Embed Size (px)
Citation preview

©2019 MFMER | slide-1
Delirium Management: Are You Pro- or “Anti-” Psychotic?
Abby Hendricks, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds March 12, 2019

©2019 MFMER | slide-2
Objectives
• Identify risk factors for the development of delirium
• Discuss literature assessing the use of antipsychotics for delirium in various patient populations
• Describe treatment options for managing delirious patients

©2019 MFMER | slide-3
What is Delirium?
• Disturbance in attention and awareness
• Develops acutely
• Fluctuating severity
Assessment Scales
CAM-ICU
ICDSC
DRS-R-98
MDAS
NuDESC
Marcantonio ER. NEJM 2017;377:1456-66.
Attard A et al. CNS Drugs 2008;22(8):631-644.
Kalabalik J. JPP 2013;XX:1-13.

©2019 MFMER | slide-4
Classification
Hypoactive Hyperactive
M
I
X
E
D
Marcantonio ER. NEJM 2017;377:1456-66.
Attard A et al. CNS Drugs 2008;22(8):631-644.
Kalabalik J. JPP 2013;XX:1-13.

©2019 MFMER | slide-5
Predisposing Risk Factors
70 YOM
PMH: HTN, DM, HFrEF,
dementia, alcohol abuse
70 YOM
PMH: HTN, DM, HFrEF,
dementia, alcohol abuse
135
3.8
103
25
37
1.5 126
135
3.8
103
25
37
1.5 126
Marcantonio ER. NEJM 2017;377:1456-66.
Attard A et al. CNS Drugs 2008;22(8):631-644.
Kalabalik J. JPP 2013;XX:1-13.

©2019 MFMER | slide-6
Precipitating Risk Factors
Now s/p CABG x 3 following STEMI
Evidence of surgical site infection
Medications
Pain score: 9/10
IV
Last BM: 3 d ago
UOP
Zzzz.. Now s/p CABG x 3 following STEMI
Evidence of surgical site infection
130
3.3
103
25
34
1.5 126
130
3.3
103
25
34
1.5 126
7.6
29 15 250
7.6
29 15 250
Pain score: 9/10
Last BM: 3 d ago
Medications
Marcantonio ER. NEJM 2017;377:1456-66.
Attard A et al. CNS Drugs 2008;22(8):631-644.
Kalabalik J. JPP 2013;XX:1-13.

©2019 MFMER | slide-7
Contributing Medications
Benzodiazepines Opioid analgesics Nonbenzodiazepine sedative hypnotics
Antihistamines Anticholinergics Anticonvulsants
Tricyclic antidepressants
Antiparkinsonian agents
Barbiturates
Marcantonio ER. NEJM 2017;377:1456-66.

©2019 MFMER | slide-8
Audience Response Question #1
• JB is a 68 YOM admitted to the MICU for HAP
• PMH:
• CAD
• HTN
• Depression
135
3.2
103
25
37
1.5 126
Medications: • Aspirin 81 mg daily
• Lisinopril 20 mg daily
• Levofloxacin 750 mg daily
• Oxycodone 10 mg q4h prn

©2019 MFMER | slide-9
Audience Response Question #1
• Which of the following is a modifiable risk factor for the development of delirium?
• Age 68 years
• Oxycodone 10 mg q4h prn
• HTN
• Aspirin 81 mg daily

©2019 MFMER | slide-10
Management of Delirium
Provide supportive
care
Manage symptoms
Address modifiable risk factors
Marcantonio ER. NEJM 2017;377:1456-66.
Throm RP et al. CCJM 2017;84(8):616-622.

©2019 MFMER | slide-11
Antipsychotics in ICU Delirium
2019
Devlin et al. Girard et al.
2013 SCCM Guideline
AAPs may reduce
duration of delirium
2010
2013
Page et al.
2018 SCCM Guideline
Suggest not routinely
using HAL or AAP to
treat delirium
2018
Girard et al.
2002 SCCM Guideline
HAL is preferred agent for
treatment of delirium in
critically ill patients
2004
Skrobik et al.
HAL – haloperidol, OLZ – olanzapine, QTP – quetiapine, ZPR – ziprasidone, PBO – placebo, AAP – atypical antipsychotic
Jacobi J et al. Crit Care Med 2002;30(1):119-41
Barr J et al. Crit Care Med 2013;41(1):263-306.
Devlin JW et al. Crit Care Med 2018;46(9):e825-e873.
Skrobik et al. Intensive Care Med 2004;30:444-9.
Devlin et al. Crit Care Med 2010;38:419-27.
Girard et al. Crit Care Med 2010;38:428-37.
Page et al. Lancet Resp Med 2013;1:515-23.

©2019 MFMER | slide-12
Haloperidol and Ziprasidone for Treatment of Delirium in Critical Illness
Girard et al. NEJM 2018; 379: 2506-2516
©2019 MFMER | slide-13
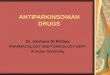
Girard et al. 2018
N = 566
• ≥ 18 y.o.
• Medical/surgical ICU
• Ventilation, vasopressors,
or IABP
• Delirium (CAM-ICU)
Haloperidol 2.5 mg IV q12h
Max:10 mg/dose or 20 mg/d
Ziprasidone 5 mg IV q12h
Max: 20 mg/dose or 40 mg/d
Placebo
R
A
N
D
O
M
I
Z
E
1:1:1
Assessed
q12h using
CAM-ICU
• Positive for delirium, not at max dose = 2 x dose
• 2 consecutive assessments without delirium = ½ dose
• 4 consecutive assessments without delirium = dose held
IABP – intra-aortic balloon pump
Girard et al. NEJM 2018; 379: 2506-2516.

©2019 MFMER | slide-14
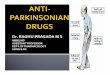
Girard et al. 2018
0 2 4 6 8 10 12 14
ZPR
HAL
PBO
Adjusted median days (95% CI)
8.7 days
7.9 days
8.5 days
Primary
Efficacy
Days alive without delirium or coma during
14 day follow-up
P = 0.26
for overall effect
across trial groups
HAL – haloperidol, ZPR – ziprasidone, PBO – placebo
Girard et al. NEJM 2018; 379: 2506-2516.
©2019 MFMER | slide-15
Girard et al. 2018
• Secondary Efficacy
• Safety • Sedation most common ADE in all groups • QTc prolongation more common with ziprasidone
Endpoint Placebo Haloperidol Ziprasidone
Time to liberation from
ventilation, days 3 2 3
ICU discharge, days 5 5 6
Death at 30 days, n (%) 50 (27) 50 (26) 53 (28)
ADE – adverse drug effect
Girard et al. NEJM 2018; 379: 2506-2516.

©2019 MFMER | slide-16
Girard et al. 2018
• Limitations
• Composite endpoint
• Suboptimal ziprasidone dosing
• Haloperidol 11 mg IV = ziprasidone 660 mg PO
• Ziprasidone IV formulation not commercially available
• Conclusions
• No evidence for benefit of antipsychotics in critically ill patients with hypoactive delirium
Girard et al. NEJM 2018; 379: 2506-2516.

©2019 MFMER | slide-17
Audience Response Question #2
• On day 3 of hospitalization JB becomes confused and withdrawn. Nursing staff notes he is no longer following commands or cooperating with staff members.

©2019 MFMER | slide-18
Audience Response Question #2
• Based on results from the Girard et al trial, which of the following is the most appropriate management strategy:
• A: Initiate haloperidol 2.5 mg IV q12h
• B: Address modifiable contributors
• C: Initiate ziprasidone 20 mg IV q12h

©2019 MFMER | slide-19
Antipsychotics in Non-ICU Delirium
2019
2016
Grover et al.
2013
Maneeton et al.
2011
Grover et al.
2010
Tahir et al.
2006
Hu et al.
2017
Agar et al.
2004
Han & Kim
et al.
HAL – haloperidol, OLZ – olanzapine, QTP – quetiapine, ZPR – ziprasidone, PBO – placebo, AAP – atypical antipsychotic
Han et al. Psychosomatics 2004;45(4):297-301.
Hu et al. Chin J Clin Rehabil 2006;10(42):188-90.
Tahir et al. J Psychosom Res 2010;69(5):485-90.
Grover et al. J Psychosom Res 2011;71(4):277-81.
Maneeton et al. J Med Assoc Thai 2007;90(10):2158-63.
Grover et al. World J Psychiatry 2016;6(3):365-71.
Agar et al. JAMA 2017; 177(1):34-42

©2019 MFMER | slide-20
Efficacy of Oral Risperidone, Haloperidol, or Placebo for Symptoms of Delirium Among Patients in Palliative Care: A Randomized Clinical Trial
Agar et al. JAMA 2017; 177(1):34-42

©2019 MFMER | slide-21
Agar et al. 2017
N = 247
• ≥ 18 y.o.
• Hospice or palliative care
• Delirium diagnosed via DSM-
IV, MDAS score ≥ 7, with
target symptoms associated
with distress (NuDESC ≥ 1)
Risperidone
0.5 mg PO q12h
Haloperidol
0.5 mg PO q12h
Placebo
1:1:1
R
A
N
D
O
M
I
Z
E
Assessed
q8h using
NuDESC
score
• NuDESC score ≥ 1 = ↑ dose (max 4 mg/day)
• Adverse effects, MDAS score < 7, NuDESC < 1 = ↓ dose
>65 yo = ½ dose
MDAS – Memorial delirium assessment scale, NuDESC – Nursing delirium screening scale
Agar et al. JAMA 2017; 177(1):34-42

©2019 MFMER | slide-22
Agar et al. 2017
0 1 2 3
Time (days)
NuD
ES
C S
core
4
3
2
1
0
Placebo
Risperidone
Haloperidol
Agent NuDESC Scores
Study End Daily
Risperidone
(v. placebo)
+0.48 Units
(p=0.02)
+0.24 Units
(p<0.001)
Haloperidol
(v. placebo)
+0.24 Units
(p=0.009)
+0.21 Units
(p=0.002)
Primary
Efficacy
Improvement in mean NuDESC score
between baseline and day 3
NuDESC – Nursing delirium screening scale
Agar et al. JAMA 2017; 177(1):34-42

©2019 MFMER | slide-23
Agar et al. 2017
• Midazolam use (any antipsychotic vs. placebo)
• Day 1: 34.7% v 17.3% (p = 0.007)
• Day 2: 33.1% v 16.8% (p = 0.01)
• Day 3: 29.6% v 13.6% (p = 0.02)
Risperidone Haloperidol
Daily MDAS score
EPS
Median Survival
*Compared to placebo
MDAS – Memorial delirium assessment scale, EPS – extrapyramidal symptoms
Agar et al. JAMA 2017; 177(1):34-42

©2019 MFMER | slide-24
Agar et al. 2017
• Limitations
• Symptom and severity based outcomes
• PRN midazolam use
• Low doses?
• Conclusions
• No evidence for benefit of antipsychotics in reducing symptoms of hyperactive/mixed delirium in palliative care patients
• May be harmful?
Agar et al. JAMA 2017; 177(1):34-42

©2019 MFMER | slide-25
Antipsychotics – Yes or No?
X X
? ?
Hypoactive
Hyperactive
ICU Non-ICU

©2019 MFMER | slide-26
Delirium
Address
Modifiable
Risk Factors
Provide
Supportive
Care
Non-pharmacologic
Interventions
Antipsychotics
Alternative
Agents
Non-pharmacologic
Interventions
Antipsychotics
Marcantonio ER. NEJM 2017;377:1456-66.
Throm RP et al. CCJM 2017;84(8):616-622.

©2019 MFMER | slide-27
Non-Pharmacologic Interventions
• Reduce duration of delirium, LOS, and mortality
Cognition/
Orientation
• Cognitive stimulation activities
• Reorient to time, place, and person
Early mobility • Ambulation and active range-of-motion exercises
• Minimize use of physical restraints
Hearing • Encourage use of hearing aids or portable amplifiers
• Special communication techniques as indicated
Vision • Encourage use of eyeglasses and/or magnifying lenses
• Utilize adaptive equipment (i.e. large print books)
Sleep-wake
cycle
• Implement non-pharmacologic nighttime sleep protocol
• Minimize unnecessary awakenings
Hydration/
Feeding
• Encourage fluids
• Monitor dietary intake and provide assistance as needed
Hshieh TT et al. JAMA Intern Med 2015 1;175(4):512–20.
Marcantonio ER. NEJM 2017;377:1456-66.
Kalabalik J. JPP 2013;XX:1-13.

©2019 MFMER | slide-28
Antipsychotic Selection
Agent D2 a1 H1 M1
Haloperidol +++ --- --- ---
Olanzapine ++ + +++ +++
Risperidone +++ ++ + +/-
Quetiapine + + ++ ++
Ziprasidone ++ +/- + ---
Receptor
profile
a1 H1
5-HT2A
M1
D2
Effectiveness Safety
Farah A. Prim Care Companion J Clin Psychiatry 2005;7:268-74.
Marcantonio ER. NEJM 2017;377:1456-66.
Riviere J et al. Psychosomatics 2019;60:18-26.

©2019 MFMER | slide-29
Antipsychotic Selection Agent Dose
Equivalence*
QTc
Prolongation
Comments
Haloperidol 2
IV – High
PO - Low
Only IV option
IV to PO is 1:2
Risperidone
1 Low
EPS > 6 mg
Orthostasis
Olanzapine
5 Low
ODT - must swallow
Avoid IM with IV/IM BZD
Quetiapine
75 Low
Sedation – qHS dosing
Suppository form (MCR)
Ziprasidone 60 High Give PO with food
*PO equivalent doses listed; EPS – extrapyramidal symptoms, BZD - benzodiazepines
Patel MX et al. Schizophrenia Research 2013;149:141-48.
Marcantonio ER. NEJM 2017;377:1456-66.
Throm RP et al. CCJM 2017;84(8):616-622.

©2019 MFMER | slide-30
Audience Response Question #3
• On day 5 of hospitalization JB’s mental status changes and he becomes acutely agitated, starts pulling out his IV lines, and endorses hallucinations.

©2019 MFMER | slide-31
Audience Response Question #3
• Which of the following is associated with the highest risk of QTc prolongation?
• A: Quetiapine
• B: Olanzapine
• C: Risperidone
• D: Ziprasidone

©2019 MFMER | slide-32
Summary
• Recent evidence demonstrates lack of benefit for the use of antipsychotics in hypoactive delirium
• Antipsychotic use may be warranted for acutely agitated delirious patients
• Consider adverse effect profiles and dose equivalence when selecting a regimen
• Non-pharmacologic strategies remain the cornerstone of delirium management

©2019 MFMER | slide-33
Delirium Management: Are You Pro- or “Anti-” Psychotic?
Abby Hendricks, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds March 12, 2019

©2019 MFMER | slide-34
Antipsychotic Dosing (TDD) Agent Schizophrenia
Delirium Suggested
Dosing
Haloperidol 5-20 0.5-10 5-20
Risperidone 4-8 0.25-4 2.5-4
Olanzapine 10-20 1-20 10-20
Quetiapine 400-800 12.5-200 150-400
Ziprasidone 80-160 5-160 80-160
TDD – Total Daily Dose







![Welcome [ce.mayo.edu]€¦ · Web viewMayo Clinic School of Continuous Professional Development 10 th Annual Hospital Medicine for Nurse Practitioners and Physicians Assistants June](https://img.pdfslide.net/doc/110x75/5ecdaff9c36c81086508e443/welcome-cemayoedu-web-view-mayo-clinic-school-of-continuous-professional-development.jpg)




![Welcome [ce.mayo.edu] · Web viewMayo Clinic School of Continuous Professional DevelopmentWednesday, February 7, 2018 6:30 a.m. – 4:00 p.m. Plummer 2-60, 200 1st ST …](https://img.pdfslide.net/doc/110x75/5ecdaff8c36c81086508e442/welcome-cemayoedu-web-view-mayo-clinic-school-of-continuous-professional-developmentwednesday.jpg)