Embed Size (px)
Citation preview

DEPRESSION AND ANXIETY 32:383–391 (2015)
ReviewQUANTITATIVE EVALUATION OF THE CLINICALEFFICACY OF ATTENTION BIAS MODIFICATION
TREATMENT FOR ANXIETY DISORDERS
Marian Linetzky, M.A.,1∗ Lee Pergamin-Hight, M.A.,1 Daniel S. Pine, M.D.,2 and Yair Bar-Haim, Ph.D.1,3
Background: Attention bias modification treatment (ABMT) is a novel treat-ment for anxiety disorders. Although a number of other meta-analytic reviewsexist, the purpose of the present meta-analysis is to examine issues unaddressedin prior reviews. Specifically, the review estimates the efficacy of ABMT inclinically anxious patients and examines the effect of delivery context (clinicvs. home) on symptom reduction. Methods: A literature search using Psych-Info and Web of Science databases was performed. Only randomized controlledtrials (RCTs) examining dot-probe-based ABMT in clinically diagnosed anx-ious patients were included. From 714 articles located through the search,36 ABMT studies were identified and 11 studies met inclusion criteria (N= 589 patients). Results: ABMT was associated with greater clinician-ratedreductions in anxiety symptoms relative to control training: between-groupseffect (d = 0.42, P = .001, confidence interval (CI) = 0.18–0.66), contrastof within-group effects (Q = 7.25, P < .01). More patients in the treatmentgroup no longer met formal diagnostic criteria for their anxiety disorder post-treatment relative to patients in the control condition (P < .05). Analyses ofpatients’ self-reported anxiety were nonsignificant for the between-groups con-trast (P = .35), and were at a trend level of significance for the contrast be-tween the within-group effects (P = .06). Moderation analysis of the between-groups effect revealed a significant effect for ABMT delivered in the clinic(d = 0.34, P = 0.01, CI = 0.07–0.62), and a nonsignificant effect for ABMTdelivered at home (d = −0.10, P = 0.40, CI = −0.33–0.13). Conclusions: Thecurrent meta-analysis provides support for ABMT as a novel evidenced-basedtreatment for anxiety disorders. Overall, ABMT effects are mainly evident whenit is delivered in the clinic and when clinical outcome is evaluated by a clinician.More RCTs of ABMT in specific anxiety disorders are warranted. Depressionand Anxiety 32:383–391, 2015. C© 2015 Wiley Periodicals, Inc.
Key words: anxiety; anxiety disorders; clinical trials; treatment; cognition; com-puter; Internet technology
INTRODUCTIONAttention bias modification treatment (ABMT) foranxiety disorders grew out of data on threat-related
1School of Psychological Sciences, Tel Aviv University, TelAviv, Israel2Section on Development and Affective Neuroscience, Emo-tion and Development Branch, Intramural Research Program,National Institute of Mental Health, Bethesda, Maryland3The Sagol School of Neuroscience, Tel Aviv University, TelAviv, Israel
This research was supported by Grant No 01014599 from theUnited States-Israel Binational Science Foundation (BSF).
∗Correspondence to: Marian Linetzky, School of psychological sci-ences, Tel Aviv University, Tel Aviv 69978, Israel.E-mail: [email protected] for publication 31 July 2014; Revised 2 November 2014;Accepted 30 November 2014
DOI 10.1002/da.22344Published online 24 February 2015 in Wiley Online Library(wileyonlinelibrary.com).
C© 2015 Wiley Periodicals, Inc.

384 Linetzky et al.
attentional biases in anxiety.[1, 2] ABMT utilizescomputer-based attention training protocols to implic-itly modify biased attentional patterns in anxious indi-viduals. Much of the anxiety-related research on ABMThas been conducted within the framework of experimen-tal psychopathology, mostly conducted with volunteersfree of symptoms or in subclinical populations (e.g., El-dar and Bar-haim;[3] Dandeneau et al.;[4] but see Heerenet al.[5]). This work has applied various adaptations ofmultiple cognitive tasks (Dandeneau et al.;[4] Bar-Haimet al.;[6] Waters et al.[7]).
Four published meta-analyses have examined the ef-fects of attention bias modification on symptoms, asa group reporting small-to-medium effect sizes.[8–11]
However, each of these meta-analyses reports a varietyof effects and moderator analyses that are based on di-verse inclusion criteria in terms of psychiatric disorders(e.g., anxiety disorders, depression, substance abuse), tar-get populations (clinical, subclinical, healthy), cognitivetasks utilized to modify attention bias (e.g., dot-probe,spatial cueing, visual search), or context of ABMT de-livery (e.g., laboratory, over the Internet). Clearly, theextant corpus of ABMT research and its previous meta-analytic reviews played an important role in elucidat-ing potential mechanisms and boundary conditions ofABMT. However, prior reviews do not focus specificallyon results in clinically affected patients. As a result, noreview provides a direct meta-analytic test of the utilityof ABMT as a stand-alone treatment for clinical anxietydisorders. Such information can only be derived from aspecific analysis of randomized controlled trials (RCTs)of ABMT in clinically diagnosed anxiety patients thatcollected standardized data on anxiety symptoms beforeand after treatment. Only one ABMT type, based on thedot-probe task, generates sufficient data from RCTs tosupport a meaningful meta-analysis of the efficacy of aspecific treatment protocol. Surely, the previous meta-analyses address such specifications by considering typeof task or clinical status as moderators.[8–11] However,these moderators were tested either across varied pop-ulations (e.g., clinical and nonclinical), or aggregatedacross different ABMT tasks (e.g., dot-probe, spatialcueing, visual search). Thus, the efficacy of ABMT forclinical anxiety disorders using one standardized ABMTtechnique (i.e., the dot-probe) remains unreported.For instance, even in the careful, thorough review byMogoese et al., where most relevant moderators weretested, the single, most critical effect size, from stud-ies in patients, was not reported. That is, when testingfor the effect of clinical versus subclinical population,nondot-probe studies were included. Furthermore, allother moderators, such as task-type or delivery setting,were aggregated across clinical and subclinical popula-tions.
Twelve RCTs of ABMT in clinically diagnosed anx-iety patients were published to date. Eleven of theseRCTs used variants of the dot-probe task as means ofattention bias modification (cf. Waters et al.[7]).[12–22]
Here, we provide a meta-analysis of these 11 dot-
probe-based RCTs estimating the combined effect sizesof between-groups effects, indicative of the effects ofABMT above and beyond placebo training protocols;as well as contrasting combined within-group effects,providing an overall estimate of the magnitude of treat-ment effects. To provide a direct estimate of the effi-cacy of ABMT for anxiety disorders in what appears tobe the most evidence-grounded treatment protocol, weonly include studies: (1) with formally diagnosed anxietypatients; (2) using RCT designs; (3) exclusively target-ing threat-related attention patterns; (4) assessing clini-cal symptoms before and after treatment; and (5) usingthe dot-probe task for attention bias modification. Be-cause some of the more recent RCTs used internet deliv-ery of ABMT rather than the more classic in-clinic/labsettings, we also examined delivery context (clinic vs.home) as a moderator for the effect of ABMT on anxietysymptoms.
METHODLITERATURE SEARCH AND INCLUSIONCRITERIA
Studies were searched using PsychInfo and Web of Sciencedatabases with the keywords "attentional training" or "attention mod-ification" and anxiety. In addition, the references lists of publishedmeta-analyses on ABM were systematically reviewed, and a search ofpublications by leading researchers in the field was also conducted.Studies were selected using the following inclusion criteria: (1) thestudy was published in the English language prior to January 2014; (2)the participants were formally diagnosed with a primary anxiety dis-order according to DSM criteria; (3) the study delivered ABMT usingthe dot-probe task; (4) the study investigated the impact of ABMT ina randomized double-blind controlled trial (RCT); and (5) the studyreported data on the impact of ABMT on anxiety that allowed a com-putation of an effect size (i.e., reported data on anxiety symptoms col-lected before and after treatment). Finally, studies that administeredABMT alongside another intervention such as cognitive behavioraltherapy (CBT) were excluded.[23]
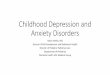
The initial search yielded 714 articles, from which 36 were identifiedas potentially eligible for inclusion in the meta-analysis. Eleven studiesmet the inclusion criteria collectively reflecting an accumulation of 589participants across samples. A flow diagram of samples selection as wellas number and reasons for exclusions are provided in Fig. 1.
DATA EXTRACTION AND META-ANALYTICPROCEDURES
Means, standard deviations or standard errors, and F, t, andP values were extracted from the text and tables of the included pa-pers to generate Cohen’s d effect size index for both between-groupseffects and within-groups effects. For the between-groups effect (ABMTvs. control), we computed the difference in means between the twoconditions at posttreatment divided by their pooled standard devia-tion, for posttreatment assessment and, if available, also for follow-upassessment. Positive values reflect greater improvement in symptomsor reduction in bias scores in the ABMT condition compared to thecontrol condition. Negative d values reflect the opposite pattern. Toestimate within-group treatment effects, we computed Cohen’s d as thedifference in means from pre- to posttreatment or from pretreatmentto follow-up within each group (ABMT, control), divided by the stan-dard deviation of the measurement before treatment.[24] Positive values
Depression and Anxiety

Review: ABMT for Anxiety Disorders: A Meta-Analysis 385
Figure 1. Flow diagram of sample selection process.
reflect reduction in symptoms or attention bias scores over time,whereas negative values reflect the opposite patterns. Q-tests were usedto compare the magnitudes of these two within-group effects. The ef-fect of ABMT delivery context as a moderator was evaluated using theQ-test for within-group contrasts.
To estimate the potential magnitude of a “file-drawer problem,”fail-safe numbers were computed for main effects, representing thenumber of studies with average sample size and nonsignificant out-comes that would be required to bring the combined effect size ofthe meta-analysis down to a nonsignificance level.[25] Further consid-eration of the possible impact of publication bias (e.g., trim-and-fillmethod) was not possible due to the small number of samples. [26]
All analyses were carried out using the Comprehensive Meta-Analysis software, version 2.002 (Biostat, Englewood, NJ). Becausethe extracted data were heterogeneous, effect sizes were calculated inthe context of random effects model, which is also considered to bemore conservative than fixed effect model.
OUTCOMESThe effect of ABMT on anxiety symptoms was estimated for
three types of outcomes: (1) clinician-rated measures; (2) self-reported
measures; and (3) change in diagnostic status (i.e., number of pa-tients no longer meeting criteria for their primary anxiety diagnosis).We also evaluated treatment effects on attention bias scores and onself-reported depression. To enhance consistency, when studies usedmore than one measurement scale in one of the above-described out-come types, we selected the scale typically considered the “gold stan-dard” measure for the specific disorder. For example, we used theLiebowitz Social Anxiety Scale (LSAS[27]) in studies of social anxietydisorder (SAD), Spielberger’s Trait Anxiety Inventory (STAI-T[28]) instudies of generalized anxiety disorder (GAD), and the Beck Depres-sion Inventory (BDI-II[29]) as a measure of depression.
RESULTSOut of the 11 studies included in the meta-analysis,
eight studied ABMT for SAD,[14–18],[20–22] one forGAD[19], one for posttraumatic stress disorder,[13]
and one for a group of pediatric anxiety disorders(SAD, GAD, specific phobia, and separation anxietydisorder).[12] ABMT was delivered through an averageof 7.82 sessions across studies (range = 4–14 sessions),
Depression and Anxiety

386 Linetzky et al.
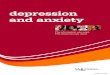
TABLE 1. Standard difference in means within groups for clinician-ratings and self-reported measures of anxiety
with mean total number of trials of 1603 (range = 1280–2976). All the effect sizes reported here were tested foroutliers, and no outliers exceeding standardized effect of±2.5 were found.
ANXIETY SYMPTOMSWithin-group effects for individual studies are reported
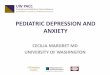
in Table 1. Between-groups effect sizes of the differencebetween ABMT and control at posttraining are pre-sented in Table 2.
Clinician-Ratings. The overall between-groupscombined effect size based on clinician-rated measuresof anxiety was significant, d = 0.42, P = .001, CI =0.18–0.66, k = 6, fail-safe number = 14. Within-groupeffects indicate that ABMT is associated with significant
and greater reductions in anxiety symptom (d = 1.00,P < .001, 95% CI = 0.65–1.35, k = 6), relative to controltraining (d = 0.42, P < .001, CI = 0.19–0.65, k = 6),Q = 7.25, P < .01. Fail-safe number analysis suggeststhat this effect could be reduced to insignificance withthe addition of 108 new studies with null results forthe ABMT group and with 15 new studies with nullresults for the control group. Finally, the combinednumber of patients no longer meeting DSM criteria foran anxiety disorder following ABMT was significantlyhigher relative to the number of patients no longermeeting diagnostic criteria for their anxiety disorder inthe control training condition, d = 0.40, P < .05, CI =0.02–0.78, k = 8, fail-safe number = 14.
Self-Reports. The overall combined between-groupseffect at posttreatment was nonsignificant (d = 0.08,
Depression and Anxiety

Review: ABMT for Anxiety Disorders: A Meta-Analysis 387
TABLE 2. Standard difference in means between groups for clinician-ratings and self-reported measures of anxiety
P = .35, CI = −0.09–0.26, k = 10), as was the combinedbetween-groups effect at follow-up (d = 0.23, P = .18, CI= −0.10–0.57). For within-group combined effects, bothABMT (d = 0.89, P < .001, CI = 0.52–1.26) and controltraining (d = 0.49, P < .001, CI = 0.29–0.69) showedsignificant reductions in symptoms. However, the dif-ference between the two conditions was nonsignificant,Q = 3.49, P = 0.06, with a trend for greater reductionin ABMT relative to control training. Within-group ef-fect sizes for studies reporting a follow-up measurement(k = 8, mean time to follow-up =12.62, range = 2–16 weeks) revealed a similar pattern of results to thatobserved at posttreatment (ABMT: d = 1.10, P < .001,CI = 0.54–1.66; control training: d = 0.54, P < .001, CI= 0.32–0.75), Q = 3.43, P = .06.
ATTENTION BIASThe overall combined effect size for between-groups
contrasts posttreatment reflects significantly lower at-tention bias score in the ABMT relative to the controlcondition, d = 0.61, P < .05, CI = 0.09–1.12, k = 8,suggesting that ABMT produces greater reductions inthreat-related attention bias than control training. Com-bined within-group effects indicate that ABMT produces
significant and greater reductions in attention bias (d =0.85, P < .01, CI = 0.24–1.46, k = 7), relative to controltraining (d = 0.04, P = .76, CI = −0.20–0.27, k = 7),Q = 5.89, P < .05 (Table 3).
MODERATION OF ABMT EFFECTS BY DELIVERYCONTEXT: CLINIC VERSUS HOME
Based on the number of available studies, meta-analysis of this moderation was viable only for self-reported measures of anxiety. We examined thecombined between-groups effects separately for studiesconducted in the clinic (k = 6) and studies conductedat home over the Internet (k = 4), see Table 2. Theseanalyses revealed a significant effect for studies con-ducted in a clinic setting (d = 0.34, P = .01, CI = 0.07–0.62), indicating less anxiety symptoms post-ABMT rel-ative to control training. Nonsignificant effect was foundfor studies delivering ABMT at home over the Internet(d = −0.10, P = .40, CI = −0.33–0.13). The differencebetween the magnitudes of these effects was significant,Q = 5.85, P < .05.
To probe whether this context dependent differencein symptom reduction may be mirrored by greaterreductions in attentional threat bias in participants who
Depression and Anxiety

388 Linetzky et al.
TABLE 3. Standard difference in means within groups for attention bias scores
ABMT = attention bias modification treatment. P<0.10 ∗P<0.05 ∗∗P<0.01.
received ABMT in the clinic relative to those who re-ceived it at home over the Internet, we also examinedthe influence of this moderator on the combined between-groups effects of attention bias posttreatment. A signifi-cant effect of reduction in attention bias was found forstudies conducted in a clinic setting (d = 1.27, P < .01, CI= 0.41–2.14, k = 4), indicating less attention bias post-ABMT relative to control training, whereas a nonsignif-icant effect was found for studies delivering ABMT athome over the Internet (d = 0.07, P = .72, CI = −0.30–0.43, k = 4). The difference between these effects wassignificant, Q = 6.33, P < .05.
DEPRESSION SYMPTOMSThe combined between-groups effects were not signifi-
cant (d = −0.02, P = .88, CI = −0.23–0.20, k = 9). Thecombined within-group effect sizes of change in depres-sion symptoms from pre- to posttreatment were signifi-cant, both for the ABMT condition (d = 0.41, P < .001,CI = 0.22–0.60) and the control training condition (d =0.32, P < .01, CI = 0.10–0.53). The difference betweenthese effects was not significant, Q = 0.37, P = .54.
DISCUSSIONThe current meta-analysis suggests that ABMT is
a clinically beneficial treatment for anxiety disorders.A significant, medium size between-groups effect wasfound for clinician ratings of anxiety reflecting greaterposttreatment improvement in ABMT relative to con-trol treatment. Between-groups effects of change in anx-iety measured with self-reports were found only for stud-ies conducted in a clinic setting, whereas the overall effectfor self-reported measures was not significant. Possiblereasons and potential implications of this pattern of re-sults are discussed below. The between-groups effectsfound here directly reflect the added therapeutic valueof ABMT relative to placebo training, and are notablein light of the control used in the RCTs included inthe meta-analysis. Many RCTs of psychological treat-ments for anxiety disorders employ control conditionsthat poorly match the treatment group.[30, 31] Relative tosuch studies, ABMT studies include tighter experimen-tal control in which the procedures in the experimentaltreatment closely resemble those in the control treat-ment. Importantly, the combined number of patients
Depression and Anxiety

Review: ABMT for Anxiety Disorders: A Meta-Analysis 389
no longer meeting DSM criteria for their anxiety dis-order following ABMT was significantly higher relativeto the control condition. Contrasting within-group ef-fect sizes suggests large overall therapeutic effects fol-lowing ABMT relative to control training. Indeed, allABMT effects, across all samples, were associated withsome improvement in clinical status (see Table 1, allsamples aligned greater than zero), highlighting the po-tential therapeutic effect of ABMT even in studies thatfailed to find a significant between-groups effect aboveand beyond placebo. Additionally, the effects of symp-toms reduction are corroborated by treatment effects ofattention bias change, showing significant and greaterreductions in attention bias in ABMT relative to con-trol training. Finally, there is a preliminary indicationthat therapeutic gains are maintained at a few monthsfollow-up. Taken together, the current meta-analysis in-dicates significant treatment gains following ABMT forclinically anxious patients.
The meta-analysis revealed that treatment effects ofABMT were more pronounced in clinician-reportedthan in self-reported measures. Clinician-rated mea-sures may be more sensitive to clinical change thanself-reported measures.[32] Alternatively, self-reportedchange in symptoms may evolve more slowly over timethan changes on clinician-rated measures. Moreover,some self-report instruments used in ABMT studies mayfail to capture meaningful symptomatic changes acrossthe short duration of the intervention. For instance,some of the employed inventories require participantsto report the symptoms that they generally experiencerather than the symptoms they currently experience.Thus, participants’ self-reports collected immediatelyfollowing ABMT may reflect, at least in part, the anxietythey have experienced prior to the intervention. To dis-tinguish between these alternative possibilities, futurestudies may wish to: (1) utilize self-reported measuresthat emphasize and focus on current symptoms; and (2)examine symptom change with a longer time interval atfollow-up.
Although therapeutic effects were significantly atten-uated in control training conditions relative to ABMT,these control trainings were still associated with sig-nificant reduction in anxiety symptoms. These reduc-tions could reflect expectancy or other known effects ofplacebo as well as other nonspecific treatment effects.None of the included studies evaluates the degree towhich sham-ABMT delivers therapeutic benefits aboveand beyond the benefit produced by other control treat-ments, such as pill placebo. Future research comparingsham-ABMT with other active and control conditionscould shed light on this issue. It is conceivable that thetypically used control condition in ABMT studies in factenhances general attention control[33], or provides re-peated exposure to the minor threats engraved in each ofthe probe detection trials and could thus trigger desensi-tization and extinction processes.[12] These possibilitiescould be clarified in mechanistic research designed toestimate the potential contributions of such processes to
the overall therapeutic effect of ABMT. It also appearsthat time may be ripe for RCTs that directly contrastthe efficacy of ABMT and other first-line treatments foranxiety disorders (i.e., CBT and Selective Serotonin Re-uptake Inhibitor (SSRI)). It is conceivable that in suchdesigns, in which patients are not presented with the pos-sibility of being assigned to a placebo condition, ABMT’soverall effects could increase.
As a new treatment with increasing evidence-base sup-port, question arises on the scalability of ABMT. Beingcomputer based, one potential avenue for scalability isuse of the Internet or alternative installations to deliverABMT away from the clinic at patients’ homes. How-ever, the current moderator analysis regarding deliverycontext suggests that the self-reported effect of ABMTfound in the clinic attenuates to nonsignificance whenABMT is delivered at home. Various factors could ex-plain this finding. When performed in the home unob-served by clinicians or staff, patients may fail to optimallyattend to the ABMT task and training schedule, therebyreducing its effect. Factors, such as external noise, pos-ture during training, illumination, general attentiveness,and potentially competing tasks, are carefully monitoredin the clinic. Such factors could further reduce the effi-cacy of ABMT delivered in the home context. Indeed,attention bias combined effects were also moderated bydelivery context, with only studies conducted in a clinicsetting, but not the home setting, showing significantreduction in attention bias. Thus, attenuated clinical ef-fects found for home-delivered ABMT might reflect at-tenuated effects on threat-related attention bias in thissetting.
Other factors related to delivery context could furtherimpact ABMT. For example, benefits may accrue whenanxious patients approach clinics for treatment, meetwith staff, and perform ABMT while being monitored.For instance, the act of attending a clinic could instillhope in a patient and create an expectancy of improve-ment that interacts with active ABMT. Alternatively,ABMT may interact with particular aspects of clinic vis-its among patients with anxiety disorders. Specifically,ABMT delivered in a clinic may promote exposure, andthe lack of such an exposure element in home-basedABMT could attenuate efficacy. Available data provideindirect support for this possibility; in one Internet-based ABMT study, Kuckertz et al.[34] found that par-ticipants instructed to activate their social anxiety fearsprior to each ABMT session demonstrated significantlygreater anxiety reductions than participants receivingABMT without these additional instructions. Directingpatients to undergo exposure could potentiate the effectsof ABMT, and this could account for the enhanced ef-ficacy of ABMT conducted in a clinic as opposed to ahome-based setting. Future studies could explicitly testthis hypothesis. Of note, ABMT delivery in any con-text still requires far less resources than other commonpsychological treatments for anxiety (e.g., CBT), sug-gesting that ABMT for anxiety disorders delivered inthe clinic also has potential advantages. Furthermore,
Depression and Anxiety

390 Linetzky et al.
although beyond the scope of the current meta-analysis,there are promising indications that ABMT may be auseful add-on to CBT.[23, 35]
The current meta-analytic findings highlight the im-portance of providing a direct proof for the presumedtherapeutic mechanisms underpinning ABMT. ABMTis based on the notion that reduction in attentionbias toward threat via training drives the reduction inanxiety symptoms.[36] Hence, attention bias change isexpected to have a tight association with reduction inanxiety symptoms. Success in changing attention biasis expected to have a moderating role on treatment ef-fects. Unfortunately, despite the importance of this is-sue, not all studies included in the present meta-analysisreported pre- and posttreatment attention bias scores.Examination of attention bias patterns in studies withavailable data only provides indirect insights on the mech-anism through which ABMT reduces symptoms. First,the combined between-groups effect size for posttreat-ment attention bias indicates a significantly lower at-tention bias score in the ABMT relative to the controlcondition; this suggests that ABMT more effectively re-duces threat-related attention bias than control training.Second, a comparison of the combined within-group ef-fects suggests that active ABMT produces significantlygreater reduction in attention bias than control training.Finally, data on ABMT delivery context (clinic vs. home)reveal similar patterns for attention and anxiety symp-toms. That is, a significant effect on attention bias wasfound only for studies conducted in a clinic setting butnot for studies delivering ABMT at home over the In-ternet. Importantly, however, these data only indirectlymodel the relationship between changes in attention biasand symptoms. A more direct evaluation requires a for-mal meta-analytic moderation analysis, which cannot beperformed due to insufficient published data. To directlytest attention bias change as a moderator, ABMT sam-ples could be divided into those that report significantchange in attention bias and those that do not. Separateeffect sizes of symptoms change could be computed foreach level of the moderator, and the difference betweenthese effects models the role of attention bias change as amoderator of treatment outcome. Such analysis was notviable due to the small number of studies that system-atically reported attention bias scores. Researchers areencouraged to report attention bias scores before andafter ABMT in future studies.[37]
Some limitations and further suggestions for futureresearch can be noted. First, the relatively small num-ber of RCTs of ABMT in clinical anxiety disorderscalls for additional research effort in this field. Second,most RCTs are probably underpowered to detect thereported between-groups effect (d = 0.42). Power anal-ysis for this between-groups effect (power = 0.80, al-pha < 0.05) indicates that single studies should consistof samples of at least 142 participants (71 per group)to have enough power to detect a significant between-groups effect. Thus, future RCTs should considerlarger samples if interested in establishing this particular
effect. Third, clinician-rated measures yielded consider-ably stronger findings than self-reported measures. Thisdifference may be attributed to the different distributionof ABMT delivery context relative to each measure type.Clinician-rated measures were reported mainly in stud-ies conducted in a clinic. It is therefore recommendedthat both types of measures be used in future RCTs ofABMT, including in those delivered over the Internet.Fourth, currently there are not enough RCTs that mea-sured follow-up outcomes to enable a comprehensiveanalysis of ABMT’s long-lasting effects. It is stronglyrecommended that future studies include follow-upmeasurements. Fifth, this meta-analysis included 11RCTs performed in clinically anxious patients with vari-ous anxiety disorders. More RCTs for specific disorders(e.g., GAD) could hopefully delineate specific ABMTparameters for specific anxiety disorders.
In conclusion, the current meta-analysis provides sup-port for ABMT as a treatment for anxiety disorders.More focused research exploring the influence of deliv-ery context and variables of disorder specificity is essen-tial for the establishment of benchmark ABMT protocolsfor anxiety disorders.
References marked with an asterisk indicate studiesincluded in the meta-analysis.
REFERENCES1. Armstrong T, Olatunji BO. Eye tracking of attention in the affec-
tive disorders: a meta-analytic review and synthesis. Clin PsycholRev 2012;32(8):704–723.
2. Bar-Haim Y, Lamy D, Pergamin L, et al. Threat-related atten-tional bias in anxious and nonanxious individuals: a meta-analyticstudy. Psychol Bull 2007;133(1):1–24.
3. Eldar S, Bar-Haim Y. Neural plasticity in response to attentiontraining in anxiety. Psychol Med 2010;40(4):667–677.
4. Dandeneau SD, Baldwin MW, Baccus JR, et al. Cutting StressOff at the Pass: Reducing Vigilance and Responsiveness to So-cial Threat by Manipulating Attention. 4th ed. Washington, DC:American Psychological Association; 2007:651–666.
5. Heeren A, Lievens L, Philippot P. How does attention train-ing work in social phobia: disengagement from threat or re-engagement to non-threat? J Anxiety Disord 2011;25(8):1108–1115.
6. Bar-Haim Y, Morag I, Glickman S. Training anxious children todisengage attention from threat: a randomized controlled trial. JChild Psychol Psychiatry 2011;52(8):861–869.
7. Waters AM, Pittaway M, Mogg K, et al. Attention training towardspositive stimuli in clinically anxious children. Deve Cogn Neurosci2013;4:77–84.
8. Hakamata Y, Lissek S, Bar-Haim Y, et al. Attention bias modifica-tion treatment: a meta-analysis toward the establishment of noveltreatment for anxiety. Biol Psychiatry 2010;68(11):982–990.
9. Hallion LS, Ruscio AM. A meta-analysis of the effect of cogni-tive bias modification on anxiety and depression. Psychol Bull2011;137(6):940–958.
10. Beard C, Sawyer AT, Hofmann SG. Efficacy of attention biasmodification using threat and appetitive stimuli: a meta-analyticreview. Behav Ther 2012;43(4):724–740.
Depression and Anxiety

Review: ABMT for Anxiety Disorders: A Meta-Analysis 391
11. Mogoase C, David D, Koster EHW. Clinical efficacy of atten-tional bias modification procedures: an updated meta-analysis. JClin Psychol 2014;70(12):1133–1157.
12. ∗Eldar S, Apter A, Lotan D, et al. Attention bias modificationtreatment for pediatric anxiety disorders: a randomized controlledtrial. Am J Psychiatry 2012;169(2):213–220.
13. ∗Schoorl M, Putman P, van Der Does W. Attentional bias modi-fication in posttraumatic stress disorder: a randomized controlledtrial. Psychother Psychosom 2013;82(2):99–105.
14. ∗Schmidt NB, Richey JA, Buckner JD, Timpano KR. Attentiontraining for generalized social anxiety disorder. J Abnorm Psychol2009;118(1):5–14.
15. ∗Neubauer K, von Auer M, Murray E, et al. Internet-deliveredattention modification training as a treatment for social pho-bia: a randomized controlled trial. Behav Res Ther 2013;51(2):87–97.
16. ∗Heeren A, Reese HE, McNally RJ, Philippot P. Attention train-ing toward and away from threat in social phobia: effects on sub-jective, behavioral, and physiological measures of anxiety. BehavRes Ther 2012;50(1):30–39.
17. ∗Carlbring P, Apelstrand M, Sehlin H, et al. Internet-deliveredattention bias modification training in individuals with social anx-iety disorder—a double blind randomized controlled trial. BMCPsychiatry 2012;66(1):12.
18. ∗Boettcher J, Leek L, Matson L, et al. Internet-based attentionbias modification for social anxiety: a randomised controlled com-parison of training towards negative and training towards positivecues. PLoS One 2013;8(9):e71760.
19. ∗Amir N, Beard C, Burns M, Bomyea J. Attention modificationprogram in individuals with generalized anxiety disorder. J Ab-norm Psychol 2009a;118(1):28–33.
20. ∗Amir N, Beard C, Taylor CT, et al. Attention training in indi-viduals with generalized social phobia: a randomized controlledtrial. J Consult Clin Psychol 2009b;77(5):961–973.
21. ∗Boettcher J, Berger T, Renneberg B. Internet-based attentiontraining for social anxiety: a randomized controlled trial. CognitTher Res 2012;36(5):522–536.
22. ∗Bunnell BE, Beidel DC, Mesa F. A randomized trial of atten-tion training for generalized social phobia: does attention trainingchange social behavior? Behav Ther 2013;44(4):662–673.
23. Amir N, Taylor CT. Combining computerized home-based treat-ments for generalized anxiety disorder: an attention modifica-tion program and cognitive behavioral therapy. Behav Ther2012;43(3):546–559.
24. Morris SB, DeShon RP. Combining effect size estimates in
meta-analysis with repeated measures and independent-groupsdesigns. Psychol Methods 2002;7(1):105–125.
25. Mullen B. Advanced BASIC Meta-Analysis. Hillsdale, NJ:Lawrence Erlbaum; 1989.
26. Sterne JAC, Sutton AJ, Ioannidis JPA, et al. Recommenda-tions for examining and interpreting funnel plot asymmetry inmeta-analyses of randomised controlled trials. Br Med J 2011;d4002:343.
27. Liebowitz MR. Social phobia. Mod Probl Pharmacopsychiatry1987;22:141–173.
28. Spielberger C, Gorsuch R, Lushene R, et al. The Manual for theState-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psy-chologists Press; 1983.
29. Beck AT, Steer RA, Brown GK. Beck Depression Inventory-II(BDI-II). Toronto, Canada: Psychological Corporation, HarcourtBrace; 1996.
30. Clarke PJF, Notebaert L, MacLeod C. Absence of evidence orevidence of absence: reflecting on therapeutic implementations ofattentional bias modification. BMC Psychiatry 2014;8(1):14.
31. Arch JJ, Craske MG. First-line treatment: a critical appraisal ofcognitive behavioral therapy developments and alternatives. Psy-chiatr Clin North Am 2009;32(3):525–547.
32. Cuijpers P, Li J, Hofmann SG, Andersson G. Self-reported ver-sus clinician-rated symptoms of depression as outcome measuresin psychotherapy research on depression: a meta-analysis. ClinPsychol Rev 2010;30(6):768–778.
33. Derakshan N, Eysenck MW. Anxiety, processing efficiency, andcognitive performance: new developments from attentional con-trol theory. Eur Psychol 2009;14(2):168–176.
34. Kuckertz JM, Gildebrant E, Liliequist B, et al. Moderation andmediation of the effect of attention training in social anxiety dis-order. Behav Res Ther 2014;53:30–40.
35. Shechner T, Rimon-Chakir A, Britton JC, et al. Attentionbias modification treatment augmenting effects on cognitivebehavioral therapy in children with anxiety: randomized con-trolled trial. J Am Acad Child Adolesc Psychiatry 2014;53(1):61–71.
36. MacLeod C, Rutherford E, Campbell L, et al. Selective Atten-tion and Emotional Vulnerability: Assessing the Causal Basis ofTheir Association Through the Experimental Manipulation of At-tentional Bias. 1st ed. Washington, DC: American PsychologicalAssociation; 2002:107–123.
37. Koster EHW, Fox E, MacLeod C. Introduction to the specialsection on cognitive bias modification in emotional disorders. JAbnorm Psychol 2009;118(1):1–4.
Depression and Anxiety