Embed Size (px)
Citation preview

Delayed Repair of Congenital Diaphragmatic Hernia With Early High-Frequency Oscillatory Ventilation
During Preoperative Stabilization
By Cynthia Reyes, Lynn K. Chang, Feizal Waffarn, Halleh Mir, M. James Warden, and Jack Sills
Orange, California
Purpose: The authors reviewed their experience in the man- agement of CDH after the introduction of early high- frequency oscillatory ventilation (HFOV) during the preopera- tive stabilization period and delayed CDH repair.
Methods: This is a retrospective analysis of 24 consecutive infants with CDH treated at University of California, Irvine Medical Center (UCIMC) during a 36-month period from January 1993 to December 1996.
Results: Two patients were excluded from the study: one fetus with a prenatal diagnosis was referred for fetal surgery; one infant received CDH repair at another institution 2 weeks before transfer to UCIMC. Eight (36%) infants were inborn, and nine (41%) had a prenatal diagnosis of CDH. Median gestational age was 40 weeks (range, 29 to 42 weeks). Median birth weight was 3,019 g (range, 1,205 to 4,337 g). The defect was left sided in 18 infants (86%). Twenty-one infants were intubated within 5 hours of life, 15 had an AaD greater than 610,ll had an oxygenation index greater than 40, and 11 had a pH of less than 7.2. The median ratio of pulmonary artery pressure to systemic blood pressure was 0.93 (range, 0.51 to 1.15) in 12 infants. Eighteen infants were placed on HFOV within a median of 1 hour of life. Nitric oxide was given to six infants and surfactant to eight. Four infants were referred for
T HE MANAGEMENT of neonatal respiratory failure with mechanical-assisted ventilation has evolved
with advances in technology and a better understanding of the pathophysiological mechanisms contributing to hypoxia, hypercarbia, and acidosis. Besides pulmonary parenchymal disorders, decreased pulmonary blood flow with intra- and extrapulmonary shunts resulting in pulmo- nary artery hypertension further complicate the clinical treatment of these infants.
In the late 1970s hyperventilation-induced alkalosis
From the Division of Pediatric Surgery, Department of Surgery, and the Department of Neonatal Medicine, University of California, Irvine Medical Center Orange, CA.
Presented at the 1997 Annual Meeting of the Section on Surgery of the American Academy of Pediatrics, New Orleans, Louisiana, October 31.November 2, 1997.
Address reprint requests to Cynthia Reyes, MD, Assistant Professor Department of Surgery, Chief Division of Pediatric Surgery, UC Irvine Medical Center; IO1 City Dr; Bldg 53, Rt # 81, Orange, CA 92868.
Copyright 0 1998 by WB. Saunders Company 0022-3468/98/3307-OOIO$O3.00/0
1010
extracorporeal membrane oxygenation (ECMO). Repair of CDH was performed on infants at a median age of 33.5 hours (range, 5.5 to 322). Six (30%) received a prosthetic patch. Overall 18 of 22 infants survived (81%); three survivors received ECMO. Two infants of the survivor group had congenital heart anomalies: one ventricular septal defect (VSD) and one double-outlet right ventricle with a VSD. Of the four nonsurvivors, one had lethal cardiac anomalies and bilateral CDH, two had severe bilateral pulmonary hypoplasia (one received ECMO), and one infant was a 29-week prema- ture babywho did not qualify for ECMO.
Conclusion: We report a survival rate of 81% (18 of 22) with the management of CDH by delayed surgical repair, early postnatal HFOV, and selective referral for ECMO. J Pediatr Surg 33:1070-1016. Copyright o 1998 by W.B. Saunders Company.
INDEX WORDS: Congenital diaphragmatic hernia, delayed surgery, high frequency oscillatory ventilation, respiratory failure, extracorporeal membrane oxygenation, nitric oxide, surfactant, persistent pulmonary hypertension of the new- born.
was introduced to lower pulmonary arterial pressure in the management of persistent pulmonary hypertension. * During the same period, Bartlett et al2 developed extracor- poreal membrane oxygenation (ECMO) for support of the moribund neonate from respiratory failure. In the 1980s Kolobow et al3 demonstrated pulmonary injury as a result of hyperventilation and Wung et al4 pioneered the art of “gentle ventilation” and permissive hypercapnia. High-frequency oscillatory ventilation (HFOV) provided an additional tool to support neonatal respiratory fail- ure.5Jj The 1990s introduced inhaled nitric oxide (NO) as a selective pulmonary vasodilator that improved oxygen- ation in infants with respiratory failure.7
Likewise, the perioperative management of congenital diaphragmatic hernia (CDH) has evolved over the recent years. Immediate postnatal repair of the hernia previously was the standard of care.* Recently, the care of the CDH patient has included early CDH repair with ECMO rescue,9 ECMO rescue with CDH repair on ECMO,lO CDH repair after ECMO, delayed CDH repair with preoperative stabilization,ll and fetal surgery.12 Exog-
Joorna/ofPediatricSurgery,Vol33,No7 (Julyj,1998:pp 1010-1016
DELAYED REPAIR OF CDH AND EARLY HFOV 1011
enous surfactant13 and inhaled nitric oxide14s’5 have been used as adjunct therapies in the perioperative care of the CDH infant. Liquid ventilation with perflourocarbon16 has shown promise in the treatment of CDH, but remains experimental. Lung transplantation has been successfully performed in a neonate with CDH.17
Our institution adopted the approach of delayed CDH repair and preoperative stabilization using HFOV in January 1993. This is a retrospective chart review of 24 CDH patients treated during January 1993 to December 1996.
MATERIALS AND METHODS
A retrospective analysis of the medical records of 24 neonates with CDH treated at the University of California, Irvine Medical Center (UCIMC) from January 1993 to December 1996 was performed. The same clinicians were involved in the care of these patients.
The management of CDH at UCIMC before 1993 consisted of early repair with postoperative support using conventional positive pressure ventilation and ECMO support when necessary. The strategy of delayed CDH repair with preoperative stabilization and preferential use of HFOV was initiated in early 1993. At UCIMC, the neonatologists’ experience with HFOV in the management of pulmonary hypoplasia and conditions with low lung volume (ie, oligohydramnios) demon- strated rapid alveolar recruitment that resulted in optimal lung volumes. optimal oxygenation, and carbon dioxide clearance. Based on the knowledge that infants with CDH also had pulmonary hypoplasia, HFOV was adopted as a treatment strategy for the CDH patient. As a result, HFOV was offered early to CDH infants in respiratory distress.
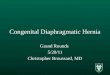
Infants born in our center received a clinical and radiological assessment of the pulmonary status, Those infants requiring intubation were placed immediately on HFOV (SensorMedics 3 lOOA: SensorMed- its, Yorba Linda, CA). Infants that were intubated before transfer were placed on HFOV at our institution if there was evidence of poor lung expansion and pulmonary parenchymal disease. The infants that required intubation after transfer to our institution were usually placed on HFOV immediately. The ventilator settings were adjusted to achieve adequate lung volume. Adequate lung volume was defined as an eight-rib expansion of the contralateral lung. Preductal and postductal oxygen saturation was monitored with pulse oximetry. Arterial blood gases were monitored from the right radial artery or the umbilical artery. The paces was maintained at normal levels. No attempt was made to hyperventilate or induce permissive hypercapnia. The mean airway pressure was weaned after adequate lung volume and acceptable blood gases were achieved (Fig 1).
A Replogle was inserted for decompression of the gastrointestinal
25
i \
intubation prew
Fig 1. Mean airway pressure at intubation and before surgery.
tract. Prophylactic broad-spectrum antibiotics were given. Vasopressors (dopamine and dobutamine) were infused when necessary to maintain mean blood pressure appropriate for birth weight and gestational age. Surfactant use was not routine but was administered for evidence of surfactant deficiency such as history of prematurity with typical radiological findings consistent with surfactant deficiency.
All infants received echocardiographic evaluation for congenital heart disease, as well as estimation of pulmonary artery pressure based on tricuspid jet and direction of shunts. Systolic pulmonary artery pressure (SPAP) was estimated from Doppler echocardiography (Toshiba, model SSH-140A) using the equation:
SPAP = 4 X (tricuspid regurgitation velocity)’ + CVP
Central venous pressure (CVP) was measured through an umbilical vein catheter positioned in the right atrium or assumed to be 5 to 6 cm Hz0 when a direct CVP measurement was not possible. Surgery was delayed until there was hemodynamic stability, an acceptable pa02 generally greater than 60 mm Hg, correction of metabolic acidosis, and echocardiographic evidence of decreasing pulmonary artery pressure.i8 The ratio of the peak pulmonary artery to systemic aortic pressure (p/s ratio) was calculated preoperatively. A p/s ratio of 0.75 or greater was interpreted as reflective of pulmonary artery hypertension.t9
Inhaled nitric oxide (Medical Grade Nitric Oxide, 780; Scott Specialty Gases, Plumsteadville, PA) was administered at 20 parts per million when there was refractory hypoxemia and pulmonary hyperten- sion to maximal support with HFOV and conventional measures. The infant was referred for ECMO if there was cardiovascular instability or refractory hypoxemia.
The neonatal and surgical teams jointly reviewed the patient to determine the optimal time far surgical intervention based on a stable blood pressure and heart rate, adequate peripheral perfusion. acceptable blood gases, adequate lung expansion on chest x-ray, and evidence of a fall in pulmonary artery pressure.
Data retrieval included place of birth, prenatal diagnosis, gestational age; birth weight, apgar scores, gender, and associated congenital anomalies. Preoperative respiratory data included age at intubation, method of ventilation, mean airway pressure, age when HFOV was instituted, best Paz and Pcoz, alveolar arterial difference (AaDO?), and oxygenation index (01). The use of surfactant and nitric oxide were recorded. The side of CDH, type of repair, and location at which the surgery was performed were recorded. The time of extubation and chronic oxygen dependency was reviewed. Mortality is described for the entire group. We did not think that a historical control was an appropriate cohort because of extreme differences in the clinical management of CDH.
RESULTS
The charts of 24 patients were reviewed. Two patients were excluded from the study; one patient with a prenatal diagnosis of CDH was referred to an outside facility for consideration of fetal surgery, the second patient had the CDH repair performed at another institution 2 weeks before transfer to our institution. Twenty-two patients were included in this study: 12 girls and 10 boys. Eight of 22 (36%) infants were inborn. Nine (41%) had a prenatal diagnosis. Mean gestational age was 40 weeks (range, 29 to 42 weeks). Median birth weight was 3,079 g (range, 1,205 to 4,337 g).
Table 1 lists the demographics of these patients. Fifteen infants survived without ECMO (group A). Four patients received ECMO (group B). Four infants died
1012 REYES ET AL
Table 1. Demographics, 1993-1996
GA (wk)
BW (kg)
Prenatal Diagnosis
Apw (I mid
Awar (5 min)
A 39 3.1 33% 8 9 n= 15 (30-42) (1.5-4.0) (d-9) (5-9)
B 39.5 3.3 50% 3 5 n=4 (38-41) (3.0-4.3) (O-5) (I-9)
C 40 2.8 75% 3.5 7.5 n=4 (29-40) (I .2-4.3) (l-6) P-9)
NOTE. Groups identified as A, non-ECMO survivors; B, ECMO; C,
non-survivors. Abbreviations: GA, gestational age; SW, birth weight.
(group C). An ECMO patient who died is included in groups B and C. We wanted to review the data of all ECMO patients and deaths separately.
The median gestational age and birth weight of the three groups were similar. The survivors that did not require ECMO had a prenatal diagnosis in 33%. ECMO patients and nonsurvivors had a prenatal diagnosis in 50% and 75%, respectively. The apgar scores of the ECMO patients and nonsurvivors were lower than the survivors, demonstrating sicker patients at birth in the former two groups. Six of the eight inborn infants had a prenatal diagnosis of CDH, and six survived. Three of the outbom infants had a prenatal diagnosis, and two died. Infants with a prenatal diagnosis had a better survival if they were born at our tertiary neonatal center.
All eight inborn infants received intubation immedi- ately after delivery for respiratory distress and were placed on HFOV. Twelve of the 14 infants transferred from another hospital received intubation before arrival. Ten of these infants were placed on HFOV at a mean age of 3 hours. One infant received HFOV before arrival. Of the four infants that did not receive HFOV, three were not as sick as demonstrated by low oxygen requirement (Fro, < 0.5) and minimal support with conventional mechanical ventilation (mean airway pressure < 6 to 7 cm H20). The fourth infant with a two-chamber heart and bilateral CDH died after 4 hours of manual ventilation.
Three patients received conventional mechanical venti- lation (CMV), 18 received HFOV, and one underwent manual ventilation. All three CMV patients and 14 of 18 HFOV patients survived. We did not make a comparison between the CMV and HFOV patients because a compari- son between CMV and HFOV during the care of these patients was not intended. The CMV patients were not placed on HFOV by virtue of their stable course. There was a bias for placement of sick infants on HFOV based on previous experience, and these patients were self- selected for treatment with HFOV.
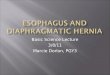
The indices of severity of illness for the three groups (survivors, ECMO and nonsurvivors) are listed in Fig 2. The median preoperative AaDO? for three groups were similar. The median 01 was higher in ECMO and
700
600
500
400
300
200
100
0 A B C
n=15 n=4 n=4
Fig 2. Median 01 and AaDO* in the first 24 hours of life. (A) Non-ECMO survivors, (6) ECMO, (C) nonsurvivors.
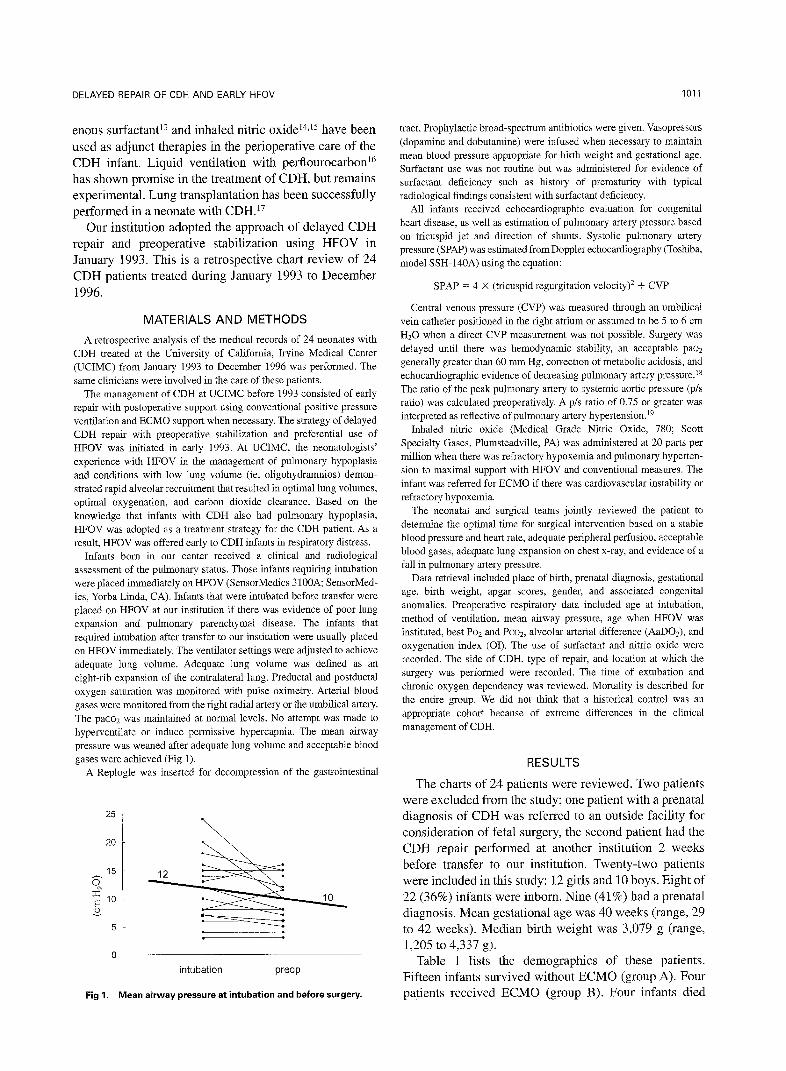
nonsurvivor group. The best PO? in the first 24 hours of life (pre or postductal) was substantially lower in the ECMO patients and nonsurvivors. (Fig 3) These data predictably confirm that ECMO patients and nonsurvi- vors were sicker.
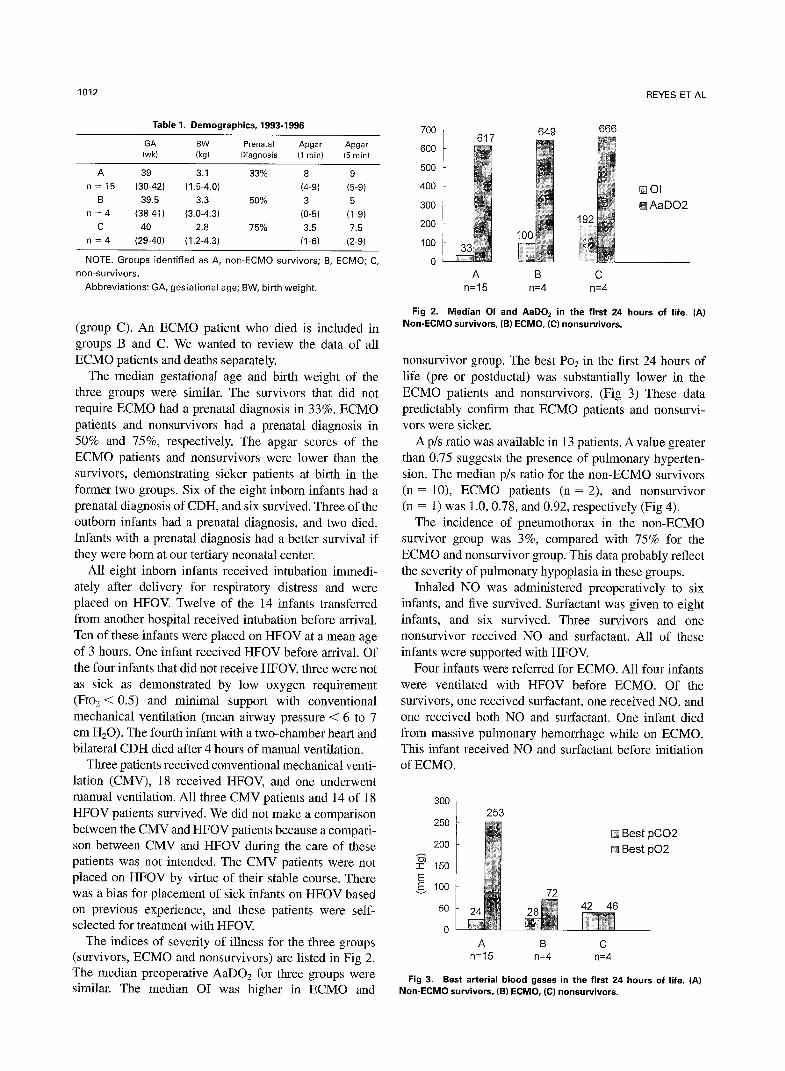
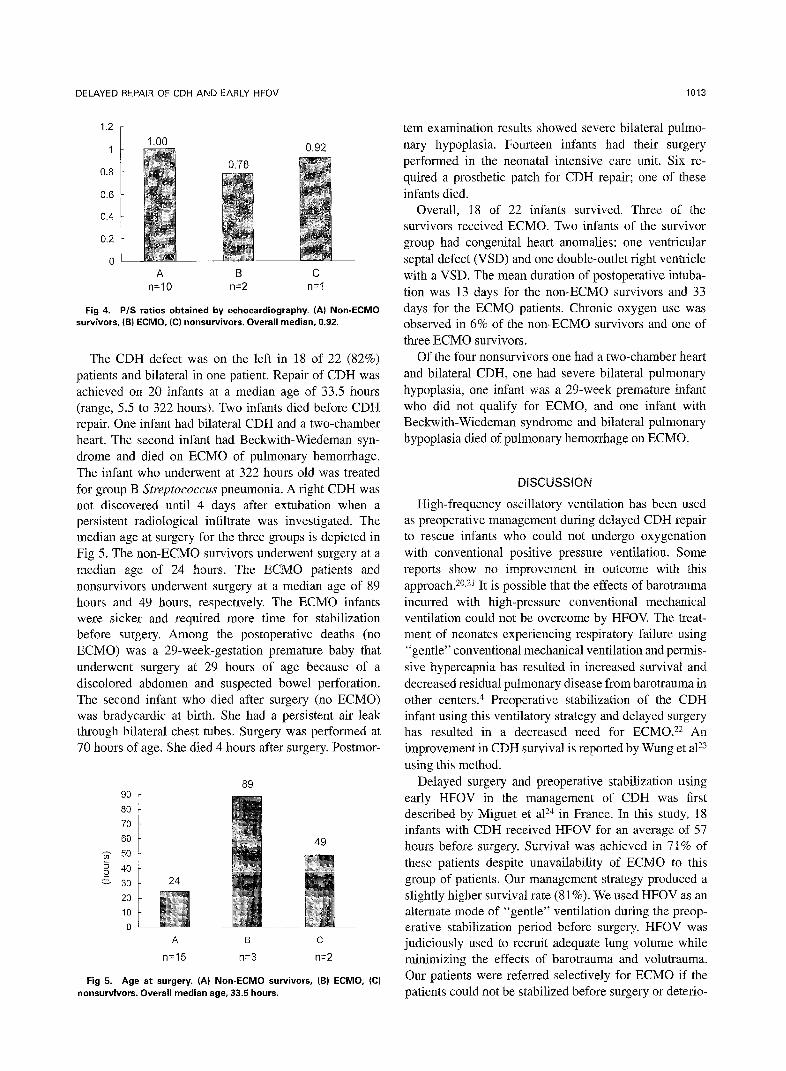
A p/s ratio was available in 13 patients. A value greater than 0.75 suggests the presence of pulmonary hyperten- sion. The median p/s ratio for the non-ECMO survivors (n = lo), ECMO patients (n = 2), and nonsurvivor (n = 1) was 1.0,0.78, and 0.92, respectively (Fig 4).
The incidence of pneumothorax in the non-ECMO survivor group was 3%, compared with 75% for the ECMO and nonsurvivor group. This data probably reflect the severity of pulmonary hypoplasia in these groups.
Inhaled NO was administered preoperatively to six infants, and five survived. Surfactant was given to eight infants, and six survived. Three survivors and one nonsurvivor received NO and surfactant. All of these infants were supported with HFOV.
Four infants were referred for ECMO. All four infants were ventilated with HFOV before ECMO. Of the survivors, one received surfactant, one received NO, and one received both NO and surfactant. One infant died from massive pulmonary hemorrhage while on ECMO. This infant received NO and surfactant before initiation of ECMO.
250
200
s I 150
E 100
50
0
q Best pCO2
Best pO2
42 46
A B C n=15 n=4 rl=4
Fig 3. Best arterial blood gases in the first 24 hours of life. (A) Non-ECMO survivors, (Bl ECMO, (C) nonsurvivors.
DELAYED REPAIR OF CDH AND EARLY HFOV 1013
1.2
1 0.92
0.8
0.6
0.4
0.2
0 A B C
n=lO n=2 n=l
Fig 4. P/S ratios obtained by echocardiography. (A) Non-ECMO survivors, (B1 ECMO, ICI nonsurvivors. Overall median, 0.92.
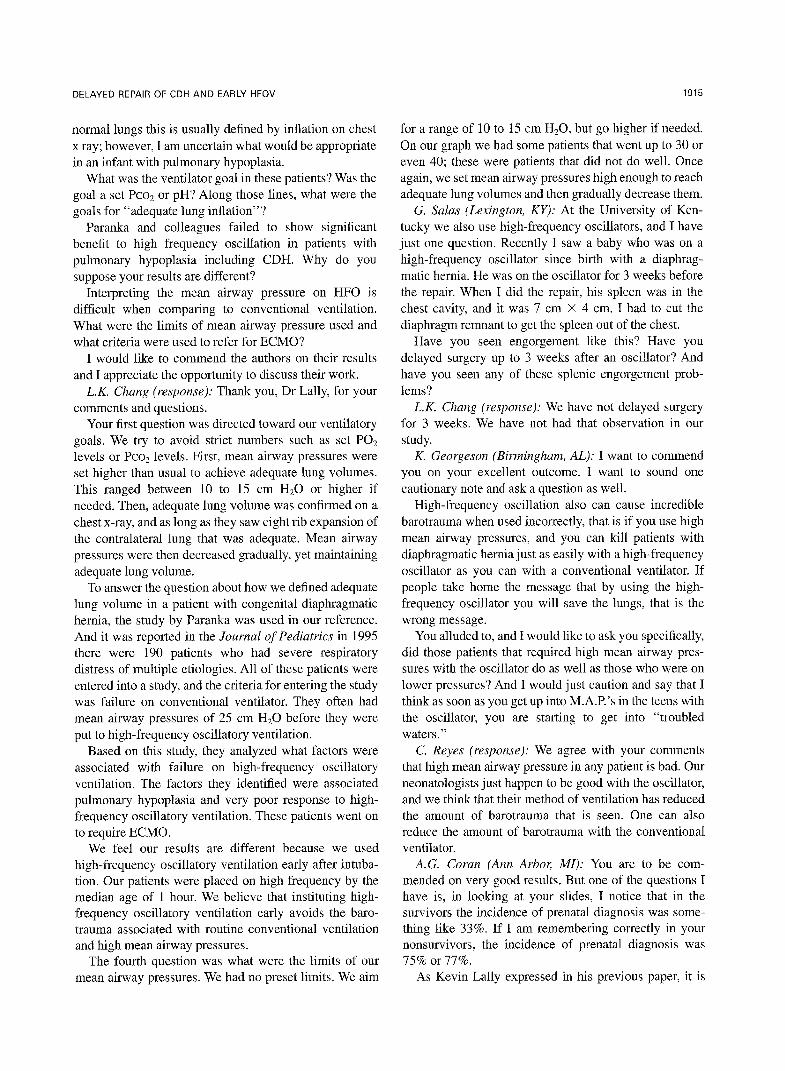
The CDH defect was on the left in 18 of 22 (82%) patients and bilateral in one patient. Repair of CDH was achieved on 20 infants at a median age of 33.5 hours (range, 5.5 to 322 hours). Two infants died before CDH repair. One infant had bilateral CDH and a two-chamber heart. The second infant had Beckwith-Wiedeman syn- drome and died on ECMO of pulmonary hemorrhage. The infant who underwent at 322 hours old was treated for group B Stveptococc~s pneumonia. A right CDH was not discovered until 4 days after extubation when a persistent radiological infiltrate was investigated. The median age at surgery for the three groups is depicted in Fig 5. The non-ECMO survivors underwent surgery at a median age of 24 hours. The ECMO patients and nonsurvivors underwent surgery at a median age of 89 hours and 49 hours, respectively. The ECMO infants were sicker and required more time for stabilization before surgery. Among the postoperative deaths (no ECMO) was a 29-week-gestation premature baby that underwent surgery at 29 hours of age because of a discolored abdomen and suspected bowel perforation. The second infant who died after surgery (no ECMO) was bradycardic at birth. She had a persistent air leak through bilateral chest tubes. Surgery was performed at 70 hours of age. She died 4 hours after surgery. Postmor-
89 90
80
70
60
s 50
2 40
5 30
20
10
0
A 8 C
n=l!i n=3 n=2
Fig 5. Age at surgery. (A) Non-ECMO survivors, (B) ECMO, (C) nonsurvivors. Overall median age, 33.5 hours.
tern examination results showed severe bilateral pulmo- nary hypoplasia. Fourteen infants had their surgery performed in the neonatal intensive care unit. Six re- quired a prosthetic patch for CDH repair; one of these infants died.
Overall, 18 of 22 infants survived. Three of the survivors received ECMO. Two infants of the survivor group had congenital heart anomalies: one ventricular septal defect (VSD) and one double-outlet right ventricle with a VSD. The mean duration of postoperative intuba- tion was 13 days for the non-ECMO survivors and 33 days for the ECMO patients. Chronic oxygen use was observed in 6% of the non-ECMO survivors and one of three ECMO survivors.
Of the four nonsurvivors one had a two-chamber heart and bilateral CDH, one had severe bilateral pulmonary hypoplasia, one infant was a 29-week premature infant who did not qualify for ECMO, and one infant with Beckwith-Wiedeman syndrome and bilateral pulmonary hypoplasia died of pulmonary hemorrhage on ECMO.
DISCUSSION
High-frequency oscillatory ventilation has been used as preoperative management during delayed CDH repair to rescue infants who could not undergo oxygenation with conventional positive pressure ventilation. Some reports show no improvement in outcome with this approach. 20,21 It is possible that the effects of barotrauma incurred with high-pressure conventional mechanical ventilation could not be overcome by HFOV The treat- ment of neonates experiencing respiratory failure using “gentle” conventional mechanical ventilation and permis- sive hypercapnia has resulted in increased survival and decreased residual pulmonary disease from barotrauma in other centers4 Preoperative stabilization of the CDH infant using this ventilatory strategy and delayed surgery has resulted in a decreased need for ECM0.22 An improvement in CDH survival is reported by Wung et al” using this method.
Delayed surgery and preoperative stabilization using early HFOV in the management of CDH was first described by Miguet et a124 in France. In this study, 18 infants with CDH received HFOV for an average of 57 hours before surgery. Survival was achieved in 71% of these patients despite unavailability of ECMO to this group of patients. Our management strategy produced a slightly higher survival rate (8 1%). We used HFOV as an alternate mode of “gentle” ventilation during the preop- erative stabilization period before surgery. HFOV was judiciously used to recruit adequate lung volume while minimizing the effects of barotrauma and volutrauma. Our patients were referred selectively for ECMO if the patients could not be stabilized before surgery or deterio-

1014 REYES ET AL
rated after surgery. We feel that some infants with prevention of barotrauma using either conventional me- refractory pulmonary artery hypertension can be saved chanical ventilation or HFOV during the preoperative with ECMO after an adequate trial of HFOV and inhaled stabilization period.23,24 Our results suggest that HFOV is NO. an alternative and safe ventilatory strategy that can be
Some centers have reported improved survival with judiciously used to support CDH infants during preopera- delayed repair of CDH with particular attention to tive stabilization and delayed surgical repair.
REFERENCES
1. Peckman GJ, Fox WW: Physiologic factors affecting pulmonary artery pressure in infants with persistent pulmonary hypertension. .I Pediatr 93:1005-1010, 1978
2. Bartlett RH, Gazzaniga AB, Jeffries R, et al: Extracorporeal membrane oxygenation (ECMO) cardiopulmonary support in infancy. Trans ASAIO 22:80-88, 1976
3. Kolobow T, Moretti MP, Fumagalli R, et al: Severe impairment of lung function induced by high peak airway pressure during mechanical ventilation. Am Rev Respir Dis 135:312-315, 1987
4. Wung J-T, James LS, Kilchevsky E, et al: Management of infants with severe respiratory failure and persistence of the fetal circulation without hyperventilation. Pediatrics 76488-494, 1985
5. Heijman K, Sjostrand U: Treatment of the respiratory distress syndrome: Apreliminary report. Opusc Med 19:235-239,1974
6. Bland RD, Kim MH, Light MJ, et al: High-frequency mechanical ventilation in severe hyaline membrane disease: an alternative treat- ment? Crit Care Med 8:275-280, 1980
7. Kinsella JP, Neish SR, Shaffer E, et al: Inhaled nitric oxide in persistent pulmonary hypertension. Lancet 340:818-820, 1992
8. Gross RE: Congenital hernia of the diaphragm. Am J Dis Child 71579, 1946
9. Stolar CJH, Dillon PW, Reyes C: Selective use of extracorporeal membrane oxygenation in the management of congenital diaphragmatic hernia. J Pediatr Surg 23:207-211, 1988
10. Wilson JM, Lund DP, Lillehei CW, et al: Delayed surgery and preoperative ECMO does not improve survival in high-risk congenital diaphragmatic hernia. J Pediatr Surg 27:368-372, 1992
11. Cartlidge PHT, Mann NP, Kapila L: Preoperative stabilization in congenital diaphragmatic hernia. Arch Dis Child 61:1226-1228, 1986
12. Harrison MR, Langer JC, Adzick NS, et al: Correction of diaphragmatic hernia in utero. V. Initial clinical experience. J Pediatr Surg 20:673, 1990
13. Glick PL, Leach CL, Besner GE, et al: Pathophysiology of congenital diaphragmatic hernia. III: Exogenous surfactant therapy for the high-risk neohate with CDH. J Pediatr Surg 27:866-869, 1994
14. Karamanoukian HL, Glick PL, Zayeh M, et al: Inhaled nitric oxide in infants referred for extracorporeal membrane oxygenation: Dose response. J Pediatr 124:302-308, 1994
15. Shah N, Jacob T, Exler R, et al: Inhaled nitric oxide in congenital diaphragmatic hernia. J Pediatr Surg 29:1010-1014, 1994
16. Pranikoff T, Gauger PG, Hirsch1 RB: Partial liquid ventilation in newborn patients with congenital diaphragmatic hernia. J Pediatr Surg 31:613-618, 1996
17. Van Meurs KP, Rhine WD, Benitz WE, et al: Lobar lung transplantation as a treatment for congenital diaphragmatic hernia. J Pediatr Surg 29:1557-1560, 1994
18. Haugen SE, Linker D, Eik-Nes S, et al: Congenital diaphrag- matic hernia: Determination of the optimal time for operation by echocardiographic monitoring of the pulmonary artery pressure. J Pediatr Surg 26:560-562, 1991
19. Ochikubo CG, Waffarn F, Turbow R, et al: Echocardiographic evidence of improved hemodynamics during inhaled nitric oxide therapy for persistent pulmonary hypertension of the newborn. Pediatr Cardiol 18:282-287, 1997
20. Paranka MS. Clark RHC, Yoder BA, et al: Predictors of failure of high frequency ventilation in term infants with severe respiratory failure. Pediatrics 95:400-404, 1995
21. Azarow K, Messineo A, Pearl R, et al: Congenital diaphragmatic hernia-A tale of two cities: The Toronto experience. J Pediatr Surg 32:395-400, 1997
22. Wilson JM, Lund DP, Lillihei CW, et al: Congenital diaphrag- matic hernia-A tale of two cities: The Boston experience. J Pediatr Surg 32:401-405, 1997
23. Wung JT. Sahni ST, Lipsitz ME, et al: Congenital diaphragmatic hernia: Survival treated with very delayed surgery, spontaneous respira- tion. and no chest tube. J Pediatr Surg 30:406-409, 1995
24. Miguet D, Olivier OC, Lapillonne A, et al: Preoperative Stabili- zation using high-frequency ventilation in the management of congeni- tal diaphragmatic hernia. Crit Care Med 22:S77-S82, 1994
Discussion
K.P. Ldly (Houston, TX): The authors present a series same team treated the patients in this report but not in an of patients with an excellent outcome over a relatively identical fashion. Some received stufactant, some inhaled short period. Although they show that HFOV can be used NO, and some patients had neither. It is possible that safely in infants with CDH, they do not present compel- these may have had some effect on outcome. Hyperventi- ling data to support a broad application of high-frequency lation becomes a commonly used strategy in the treat- oscillation as the primary ventilator strategy for patients ment of these patients, but general interest in high levels with CDH. Interpreting this series does highlight some of of support to achieve an arbitrary Pco? is clearly declin- the problems in CDH today as we have discussed. ing.
Because of the heterogeneity of this disease, there have The authors adjusted the ventilator settings to achieve been several other reports in the literature with superb an adequate lung volume. A solid definition of adequate results that were not maintained over the long term. The lung volume is problematic on HFO. In patients with two
DELAYED REPAIR OF CDH AND EARLY HFOV 1015
normal lungs this is usually defined by inflation on chest x ray; however, I am uncertain what would be appropriate in an infant with pulmonary hypoplasia.
What was the ventilator goal in these patients? Was the goal a set PCO, or pH? Along those lines, what were the goals for “adequate lung inflation”?
Paranka and colleagues failed to show significant benefit to high frequency oscillation in patients with pulmonary hypoplasia including CDH. Why do you suppose your results are different?
Interpreting the mean airway pressure on HFO is difficult when comparing to conventional ventilation. What were the limits of mean airway pressure used and what criteria were used to refer for ECMO?
I would like to commend the authors on their results and I appreciate the opportunity to discuss their work.
L.K. Chang (response): Thank you, Dr Lally, for your comments and questions.
Your first question was directed toward our ventilatory goals. We try to avoid strict numbers such as set POZ levels or Pco, levels. First, mean airway pressures were set higher than usual to achieve adequate lung volumes. This ranged between 10 to 15 cm HZ0 or higher if needed. Then, adequate lung volume was confirmed on a chest x-ray, and as long as they saw eight rib expansion of the contralateral lung that was adequate. Mean airway pressures were then decreased gradually, yet maintaining adequate lung volume.
To answer the question about how we defined adequate lung volume in a patient with congenital diaphragmatic hernia, the study by Paranka was used in our reference. And it was reported in the Journal of Pediatrics in 1995 there were 190 patients who had severe respiratory distress of multiple etiologies. All of these patients were entered into a study, and the criteria for entering the study was failure on conventional ventilator. They often had mean airway pressures of 25 cm Hz0 before they were put to high-frequency oscillatory ventilation.
Based on this study, they analyzed what factors were associated with failure on high-frequency oscillatory ventilation. The factors they identified were associated pulmonary hypoplasia and very poor response to high- frequency oscillatory ventilation. These patients went on to require ECMO.
We feel our results are different because we used high-frequency oscillatory ventilation early after intuba- tion. Our patients were placed on high frequency by the median age of 1 hour. We believe that instituting high- frequency oscillatory ventilation early avoids the baro- trauma associated with routine conventional ventilation and high mean airway pressures.
The fourth question was what were the limits of our mean airway pressures. We had no preset limits. We aim
for a range of 10 to 15 cm HzO, but go higher if needed. On our graph we had some patients that went up to 30 or even 40; these were patients that did not do well. Once again, we set mean airway pressures high enough to reach adequate lung volumes and then gradually decrease them.
G. Salas (Lexington, KY): At the University of Ken- tucky we also use high-frequency oscillators, and I have just one question. Recently I saw a baby who was on a high-frequency oscillator since birth with a diaphrag- matic hernia. He was on the oscillator for 3 weeks before the repair. When I did the repair, his spleen was in the chest cavity, and it was 7 cm X 4 cm, I had to cut the diaphragm remnant to get the spleen out of the chest.
Have you seen engorgement like this? Have you delayed surgery up to 3 weeks after an oscillator? And have you seen any of these splenic engorgement prob- lems?
L.K. Chang (response): We have not delayed surgery for 3 weeks. We have not had that observation in our study.
K. Georgeson (Birmingham, AL): I want to commend you on your excellent outcome. I want to sound one cautionary note and ask a question as well.
High-frequency oscillation also can cause incredible barotrauma when used incorrectly, that is if you use high mean airway pressures, and you can kill patients with diaphragmatic hernia just as easily with a high-frequency oscillator as you can with a conventional ventilator. If people take home the message that by using the high- frequency oscillator you will save the lungs, that is the wrong message.
You alluded to, and I would like to ask you specifically, did those patients that required high mean airway pres- sures with the oscillator do as well as those who were on lower pressures? And I would just caution and say that I think as soon as you get up into M.A.I?‘s in the teens with the oscillator, you are starting to get into “troubled waters.”
C. Reyes (response): We agree with your comments that high mean airway pressure in any patient is bad. Our neonatologists just happen to be good with the oscillator, and we think that their method of ventilation has reduced the amount of barotrauma that is seen. One can also reduce the amount of barotrauma with the conventional ventilator.
A.G. Coran (Ann Arbor; MI): You are to be com- mended on very good results. But one of the questions I have is, in looking at your slides, I notice that in the survivors the incidence of prenatal diagnosis was some- thing like 33%. If I am remembering correctly in your nonsurvivors, the incidence of prenatal diagnosis was 75% or 77%.
As Kevin Lally expressed in his previous paper, it is

1016 REYES ET AL
very difficult for us to stratify severity of illness in this lesion in comparing one series with another, but one of the things that has been somewhat correlated with the severity of illness is the incidence of prenatal diagnosis. So I just raise the point that very good survival may be that these babies were just not as sick because so many of them did not receive diagnosis prenatally.
L.K. Chang (response): We showed our AA gradients for all three groups were over 610, which for some centers qualifies for ECMO criteria. The best PAo,s, and the best PCO~S were also indicative of the high severity of illness in this index, as well as the pulmonary artery pressure, many of which approached an index of 1. I appreciate your comments though, Dr Coran.