Embed Size (px)
Citation preview

Ann Hematol (2003) 82:61–63DOI 10.1007/s00277-002-0580-2
C A S E R E P O R T
K. Kojima · N. Fujii · E. Omoto · S. Nose ·M. Yoneyama · Y. Sugii · H. Hiramatsu ·M. Chikatsune · M. Sato · S. Takata · T. Itoshima ·M. Tanimoto
Cyclic thrombocytopenia and polycythemia vera
Received: 26 July 2002 / Accepted: 16 October 2002 / Published online: 6 December 2002� Springer-Verlag 2002
Abstract A periodic fall of platelet number characterizesan acquired pathological condition named cyclic throm-bocytopenia. We describe an unusual case of polycythe-mia vera in which the episodes of thrombocytopenia werefollowed regularly by thrombocytosis. The period ofplatelet count fluctuation was about 50 days, with thecounts ranging from 34 to 820�109/l. Bone marrowmegakaryocytes were decreased in number during plateletnadir. Circulating thrombopoietin levels fluctuated out ofphase with the platelet count. We suggest that at leastsome cases of polycythemia vera may have an unstablehematopoietic stem cell pool in nature, which couldcontribute to the development of unprovoked cyclicthrombocytopenia.
Keywords Cyclic thrombocytopenia · Polycythemiavera · Chronic myeloproliferative disorder ·Thrombopoietin
Introduction
Polycythemia vera (PV) is characterized by an increasedand uncontrolled proliferation of all the hematopoieticprogenitors and it involves the transformation of a singlepluripotential stem cell [1]. Cyclic thrombocytopenia is arare syndrome characterized by periodic oscillations in
the peripheral blood platelet count, which is associatedwith either intermittent immune-mediated platelet de-struction [2] or cyclic failure of platelet production [3, 4].Recently, Tefferi et al. [5] have reported two PV patientswhose platelet counts showed periodic fluctuation duringtreatment with hydroxyurea. Here we report the first caseof unprovoked cyclic thrombocytopenia in a patient withPV.
Case report
An 84-year-old Japanese man was referred to usbecause of erythrocytosis on 29 August 2000. On physicalexamination, the spleen was enlarged 1 cm below thecostal margin. His red cell count was 778�109/l, hemo-globin concentration 18.3, hematocrit level 57%, whiteblood cell count 361�109/l with 87% mature neutrophils,and platelet count 634.0�109/l. A determination of the redcell mass revealed an absolute erythrocytosis (40 ml/kg).A bone marrow (BM) biopsy specimen showed trilineagehyperplasia and clustering pleomorphic megakaryocyteswith giant forms. The reticulin was normal and iron storeswere absent. BM cytogenetic studies were normal, andreverse transcriptase polymerase chain reaction amplifi-cation did not yield BCR/ABL fusion transcripts. Adiagnosis of PV was made, and he was observed withoutmedication or phlebotomies.After 3 weeks, transient thrombocytopenia (84�109/l)developed, which was followed by spontaneous recoveryto 577�109/l after the next 3 weeks. The episodes ofthrombocytopenia were thereafter followed regularly bythrombocytosis, with platelet counts ranging from 34 to820�109/l. Serial tests for serum antiplatelet antibodieswere negative and platelet-associated immunoglobulinlevels were normal throughout the platelet cycle. Theperiod of platelet count fluctuation was about 50 days.White cell counts fluctuated in synchrony with theplatelet count, but red cell count and reticulocyte numberdid not show clear fluctuation. The periodic oscillations
K. Kojima ()) · N. Fujii · M. TanimotoDepartment of Medicine II, Okayama University Medical School,2–5-1 Shikata-cho, Okayama 700–8558, Japane-mail: [email protected].: +81-89-9605296Fax: +81-89-9605299
E. Omoto · S. Nose · M. Yoneyama · Y. Sugii · H. Hiramatsu ·M. Chikatsune · M. Sato · S. Takata · T. ItoshimaDepartment of Internal Medicine,Okayama Saiseikai General Hospital, Japan
Current address:K. Kojima, First Department of Internal Medicine,Ehime University School of Medicine, Shigenobu,Ehime 791–0295, Japan

of the platelet count still continued for more than20 months.
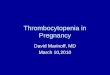
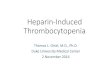
BM biopsy specimens were obtained while the plateletcount was decreasing towards its nadir and while it wasincreasing towards its zenith, respectively. BM megakar-yocytes were markedly increased when platelet countswere increasing (Fig. 1 A) while they were decreased innumber during platelet nadir (Fig. 1B). Serum levels ofthrombopoietin (TPO) were serially measured 17 timesduring one complete platelet cycle [6]. The limit ofdetection of the assay is 0.2 fmol/ml, and it is sensitiveenough to detect circulating TPO in normal subjects(1.08€0.81 fmol/ml, n=42). As shown in Fig. 2, TPOlevels rose rapidly when the platelet count decreasedbelow 14.6�109/l to peak at 5.59 fmol/ml during theplatelet count nadir. TPO levels rapidly decreased con-comitant with the increase in platelet count.
Discussion
In the present case, cyclic thrombocytopenia was closelyassociated with cyclic failure of platelet production andthe variation in serum TPO level appeared to represent anautoregulatory response. Since there were synchronousoscillations in two blood elements (white cells andplatelets), the oscillations might be a consequence ofregulatory mechanisms affecting multilineage hematopoi-esis.
Recently, Tefferi et al. [5] reported two patients withPV whose platelet counts showed marked periodicfluctuation during treatment with hydroxyurea, and theysuggested that the cyclic phenomenon may be related toboth a transient state of hydroxyurea-induced depletion ofmegakaryocytes and a concentration-dependent mitiga-tion by TPO of the hydroxyurea effect on megakaryocytesand their precursors. The present case is clinically ofinterest from the point of view that the patient had notreceived any myelosuppressive agents. This suggests thatthe induction of oscillatory changes does not alwaysrequire an extrinsic myelosuppression. Interestingly, amild degree of unprovoked periodic oscillations in theplatelet counts have been reported in a minority ofpatients with PV [7]. We think that at least some cases ofPV have an unstable hematopoietic stem cell pool innature and that this instability might contribute to thedevelopment of cyclic thrombocytopenia in our patient.
Fig. 1A, B Bone marrow. A Photomicrograph of a bone marrowbiopsy done while the platelet count was increasing (platelet count514�109/l). There were increased numbers of pleomorphic mega-karyocytes with giant forms (original magnification �100). BPhotomicrograph of a bone marrow biopsy done while the plateletcount was decreasing towards its nadir (platelet count 74�109/l).There were decreased numbers of megakaryocytes (originalmagnification �100)
Fig. 2 White cells, platelet counts, and serum thrombopoietinlevel. There were synchronous oscillations in white cells andplatelets. The thrombopoietin level increased about eightfold overbaseline levels as the platelet count decreased and then decreasedrapidly as the platelet count started to rise
62

References
1. Spivak JL (2002) The optimal management of polycythaemiavera. Br J Haematol 116:243–254
2. Kosugi S, Tomiyama Y, Shiraga M, Kashiwagi H, Nakao H,Kanayama Y, Kurata Y, Matsuzawa Y (1994) Cyclic throm-bocytopenia associated with IgM anti-GPIIb-IIIa autoantibod-ies. Br J Haematol 88:809–815
3. Balduini CL, Stella CC, Rosti V, Bertolino G, Noris P, Ascari E(1993) Acquired cyclic thrombocytopenia-thrombocytosis withperiodic defect of platelet function. Br J Haematol 85:718–722
4. Zent CS, Ratajczak J, Ratajczak MZ, Anastasi J, Hoffman PC,Gewirtz AM (1999) Relationship between megakaryocyte massand serum thrombopoietin levels as revealed by a case of cyclic
amegakaryocytic thrombocytopenic purpura. Br J Haematol105:452–458
5. Tefferi A, Elliott MA, Kao PC, Yoon S, El-Hemaidi I,Pearson TC (2000) Hydroxyurea-induced marked oscillationsof platelet counts in patients with polycythemia vera. Blood96:1582–1584
6. Tahara T, Usuki K, Sato H, Ohashi H, Morita H, Tsumura H,Matsumoto A, Miyazaki H, Urabe A, Kato T (1996) A sensitivesandwich ELISA for measuring thrombopoietin in humanserum: serum thrombopoietin levels in healthy volunteers andin patients with haemopoietic disorders. Br J Haematol 93:783–788
7. Morley A (1969) Blood-cell cycles in polycythaemia vera.Australas Ann Med 18:124–126
63