Embed Size (px)
Citation preview
1
DEPARTMENT OF TRANSFUSION MEDICINE
BLOOD TRANSFUSION PRACTICE FOR
RESIDENTS
JAWAHARLAL INSTITUTE OF POSTGRADUATE MEDICAL EDUCATION & RESEARCH
PUDUCHERRY – 605 006
2
INDEX
1. Role of blood transfusion service of JIPMER
2. Blood donation and donor referral
3. Requisition for blood and components
4. Issue of blood and components
5. Administration of blood and components
6. Blood component therapy
7. Neonatal and childhood transfusion
8. Transfusion in special settings
9. Leuco-depleted and Irradiated Blood Components
10. Transfusion reactions
11. Stem cell Transplant and Therapeutic Plasmapheresis
12. Good Blood Management Practice
13. Maximum Surgical Blood Ordering Schedule
14. Biosafety
3
1. Role of Blood Transfusion Service of JIPMER
The blood transfusion service is committed to provide the safe blood to
the patients of this hospital. The main role of the blood bank is to provide safe and
timely blood and blood components to the patients and provide accurate results of
the tests ordered by various departments which can happen with mutual
cooperation and coordination between departments.
The blood bank strives to ensure that there is an adequate inventory of all
blood types and blood components to meet the needs of the patients. The blood
bank does donor selection, blood collection, component preparation, screening for
transfusion – transmitted infections and blood processing. Serologically compatible
blood and components are provided to the patients after pre-transfusion testing as
per the standard protocol. In addition, serological investigations for autoimmune
disorders, hemolytic disease of newborn and transfusion reactions are carried out.
Single Donor Platelets, Therapeutic Leukapheresis and Therapeutic Plasma
Exchange procedures are also available in selected cases. Necessary infrastructure is
being developed to meet the requirement of special blood components such as
peripheral blood stem cell, irradiated components etc.
The blood bank is involved in training of Medical Laboratory Technicians,
Undergraduate Medical students and Residents of Transfusion Medicine and
Pathology.
This informative manual on blood transfusion is designed to disseminate
knowledge about safe blood transfusion practices to the Clinical Residents, Nursing
staff and other Medical Personnel involved in arranging blood or component
transfusion to the patients.
4
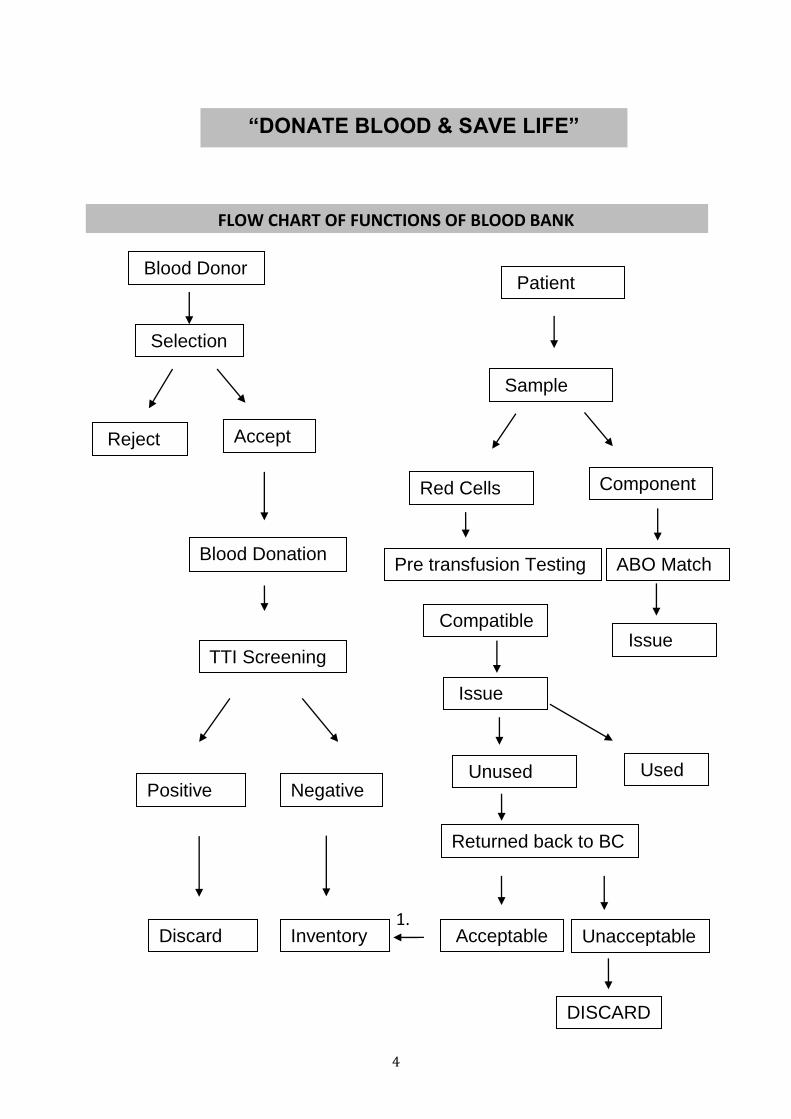
“DONATE BLOOD & SAVE LIFE”
FLOW CHART OF FUNCTIONS OF BLOOD BANK
1.
Blood Donor
Selection
Reject Accept
Blood Donation
TTI Screening
Positive Negative
Discard Inventory
Patient
Sample
Red Cells Component
Pre transfusion Testing ABO Match
Compatible
Used Unused
Issue
Returned back to BC
Acceptable Unacceptable
DISCARD
Issue
5
2. Blood donation and donor referral
All efforts are made to provide Blood and components by the transfusion services to
the patients irrespective of replacement donation.
For planned / elective surgeries, blood donation may be made well in advance, at
least 72 hours prior the surgery. The patient’s relatives should be instructed to
donate required quantity of blood.
Guidelines for referring the donor to Blood bank:
1. Timing of blood donation: 9.00 AM to 4.00 PM from Monday to Friday and 9.00
AM to 12.30 PM on Saturday. Blood donation is closed on Sundays and Gazetted
Holidays.
2. On certain days when voluntary blood donation camps are held (Expected
collection more than 100 units) most of blood bank bleeding section will be
deputed to camp, hence either bleeding at blood bank will be restricted or it may
be closed.
3. Only relatives and friends of the patients who voluntarily agree; and voluntary
donors will be accepted for blood donation. Paid donation is strictly prohibited
and punishable by the law.
4. Certain categories of donors called as Captive or Coerced donors, such as
servants working in a household, subordinates, donors having multiple sex
partners, jail inmates, drug abusers or long term medication ( except few) are not
safe donors and therefore should be discouraged.
5. Before referring the blood donor to the blood bank, ensure that the donor is in
good health, free from chronic ailments, not on medication and in the age group
of 18 to 60 years (Ideally 20-50 years). Minimum weight more than 45 Kgs
(Ideally-50 Kgs.) Donor will be bled only if found fit after thorough questionnaire,
required physical examination with investigations conducted at the blood bank.
Details of donor selection criteria can be obtained from the Blood bank.
6
6. Donors can donate blood irrespective of their ABO/Rh groups. Blood group
specific compatible blood will be provided to the patients. In some cases Group
specific donations are required particularly in Rh Negatives, Bombay, A2, and A2B
etc.
7. When the donors are sent to blood bank for donation, they must be given a
requisition slip containing the name of the patient, hospital number,
Unit/Ward/OPD for whom the donation is to be made and the number of units
to be collected.
8. After blood donation, blood donation slip will be given indicating donation
number which should be retained, in the patient file.
9. This blood donation number is “NON-TRANSFERABLE”.
Referral of Plateletpheresis donors:
1. Single donor apheresis platelets (SDP) are prepared by the use of Cell Separators.
2. While every effort will be made to arrange voluntary donors for plateletpheresis,
however, primary responsibility for arranging suitable donors rests with the
Relatives / Consultant in charge of the case.
3. Timing for Apheresis: Donors should be sent before 10.30 AM for evaluation or
screening with the special request after informing the Blood bank. Apheresis
screening or procedure will not be performed routinely on Sundays and Gazetted
Holidays. If found fit then donor should come on any working day with prior
information (in case of camps it may not be possible) before 11am within 15
days.
4. In case of adverse donor reactions or problem with kit or equipment the
apheresis procedure may have to be abandoned and component may have to be
discarded.
7
Plateletpheresis Donor Screening
Plateletpheresis donors should be ABO and Rh matched and they are pre-
screened for transfusion transmitted infections before the procedure
When donors are referred to the blood bank for evaluation, they should bring a
request containing the name, hospital number, diagnosis, blood group and
platelet count of the patient.
The Resident in charge of Apheresis will draw the blood sample from the donors
for ABO, Rh and TTI screening.
ABO and Rh matched and TTI screened plateletpheresis donors will be kept
reserved for the procedure. Repeat TTI screening is required if the duration
between screening and apheresis procedure is more than 15 days.
It will be the responsibility of clinical service resident to ensure that selected
donors are available at the time of the procedure.
Donor should avoid oily food before the procedure on that day.
Donors apart being fit for whole blood donation should not be on medication
with aspirin, Anti platelet aggregating medication and should have Platelet
counts more than 1.5lakh/cumm with normal complete blood count.
8
3. Requisition for blood and components
1. All blood requisition must have following information, without which requisition
will not be accepted.
Name of the patient & Father’s or Husband’s Name
Hospital Number
Location of patient( ward/ bed/OPD Unit )
Gender
Age
Haemoglobin, other hematological parameters as required for different blood
components.
Name of the Consultant & Signature of Resident In Charge with date
Mobile number of Resident and PABX number of ward. (IMPORTANT)
In case of previous transfusions feedback form with Blood group & Rh type is
mandatory.
2. Check the appropriate box to indicate what type of component and number of
units to be cross-matched.
3. MSBOS given below may be referred for number of blood units required.
4. Provide relevant clinical details, such as diagnosis, indication for transfusion, past
history of transfusion or reactions, any medications, history of hemolytic disease
etc.
5. Check the appropriate box to indicate the priority of the transfusion
requirement.

9
ROUTINE: Blood or component is not required for at least 8 hrs. from the requisition
is received. In this type, every unit of blood is tested for irregular antibodies with
Coomb’s test etc. by standard techniques.
URGENT: Blood or component is not required for at least 1 hour from the time
requisition is received. In this type, only Immediate Spin cross match is done which
does not rule out irregular warm antibodies.
IMMEDIATE: Blood is required in less than 30 minutes from the time sample is
received. In this type no cross matching is performed, only ABO and Rh matched
blood is provided. Therefore, this option should be used with utmost care, as the
ordering physician will be responsible for the adverse effects. This option is rarely
required.
6. The person who draws the sample must affix his/her signature in the label on the
sample. Initials are not acceptable. The person signing is attesting that the
sample has been drawn from the patient by him / her.
7. Although, every blood sample is potentially infectious, special precautions are
taken for HIV, HBsAg, or HCV positive samples. Please indicate in bold letters or
use the sticker “BIO-HAZARD” on the top of the requisition form and sample so
that persons handling the specimen can take additional precautions.
8. Send the request form along with blood sample by ward attendant for cross
matching. Requisitions sent along with relatives or a friend of the patients is not
considered a good laboratory practice and will not be accepted.
10
Guidelines for samples for blood and components:
SAMPLE FOR CROSS MATCH (For Red Cell transfusion only)
2ml EDTA & 5 ml clotted blood sample is required for cross-match of a unit of red
cells in adults. Additional sample is required at 1 ml / additional unit. (e. g. for cross-
match of 6 units of blood 10 ml of sample is required.
Justification for samples is:
i) Forward grouping will be done with EDTA & Reverse grouping and cross
matching with plain sample. It may decrease chances of wrong blood in tube
incidents.
ii) We have to keep pretransfusion samples for 7 days for any transfusion
reaction workup, in that we have to do DCT both on pre transfusion and post
transfusion samples.
SAMPLE FOR BLOOD GROUP ONLY
2 ml EDTA blood sample is required for ABO grouping and Rh typing.
The sample must be received in the blood bank by 12 noon one day before to ensure
availability of blood for routine transfusions. For urgent transfusions, sample must
reach Blood bank at least 2 hour before transfusion. In case of immediate transfusion
of uncross matched blood, sample must reach Blood bank 30 min before transfusion.
SAMPLE FOR FFP, CRYO OR PLATELET TRANSFUSION
For repeat transfusions of these components, there is no need for any blood sample,
provided the blood bank has record of the blood group of the patient or same may
be recorded at ward mentioning previous issue number with date.. For fresh / first
time transfusions, 2 ml EDTA and 3 ml Clotted sample will be required to determine
the blood group.
11
SAMPLE FOR TRANSFUSION IN NEONATES
Serum of the newborn will have ABO antibodies of mother’s origin passively
transferred across the placenta. Therefore, cross matching will be performed using
mother’s sample for neonate till the age of 6 months and blood compatible with
both neonates and mother will be issued. 5 ml of clotted sample from mother and 2
ml EDTA sample from the new born will be required
1. Information required on the sample.
Name of the patient & Father’s or husband’s Name. It should match with the
name on the requisition form.
Hospital number of the patient matching with that on the requisition form.
Name of the test to be performed ( Grouping, cross matching)
Signature of the resident.
Date of collection of sample.
2. Samples from new born should be labeled as “Baby of mother’s name with
husband’s name” and should be labeled with mother’s identification, incase case
sheet is not made for the baby. All labelling should be done at one place not
around the bulb.
Labeling errors
Labeling errors are potentially life threatening and may result in transfusion of
incompatible blood/components.
Significant labeling errors include the following:
Overwriting
Correction not authenticated by signature.
Wrong or no Hospital No on specimen or requisition
Specimen drawn from the wrong patient, this can be avoided by withdrawing
sample into pre labeled tube at the bed side, one sample at a time.
12
Name and / or Hospital number on the specimen not matching with name and /
or Hospital number on requisition.
Note: The specimen and requisition will be discarded by the blood bank if these
types of labeling errors are found. The Resident and / or Nurse will be informed
that a new specimen is required.
3. Minor labeling errors include the following:
Small spelling errors in name
No signature of the resident on the requisition.
In such cases, information will be conveyed by phone and unless the concerned
resident corrects the error, the specimen and requisition will be rejected and
fresh sample will be required.
4. Requisition for Fresh Frozen Plasma
Fresh frozen plasma is issued ABO group specific only. There is no need for cross
match.
The blood bank must have a record of the blood group of the patient on HIS. If
the record is not available as in case of fresh admission, a specimen for ABO
grouping must be sent along with the requisition.
The components are issued in 1 hour or less after the receiving requisition.
FFP thawed for more than 4 hrs. is deficient in labile coagulation factors.
Therefore, this product should not be asked in advance and store in refrigerator
in the ward.
Further details regarding contents, dose and indications for FFP can be found in
Section 5.
NEVER REFREEZE FFP
13
5. Requisition for Cryoprecipitate
Cryoprecipitate is issued irrespective of ABO & Rh of the recipient
Rest all procedures and storage are similar to FFP
6. Requisition for Platelet Concentrate
The blood bank must have a record of ABO group on the HIS before platelets can
be issued.
ABO and Rh matched Platelets are issued as far as possible subject to availability.
There is no need of blood specimen provided the record of group is already done
and available on the HIS.
Platelets are not always available in stock and therefore additional time may
be required for preparation, TTI screening etc.
Since platelets need to be kept on agitator and wards do not have proper storage
for platelets they should not be ordered in advance. Send the requisition 30
minutes before transfusion is planned.
NEVER KEEP PLATELETS IN REFRIGERATOR
Further details regarding contents, dose and indications for platelet transfusion
can be found in Section 5.
Guidelines for requisition of blood and components in special circumstances
1. Non Group Specific transfusion:
While every effort is made to cross match ABO group specific blood to the
patient, non-ABO group specific blood or component may be issued in cases of
emergency due to blood shortages. Contact the blood bank in case any
clarification is needed.
14
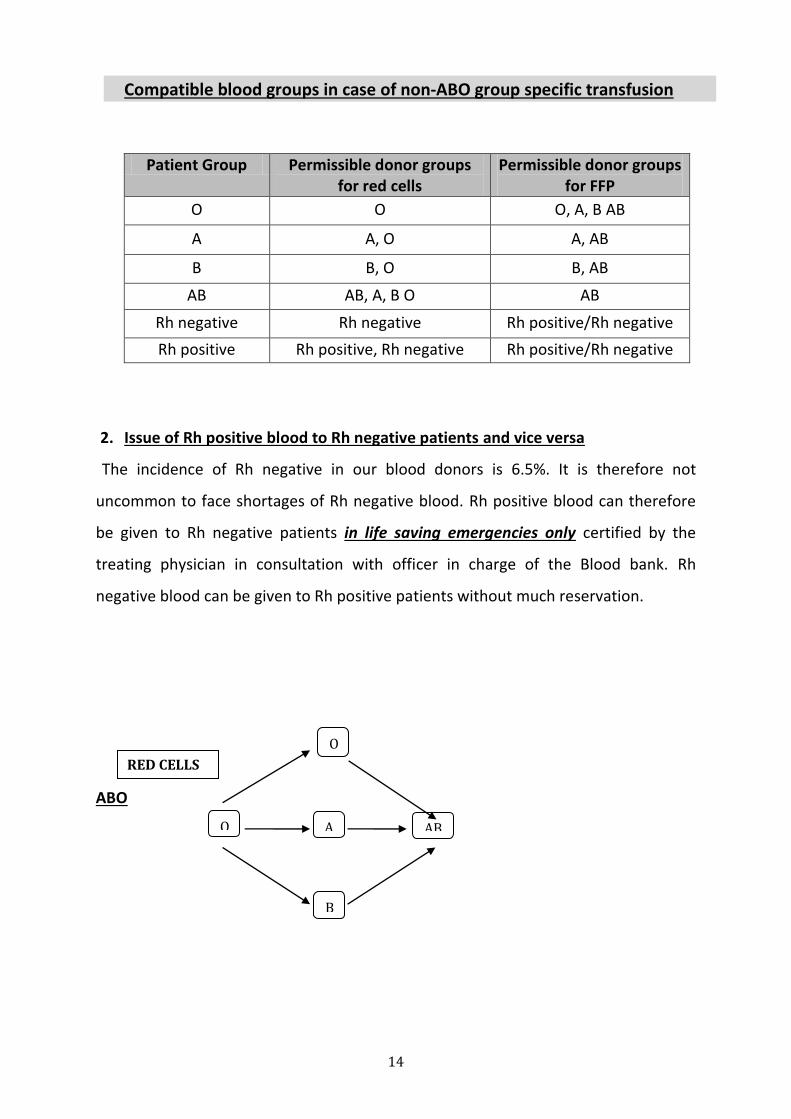
Compatible blood groups in case of non-ABO group specific transfusion
Patient Group Permissible donor groups for red cells
Permissible donor groups for FFP
O O O, A, B AB
A A, O A, AB
B B, O B, AB
AB AB, A, B O AB
Rh negative Rh negative Rh positive/Rh negative
Rh positive Rh positive, Rh negative Rh positive/Rh negative
2. Issue of Rh positive blood to Rh negative patients and vice versa
The incidence of Rh negative in our blood donors is 6.5%. It is therefore not
uncommon to face shortages of Rh negative blood. Rh positive blood can therefore
be given to Rh negative patients in life saving emergencies only certified by the
treating physician in consultation with officer in charge of the Blood bank. Rh
negative blood can be given to Rh positive patients without much reservation.
ABO
O
B
AB O A
RED CELLS
15
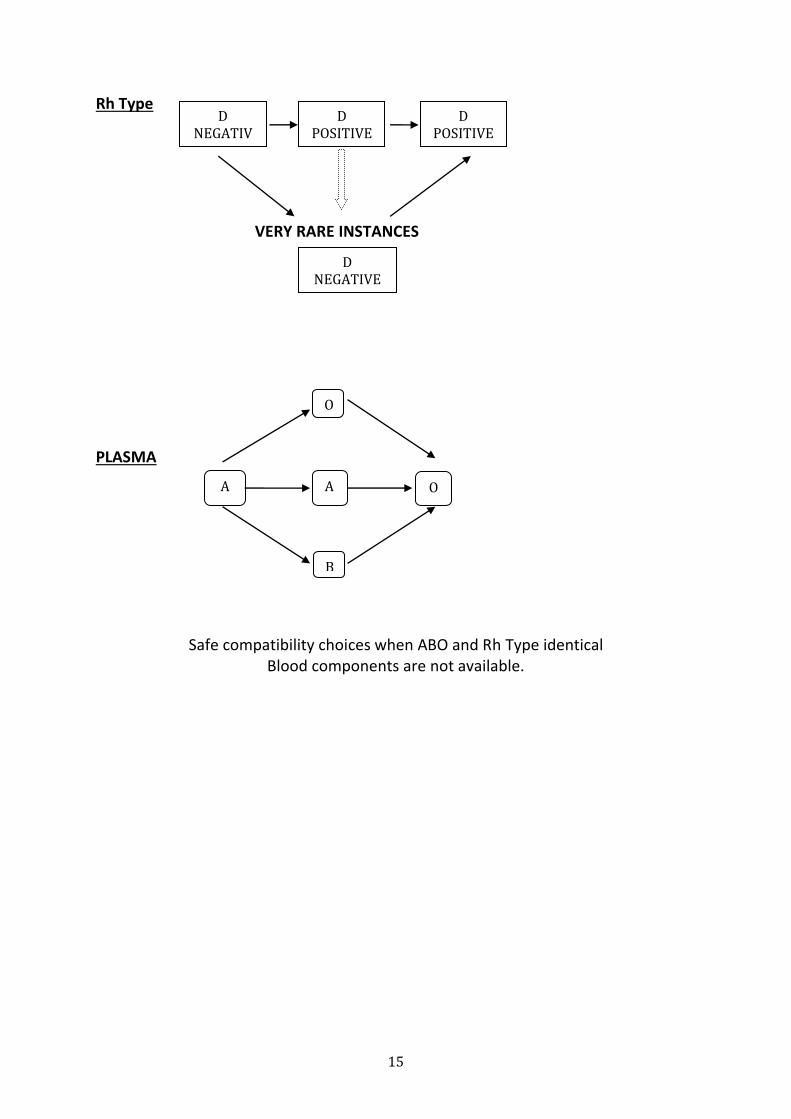
Rh Type
VERY RARE INSTANCES
PLASMA
Safe compatibility choices when ABO and Rh Type identical Blood components are not available.
D NEGATIV
E
D POSITIVE
D POSITIVE
D NEGATIVE
O
B
O A A
16
4. Issue of blood and components
1. In case of routine cross matches if ICT is negative blood units will be issued on
demand after doing immediate spin technique at Room temperature.
2. In case if Blood units are not lifted then they will be stored in the blood bank
refrigerator after cross match.
3. At present matched blood is collected from the Blood bank by interns/resident
doctors. Relatives or friends of the patients will not be allowed to collect blood
units from the blood bank.
4. Interns are required to bring proper details such as Patient name, Hospital
number, indication, diagnosis and type of blood components to be taken.
5. The blood bank personnel will enter the details of the blood units, including time
and date of issue. The intern/resident doctor will have to confirm details of blood
units in the issue register, compatibility form, cross match label and sign in the
register and write the name in capital letters before leaving. The intern will have
to cross check compatibility and certify, if necessary.
6. Return of unused blood
If the blood is not to be used for any reasons, return it to blood bank
immediately within 30 minutes.
Compatibility forms need to be sent to the Blood bank along with unused
blood.
The red cells units will not be accepted if one of the ports is opened. The
blood bag should have the labels attached to it which will help to proper
identification of units.
Note: Blood units should not be stored in the refrigerator in the ward. These
refrigerators are not specifically designated, monitored, tested and controlled, as
are blood bank fridges. Blood should be collected only 30 minutes in advance
before planned transfusion.
17
5. Administration of blood and components
General Guidelines:
1. Check the blood or components before starting the transfusion. The following
must be checked.
Verify that you have received the required blood or component ordered.
Match ABO and Rh group of the patient with the ABO & Rh group of the blood
product label. If there is discrepancy, do not start transfusion. Report to the blood
bank and Residents in the ward immediately.
Check expiration date, unit number and component label.
Check the integrity of the unit by applying light pressure to the unit and examine
for any leaks.
Check the bag for presence of clots.
Compare the blood bag number with the number listed on compatibility report
Carefully observe the appearance of the unit.
2. Identification of the Patient:
This is a very important step before starting the transfusion, as misidentification of
the patient is the most common cause of mismatched transfusion and prove fatal
to the patient
Compare the patient name, Hospital number and blood group on the blood bag
with the patient name and Hospital number and blood group on the patient file.
If the patient is conscious, confirm the name by having him/her state the name
and compare it with the name on the compatibility report.
Before starting the transfusion, record the time, temperature of the patient, pulse
rate and BP on the patient file. This will be helpful to monitor any changes in the
vitals during transfusion.
The red cells should not be kept outside if transfusion is delayed. They should be
stored at 2 to 4 C.
RED CELLS SHOULD NOT BE STORED IN THE FREEZER COMPARTMENT
18
Administration of red blood cell components:
1. Ensure the IV line is patent and Gauge of the needle is adequate to transfuse the
blood component. Use a standard blood transfusion set with filter issued by the
blood bank.
2. Examine the red cell bag for clots, abnormal dark purple blue color. Red cells will
usually be dark red in color. If anything seems abnormal, check with the blood
bank.
3. Invert the bag several times to ensure re-suspension of red cells. Follow the
administration instructions on the blood bag label.
4. Concurrent fluids along with red cell transfusion:
Avoid additions of any type of fluid or drug in to the blood bag.
Only compatible IV solution compatible with blood is isotonic (0.9%) saline and
may be used along with red cell transfusion.
Do not mix any medication along with red cell unit. Some drugs can cause
hemolysis due to their high pH. 5% dextrose can cause agglutination of red blood
cells. Ringer lactate solution can result in clotting because of its calcium content.
If medication were added to the blood component it would be difficult to
investigate the cause of the transfusion reaction if there is any.
Do not mix blood components together, e.g. red cells and platelets before
transfusion.
5. Start the transfusion slowly for first 15 minutes and observe the patient. If the
clinical status is OK, remaining unit can be transfused as per the indication.
However, check the patient frequently for any significant change in the vitals.
Record all vital signs on the case file and compatibility form.
6. Change the transfusion set after 4 units of blood.
7. Red Cell transfusion should be completed within 4 hours of starting. Beyond 4
hours, there is a risk of bacterial contamination.
8. If the transfusion is uneventful, return one copy of the compatibility form duly
filled to the blood bank and paste one in the case file.
19
9. If there is any adverse reaction to the transfusions, see “Section 5” for action to
be initiated.
Note: If the blood product is not to be used for any reason, do not store in the
refrigerator in the ward as these refrigerators are not designated for blood
storage. Return unused blood bags to the blood bank immediately.
10. Discard the empty blood component bag in the Biohazard Waste Container in
the Ward, unless the patient has suffered an adverse reaction in that case the
bag has to be returned to the blood bank along with the completely filled
reaction form with filled in reaction form for investigation.
Administration of Plasma & Cryoprecipitate:
Follow the general guidelines of identification and inspection of blood
components as mentioned in red cell administration.
Thawed FFP will be clear with yellow straw color. Cryoprecipitate will usually be
cloudy.
Get FFP thawed in the blood bank.
Thawing of plasma components:
Thawing of FFP and Cryo is done at 37 C water bath.
Place the unit in a plastic over wrap so that water in the bath will not
contaminate the component.
The ports of the component bag should not come in contact with the water.
Squeeze the component intermittently to ensure rapid thawing.
Generally, thawing of FFP takes 10 to 15 minutes.
Note: Once thawed, plasma components should not be frozen. They can be
kept at 4 C for not more than 4 hrs.
A standard blood administration set is satisfactory for transfusion of plasma
components.
20
Cryoprecipitate:
Cryo can be administered using a 50 ml syringe. After thawing, aspirate all Cryo
in a syringe with needle. A significant amount of Cryo will remain attached to the
walls of the plastic containers. Injecting 25 ml of isotonic saline in the bag and
rinsing it thoroughly can rectify this.
Follow rest of the procedure as mentioned in Red Cell administration.
Thawed cryoprecipitate should be stored at 4 C and used within 4 hours.
Administration of Platelet Products
1. General guidelines for patient identification and component inspection are same
as red cell administration.
2. A blood administration set issued by the blood bank should be used for platelet
transfusion. After platelets are transfused, it is preferred to rinse entrapped
platelets from the filter by flowing 50 ml of isotonic saline through it.
Platelet concentrates should not be transfused through the set used for
transfusing other blood components.
3. Transfusion of one unit of random unit of platelets should be completed in 20
minutes due to the risk of bacterial contamination.
4. Since platelets need to be stored on agitator, request and collect platelets from
blood bank just before transfusion.
5. Rest of the procedure is same as for red cell administration.
Note: Platelet products must “NOT” be refrigerated at any state.
21
Use of Filters for administration of blood and components:
1. Routine blood transfusion sets have a filter with 170µ pore size.
2. Micro-aggregate filters: Micro-aggregate filters have a pore size of 40 micron.
They allow rapid transfusion of blood and components at the same time prevent
micro-aggregate from entering the circulation. They are used in cardio
pulmonary bypass surgery.
3. Leukocyte filters:
Leukocyte filters are used to prevent febrile transfusion reactions and CMV
transmission. They are especially useful in multiply transfused patients. Two
units of red cells can be transfused using a single filter. The proper selection of
the leukocyte filter should be made, depending on the type of component to be
transfused.
Warming of blood Products:
1. Generally, there is no need to warm the unit of red cells before transfusion.
Keeping the blood unit at room temperature for 30 minutes will be enough in
most cases.
2. In special circumstances, such as patients with cold agglutinins in the serum, it
is important to pre warm the unit at 37 C before transfusion. Special blood
warmers may be used for this purpose. Blood should not be warmed in Dry
Incubator in the laboratory. It is important to keep the patient warm during
transfusion.
3. Always check for the presence of hemolysis while using a blood warmer.
There is no need to warm blood before transfusion except in massive transfusion.
(Infusion rate @ 15 ml/Kg body weight/hour in children or @ 50 ml/Kg body
weight/hour in adults.)
22
Hemoglobinuria may be due to following causes also: Transfusion of hemolysed donor red cells due to any cause will result in
hemoglobinuria
Bacterial contamination;
Excessive warming;
Erroneous freezing;
Addition of drugs or intravenous fluids;
Trauma from extracorporeal devices
Red cell enzyme deficiency.
Blood Transfusion in Autoimmune haemolytic anaemia may exacerbate the
hemolysis and be associated with hemoglobinuria.
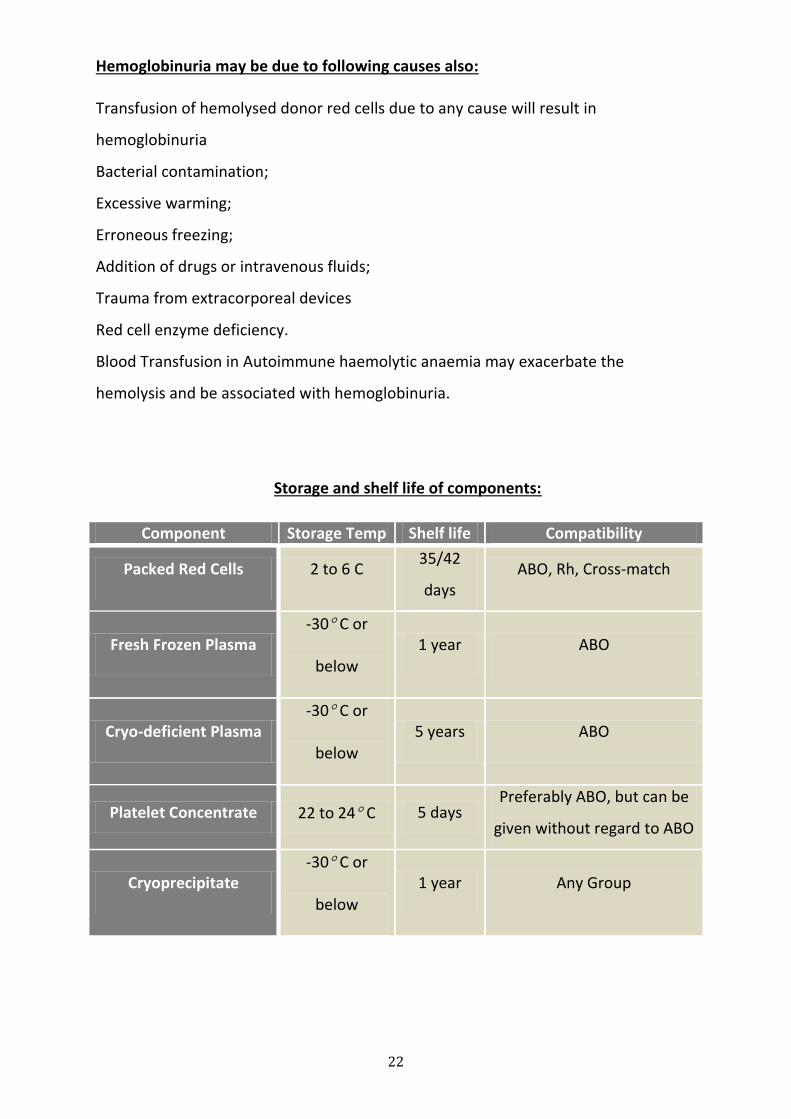
Storage and shelf life of components:
Component Storage Temp Shelf life Compatibility
Packed Red Cells 2 to 6 C 35/42
days ABO, Rh, Cross-match
Fresh Frozen Plasma -30 C or
below
1 year ABO
Cryo-deficient Plasma -30 C or
below
5 years ABO
Platelet Concentrate 22 to 24 C 5 days Preferably ABO, but can be
given without regard to ABO
Cryoprecipitate -30 C or
below
1 year Any Group
23
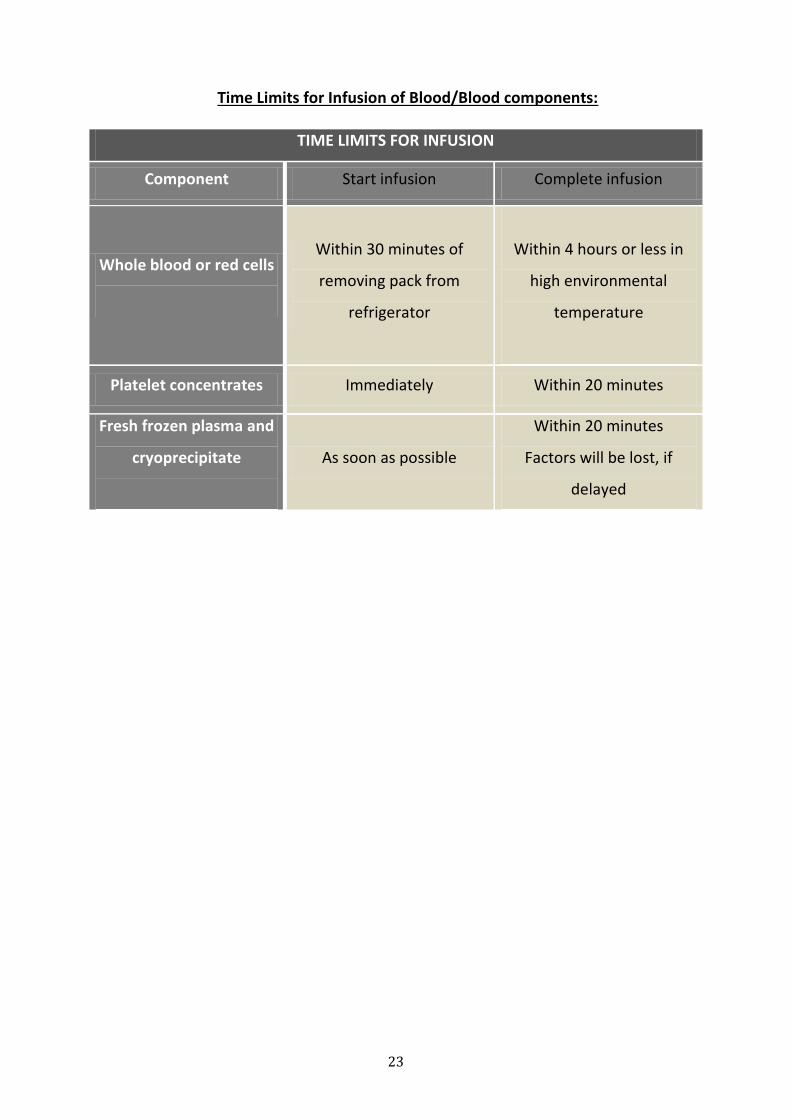
Time Limits for Infusion of Blood/Blood components:
TIME LIMITS FOR INFUSION
Component Start infusion Complete infusion
Whole blood or red cells
Within 30 minutes of
removing pack from
refrigerator
Within 4 hours or less in
high environmental
temperature
Platelet concentrates Immediately Within 20 minutes
Fresh frozen plasma and
cryoprecipitate
As soon as possible
Within 20 minutes
Factors will be lost, if
delayed
24
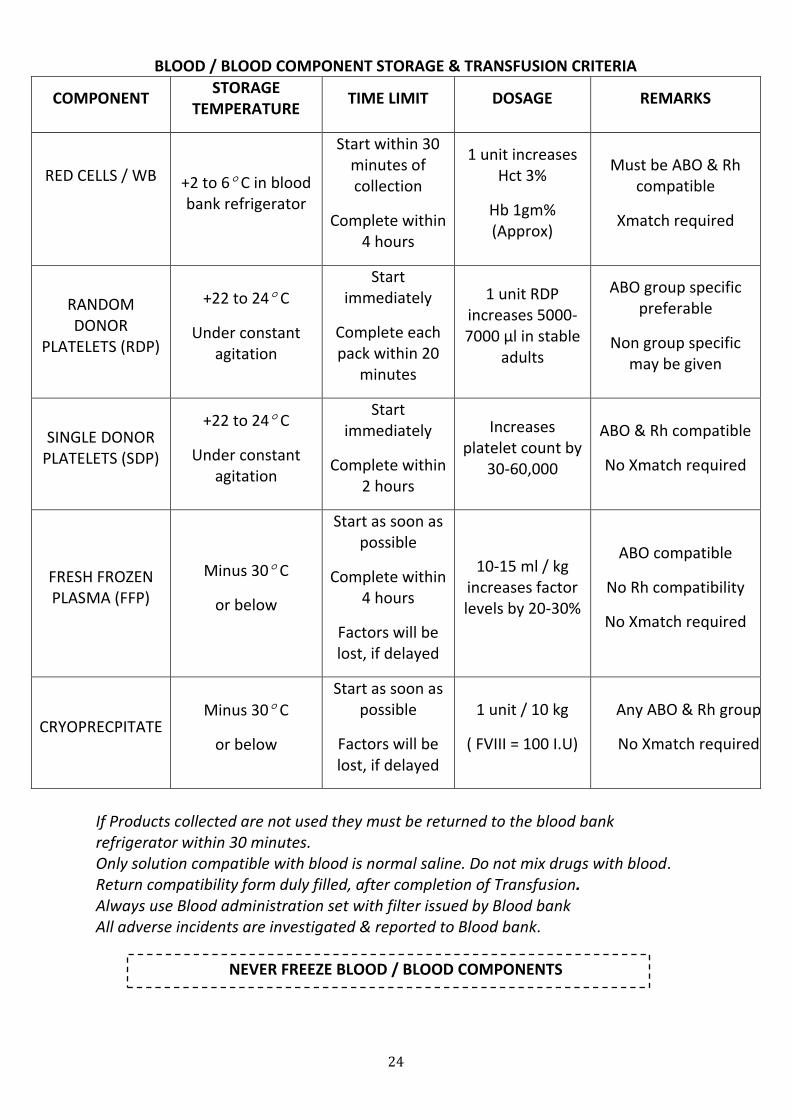
BLOOD / BLOOD COMPONENT STORAGE & TRANSFUSION CRITERIA
COMPONENT STORAGE
TEMPERATURE TIME LIMIT DOSAGE REMARKS
RED CELLS / WB
+2 to 6 C in blood bank refrigerator
Start within 30 minutes of collection
Complete within 4 hours
1 unit increases Hct 3%
Hb 1gm% (Approx)
Must be ABO & Rh compatible
Xmatch required
RANDOM DONOR
PLATELETS (RDP)
+22 to 24 C
Under constant agitation
Start immediately
Complete each pack within 20
minutes
1 unit RDP increases 5000-7000 µl in stable
adults
ABO group specific preferable
Non group specific may be given
SINGLE DONOR PLATELETS (SDP)
+22 to 24 C
Under constant agitation
Start immediately
Complete within 2 hours
Increases platelet count by
30-60,000
ABO & Rh compatible
No Xmatch required
FRESH FROZEN PLASMA (FFP)
Minus 30 C
or below
Start as soon as possible
Complete within 4 hours
Factors will be lost, if delayed
10-15 ml / kg increases factor levels by 20-30%
ABO compatible
No Rh compatibility
No Xmatch required
CRYOPRECPITATE Minus 30 C
or below
Start as soon as possible
Factors will be lost, if delayed
1 unit / 10 kg
( FVIII = 100 I.U)
Any ABO & Rh group
No Xmatch required
If Products collected are not used they must be returned to the blood bank refrigerator within 30 minutes. Only solution compatible with blood is normal saline. Do not mix drugs with blood. Return compatibility form duly filled, after completion of Transfusion. Always use Blood administration set with filter issued by Blood bank All adverse incidents are investigated & reported to Blood bank.
NEVER FREEZE BLOOD / BLOOD COMPONENTS
25
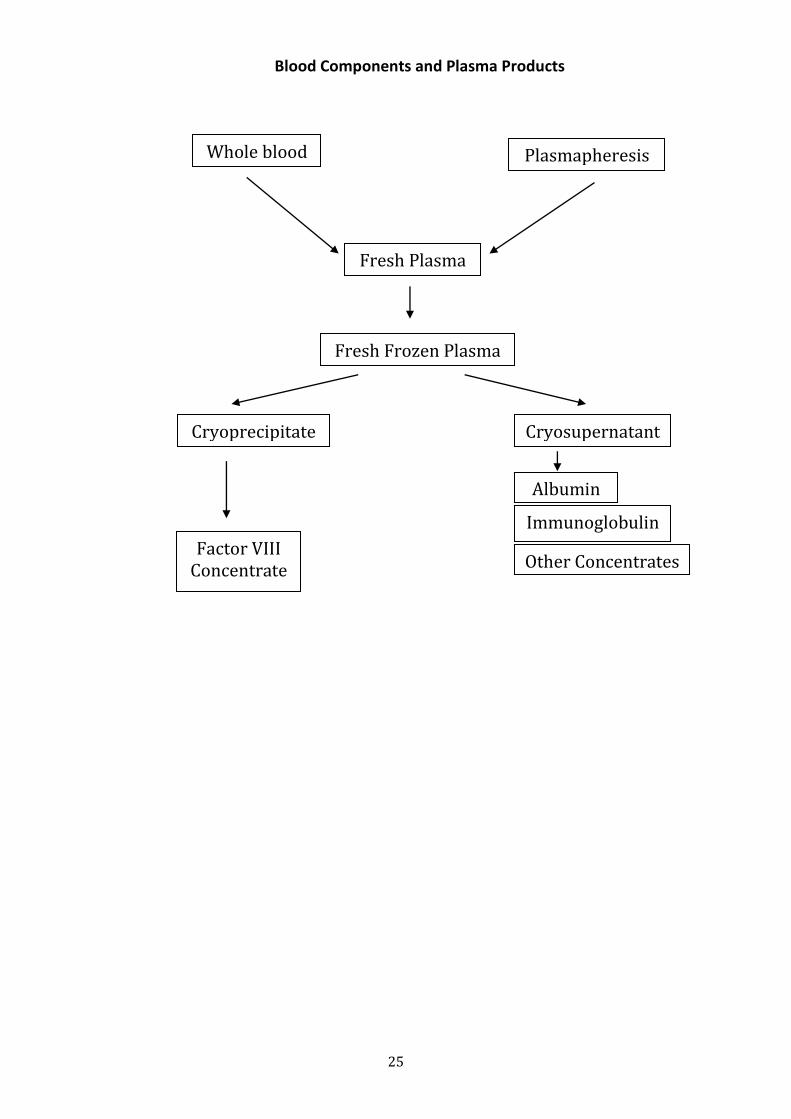
Blood Components and Plasma Products
Fresh Plasma
Whole blood Plasmapheresis
Fresh Frozen Plasma
Cryoprecipitate Cryosupernatant
Factor VIII Concentrate
Albumin
Immunoglobulin
s Other Concentrates
26
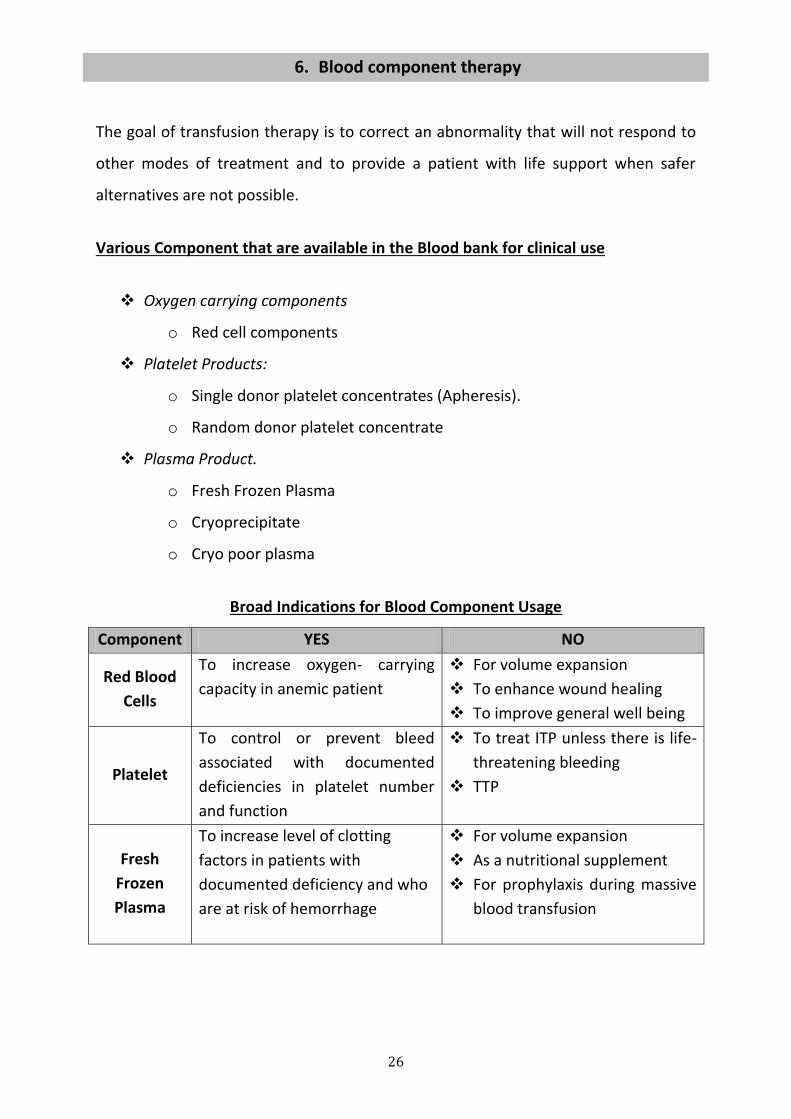
6. Blood component therapy
The goal of transfusion therapy is to correct an abnormality that will not respond to
other modes of treatment and to provide a patient with life support when safer
alternatives are not possible.
Various Component that are available in the Blood bank for clinical use
Oxygen carrying components
o Red cell components
Platelet Products:
o Single donor platelet concentrates (Apheresis).
o Random donor platelet concentrate
Plasma Product.
o Fresh Frozen Plasma
o Cryoprecipitate
o Cryo poor plasma
Broad Indications for Blood Component Usage
Component YES NO
Red Blood
Cells
To increase oxygen- carrying
capacity in anemic patient
For volume expansion
To enhance wound healing
To improve general well being
Platelet
To control or prevent bleed
associated with documented
deficiencies in platelet number
and function
To treat ITP unless there is life-
threatening bleeding
TTP
Fresh
Frozen
Plasma
To increase level of clotting
factors in patients with
documented deficiency and who
are at risk of hemorrhage
For volume expansion
As a nutritional supplement
For prophylaxis during massive
blood transfusion
27
Packed Red Cell Concentrate (PRBC)
Red Blood cells are the cellular product obtained after centrifugation of whole blood
and removal of most of the Plasma. The usual unit of PRBC should raise Hct or Hb by
approximately 3% or 1 gm% respectively in an average adult patient and 3 gm% Hb in
infants.
Indication of PRBC
There is no universal trigger for red cell transfusion. Clinical judgment plays vital role
in the decision to transfuse red cells or not. RBCs are the component of choice for
most patients with symptomatic deficit of oxygen carrying capacity.
Estimation of need based on haemoglobin concentration
Most patients with Hb of 6-7 gm/dl tolerate anemia well and need not be transfused
unless there are symptoms of anoxia. Patient with Hb >10gm/dl almost certainly
never require red cell transfusion. Therefore, in any given anemic patient, the aim of
transfusion therapy should be to correct the symptoms of the patient rather than
correcting the hemoglobin level.
Estimation of need based on Acute Blood Loss
15% loss of blood volume (750 ml in adult) No need of transfusion, if there is no
preexisting anaemia or cardiac or respiratory disease
15 -30% loss of blood volume (800 – 1500 ml in an adult) Need to transfuse
crystalloids or colloids. Need for red cell transfusion unlikely in the absence
preexisting disease
30 – 40% loss of blood volume (1500 – 2000 ml in an adult) Need rapid replacement
of volume with crystalloids or synthetic colloids and red cell transfusion will probably
required.
40% loss of blood volume (> 2000 ml in an adult) need rapid volumere placement
including red cell transfusion is required.
28
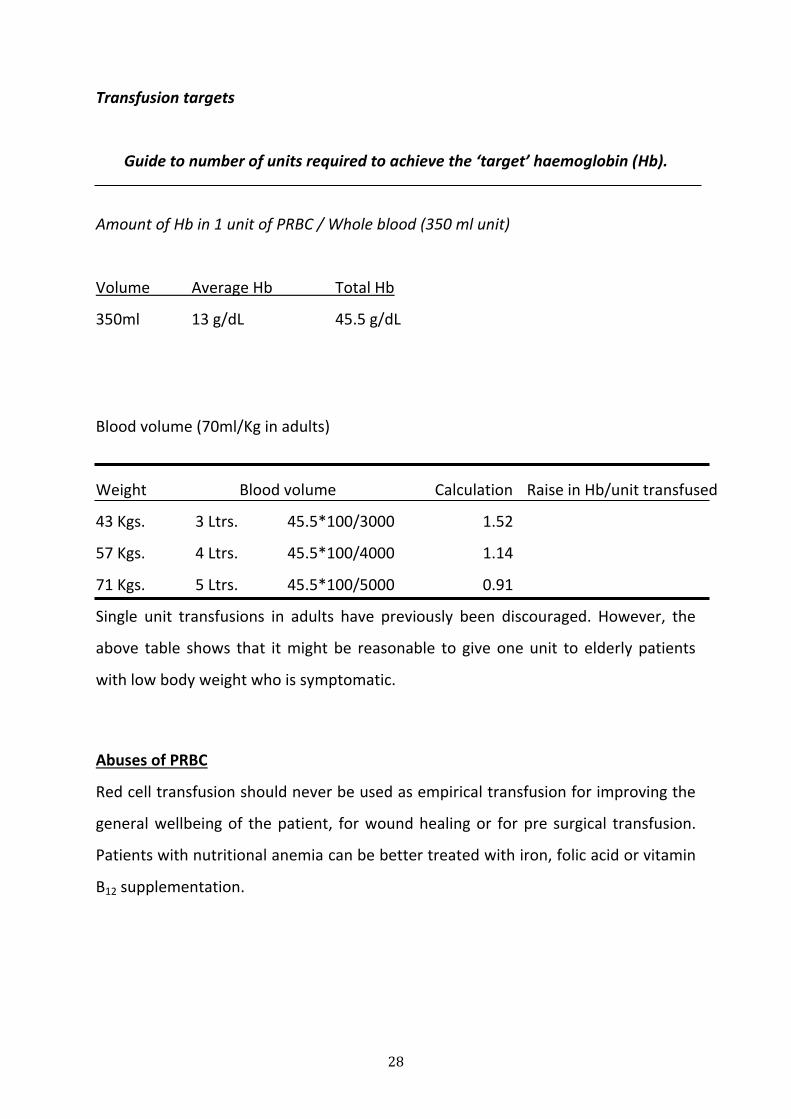
Transfusion targets
Guide to number of units required to achieve the ‘target’ haemoglobin (Hb).
Amount of Hb in 1 unit of PRBC / Whole blood (350 ml unit)
Volume Average Hb Total Hb
350ml 13 g/dL 45.5 g/dL
Blood volume (70ml/Kg in adults)
Weight Blood volume Calculation Raise in Hb/unit transfused
43 Kgs. 3 Ltrs. 45.5*100/3000 1.52
57 Kgs. 4 Ltrs. 45.5*100/4000 1.14
71 Kgs. 5 Ltrs. 45.5*100/5000 0.91
Single unit transfusions in adults have previously been discouraged. However, the
above table shows that it might be reasonable to give one unit to elderly patients
with low body weight who is symptomatic.
Abuses of PRBC
Red cell transfusion should never be used as empirical transfusion for improving the
general wellbeing of the patient, for wound healing or for pre surgical transfusion.
Patients with nutritional anemia can be better treated with iron, folic acid or vitamin
B12 supplementation.
29
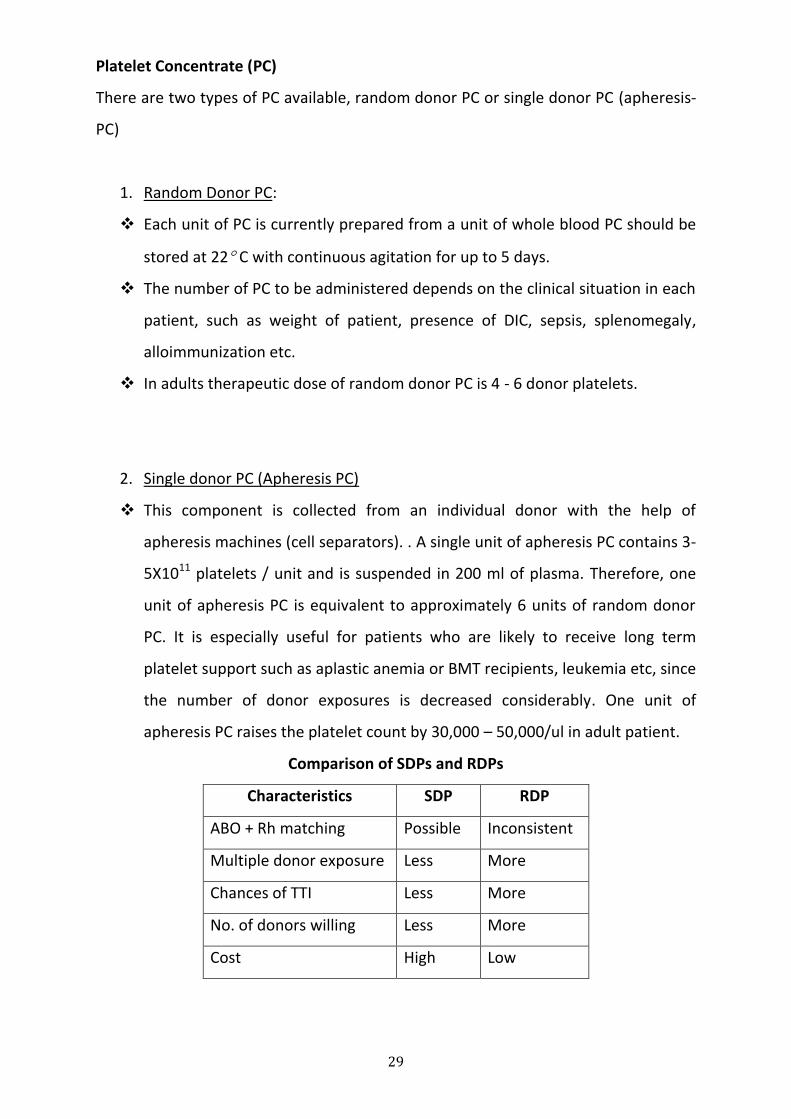
Platelet Concentrate (PC)
There are two types of PC available, random donor PC or single donor PC (apheresis-
PC)
1. Random Donor PC:
Each unit of PC is currently prepared from a unit of whole blood PC should be
stored at 22 C with continuous agitation for up to 5 days.
The number of PC to be administered depends on the clinical situation in each
patient, such as weight of patient, presence of DIC, sepsis, splenomegaly,
alloimmunization etc.
In adults therapeutic dose of random donor PC is 4 - 6 donor platelets.
2. Single donor PC (Apheresis PC)
This component is collected from an individual donor with the help of
apheresis machines (cell separators). . A single unit of apheresis PC contains 3-
5X1011 platelets / unit and is suspended in 200 ml of plasma. Therefore, one
unit of apheresis PC is equivalent to approximately 6 units of random donor
PC. It is especially useful for patients who are likely to receive long term
platelet support such as aplastic anemia or BMT recipients, leukemia etc, since
the number of donor exposures is decreased considerably. One unit of
apheresis PC raises the platelet count by 30,000 – 50,000/ul in adult patient.
Comparison of SDPs and RDPs
Characteristics SDP RDP
ABO + Rh matching Possible Inconsistent
Multiple donor exposure Less More
Chances of TTI Less More
No. of donors willing Less More
Cost High Low
30
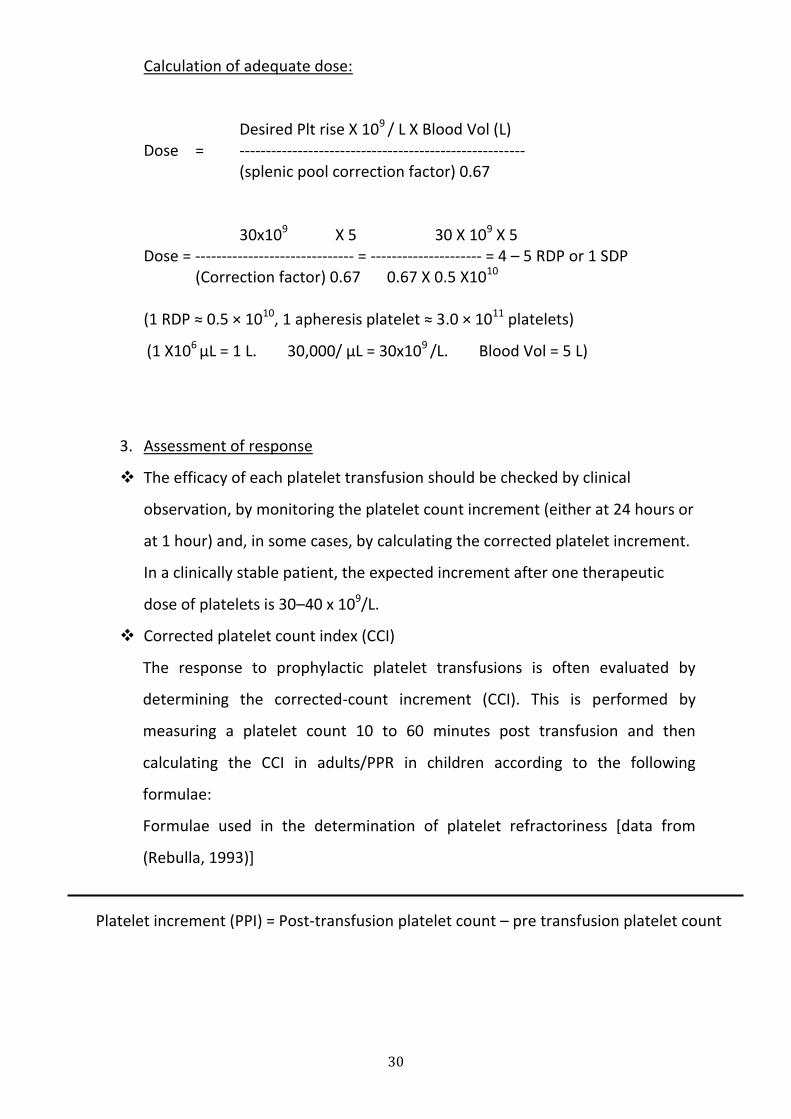
Calculation of adequate dose:
Desired Plt rise X 109 / L X Blood Vol (L) Dose = ------------------------------------------------------ (splenic pool correction factor) 0.67
30x109 X 5 30 X 109 X 5 Dose = ------------------------------ = --------------------- = 4 – 5 RDP or 1 SDP (Correction factor) 0.67 0.67 X 0.5 X1010
(1 RDP ≈ 0.5 × 1010, 1 apheresis platelet ≈ 3.0 × 1011 platelets)
(1 X106 μL = 1 L. 30,000/ μL = 30x109 /L. Blood Vol = 5 L)
3. Assessment of response
The efficacy of each platelet transfusion should be checked by clinical
observation, by monitoring the platelet count increment (either at 24 hours or
at 1 hour) and, in some cases, by calculating the corrected platelet increment.
In a clinically stable patient, the expected increment after one therapeutic
dose of platelets is 30–40 x 109/L.
Corrected platelet count index (CCI)
The response to prophylactic platelet transfusions is often evaluated by
determining the corrected-count increment (CCI). This is performed by
measuring a platelet count 10 to 60 minutes post transfusion and then
calculating the CCI in adults/PPR in children according to the following
formulae:
Formulae used in the determination of platelet refractoriness [data from
(Rebulla, 1993)]
Platelet increment (PPI) = Post-transfusion platelet count – pre transfusion platelet count
31
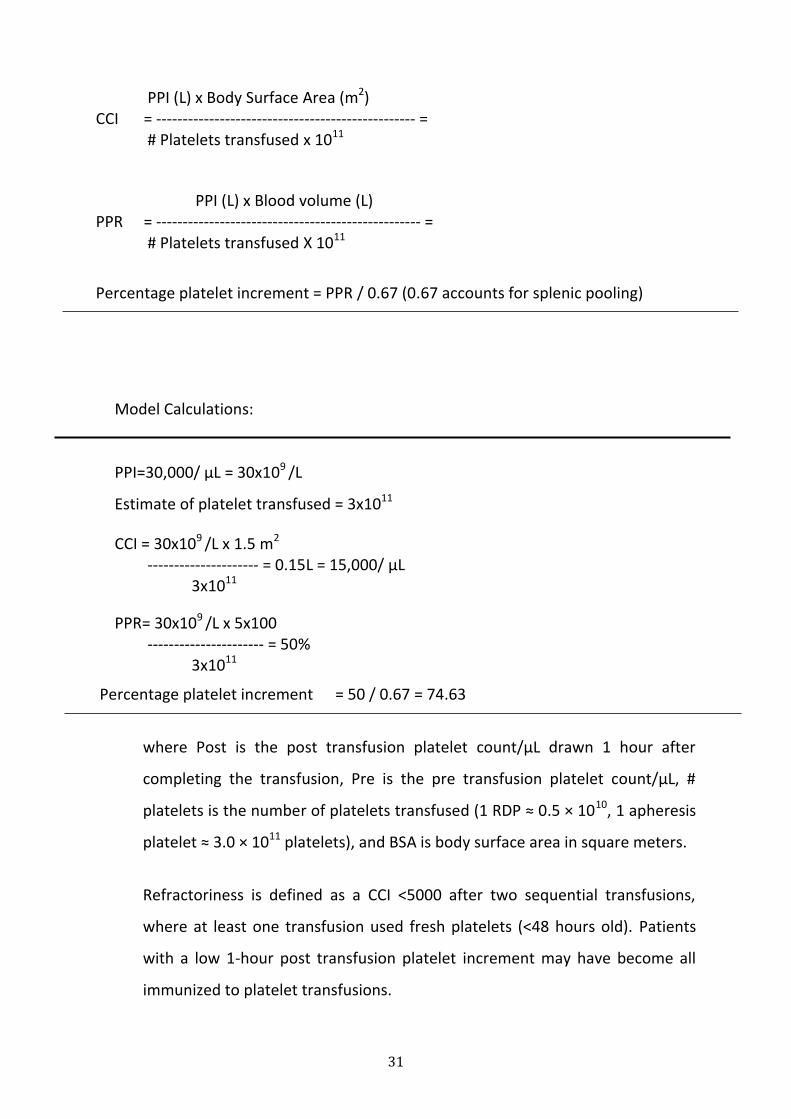
PPI (L) x Body Surface Area (m2) CCI = ------------------------------------------------- = # Platelets transfused x 1011
PPI (L) x Blood volume (L) PPR = -------------------------------------------------- = # Platelets transfused X 1011
Percentage platelet increment = PPR / 0.67 (0.67 accounts for splenic pooling)
Model Calculations:
PPI=30,000/ μL = 30x109 /L
Estimate of platelet transfused = 3x1011
CCI = 30x109 /L x 1.5 m2 --------------------- = 0.15L = 15,000/ μL 3x1011
PPR= 30x109 /L x 5x100 ---------------------- = 50% 3x1011
Percentage platelet increment = 50 / 0.67 = 74.63
where Post is the post transfusion platelet count/μL drawn 1 hour after
completing the transfusion, Pre is the pre transfusion platelet count/μL, #
platelets is the number of platelets transfused (1 RDP ≈ 0.5 × 1010, 1 apheresis
platelet ≈ 3.0 × 1011 platelets), and BSA is body surface area in square meters.
Refractoriness is defined as a CCI <5000 after two sequential transfusions,
where at least one transfusion used fresh platelets (<48 hours old). Patients
with a low 1-hour post transfusion platelet increment may have become all
immunized to platelet transfusions.
32
Causes of refractoriness:
Immune
HLA alloantibodies
Platelet specific antibodies
Platelet autoantibodies
ABO incompatibility – rare
Nonimmune
Sepsis
Antibiotic/antifungal therapy
Disseminated intravascular coagulation
Splenomegaly
If non-immune platelet consumption appears likely, correct the clinical factors
responsible and platelet transfusions from random donors should be continued.
Indications:
PC are indicated for the prevention ( prophylactic) or treatment (therapeutic)
of bleeding in patients with decreased platelet count ( thrombocytopenia) or
defective platelet function or both.
1. Prophylactic transfusion
10,000 / μL without additional risk factors
2. Therapeutic transfusion
Standard for the treatment of thrombocytopenic bleeding
Haematological malignancies
Hypoproliferative states – aplastic anaemia
Massive transfusion
Acute DIC
Inherited or acquired platelet function disorder
Neonatal alloimune thrombocytopenia
33
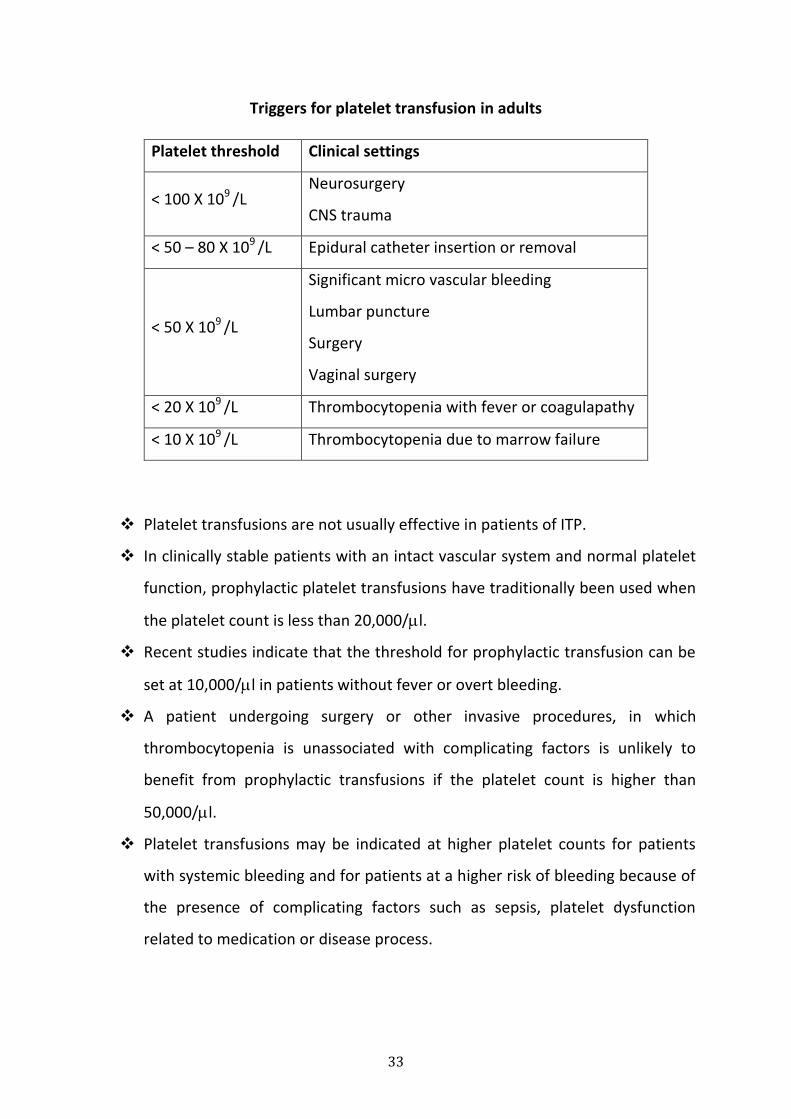
Triggers for platelet transfusion in adults
Platelet threshold Clinical settings
< 100 X 109 /L Neurosurgery
CNS trauma
< 50 – 80 X 109 /L Epidural catheter insertion or removal
< 50 X 109 /L
Significant micro vascular bleeding
Lumbar puncture
Surgery
Vaginal surgery
< 20 X 109 /L Thrombocytopenia with fever or coagulapathy
< 10 X 109 /L Thrombocytopenia due to marrow failure
Platelet transfusions are not usually effective in patients of ITP.
In clinically stable patients with an intact vascular system and normal platelet
function, prophylactic platelet transfusions have traditionally been used when
the platelet count is less than 20,000/l.
Recent studies indicate that the threshold for prophylactic transfusion can be
set at 10,000/l in patients without fever or overt bleeding.
A patient undergoing surgery or other invasive procedures, in which
thrombocytopenia is unassociated with complicating factors is unlikely to
benefit from prophylactic transfusions if the platelet count is higher than
50,000/l.
Platelet transfusions may be indicated at higher platelet counts for patients
with systemic bleeding and for patients at a higher risk of bleeding because of
the presence of complicating factors such as sepsis, platelet dysfunction
related to medication or disease process.
34
Contraindications:
Patients with thrombotic thrombocytopenic purpura.
Patients with ITP unless there is life threatening bleeding or intracranial
hemorrhage.
Heparin induced thrombocytopenia
Adverse effects of platelet transfusion
febrile nonhaemolytic transfusion reaction(FNHTR)
allimmunization
bacterial sepsis
Unwarranted platelet transfusion generates alloimmunization reduing efficacy of
future transfusion, in addition to the usual adverse effects of blood component.
Fresh Frozen Plasma (FFP)
FFP is indicated in the control or prevention of bleeding in patients with multiple
coagulation factor defects. FFP must be thawed at 37 C in a water bath with due
precautions. FFP should be used as soon as it is thawed to avoid the decay of clotting
factors. Dose of FFP is 10 - 15ml/Kg body weight.
Indications for FFP
Each unit of transfused FFP will increase the level of any clotting factors by 2 to 3 %
in an average adult. Laboratory tests such as PT and APTT should be done to monitor
the FFP use in patients.
Broad spectrum coagulation factor deficiency.
severe liver disease
oral anticoagulant overdose
disseminated intravascular coagulation
massive transfusion with coagulation problems
Thrombotic thrombocytopenic purpura
AT III deficiency
35
Note: Most common abuses of FFP
1. Volume expansion
2. As protein supplements
3. Prolonged bleeding in the absence of coagulation defects.
Cryoprecipitate
Cryoprecipitate is the cold insoluble precipitate having Factor VIII, vWF, fibrinogen
and factor XIII as its major constituents. Standards require an average of 80 IU of
FVIII in each unit.
Dose: 1 Donor unit / 10 Kg patient’s body weight. Alternatively, number of cryo bags
required can be calculated substituting the value 80 IU / 1 cryo bag and formula
given below for Factor VIII concentrate.
Indications:
1. Factor VIII Deficiency (Hemophilia A): The treatment of choice is virus
inactivated factor VIII concentrates
2. Von Willebrand’s Disease
3. Hypofibrinogenemia (<80 mg/dl):
Consumptive coagulopathy ( DIC),
Dysfibrinogenemia or Afibrinogenemia.
4. Fibrin Glue for topical hemostasis.
5. Reversal of fibrinolytic therapy
6. Factor XIII deficiency
36
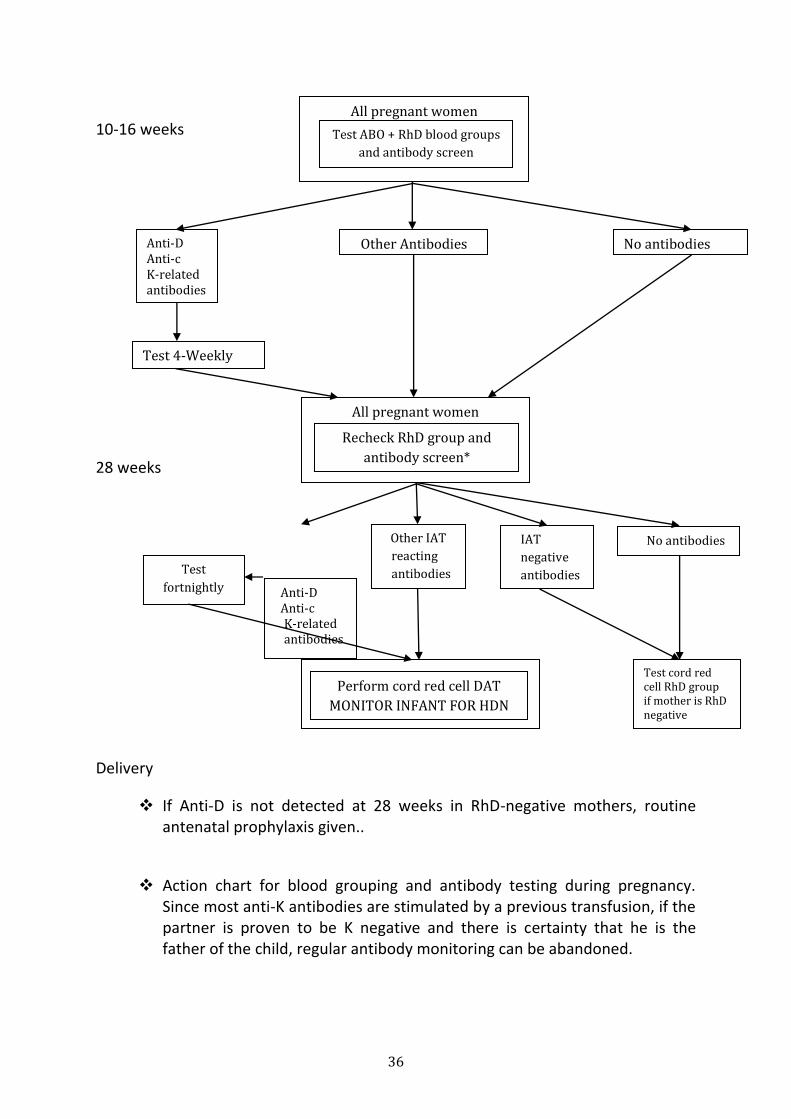
All pregnant women
All pregnant women
10-16 weeks
28 weeks
Delivery
If Anti-D is not detected at 28 weeks in RhD-negative mothers, routine antenatal prophylaxis given..
Action chart for blood grouping and antibody testing during pregnancy. Since most anti-K antibodies are stimulated by a previous transfusion, if the partner is proven to be K negative and there is certainty that he is the father of the child, regular antibody monitoring can be abandoned.
Test ABO + RhD blood groups
and antibody screen
Other Antibodies Anti-D Anti-c K-related antibodies
No antibodies
Test 4-Weekly
Recheck RhD group and
antibody screen*
Anti-D Anti-c K-related antibodies
Other IAT
reacting
antibodies
IAT
negative
antibodies
No antibodies
Test
fortnightly
Perform cord red cell DAT
MONITOR INFANT FOR HDN
Test cord red cell RhD group if mother is RhD negative
37
Post-delivery cord blood tests to be undertaken if
the mother has clinically significant antibody/ies
Direct antiglobalin test or DAT (positive if baby has corresponding antigen/s).
If the DAT is positive, test: o Haemoglobin o Bilirubin o Blood film (spherocytes are present if there is
significant haemolysis)
38
7. Neonatal and Childhood Transfusions
Pre transfusion testing for neonates and infants within the first four postnatal
months
Samples from both mother and infant should be obtained for ABO and Rh D typing.
Investigations on the maternal sample:
ABO and Rh D group
Screen for the presence of atypical red cell antibodies.
Investigations on the infant sample:
ABO and Rh D
ABO by cell group only (a reverse group would detect passive maternal
antibodies).
Direct antiglobulin test (DAT) performed on the neonate’s red cells.
In the absence of maternal serum, screen infant’s serum for atypical antibodies by an
indirect antiglobulin technique (IAT). A positive DAT on the neonate’s red cells or an
atypical red cell antibody in maternal or neonatal serum suggests possible
haemolytic disease of the newborn (HDN).
Selection of blood component
Components should be of the neonate’s own ABO and RhD group, or an alternative
compatible ABO and RhD group and compatible with any ABO or atypical red cell
antibody present in the maternal or neonatal plasma.
After the postnatal age of 4 months, compatibility tests should be conducted in
accordance
with pre transfusion testing in adult practice.
39
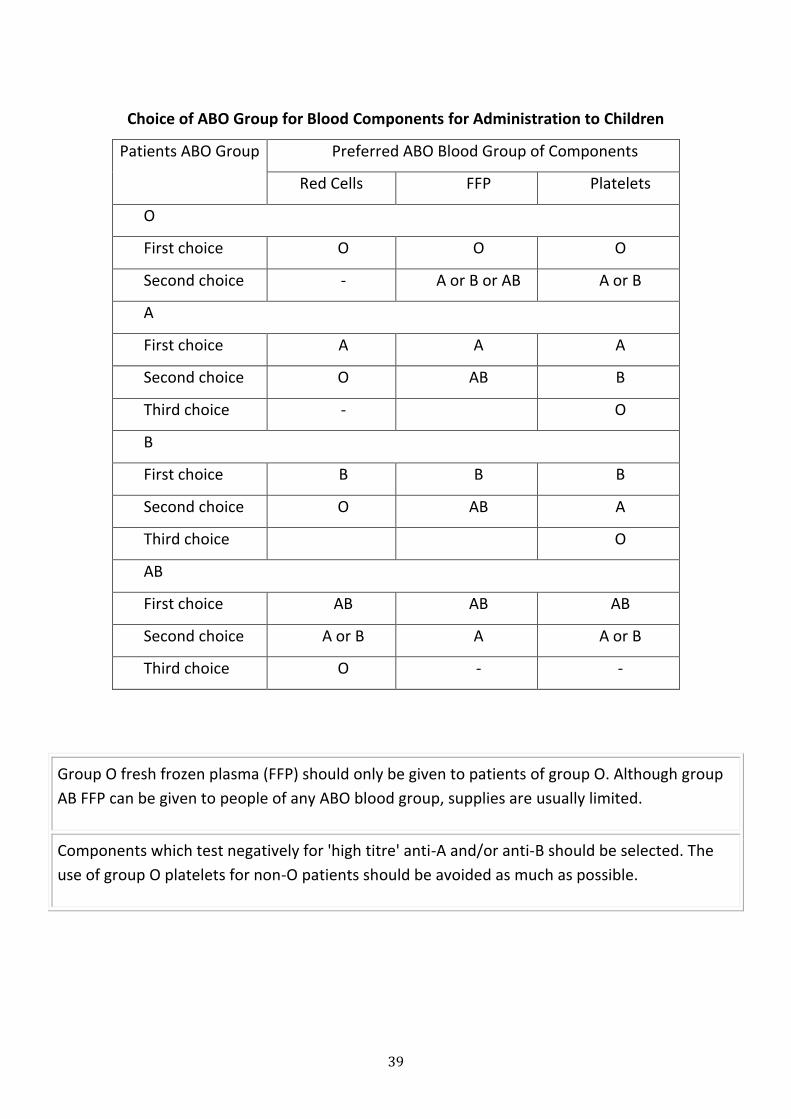
Choice of ABO Group for Blood Components for Administration to Children
Patients ABO Group Preferred ABO Blood Group of Components
Red Cells FFP Platelets
O
First choice O O O
Second choice - A or B or AB A or B
A
First choice A A A
Second choice O AB B
Third choice - O
B
First choice B B B
Second choice O AB A
Third choice O
AB
First choice AB AB AB
Second choice A or B A A or B
Third choice O - -
Group O fresh frozen plasma (FFP) should only be given to patients of group O. Although group
AB FFP can be given to people of any ABO blood group, supplies are usually limited.
Components which test negatively for 'high titre' anti-A and/or anti-B should be selected. The
use of group O platelets for non-O patients should be avoided as much as possible.
40
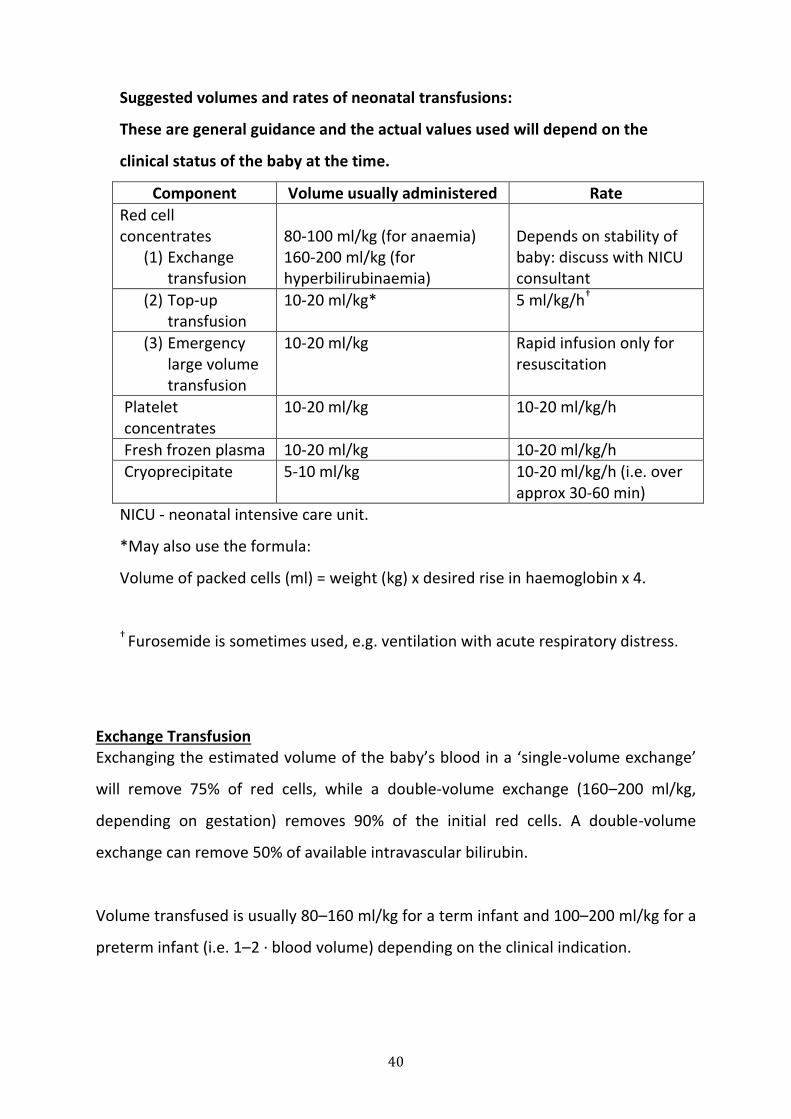
Suggested volumes and rates of neonatal transfusions:
These are general guidance and the actual values used will depend on the
clinical status of the baby at the time.
Component Volume usually administered Rate
Red cell concentrates
(1) Exchange transfusion
80-100 ml/kg (for anaemia) 160-200 ml/kg (for hyperbilirubinaemia)
Depends on stability of baby: discuss with NICU consultant
(2) Top-up transfusion
10-20 ml/kg* 5 ml/kg/h†
(3) Emergency large volume transfusion
10-20 ml/kg Rapid infusion only for resuscitation
Platelet concentrates
10-20 ml/kg 10-20 ml/kg/h
Fresh frozen plasma 10-20 ml/kg 10-20 ml/kg/h
Cryoprecipitate 5-10 ml/kg 10-20 ml/kg/h (i.e. over approx 30-60 min)
NICU - neonatal intensive care unit.
*May also use the formula:
Volume of packed cells (ml) = weight (kg) x desired rise in haemoglobin x 4.
† Furosemide is sometimes used, e.g. ventilation with acute respiratory distress.
Exchange Transfusion Exchanging the estimated volume of the baby’s blood in a ‘single-volume exchange’
will remove 75% of red cells, while a double-volume exchange (160–200 ml/kg,
depending on gestation) removes 90% of the initial red cells. A double-volume
exchange can remove 50% of available intravascular bilirubin.
Volume transfused is usually 80–160 ml/kg for a term infant and 100–200 ml/kg for a
preterm infant (i.e. 1–2 · blood volume) depending on the clinical indication.
41
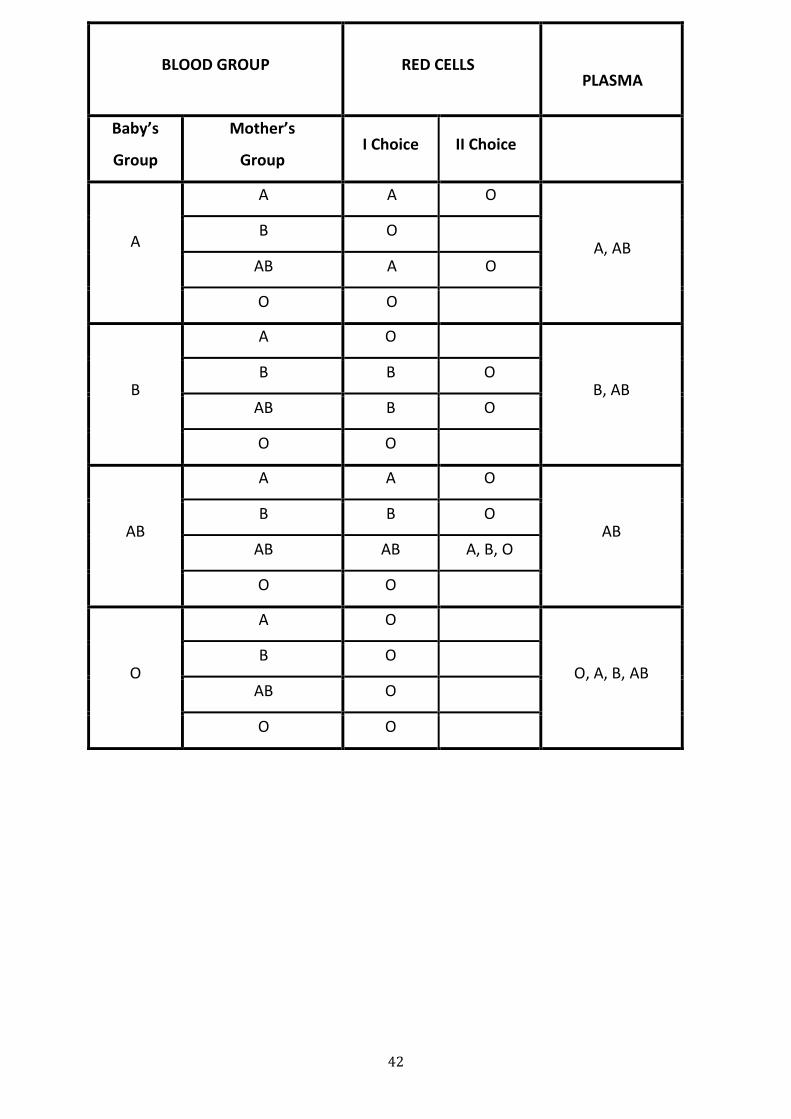
SELECTION OF BLOOD FOR EXCHANGE TRANSFUSION IN Rh HDN
Blood selected should be should not be more than 5 days old.
Select blood collected into CPD anticoagulant. Avoid SAGM and other additive
solutions
If ABO group of the baby is the same as that of mother or compatible with
mother’s blood, Rh negative blood of same ABO group as that of baby is used
When baby’s ABO group is not compatible with mother’s ABO group , O Rh
Negative blood free of hemolysins anti A and Anti B is used
If exchange transfusion required more than once, subsequent blood should be
of same ABO and Rh type as that of first time
If no compatible blood is available, exchange transfusion with incompatible
blood is preferred to no transfusion at all. Baby`s ABO group may be used.
42
BLOOD GROUP RED CELLS
PLASMA
Baby’s
Group
Mother’s
Group I Choice II Choice
A
A A O
A, AB B O
AB A O
O O
B
A O
B, AB B B O
AB B O
O O
AB
A A O
AB B B O
AB AB A, B, O
O O
O
A O
O, A, B, AB B O
AB O
O O
43
ABO haemolytic disease of the newborn
Clinically significant haemolysis generally occurs only if the mother is group O
and the infant group A (occasionally in group B babies).
Group O blood, compatible with the maternal plasma, should be used for
transfusion (level If an ET is required in ABO HDN, this should be with group O red
cells with low titre plasma anti-A and anti-B, or with group O red cells suspended in
AB plasma.
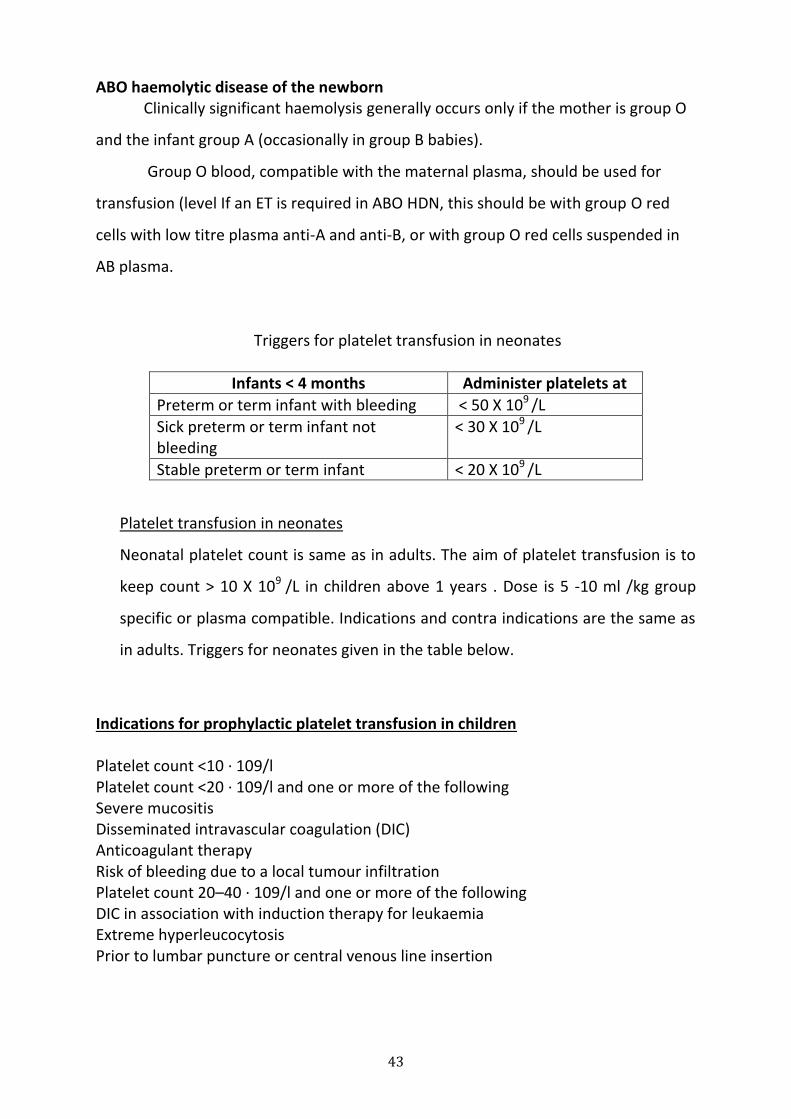
Triggers for platelet transfusion in neonates
Infants < 4 months Administer platelets at
Preterm or term infant with bleeding < 50 X 109 /L
Sick preterm or term infant not bleeding
< 30 X 109 /L
Stable preterm or term infant < 20 X 109 /L
Platelet transfusion in neonates
Neonatal platelet count is same as in adults. The aim of platelet transfusion is to
keep count > 10 X 109 /L in children above 1 years . Dose is 5 -10 ml /kg group
specific or plasma compatible. Indications and contra indications are the same as
in adults. Triggers for neonates given in the table below.
Indications for prophylactic platelet transfusion in children Platelet count <10 · 109/l Platelet count <20 · 109/l and one or more of the following Severe mucositis Disseminated intravascular coagulation (DIC) Anticoagulant therapy Risk of bleeding due to a local tumour infiltration Platelet count 20–40 · 109/l and one or more of the following DIC in association with induction therapy for leukaemia Extreme hyperleucocytosis Prior to lumbar puncture or central venous line insertion
44
8. Transfusion In Special Settings
Massive transfusion is the loss of more than one blood volume within 24 hours.
1. The aim of immediate resuscitation is to maintain adequate tissue oxygenation
through adequate numbers of circulating red cells.
2. Check the full blood count and coagulation screen regularly.
3. Maintain haemoglobin >8 g/dL.
4. Maintain INR and APTT ratio <1.5 with fresh frozen plasma at 15 mL/kg.
5. Maintain platelet count >50 × 109/L with platelet transfusion.
6. Maintain fibrinogen >1 g/L with cryoprecipitate.
7. Consider tranexamic acid 2–3 g.
Other possible complications of blood transfusion:
Hypocalcaemia. Calcium gluconate (2 mL of 10% solution per unit of blood)
when calcium concentration is low or there are clinical signs or ECG changes.
Hyperkalaemia may occur due to its high concentration (approximately 40
mmol/L) in stored blood. This is usually only a problemin those with hepatic or renal
disease.
Acid–base disturbances. Despite the presence of lactic acid in transfused blood fluid
resuscitation, this usually improves acidosis in shocked patients. Furthermore,
transfused citrate produces an alkalosis once it is metabolised. Hypothermia. Warm
patient and blood.
Disseminated Intravascular Coagulation
DIC is caused by a stimulus that leads to abnormal and constant thrombin
generation16. Many etiologies for DIC exist, but the most severe, acute cases of DIC
are obstetrically related. Causes of DIC in pregnant women include amniotic fluid
embolus, infection and retained products of conception. While clinicians search for
the underlying cause of the DIC, the blood bank must provide product support before
and after the underlying cause is treated.
45
In addition to thrombin generation, DIC also results in activation of the
fibrinolytic system and abnormal amounts of plasmin are generated16. Thrombin
converts fibrinogen to fibrin, and plasmin not only digests cross-linked fibrin clots,
but also destroys fibrinogen before it is converted to fibrin. Therefore, DIC results in
a rapid, and disproportionate reduction in fibrinogen levels relative to other clotting
factors. Treatment must include rapid replacement of fibrinogen, and cryoprecipitate
is the ideal blood product for this purpose.
Laboratory findings will show the hallmarks of DIC. Most notably, no
detectable fibrinogen and extremely high D-dimer levels.
DIC is one of the most feared clinical conditions facing Transfusion Medicine
Services. Severe, acute DIC is most commonly related to obstetrical cases and has a
high mortality rate. Successful treatment must be directed at the underlying cause
and the blood bank must focus on rapid replacement of fibrinogen. This is best
accomplished with the use of adequate amounts of cryoprecipitate. Plasma and
platelets will also be required to provide the factors not contained in cryoprecipitate.
Factor VIII Concentrate:
One unit factor VIII/kg body weight will result in an increase in plasma factor VIII
level by 2%. The level of factor VIII concentrate required to achieve adequate
haemostasis will depend on the type of bleeding, but can be calculated according to
the formula:
Units of factor VIII required = weight (kg) × desired level (%) × 0.5
The plasma half-life of factor VIII is 8–12 hours and thus repeated doses at 12-hourly
intervals are usually needed.
DDAVP: (for mild disease only – baseline factor VIII above 15%).
46
Mild haemophilia A should be treated with DDAVP (with or without
tranexamic acid) rather than coagulation factor concentrates where possible. DDAVP
(0.3g/kg body weight) is given intravenously, subcutaneously. Hyponatraemia and
water intoxication are side effects of this drug, and hence it is not recommended for
patients with cardiac failure or children under 2 years of age.
Factor IX Concentrate:
One unit factor IX/kg body weight will result in an increase in plasma factor IX level
by 0.8%. The plasma half-life of factor IX is 18–30 hours, and therefore if repeated
doses are needed, they should be given every 12–24 hours.
Dose: Units of factor IX required = weight (kg) × desired level (%) × 0.8
Treatment of patients with inhibitors
Recombinant – activated factor VIIa: (rFIIa)
rFVIIa is approved for haemophiliacs with inhibitors to factor VIII or IX. In addition
now, it is approved for the management of
acquired haemophilia
congenital FVII deficiency
Glanzmans thrombasthenia with antibodies to GP IIb / IIIa or HLA and with
platelet refractoriness.
rVIIa binds to activated platelets and tissue factor. Coagulation occurs locally at the
site of bleeding without disseminate activation. Dose is 90microgm/kg. Higher dose
upto 300 microgm/kg is clinically more efficacious. Due to short half life dosing
interval in treating bleeding episodes is 2 – 4 hours. There is no increased risk of
thromboembolism.
Prothrombin complex concentrates (PCCs) are plasma-derived intermediate
purity products containing coagulation factors IX, X and II, and sometimes factor VII.
They are used for the reversal of severe over anticoagulation and/or bleeding due to
47
treatment with vitamin K antagonists (reversal of warfarin). They are also used for
the treatment of the severe rare bleeding disorders of factor X and factor II
deficiency. PCCs are now being used in patients with liver failure. In liver disease
PCCs can correct only part of the overall haemostatic abnormality, and carry a risk of
provoking DIC. DIC can also occur in patients without liver disease who are treated
with repeated doses of PCCs. Activated PCCs are used as ‘bypassing agents’, as an
alternative to recombinant factor VIIa, for the treatment of patients with severe
haemophilia with an inhibitor.
VonWillebrand Disease:
Patients with type 1 disease, DDAVP is the treatment of choice and a dose of
0.3g/kg body weight is usually given intravenously or subcutaneously. These doses
give a two to fivefold increase in vWF and factor VIII levels. Tranexamic acid is often
given in vWD.
For patients with types 2 and 3 diseases, vWF ‘replacement therapy’ is
generally required. Factor VIII concentrate rich in vWF, e.g Humate P / Alphante or
similar preparations is the treatment of choice. The recommended treatment goals
are similar to Factor VIIIc.It may be necessary to give single first dose of purified FVIII
concentrate to ensure immediate correction of the low FVIII levels in Type 1 patients.
If specific preparations are not available, cryoprecipitate can be used at a dose of 1
donor unit / 10 kg patient body weight.
48
9. Modified Red Cell Components
A-Leuco-depleted red cell components:
Until recently, little attention was paid to the leukocytes present in various
blood components. However, it has been shown that the removal of leukocytes from
various blood products can minimize the risks associated with these contaminating
leukocytes.
106 WBCs (3-4 log) reduction of leukocytes can be achieved by filtration and
apheresis by approved cell separators. Buffy coat method of component preparation
by automated blood component extractor gives 108 WBCs (1 log reduction) and to a
great extent minimize the FNHTRs, but it is not effective for preventing HLA
alloimmunization.
Removal leukocytes below the threshold of < 5X106 in blood components
helps in prevention of alloimmunization. Leuko depletion can be achieved with the
help of 3 or 4 th generation leukofiltes 1) pre storage in the blood bank, 2) post
storage in the patients bed side and 3) collection blood components with approved
cell separator machine. Pre storage leuko rdepletion eliminates accumulation of
inflammatory cytokines (interleukin 1, interleukin 6, tumour necrosis factor) released
by leukocytes during storage. Pre storage leuko depletion is quite effective in the
prevention of febrile nonhaemolytic transfusion reaction. Hence, pre storage leuko
depletion is most widely accepted.
Clinical benefits of leukocyte reduction
Proven benefits clinically relevant
Reduced frequency and severity of FNHTRs
Reduced risk of CMV transmission
Reduced risk of HLA alloimmunization and platelet refractoriness
Probably clinically relevant
Reducd infectious risk associated with immunomodulation (TRIM)
Reduced organ dysfunction and mortality
Reduced direct risk of transfusion transmissible bacteria
49
Packed red cell selective pre storage leukofiltration policy can be adopted for
patients who receive multiple transfusions such as thalassemics, hemodialysis
patients, aplastic anemia and hemato-oncology patients to prevent febrile
transfusion reactions to standard products.Platelet concentrates can be pooled and
leukofilterd pre storage for select group of haemato oncology patients.
B-Irradiated blood products:
In order to minimize the risk of transfusion associated graft versus host disease in
susceptible individuals, cellular blood products (PRBC, platelets) should be irradiated
to a dose of 25 Gy prior to transfusion. Red cells, platelets and granulocyte
components must be irradiated for all at-risk patients. It is not necessary to irradiate
fresh frozen plasma, cryoprecipitate, cryosupernatant or plasma derivatives. It is not
necessary to irradiate components for patients with solid tumours, organ
transplants, HIV or aplastic anaemia. Patient groups who should receive irradiated
blood products are as follows:
Transfusions from first- or second-degree relatives
Any granulocyte transfusion for any recipient
HLA-selected platelet units
Patients receiving purine analogues (fludarabine, cladribine, deoxycoformycin):
probably safer to use indefinitely
Intrauterine transfusion (IUT)
Exchange transfusion (provided that irradiation does not unduly delay transfusion)
Red cell or platelet transfusion in neonates – only if there has been a previous IUT or
if blood is from first- or second-degree relative
All recipients of allogeneic haemopoietic stem cell (HSC) grafts, from start of
conditioning therapy and while patient remains on GvHD prophylaxis
Blood transfused to allogeneic HSC donors before or during the harvest of their HSC
Patients who will have autologous HSC graft:
50
• any transfusion within 7 days of the collection of their HSC
• any transfusion from the start of conditioning therapy until:
3 months post transplant
6 months post transplant if conditioning TBI has been given
Hodgkin’s disease, at all stages of the disease
Congenital immunodeficiency with defective cell-mediated immunity (e.g. SCID, Di
George syndrome, Wiskott Aldrich syndrome, purine nucleoside deficiency, reticular
dysgenesis, ADA, Ataxia telangectasia, chronic mucosal candidiasis,
MHC class 1 or 2 deficiency)
51
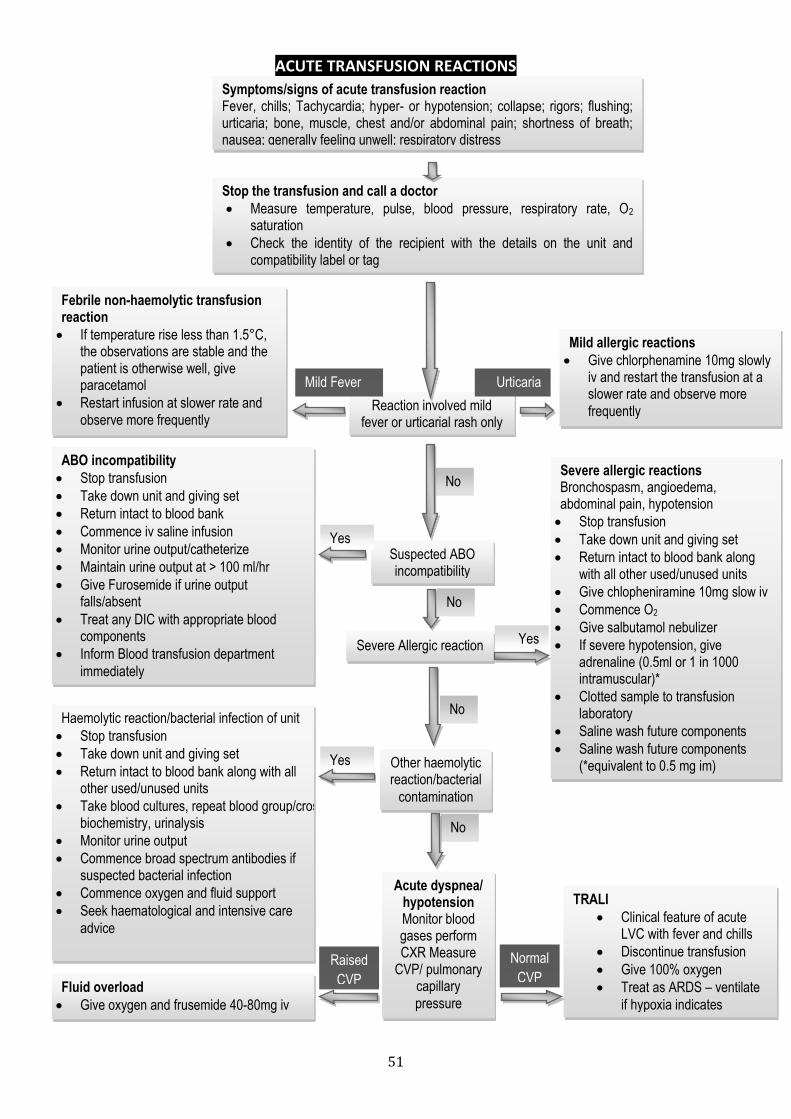
ACUTE TRANSFUSION REACTIONS
Symptoms/signs of acute transfusion reaction Fever, chills; Tachycardia; hyper- or hypotension; collapse; rigors; flushing; urticaria; bone, muscle, chest and/or abdominal pain; shortness of breath; nausea; generally feeling unwell; respiratory distress
Stop the transfusion and call a doctor Measure temperature, pulse, blood pressure, respiratory rate, O2
saturation
Check the identity of the recipient with the details on the unit and compatibility label or tag
Febrile non-haemolytic transfusion reaction If temperature rise less than 1.5°C,
the observations are stable and the patient is otherwise well, give paracetamol
Restart infusion at slower rate and observe more frequently
Mild allergic reactions Give chlorphenamine 10mg slowly
iv and restart the transfusion at a slower rate and observe more
frequently Reaction involved mild fever or urticarial rash only
Mild Fever Urticaria
ABO incompatibility Stop transfusion
Take down unit and giving set
Return intact to blood bank
Commence iv saline infusion
Monitor urine output/catheterize
Maintain urine output at > 100 ml/hr
Give Furosemide if urine output falls/absent
Treat any DIC with appropriate blood components
Inform Blood transfusion department
immediately
Haemolytic reaction/bacterial infection of unit
Stop transfusion
Take down unit and giving set
Return intact to blood bank along with all other used/unused units
Take blood cultures, repeat blood group/crossmatch/FBC, coagulation screen, biochemistry, urinalysis
Monitor urine output
Commence broad spectrum antibodies if suspected bacterial infection
Commence oxygen and fluid support
Seek haematological and intensive care
advice
Fluid overload Give oxygen and frusemide 40-80mg iv
Severe allergic reactions Bronchospasm, angioedema, abdominal pain, hypotension
Stop transfusion
Take down unit and giving set
Return intact to blood bank along with all other used/unused units
Give chlopheniramine 10mg slow iv
Commence O2
Give salbutamol nebulizer
If severe hypotension, give adrenaline (0.5ml or 1 in 1000 intramuscular)*
Clotted sample to transfusion laboratory
Saline wash future components
Saline wash future components (*equivalent to 0.5 mg im)
Suspected ABO incompatibility
No
Yes
Severe Allergic reaction
Other haemolytic reaction/bacterial
contamination
Acute dyspnea/ hypotension Monitor blood gases perform CXR Measure
CVP/ pulmonary capillary
pressure
TRALI Clinical feature of acute
LVC with fever and chills
Discontinue transfusion
Give 100% oxygen
Treat as ARDS – ventilate
if hypoxia indicates
No
Yes
No
No
Yes
Raised
CVP
Normal
CVP
52
10. Transfusion Reactions
1. Types of reactions:
Acute hemolytic transfusion reaction
These reactions are generally due to ABO mismatch. Clerical errors, such as
misidentification of the patient, failure to match the ABO type on the
blood bag label with the blood group on patient’s file are the most
common causes. Anxiety, loin pain, chest pain, dyspnea, tachycardia
(increase more than 20% from baseline) and hypotension (fall more than
20% from baseline) soon after starting the transfusion are the presenting
symptoms.
Febrile hemolytic reaction
These are the most frequent type of reaction characterized by an increase
of 1 C or more in the patient’s temperature. These reactions are most
commonly seen in multiply transfused patients and follow after platelet
transfusion. Cytokines generated during storage of blood components and
anti-leucocytes antibodies in the recipient are responsible for these
reactions.
Allergic or Urticarial reactions
They are characterized by development of hives or skin rash following
transfusion. They are thought to be due to hypersensitivity reaction to
plasma proteins. Rarely, these reactions can lead to anaphylaxis.
Septic reactions
Transfusion of bacterial contaminated blood products can result in a
profound shock with high degree fever. They are characterized by high
fever, vomiting, diarrhea and severe hypotension. Can be more common
with platelet transfusion, due to its storage temperature.
TRALI: Transfusion related acute lung injury
Delayed Hemolytic Transfusion
53
DHTR is most often the result of an anamnestic response in a patient who
has previously been sensitized by transfusion, pregnancy, or transplant and
in whom antibody is not detectable by standard pre transfusion methods.
Clinical signs and symptoms are usually mild; severe DHTR cases and
fatalities are uncommon, unexpected or unexplained decreases in
hemoglobin or hematocrit values following transfusion should be
investigated as a possible DHTR.
Common Antibodies implicated in DHTR
Anti-Jka, Anti-E, Anti-D, Anti-C, Anti-K, Anti-Fya, Anti-M
Clinical Signs and Symptoms of DHTR
Common Signs and symptoms Unusual Signs and symptoms
Fever Hemoglobinemia
Anemia Hemoglobinuria
Mild Jaundice Shock
Renal failure
2. Action to be taken in the event of a reaction.
STOP THE TRANSFUSION IMMEDIATELY. Keep the Intravenous line open
with normal saline infusion.
Report the event to Resident and Consultant to determine whether the
transfusion is to be only temporarily or permanently discontinued.
If the transfusion is to be discontinued permanently, preserve the blood
bag with administration set removing the needle.
Complete the Reaction Report sent along with compatibility form.
It is the responsibility of the Clinical resident in charge to completely fill all
the details in the reaction form such as, vitals of the patients both pre
transfusion and post transfusion, time of start of transfusion, presence of
fever before transfusion, time of occurrence of reaction, amount of blood
54
transfused, any drug administered during transfusion and signs and
symptoms associated with transfusion.
Withdraw from the patient from a different site of transfusion, 2 ml EDTA
blood sample and 5 ml clotted blood in plain vial; label it with name of the
patient, Hospital number and POST REACTION SAMPLE.
The time of withdrawal of sample is important. The post reaction sample
should be withdrawn as early as possible and sent to the blood bank for
investigation. Delaying may result in loss of important finding which may
again result in adverse event during transfusion in the patient when
transfused.
The blood bag should be sent along with the transfusion set attached.
Transfusion Reactions Investigation form is available in Blood bank.
Send blood sample, implicated blood unit with administration set and
Reaction Report to the blood bank immediately for evaluation.
After completion of investigation, the blood bank Resident will notify the
clinical services of the results, offer advice for further transfusion and
suggestions for management.
Clinical judgment should be used to decide what reactions to investigate
more fully. Aggressive investigations of mild reactions can burden
resources within the health care settings and may cause unnecessary delay
in transfusion therapy for a patient in critical need of blood products. All
Blood transfusion reactions however minor should be brought to the
notice of the blood bank. The following algorithm can be used as a guide
for managing transfusion reactions. Summary of Transfusion Reactions is
enclosed in Appendix.
55
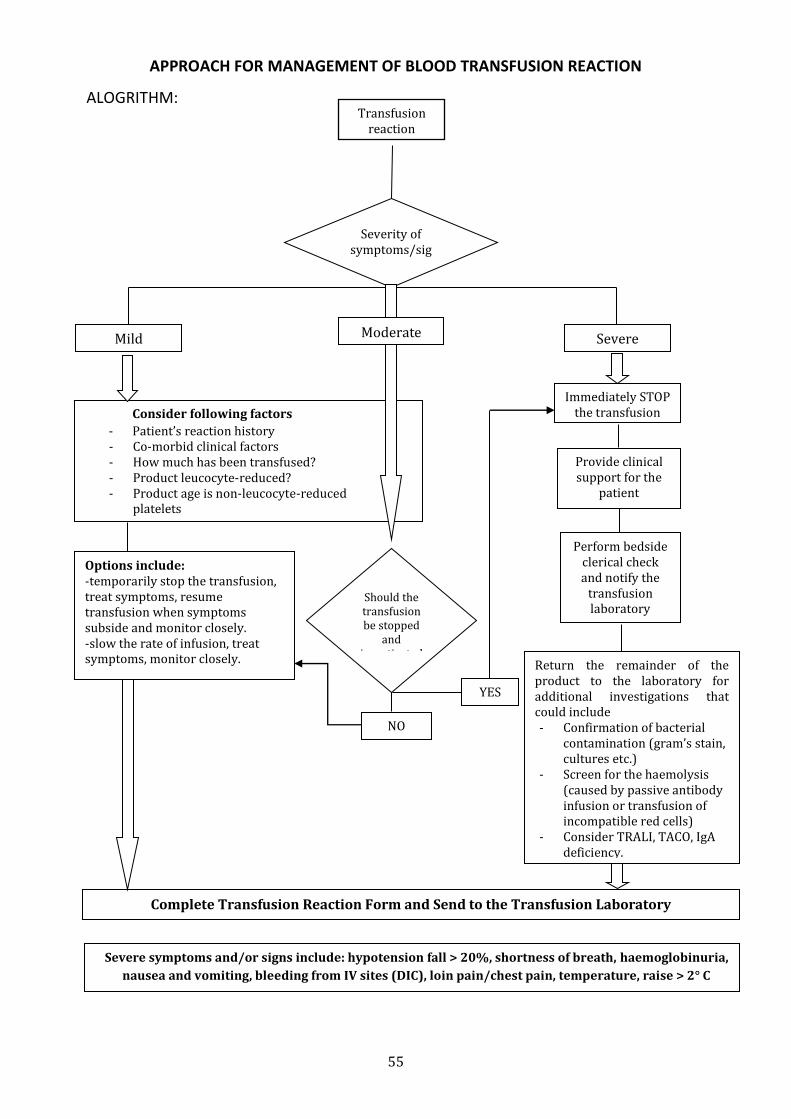
APPROACH FOR MANAGEMENT OF BLOOD TRANSFUSION REACTION
ALOGRITHM:
0. Transfusion
reaction
Severity of symptoms/sig
ns
Mild Severe
Consider following factors
- Patient’s reaction history - Co-morbid clinical factors - How much has been transfused? - Product leucocyte-reduced? - Product age is non-leucocyte-reduced
platelets
Immediately STOP the transfusion
Provide clinical support for the
patient
Perform bedside clerical check and notify the
transfusion laboratory
Should the transfusion be stopped
and investigated
NO
YES
Options include: -temporarily stop the transfusion, treat symptoms, resume transfusion when symptoms subside and monitor closely. -slow the rate of infusion, treat symptoms, monitor closely. Return the remainder of the
product to the laboratory for additional investigations that could include - Confirmation of bacterial
contamination (gram’s stain, cultures etc.)
- Screen for the haemolysis (caused by passive antibody infusion or transfusion of incompatible red cells)
- Consider TRALI, TACO, IgA deficiency.
Complete Transfusion Reaction Form and Send to the Transfusion Laboratory
Severe symptoms and/or signs include: hypotension fall > 20%, shortness of breath, haemoglobinuria,
nausea and vomiting, bleeding from IV sites (DIC), loin pain/chest pain, temperature, raise > 2° C
Moderate
56
11. Therapeutic Apheresis & Stem Cell Transplant
Therapeutic Plasma Exchange is performed for removal of circulating pathogenic
substance such as immune complexes, lipoproteins, toxins and antibodies. In this
procedure blood from patient is withdrawn anticoagulant added, separated in to
plasma and cellular components. The harmful plasma is discarded and replaced with
saline/FFP/albumin.
With one body plasma volume exchange 50% of pathogenic component is removed.
Hence, it is recommended that 40-50ml plasma/kg body weight should be removed in
one cycle, repeating the cycle 4 or 5 times over a period of 10-15 days. Plasma
exchange is a treatment of choice for TTP. The indications are given below:
Standard and acceptable indication for Therapeutic Plasma Exchange
1. Chronic inflammatory demyelinating polyneuropathy
2. Thrombotic thrombocytopenic purpura
3. Guillaian-Barre syndrome
4. Myasthenia gravis
5. Anti-GBM antibody disease (Goodpasture syndrome)
6. Hyperviscosity syndrome
7. Post transfusion purpura
8. Cryoglobulinemia
For carrying out Therapeutic Plasma Exchange prior intimation is necessary. The
clinical unit may contact Blood bank with request form duly filled in and signed by the
consultant. Therapeutic plasma exchange is not available for paediatric patients.
Haemotopoietic Stem Cells
Haemotopoietic Stem Cells can be obtained either from bone marrow or peripheral
blood. Peripheral blood stem cells (PBSC)are being increasingly used now. Using Cell
Separtors PBSC can be collected in a procedure lasting for 4 hours with venous access
without general anaethesia or hospitalization of donors.
57
Sources of PBSC
1. Allogenic
Another sibling
Unrelated adults
Cord blood cells
2. Syngeneic – Identical twins
3. Autologous
Indications for PSBC Treatment
Allogeneic
Acute myeloid leukaemia: high risk/relapsed
Acute lymphoblastic leukaemia: high risk/relapsed
Chronic myeloid leukaemia
Myelodysplastic syndromes
Aplastic anaemia
Thalassemia major
Primary immune defi ciencies Autologous
Acute myeloid leukaemia: high risk/relapsed
Non-Hodgkin’s lymphoma, high grade/relapsed
Hodgkin’s disease: relapsed
Multiple myeloma
Germ cell cancer: relapsed
Ewing’s sarcoma: high risk/relapsed
58
12. Good Blood Management Practice
The transfusion requirements in critical care (TRICC) study, the first and still
the most influential report on liberal transfusion policy delivered a clear conclusion –
improved patient survival was associated with a more restrictive transfusion regime.
This randomized trial of patients in intensive care showed that less severely ill patients
(Acute Physiology and Chronic Health Evaluation II score _<20) and patients under 55
years actually had a survival advantage if the Hb was maintained between 7 and 9 g/dL
rather than between 10 and 12 g/dl. For patients with clinically significant cardiac
disease the mortality was similar in both groups.
Three large retrospective studies have shown that receiving a perioperative
blood transfusion is an independent risk factor for short and long term survival
following cardiac surgery and avoiding transfusion could offer at least 5% improved
survival.
Perioperative correction of anaemia, intraoperative blood avoidance
interventions and a scrupulous attention to bloodless surgical technique must become
the standard of care.
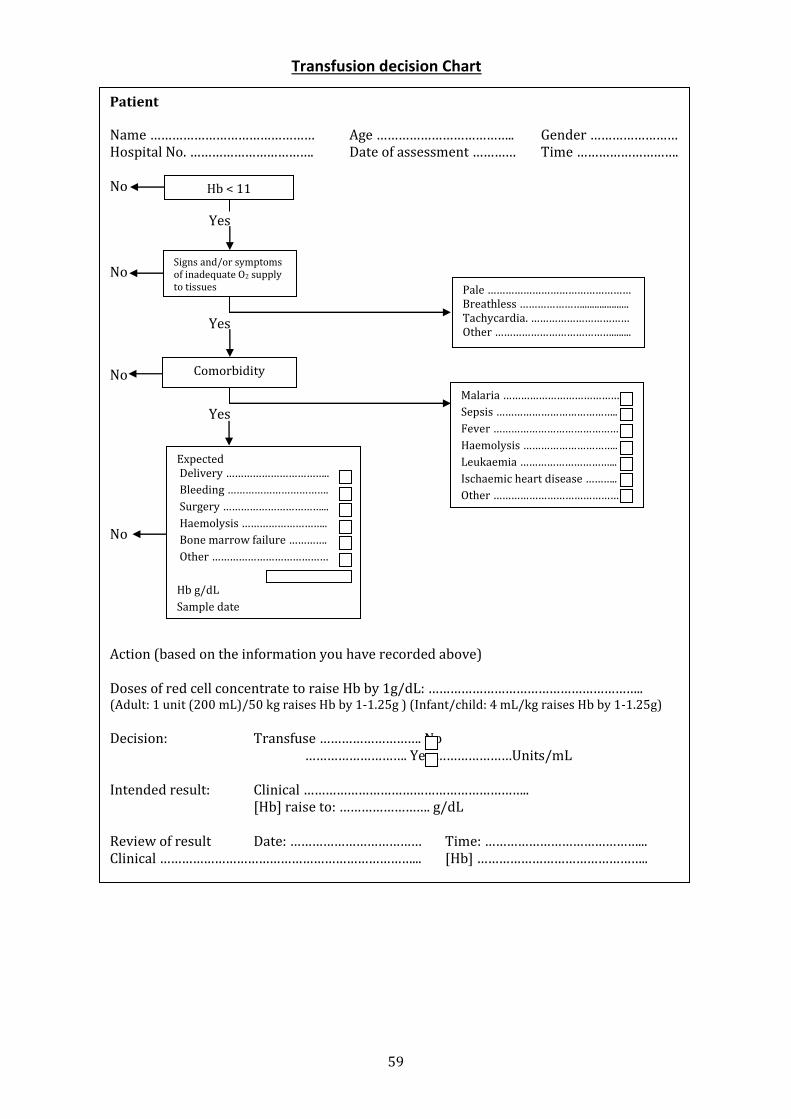
The reasons for transfusion of blood should be recorded and review every
transfusion later on. This will enable efficient use of blood / blood components
transfusion for the benefit of patient. The model chart given below can be used.
59
Transfusion decision Chart
Patient
Name ……………………………………… Age ……………………………….. Gender …………………… Hospital No. ……………………………. Date of assessment ………… Time ………………………. No Yes No Yes No
Yes No Action (based on the information you have recorded above) Doses of red cell concentrate to raise Hb by 1g/dL: ………………………………………………….. (Adult: 1 unit (200 mL)/50 kg raises Hb by 1-1.25g ) (Infant/child: 4 mL/kg raises Hb by 1-1.25g)
Decision: Transfuse ………………………. No ………………………. Yes …………………Units/mL Intended result: Clinical …………………………………………………….. [Hb] raise to: ……………………. g/dL Review of result Date: ……………………………… Time: ……………………………………... Clinical ……………………………………………………………... [Hb] ………………………………………..
Hb < 11
Signs and/or symptoms of inadequate O2 supply to tissues Pale …………………………………………
Breathless …………………................... Tachycardia. …………………………… Other …………………………………........
Expected Delivery ……………………………..
Bleeding …………………………….
Surgery ……………………………...
Haemolysis ………………………..
Bone marrow failure ………….
Other …………………………………
Hb g/dL
Sample date ………………………………..
Comorbidity
Malaria …………………………………
Sepsis …………………………………..
Fever ……………………………………
Haemolysis …………………………..
Leukaemia …………………………...
Ischaemic heart disease ………..
Other ……………………………………
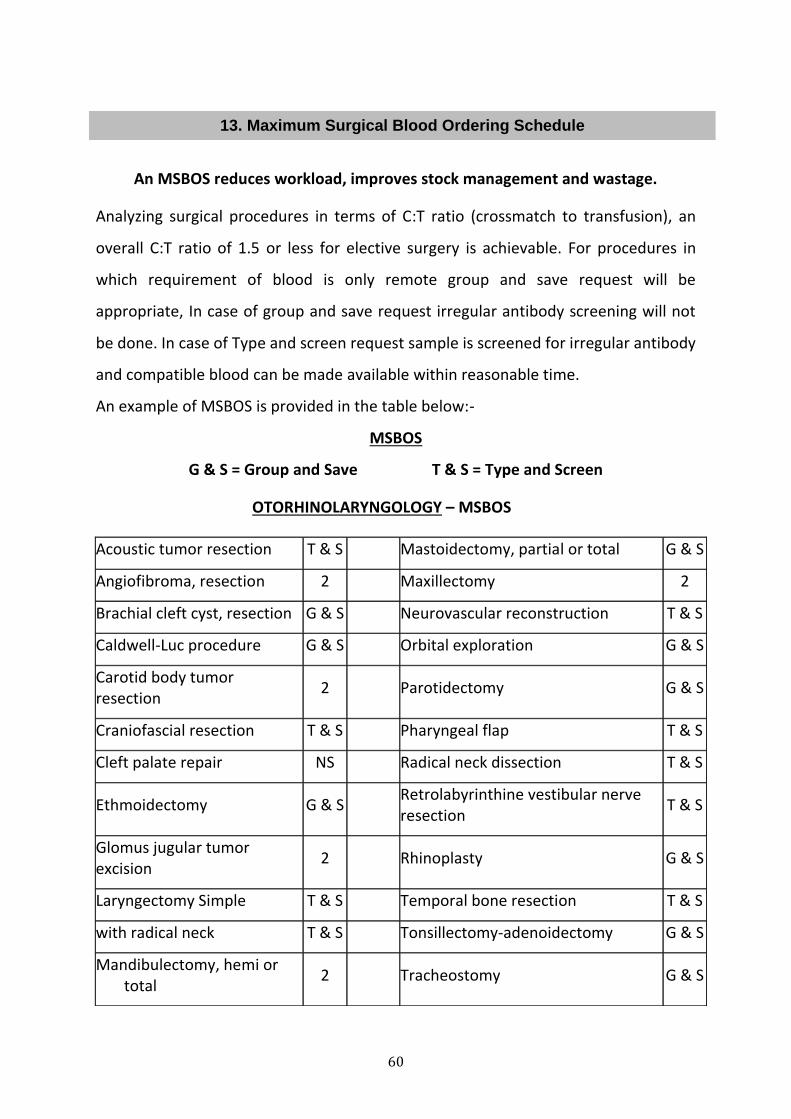
60
13. Maximum Surgical Blood Ordering Schedule
An MSBOS reduces workload, improves stock management and wastage.
Analyzing surgical procedures in terms of C:T ratio (crossmatch to transfusion), an
overall C:T ratio of 1.5 or less for elective surgery is achievable. For procedures in
which requirement of blood is only remote group and save request will be
appropriate, In case of group and save request irregular antibody screening will not
be done. In case of Type and screen request sample is screened for irregular antibody
and compatible blood can be made available within reasonable time.
An example of MSBOS is provided in the table below:-
MSBOS
G & S = Group and Save T & S = Type and Screen
OTORHINOLARYNGOLOGY – MSBOS
Acoustic tumor resection T & S Mastoidectomy, partial or total G & S
Angiofibroma, resection 2 Maxillectomy 2
Brachial cleft cyst, resection G & S Neurovascular reconstruction T & S
Caldwell-Luc procedure G & S Orbital exploration G & S
Carotid body tumor resection
2 Parotidectomy G & S
Craniofascial resection T & S Pharyngeal flap T & S
Cleft palate repair NS Radical neck dissection T & S
Ethmoidectomy G & S Retrolabyrinthine vestibular nerve resection
T & S
Glomus jugular tumor excision
2 Rhinoplasty G & S
Laryngectomy Simple T & S Temporal bone resection T & S
with radical neck T & S Tonsillectomy-adenoidectomy G & S
Mandibulectomy, hemi or total
2 Tracheostomy G & S
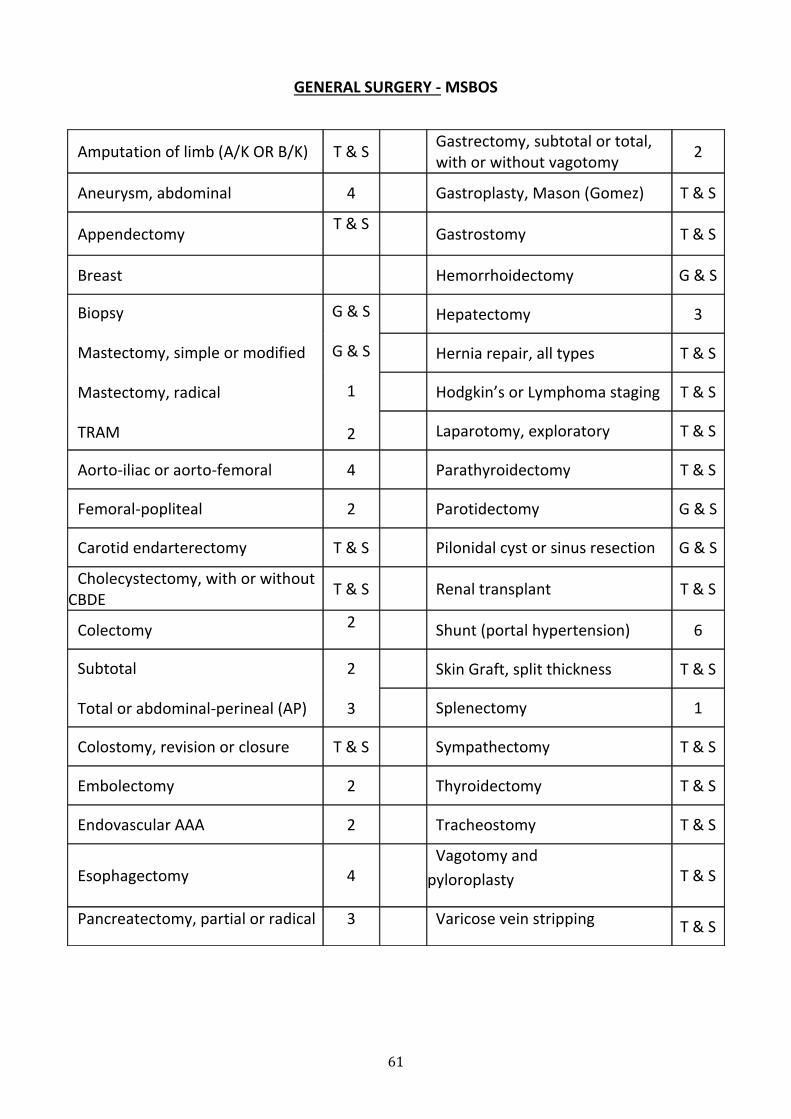
61
GENERAL SURGERY - MSBOS
Amputation of limb (A/K OR B/K) T & S Gastrectomy, subtotal or total, with or without vagotomy
2
Aneurysm, abdominal 4 Gastroplasty, Mason (Gomez) T & S
Appendectomy T & S
Gastrostomy T & S
Breast Hemorrhoidectomy G & S
Biopsy
Mastectomy, simple or modified
Mastectomy, radical
TRAM
G & S
G & S
1
2
Hepatectomy 3
Hernia repair, all types T & S
Hodgkin’s or Lymphoma staging T & S
Laparotomy, exploratory T & S
Aorto-iliac or aorto-femoral 4 Parathyroidectomy T & S
Femoral-popliteal 2 Parotidectomy G & S
Carotid endarterectomy T & S Pilonidal cyst or sinus resection G & S
Cholecystectomy, with or without CBDE
T & S Renal transplant T & S
Colectomy 2 Shunt (portal hypertension) 6
Subtotal
Total or abdominal-perineal (AP)
2
3
Skin Graft, split thickness T & S
Splenectomy 1
Colostomy, revision or closure T & S Sympathectomy T & S
Embolectomy 2 Thyroidectomy T & S
Endovascular AAA 2 Tracheostomy T & S
Esophagectomy 4 Vagotomy and
pyloroplasty T & S
Pancreatectomy, partial or radical 3 Varicose vein stripping T & S
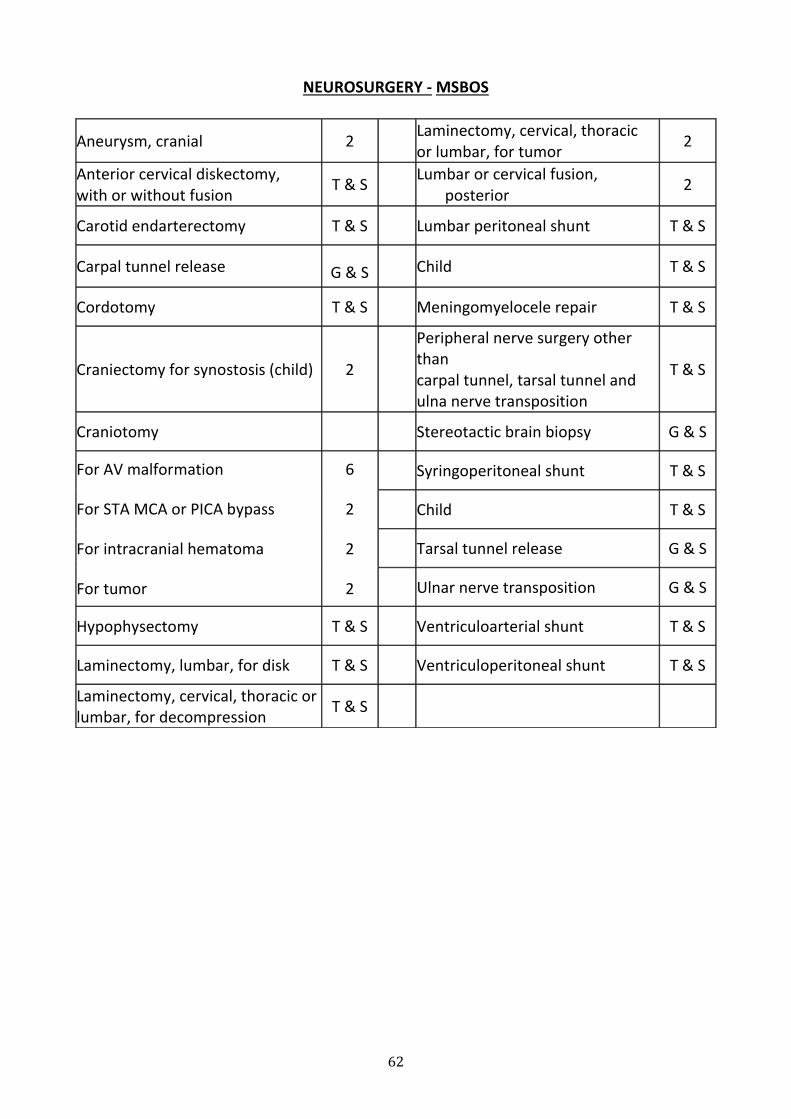
62
NEUROSURGERY - MSBOS
Aneurysm, cranial 2 Laminectomy, cervical, thoracic or lumbar, for tumor
2
Anterior cervical diskectomy, with or without fusion
T & S Lumbar or cervical fusion, posterior
2
Carotid endarterectomy T & S Lumbar peritoneal shunt T & S
Carpal tunnel release G & S Child T & S
Cordotomy T & S Meningomyelocele repair T & S
Craniectomy for synostosis (child) 2
Peripheral nerve surgery other than carpal tunnel, tarsal tunnel and ulna nerve transposition
T & S
Craniotomy Stereotactic brain biopsy G & S
For AV malformation
For STA MCA or PICA bypass
For intracranial hematoma
For tumor
6
2
2
2
Syringoperitoneal shunt T & S
Child T & S
Tarsal tunnel release G & S
Ulnar nerve transposition G & S
Hypophysectomy T & S Ventriculoarterial shunt T & S
Laminectomy, lumbar, for disk T & S Ventriculoperitoneal shunt T & S
Laminectomy, cervical, thoracic or lumbar, for decompression
T & S
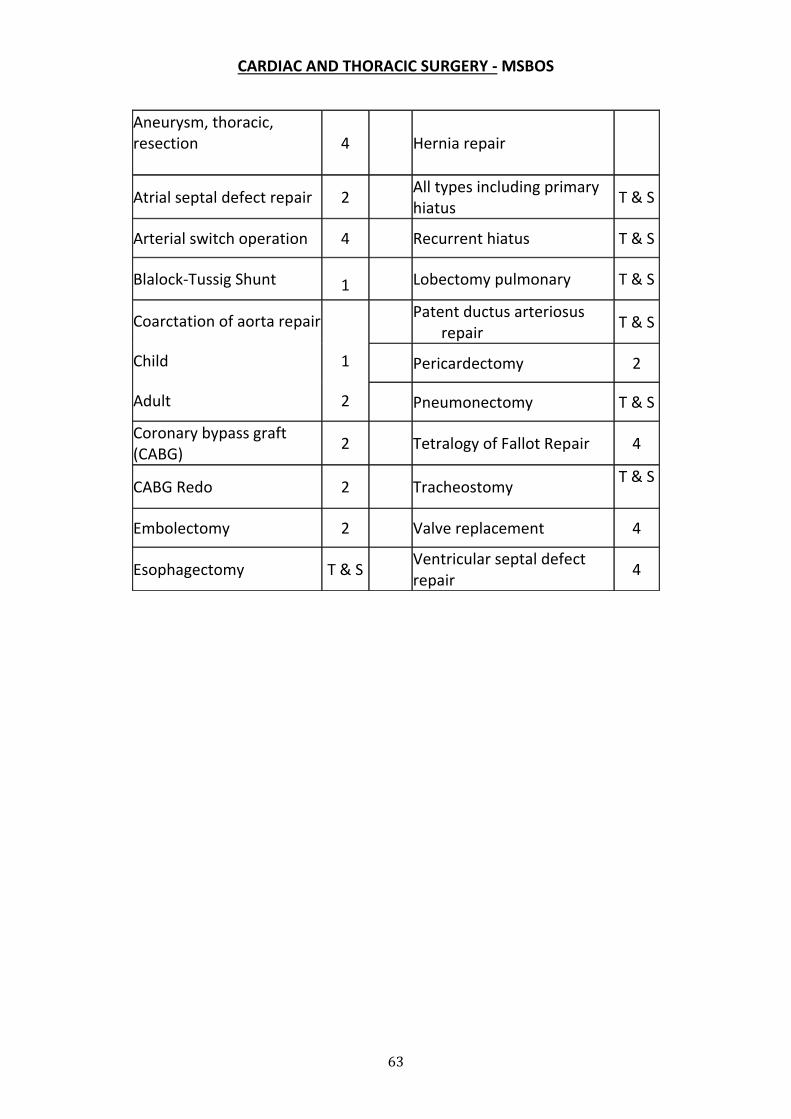
63
CARDIAC AND THORACIC SURGERY - MSBOS
Aneurysm, thoracic, resection
4 Hernia repair
Atrial septal defect repair 2 All types including primary hiatus
T & S
Arterial switch operation 4 Recurrent hiatus T & S
Blalock-Tussig Shunt 1 Lobectomy pulmonary T & S
Coarctation of aorta repair
Child
Adult
1
2
Patent ductus arteriosus repair
T & S
Pericardectomy 2
Pneumonectomy T & S
Coronary bypass graft (CABG)
2 Tetralogy of Fallot Repair 4
CABG Redo 2 Tracheostomy T & S
Embolectomy 2 Valve replacement 4
Esophagectomy T & S Ventricular septal defect repair
4
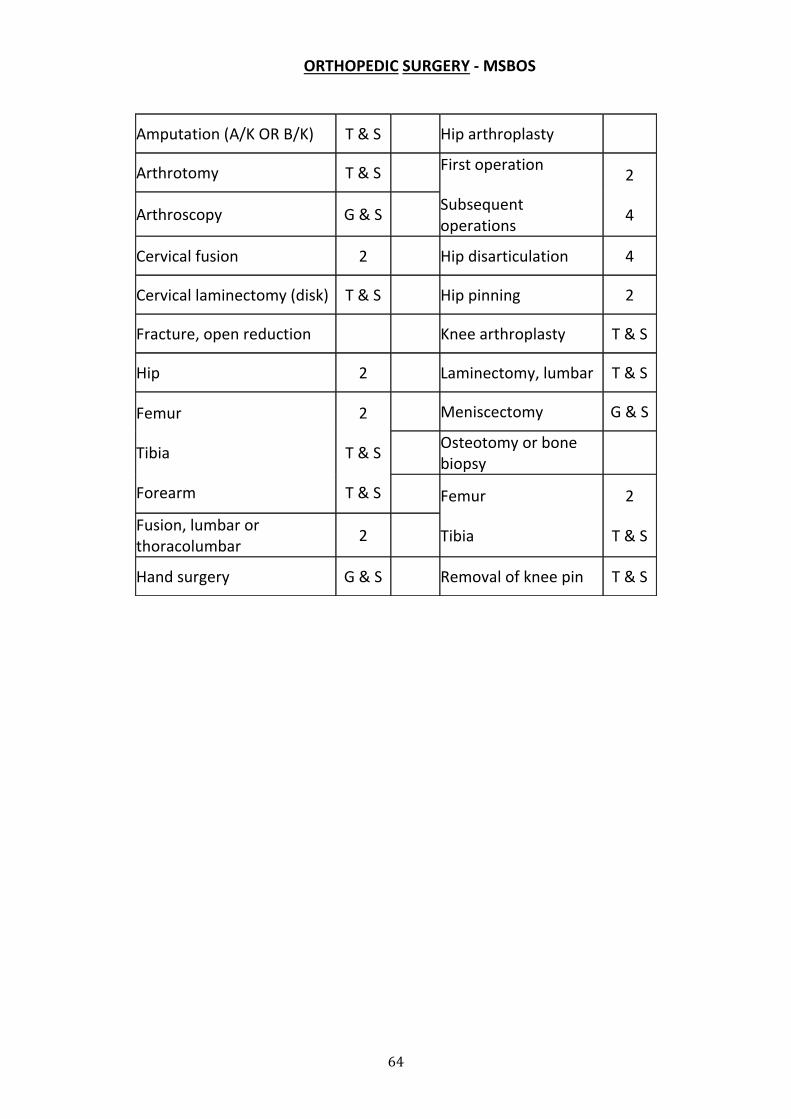
64
ORTHOPEDIC SURGERY - MSBOS
Amputation (A/K OR B/K) T & S Hip arthroplasty
Arthrotomy T & S First operation
Subsequent operations
2
4 Arthroscopy G & S
Cervical fusion 2 Hip disarticulation 4
Cervical laminectomy (disk) T & S Hip pinning 2
Fracture, open reduction Knee arthroplasty T & S
Hip 2 Laminectomy, lumbar T & S
Femur
Tibia
Forearm
2
T & S
T & S
Meniscectomy G & S
Osteotomy or bone biopsy
Femur
Tibia
2
T & S Fusion, lumbar or thoracolumbar
2
Hand surgery G & S Removal of knee pin T & S
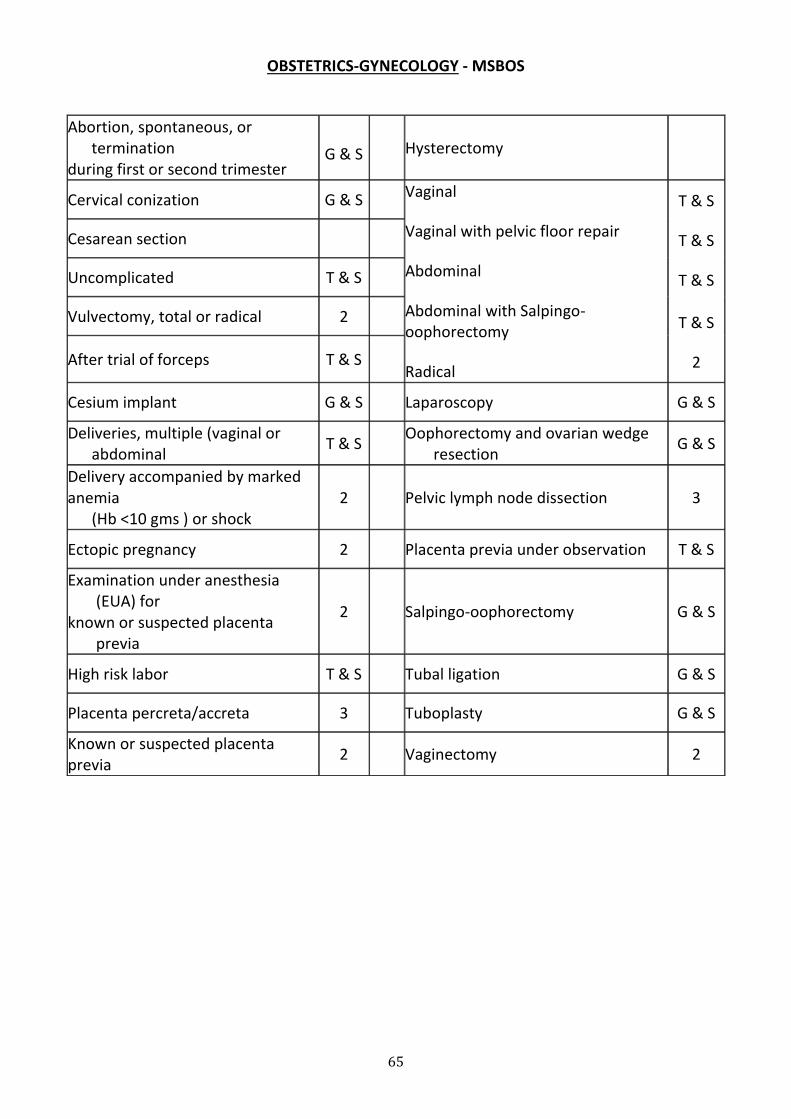
65
OBSTETRICS-GYNECOLOGY - MSBOS
Abortion, spontaneous, or termination
during first or second trimester G & S
Hysterectomy
Cervical conization G & S Vaginal
Vaginal with pelvic floor repair
Abdominal
Abdominal with Salpingo-oophorectomy
Radical
T & S
T & S
T & S
T & S
2
Cesarean section
Uncomplicated T & S
Vulvectomy, total or radical 2
After trial of forceps T & S
Cesium implant G & S Laparoscopy G & S
Deliveries, multiple (vaginal or abdominal
T & S Oophorectomy and ovarian wedge resection
G & S
Delivery accompanied by marked anemia
(Hb <10 gms ) or shock 2 Pelvic lymph node dissection 3
Ectopic pregnancy 2 Placenta previa under observation T & S
Examination under anesthesia (EUA) for
known or suspected placenta previa
2 Salpingo-oophorectomy G & S
High risk labor T & S Tubal ligation G & S
Placenta percreta/accreta 3 Tuboplasty G & S
Known or suspected placenta previa
2 Vaginectomy 2
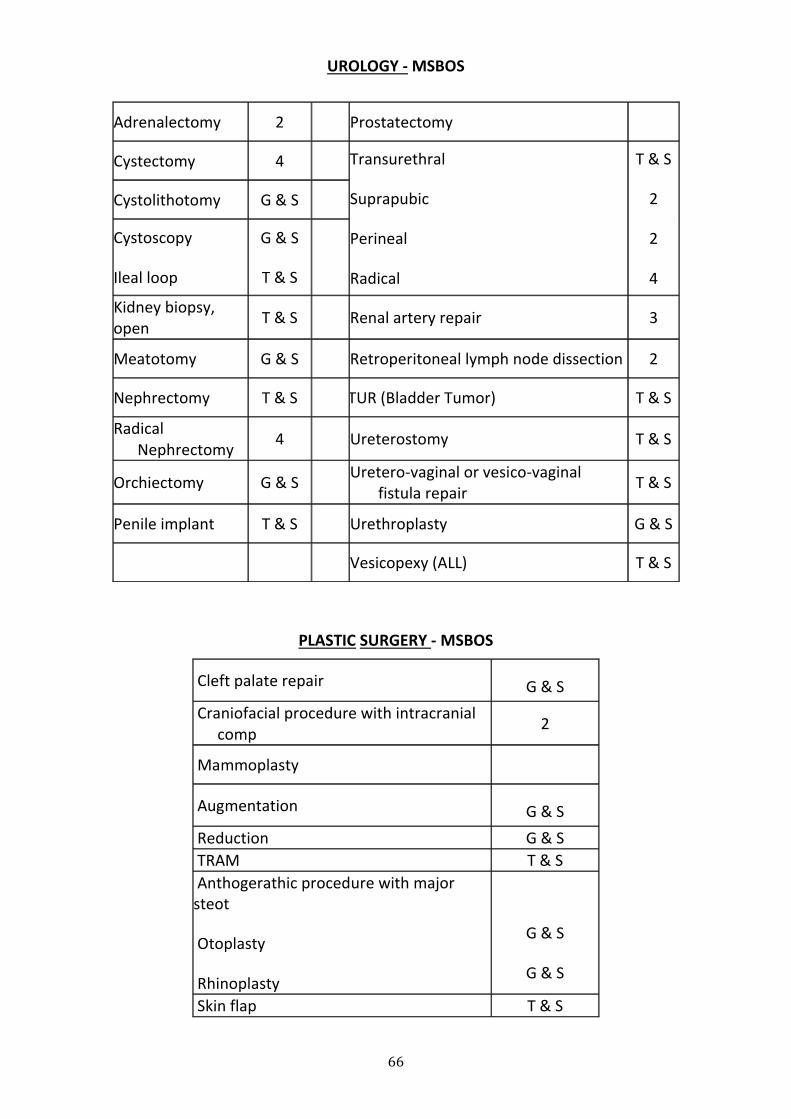
66
UROLOGY - MSBOS
PLASTIC SURGERY - MSBOS
Cleft palate repair G & S
Craniofacial procedure with intracranial comp
2
Mammoplasty
Augmentation G & S
Reduction G & S
TRAM T & S
Anthogerathic procedure with major steot
Otoplasty
Rhinoplasty
G & S
G & S
Skin flap T & S
Adrenalectomy 2 Prostatectomy
Cystectomy 4 Transurethral
Suprapubic
Perineal
Radical
T & S
2
2
4
Cystolithotomy G & S
Cystoscopy
Ileal loop
G & S
T & S
Kidney biopsy, open
T & S Renal artery repair 3
Meatotomy G & S Retroperitoneal lymph node dissection 2
Nephrectomy T & S TUR (Bladder Tumor) T & S
Radical Nephrectomy
4 Ureterostomy T & S
Orchiectomy G & S Uretero-vaginal or vesico-vaginal fistula repair
T & S
Penile implant T & S Urethroplasty G & S
Vesicopexy (ALL) T & S
67
14. BIOSAFETY
1. All blood and blood components are to be considered potentially infectious
and Universal Precautions must be observed during handling of blood unit.
2. Discard the empty blood component bag in the Biohazard Waste Container in
the Ward, unless the patient has suffered from adverse reaction, then the
blood bag has to returned to the blood bank
3. If there is blood spillage, treat it as per the standard guidelines. Disinfect
blood spillage with 10% sodium hypochlorite solution. At least 30 minutes
should be allowed for hypochlorite solution to act during which spillage is
covered with gauze cloth soaked in hypochlorite.
4. All needles should be destroyed in the needle cutter and used syringes are
destroyed appropriately before discarding.
5. The sharps and needles should be discarded in a puncture proof container.
References:
1. Michael F. Murphy and Derwood H. Pamphilon (ed.). Practical Transfusion
Medicine,2009;
2. Morcela Contreras (ed.). ABC of Transfusion, 4th edition
3. Resident Manual, SGPGI, Lucknow.
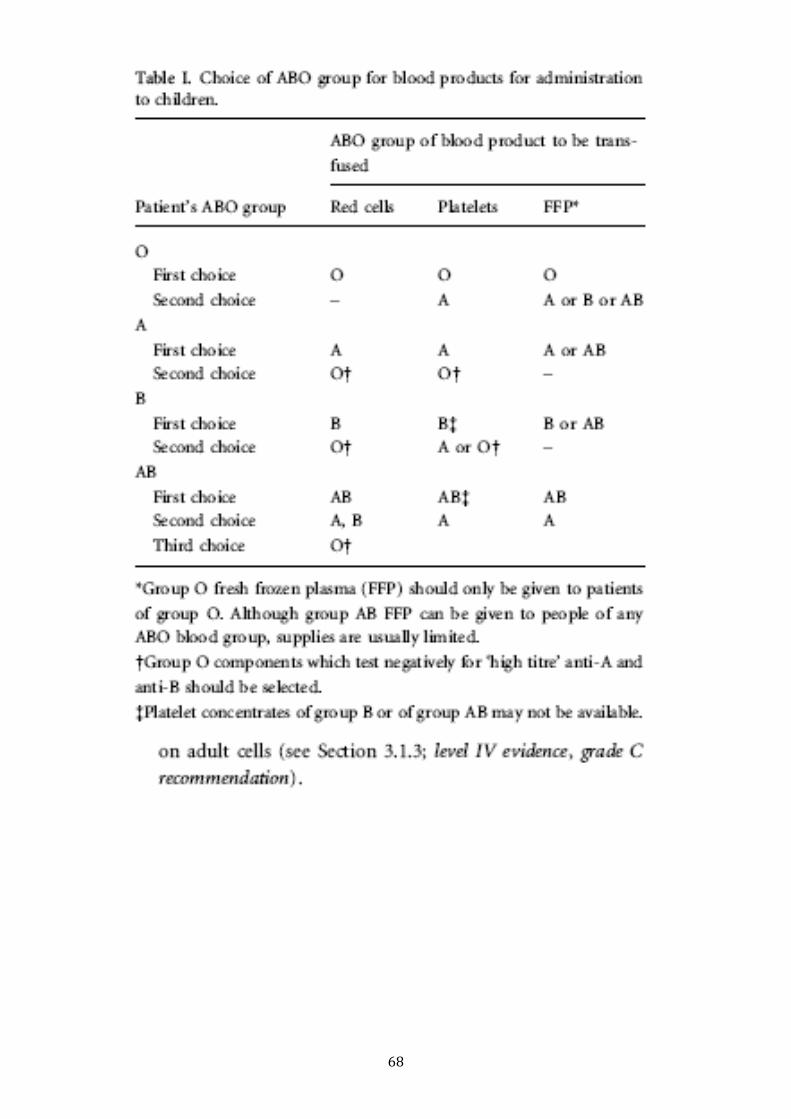
68





























