Embed Size (px)
Citation preview
RESEARCH ARTICLE
Decreasing Exposure to Radiation, Surgical Risk,and Costs for Pediatric Complicated Pneumonia:A Guideline EvaluationRachel D. Quick, RN, MSN, CNS, Michael J. Auth, DO, Marisol Fernandez, MD, Tory Meyer, MD, Kathryn G. Merkel, PharmD, BCPS, AQ ID, Lynn M. Thoreson, DO,
Sarmistha B. Hauger, MD
A B S T R A C T OBJECTIVES: This report describes the creation and successful implementation of a complicatedpneumonia care algorithm at our institution. Outcomes are measured for specific goals of thealgorithm: to decrease radiation exposure, surgical risk, and patient charges without adverselyaffecting clinical outcomes.
METHODS: We describe steps involved in algorithm creation and implementation at ourinstitution. To depict outcomes of the algorithm, we completed a retrospective cohort study ofhospitalized pediatric patients with a diagnosis of complicated pneumonia at a single institutionbetween January 2010 and April 2016 who met criteria for the algorithm. Charts were manuallyreviewed and data were analyzed via Wilcoxon rank sum, x2, and Fisher’s exact tests.
RESULTS: Throughout the algorithm creation process, our institution began to see a change inpractice. We saw a statistically significant decrease in the number of patients who underwent achest computed tomography scan and an increase in patients who underwent a chest ultrasound(P , .001). We also saw an increase in the use of chest tube placement with fibrinolytics and adecrease in the use of video-assisted thoracoscopic surgery as the initial chest procedure (P # .001)after algorithm implementation. These interventions reduced related charges without significantlyaffecting length of stay, readmission rate, or other variables studied.
CONCLUSIONS: The collaborative creation and introduction of an algorithm for the managementof complicated pneumonia at our institution, combined with an effort among physicians toincorporate evidence-based clinical care into practice, led to reduced radiation exposure, surgicalrisk, and cost to patient.
Seton Healthcare Family,Austin, Texas
www.hospitalpediatrics.orgDOI:10.1542/hpeds.2016-0077Copyright © 2017 by the American Academy of Pediatrics
Address correspondence to Sarmistha B. Hauger, MD, Specially for Children, 1301 Barbara Jordan Blvd, Austin, TX 78723. E-mail:[email protected]
HOSPITAL PEDIATRICS (ISSN Numbers: Print, 2154-1663; Online, 2154-1671).
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Ms Quick designed the data collection instruments, performed data collection, coordinated and supervised initial analysis, and drafted the initialmanuscript; Dr Auth conceptualized the algorithm used in the study and was instrumental in carrying out the algorithm; Drs Fernandez, Meyer,Merkel, and Thoreson conceptualized the algorithm used in the study, were instrumental in carrying out the algorithm, and critically reviewedand revised the manuscript; Dr Hauger conceptualized the study design and algorithm used in the study, was instrumental in carrying out thealgorithm, and critically reviewed and revised the manuscript; and all authors approved the final manuscript as submitted.
HOSPITAL PEDIATRICS Volume 7, Issue 5, May 2017 287
by guest on July 18, 2018http://hosppeds.aappublications.org/Downloaded from

Evidence-based research has pointed topotential improvements in the care ofpediatric patients with complicatedpneumonia, specifically in the area ofimaging and surgical intervention. Previousimaging recommendations have favoredchest computed tomography (CT) as themodality of choice for evaluating complicatedpneumonia. Recent studies demonstrateultrasound to be as effective, with CT failingto provide any additional clinically usefulinformation when compared with ultrasound,even in the setting of lung abscess andnecrosis.1–4 Chest ultrasound has shownto be more cost-effective than CT, whichbecomes a consideration when equal clinicalinformation can be attained from either test.4
Surgical preference and data about chesttube placement with fibrinolytics in lieuof video-assisted thoracoscopic surgery(VATS) are more controversial, becauseinformation about outcomes is sparse.Although previous approaches to surgicalintervention in cases of complicatedpneumonia supported the use of early VATS,more recent prospective studies comparingthe effectiveness of VATS and chest tubeplacement with fibrinolytics have pointedtoward chest tube placement withfibrinolytics as the procedure of choice inmost cases.5–8 In 3 prospective, randomizedstudies chest tube with instillation offibrinolytics was equal to VATS for thetreatment of empyema and resulted inshorter or equal length of stay and lowercost.6–8 Studies that looked at cost sawsignificantly lower cost as an advantage tousing a chest tube with fibrinolytics.6,7 In aretrospective study comparing multiplechest procedures, Gates et al9 found thatcases without surgery had a shorterlength of stay and hospital chargescompared with patients with surgery.
Evidence supports favorable outcomeswhen both of these managementapproaches are combined to managecomplicated pneumonia. In 2 studieswhere a complicated pneumonia algorithmwas evaluated, decrease in chest CT usewas seen along with other favorableindicators such as lower readmission rateand fewer VATS, without any negative impacton length of stay or painful procedures.10,11
Improved care based on current evidenceis essential in medical practice. At ourinstitution, the creation of an evidence-based algorithm to standardize thetreatment of complicated pneumonia wasprompted by an abstract describingsuccess in using an algorithm at anotherhospital.12 Through dedicated collaborationbetween multiple disciplines to create,educate, disseminate, and evaluate thealgorithm, we have been able tosuccessfully reach specific goals ofimproving patient care, including reducingunnecessary radiation and decreasingsurgical risk in children with complicatedpneumonia.
METHODS
The overall goal of the complicatedpneumonia algorithm was to standardizeand improve care, basing decisions onclinical judgment, paired with evidence-based recommendations. The primary aimof this study is to describe this processand evaluate the effect of algorithmimplementation on imaging, proceduralintervention, and associated charges. Thesecondary aim is to compare the subgroupof patients with VATS and those withchest tube with fibrinolytics to assess theimpact of using the less invasive procedureon hospital course and cost.
Algorithm Creation andImplementation
Our institution previously used chest CT andearly VATS in the management approach ofcomplicated pneumonia. As new researchwas published about the use of ultrasoundin lieu of CT scans, some physicians beganto use ultrasound more frequently, but thepractice was not widely accepted. Motivatedby an abstract at a national conferenceabout the implementation of a complicatedpneumonia guideline at another institution,one of the authors (M.A.) organized a groupof interested physician leaders to review theliterature and present at a formal journalclub.12 The journal club, held in January2012, included a team of physicians fromthe hospitalist, general surgical, infectiousdisease, radiology, and pulmonologyservices, as well as representatives frompharmacy, nursing, imaging, and quality
improvement teams. A selected physicianfrom each team rigorously reviewed theliterature and presented relevantinformation based on the strength of thestudy and results. The literature review,discussion during the journal club, localantibiotic resistance patterns, andadditional discussions between thephysician champions led to the agreed-uponalgorithm. The algorithm includes specificimaging modalities, antibiotic selection,early surgical consultation, and evidence-based guidance on chest tube placementwith fibrinolytics compared with VATS. Thedraft of the algorithm was disseminatedto all team members in April of that yearfor review and edits before widespreadimplementation and dissemination.
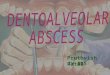
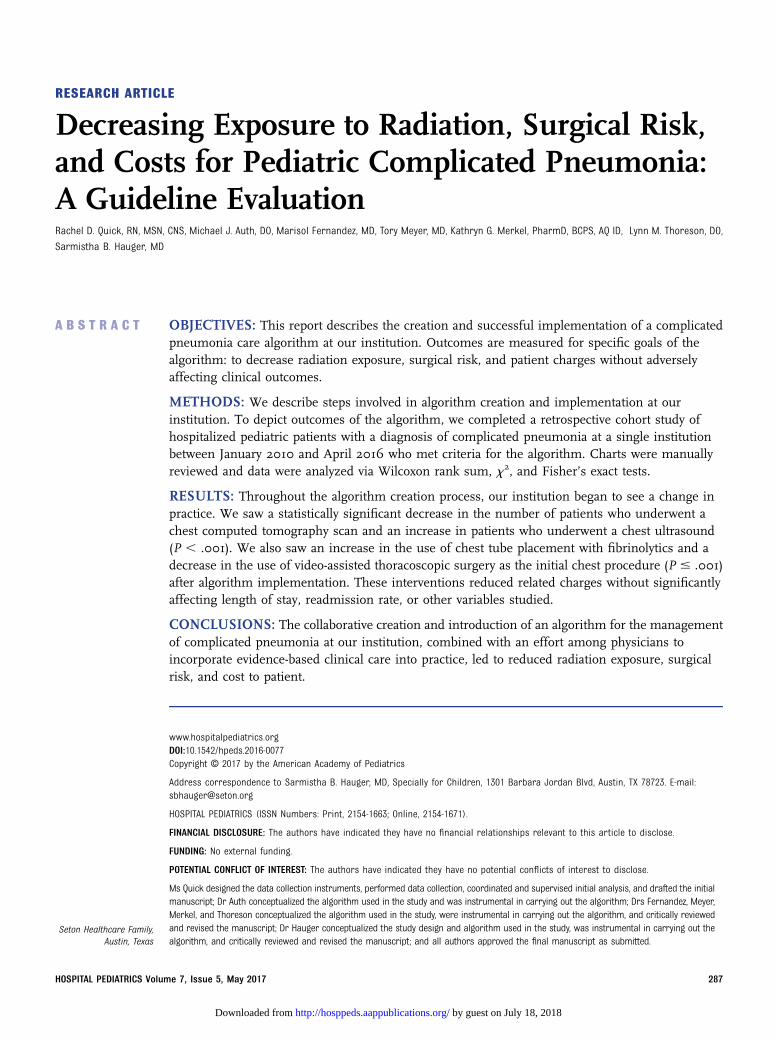
The pathway and recommendation in itsentirety were made available online on ourhospital system intranet site on April 1, 2013.Figure 1 includes the visual pathway, whichis part of a larger educational document.Dissemination and use of the algorithminvolved several approaches beginningdirectly after the initial meeting andcontinuing after the official rollout. A majorpoint of clarity reached through literaturereview was the choice of imaging.1–4
In the earliest stages, physicians on theteam began to personally educatecolleagues when a CT was ordered on apatient with complicated pneumonia. Thisinformal education helped push the initialsuccess in imaging change.
Additional adoption of the algorithm wasaccomplished with 2 major efforts:incorporation of the algorithmrecommendations into the electronic medicalrecord order set and education of thepediatric residents. An order set was createdthat highlighted the use of ultrasound overCT as the preferred modality and providedthe correct antibiotic and fibrinolytic dosingas recommended in the algorithm. A link tothe algorithm in the order set allowed easyaccess to the algorithm and supportinginformation for reference. The order set wascreated in partnership between the PICU andhospitalist services facilitating the use inboth areas of the hospital.
In a teaching institution with a medium-sized pediatric residency program with
288 QUICK et al
by guest on July 18, 2018http://hosppeds.aappublications.org/Downloaded from
house officers that provide 24-hour servicesin the emergency department, PICU, andinpatient service, the opportunity forwidespread adoption hinged on educationof the pediatric house staff. The physicianchampions used existing resident didacticsessions and grand rounds presentationsas venues for distributing the algorithm andthe evidence supporting its implementation.
The algorithm has been incorporated in theinpatient curriculum, and senior residentsare expected to understand and teach thecomponents and evidence-based literaturefor complicated pneumonia to interns androtating students.
After implementation of the algorithm,patient data were collected to trackadherence and successes. The algorithm
does not attempt to override clinicianjudgment, and although its use was stronglyencouraged, it was not strictly enforced.Throughout its implementation, weevaluated adherence by tracking outcomessuch as timing and use of laboratory tests,timing of surgical consults, use ofultrasound over CT scans, and use ofrecommended initial antibiotic choice.
FIGURE 1 Complicated bacterial pneumonia pathway. BMP, basic metabolic panel; CBC, complete blood cell count; CRP, C-reactive protein; ESR,erythrocyte sedimentation rate; FIO2, fraction of inspired oxygen; ID, infectious disease; IV, intravenous.
HOSPITAL PEDIATRICS Volume 7, Issue 5, May 2017 289
by guest on July 18, 2018http://hosppeds.aappublications.org/Downloaded from

Preliminary data were presented at amorbidity and mortality conference 1 yearafter the official algorithm implementationand described remarkable success inusing ultrasound over CT scans butuncovered system issues related to chesttube care and fibrinolytic administrationwhen chest tubes were placed byinterventional radiology. After placement ofchest tubes by interventional radiology,care was transitioned to the hospitalistservice staff, who had little experience withmanagement or administration offibrinolytics. This led to an importantdialogue and decision by surgical servicesto manage all chest tubes and fibrinolyticsregardless of the method of chest tubeplacement. The resolution of this importantsystem problem resulted in a more linearincrease in the use of chest tubes withfibrinolytics.
Evaluating the ComplicatedPneumonia Algorithm
To evaluate the success of the complicatedpneumonia guideline at our hospital, wecompleted a retrospective cohort study forpediatric patients age 3 months to 18 yearsadmitted to our institution between January1, 2010 and April 1, 2016 with a diagnosis ofcomplicated pneumonia. Initial charts wereidentified with International Classification ofDiseases, Ninth Revision (ICD-9) diagnosiscodes for pneumonia-related illness and1 of the following additional qualifiers usedto filter cases of simple pneumonia: chestCT, chest ultrasound, or pleural culture.ICD-9 codes related to pneumonia included011.2, 481, 482.0, 482.1, 482.30, 482.31,482.32, 482.39, 482.40, 482.41, 482.42, 482.81,482.82, 482.89, 482.9, 483.8, 486, 490, 510.0,510.9, 511.1, 511.9, 513.0, and 518.89.Equivalent ICD-10 codes were substitutedafter the updates in coding. Charts werethen manually reviewed to ensure thatcases met the inclusion and exclusioncriteria chosen for the pediatriccomplicated pneumonia algorithm (Fig 1).
Methods of Comparison Before andAfter Algorithm Implementation
Using the above methods, we identified570 cases with a diagnosis of pneumoniaand chest CT, chest ultrasound, or pleural
culture. After inclusion and exclusioncriteria for the algorithm were applied bymanual review, 244 cases were included:131 preguideline and 113 postguideline.Although some practice change occurredwith algorithm development, the officialrollout date was selected as the pre/postcomparison because it representedwidespread availability to hospitalpersonnel.
The study population of 244 cases withcomplicated pneumonia across 6.25 yearswas evaluated as a whole, and then specificvariables were compared between the2 cohorts: admission before and afterguideline implementation. Variables werechosen for their effect on imaging, hospitalcourse, and illness course and includedreadmission for pneumonia within 30 days,length of stay, use of chest CT, use of chestultrasound, ICU admission, ICU length ofstay, chest tube requirement and procedure,hospital day of chest tube placement, dayswith a chest tube, complications, number ofantibiotics received, and hospital chargesfor imaging and chest proceduresrecommended in the algorithm.
Methods of Comparison of ChestProcedures: VATS Versus Chest TubeWith Fibrinolytics
Patients who had, as their initialprocedure, either VATS or chest tubewith fibrinolytics were compared. A totalof 105 cases needed chest drainageand had chest tube with fibrinolytics orVATS specifically as their first chestprocedure; 71 cases with VATS as the initialchest procedure and 34 with chest tubewith fibrinolytics. Cases with thoracentesisonly or with chest tube placement withoutfibrinolytics were excluded from thisanalysis because they were not part ofthe algorithm or were so infrequentlyused. The focus of our comparison wasbetween VATS and chest tube fibrinolytics.These 105 cases were compared as asubgroup for the following outcomes:length of stay, chest procedure failurerate (defined as the need for asecond chest procedure), total dayswith chest tube (including days withsecond chest tube where applicable),readmission rate, and hospital charges
associated with these variables. Thedecision to compare these specific casesagainst one another was made in anattempt to minimize confoundingvariables that would influence outcomemeasures.
Methods for Calculating Charges
Charges applied for analysis includedprofessional charges and facility charges.The following Current ProceduralTerminology codes were used to assesscharges: VATS (an average of charges for32651 and 32652, plus 32551 for chest tubeplacement), chest tube placement withimaging guidance (32557), chest ultrasound(76604), and chest CT (an average ofcharges for 71250, 71260, and 71270).
All cases had either a chest CT or chestultrasound; therefore, the hospital chargeper patient was calculated for the overallnumber of these procedures and chargeswere compared before and after algorithmimplementation.
Charges for the subset of patients with VATSor chest tube with fibrinolytics werecompared as a subgroup. Chargescalculated for each patient in the subgroupincluded charges for initial chest procedure,room rates for total ICU days and warddays, readmission days, and subsequentchest procedures. Charge comparisonsbetween VATS and chest tube withfibrinolytics were categorized according tothe initial chest procedure.
We predicted that using chest ultrasoundover chest CT and chest tube withfibrinolytics over VATS would reduce hospitalcharges while also reducing exposure toradiation and surgical risk without negativeimpact on illness course. We chose chestultrasound and chest tube with fibrinolyticsas outcome measures to assess theimpact of the algorithm itself. We selectedspecific variables to describe the illnesscourse, including length of stay, need foradditional chest procedures, andreadmission rate.
All information was entered into aRedcap database. Data were analyzed inRStudio software (RStudio, Boston, MA)including Wilcoxon rank-sum, Fisher’s exact,and x2 tests.13,14
290 QUICK et al
by guest on July 18, 2018http://hosppeds.aappublications.org/Downloaded from
RESULTS
The median age of children included in thestudy was 4.9 years (interquartile range[IQR] 2.5–9.6); gender was nearly equal at49% male and 51% female. The entirepopulation of 244 cases was used tocompare variables between 2 cohorts,before and after algorithm implementation.
Imaging Results
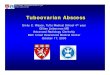
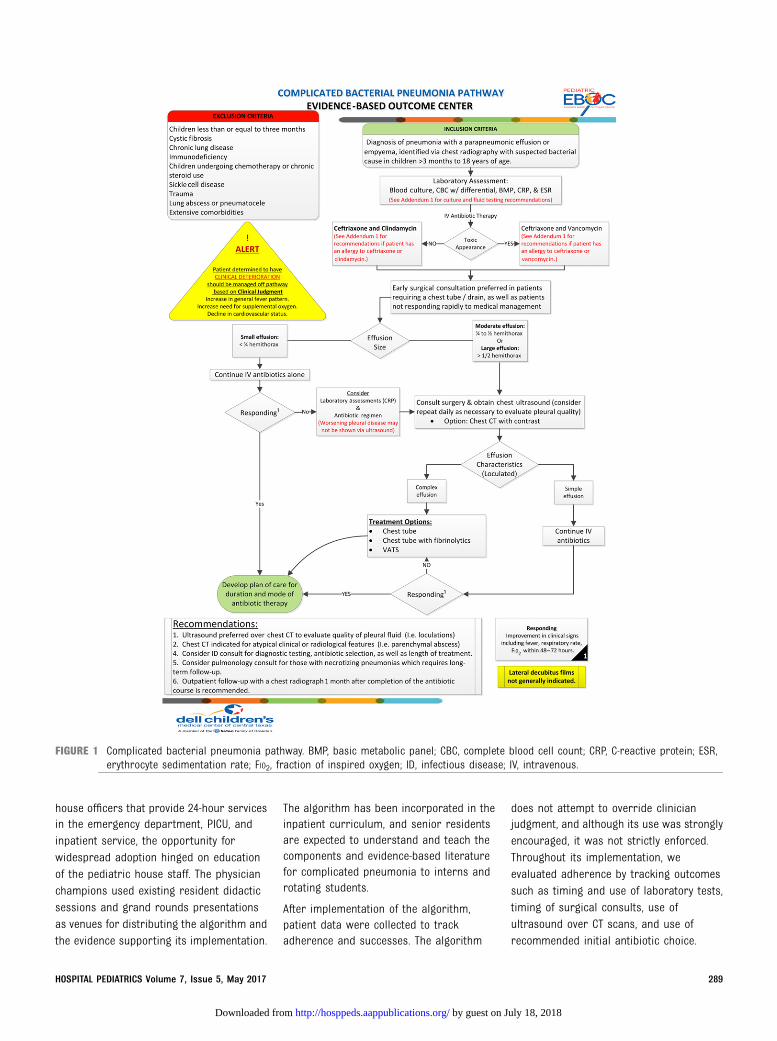
When comparing chest ultrasound andchest CT use before and after theimplementation of the complicatedpneumonia algorithm, we found astatistically significant decrease in thenumber of patients who underwent a chestCT scan and increase in the number ofpatients who underwent a chest ultrasound(P , .001 for both, Fig 2). During the sametime period, no significant difference wasseen in any of the other variablesdescribing the illness course and hospitalstay, including ICU admission rates, ICUlength of stay, hospital length of stay, dayswith a chest tube, rate of chest procedures,or readmission. Changes in this variablecan be seen on the graph as beginning evenbefore the official rollout of the algorithm.
Chest Procedure Results
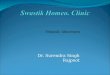
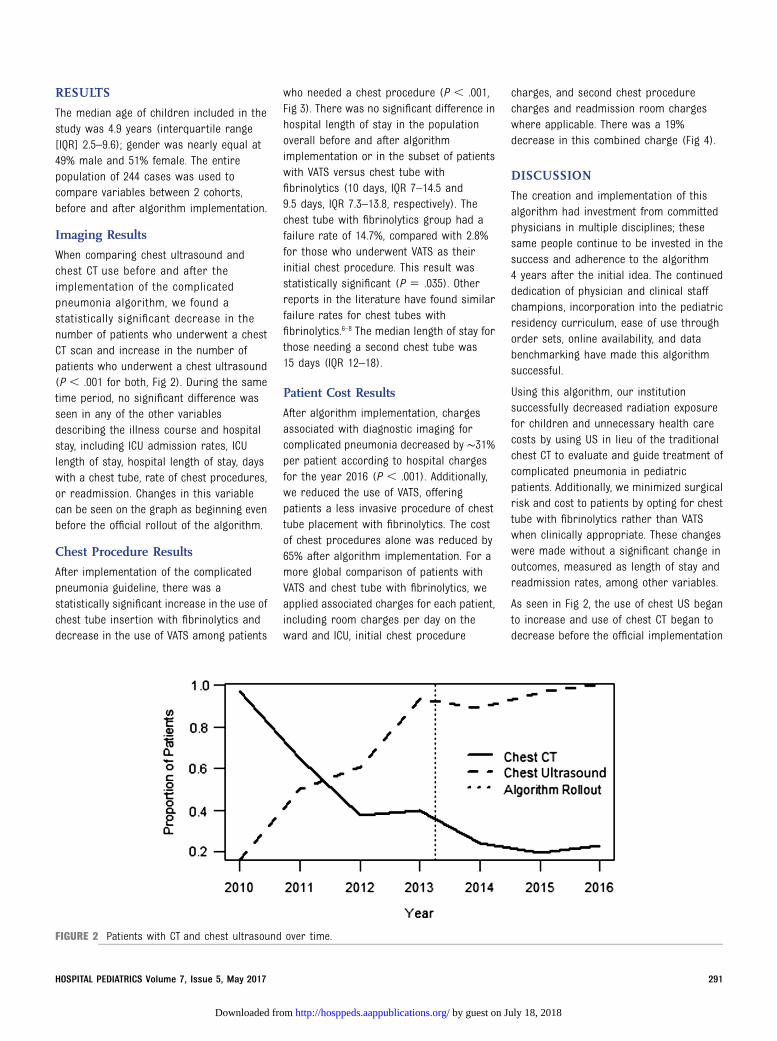
After implementation of the complicatedpneumonia guideline, there was astatistically significant increase in the use ofchest tube insertion with fibrinolytics anddecrease in the use of VATS among patients
who needed a chest procedure (P , .001,Fig 3). There was no significant difference inhospital length of stay in the populationoverall before and after algorithmimplementation or in the subset of patientswith VATS versus chest tube withfibrinolytics (10 days, IQR 7–14.5 and9.5 days, IQR 7.3–13.8, respectively). Thechest tube with fibrinolytics group had afailure rate of 14.7%, compared with 2.8%for those who underwent VATS as theirinitial chest procedure. This result wasstatistically significant (P 5 .035). Otherreports in the literature have found similarfailure rates for chest tubes withfibrinolytics.6–8 The median length of stay forthose needing a second chest tube was15 days (IQR 12–18).
Patient Cost Results
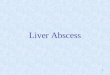
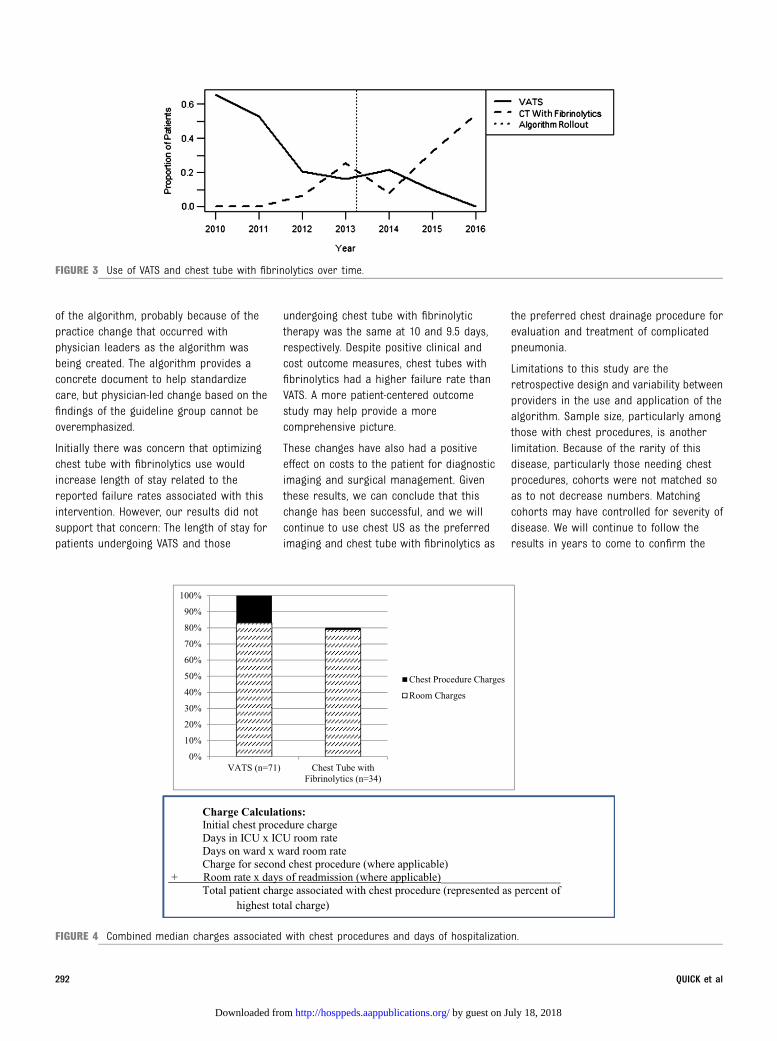
After algorithm implementation, chargesassociated with diagnostic imaging forcomplicated pneumonia decreased by ∼31%per patient according to hospital chargesfor the year 2016 (P , .001). Additionally,we reduced the use of VATS, offeringpatients a less invasive procedure of chesttube placement with fibrinolytics. The costof chest procedures alone was reduced by65% after algorithm implementation. For amore global comparison of patients withVATS and chest tube with fibrinolytics, weapplied associated charges for each patient,including room charges per day on theward and ICU, initial chest procedure
charges, and second chest procedurecharges and readmission room chargeswhere applicable. There was a 19%decrease in this combined charge (Fig 4).
DISCUSSION
The creation and implementation of thisalgorithm had investment from committedphysicians in multiple disciplines; thesesame people continue to be invested in thesuccess and adherence to the algorithm4 years after the initial idea. The continueddedication of physician and clinical staffchampions, incorporation into the pediatricresidency curriculum, ease of use throughorder sets, online availability, and databenchmarking have made this algorithmsuccessful.
Using this algorithm, our institutionsuccessfully decreased radiation exposurefor children and unnecessary health carecosts by using US in lieu of the traditionalchest CT to evaluate and guide treatment ofcomplicated pneumonia in pediatricpatients. Additionally, we minimized surgicalrisk and cost to patients by opting for chesttube with fibrinolytics rather than VATSwhen clinically appropriate. These changeswere made without a significant change inoutcomes, measured as length of stay andreadmission rates, among other variables.
As seen in Fig 2, the use of chest US beganto increase and use of chest CT began todecrease before the official implementation
FIGURE 2 Patients with CT and chest ultrasound over time.
HOSPITAL PEDIATRICS Volume 7, Issue 5, May 2017 291
by guest on July 18, 2018http://hosppeds.aappublications.org/Downloaded from
of the algorithm, probably because of thepractice change that occurred withphysician leaders as the algorithm wasbeing created. The algorithm provides aconcrete document to help standardizecare, but physician-led change based on thefindings of the guideline group cannot beoveremphasized.
Initially there was concern that optimizingchest tube with fibrinolytics use wouldincrease length of stay related to thereported failure rates associated with thisintervention. However, our results did notsupport that concern: The length of stay forpatients undergoing VATS and those
undergoing chest tube with fibrinolytictherapy was the same at 10 and 9.5 days,respectively. Despite positive clinical andcost outcome measures, chest tubes withfibrinolytics had a higher failure rate thanVATS. A more patient-centered outcomestudy may help provide a morecomprehensive picture.
These changes have also had a positiveeffect on costs to the patient for diagnosticimaging and surgical management. Giventhese results, we can conclude that thischange has been successful, and we willcontinue to use chest US as the preferredimaging and chest tube with fibrinolytics as
the preferred chest drainage procedure forevaluation and treatment of complicatedpneumonia.
Limitations to this study are theretrospective design and variability betweenproviders in the use and application of thealgorithm. Sample size, particularly amongthose with chest procedures, is anotherlimitation. Because of the rarity of thisdisease, particularly those needing chestprocedures, cohorts were not matched soas to not decrease numbers. Matchingcohorts may have controlled for severity ofdisease. We will continue to follow theresults in years to come to confirm the
FIGURE 3 Use of VATS and chest tube with fibrinolytics over time.
FIGURE 4 Combined median charges associated with chest procedures and days of hospitalization.
292 QUICK et al
by guest on July 18, 2018http://hosppeds.aappublications.org/Downloaded from
trends seen in these data. The variablesassessed in this study are part of a largeralgorithm and were implemented along withother changes such as initial antibiotics andlaboratory data, introducing the risk ofconfounding variables. We plan tocontinuously evaluate other portions of thealgorithm with the goal of providing thesafest, most efficient care to our patients.
Acknowledgment
We would like to acknowledge thecontributions made by Patrick Boswell atour local Evidence Based Outcomes Center.Patrick helped this project by providing caselists, aiding in figure formatting,brainstorming for cost analysis, andparticipating in feedback during periodicmeetings to review process of guidelineimplementation.
REFERENCES
1. Kurian J, Levin TL, Han BK, Taragin BH,Weinstein S. Comparison of ultrasoundand CT in the evaluation of pneumoniacomplicated by parapneumonic effusionin children. AJR Am J Roentgenol. 2009;193(6):1648–1654
2. Blaivas M. Lung ultrasound in evaluationof pneumonia. J Ultrasound Med. 2012;31(6):823–826
3. Caiulo VA, Gargani L, Caiulo S, et al. Lungultrasound characteristics of community-acquired pneumonia in hospitalized children.Pediatr Pulmonol. 2013;48(3):280–287
4. Bierig SM, Jones A. Accuracy and costcomparison of ultrasound versusalternative imaging modalities, includingCT, MR, PET, and angiography. J DiagnMed Sonogr. 2009;25(3):138–144
5. Bender MT, Ward AN, Iocono JA, Saha SP.Current surgical management of empyemathoracis in children: a single-centerexperience. Am Surg. 2015;81(9):849–853
6. St Peter SD, Tsao K, Spilde TL, et al.Thoracoscopic decortication vs tubethoracostomy with fibrinolysis forempyema in children: a prospective,randomized trial [published correctionappears in J Pediatr Surg. 2009;44(9):1865]. J Pediatr Surg. 2009;44(1):106–111, discussion 111
7. Sonnappa S, Cohen G, Owens CM, et al.Comparison of urokinase and video-assisted thoracoscopic surgery fortreatment of childhood empyema. Am JRespir Crit Care Med. 2006;174(2):221–227
8. Cobanoglu U, Sayir F, Bilici S, Melek M.Comparison of the methods offibrinolysis by tube thoracostomy andthoracoscopic decortication in childrenwith stage II and III empyema: aprospective randomized study. PediatrRep. 2011;3(4):e29
9. Gates RL, Hogan M, Weinstein S, Arca MJ.Drainage, fibrinolytics, or surgery: acomparison of treatment options in
pediatric empyema. J Pediatr Surg.2004;39(11):1638–1642
10. Pillai D, Song X, Pastor W, et al.Implementation and impact of aconsensus diagnostic and managementalgorithm for complicated pneumonia inchildren. J Investig Med. 2011;59(8):1221–1227
11. Shomaker KL, Weiner T, Esther CR Jr.Impact of an evidence-based algorithmon quality of care in pediatricparapneumonic effusion and empyema.Pediatr Pulmonol. 2011;46(7):722–728
12. Pillai D, Song X, Pastor W, et al.Implementation and impact of aconsensus diagnostic and managementalgorithm for complicated pneumoniain children. In: Oral abstract sessionpresented at the 49th annual meetingof the Infectious Diseases Society ofAmerica; October 20–23, 2011; Boston,MA
13. Harris PA, Taylor R, Thielke R, Payne J,Gonzalez N, Conde JG. Researchelectronic data capture (REDCap): ametadata-driven methodology andworkflow process for providingtranslational research informaticssupport. J Biomed Inform. 2009;42(2):377–381
14. RStudio Team. RStudio: IntegratedDevelopment for R. Boston, MA: RStudio,Inc; 2015. Available at: www.rstudio.com/
HOSPITAL PEDIATRICS Volume 7, Issue 5, May 2017 293
by guest on July 18, 2018http://hosppeds.aappublications.org/Downloaded from

originally published online April 27, 2017; Hospital Pediatrics Merkel, Lynn M. Thoreson and Sarmistha B. Hauger
Rachel D. Quick, Michael J. Auth, Marisol Fernandez, Tory Meyer, Kathryn G.Complicated Pneumonia: A Guideline Evaluation
Decreasing Exposure to Radiation, Surgical Risk, and Costs for Pediatric
ServicesUpdated Information &
2016-0077http://hosppeds.aappublications.org/content/early/2017/04/25/hpeds.including high resolution figures, can be found at:
Subspecialty Collections
provement_subhttp://classic.hosppeds.aappublications.org/cgi/collection/quality_imQuality Improvementdiseases_subhttp://classic.hosppeds.aappublications.org/cgi/collection/infectious_Infectious Diseaseion:practice_management_subhttp://classic.hosppeds.aappublications.org/cgi/collection/administratAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
mlhttp://classic.hosppeds.aappublications.org/site/misc/Permissions.xhtin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.hosppeds.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 18, 2018http://hosppeds.aappublications.org/Downloaded from
originally published online April 27, 2017; Hospital Pediatrics Merkel, Lynn M. Thoreson and Sarmistha B. Hauger
Rachel D. Quick, Michael J. Auth, Marisol Fernandez, Tory Meyer, Kathryn G.Complicated Pneumonia: A Guideline Evaluation
Decreasing Exposure to Radiation, Surgical Risk, and Costs for Pediatric
http://hosppeds.aappublications.org/content/early/2017/04/25/hpeds.2016-0077located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Pediatrics. All rights reserved. Print ISSN: 2154-1663. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2017 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 2012. Hospital Pediatrics is owned, Hospital Pediatrics is the official journal of the American Academy of Pediatrics. A monthly
by guest on July 18, 2018http://hosppeds.aappublications.org/Downloaded from