nutritional Sci-nces, The Pennsylvania State University, Universityark.Address correspondence to: Xavier Pi-Sunyer, MD,PH, Director, Obesity Research Center, Department ofedicine, St Luke’s-Roosevelt Hospital Center, 1111msterdam Ave, Room 1020, New York, NY 10025.-mail: [email protected] © 2005 by the American Dietetic
ssociation.0002-8223/05/10505-1012$30.00/0
vdoi: 10.1016/j.jada.2005.02.027
14 Supplement to the Journal of the AMERICAN DIETETIC ASSOCIATION
ating more and exercising less, and this imbalance be-ween energy intake and energy expenditure leads to aituation in which adults between 20 and 40 years of agen this country gain about 1.8 to 2.0 pounds per year (8).
What are the future directions in the field that couldmprove health outcomes? It is evident that much re-
ains to be learned about all aspects of obesity, rangingrom basic biology to effective intervention programs forrevention and treatment. We have learned a great dealver the years about many important aspects of obesity;onetheless, we have not been able to translate it toetter intervention for prevention and treatment. Asentioned earlier, there is still an alarming increase in
verweight and obesity in all population groups.We need to do everything we can to get people to un-
erstand that they are ingesting too many calories. Weeed to improve nutrition education. This will require aombined effort of nutrition professionals, physicians,ealth maintenance organizations, insurance companies,overnment, and industry. We need to alert people tovoid large portion sizes, energy-dense foods, indiscrimi-ate snacking, high intake of caloric beverages, andmpty calories. A better understanding of the basis of aound diet that brings adequate micronutrients withoutxtra calories is required.We also need to encourage people to be more physically
ctive. This will require public awareness campaigns byhe government, the medical profession, voluntary healthgencies, and private groups. In addition, we need tomprove the environment to create the venues in whichhysical activity can take place. This includes safe streetsnd sidewalks, better and safer parks, more and openymnasiums, and more bike paths and public swimmingools.Studies to date have shown that relatively small de-
reases in weight and relatively small increases in exer-ise can have a profound effect on health. The Diabetesrevention Program (9) and the Finnish Diabetes Pre-ention Study (10) have both reported this. A 6% to 7%ecrease in weight and a 30-minute per-day increase inhysical activity can decrease the conversion of impairedlucose tolerance to diabetes by more than 50%.We need to get industry to undertake changes that can
elp to ameliorate the obesity problem. These include,oth for food companies and for restaurants, better nu-rition labeling, smaller portion sizes, lower energy den-ity, and more low-calorie alternatives. Adolescent obe-ity tracks to adult obesity, so it is particularly importanto attempt to stem the increase in obesity in this group.chool-based initiatives should be created to try to de-
elop efficacious and practical programs to prevent and© 2005 by the American Dietetic Association

rpd
tktseWpeodticpinedpeTr
prddsbrtct
esbttard
w2tdtarapAomagsl
ntiocmhrinlidticshpstprhmemoeati
iTlrlpnbapil
ptpwdloavqTl
mso
everse obesity. More and better nutrition education andhysical education are needed in the schools. We areeficient in this regard in the United States.We have learned a great deal in the last decade about
he biology of the regulation of food intake, but we need tonow much more. More research funding is needed fromhe federal government. Research is necessary for under-tanding how important centers in the gut, the brain, andlsewhere control hunger, satiety, and thermogenesis.e need to understand more about which genes are im-
ortant in turning food intake on and off and influencingnergy expenditure. We need to identify the peptides andther molecules that are important, and we need to un-erstand the mechanisms by which they work. We haveo look seriously at the genetic underpinnings of behav-or. Little work has been done in this area to date. The fatell as an endocrine organ must be studied because itroduces bioactive molecules that have an influence onnflammation, thrombosis, endothelial function, macro-utrient disposal, and energy production. The role thatctopic fat plays in the development of diabetes and car-iovascular disease needs to be better defined and ex-lained. How inflammatory stimuli abet the chronic dis-ases associated with obesity has to be further explored.he role of vascular reactivity and its relation to productseleased by excessive and ectopic fat must be defined.
We need to learn more about effective weight-loss diets/rograms and how best to counsel patients. This willequire more research that is designed to understandietary patterns (including individual components of theiet) that result in the prevention of weight gain anduccessful treatment of obesity. This research will need toe in the form of intervention trials that actually test theole of nutrients and their effects. Simply doing observa-ional longitudinal studies is not enough. Observationalross-sectional studies are worse than useless becausehey are often misleading.
Although our current tools for confronting the obesitypidemic are weak because our knowledge base is stillmall, we know enough now to make concerted efforts toegin to improve public health. This will require, as men-ioned earlier, changes in people’s consciousness abouthe problem, improved education about healthful dietsnd physical activity, an improved environment, and se-ious efforts by government and industry to help in theifficult task of turning this epidemic around.Recent dietary guidelines have addressed the over-eight and obesity problem in the United States. The005 Dietary Guidelines (11) have stressed for the firstime the importance of physical activity. The recommen-ations take into consideration the growth of obesity inhe United States and address the important issues. Inddition to the guidelines themselves, an evidence-basedeport by the Dietary Guidelines Advisory Committee haslso been published (12) and is available to all healthrofessionals and the general public. Similarly, themerican Heart Association Dietary Guidelines (13) rec-mmend that the major emphasis for weight manage-ent should be on avoiding excess total energy intake
nd following a regular pattern of physical activity. Theseuidelines are written for the general population. Wide-pread implementation of these guidelines, though chal-
enging, is necessary. Strategically, the dietetics commu- tMay 2005 ●
ity is confronted with what to do to lessen the burden ofhe obesity epidemic. Simply stated, this means develop-ng and implementing effective strategies for treatingverweight and obesity on an individual level and in largeohorts at the community, state, and national levels. Theagnitude of the obesity epidemic is so serious that, to
ave a major impact on slowing (and even stopping) theate of increase and ultimately dramatically reducing thencidence of obesity, dietetics professionals must identifyew strategies to deal with this enormous health prob-
em. Although some optimistic observers suggest that thencidence of obesity is plateauing, we see no such evi-ence to date. Hopefully, some of our remedial sugges-ions may help to bring this about. The role of the dietet-cs professional in practice has evolved in response tohanging societal needs. When the American Dietetic As-ociation (ADA) was founded in 1917, it was dedicated toelping the government conserve food and improve theublic’s health and nutrition during World War I. Historyhows that the early ADA provided valuable assistance tohis cause. The nutrition and health needs of the USopulation are different today than in 1917, with diseaseselated to overconsumption assuming prominence inealth care. In parallel, dietetics practice has changedarkedly with the evolution of many different practice
mphases (such as private practice, foodservice manage-ent, nutrition education, clinical nutrition, and many
thers) that relate to food behaviors. Thus, with the broadducation and training required of dietetics professionalsnd the diversity of expertise in the ADA membership,he dietetics profession is in a strong position to developnnovative and effective obesity intervention programs.
Traditionally, a model that favors one-on-one counsel-ng approaches has guided medical nutrition therapy.here is much information in the literature about guide-
ines for the treatment of overweight and obesity summa-ized in the National Institutes of Health Clinical Guide-ines Report (14). The role of the dietetics professional inroviding medical nutrition therapy involves assessingutritional status and planning and recommending foodehavior interventions (15). Medical nutrition therapylso involves identifying effective interviewing ap-roaches, treatment plans that involve patients/clients,deal documentation strategies, suitable follow-up time-ines, and appropriate referrals when indicated.
Although there is little dispute that dietitians are ex-erts at delivering medical nutrition therapy using thisime-honored approach, the magnitude of the obesityroblem argues that the profession must develop neways to have a substantial impact on the obesity epi-emic. The reality is that the health care profession is aong way from where it needs to be if it is to rein in thebesity epidemic. There is no question that innovativend bold new approaches must be developed for the pre-ention and treatment of obesity. The critically pressinguestion is: what are they? There is no simple solution.he dietetics profession confronts a complex and chal-
enging problem (16).What should dietetics practice look like in the future? Itust go beyond the traditional in all areas of the profes-
ion. The future paradigm will involve population-basedbesity interventions that will require the full coopera-
ion of the entire health care community. Moreover, itSupplement to the Journal of the AMERICAN DIETETIC ASSOCIATION S15

wrdottttt
psdFrsaftcldmwa
mptwiwpasswetst
elpltntmattU
R
1
1
1
1
1
1
1
1
S
ill require coordinated integration of the expertise rep-esented by different health care disciplines with theiversity of skills to develop innovative ways to tackle thebesity problem. The magnitude of the problem is suchhat the food industry and government also must be ac-ive participants in planning and implementing solu-ions. Active cooperation of the health care community,he private sector, and policymakers is essential if we areo make marked progress.
The expertise and diversity of skills of the dieteticsrofession offers much for a bold initiative to battle obe-ity. A major effort will be required to meaningfully re-uce the incidence of obesity in the population at large.irst, new education efforts are needed to overcome theampant public misunderstanding about what lifestyletrategies are effective for weight loss. The importance ofbalanced diet for lifetime health has to be at the fore-
ront of our effort. Given the public’s perceptions abouthe efficacy of unbalanced diets, this will be a majorhallenge. Dietetics professionals are well positioned toead this nutrition education effort. It is essential thatietetics professionals continue their legacy of imple-enting practice guidelines for the treatment of over-eight and obesity. This will continue to make an impactt the individual level.Dietetics professionals must emphasize sound weight-anagement approaches in all counseling sessions. Re-
eated messages about a healthful diet and physical ac-ivity patterns for achieving and maintaining a goaleight will reinforce important messages about prevent-
ng overweight and obesity, and even preventing smalleight changes that occur slowly over time. A dieteticsrofessional and patient partnership that defines reason-ble changes and expectations is important to set thetage for smaller, permanent changes. By implementingtate-of-the-art counseling skills, dietetics professionalsill have a long-term impact on the weight-managementfforts of individual clients. With advances in pharmaco-herapy for obesity, it is important for dietetics profes-ionals to work with physicians in implementing medica-ion use within the context of lifestyle change.
On a grander scale, dietetics professionals should bencouraged to participate in nutrition advocacy at theocal, state, and federal levels with policymakers and therivate sector, and to encourage healthful eating andifestyle behaviors, including developing public informa-ion campaigns (17). Importantly, they must spearheadutrition efforts to promote healthful eating behaviors athe grassroots level. Collectively, the dietetics communityust participate in the public and scientific discussions
t all levels to identify solutions and sensible and effec-ive government policies to catalyze a new frameworkhat makes substantive strides in reducing obesity in thenited States.
eferences1. Flegal KM, Carroll MD, Ogden CL, Johnson CL.
Prevalence and trends in obesity among US adults,1999-2000. JAMA. 2002;288:1723-1727.
2. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prev-alence and trends in overweight among US children and
adolescents, 1999-2000. JAMA. 2002;288:1728-1732.16 May 2005 Suppl 1 Volume 105 Number 5
3. World Health Organization. Obesity: Preventing andManaging the Global Epidemic. Report of a WHO Con-sultation on Obesity. Geneva, Switzerland, 3-5 June,1997. Geneva, Switzerland: World Health Organiza-tion; 1998. WHO Technical Report Series, No. 894.
4. Pi-Sunyer FX. Medical hazards of obesity. Ann InternMed. 1993;119:655-660.
5. Kortt M, Langley P, Cox E. A review of cost-of-illnessstudies on obesity. Clin Ther. 1998;20:772-779.
6. Wolf A, Colditz G. Current estimates of the economiccost of obesity in the United States. Obes Res. 1998;6:97-106.
7. Bouchard C, Perusse L, Rice T, Rao DC. Genetics ofhuman obesity. In: Bray G, Bouchard C, eds. Hand-book of Obesity. New York, NY: Marcel Dekker; 2004
8. Hill J, Wyatt HR, Reed GW, Peters JC. Obesity andthe environment: Where do we go from here? Science.2003;299:853-855.
9. Diabetes Prevention Program Research Group. Re-duction in the incidence of type 2 diabetes with life-style intervention or metformin. N Engl J Med. 2003;346:393-403.
0. Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT,Hamalainen H, Ilanne-Parikka P, Keinanen-Kiu-kaanniemi S, Laakso M, Louheranta A, Rastas M,Salminen V, Uusitupa M, Finnish Diabetes Preven-tion Study Group. Prevention of type 2 diabetes mel-litus by changes in lifestyle among subjects with im-paired glucose tolerance. N Engl J Med. 2001;344:1343-1350.
1. US Department of Health and Human Services andUS Department of Agriculture. Dietary Guidelinesfor Americans 2005. Available at: http://www.healthierus.gov/dietaryguidelines. Accessed Janu-ary 12, 2005.
2. United States Department of Agriculture. Report ofthe Dietary Guidelines Advisory Committee on theDietary Guidelines for Americans. USDA; Agricul-tural Research Service, 2005.
3. Krauss RM, Eckel RH, Howard B, Appel LJ, DanielsSR, Deckelbaum RJ, Erdman JW Jr, Kris-EthertonP, Goldberg IJ, Kotchen TA, Lichtenstein AH, MitchWE, Mullis R, Robinson K, Wylie-Rosett J, St Jeor S,Suttie J, Tribble DL, Bazzarre TL. AHA DietaryGuidelines—Revision 2000: A statement for health-care professionals from the Nutrition Committee ofthe American Heart Association. Stroke. 2000;31:2751-2766.
4. Clinical Guidelines on the Identification, Evaluation,and Treatment of Overweight and Obesity in Adults.The Evidence Report. Bethesda, MD: National Insti-tutes of Health. National Heart, Lung, and BloodInstitute; 1998.
5. Medical Nutrition Therapy Across the Continuum ofCare. 2nd ed. Chicago, IL: American Dietetic Associ-ation; 1998.
6. American Dietetic Association. Position of the Amer-ican Dietetic Association: Weight Management. J AmDiet Assoc. 2002;102:1145-1155.
7. North American Association for the Study of Obesity.National Nutrition Summit Position Paper. Availableat: http://www.naaso.org/nutsummit.htm. Accessed
October 2002.











C
ECNAJ
AOlDiSsIuteMcaSeRpp�
AacBHcavBH
IS2
A
©
RESEARCH
urrent Research
Continuing Education Questionnaire, page 1381Meets Learning Need Codes 1000, 4000, 5000, and 7000
ffects of Lifestyle Intervention on Health Careosts: Improving Control with Activity andutrition (ICAN)
NNE M. WOLF, MS, RD; MIR SIADATY, MD; BEVERLY YAEGER, MS, RN; MARK R. CONAWAY, PhD; JAYNE Q. CROWTHER, MS, RN;
ERRY L. NADLER, MD; VIKTOR E. BOVBJERG, PhD, MPHpd�9falClimdtTtmhJ
TddAbacop
co(lIfps
BSTRACTbjective To evaluate program and health care costs of aifestyle intervention in a high-risk obese population.esign Twelve-month randomized controlled trial compar-ng lifestyle case management to usual care.ubjects/setting Health plan members (n�147) with obe-ity (body mass index �27) and type 2 diabetes.ntervention Lifestyle case management entailed individ-al and group education, support, and referrals by regis-ered dietitians. Those in the usual-care group receivedducational material.ain outcome measures Medical and pharmaceutical health
are costs reimbursed by the participant’s primary insur-nce company.tatistical analysis Total costs were modeled using the four-quation model using previous year cost as a predictor.esults Net cost of the intervention was $328 per personer year. After incorporating program costs, mean healthlan costs were $3,586 (95% confidence interval [CI]:$8,036, �$25, P�0.05) lower in case management com-
. M. Wolf is an instructor of research, M. Siadaty is anssistant professor, M. Conaway is a professor andhair, J. Q. Crowther is project director, and V. E.ovbjerg is an associate professor, Department of Publicealth Sciences, University of Virginia School of Medi-
ine, Charlottesville. L. Nadler is chair of Endocrinologynd Metabolism, Department of Internal Medicine, Uni-ersity of Virginia School of Medicine, Charlottesville.. Yaeger is a senior health care analyst, Southernealth Services, Inc, Charlottesville, VA.Address correspondence to: Anne M. Wolf, MS, RD,
nstructor of Research, Department of Public Healthciences, 1710 Allied St, Suite 34, Charlottesville, VA2903. E-mail: [email protected] © 2007 by the American Dietetic
ssociation.0002-8223/07/10708-0007$32.00/0
tdoi: 10.1016/j.jada.2007.05.015
2007 by the American Dietetic Association
ared to usual care. The difference was driven by groupifferences in medical (�$3,316, 95% CI: �$7,829 to$320, P�0.05) but not pharmaceutical costs (�$239,5% CI: �$870 to $280, not statistically significant), withewer inpatient admissions and costs among case man-gement compared with usual care (admission preva-ence: 2.8% vs 22.5% respectively, P�0.001).onclusion Addition of a modest-cost, registered dietitian–ed lifestyle case-management intervention to usual med-cal care did not increase health care costs and suggested
odest cost savings among obese patients with type 2iabetes. Larger trials are needed to determine whetherhese results can be replicated in a broader population.he findings can be judiciously applied to support thathe addition of a registered dietitian–led lifestyle case-anagement program to medical care does not increase
ealth care costs.Am Diet Assoc. 2007;107:1365-1373.
he direct cost of diabetes in the United States was$91.8 billion in 2002 (1). The cost of overweight andobesity was equally high (2). As prevalence of both
iabetes and obesity in the United States increases (3), sooes the human and financial burden of these conditions.n estimated 38% of the increase in the cost of diabetesetween 1987 and 2001 was due to increases in the prev-lence of obesity as well as increased medical spending onare of obese individuals (4). This suggests that treatingbesity in the context of diabetes management may im-rove both health and economic outcomes.Lifestyle treatment (diet and physical activity) is the
ornerstone of treatment for both type 2 diabetes andbesity. Modest weight loss improves insulin sensitivity5) and improves glycemic control, blood pressure, andipid profiles in people with existing type 2 diabetes (6-9).ndependent of weight loss, lifestyle treatment is an ef-ective means of improving glycemic control (10), bloodressure (11,12), and lipid levels (13-18). Moreover, life-tyle treatment with modest weight loss has been shown
o be an effective (19-21) and a more cost-effective meansJournal of the AMERICAN DIETETIC ASSOCIATION 1365

tpidict
gidtcPhTctd
RtictTtwc
MT(cIcci
STdcmcweiwgd
n2p(aSilp
tpou
IDOiemopcItaGm(mbtmmfmwR
CUttfnqdl
OTtUyzbdnmrCioctft
1
o prevent diabetes than metformin or usual care inatients at high risk of developing diabetes (22,23). Reg-stered dietitians (RDs) could play a vital role in theelivery of lifestyle treatment considering their trainingn food and nutritional sciences, health, and behaviorhange. In addition, many RDs have advanced certifica-ion in diabetes and weight management.
Despite this, health systems have generally not inte-rated lifestyle treatment into clinical practice or systemat-cally reimbursed for nutrition services. The resource bur-en of some lifestyle treatments demonstrated in efficacyrials may be too great for patients, clinicians, and healthare systems to sustain. During the 3 years of the Diabetesrevention Project, the cost for lifestyle treatment, from aealth system’s perspective, was $2,780 per person (24).ranslation of lifestyle efficacy trials into lower-intensity,ost effective interventions is one approach to maximizeheir applicability and long-term maintenance for obese in-ividuals with type 2 diabetes (25,26).We have previously reported that a modestly priced,D-led case management approach to lifestyle modifica-
ion was more effective than usual medical care formproving clinical and health-related quality of life out-omes and decreasing self-reported prescription medica-ion use of patients with obesity and type 2 diabetes (27).he purpose of this analysis is to evaluate the within-rial program costs and economic outcomes associatedith a 1-year lifestyle intervention led by an RD lifestyle
ase manager.
ETHODS AND PROCEDUREShe Improving Control with Activity and Nutrition
ICAN) study was a randomized controlled trial (RCT)onducted from 2001 to 2003. The University of Virginianstitutional Review Board approved the study. It is inompliance with Health Insurance Portability and Ac-ountability Act of 1996, and all patients gave writtennformed consent.
tudy Designhe purpose of the ICAN pilot project was to evaluate theifferences in clinical, humanistic, and economic out-omes of a nutrition intervention involving lifestyle caseanagement and medical nutrition therapy by an RD
ompared with usual medical care for obese individualsith type 2 diabetes. The intervention is aimed at mod-rate weight loss (5% to 10%), improvement in diet qual-ty, and an increase in physical activity. In addition, weanted to obtain effect sizes of the intervention andather necessary data critical to planning a larger ran-omized trial.Eligibility criteria were: type 2 diabetes (ICD-9 [Inter-
ational Classification of Diseases-9th edition] code50.XX, 357.2 362.0, 362.02, or 366.41, and confirmed byhysician), diabetes medication use, body mass indexcalculated as kg/m2) of 27 or more, age 20 years or older,bility to comprehend English, and membership inouthern Health Services health plan as primary health
nsurance. Exclusion criteria were: pregnancy, cognitiveimitations, or medical reasons precluding dietary and
hysical activity modifications. g366 August 2007 Volume 107 Number 8
Eligible participants were randomly assigned to ei-her case management or usual care using randomermuted blocks with randomly chosen block sizes of 2r 4. Study personnel were blinded to allocation schedulentil assignment.
ntervention—Lifestyle Case Management by a Registeredietitianne RD case manager met with participants individually,
n groups, and by phone for assessment, goal setting,ducation, and referrals to community resources. The RDeasured weight and waist circumference, reviewed lab-
ratory results, and discussed patient-care issues withhysicians when appropriate. Individual sessions oc-urred six times throughout the year, totaling 4 hours.ndividual sessions were similar to an outpatient nutri-ion visit during which the participant’s lifestyle wasssessed and patient-centered goals were developed.oals were tailored but based on national dietary recom-endations for people with type 2 diabetes and obesity
28,29). Follow-up visits reassessed whether participantset their goals and, if not, discussed ways to overcome
arriers; goals were reset to more achievable levels. Par-icipants also attended six, 1-hour small group (10 orore people per group) sessions developed to provide theajority of education regarding diet and physical activity
or improved glucose control and weight loss. Briefonthly phone contacts provided support. Participantsere given the LEARN (Lifestyle, Exercise, Attitudes,elationships, Nutrition) manual (30).
ontrol Group—Usual Caresual care participants received written educational ma-
erial including the LEARN manual (30). Usual care pa-ients were seen by a research associate every 3 monthsor weight measurements and to complete question-aires. The research associate was allowed to answeruestions but did not assess, set goals, or have an ongoingialogue about a participant’s diet or physical activityevel.
utcome Measureshe primary outcome measures were health care utiliza-ion and health plan costs during the year of the trial.tilization is defined as the number of claims during theear, except for inpatient and pharmaceutical use. Utili-ation within the inpatient analysis represents the num-er of unique hospital admissions. Length of stay wasefined by Southern Health Services and represents theumber of nights in the hospital. Utilization in the phar-acy analysis represents the 12-month change in self-
eported number of prescription medications taken daily.ost is defined as the dollar amount paid by the health
nsurance company. We also explored other perspectivesf health care cost, including costs to patients (medicalosts�copay) and charges, but focused on costs paid byhe insurer. Direct nonmedical costs (out-of-pocket costsor exercise equipment and diet food) were not included inhis analysis.
The health plan variable “place of service” was aggre-
ated from 11 potential place of service categories. Inpa-
tOitscbagcmaocdccd9a
PPctwot2ctsmwtganlLiome
DDmhccapmtbmcccm
lCAtotci
SOsTiup
tdscmvdpwhtcs6wedcm
SAMWm(t(
womtptttPlb
RBG
ient services included all paid claims for care in hospitals.utpatient included all paid claims for services occurring
n physician offices and other clinical practices, outpa-ient hospital services, and independent laboratories out-ide physician offices. Emergency room included all paidlaims originating from emergency departments and am-ulance use. Procedures included all paid claims gener-ted by ambulatory surgical centers. Pharmaceutical wasenerated from the pharmacy database and representslaims and payment for insurance-covered prescriptionedications. Other types of services (ie, nursing home
nd rehabilitative facilities) were not included due to lowccurrence. The outcomes were defined as the sum oflaims and cost for a person from the initial visit to 365ays after that visit. There were 23 participants whoompleted the trial whose pharmaceutical claims did notover a full 365 days (three with fewer than 3 months ofata; six with fewer than 6 months; five with fewer thanmonths; and nine with fewer than 12 months). All
vailable data within that timeframe were used.
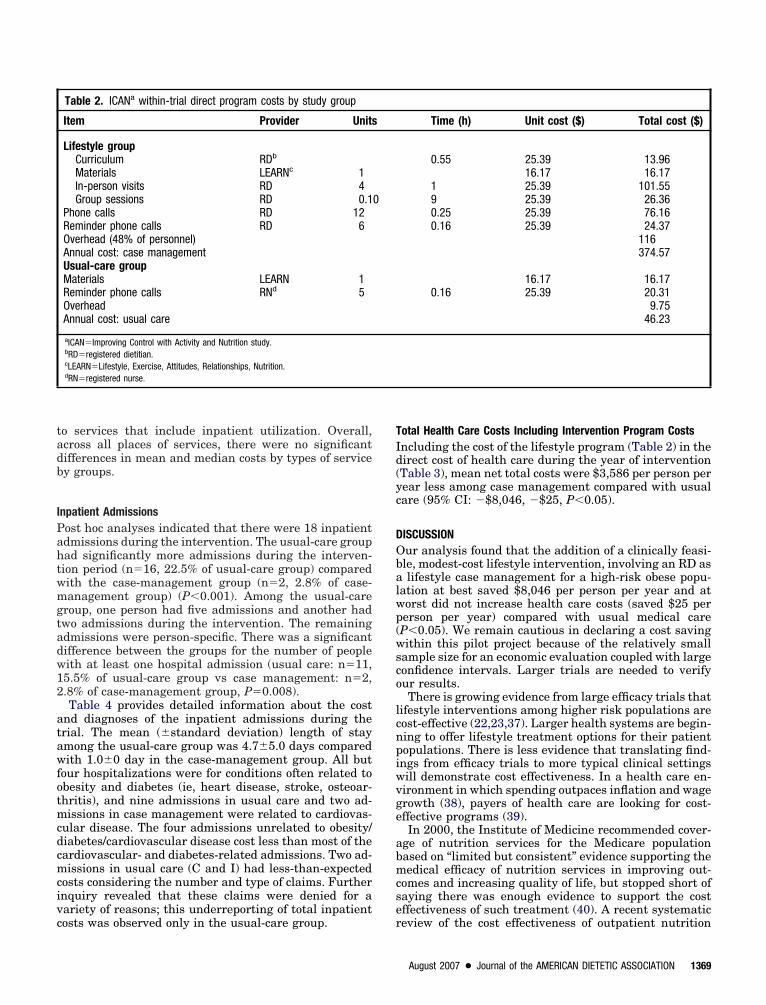
rogram Costsrogram costs were calculated by applying standard unitosts to the resources used. Resource use included educa-ional materials and patient care unit time. Unit costsere actual costs of educational material. Salary andverhead were based on published costs from the Diabe-es Prevention Project (24). All costs were adjusted to002 US dollars using the medical component of theonsumer price index (in accordance with the interven-ion year and the direct medical costs). Net program costsubtract usual-care program costs from the case manage-ent intervention program costs. Although both groupsere allowed to join other weight management or diabe-
es care programs outside the ICAN program, these pro-ram costs were minimal and are not included in thenalysis. We excluded the costs of the research compo-ent including resources used for recruitment, data col-
ection and surveillance of complications and outcomes.aboratory costs incurred as part of the study were not
ncluded in the cost of the intervention. Clinical lab testsrdered by participants’ physicians as part of their usualedical care are included as part of their direct medical
xpenses. This avoids double-counting laboratory costs.
irect Medical Costsirect medical costs typically represent expenditures foredical services and products that are usually paid for byealth systems and include costs of hospitalization, urgentare, outpatient care, laboratory tests, and procedures. Theost variables within this analysis represent the dollarmount that the health insurance plans paid the practice orrovider (physician, pharmacy, hospital). Health plan ad-inistrative data were linked to research databases by par-
icipant number. The health plans used two internal data-ases to document payments: the pharmaceutical and theedical care databases. The pharmaceutical database in-
luded outpatient prescription pharmaceutical claims andosts. The medical care database included all medicallaims (except outpatient pharmaceuticals): inpatient phar-
aceuticals, procedures and care; outpatient visits; ambu- satory procedures and diagnostic testing; and urgent care.laim and cost data were carefully evaluated for validity.bsolute cost differences between groups are reported for
he year of the trial because participants were all membersf Southern Health Services. Relative cost differences be-ween groups are reported when comparing the year pre-eding the year of the trial due to an administrative changen insurance companies between these years.
tudy and Analysis Groupne hundred forty-seven participants were randomly as-
igned to usual care (n�74) or case management (n�73).hree patients withdrew before baseline assessment, so the
ntention-to-treat analysis population was comprised of 72sual-care participants and 72 case-management partici-ants.For health care cost data in the year preceding the
rial, there were five participants without medical claimsata (ie, they were not health plan members before thetudy) and 14 participants without pharmaceuticallaims data (non–health plan members or lack of phar-aceutical benefits within their Southern Health Ser-
ices medical care coverage). For health care cost datauring the intervention (primary analysis), there were 11eople with missing pharmaceutical claims data (8 peopleithout pharmacy benefits and 3 people who: [a] didn’tave pharmacy benefits, [b] had no claims data duringhe intervention period, or [c] changed health insuranceompanies at the beginning of the trial). The final sampleize for pharmaceutical cost was 133 (65 in usual care and8 in case management). For medical claims data, thereere two participants with missing claims data for the
ntire year due to changing health insurance companiesuring the trial. Hence, the final sample size for medicallaims cost was 142 (71 in usual care and 71 in caseanagement).
tatistical Analysisdministrative data were extracted and transferred byicrosoft Access (version 5.0, 2002, Microsoft, Redmond,A). Data preparation and quality assurance was imple-ented in SPSS (version 11, 2001, SPSS, Chicago, IL)
31). Estimation of descriptive statistics, significanceests, and fitting of models has been done in both RR version 2.0, 2004, Vienna, Austria) (32) and SPSS.
The “four equation model” of Duan and colleagues (33)as used to model total costs. This approach was devel-
ped by authors of the RAND Health Insurance Experi-ent (34) to account for the wide variability observed due
o inpatient health care costs and is now commonly ap-lied to medical cost data. This method was applied onlyo medical costs and cannot be applied to the pharmaceu-ical database or to categories of health care (ie, outpa-ient care) that do not include inpatient hospitalizations.revious year cost was a predictor in the equations. Logit
ink and bias corrected and accelerated nonparametricootstrap (35) was used for obtaining standard errors.
ESULTSaseline Characteristicsroups were similar in all demographic and clinical mea-
ures at baseline (Table 1). Study participants, on aver-
August 2007 ● Journal of the AMERICAN DIETETIC ASSOCIATION 1367

aah(hbwcp
PTpc
MTcpmya
p$noicscpccmCtha
HMop
/L trigly
1
ge, were in class 2 (body mass index�35 to 39.9) obesitynd had a high-risk waist circumference, suggesting veryigh-risk obesity (36). Participants reported a mean�standard deviation) of 2.6�1.6 “health problems” (eg,ypertension) in addition to diabetes; this was similaretween groups. For the year preceding the trial, thereere no significant differences between usual-care and
ase-management participants in medical (P�0.65) orharmaceutical costs (P�0.39).
rogram Costshe direct cost of the intervention and usual care (pererson per year) are presented in Table 2. Net programosts were approximately $325 per person per year.
ean Annual Health Care Costs During Interventionhere were 5,329 pharmaceutical and 6,921 medicallaims for all participants during the 1-year interventioneriod. Total health care costs (sum of medical and phar-aceutical costs) paid by the health plan during the 1
ear of intervention were $3,911 per person per year less
Table 1. Baseline characteristics of ICANa participants by study gro
Categorical variablesFemaleWhiteSmoking status
NeverFormerCurrent
Continuous variablesAge (y)Years with diabetes diagnosisBody mass indexc
Waist circumference (cm)Glycosylated hemoglobin (%)Cholesterol (mg/dL)d
TotalLDLe
HDLf
Triglyceride (mg/dL)g
Number of medical conditions other than diabetesNumber of prescription medications/dayNumber of diabetes medications/dayAnnual medical care cost year prior to intervention ($)Annual pharmaceutical cost year prior to intervention ($)
aICAN�Improving Control with Activity and Nutrition study.bSD�standard deviation.cBody mass index calculated as kg/m2.dTo convert mg/dL cholesterol to mmoL/L, multiply mg/dL by 0.026. To convert mmol/LeLDL�low-density lipoprotein.fHDL�high-density lipoprotein.gTo convert mg/dL triglycerides to mmol/L, multiply mg/dL by 0.0113. To convert mmol
mong those receiving lifestyle case management com- b
368 August 2007 Volume 107 Number 8
ared with usual care (95% confidence interval [CI]):�8,374 to $�353, P�0.05) (Table 3). There was a sig-ificant difference in medical care costs (eg, inpatient,utpatient, procedures) (95% CI for the mean differencen cost: $�7,829 to $�320, P�0.05). Mean and medianosts and utilization for prescription medications was nottatistically significant (95% CI for the mean difference inost: $�870 to $280, P�0.28). Evaluating “cost” from theerspectives such as medical charges or adding patiento-pay onto medical costs were not statistically signifi-ant (95% CI charges: $�14,391 to $640, not significant);edical costs�co-pay: $�7,617 to $69, not significant).omparing health care costs from the year preceding to
he year of the trial, there was a relative increase inealth care costs among both groups; 84% in usual carend 41% in case management.
ealth Care Costs by Place of Serviceean and median cost and mean utilization data by place
f service are presented in Table 3. Group differences bylace of service are provided for descriptive purposes only
Usual-Care Group(n�72)
Case-ManagementGroup (n�72)
n % n %
42 58 45 6253 74 61 85
40 56 41 5730 42 27 382 3 4 64™™™™™™™™™™™™™™™™™™™™ mean�SD b ™™™™™™™™™™™™™™™™™™353.4�8.0 53.3�8.6
7.7�7.3 6.9�5.737.5�6.4 37.6�7.7
118.1�16.5 116.8�15.57.5�1.5 7.9�1.6
181�37.2 183�43.4105�33.3 105�33.744.6�12.3 45.4�12.8167�77.2 193�76.72.4�1.6 2.8�1.75.8�2.6 6.3�2.91.8�0.85 1.8�0.92
3,984�8,413 3,328�8,9672,221�2,411 1,990�2,180
sterol to mg/dL, multiply mmol/L by 38.7. Cholesterol of 193 mg/dL�5.00 mmol/L.
cerides to mg/dL, multiply mmol/L by 88.6. Triglycerides of 159 mg/dL�1.80 mmol/L.
up
chole
ecause the Duan and colleagues method is applied only
tadb
IPahtwmgtadw12
atawfotmcdcmcivc
TId(yc
DObalwp(wsco
lcnpiwvge
abmcse
o services that include inpatient utilization. Overall,cross all places of services, there were no significantifferences in mean and median costs by types of servicey groups.
npatient Admissionsost hoc analyses indicated that there were 18 inpatientdmissions during the intervention. The usual-care groupad significantly more admissions during the interven-ion period (n�16, 22.5% of usual-care group) comparedith the case-management group (n�2, 2.8% of case-anagement group) (P�0.001). Among the usual-care
roup, one person had five admissions and another hadwo admissions during the intervention. The remainingdmissions were person-specific. There was a significantifference between the groups for the number of peopleith at least one hospital admission (usual care: n�11,5.5% of usual-care group vs case management: n�2,.8% of case-management group, P�0.008).Table 4 provides detailed information about the cost
nd diagnoses of the inpatient admissions during therial. The mean (�standard deviation) length of staymong the usual-care group was 4.7�5.0 days comparedith 1.0�0 day in the case-management group. All but
our hospitalizations were for conditions often related tobesity and diabetes (ie, heart disease, stroke, osteoar-hritis), and nine admissions in usual care and two ad-issions in case management were related to cardiovas-
ular disease. The four admissions unrelated to obesity/iabetes/cardiovascular disease cost less than most of theardiovascular- and diabetes-related admissions. Two ad-issions in usual care (C and I) had less-than-expected
osts considering the number and type of claims. Furthernquiry revealed that these claims were denied for aariety of reasons; this underreporting of total inpatient
Table 2. ICANa within-trial direct program costs by study group
Item Provider Units
Lifestyle groupCurriculum RDb
Materials LEARNc 1In-person visits RD 4Group sessions RD 0.1
Phone calls RD 12Reminder phone calls RD 6Overhead (48% of personnel)Annual cost: case managementUsual-care groupMaterials LEARN 1Reminder phone calls RNd 5OverheadAnnual cost: usual care
aICAN�Improving Control with Activity and Nutrition study.bRD�registered dietitian.cLEARN�Lifestyle, Exercise, Attitudes, Relationships, Nutrition.dRN�registered nurse.
osts was observed only in the usual-care group. r
otal Health Care Costs Including Intervention Program Costsncluding the cost of the lifestyle program (Table 2) in theirect cost of health care during the year of interventionTable 3), mean net total costs were $3,586 per person perear less among case management compared with usualare (95% CI: �$8,046, �$25, P�0.05).
ISCUSSIONur analysis found that the addition of a clinically feasi-le, modest-cost lifestyle intervention, involving an RD aslifestyle case management for a high-risk obese popu-
ation at best saved $8,046 per person per year and atorst did not increase health care costs (saved $25 pererson per year) compared with usual medical careP�0.05). We remain cautious in declaring a cost savingithin this pilot project because of the relatively small
ample size for an economic evaluation coupled with largeonfidence intervals. Larger trials are needed to verifyur results.There is growing evidence from large efficacy trials that
ifestyle interventions among higher risk populations areost-effective (22,23,37). Larger health systems are begin-ing to offer lifestyle treatment options for their patientopulations. There is less evidence that translating find-ngs from efficacy trials to more typical clinical settingsill demonstrate cost effectiveness. In a health care en-ironment in which spending outpaces inflation and wagerowth (38), payers of health care are looking for cost-ffective programs (39).In 2000, the Institute of Medicine recommended cover-
ge of nutrition services for the Medicare populationased on “limited but consistent” evidence supporting theedical efficacy of nutrition services in improving out-
omes and increasing quality of life, but stopped short ofaying there was enough evidence to support the costffectiveness of such treatment (40). A recent systematic
Time (h) Unit cost ($) Total cost ($)
0.55 25.39 13.9616.17 16.17
1 25.39 101.559 25.39 26.360.25 25.39 76.160.16 25.39 24.37
116374.57
16.17 16.170.16 25.39 20.31
9.7546.23
0
eview of the cost effectiveness of outpatient nutrition
August 2007 ● Journal of the AMERICAN DIETETIC ASSOCIATION 1369
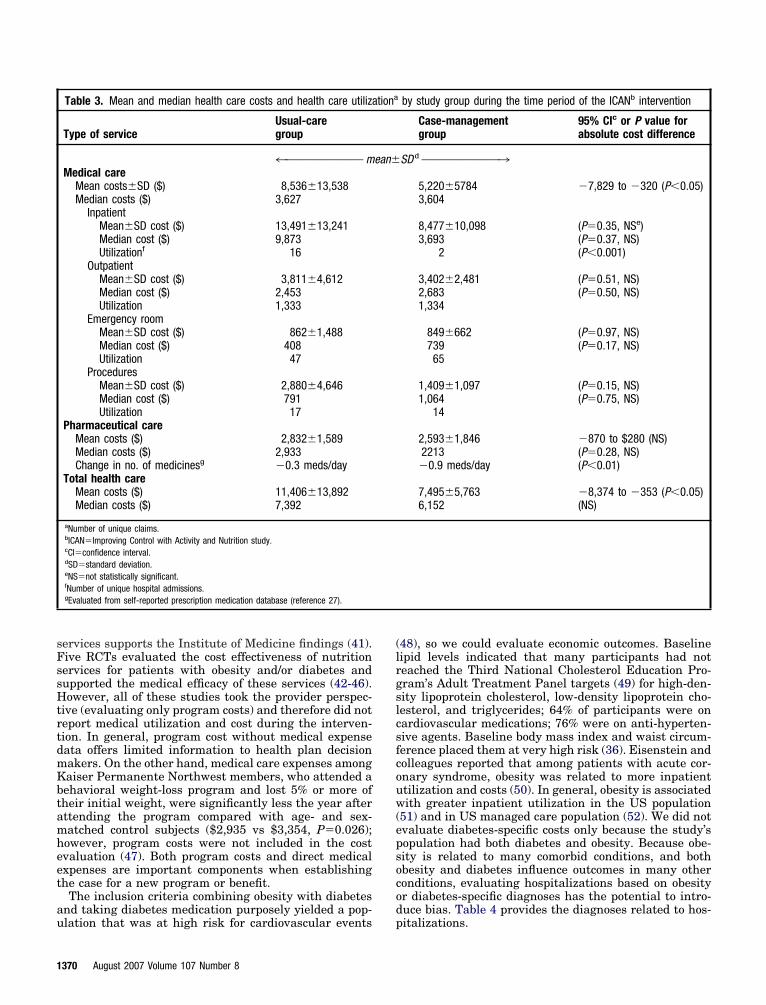
sFssHtrtdmKbtamheet
au
(lrgslcsfcouw(epsocod
1
ervices supports the Institute of Medicine findings (41).ive RCTs evaluated the cost effectiveness of nutritionervices for patients with obesity and/or diabetes andupported the medical efficacy of these services (42-46).owever, all of these studies took the provider perspec-
ive (evaluating only program costs) and therefore did noteport medical utilization and cost during the interven-ion. In general, program cost without medical expenseata offers limited information to health plan decisionakers. On the other hand, medical care expenses amongaiser Permanente Northwest members, who attended aehavioral weight-loss program and lost 5% or more ofheir initial weight, were significantly less the year afterttending the program compared with age- and sex-atched control subjects ($2,935 vs $3,354, P�0.026);owever, program costs were not included in the costvaluation (47). Both program costs and direct medicalxpenses are important components when establishinghe case for a new program or benefit.
The inclusion criteria combining obesity with diabetesnd taking diabetes medication purposely yielded a pop-
Table 3. Mean and median health care costs and health care utiliza
Type of serviceUsual-caregroup
4™™™™™™™™™™™™™ mMedical care
Mean costs�SD ($) 8,536�13,538Median costs ($) 3,627
InpatientMean�SD cost ($) 13,491�13,241Median cost ($) 9,873Utilizationf 16
OutpatientMean�SD cost ($) 3,811�4,612Median cost ($) 2,453Utilization 1,333
Emergency roomMean�SD cost ($) 862�1,488Median cost ($) 408Utilization 47
ProceduresMean�SD cost ($) 2,880�4,646Median cost ($) 791Utilization 17
Pharmaceutical careMean costs ($) 2,832�1,589Median costs ($) 2,933Change in no. of medicinesg �0.3 meds/day
Total health careMean costs ($) 11,406�13,892Median costs ($) 7,392
aNumber of unique claims.bICAN�Improving Control with Activity and Nutrition study.cCI�confidence interval.dSD�standard deviation.eNS�not statistically significant.fNumber of unique hospital admissions.gEvaluated from self-reported prescription medication database (reference 27).
lation that was at high risk for cardiovascular events p
370 August 2007 Volume 107 Number 8
48), so we could evaluate economic outcomes. Baselineipid levels indicated that many participants had noteached the Third National Cholesterol Education Pro-ram’s Adult Treatment Panel targets (49) for high-den-ity lipoprotein cholesterol, low-density lipoprotein cho-esterol, and triglycerides; 64% of participants were onardiovascular medications; 76% were on anti-hyperten-ive agents. Baseline body mass index and waist circum-erence placed them at very high risk (36). Eisenstein andolleagues reported that among patients with acute cor-nary syndrome, obesity was related to more inpatienttilization and costs (50). In general, obesity is associatedith greater inpatient utilization in the US population
51) and in US managed care population (52). We did notvaluate diabetes-specific costs only because the study’sopulation had both diabetes and obesity. Because obe-ity is related to many comorbid conditions, and bothbesity and diabetes influence outcomes in many otheronditions, evaluating hospitalizations based on obesityr diabetes-specific diagnoses has the potential to intro-uce bias. Table 4 provides the diagnoses related to hos-
by study group during the time period of the ICANb intervention
Case-managementgroup
95% CIc or P value forabsolute cost difference
SD d ™™™™™™™™™™™™™3
5,220�5784 �7,829 to �320 (P�0.05)3,604
8,477�10,098 (P�0.35, NSe)3,693 (P�0.37, NS)
2 (P�0.001)
3,402�2,481 (P�0.51, NS)2,683 (P�0.50, NS)1,334
849�662 (P�0.97, NS)739 (P�0.17, NS)65
1,409�1,097 (P�0.15, NS)1,064 (P�0.75, NS)
14
2,593�1,846 �870 to $280 (NS)2213 (P�0.28, NS)�0.9 meds/day (P�0.01)
7,495�5,763 �8,374 to �353 (P�0.05)6,152 (NS)
tiona
ean�
italizations.
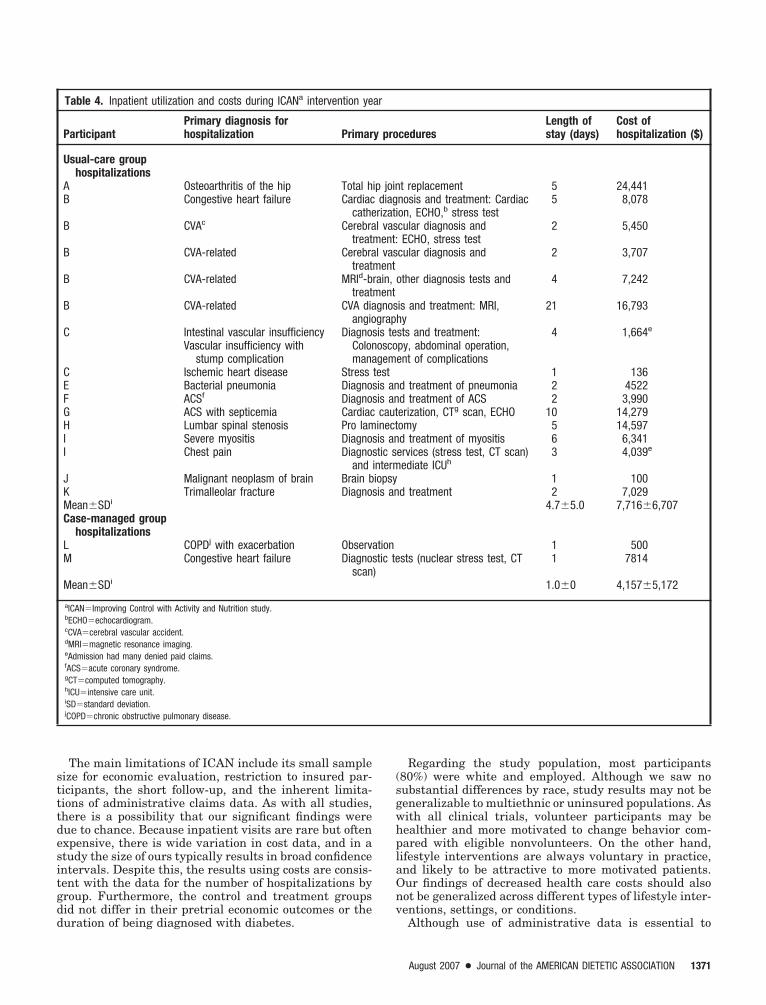
stttdesitgdd
(sgwhplaOnv
The main limitations of ICAN include its small sampleize for economic evaluation, restriction to insured par-icipants, the short follow-up, and the inherent limita-ions of administrative claims data. As with all studies,here is a possibility that our significant findings wereue to chance. Because inpatient visits are rare but oftenxpensive, there is wide variation in cost data, and in atudy the size of ours typically results in broad confidencentervals. Despite this, the results using costs are consis-ent with the data for the number of hospitalizations byroup. Furthermore, the control and treatment groupsid not differ in their pretrial economic outcomes or the
Table 4. Inpatient utilization and costs during ICANa intervention ye
ParticipantPrimary diagnosis forhospitalization Primar
Usual-care grouphospitalizations
A Osteoarthritis of the hip Total hB Congestive heart failure Cardiac
catheB CVAc Cerebra
treatB CVA-related Cerebra
treatB CVA-related MRId-b
treatB CVA-related CVA dia
angioC Intestinal vascular insufficiency
Vascular insufficiency withstump complication
DiagnosColonmana
C Ischemic heart disease StressE Bacterial pneumonia DiagnosF ACSf DiagnosG ACS with septicemia CardiacH Lumbar spinal stenosis Pro lamI Severe myositis DiagnosI Chest pain Diagnos
andJ Malignant neoplasm of brain Brain bK Trimalleolar fracture DiagnosMean�SDi
Case-managed grouphospitalizations
L COPDj with exacerbation ObservaM Congestive heart failure Diagnos
scanMean�SDi
aICAN�Improving Control with Activity and Nutrition study.bECHO�echocardiogram.cCVA�cerebral vascular accident.dMRI�magnetic resonance imaging.eAdmission had many denied paid claims.fACS�acute coronary syndrome.gCT�computed tomography.hICU�intensive care unit.iSD�standard deviation.jCOPD�chronic obstructive pulmonary disease.
uration of being diagnosed with diabetes.
Regarding the study population, most participants80%) were white and employed. Although we saw noubstantial differences by race, study results may not beeneralizable to multiethnic or uninsured populations. Asith all clinical trials, volunteer participants may beealthier and more motivated to change behavior com-ared with eligible nonvolunteers. On the other hand,ifestyle interventions are always voluntary in practice,nd likely to be attractive to more motivated patients.ur findings of decreased health care costs should alsoot be generalized across different types of lifestyle inter-entions, settings, or conditions.
ceduresLength ofstay (days)
Cost ofhospitalization ($)
t replacement 5 24,441nosis and treatment: Cardiacon, ECHO,b stress test
5 8,078
cular diagnosis andECHO, stress test
2 5,450
cular diagnosis and 2 3,707
other diagnosis tests and 4 7,242
is and treatment: MRI,y
21 16,793
sts and treatment:py, abdominal operation,ent of complications
4 1,664e
1 136d treatment of pneumonia 2 4522d treatment of ACS 2 3,990erization, CTg scan, ECHO 10 14,279omy 5 14,597d treatment of myositis 6 6,341ervices (stress test, CT scan)ediate ICUh
3 4,039e
1 100d treatment 2 7,029
4.7�5.0 7,716�6,707
1 500sts (nuclear stress test, CT 1 7814
1.0�0 4,157�5,172
ar
y pro
ip joindiagrizatil vas
ment:l vas
mentrain,mentgnosgraphis teoscogem
testis anis ancautinectis antic s
intermiopsyis an
tiontic te
)
Although use of administrative data is essential to
August 2007 ● Journal of the AMERICAN DIETETIC ASSOCIATION 1371

ciiupcrtbfidcatacttpddiaSSccg
CI4tnlptc(Gspttfca
TDDgs
Rad
ars
R
1
1
1
1
1
1
1
1
1
1
2
2
2
1
apture costs from a payer’s perspective, there can bemprecision and change. A major administrative changen Southern Health Services is one example of this andnderlies the importance of including longitudinal com-arison groups (eg, in RCT or cohorts) when working withommercial health plans. Throughout the trial, the ICANesearch team collaborated with health plan counterpartso minimize the imprecision and bridge the data gapetween clinical research, clinical care, and business. Thending that inpatient costs among usual care were un-erreported due to our definition of cost being limited toosts reimbursed by the primary insurer is one such ex-mple. In addition, the increase in health care costs fromhe year previous to the year of the trial is another ex-mple. Brown and colleagues report that health careosts for people with diabetes varies little over time, buthat costs, especially inpatient costs begin to increase inhe seventh and eight year after diagnosis (53). The ICANarticipants were a mean of 7.3 years from the time ofiagnosis. The annual increase in health care cost asiabetes progresses, however, cannot explain the largencrease we observed. A further explanation may be theccounting practice differences between Southern Healthervices and Qual Choice, the health system acquired byouthern Health Services; hence, we report relativehanges over time. The strength of the RCT design wasritical to distribute inaccuracies randomly, resulting inroups with data of comparable accuracy.
ONCLUSIONSn 1999-2000, only 52% of third-party payers (54) and5% of Fortune 100 firms (55) covered outpatient nutri-ion services. Health plans, insurers, and employers mayeed business cases to support the decision to provide
ifestyle behavior modification by an RD. The ICANroject provides preliminary evidence that moderate-in-ensity lifestyle intervention using an RD as a lifestylease management reduces risk, improves quality of life27), and does so without increasing health care costs.iven the growing prevalence of both diabetes and obe-
ity and the substantial burden of health care costs toatients, employers, and society, effective interventionshat are at least cost-neutral should be welcome additionso comprehensive medical care. Food and nutrition pro-essionals can use these results to judiciously support theost neutrality and effectiveness (27) of their services asn integral component of medical care.
his protocol was funded by grants from the Americanietetic Association, National Institute of Diabetes andigestive and Kidney Diseases (R18 DK062942) and arant to the University of Virginia General Clinical Re-earch Center, MO1 RR00847.The authors thank Kristen Yonkers-Hazen, the ICAND case manager, for her commitment and dedication,nd to ICAN study participants for their dedication toiabetes and obesity treatment.Any opinions, results, or conclusions set forth in this
rticle are those of the authors and do not necessarilyeflect the policies or opinions of Southern Health or any
ubsidiaries or affiliate companies.372 August 2007 Volume 107 Number 8
eferences1. American Diabetes Association. Economic costs of diabetes in the U.S.
in 2002. Diabetes Care. 2003:26:917-932.2. Finkelstein EA, Fiebelkorn IC, Wang G. National medical spending
attributable to overweight and obesity: How much and who’s paying?Health Affairs. 2003;W3:219-226.
3. Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS,Marks JS. Prevalence of obesity, diabetes, and obesity-related healthrisk factors. JAMA. 2003;289:76-79.
4. Thorpe KE, Florence CS, Howard DH, Joski P. The impact of obesityon rising medical spending. Health Affairs. 2004;W4:480-486.
5. McAuley KA, Williams SM, Mann JI, Goulding A, Chisholm A, WilsonN, Story G, McLay RT, Hargper MJ, Jones IE. Intensive lifestylechanges are necessary to improve insulin sensitivity. Diabetes Care.2002;25:445-452.
6. Kelley DE, Bray GA, Pi-Sunyer FX, Klein S, Hill J, Miles J, HollanderP. Clinical efficacy of Orlistat therapy in overweight and obese pa-tients with insulin-treated type 2 diabetes: A 1-year randomized con-trolled trial. Diabetes Care. 2002;25:1033-1041.
7. Fujioka K, Seaton TB, Rowe E, for the Sibutramine/Diabetes ClinicalStudy Group. Weight loss with sibutramine improves glycaemic con-trol and other metabolic parameters in obese patients with type 2diabetes mellitus. Diabetes Obes Metab. 2000;2:175-187.
8. Hollander PA, Elbein SC, Hirsch IB, Kelley D, McGill J, Taylor T,Weiss SR, Crockett SE, Kaplan RA, Comstock J, Lucas CP, LodewickPA, Canovatchel W, Chung J, Hauptman J. Role of Orlistat in thetreatment of obese patients with type 2 diabetes: A 1-year randomizeddouble blind study. Diabetes Care. 1998;21:1288-1294.
9. Miles JM, Leiter L, Hollander P, Wadden T, Anderson JW, Doyle M,Foreyt J, Aronne L, Klein S. Effect of Orlistat in overweight and obesepatients with type 2 diabetes treated with metformin. Diabetes Care.2002;25:1123-1128.
0. Eriksson KF, Lindgarde F. Prevention of type 2 (non-insulin-depen-dent) diabetes mellitus by diet and physical exercise. The 6-yearMalmo feasibility study. Diabetologia. 1991;34:891-898.
1. Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, SacksFM, Bray GA, Vogt TM, Cutler JA, Windhauser MM, Lin PH, KaranjaN. A clinical trial of the effects of dietary patterns on blood pressure.N Engl J Med. 1997;336:1117-1124.
2. Krotkiewski M, Mandroukas K, Sjostrom L, Sullivan L, Wetterqvist H,Bjorntorp P. Effects of long-term physical training on body fat, metabo-lism, and blood pressure in obesity. Metabolism. 1979;28:650-658.
3. Blankenhorn DH, Johnson RL, Mack WJ, El Zein HA, Vailas LI. Theinfluence of diet on the appearance of new lesions inhuman coronaryarteries. JAMA. 1990;263:1646-1652.
4. Arntzenius AC, Kromhout JD, Reiber JH, Bruschke AV, Buis B, vanGent CM, Kempen-Voogd N, Strikwerda S, van der Velde EA. Diet,lipoproteins, and the progression of coronary artherosclerosis: Theleiden intervention trial. N Engl J Med. 1985;312:805-811.
5. de Lorgeril MS, Renaud S, Mamelle N, Salen P, Martin JL, MonjaudI, Guidollet J, Touboul P, Delaye J. Mediterranean alpha-linolenicacid-rich diet in secondary prevention of coronary heart disease. Lan-cet. 1994;343:1454-1459.
6. Lehmann R, Vokac A, Niedermann K, Agosti K, Spinas GA. Loss ofabdominal fat and improvement of the cardiovascular risk profile byregular moderate exercise training in patients with NIDdiabetes.Diabetologia. 1995;38:1313-1319.
7. Ehnholm C, Huttunen JK, Pietinen P, Leino U, Mutanen M, Kosti-ainen E, Pikkarainen J, Dougherty R, Iacono J, Puska P. Effect of dieton serum lipoproteins in a population with a high risk of coronaryheart disease. N Engl J Med. 1982;307:850-855.
8. Barnard RJ. Effects of life-style modification on serum lipids. ArchIntern Med. 1991;151:1389-1394.
9. Diabetes Prevention Program Research Group. Reduction in the in-cidence of type 2 diabetes with lifestyle intervention or metformin.N Engl J Med. 2002;346:393-403.
0. Tuomilehto J, Lindström J, Eriksson JG, for the Finnish DiabetesPrevention Study Group. Prevention of type 2 diabetes mellitus bychanges in lifestyle among subjects with impaired glucose tolerance.N Engl J Med. 2001;344:1343-1350.
1. Pan XR, Li GW, Hu YH, for the Da Qing IGT and Diabetes StudyGroup. Effects of diet and exercise in preventing NIDdiabetes inpeople with impaired glucose tolerance: the Da Qing IGT and Diabe-tes Study. Diabetes Care. 1997;20:537-544.
2. The Diabetes Prevention Program Research Group. Within-trial cost-
effectiveness of lifestyle intervention or metformin for the primaryprevention of type 2 diabetes. Diabetes Care. 2003;26:2518-2523.
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
3. Herman WH, Hoerger TJ, Brandle M, for the Diabetes PreventionProgram Research Group. Ann Intern Med. 2005;142:323-332.
4. The Diabetes Prevention Program Research Group. Costs associatedwith the primary prevention of type 2 diabetes mellitus in the Dia-betes Prevention Program. Diabetes Care. 2003;26:36-47.
5. Glasgow RE. Translating research to practice: Lessons learned, areasfor improvement, and future directions. Diabetes Care. 2003;26:2451-2456.
6. Glasgow RE, Lichtenstein E, Marcus AC. Whey don’t we see moretranslation of health promotion research to practice? Rethinking theefficacy to effectiveness transition. Am J Public Health. 2003;93:1261-1267.
7. Wolf AM, Conaway MR, Crowther JQ, Hazen KY, Nadler JL, OneidaB, Bovbjerg VE. Translating lifestyle intervention to practice in obesepatients with type 2 diabetes: Improving control with activity andnutrition (ICAN). Diabetes Care. 2004;27:1570-1576.
8. American Dietetic Association. Position of the American Dietetic As-sociation: Weight management. J Am Diet Assoc. 2002;102:1145-1155.
9. Tinkler LF, Heins JM, Holler HJ. Commentary and Translation: 1994nutrition recommendations for diabetes. Diabetes Care and Educa-tion: A practice group of the American Dietetic Association. J Am DietAssoc. 1994;94:507-511.
0. Brownell K. The LEARN Program for Weight Management. Dallas,TX: American Health Publishing Company; 2000.
1. SPSS Inc. SPSS Base 11.0 for Windows User’s Guide. Chicago, IL:SPSS Inc; 2001.
2. R Development Core Team. R. A language and environment for sta-tistical computing. Vienna, Austria: R Foundation for StatisticalComputing; 2004. Available at: http://www.R-project.org. AccessedMay 4, 2004.
3. Duan N, Newhouse JP, Morris CN, Manning WG. A comparison ofalternative models for the demand for medical care. J Bus Econ Stats.1983;1:115-126.
4. Manning W, Newhouse J, Duan N, Keeler E, Leibowitz A. Healthinsurance and the demand for medical care: Evidence from a random-ized experiment. Am Econ Rev. 1987;77:251-277.
5. Efron B, Tibshirani RT. An Introduction to the Bootstrap. Boca Raton,FL: Chapman & Hall/CRC; 1994.
6. The Clinical Guidelines on the Identification, Evaluation, and Treat-ment of Overweight and Obesity in Adults. The Evidence Report.National Heart, Lung, and Blood Institute in cooperation with TheNational Institutes of Diabetes and Digestive and Kidney Diseases.NIH publication no. 98-4083 September 1998 NIH.
7. Sevick MA, Dunn AL, Morrow MS, Marcus BH, Chen GJ, Blair SN.Cost effectiveness of lifestyle and structured exercise intervention insedentary adults: Results of project ACTIVE. Am J Prev Med. 2000;19:1-8.
8. California HealthCare Foundation. 2005 Health care costs 101. Avail-able at: http://www.chcf.org. Accessed August 1, 2005.
9. Goetzel RZ, Dunn RL, Ozminkowski RJ, Satin K, Whitehead D, CahillK. Differences between descriptive and multivariate estimates of the
impact of Chevron Corporation’s Health Quest Program on medicalexpenditures. J Occup Environ Med. 1998;40:538-545.
0. The role of nutrition in maintaining health in the nation’s elderly.Evaluating coverage of nutrition services for the Medicare population.Washington, DC: National Academies Press; 2000.
1. Pavlovich WD, Waters H, Weller W, Bass EB. Systematic review ofliterature on the cost-effectiveness of nutrition services. J Am DietAssoc. 2004;104:226-232.
2. Glasgow RE, La Chance PA, Toobert DJ, Brown J, Hampson SE,Riddle MC. Long-term effects and costs of a brief behavioral dietaryintervention for patients with diabetes delivered from the medicaloffice. Patient Educ Couns. 1997;32:175-184.
3. Pritchard DA, Hyndman J, Taba F. Nutritional counseling in generalpractice: A cost effective analysis. J Epidemiol Community Health.1999;53:311-316.
4. Brownell KD, Stunkard, AJ, McKeon PE. Weight reduction at thework site: A promise partially fulfilled. Am J Psychiatry. 1985;142:47-52.
5. Myers AW, Graves TJ, Whelan JP, Barclay DR. An evaluation of atelevision-delivered behavioral weight loss program: Are the ratingsacceptable? J Consult Clin Psychol. 1996;64:172-178.
6. Franz MJ, Splett PL, Monk A, Barry B, McClain K, Weaver T, Upham P,Bergenstal R, Mazze RS. Cost-effectiveness of medical nutrition therapyprovided by dietitians for person with non-insulin-dependent diabetesmellitus. J Am Diet Assoc. 1995;95:1018-1024.
7. Nichols G, Brown J, Stevens V, Crawford J. Medical care costs reduc-tions resulting from intentional weight loss. Obes Res. 2004;125:67-OR.
8. Isomaa B, Almgren P, Tuomi T, Forsen B, Lahti K, Nissen M, Taski-nen MR, Group L. Cardiovascular morbidity and mortality associatedwith metabolic syndrome. Diabetes Care. 2001;24:683-689.
9. National Institutes of Health. Third report of the National Choles-terol Education Program Expert Panel on Detection, Evaluation, andTreatment of High Blood Cholesterol in Adults (Adult TreatmentPanel III). Bethesda, MD: National Institutes of Health; 2001. NIHPublication 01-3670.
0. Eisenstein EL, Shaw LK, Nelson CL, Anstrom KJ, Hakim Z, MarkDB. Obesity and long-term clinical and economic outcomes in coro-nary artery disease patients. Obes Res. 2002;10:83-91.
1. Wee CC, Phillips RS, Legedza ATR, Davis RB; Soukup JR, ColditzGA, Hamel MB. Health care expenditures associated with overweightand obesity among US adults: Importance of age and race. Am JPublic Health. 2005;95:159-165.
2. Raebel MA, Malone DC, Conner DA, Xu S, Potter JA, Lanty FA.Health services use and health care costs of obese and nonobeseindividuals. Arch Intern Med. 2004;164:2135-2140.
3. Brown JB, Nichols GA, Glauber HS, Bakst AW. Type 2 Diabetes:Incremental Medical Care Costs during the First 8 Years After Diag-nosis. Diabetes Care. 1999;22:1116-1124.
4. Barnaoski CLN, King SL. Insurance companies are reimbursing formedical nutrition therapy. J Am Diet Assoc. 2000;100:1530-1532.
5. Montenegro-Torres G, Engelhardt T, Thamer M, Anerson G. Are
Fortune 100 companies responsive to chronically ill workers? HealthAffairs. 2001;20:209-219.August 2007 ● Journal of the AMERICAN DIETETIC ASSOCIATION 1373