Embed Size (px)
Citation preview
….. foundation of clinical medicine
Shashidhar Venkatesh MurthyA/Prof & Head of Pathology
College of Medicine & Dentistry
Clinical Pathology:
RBC 1.3: Anemia Summary
CPC : Term2 Week1 - Haem 1/2.
System : Haematology - RBC Disorders.
Topic : 1: Anemia Intro 2: IDA, MBA & ACD 3: Acquired HA 4: Congenital HA. 5: Others.
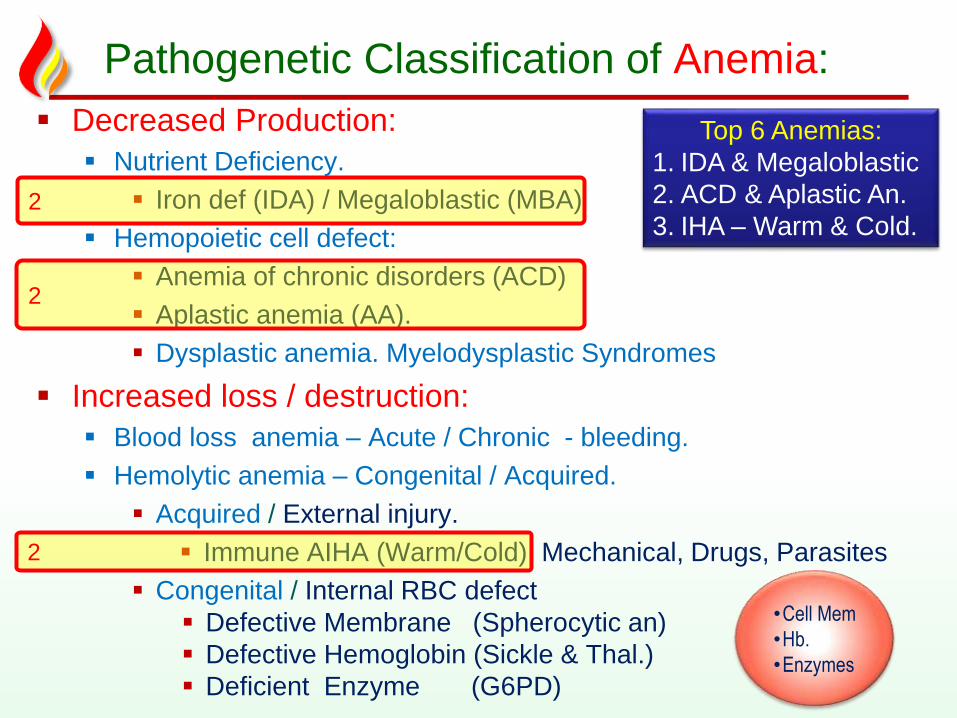
Pathogenetic Classification of Anemia:
Decreased Production:
Nutrient Deficiency.
Iron def (IDA) / Megaloblastic (MBA)
Hemopoietic cell defect:
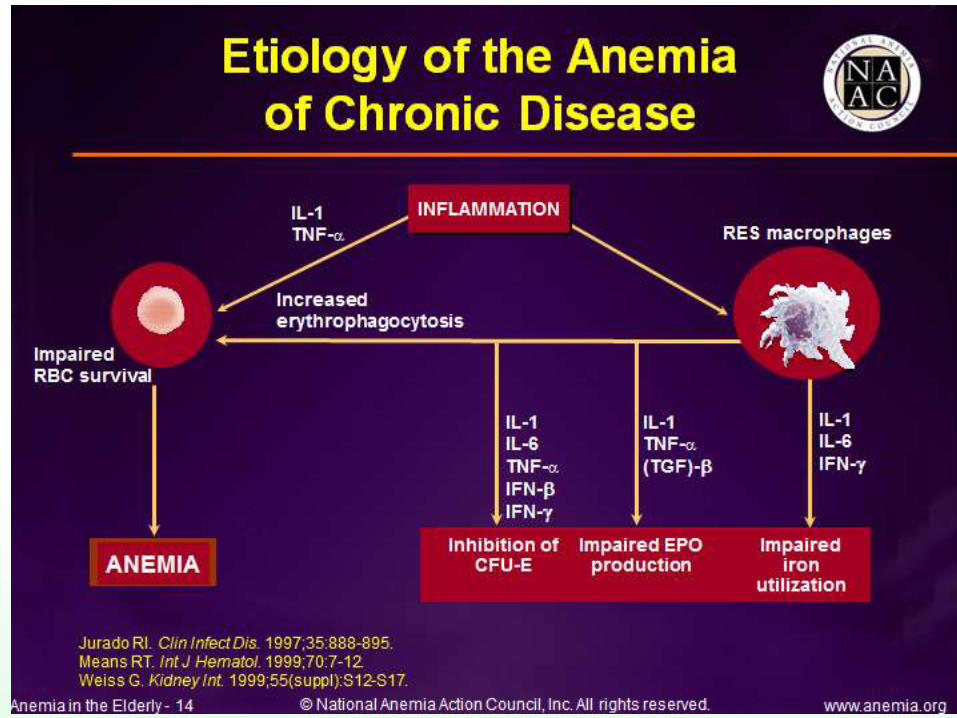
Anemia of chronic disorders (ACD)
Aplastic anemia (AA).
Dysplastic anemia. Myelodysplastic Syndromes
Increased loss / destruction:
Blood loss anemia – Acute / Chronic - bleeding.
Hemolytic anemia – Congenital / Acquired.
Acquired / External injury.
Immune AIHA (Warm/Cold) Mechanical, Drugs, Parasites
Congenital / Internal RBC defect
Defective Membrane (Spherocytic an)
Defective Hemoglobin (Sickle & Thal.)
Deficient Enzyme (G6PD)
2
•Cell Mem
•Hb.
•Enzymes
Top 6 Anemias:
1. IDA & Megaloblastic
2. ACD & Aplastic An.
3. IHA – Warm & Cold.
2
2
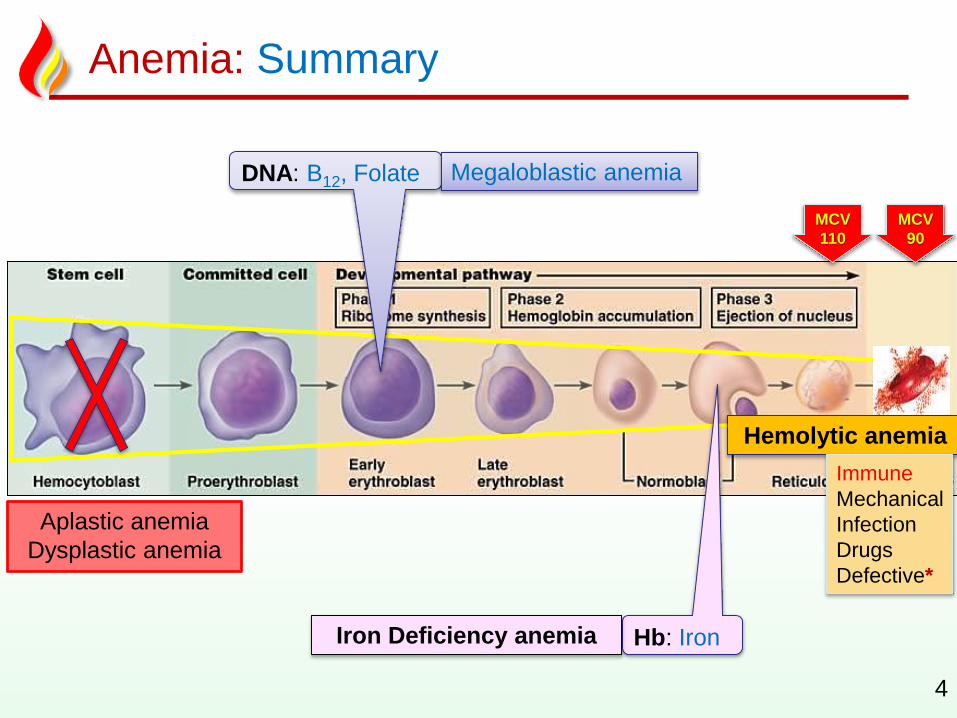
Anemia: Summary
4
MCV
90
MCV
110
DNA: B12, Folate
Hb: Iron
Megaloblastic anemia
Iron Deficiency anemia
Aplastic anemia
Dysplastic anemia
Hemolytic anemia
Immune
Mechanical
Infection
Drugs
Defective*
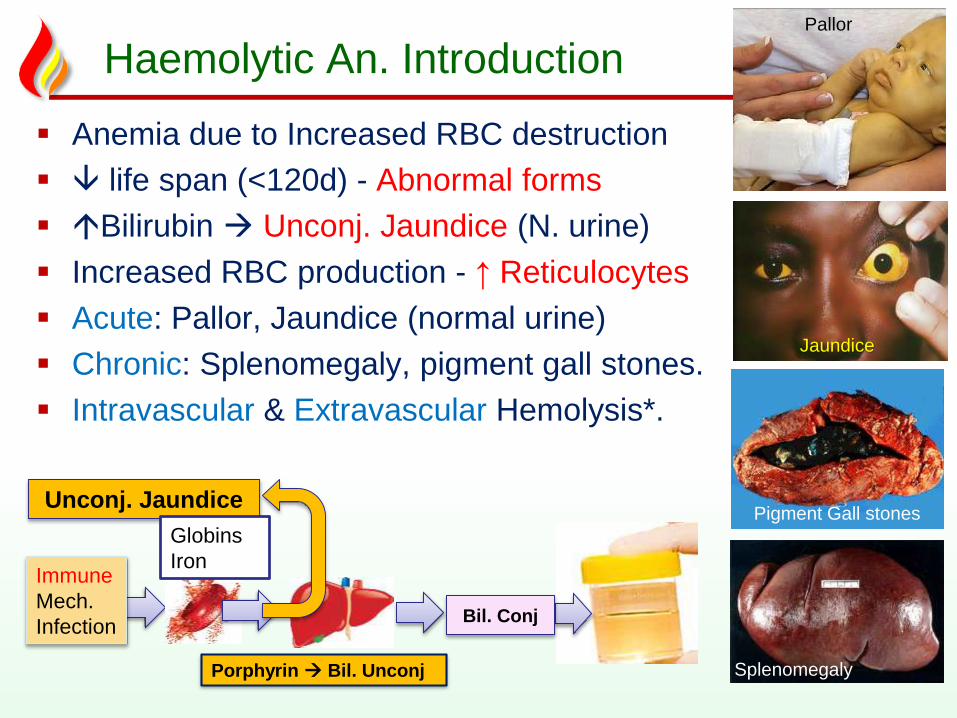
Haemolytic An. Introduction
Anemia due to Increased RBC destruction
life span (<120d) - Abnormal forms
Bilirubin Unconj. Jaundice (N. urine)
Increased RBC production - ↑ Reticulocytes
Acute: Pallor, Jaundice (normal urine)
Chronic: Splenomegaly, pigment gall stones.
Intravascular & Extravascular Hemolysis*.
Unconj. Jaundice
Immune
Mech.
Infection
Porphyrin Bil. Unconj
Globins
Iron
Bil. Conj
Jaundice
Splenomegaly
Pigment Gall stones
Pallor
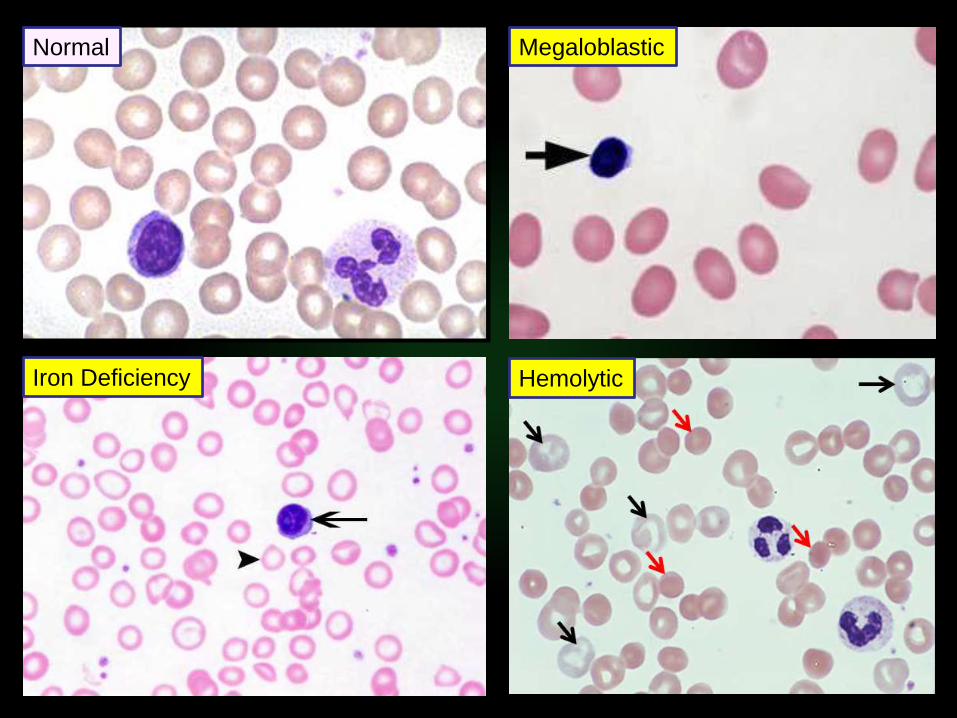
Iron Deficiency
Megaloblastic
Hemolytic
Normal
MCV
Microcytic Normocytic Macrocytic
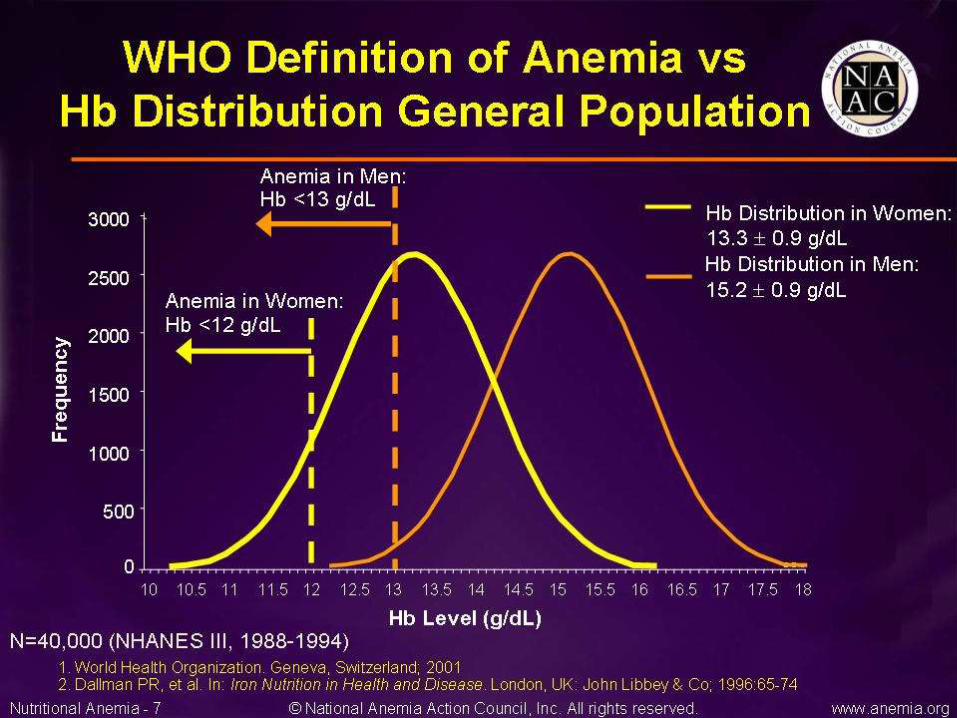
Iron studies - Ferritin
Low Normal/high
IDA ACD / Thalassemia
Reticulocyte count
high low ACD /
Aplastic anemiaHemolytic anemia or
blood loss
Measure B12 + folate
Megaloblastic
Normal Low
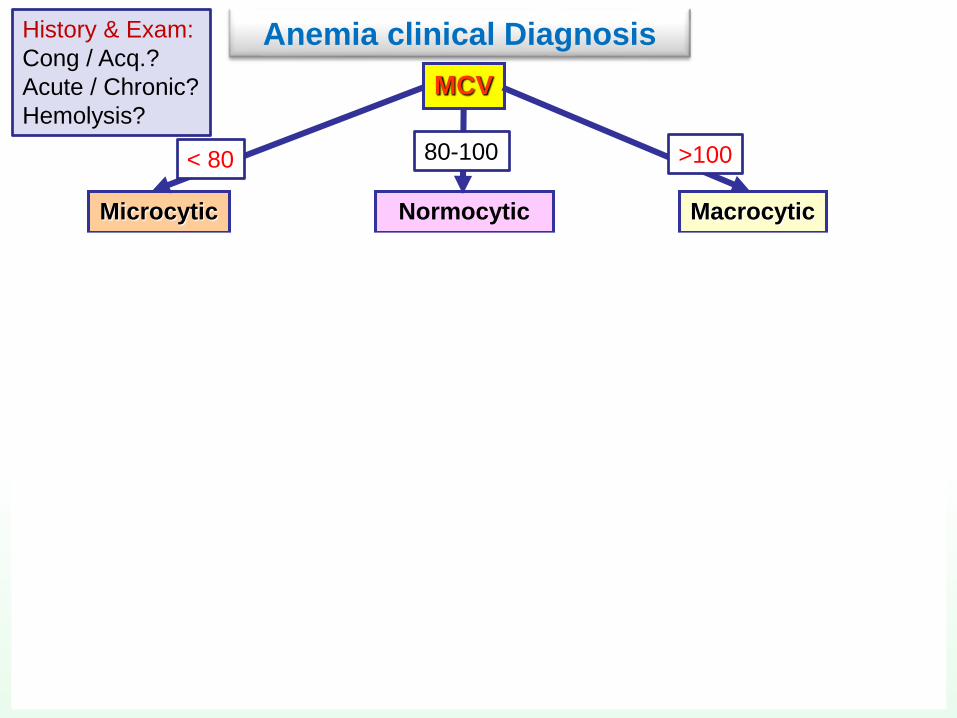
Anemia clinical DiagnosisHistory & Exam:
Cong / Acq.?
Acute / Chronic?
Hemolysis?
< 80 80-100 >100

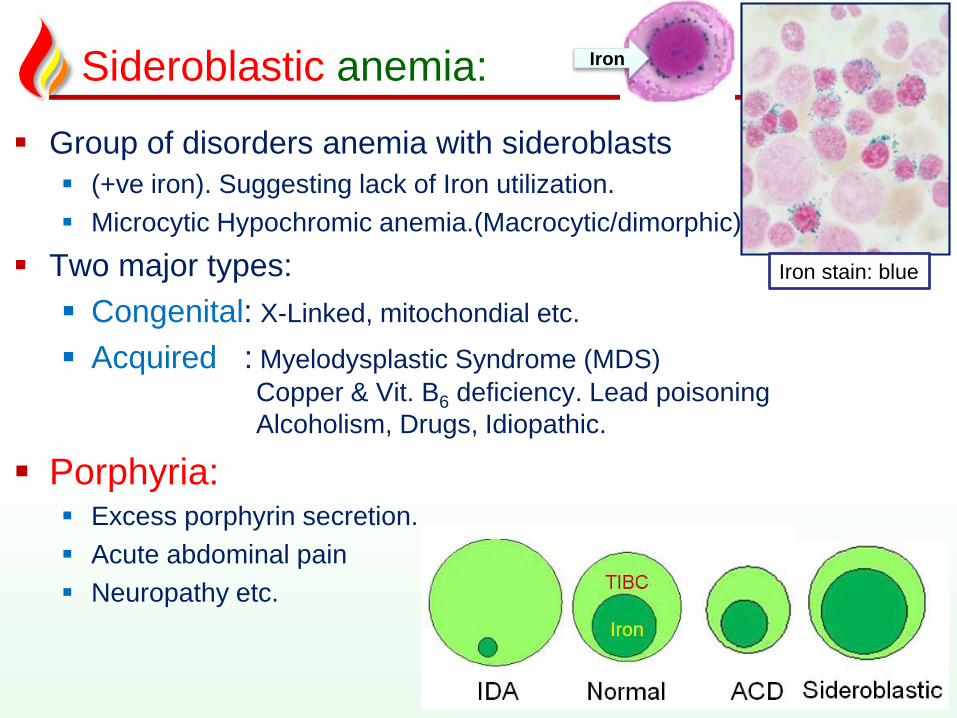
Sideroblastic anemia:
Group of disorders anemia with sideroblasts
(+ve iron). Suggesting lack of Iron utilization.
Microcytic Hypochromic anemia.(Macrocytic/dimorphic)
Two major types:
Congenital: X-Linked, mitochondial etc.
Acquired : Myelodysplastic Syndrome (MDS)
Copper & Vit. B6 deficiency. Lead poisoning
Alcoholism, Drugs, Idiopathic.
Porphyria: Excess porphyrin secretion.
Acute abdominal pain
Neuropathy etc.
Iron
Iron stain: blue
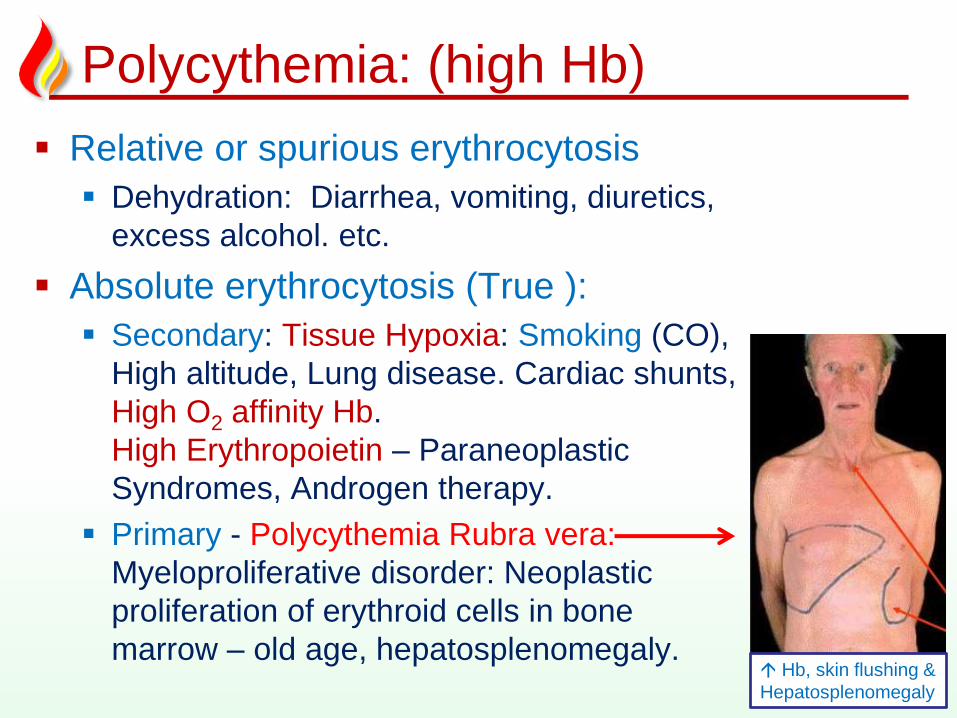
Polycythemia: (high Hb)
Relative or spurious erythrocytosis
Dehydration: Diarrhea, vomiting, diuretics,
excess alcohol. etc.
Absolute erythrocytosis (True ):
Secondary: Tissue Hypoxia: Smoking (CO),
High altitude, Lung disease. Cardiac shunts,
High O2 affinity Hb.
High Erythropoietin – Paraneoplastic
Syndromes, Androgen therapy.
Primary - Polycythemia Rubra vera:
Myeloproliferative disorder: Neoplastic
proliferation of erythroid cells in bone
marrow – old age, hepatosplenomegaly.
10 Hb, skin flushing &
Hepatosplenomegaly
Need help? contact me…
1. Office location: DB39-136 (Townsville)
2. Office Tel: 4781 4566
3. Email: [email protected]
4. Emergency?: 0416933704
Need personal coaching?Email me for an appointment.
You are the stone..
Be true to your work,
your word, & your friend.-- Henry David Thoreau
Integrity is doing the right thing when no one is watching….!
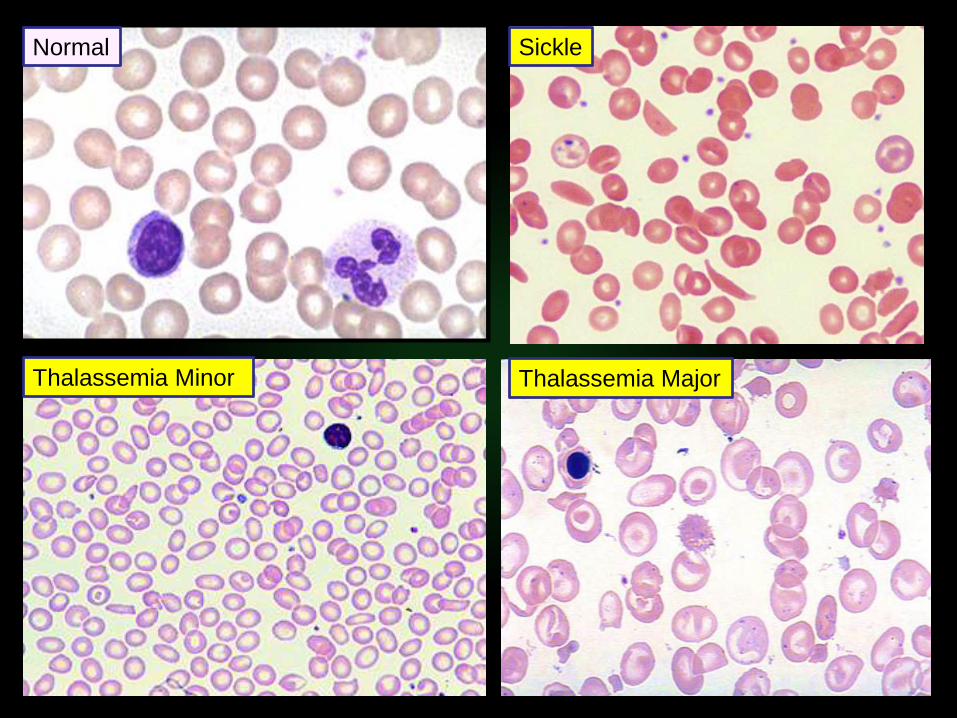
Thalassemia Minor
Sickle
Thalassemia Major
Normal