Embed Size (px)
Citation preview

DATE TOPIC PARTICIPENT
1-Feb-09 intersting cases all residents
8-Feb-09 case review maram
15-Feb-09 interesting cases all residents
22-Feb-09 topic presentation alhawas
1-Mar-09 interisting cases all residentis
8-Mar-09 ACR case review sultan
15-Mar-09 interesting cases all residents
22-Mar-09 OSCE alosaimi
29-Mar-09 interisting cases all residents

Case review
Maram Mobara

• 18 years old obese male• Presented to the ER with RIF pain • For 2 days• Difficult exam due to obesity, no typical
rebound tendrness• WBS: slightly elevated.

• CT abdomen requested to rule out acute appendicitis
• CT scan was performed utilizing pancreatitis protocol

Findings




• Acute epiploic appendagitis• Omental infarction• Subacute appendicitis

Management
• Exploratory laparoscopy • Unremarkable appendix • Fatty mass adherent to the wall of ascending
colon with enlarged inflamed appendages • Pathological result:


DIFFERENTIAL DIAGNOSIS
Inflammatory mass lesion in patient with acute abdomen

• acute epiploic appendagitis, • acute omental infarction, • acute inflammatory process such as
diverticulitis, • sclerosing mesenteritis, and • primary tumor or metastasis that involves the
mesocolon.

Acute epiploic appendagitis

Normal Epiploic Appendages
• Peritoneal pouches from serosal surface of the colon
• Attached to by vascular stalk• Composed of adipose and vascular tissue• Each one is supplied by 2 arteries and one
vein• 0.5- 5 cm• Seen on CT only if inflamed


Causes of acute epiploic appendagitis
• torsion and inflammation (73%),• hernia incarceration (18%), • intestinal obstruction (8%), and • Intra peritoneal loose body.

Association
• Obesity , ★• hernia, and • unaccustomed exercise

Clinically
• 4th- 5th decay• Men ★• Acute onset pain ★• LLQ (acute diverticulitis)• Most normal body temp and WBC

• self-limited inflammation, • before CT was available, was most commonly
diagnosed at surgery

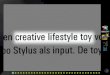
CT FINDINGS
• most common sites, in order of decreasing frequency
• areas adjacent to the sigmoid colon• descending colon, • right hemi colon ★

• oval lesion less than 5 cm in diameter • attenuation equivalent to that of fat• abuts the anterior colonic wall, • surrounded by inflammatory changes



• 2ndary changes: peritoneal inflammation and colonic wall thickening,
• Intestinal obstruction and abscess formation are rare.
• Although the presence of a central area of high attenuation due to venous thrombosis is useful for diagnosis, the absence of this feature does not preclude a diagnosis of acute epiploic appendagitis
• Rarely, appendagitis may occur in a hernia sac .




RIF

No hyper attenuation center


Evolutionary changes

US FINDINGS
• an oval non compressible hyper echoic mass at the site of maximum tenderness, adjacent to the colon,
• with no central blood flow on color Doppler US images


Mimics of acute epiploic appendagitis

Omental infarction
• Rare cause of acute abdomen• RIF pain, ? Appendicitis • >>> pediatrics

• Causes: torsion> venous insufficiency> infarction
• Predisposing factors to insufficiency : • obesity , • CHF and • recent abdominal surgery.

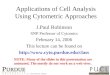
OMENTAL INFARCTION
• CT FINDINGS :• solitary large non enhancing omental mass • heterogeneous attenuation• located in the right lower quadrant, deep to
the rectus abdominis muscle and either anterior to the transverse colon or anteromedial to the ascending colon



Acute omental infarction in young female

Omental infarction
• Vs epiploic appendagitis • Larger than 5cm• Location• +/-Lack of ring enhancement and central
hyperattenuation

Acute diverticulitis

Acute diverticulitis
• Older age group• nausea, vomiting, fever, elevated leukocyte
count, and rebound tenderness

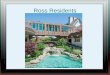
Acute diverticulitis
• CT FEATURES:• colonic diverticula with inflammation or
abscess in the mesocolon • adjacent colonic wall thickening that extends
more than 5 cm • Other un inflamed diverticulae• Fat stranding, extra luminal air or fluid
accumulation, or abscess formation around the colonic lumen

★

With 2ndary epiploic appendagitis

Sclerosing Mesenteritis

Sclerosing Mesenteritis
• Non specific inflammation and fibrosis of the fatty tissue of the mesentery
• typically occurs in the 6th to 7th decades of life.
• The cause in most cases is unknown.• acute abdominal pain, fever, nausea,
vomiting, diarrhea, and weight loss.• In the majority of cases, the disease is self
limited and the prognosis is favorable.

Sclerosing Mesenteritis• CT FEATURES:• well-defined soft- tissue mass containing areas
of fat attenuation to an ill-defined area of higher attenuation
• in the root of the small-bowel mesentery• around mesenteric vessels with- out displacing
them.• The fat plane around the mesenteric vessels
results in a CT feature that is called the “fat ring sign.”

• Fibrosis may lead to bowel loop narrowing and result in spiculation that may be mistaken for a neoplastic process.
• Calcification are uncommon




• Vs epiploic appendagitis• Larger• Root of mesentery, doesn’t abut the
abdominal wall• Not usually cause of acute abdomen• Central hyper attenuation

Primary tumors and metastasis

• fat-containing tumors such as liposarcoma, as well as exophytic angiomyolipoma and dermoid
• omental metastases

Summary
• Acute appendagitis is self limiting condition• Commonly confused cliniclly with appendicitis • CT findings decrease rate of unnecessary
operation and hospital admission.• Obese, male, 4th-5th decay of life with acute
abdomen• No leukocytosis

• CT: 5cm oval fat containing lesion• Abuts bowel loop surface• Central hyperattenuation• Surrounding peritoneal inflammation.

THANK YOU