Embed Size (px)
Citation preview

Formosan Journal of Surgery (2015) 48, 222e225
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by Elsevier - Publisher Connector
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.e-f js .com
CASE REPORT
Delayed contralateral epidural hematomaafter decompressive craniectomy for atraumatic acute subdural hematoma
Chen-Hsing Su a,b,c, Jung-Tung Liu a,b,c, Cheng-Siu Chang a,b,c,Wen-Jui Liao a,b,c, Cho-Shun Li a,b,c,*
a School of Medicine, Chung-Shan Medical University, Taichung, Taiwanb Department of Medical Education, Chung-Shan Medical University Hospital, Taichung, Taiwanc Department of Neurosurgery, Chung-Shan Medical University Hospital, Taichung, Taiwan
Received 18 May 2015; received in revised form 6 July 2015; accepted 27 August 2015Available online 25 December 2015
KEYWORDSepidural hematoma;intracranial pressure;subdural hematoma;therapeutichypothermia
Conflicts of interest: The authors* Corresponding author. Departmen
Taichung, Taiwan.E-mail addresses: [email protected]
http://dx.doi.org/10.1016/j.fjs.2015.1682-606X/Copyright ª 2015, Taiwan
Summary After falling from a height, a 29-year-old male patient developed a traumatic leftsubdural hematoma (SDH) with brain swelling and a midline shift to the right side, as well as asmall epidural hematoma (EDH) (thickness: <1 cm) overlying a contralateral temporal linearfracture. A decompressive craniectomy for SDH evacuation and the placement of an intracra-nial pressure (ICP) monitoring device were performed. Because of uncontrollable ICP(>35 mmHg) 48 hours after surgery, a left, extended decompressive craniectomy was per-formed in combination with therapeutic hypothermia for 6 days, including rewarming for 3days. The patient remained stable for several days. However, the patient developed suddenright pupil dilatation with an uncal herniation on Day 14. Computed tomography revealed aconsiderable enlargement of the contralateral EDH. An emergency craniectomy was performedfor EDH evacuation. In this paper, we describe this rare case, in which the delayed expansionof the contralateral EDH occurred 14 days after the initial surgery, and discuss its clinical man-agement and radiologic findings, in addition to reviewing the literature and presenting thepossible mechanism of this complication.Copyright ª 2015, Taiwan Surgical Association. Published by Elsevier Taiwan LLC. All rightsreserved.
declare no conflicts of interest.t of Neurosurgery, Chung-Shan Medical University Hospital, 110, Section 1, Chien-Kuo North Road,
rg.tw, [email protected] (C.-S. Li).
08.008Surgical Association. Published by Elsevier Taiwan LLC. All rights reserved.

Delayed expansion of a contralateral epidural hematoma 223
1. Introduction
Delayed expansion of a contralateral epidural hematoma(EDH) after decompressive surgery for an acute subduralhematoma (SDH) is rare. It is a life threatening conditionrequiring emergency evacuation surgery. The longestperiod for an occurrence of the enlargement of a delayedcontralateral EDH following the initial surgery is 96 hours,as reported by Su et al.1 Here, we report a patient whodeveloped delayed EDH expansion 14 days after the initialsurgery, an extensive period never reported in the litera-ture according to our research.
2. Case Report
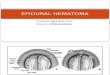
A 29-year-old male patient developed a disturbance ofconsciousness after falling from a 4-m height. His initialGlasgow Coma Scale score at the emergency room wasE2V1M4. Brain computed tomography (CT) revealed a leftSDH, a traumatic subarachnoid hemorrhage with a masseffect and a midline shift, and a small right temporal EDH(thickness: <1 cm) overlying a fracture of the right tem-poral bone (Figure 1). An emergency decompressive
Figure 1 Initial computed tomography showing (A) a small rigtemporal subdural hematoma with a midline shift, (C) and (D) a ri
craniectomy for SDH evacuation and the placement of anintracranial pressure (ICP) monitoring device (Camino;Integra Life Sciences Corporation, Plainsboro, NJ, USA)were performed. Two days following the craniectomy,Cushing’s triad, including considerable bradycardia andhypertension, and increased ICP up to 35 mmHg wereobserved. A follow-up CT scan revealed considerable brainswelling on the left side with a midline shift, whereas noenlargement of the contralateral temporal EDH wasobserved (Figure 2). An extended decompressive craniec-tomy was performed in combination with therapeutic hy-pothermia (TH). TH was maintained at a targettemperature of 33�C for 6 days, including rewarming to36�C at a rate of 1�C/d for 3 days. ICP was approximately15 mmHg during the TH. After regaining a normal bodytemperature on Day 8, repeat CT revealed residual brainswelling without a midline shift and no obvious enlargementof the right temporal EDH (Figure 3). The osmotic agentsused from Day 1 were tapered accordingly, and the patientremained stable for several days. However, 5 days followingthe completion of TH or Day 14 after his traumatic braininjury, the patient developed sudden right pupil dilatation,and his Glasgow Coma Scale score decreased from E2VTM5to E1VTM3. A follow-up CT scan revealed a considerable
ht temporal epidural hematoma (thickness: <1 cm), (B) leftght temporal bone fracture (arrows).

Figure 2 Computed tomography on Day 2 after decompressive surgery showing considerable left brain swelling with a midlineshift but no enlargement of the right temporal epidural hematoma.
Figure 3 Repeat computed tomography on Day 8 after rewarming showing residual brain swelling without a midline shift and noobvious enlargement of the right temporal epidural hematoma.
224 C.-H. Su et al.
expansion of the right temporal EDH (Figure 4). An emer-gency craniectomy with an EDH evacuation was performed.At discharge 2 months later, the patient remained in avegetative state.
3. Discussion
Delayed expansion of a contralateral EDH after decom-pressive surgery for an acute SDH is rare, with an incidenceranging from 1.3% to 5.7%.1e3 In the literature, the longestperiod for an occurrence of the enlargement of a delayedcontralateral EDH following the initial surgery is 4 days, asreported by Su et al.1 Our patient developed a delayedexpansion of the EDH 14 days after the initial surgery, anextensive period never reported in the literature according
to our research. Intraoperative brain swelling, post-operative neurologic deterioration, and uncontrollable,elevated ICP may imply a delayed expansion of thecontralateral EDH.4 A decompressive craniectomy may be apredisposing factor for a delayed expansion of the EDH.5 Animmediate postoperative CT scan is recommended for pa-tients with an acute SDH and a contralateral skull fractureto detect this rare but life threatening delayed expansionof the contralateral EDH, which has devastating conse-quences such as neurologic deficits and even death.1
Shen et al2 reviewed 37 patients with an expansion of acontralateral acute EDH following acute SDH evacuation, ofwhom 81% (30/37) had contralateral skull fractures andonly one was aged > 60 years. The low prevalence of EDHformation among elderly patients may be attributed to

Figure 4 Follow-up computed tomography on Day 14 showing considerable expansion of the right temporal epidural hematomawith uncal herniation.
Delayed expansion of a contralateral epidural hematoma 225
increased adherence between the dura and the inner tableof the skull.
The precise mechanism of the delayed formation of acontralateral EDH following a decompressive craniectomy isunclear. It has been hypothesized that the initial impactcauses a contrecoup injury with SDH and intracerebral he-matoma formation, in addition to a coup injury with a skullfracture and bleeding from the fracture site or the duramater.6 The SDH with mass effect probably increases theICP and produces a tamponade effect on the contralateralepidural bleeding source, which subsequently inducesdelayed EDH enlargement after the mass effect has sub-sided or the SDH is removed. Therefore, measures such asdecompressive surgery, the use of hyperosmolar agents,and TH are undertaken to reduce the elevated ICP, whichmay decrease the tamponade effect and promote delayedformation or expansion of a contralateral EDH.7,8
In our reported case, the uncontrollable ICP wasfrequently >35 mmHg with considerable Cushing’s triaddespite treatment with various osmotic agents. Repeat CT(Figure 2) confirmed that the intracranial hypertension wasinduced by brain swelling rather than by the rare but lifethreatening delayed expansion of the contralateral EDH.Sadaka and Veremakis et al9 reviewed the most recent 18studies using TH for ICP management in patients withtraumatic brain injury, concluding that ICP was alwayssignificantly lower in the TH group than in the normo-thermia group. We started TH as a second-line therapeuticoption; the ICP was <20 mmHg, and no TH-induced coa-gulopathy or other side effects were observed. A decom-pressive craniectomy is a predisposing factor for thedelayed expansion of an EDH.5 The prolonged use ofhyperosmolar agents and TH may further reduce the ICPand gradually decrease the tamponade effect, which isattributed to the etiology of this devastating delayedexpansion of the contralateral EDH. Based on our research,no other study has reported the delayed expansion of a
contralateral EDH occurring up to 14 days after the initialsurgery. Neurosurgeons should be aware that the rare butlife threatening delayed expansion of a contralateral EDHcan occur within an extensive period after the initial sur-gery. Additional studies should be conducted to determinewhether contralateral EDHs should be managed during theinitial surgery.
References
1. Su TM, Lee TH, Chen WF, Lee TC, Cheng CH. Contralateral acuteepidural hematoma after decompressive surgery of acute sub-dural hematoma: clinical features and outcome. J Trauma.2008;65:1298e1302.
2. Shen J, Pan JW, Fan ZX, Zhou YO, Chen Z, Zhan RY. Surgery forcontralateral acute epidural hematoma following acute sub-dural hematoma evacuation: five new cases and a short litera-ture review. Acta Neurochir (Wien). 2013;155:335e341.
3. Matsuno A, Katayama H, Wada H, et al. Significance of consec-utive bilateral surgeries for patients with acute subdural he-matoma who develop contralateral acute epi- or subduralhematoma. Surg Neurol. 2003;60:23e30. discussion 30.
4. Feuerman T, Wackym PA, Gade GF, Lanman T, Becker D. Intra-operative development of contralateral epidural hematomaduring evacuation of traumatic extraaxial hematoma. Neuro-surgery. 1988;23:480e484.
5. Chen H, Guo Y, Chen SW, et al. Progressive epidural hematoma inpatients with head trauma: incidence, outcome, and risk factors.Emerg Med Int. 2012. http://dx.doi.org/10.1155/2012/134905.
6. Lindenberg R, Freytag E. The mechanism of cerebral contusions:a pathologic-anatomic study. Arch Pathol. 1960;69:440e469.
7. Borovich B, Braun J, Guilburd JN, et al. Delayed onset of trau-matic extradural hematoma. J Neurosurg. 1985;63:30e34.
8. Thibodeau M, Melanson D, Ethier R. Acute epidural hematomafollowing decompressive surgery of a subdural hematoma. CanAssoc Radiol J. 1987;38:52e53.
9. Sadaka F, Veremakis C. Therapeutic hypothermia for the man-agement of intracranial hypertension in severe traumatic braininjury: a systematic review. Brain Inj. 2012;26:899e908.