Embed Size (px)
Citation preview
September 2002Volume 4, Number 9
Authors
Thomas Nguyen, MDAssistant Professor of Emergency Medicine, Mount SinaiSchool of Medicine, New York, NY.
Jessica Freedman, MDAssistant Professor of Emergency Medicine, AssociateResidency Director and Mount Sinai Residency SiteDirector, Mount Sinai School of Medicine, New York, NY.
Peer Reviewers
Marianne C. Burke, MDConsultant, Burke Emergency Medicine Consultants,Glendale, CA.
Stephen J. Playe, MD, FACEPAssistant Professor, Emergency Medicine, TuftsUniversity School of Medicine; Residency ProgramDirector, Department of Emergency Medicine, BaystateMedical Center, Western Campus of Tufts UniversitySchool of Medicine, Springfield, MA.
CME Objectives
Upon completing this article, you should be able to:1. describe indicators that a rash may have a potentially
life-threatening cause;2. list aspects of the history and physical examination
that may help identify life-threatening rashes;3. discuss the differential diagnosis for maculopapular,
petechial/purpuric, diffuse erythematous, andvesiculo-bullous rashes, emphasizing life-threateningcauses of each; and
4. describe the proper disposition for patients with life-threatening rashes.
Date of original release: September 1, 2002.Date of most recent review: August 7, 2002.
See “Physician CME Information” on back page.
Editor-in-Chief
Stephen A. Colucciello, MD, FACEP,Assistant Chair, Department ofEmergency Medicine, CarolinasMedical Center, Charlotte, NC;Associate Clinical Professor,Department of EmergencyMedicine, University of NorthCarolina at Chapel Hill, ChapelHill, NC.
Associate Editor
Andy Jagoda, MD, FACEP, Professorof Emergency Medicine; Director,International Studies Program,Mount Sinai School of Medicine,New York, NY.
Editorial Board
Judith C. Brillman, MD, ResidencyDirector, Associate Professor,Department of EmergencyMedicine, The University ofNew Mexico Health Sciences
Center School of Medicine,Albuquerque, NM.
W. Richard Bukata, MD, AssistantClinical Professor, EmergencyMedicine, Los Angeles County/USC Medical Center, Los Angeles,CA; Medical Director, EmergencyDepartment, San Gabriel ValleyMedical Center, San Gabriel, CA.
Francis M. Fesmire, MD, FACEP,Director, Chest Pain—StrokeCenter, Erlanger Medical Center;Assistant Professor of Medicine,UT College of Medicine,Chattanooga, TN.
Valerio Gai, MD, Professor and Chair,Department of EmergencyMedicine, University of Turin, Italy.
Michael J. Gerardi, MD, FACEP,Clinical Assistant Professor,Medicine, University of Medicineand Dentistry of New Jersey;Director, Pediatric EmergencyMedicine, Children’s MedicalCenter, Atlantic Health System;Vice-Chairman, Department of
Emergency Medicine, MorristownMemorial Hospital.
Michael A. Gibbs, MD, FACEP, Chief,Department of EmergencyMedicine, Maine Medical Center,Portland, ME.
Gregory L. Henry, MD, FACEP,CEO, Medical Practice RiskAssessment, Inc., Ann Arbor,MI; Clinical Professor, Departmentof Emergency Medicine,University of Michigan MedicalSchool, Ann Arbor, MI; President,American Physicians AssuranceSociety, Ltd., Bridgetown,Barbados, West Indies; PastPresident, ACEP.
Jerome R. Hoffman, MA, MD, FACEP,Professor of Medicine/EmergencyMedicine, UCLA School ofMedicine; Attending Physician,UCLA Emergency Medicine Center;Co-Director, The DoctoringProgram, UCLA School of Medicine,Los Angeles, CA.
Francis P. Kohrs, MD, MSPH, Associate
Professor and Chief of the Divisionof Family Medicine, Mount SinaiSchool of Medicine, New York, NY.
John A. Marx, MD, Chair and Chief,Department of EmergencyMedicine, Carolinas MedicalCenter, Charlotte, NC; ClinicalProfessor, Department ofEmergency Medicine, Universityof North Carolina at Chapel Hill,Chapel Hill, NC.
Michael S. Radeos, MD, MPH,Attending Physician, Departmentof Emergency Medicine,Lincoln Medical and MentalHealth Center, Bronx, NY;Assistant Professor in EmergencyMedicine, Weill College ofMedicine, Cornell University,New York, NY.
Steven G. Rothrock, MD, FACEP, FAAP,Associate Professorof Emergency Medicine, Universityof Florida; Orlando RegionalMedical Center; Medical Director ofOrange County Emergency
Medical Service, Orlando, FL.
Alfred Sacchetti, MD, FACEP,Research Director, Our Lady ofLourdes Medical Center, Camden,NJ; Assistant Clinical Professorof Emergency Medicine,Thomas Jefferson University,Philadelphia, PA.
Corey M. Slovis, MD, FACP, FACEP,Professor of Emergency Medicineand Chairman, Department ofEmergency Medicine, VanderbiltUniversity Medical Center;Medical Director, Metro NashvilleEMS, Nashville, TN.
Mark Smith, MD, Chairman,Department of EmergencyMedicine, Washington HospitalCenter, Washington, DC.
Charles Stewart, MD, FACEP,Colorado Springs, CO.
Thomas E. Terndrup, MD, Professorand Chair, Department ofEmergency Medicine, Universityof Alabama at Birmingham,Birmingham, AL.
EMERGENCY MEDICINE PRACTICEA N E V I D E N C E - B A S E D A P P R O A C H T O E M E R G E N C Y M E D I C I N E
EMPRACTICE.NET
Dermatologic Emergencies:Diagnosing And ManagingLife-Threatening Rashes
March 15, 2001: You see a patient for “fatigue.” This 52-year-old man wasrecently discharged from the hospital on ticlopidine and methyldopa. When youenter the room, he is fully clothed in a suit and tie—another violation of the ED’s“get naked” policy (which is more honored in breach than observance). He looksokay—he’s certainly well-dressed, and through his coat, his lungs sound clear.Looks like another “viral syndrome.”
February 25, 2002: You receive an ominous-looking certified letter. Thecomplaint is lengthy but you understand the gist. A patient you had seen almost ayear ago died two days after his visit from an intracerebral bleed. The plaintiff’slawyers cite a triage note that documented complaints of “fatigue and rash”; yourrecord did not mention a rash. The attached pathology report listed the cause ofdeath as “medication-induced TTP.”
WHILE most rashes seen in the ED are benign, some indicate a seriousor even life-threatening medical illness. This issue of Emergency
Medicine Practice provides a systematic approach to managing dangerousdermatologic complaints.
State Of The Literature
Guidelines and evidence-based literature regarding dermatologic emergen-cies are sparse. An extensive search using MEDLINE, the Cochrane Collabo-ration, and www.guidelines.gov (the National Guideline Clearinghouse)yielded no guidelines on life-threatening rashes. While specific guidelinesexist for “mycotic infections” or “psoriasis,” the only relevant guidelineregards cutaneous adverse drug reactions.1
The classification of various skin diseases has changed over time,further confounding the literature. Many of the earlier studies on Stevens-Johnson syndrome and toxic epidermal necrolysis erroneously grouped
Emergency Medicine Practice 2 www.empractice.net • September 2002
these conditions as variants of erythema multiforme.
Epidemiology
Dermatologic complaints account for approximately 5%of all ED visits. However, there are limited epidemiologicdata that analyze the types of rashes seen in EDs. Onepediatric ED reported that 31% of the cases primarilyinvolved the skin. Most cases were classified as contu-sions, lacerations, and burns; non-traumatic causesincluded viral exanthems, bacterial infections, andcontact dermatitis.2 In one survey, the most common skincomplaints diagnosed by internists were dermatitis (16%of all diagnoses), bacterial skin infections (14%), fungalinfections (5%), and acne vulgaris (5%).3 The emergencyphysician is more likely to encounter the life-threateningrashes, such as meningococcemia, toxic epidermalnecrolysis, or toxic shock syndrome.
“A thick skin is a gift from God.”—Konrad Adenauer (1876-1976), German statesman
Pathophysiology
The skin is comprised of three layers: the epidermis, thedermis, and the subcutaneous layer. The epidermiscontains basal cells and keratinocytes, which form aprotective barrier. Melanocytes produce the pigment thatfilters ultraviolet radiation. The dermis is comprised ofconnective tissues—collagen, elastin, and reticularfibers—which provide strength and elasticity to the skin.The subcutaneous layer contains mostly fat cells andconnective tissue. Sweat glands, hair follicles, nerves,capillaries, and veins are dispersed within thesethree layers.
When these capillaries leak blood into the skin,petechiae appear. Leakage results from perivascularinflammation and/or thrombocytopenia. Petechiae areoften first seen in dependent areas such as the ankles andwrists. If the petechiae are greater than 0.5 cm in size,they become purpura. In vasculitis, the purpura canbecome palpable.
The dermal-epidermal junction deserves specialmention. It is the site of immunoglobulin and comple-ment deposition and is the origin of blisters in diseasessuch as pemphigus and Stevens-Johnson syndrome.Immunofluorescence assays performed at the dermal-epidermal junction can help diagnose vesiculo-bullousskin disease.
Differential Diagnosis And Terminology
Common terminology is essential to describe cutaneouslesion, categorize rashes, and facilitate communicationamong clinicians. These descriptive terms are also crucialin developing a differential diagnosis.
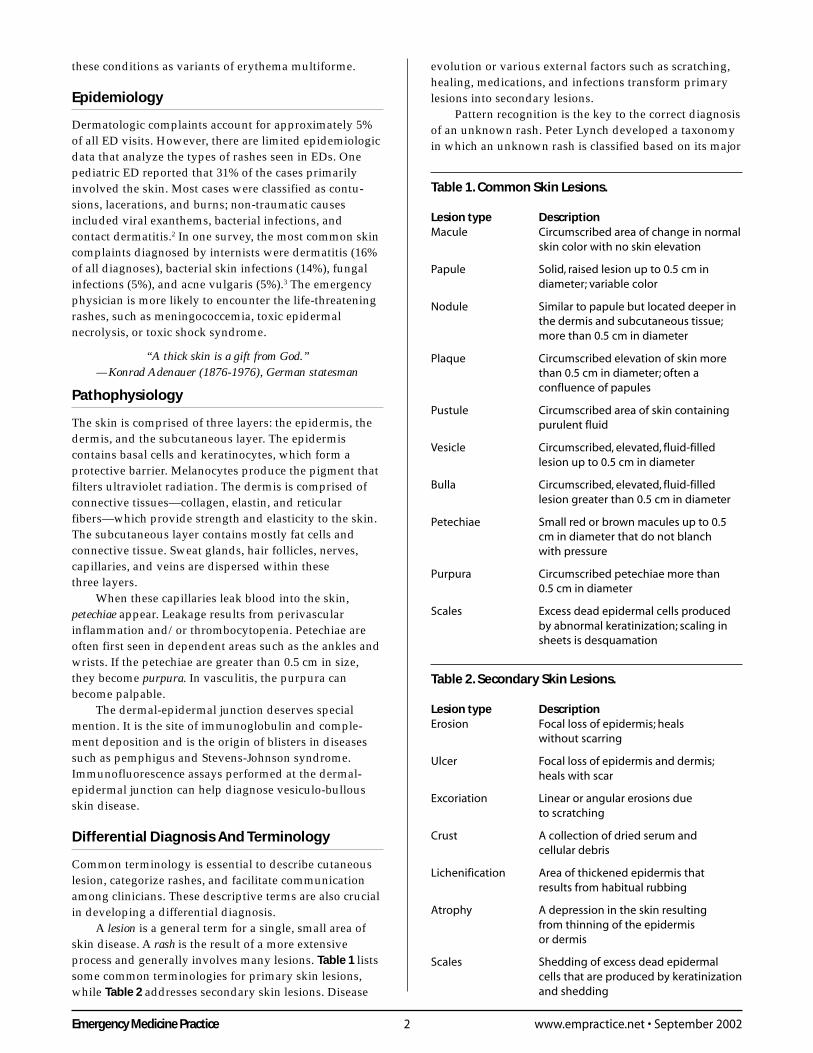
A lesion is a general term for a single, small area ofskin disease. A rash is the result of a more extensiveprocess and generally involves many lesions. Table 1 listssome common terminologies for primary skin lesions,while Table 2 addresses secondary skin lesions. Disease
evolution or various external factors such as scratching,healing, medications, and infections transform primarylesions into secondary lesions.
Pattern recognition is the key to the correct diagnosisof an unknown rash. Peter Lynch developed a taxonomyin which an unknown rash is classified based on its major
Table 2. Secondary Skin Lesions.
Lesion type DescriptionErosion Focal loss of epidermis; heals
without scarring
Ulcer Focal loss of epidermis and dermis;heals with scar
Excoriation Linear or angular erosions dueto scratching
Crust A collection of dried serum andcellular debris
Lichenification Area of thickened epidermis thatresults from habitual rubbing
Atrophy A depression in the skin resultingfrom thinning of the epidermisor dermis
Scales Shedding of excess dead epidermalcells that are produced by keratinizationand shedding
Table 1. Common Skin Lesions.
Lesion type DescriptionMacule Circumscribed area of change in normal
skin color with no skin elevation
Papule Solid, raised lesion up to 0.5 cm indiameter; variable color
Nodule Similar to papule but located deeper inthe dermis and subcutaneous tissue;more than 0.5 cm in diameter
Plaque Circumscribed elevation of skin morethan 0.5 cm in diameter; often aconfluence of papules
Pustule Circumscribed area of skin containingpurulent fluid
Vesicle Circumscribed, elevated, fluid-filledlesion up to 0.5 cm in diameter
Bulla Circumscribed, elevated, fluid-filledlesion greater than 0.5 cm in diameter
Petechiae Small red or brown macules up to 0.5cm in diameter that do not blanchwith pressure
Purpura Circumscribed petechiae more than0.5 cm in diameter
Scales Excess dead epidermal cells producedby abnormal keratinization; scaling insheets is desquamation
3 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
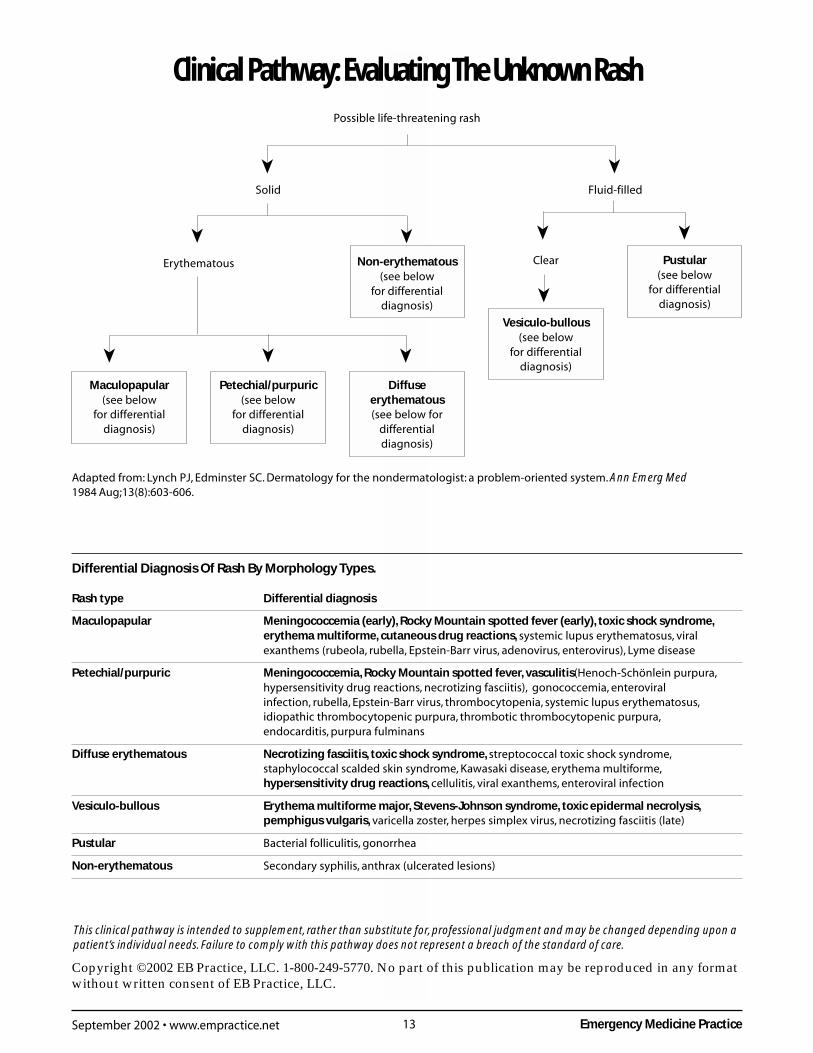
morphology, which has since been adopted by manyclinicians.4,5 The Clinical Pathway on page 13, “Evaluat-ing The Unknown Rash,” presents a modified Lynchalgorithm using six major morphological groups and liststhe differential diagnoses of potentially life-threateningrashes according to the clusters.
Prehospital Care
As a general rule, prehospital care providers shouldalways use standard precautions and assume all bodilyfluids or weeping lesions are infectious. In a patient witha fever and a petechial/purpuric rash (i.e., suspectedmeningococcemia or viral hemorrhagic fever), respiratoryand contact isolation are advised, including a properlyfitting mask for both the healthcare provider and thepatient. The ambulance should be well-ventilated inorder to eliminate potentially infectious airborne drop-lets.6 All equipment contaminated with blood or bodilyfluids should be wiped down with a disinfectant solu-tion, such as bleach diluted with water. These sameprotocols are used to disinfect a hospital room occupiedby a patient with meningococcemia. If the patient ishypotensive, medics should give IV normal saline whileen route to the hospital.
Emergency Department Evaluation
Triage/Initial Nursing InterventionsThe triage nurse should rapidly identify those patientswith a rash who appear seriously ill or likely to decom-pensate. High-risk patients include those with abnormalvital signs, altered mental status, or potential airwaycompromise. A petechial rash should also prompt earlyphysician involvement, especially when accompanied byfever or confusion. In some hospitals, patients with feverand a rash are placed in respiratory isolation, especially ifthe patient is immunocompromised. The triage nurseshould ensure early isolation of patients with lesionscompatible with chickenpox or meningococcemia.
All toxic-appearing patients with a rash require IVaccess, an ECG, and pulse oximetry monitoring. Oxygen-ation, perfusion, and a bedside blood sugar must beassessed in all patients with altered mental status.
Red FlagsLook for the following “red flags” when evaluating apatient with an unknown rash, as these may indicateserious illness. (See Table 3.)
Fever suggests that an infectious or inflammatoryprocess may be present. Infants and the elderly are more
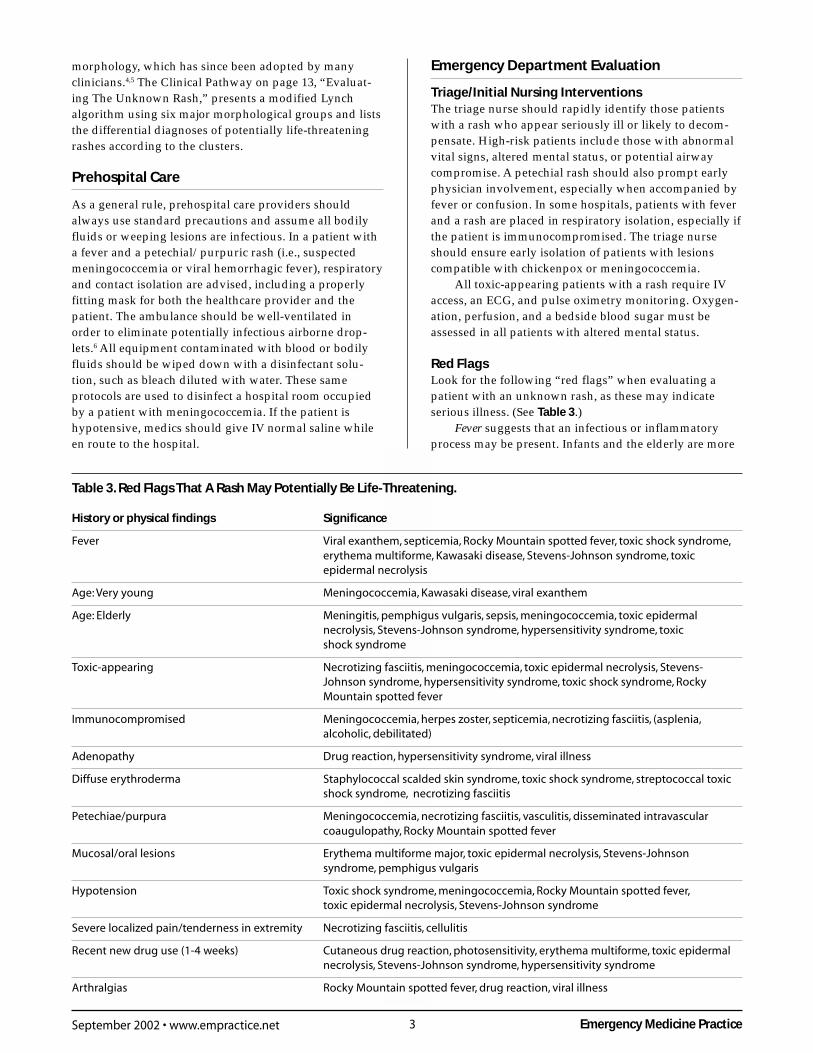
Table 3. Red Flags That A Rash May Potentially Be Life-Threatening.
History or physical findings Significance
Fever Viral exanthem, septicemia, Rocky Mountain spotted fever, toxic shock syndrome,erythema multiforme, Kawasaki disease, Stevens-Johnson syndrome, toxicepidermal necrolysis
Age: Very young Meningococcemia, Kawasaki disease, viral exanthem
Age: Elderly Meningitis, pemphigus vulgaris, sepsis, meningococcemia, toxic epidermalnecrolysis, Stevens-Johnson syndrome, hypersensitivity syndrome, toxicshock syndrome
Toxic-appearing Necrotizing fasciitis, meningococcemia, toxic epidermal necrolysis, Stevens-Johnson syndrome, hypersensitivity syndrome, toxic shock syndrome, RockyMountain spotted fever
Immunocompromised Meningococcemia, herpes zoster, septicemia, necrotizing fasciitis, (asplenia,alcoholic, debilitated)
Adenopathy Drug reaction, hypersensitivity syndrome, viral illness
Diffuse erythroderma Staphylococcal scalded skin syndrome, toxic shock syndrome, streptococcal toxicshock syndrome, necrotizing fasciitis
Petechiae/purpura Meningococcemia, necrotizing fasciitis, vasculitis, disseminated intravascularcoaugulopathy, Rocky Mountain spotted fever
Mucosal/oral lesions Erythema multiforme major, toxic epidermal necrolysis, Stevens-Johnsonsyndrome, pemphigus vulgaris
Hypotension Toxic shock syndrome, meningococcemia, Rocky Mountain spotted fever,toxic epidermal necrolysis, Stevens-Johnson syndrome
Severe localized pain/tenderness in extremity Necrotizing fasciitis, cellulitis
Recent new drug use (1-4 weeks) Cutaneous drug reaction, photosensitivity, erythema multiforme, toxic epidermalnecrolysis, Stevens-Johnson syndrome, hypersensitivity syndrome
Arthralgias Rocky Mountain spotted fever, drug reaction, viral illness

Emergency Medicine Practice 4 www.empractice.net • September 2002
prone to infections due to a decrease in their immunestatus. While most patients with rash and fever have abenign viral exanthem, fever will also accompany lethalconditions such as Rocky Mountain spotted fever andmeningococcemia. Other causes of fever include malig-nancy and certain medications.
Petechiae or purpura can be seen in some benignconditions; however, their presence should “raise theantennae” of the emergency physician.
Lesions of the oral or genital mucosa, as seen inStevens-Johnson syndrome, may suggest that a severesystemic process is present, usually due to drugs or aninfectious process.
Altered mental status or confusion should alert theemergency physician to the possibility of sepsis,hypoperfusion, and central nervous system involvement,as seen in meningococcemia.
Most rashes are not significantly painful, nor arethey exquisitely tender to the touch. Patients who havepain out of proportion to tenderness of an extremity mayhave necrotizing fasciitis. (Necrotizing fasciitis is dis-cussed in further detail in the January 2001 issue ofEmergency Medicine Practice, “Skin And Soft-TissueInfections: The Common, The Rare, And The Deadly.”)
HistoryGathering data about the character and progressionof the rash, along with other key elements of the patienthistory, is essential to detect life-threatening rashes.The following key questions should be a part of everypatient history:
1. When did the rash appear, and how quickly did itprogress? The most lethal rashes often progressrapidly. Acute urticaria with anaphylaxis can startwithin minutes after contact with the inciting agent.(See the April 2000 issue of Emergency MedicinePractice, “Allergic Emergencies And Anaphylaxis:How To Avoid Getting Stung.”) The petechial rash ofRocky Mountain spotted fever generally occurs fourdays after exposure but will then spread swiftly.7 Inmeningococcemia, the rash can progress over hours.A non-allergic drug-induced rash can take days orweeks to evolve.8
2. Did the rash change over time? Certain rashes changetheir morphology over time. For example, thelesion of anthrax begins as a pruritic papule thatthen forms an ulcer over 24-48 hours, finally becom-ing a black eschar after seven days. (See the July2002 issue of Emergency Medicine Practice,“Bioterrorism And The Emergency Physician:On The Front Lines.”)
3. What was the progression of the rash? Where did therash start? Vasculitic rashes generally spread in aperipheral-to-central pattern, whereas viral rashes(e.g., varicella) start centrally and spread peripher-ally.9 A localized rash that does not progress maymean a contact dermatitis depending on thesituation (e.g., dermatitis on both hands afterwearing latex gloves).
4. Is the lesion pruritic? Itching is probably a primitiveform of pain, mediated by histamine released bymast cells. Other mediators of itch include opioidpeptides, prostaglandins, and tachykinins. Diffusepruritus without a rash can be seen in biliarycirrhosis or certain cancers, especially lymphomas.Pruritus with a diffuse rash may be from an acuteallergic reaction or other inciting agents, such asdermatitis herpetiformis from gluten sensitivity.Scabies and poison ivy, in particular, usually presentwith a profound itch, although the most commonreason for pruritus is xerosis (dry skin).10
5. Has there been any recent travel? Travel to certaingeographical regions may expose the patient toorganisms not typically seen in your ED. Forexample, a petechial rash in someone who has beento a wooded area may be Rocky Mountain spottedfever or ehrlichiosis. Lyme disease is endemic in theNortheast, mid-Atlantic, north Central, and far Westregions of the United States.11 Consider typhus ifthere is a history of flea bites, travel to the south-western United States, and a maculopapular rashthat spreads from the trunk to the extremities.Hemorrhagic fevers present with a maculopapularrash and recent travel; dengue fever is endemic toparts of the Caribbean, while Ebola is found in sub-Saharan Africa.
6. What is the patient’s past medical history? A person’smedical history may predispose him or her to certaindermatologic findings. For example, patients with anartificial heart valve, cardiac valvular lesions, or IVdrug use may have endocarditis. Certain cutaneousconditions tend to recur in the same patient, such asherpes zoster associated with HIV or recurrenterythema multiforme following herpes simplex ormycoplasma infections.
Inquire about the patient’s immune status. Anasplenic or immunocompromised patient is suscep-tible to encapsulated organisms such as meningococ-cemia. HIV disease and chemotherapy predispose tothrombotic thrombocytopenic purpura, while thosewho are diabetic, debilitated, or alcoholic arevulnerable to necrotizing fasciitis.
7. What is the patient’s occupation? Daycare workers,college students, and military personnel are suscep-tible to outbreaks of meningococcemia, while postalworkers or healthcare professionals may be exposedto anthrax. Consider tularemia in a game trapperwho presents with regional adenopathy, an ulceratedlesion, and flu symptoms.
8. What medications is the patient taking? Cutaneous drugreactions occur in about 2%-3% of hospitalizedpatients and 1% of outpatients.12 While most reac-tions are benign maculopapular or fixed eruptions,life-threatening presentations may occur. Suchpotentially lethal conditions include Stevens-Johnson syndrome and toxic epidermal necrolysis.Immediate life-threatening drug reactions includeanaphylaxis and angioedema, both of which can
5 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
compromise the airway.13
Determine whether the patient used any creamsor medications that may have altered the morphol-ogy of the rash. Diphenhydramine or topicalcorticosteroids may decrease the erythema orurticaria of a histamine-mediated rash.
Physical ExaminationPerform the physical examination in a systematic fashionfrom head to toe, paying special attention to abnormalvital signs. When evaluating a rash, the “get naked”policy should be enforced (for the patient). Patients oftenremain blissfully unaware of a rash on their back,buttocks, perineum, or soles. Look carefully for involve-ment of the mucous membranes (mouth, lips, conjunc-tiva, anus, and vagina). Adequate exposure and goodlighting are important when looking at a rash; naturallight or white light is recommended. Touch the rash(with gloved hands, as lesions of secondary syphilisare contagious and no one knows how far scabies canjump). Press on lesions to see whether they blanch tobetter diagnose petechiae. Rub erythematous skin tosee if it sloughs. This result, known as Nikolsky’s sign,signifies a potentially life-threatening diagnosis suchas toxic epidermal necrolysis.
The goal of the physical examination is notnecessarily an instant diagnosis. In many cases, itis enough to detect toxicity and categorize the rashso that it can be identified with the aid of books ora consultant.
General Appearance And Vital SignsBefore closely examining the rash, assess the generalappearance of the patient. Abnormal vital signs orevidence of toxicity should prompt interventions andaccelerate the evaluation.
Head-To-Toe Examination• Head: Look at the patient’s scalp, conjunctiva, and
oral mucosa. Oral ulcers or blisters imply a serioussystemic reaction, as seen, for example, in Stevens-Johnson syndrome or pemphigus vulgaris. Thepresence of oral thrush suggests HIV-related disease(although it can be seen in patients with uncontrolleddiabetes and those who have recently completed acourse of antibiotics). Conjunctival injection is foundin Kawasaki disease and viral syndromes. Whenendocarditis is a possibility, a funduscopic exam mayreveal Roth’s spots, which appear as white-centeredretinal hemorrhages.
• Neck: In the ill-appearing patient, check for nuchalrigidity and other meningeal signs. In potential casesof anaphylaxis, look for signs of airway compromise,such as stridor, drooling, or laryngeal swelling.
• Lymph nodes: Adenopathy is a nonspecific findingseen with drug reactions such as serum sickness andhypersensitivity syndrome. Adenopathy may beassociated with infections, including viral, bacterial,rickettsial, and spirochetal disease. Mononucleosis isa common cause of generalized adenopathy. Theacute retroviral syndrome that occurs with the initial
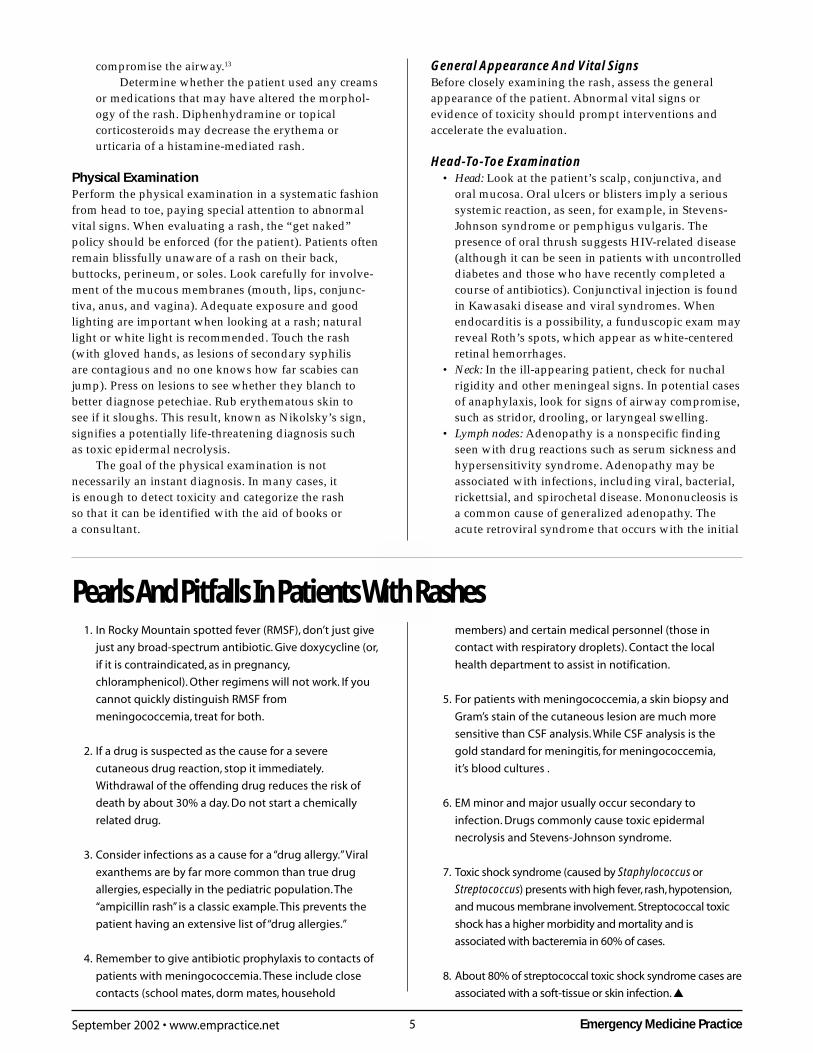
Pearls And Pitfalls In Patients With Rashes1. In Rocky Mountain spotted fever (RMSF), don’t just give
just any broad-spectrum antibiotic. Give doxycycline (or,
if it is contraindicated, as in pregnancy,
chloramphenicol). Other regimens will not work. If you
cannot quickly distinguish RMSF from
meningococcemia, treat for both.
2. If a drug is suspected as the cause for a severe
cutaneous drug reaction, stop it immediately.
Withdrawal of the offending drug reduces the risk of
death by about 30% a day. Do not start a chemically
related drug.
3. Consider infections as a cause for a “drug allergy.” Viral
exanthems are by far more common than true drug
allergies, especially in the pediatric population. The
“ampicillin rash” is a classic example. This prevents the
patient having an extensive list of “drug allergies.”
4. Remember to give antibiotic prophylaxis to contacts of
patients with meningococcemia. These include close
contacts (school mates, dorm mates, household
members) and certain medical personnel (those in
contact with respiratory droplets). Contact the local
health department to assist in notification.
5. For patients with meningococcemia, a skin biopsy and
Gram’s stain of the cutaneous lesion are much more
sensitive than CSF analysis. While CSF analysis is the
gold standard for meningitis, for meningococcemia,
it’s blood cultures .
6. EM minor and major usually occur secondary to
infection. Drugs commonly cause toxic epidermal
necrolysis and Stevens-Johnson syndrome.
7. Toxic shock syndrome (caused by Staphylococcus or
Streptococcus) presents with high fever, rash, hypotension,
and mucous membrane involvement. Streptococcal toxic
shock has a higher morbidity and mortality and is
associated with bacteremia in 60% of cases.
8. About 80% of streptococcal toxic shock syndrome cases are
associated with a soft-tissue or skin infection. ▲

Emergency Medicine Practice 6 www.empractice.net • September 2002
infection of HIV presents as a “mono-like” illnesswith diffuse rash and generalized lymphadenopathy.
Look for regional lymphadenopathy as well.Patients with Kawasaki disease usually demonstratecervical lymphadenopathy, with at least one lymphnode measuring 1.5 cm or more in diameter. Post-auricular nodes accompany adenovirus infection. Inaddition to the cervical nodes, evaluate for adenopa-thy proximal to an extremity lesion. The axillarynodes are often swollen in cutaneous anthrax of theupper extremity.
• Lung: Observe for signs of bronchial constrictionand edema, such as tachypnea, wheezing, andretractions that may accompany acute allergicreactions or early sepsis.
• Cardiovascular: While most heart murmurs areeither functional or benign, they may be associatedwith endocarditis—especially in the setting of IVdrug abuse.
• Abdominal: Palpate for hepatosplenomegaly, whichcan occur with drug hypersensitivity or viral illness.Non-surgical diffuse abdominal pain may occur withallergic angioedema, while dull right upper quadrantpain suggests a hepatitis-related rash. Look for alaparotomy scar. If present, ask the patient, “Are yousure you still have your spleen?”
• Trunk and chest: Most viral exanthems start on thetrunk and then spread to the extremities (centrifugalspread). These rashes are fine, macular papularerythematous eruptions that usually becomeconfluent. Drug allergies usually begin on the trunkas discrete macules/papules, which spare the face,and then spread to the extremities. Bullous lesions ina dermatomal pattern are likely to be herpes zoster.Fine, scaling, faint pink papules in a “Christmastree” pattern in the trunk may be pityriasis rosea,especially if accompanied by a “herald patch.” Thisoval lesion marks the first appearance of pityriasisrosea and is usually found on the trunk. It measures1-2 cm in diameter and has central pink area,sometimes lined with small scales, surrounded by adarker peripheral zone.
• Genital: Look in the mucosal areas of the anus andscrotum or vulva for target lesions and bullouslesions characteristic of erythema multiforme orStevens-Johnson syndrome.
Tinea cruris and erythrasma are also found inthe genitocrural area. Both conditions present with afinely wrinkled, scaly rash that is reddish-brown incolor. When erythrasma is viewed under a Wood’slamp, it fluoresces a bright coral red. Diffuse tendererythema around the scrotal and perineal areas(especially if associated with subcutaneous air) mayrepresent Fournier’s gangrene. (See the November2000 issue of Emergency Medicine Practice, “MaleGenitourinary Emergencies: Preserving Fertility AndProviding Relief.”)
• Extremities: Palpable purpura and petechiaeusually present in the extremities, especially
around the ankles and wrists. The petechial rashof Rocky Mountain spotted fever spreads from thewrists and ankles toward the body (centripetalspread). Pain out of proportion to tenderness isfound with necrotizing fasciitis; in this case, theaffected limb may become tense with shinyerythema. (See the January 2001 issue of EmergencyMedicine Practice, “Skin And Soft-Tissue Infections:The Common, The Rare, And The Deadly.”) Sparsehemorrhagic pustules about the hands and feetimply gonococcemia.
• Joints: Arthralgias are thought to be the result ofantibody-antigen deposits in joints and may be asign of serum sickness. Arthralgias with a rash areseen in Rocky Mountain spotted fever, drug reac-tions, and bacterial and viral illnesses. Disseminatedgonococcal infection may present with frank arthritisand a meager hemorrhagic-pustular rash.
• Palms and soles: Involvement of the palms and solesusually signifies inflammation of the small vesselsand can be drug-induced or pathogen-induced.8 Theclassic target lesions of erythema multiforme areoften found on the palms and soles. The “nickel anddime” lesions of secondary syphilis are similarlyprominent in these areas. In secondary syphilis, thesesymmetric lesions begin as faint papulosquamousmacules that darken over time. In toxic epidermalnecrolysis, Kawasaki disease, scarlet fever, and toxicshock syndrome, there is late desquamation of thehands and feet. However, since desquamationusually occurs 7-10 days after the acute illness, thisfinding is usually not helpful in the ED.
• Nails and fingers: These areas provide important cluesto the diagnosis of endocarditis. Splinter hemor-rhages are found under the nails, while Osler’snodes are pea-sized subcutaneous nodules in thepulp of the fingers or toes. Janeway lesions are non-tender erythematous, hemorrhagic macules on thepalmar aspect of the fingers.
“I’m tired of all this nonsense about beauty being onlyskin-deep….What do you want—an adorable pancreas?”
—Jean Kerr
The Skin ExaminationFirst, the clinician should get an overall view of the rash,and then the primary lesion can be closely examined. Amagnifying glass may be helpful when looking at a singlelesion. The lesion should be palpated with a glovedfinger to assess its texture and to see if the lesionblanches. If it is unclear whether a lesion blanches, use aglass slide to compress the area.
The following four major skin signs should be notedduring the evaluation of any skin lesion or rash:14
1. Type of lesion: This description should be for therepresentative lesion, as described in Table 1. Note ifthere are any secondary changes or if there arescaling, crusts, or fissures, as described in Table 2.Determine the color of the lesion and assess for
7 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
erythema, desquamation, and tenderness.2. Shape of the individual lesion: Is the lesion round, oval,
annular (ringed-shaped as in anthrax), iris-shaped(as in erythema multiforme), umbilicated (mollus-cum), or irregular (petechial)?
3. Arrangement of multiple lesions: Are the lesionsisolated, grouped (linear, annular, serpiginous),or disseminated (scattered discrete lesions, ordiffuse involvement as in viral exanthem or drugallergy)? Linear patterns not in a dermatomaldistribution usually signify contact dermatitis(e.g., poison ivy) and, when located in the fingerweb spaces, scabies. A scattered, diffuse macularrash suggests a drug allergy.
4. Pattern of the rash: Pattern is the functional/physi-ologic arrangement of the lesion, such as sun-exposed area, flexor/extensor surface, or hair-bearing areas. Also, note if the distribution issymmetrical or unilateral. Bilateral symmetryusually signifies a systemic internal event, whereasisolated lesions indicate a local process such ascontact dermatitis. A rash in a sun-exposed distribu-tion is compatible with a photosensitive drugreaction (e.g., tetracycline).
General Diagnostic TestingBlood TestsThere are few studies that provide an evidence-basedapproach to laboratory testing in patients with a rash.Furthermore, with the exception of secondary syphilis,blood tests will almost never supply the etiology of a rashin the ED. In patients who are not toxic or febrile,laboratory testing is driven by clinical suspicion. If therash appears benign, then laboratory studies are gener-ally unnecessary.
This said, toxic-appearing patients with an unex-plained rash and fever may benefit from a completeblood count with differential, along with a platelet count,chemistry panel, liver function tests, and blood cultures.The platelet count may implicate thrombocytopenia as acause of petechiae. In the patient with unstable vital signsor who appears dehydrated, a chemistry panel will detectacidosis as well as renal or electrolyte abnormalities.Patients with Stevens-Johnson syndrome or toxicepidermal necrolysis, in particular, may have electrolyteabnormalities from fluid losses through the disruptedskin. Liver function tests may tell the clinician if there ishepatitis, which is occasionally seen with some drughypersensitivity reactions.15
Serology is occasionally useful. A Venereal DiseaseResearch Laboratory (VDRL) or fluorescent treponemalantibodies (FTA) test for syphilis can be diagnostic in aperson with papulosquamous lesions suggestive of thedisease. If Lyme disease is suspected, then an IgMantibody to Lyme or rising IgG titers may be sent forconfirmation. However, the sensitivity and specificity arenot perfect, and a positive test does not discriminatebetween previous and current infection. Serologic testingfor Lyme disease is recommended only when the physi-
cian believes the patient has a 20% or greater chance ofharboring active disease.16
ScrapingsIn certain cases, aspirates or scrapings of pustular fluidmay be obtained for Gram’s stain (useful in suspectedcases of anthrax or gonococcemia). When evaluating anunknown ulceration, Tzanck smears are 74% sensitive toherpes infections.17 Potassium hydroxide preparations tolook for hyphae are sometimes useful in the diagnosis ofyeast infections.
Punch BiopsiesPunch biopsies are relatively simple to do. A circularcutting instrument called a trephine is pushed verticallyinto the skin with rotational movements until theinstrument sinks into subcutaneous tissue. The operatorthen lifts the specimen with a toothless forceps, and thebase is cut with iris scissors. Specimens can then be sentin a sterile container for Gram’s staining or other tests(e.g., immunofluorescence).18
Emergency physicians familiar with the techniquecan use punch biopsies to identify a variety of lesions.For example, a febrile patient with a petechial/purpuricrash may have either meningococcemia or RockyMountain spotted fever. A Gram’s stain of a punchbiopsy specimen may identify the organism and stream-line antibiotic selection. The sensitivity for punch biopsyin meningococcemia is approximately 72%.19
Diagnostic Decision Making
After the initial stabilization, history, and physicalexamination, formulate a differential diagnosis using themodified Lynch algorithm presented in the ClinicalPathway on page 13, “Evaluating The Unknown Rash.”The unknown lesion is classified into one of six majorcategories, as described in the Pathway. In the samplecase mentioned at the beginning of this paper, our patient(a 52-year-old man on ticlopidine and methyldopa)presented with a petechial rash and underlyingerythema. Following the Lynch algorithm, the lesionwould be classified first as solid, meaning not vesicularor bullous. Going down the algorithm, the lesion wouldthen be assessed as having erythema, then as petechial/purpuric. The differential diagnosis to entertain wouldinclude vasculitis, thrombotic thrombocytopenic pur-pura, meningococcemia, Rocky Mountain spotted fever,and endocarditis. A history of taking ticlopidine andmethyldopa moves thrombotic thrombocytopenicpurpura to the top of the list. A platelet count in the EDwould have been diagnostic—and possibly life-saving.
Maculopapular Rashes
Maculopapular rashes are the most common types ofrash and have the broadest differential diagnosis. Theyare usually seen with viral illnesses, bacterial infections,drug reactions, and other immune-related syndromes.
It is probably easiest to categorize maculopapular

Emergency Medicine Practice 8 www.empractice.net • September 2002
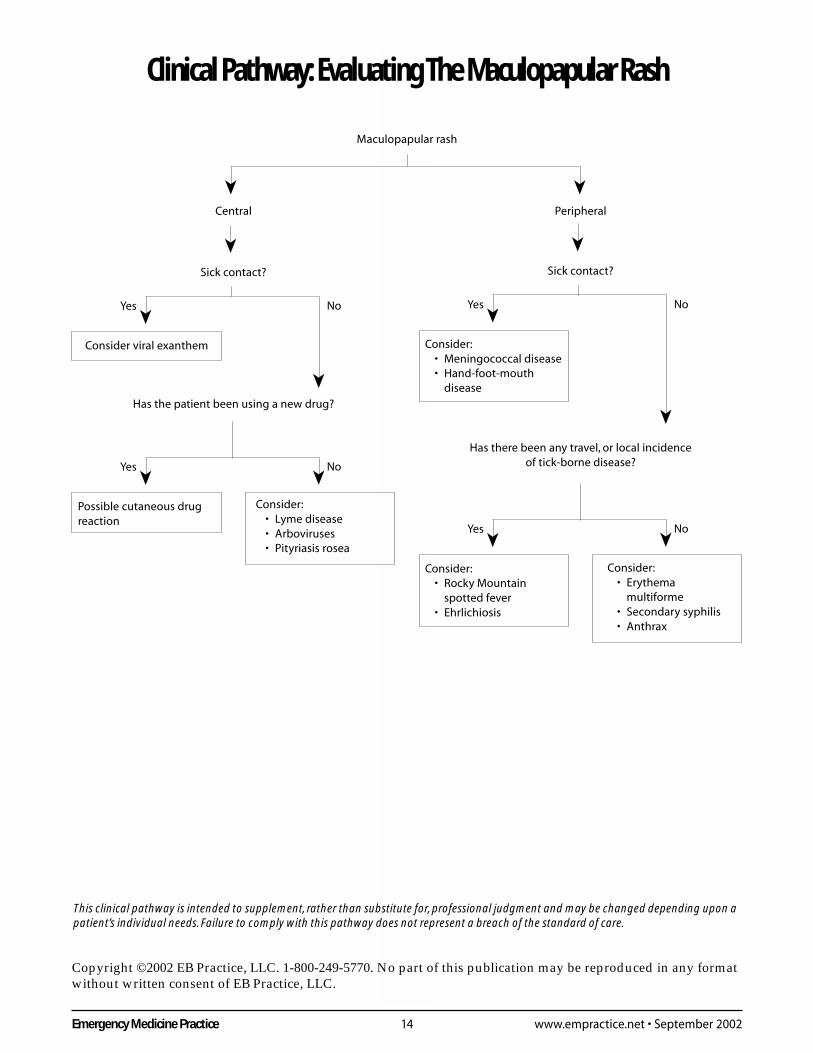
rashes as either principally centrally or peripherallydistributed. (See Table 4 and the Clinical Pathway on page14, “Evaluating The Maculopapular Rash.”) Importanthistorical questions would address sick contacts, travel, andnew medications (within 1-4 weeks).
Viral illnesses—especially mumps, measles, andrubella—generally begin as central lesions. Other viralculprits include Epstein-Barr virus, enteroviruses, andadenoviruses. In children, roseola (human herpes virus6), erythema infectiosum (fifth disease), and parvovirusB19 are frequent causes of maculopapular rash.
The lesions of Lyme disease (termed erythemamigrans) usually begin in the proximal extremities, chest,and body creases.20 The primary lesion is an expandingerythema with a central pallor, sometimes with a centralnecrosis. Arboviruses (dengue fever, West Nile virus)cause fever, chills, myalgias, and a dense maculopapularrash on the trunk.21
Ehrlichiosis is a tick-borne disease caused by anobligate intracellular bacteria commonly seen in the mid-Atlantic and central Southwest states. In 30% of the cases,there is a central-appearing maculopapular rash. Patientsmay present with fever, headaches, abdominal pain,leukopenia, lymphopenia, and thrombocytopenia.
The most serious diseases to consider with peripheralmaculopapular rashes include the early stages of menin-gococcemia and Rocky Mountain spotted fever (whichare described in further detail in a later section) as well asthe early stages of anthrax (as described in the July 2002issue of Emergency Medicine Practice.)
Cutaneous Drug ReactionsEtiologyCutaneous drug reactions commonly present as amaculopapular rash. The most commonly involved drugsare sulfonamides, penicillins, anticonvulsants, andnonsteroidal-anti-inflammatory drugs.12
EpidemiologyCutaneous allergic reactions to drugs are reportedin about 1%-3% of hospitalized patients and 1% ofoutpatients.1,8 Fortunately, most drug reactions are notserious, though life-threatening reactions can occur. Themost severe reactions include the hypersensitivitysyndrome, Stevens-Johnson syndrome (SJS), and toxicepidermal necrolysis (TEN).
PathophysiologyCutaneous drug reactions can be immunologic or non-immunologic. Non-immunologic causes account for morethan 75% of cutaneous drug reactions.12
Clinical PresentationMost cutaneous drug eruptions are morbilliform (mean-ing it looks like measles) or exanthematous. The rash iscomprised of brightly erythematous macules andpapules, mostly on the trunk and extremities, discrete insome areas and confluent in others.14 A morbilliform rashoften erupts in patients with mononucleosis who take
ampicillin. This type of rash is self-limited and usuallyresolves without permanent sequelae after the offendingagent is discontinued.
A drug hypersensitivity syndrome is a severe,idiosyncratic systemic reaction. The patient has a severeexanthematous rash that may exfoliate, often combinedwith fever, hepatitis, nephritis, carditis, facial swelling,and/or lymphadenopathy. The hypersensitivity syn-drome usually develops 2-6 weeks after a drug is started,vs. 1-3 weeks as seen in TEN or SJS. Drugs commonlyimplicated are phenytoin, carbamazepine, phenobarbital,sulfonamides, allopurinol, and dapsone. The incidencemay be higher in blacks and in people who have slowN-acetylation of sulfonamides.23 Drugs with a long half-life are more likely to result in a fatal outcome thanreactions from drugs with a short half-life.24
DiagnosisThe diagnosis is essentially clinical. While a skin biopsydoes not help identify the offending agent, it can assistthe consultant in defining the reaction pattern.8,14,22 (SeeTable 5, Table 6, and Table 7 on page 9.)
TreatmentThe first step in managing a suspected cutaneous drugreaction is removing the drug. In one retrospective study,withdrawal of the offending drug reduced the risk ofdeath by about 30% per day.24 If possible, all drug therapyshould be stopped in a patient who develops an unex-plained syndrome of blisters or substantial epidermalerosions accompanied by fever. The need for drugwithdrawal is less clear in patients who present with aminor maculopapular eruption with or without pruritus.Routine use of corticosteroids is not indicated.25,26 Oralantihistamines (diphenhydramine 25-50 mg PO q6h prn)may alleviate pruritus. Alternatives include hydroxyzine,certirizine, or loratadine, which have the advantage ofless sedation. An evidence-based review on the efficacyof antihistamines in relieving pruritus showed no
Table 4. Differential DiagnosisOf Maculopapular Rashes.
Centrally distributed rash• Viral exanthem: Rubela, rubeola, roseola,
erythema infectiosum, Epstein-Barr virus,enterovirus, adenovirus, arboviruses
• Lyme disease• Typhus fever• Ehrlichiosis• Meningococcemia (early)• Cutaneous drug allergy eruptions
Peripherally distributed rash• Rocky Mountain spotted fever• Secondary syphilis• Erythema multiforme• Meningococcemia (early)• Hand-foot-mouth disease (coxsackie 16)• Cutaneous anthrax
9 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
differences in the effectiveness of non-sedating antihista-mines vs. diphenhydramine. However, the non-sedatingantihistamines cost about 27 times more than over-the-counter diphenhydramine.27
Distinguishing Between Erythema Multiforme,Stevens-Johnson Syndrome, And ToxicEpidermal NecrolysisErythema multiforme (EM) is the archetypal maculo-papular rash of the extremities. The rash typically beginsas a macular eruption that then progresses to a papulewith a dusky center—the classic “target” lesion.
In the past, EM major and minor, Stevens-Johnsonsyndrome (SJS), and toxic epidermal necrolysis (TEN)were all believed to be part of the same clinical spectrum.Now, EM minor and major are considered distinct from
SJS and TEN.Seven factors distinguish EM minor and major from
SJS and TEN. They are: 1) the etiology; 2) the underlyingpathology; 3) the degree of mucosal involvement (mouth,conjuctiva, rectum, vagina, respiratory tract); 4) thepresence or absence of a “classic rash”; 5) the degree ofepidermal detachment; 6) the degree of multisysteminvolvement; and 7) the morbidity and mortality.8,28,29 (SeeTable 8 on page 10.)
Unlike SJS and TEN, EM minor and major are notcharacterized by epidermal detachment. EM minor presentswith the “classic rash” and has no mucosal involvement.EM major also presents with the “classic rash” but hasonly one mucous membrane involved. Neither SJS norTEN demonstrate the classic target lesions, but both arecharacterized by mucous membrane involvement andepidermal detachment. (Because SJS and TEN producewidespread purpuric macules and mucosal erosions,along with epidermal detachment, they are discussed inmore detail in the section on vesiculo-bullous rashes.) EMminor and major usually occur after an infection (when acause can be identified), whereas SJS and TEN usuallyoccur after drug exposure. In one retrospective study of76 cases, the authors reported that cases could beclassified as either EM or SJS/TEN based on the incitingcause.30 SJS and TEN have greater morbidity and mortal-ity than EM minor and major.
Erythema MultiformeEtiologyEM is a common acute inflammatory disease that isusually self-limited. Many factors have been implicatedin the etiology, including infectious agents, drugs, andmalignancy. (See Table 9 on page 10.) However, in up to50% of cases no etiologic agent can be identified. Inchildren, EM commonly follows a herpes simplex ormycoplasma infection. A recurrent form of EM may
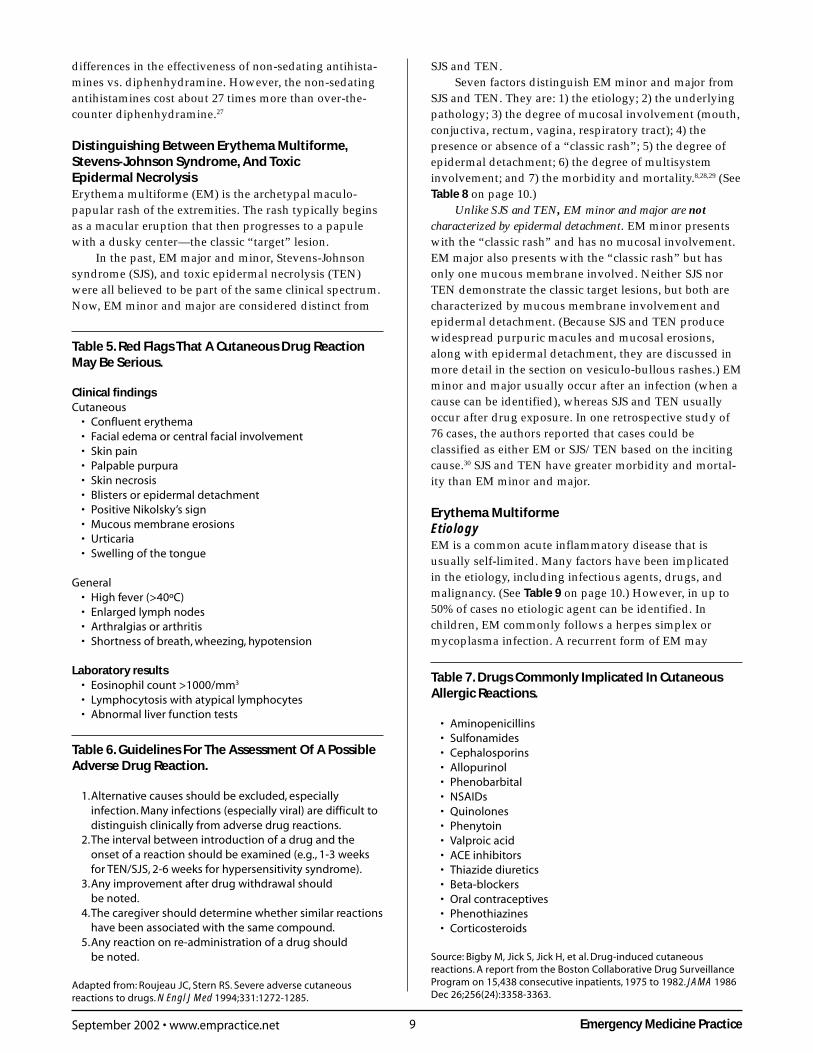
Table 7. Drugs Commonly Implicated In CutaneousAllergic Reactions.
• Aminopenicillins• Sulfonamides• Cephalosporins• Allopurinol• Phenobarbital• NSAIDs• Quinolones• Phenytoin• Valproic acid• ACE inhibitors• Thiazide diuretics• Beta-blockers• Oral contraceptives• Phenothiazines• Corticosteroids
Source: Bigby M, Jick S, Jick H, et al. Drug-induced cutaneousreactions. A report from the Boston Collaborative Drug SurveillanceProgram on 15,438 consecutive inpatients, 1975 to 1982. JAMA 1986Dec 26;256(24):3358-3363.
Table 6. Guidelines For The Assessment Of A PossibleAdverse Drug Reaction.
1.Alternative causes should be excluded, especiallyinfection. Many infections (especially viral) are difficult todistinguish clinically from adverse drug reactions.
2.The interval between introduction of a drug and theonset of a reaction should be examined (e.g., 1-3 weeksfor TEN/SJS, 2-6 weeks for hypersensitivity syndrome).
3.Any improvement after drug withdrawal shouldbe noted.
4.The caregiver should determine whether similar reactionshave been associated with the same compound.
5.Any reaction on re-administration of a drug shouldbe noted.
Adapted from: Roujeau JC, Stern RS. Severe adverse cutaneousreactions to drugs. N Engl J Med 1994;331:1272-1285.
Table 5. Red Flags That A Cutaneous Drug ReactionMay Be Serious.
Clinical findingsCutaneous
• Confluent erythema• Facial edema or central facial involvement• Skin pain• Palpable purpura• Skin necrosis• Blisters or epidermal detachment• Positive Nikolsky’s sign• Mucous membrane erosions• Urticaria• Swelling of the tongue
General• High fever (>40ºC)• Enlarged lymph nodes• Arthralgias or arthritis• Shortness of breath, wheezing, hypotension
Laboratory results• Eosinophil count >1000/mm3
• Lymphocytosis with atypical lymphocytes• Abnormal liver function tests
Emergency Medicine Practice 10 www.empractice.net • September 2002
develop after each episode of herpes simplex.
PathophysiologyThe pathogenesis of EM is not clearly understood but ismost likely caused by an immune complex-mediatedhypersensitivity reaction.31
EpidemiologyThe true incidence of EM is not known. It occurs in allage groups but is more common in those 20-40 years old.
Morbidity And MortalityDeath from EM is rare. However, if patients have ocularinvolvement, disabling and permanent visual sequelaemay occur. Scarring of the skin is unusual except inhyper-pigmented patients.
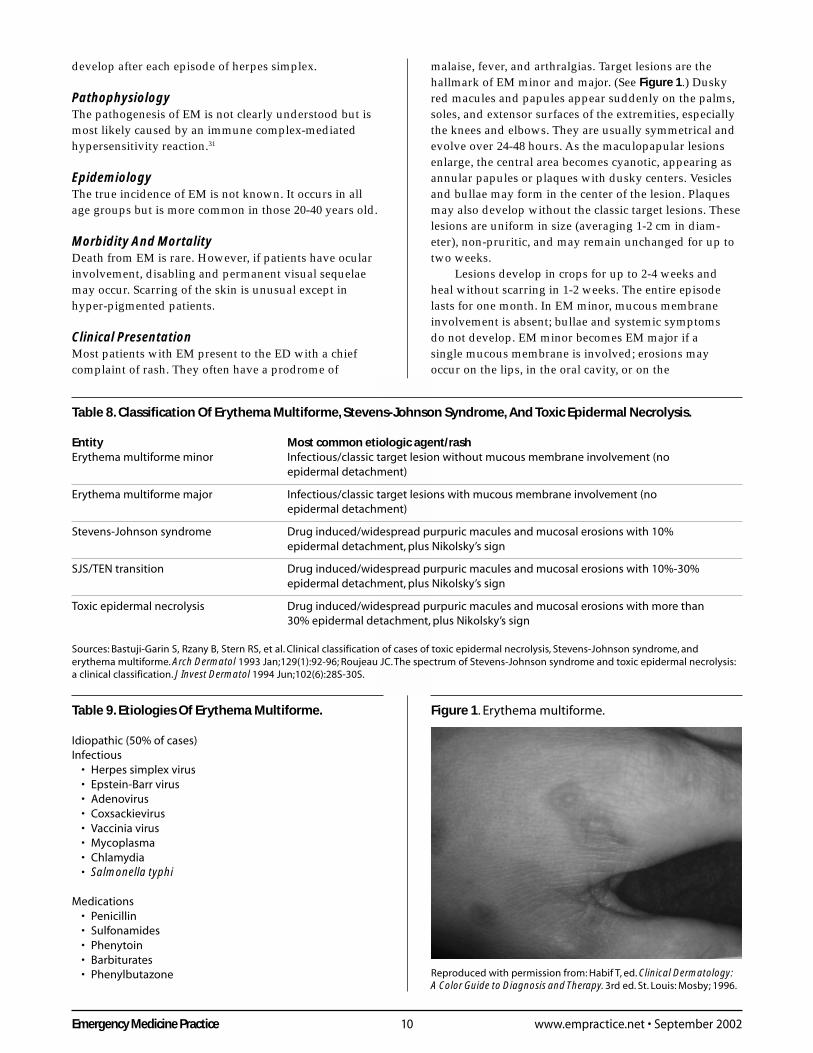
Clinical PresentationMost patients with EM present to the ED with a chiefcomplaint of rash. They often have a prodrome of
malaise, fever, and arthralgias. Target lesions are thehallmark of EM minor and major. (See Figure 1.) Duskyred macules and papules appear suddenly on the palms,soles, and extensor surfaces of the extremities, especiallythe knees and elbows. They are usually symmetrical andevolve over 24-48 hours. As the maculopapular lesionsenlarge, the central area becomes cyanotic, appearing asannular papules or plaques with dusky centers. Vesiclesand bullae may form in the center of the lesion. Plaquesmay also develop without the classic target lesions. Theselesions are uniform in size (averaging 1-2 cm in diam-eter), non-pruritic, and may remain unchanged for up totwo weeks.
Lesions develop in crops for up to 2-4 weeks andheal without scarring in 1-2 weeks. The entire episodelasts for one month. In EM minor, mucous membraneinvolvement is absent; bullae and systemic symptomsdo not develop. EM minor becomes EM major if asingle mucous membrane is involved; erosions mayoccur on the lips, in the oral cavity, or on the
Table 9. Etiologies Of Erythema Multiforme.
Idiopathic (50% of cases)Infectious
• Herpes simplex virus• Epstein-Barr virus• Adenovirus• Coxsackievirus• Vaccinia virus• Mycoplasma• Chlamydia• Salmonella typhi
Medications• Penicillin• Sulfonamides• Phenytoin• Barbiturates• Phenylbutazone
Figure 1. Erythema multiforme.
Reproduced with permission from: Habif T, ed. Clinical Dermatology:A Color Guide to Diagnosis and Therapy. 3rd ed. St. Louis: Mosby; 1996.
Table 8. Classification Of Erythema Multiforme, Stevens-Johnson Syndrome, And Toxic Epidermal Necrolysis.
Entity Most common etiologic agent/rashErythema multiforme minor Infectious/classic target lesion without mucous membrane involvement (no
epidermal detachment)
Erythema multiforme major Infectious/classic target lesions with mucous membrane involvement (noepidermal detachment)
Stevens-Johnson syndrome Drug induced/widespread purpuric macules and mucosal erosions with 10%epidermal detachment, plus Nikolsky’s sign
SJS/TEN transition Drug induced/widespread purpuric macules and mucosal erosions with 10%-30%epidermal detachment, plus Nikolsky’s sign
Toxic epidermal necrolysis Drug induced/widespread purpuric macules and mucosal erosions with more than30% epidermal detachment, plus Nikolsky’s sign
Sources: Bastuji-Garin S, Rzany B, Stern RS, et al. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, anderythema multiforme. Arch Dermatol 1993 Jan;129(1):92-96; Roujeau JC. The spectrum of Stevens-Johnson syndrome and toxic epidermal necrolysis:a clinical classification. J Invest Dermatol 1994 Jun;102(6):28S-30S.
11 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
conjunctiva. Up to 10% of patients with EM majorhave ocular involvement.32
DiagnosisThe diagnosis of EM is clinical. The diagnosis is mostensured when classic target lesions are present. If thepatient does not have target lesions, another diagnosisshould be considered. Similarly, if the patient looks toxic,has systemic complaints, or has abnormal vital signs,consider an alternative diagnosis.
ManagementEM minor and major generally resolve without treatmentin 2-3 weeks. Any underlying infection should be treated.While many physicians treat EM with prednisone,supporting data remain weak to nonexistent, involvingjust a handful of patients. A prospective study of 16children with EM major treated with steroids showed asignificant reduction in the period of fever and reductionin the period of the eruption.33 Another prospective studyof three patients with EM minor showed a rapid responseto steroid therapy.34 However, other larger studiessuggest minimal to no benefit from treatment withsteroids.35,36 Based on a review of the literature, there is nostrong evidence that steroids are beneficial in EM minor ormajor. The best ED intervention is to determine (and ifpossible treat) the cause of the rash and providesymptomatic relief using systemic antihistaminesand possibly analgesia.
DispositionEssentially all patients diagnosed with EM minor ormajor can be safely discharged home. Follow-up withthe primary medical doctor or dermatologist ishelpful. Patients must return to the ED if there israpid progression of the rash or new systemicsymptoms. Follow-up with an ophthalmologist isessential in cases of ocular involvement.
“You know what happens to scar tissue.It’s the strongest part of your skin.”—Michael R. Mantell
Vesiculo-Bullous Rashes
Vesicles and bullae appear in many disorders. Some ofthese disorders are benign—such as poison ivy or a mildcase of varicella zoster—whereas others are potentiallylife-threatening, such as SJS, TEN, and pemphigusvulgaris (PV).
Stevens-Johnson SyndromeAnd Toxic Epidermal NecrolysisEtiologySJS and TEN are related to the use of certain medications.Anticonvulsants, sulfonamides, other antibiotics, andnon-steroidal anti-inflammatory drugs (NSAIDs) are themain offenders.22 (See Table 10.) In one retrospectivestudy, sulfonamides were found to be the etiology in 30cases, NSAIDs in 29 cases, anticonvulsants in seven cases,
and allopurinol in three.37 Fewer than 5% of patients withTEN report no drug use.38
PathophysiologyThe pathophysiology of SJS and TEN is not completelyunderstood. Some studies suggest it is the result of analtered metabolism and immune-mediated response.39,40
EpidemiologyThe incidence of TEN varies from 0.4-1.2 cases permillion per year.38 TEN occurs in all age groups but ismore common in adults over 40. SJS commonly occurs inchildren and young adults. While HIV patients arepredisposed to TEN, HIV is not considered to be acausative factor.41
Morbidity And MortalityThe leading causes of death in TEN are sepsis fromStaphylococcus aureus or Pseudomonas aeruginosa andfluid/electrolyte abnormalities.38,42 The severity ofcomplications is proportional to the extent of skinnecrosis. Massive transepidermal fluid losses canproduce significant electrolyte imbalance; prerenalazotemia is common. Bacterial colonization of the skinand decreased immune responsiveness leads to sepsis.
The mortality rate is 5%-10% for SJS and 23%-30%for TEN.42 The mortality rate is higher still in elderlypatients—51% in one retrospective study of 77 elderlypatients with TEN.43 Variables associated with a poorprognosis include increased age, extent of disease, extentof disease at time of transfer to a burn center, azotemia,multiple medication use, thrombocytopenia, and neutro-penia.38,44 Ophthalmologic sequelae such as keratitis andcorneal ulcerations, cornel scarring, and blindness occurin 40%-50% of patients.45
Clinical PresentationIn both SJS and TEN, patients present with a chiefcomplaint of a rash. Some experience prodromal symp-toms similar to a viral illness such as myalgias, fever,cough, or sore throat. If a new drug is the cause, theprodrome usually begins within days of ingestion. Skinlesions then develop suddenly, after 1-2 weeks ofprodromal symptoms.
Skin lesions in SJS look like atypical target lesions orpurpuric macules on the trunk. (This is in contrast to EMminor and major, where the majority of the distribution is
Table 10. Etiologic Agents In Stevens-JohnsonSyndrome And Toxic Epidermal Necrolysis.
• Sulfonamides• Penicillins• Quinolones• Phenytoin• Phenobarbital• Carbamazepine• NSAIDs• Allopurinol

Emergency Medicine Practice 12 www.empractice.net • September 2002
on the face and extensor surfaces of the extremities.)Patients commonly develop oropharyngeal lesionscausing an erosive stomatitis. A purulent conjunctivitiscan lead to ocular erosions and blindness. SJS is a self-limited disease; new lesions may appear, but they usuallyresolve in one month.
In contrast to SJS, patients with TEN complain ofskin tenderness, pruritus, and pain. Onset is more rapidwith repeated ingestion of the inciting agent. Objectiveskin findings are characterized by a warm and tendererythema that first affects the face around the eyes, nose,and mouth. Erythema then extends to the shoulders andtrunk and proximal extremities in a symmetric fashion.All areas become confluent over several hours to days.Small, irregularly confluent bullae form within the areasof erythema. Lateral pressure on normal skin adjacent to abullous lesion dislodges the epidermis. (This is known asNikolsky’s sign.) (See Figure 2.) Bullae form between theepidermis and dermis, leading to widespread sloughingof the epidermis in large sheets and resulting in sizeableareas of exposed dermis.
Mucous membrane involvement is characteristic ofTEN. Stomatitis or conjunctivitis may precede thegeneralized erythematous rash by 24-48 hours. Mostpatients have erythema and sloughing of the lips andbuccal mucosa. In about three-quarters of patients, theeyes are also affected, producing conjunctivitis or painfulerosions. These lesions can form synechiae between theeyelids and the conjunctiva, causing blindness. Up to halfof patients develop genital and anal lesions.46 Respiratoryfailure can also occur.
The appearance of dermatologic manifestations ofTEN is variable and unpredictable, ranging from 24hours to two weeks. Re-epithelialization begins afterseveral days, and most of the skin surface is re-epithelial-ized in three weeks. Mucosal lesions may remain crustedfor two or more weeks.
The clinically distinguishing features of SJS and TEN isthe degree of epidermal detachment. SJS involves mucosalerosions and less than 10% of epidermal detachment.TEN is defined by more than 30% of epidermal detach-ment. (See Figure 3.) Between 10%-30% is considered theoverlap zone of SJS and TEN.
DiagnosisAs with most rashes, the diagnosis SJS and TEN isclinical. However, it can be confirmed by biopsy, whichwill demonstrate detachment of the epidermis from thedermis. The visual appearance of TEN is very similar tothat of staphylococcal scalded skin syndrome (SSSS).Biopsy distinguishes these conditions, as the split in SSSSis high in the epidermis below the stratum corneum. SSSSalso tends to occur in infants and children less than fiveyears of age and is rare in adults.
TreatmentTreatment for SJS and TEN is supportive. Managementfocuses on removal of the offending agent and replace-ment of fluid losses. Patients are treated in a mannersimilar to burn victims. They should have two IV lines inplace and be placed on a monitor. IV fluid repletion withlarge volumes of colloids and crystalloids is essential,with special attention to electrolyte balance. Provideliberal doses of analgesics; oral symptoms can be relievedwith viscous lidocaine. All drugs started within the pastmonth should be discontinued. Avoid topical sulfa-containing preparations such as Silvadene (silversulfadiazine) due to possible cross-reactivity.
The role of corticosteroids in SJS and TEN ishighly controversial. In one retrospective study of 32children with SJS, systemic corticosteroid therapy didnot affect the course of disease.36 One prospective studyshowed higher rates of morbidity and mortality in
Reproduced with permission from: Habif T, ed. Clinical Dermatology:A Color Guide to Diagnosis and Therapy. 3rd ed. St. Louis: Mosby; 1996.
Figure 3. Toxic epidermal necrolysis.
Reproduced with permission from: Habif T, ed. Clinical Dermatology:A Color Guide to Diagnosis and Therapy. 3rd ed. St. Louis: Mosby; 1996.
Figure 2. A positive Nikolsky’s sign in toxic epidermalnecrolysis.
Continued on page 16
13 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
This clinical pathway is intended to supplement, rather than substitute for, professional judgment and may be changed depending upon apatient’s individual needs. Failure to comply with this pathway does not represent a breach of the standard of care.
Copyright ©2002 EB Practice, LLC. 1-800-249-5770. No part of this publication may be reproduced in any formatwithout written consent of EB Practice, LLC.
Clinical Pathway: Evaluating The Unknown Rash
Differential Diagnosis Of Rash By Morphology Types.
Rash type Differential diagnosis
Maculopapular Meningococcemia (early), Rocky Mountain spotted fever (early), toxic shock syndrome,erythema multiforme, cutaneous drug reactions, systemic lupus erythematosus, viralexanthems (rubeola, rubella, Epstein-Barr virus, adenovirus, enterovirus), Lyme disease
Petechial/purpuric Meningococcemia, Rocky Mountain spotted fever, vasculitis(Henoch-Schönlein purpura,hypersensitivity drug reactions, necrotizing fasciitis), gonococcemia, enteroviralinfection, rubella, Epstein-Barr virus, thrombocytopenia, systemic lupus erythematosus,idiopathic thrombocytopenic purpura, thrombotic thrombocytopenic purpura,endocarditis, purpura fulminans
Diffuse erythematous Necrotizing fasciitis, toxic shock syndrome, streptococcal toxic shock syndrome,staphylococcal scalded skin syndrome, Kawasaki disease, erythema multiforme,hypersensitivity drug reactions, cellulitis, viral exanthems, enteroviral infection
Vesiculo-bullous Erythema multiforme major, Stevens-Johnson syndrome, toxic epidermal necrolysis,pemphigus vulgaris, varicella zoster, herpes simplex virus, necrotizing fasciitis (late)
Pustular Bacterial folliculitis, gonorrhea
Non-erythematous Secondary syphilis, anthrax (ulcerated lesions)
Possible life-threatening rash
Fluid-filledSolid➤➤
➤➤
Erythematous Clear Pustular(see below
for differentialdiagnosis)
➤
Vesiculo-bullous(see below
for differentialdiagnosis)
➤➤
Adapted from: Lynch PJ, Edminster SC. Dermatology for the nondermatologist: a problem-oriented system. Ann Emerg Med1984 Aug;13(8):603-606.
➤➤
Petechial/purpuric(see below
for differentialdiagnosis)
Diffuseerythematous(see below for
differentialdiagnosis)
Maculopapular(see below
for differentialdiagnosis)
➤
Non-erythematous(see below
for differentialdiagnosis)
Emergency Medicine Practice 14 www.empractice.net • September 2002
This clinical pathway is intended to supplement, rather than substitute for, professional judgment and may be changed depending upon apatient’s individual needs. Failure to comply with this pathway does not represent a breach of the standard of care.
Copyright ©2002 EB Practice, LLC. 1-800-249-5770. No part of this publication may be reproduced in any formatwithout written consent of EB Practice, LLC.
Clinical Pathway: Evaluating The Maculopapular Rash
Maculopapular rash
PeripheralCentral
➤➤➤
Sick contact?
➤
Sick contact?
➤
➤
Consider viral exanthem
Has the patient been using a new drug?
Yes No
➤
➤
Consider:• Meningococcal disease• Hand-foot-mouth
disease
Has there been any travel, or local incidenceof tick-borne disease?
Yes No
➤➤
Consider:• Rocky Mountain
spotted fever• Ehrlichiosis
Consider:• Erythema
multiforme• Secondary syphilis• Anthrax
Yes No
➤➤
Possible cutaneous drugreaction
Yes No
Consider:• Lyme disease• Arboviruses• Pityriasis rosea
15 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
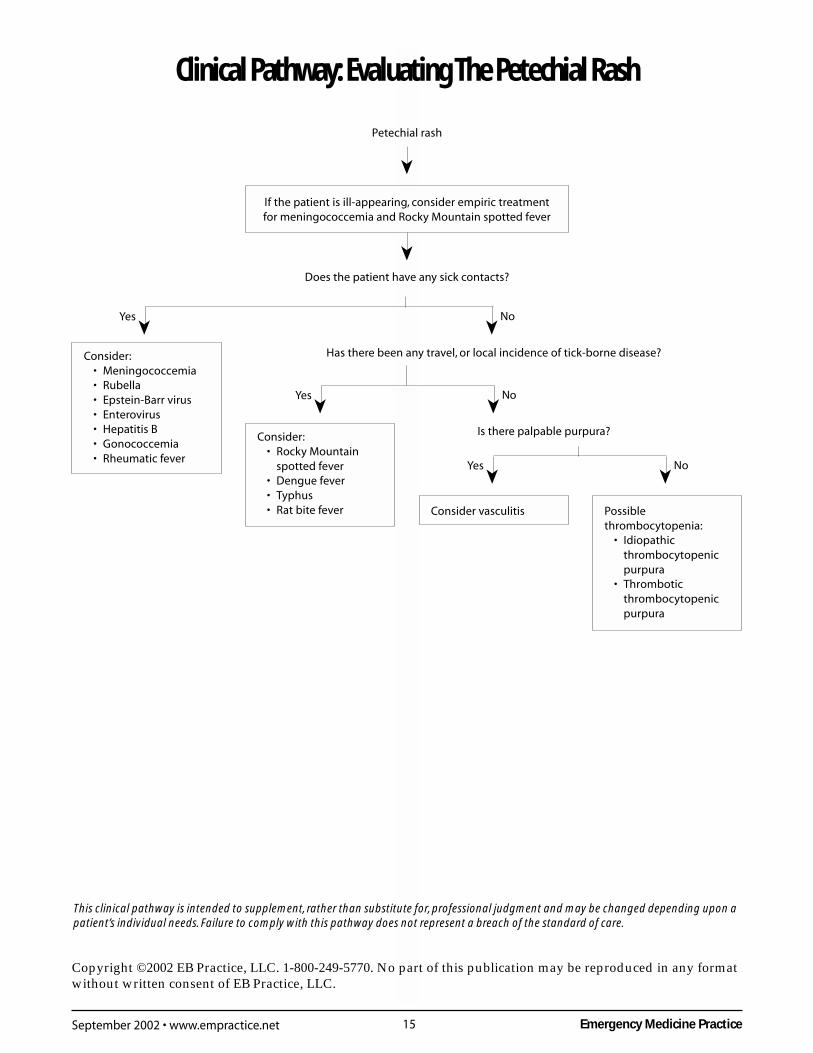
Clinical Pathway: Evaluating The Petechial Rash
Petechial rash
➤
If the patient is ill-appearing, consider empiric treatmentfor meningococcemia and Rocky Mountain spotted fever
➤
Does the patient have any sick contacts?
Consider:• Meningococcemia• Rubella• Epstein-Barr virus• Enterovirus• Hepatitis B• Gonococcemia• Rheumatic fever
Has there been any travel, or local incidence of tick-borne disease?
➤Yes No➤
➤Yes No➤
Consider:• Rocky Mountain
spotted fever• Dengue fever• Typhus• Rat bite fever
Is there palpable purpura?
➤Yes No➤
Consider vasculitis Possiblethrombocytopenia:
• Idiopathicthrombocytopenicpurpura
• Thromboticthrombocytopenicpurpura
This clinical pathway is intended to supplement, rather than substitute for, professional judgment and may be changed depending upon apatient’s individual needs. Failure to comply with this pathway does not represent a breach of the standard of care.
Copyright ©2002 EB Practice, LLC. 1-800-249-5770. No part of this publication may be reproduced in any formatwithout written consent of EB Practice, LLC.
Emergency Medicine Practice 16 www.empractice.net • September 2002
patients treated with corticosteroids—66% survival inthe group treated without corticosteroids vs. 33% inthose treated with corticosteroids. Other trials suggestthat steroids increase the risk of sepsis and delay epithe-lialization,44,45,47 although one prospective trial of 67consecutive patients with SJS treated with steroidsreported no fatalities or adverse affects.48 Based on areview of the literature, there does not appear to be aconsensus on the use of steroids in the treatment of SJS andTEN. Since there is no evidence to support their use,and because steroids may increase morbidity andmortality, avoid using them.
Cyclosporin is occasionally used to treat SJS andTEN, based on very small case series.49,50
As with the burn patient, those with SJS or TENrequire aseptic technique to avoid infection. Use ofadhesive material, ointments, and creams should beavoided. Patients should be covered in a clean whitesheet. Debridement of necrotic tissue may be necessary(usually after the patient is admitted). Prophylacticantibiotic therapy is no longer given for fear of cross-reactivity with the drug that initiated the TEN andbecause of the risk of selecting for resistant organisms.51
DispositionSome patients diagnosed with SJS can be safelydischarged from the ED if all of the following criteriaare met: 1) the patient is non-toxic and has stable vitalsigns; 2) the patient is tolerating oral fluids; 3) the rashis not rapidly progressing; 4) the patient is notimmunocompromised; and 5) close follow-up is ensured.All patients with ocular involvement should be evaluatedby an ophthalmologist soon after discharge.
If these criteria are not met, patients with SJS shouldbe admitted to the hospital for 24-hour observation, IVhydration, local skin care, and nutritional support. Ifthere is any progression of lesions, transfer to a burn orintensive care unit should be considered.
All patients suspected of having TEN should beadmitted to an intensive care unit. Depending on hospitalresources, early transfer to a burn unit may be necessary.In one retrospective review, patients who were treated ina burn unit had lower rates of bacteremia, septicemia,and mortality if transfer was done early in the hospitalcourse (less than seven days).52 An earlier study yieldedsimilar results.53
Pemphigus VulgarisEtiologyPemphigus vulgaris (PV) is a rare but potentially lethalblistering condition predominantly seen in the elderly.This autoimmune disease is characterized by erosionsand blistering of epithelial surfaces of the oral mucosaand skin.
EpidemiologyThe incidence of PV is estimated to be about 4500 cases a
year with a mean age of onset in the sixth decade.Because of a genetic predisposition, patients with PVmay report a family member who once had “bad blis-ters.”54 If not recognized and treated early, PV can leadto significant morbidity (due to pain and disfigurement)and mortality (due to loss of protective barrier andsecondary infection). The natural course of PV isrelentless and progressive over months to years.55 Insome cases, patients may have a rapid progressionwith extensive involvement.56
PathophysiologyPV is characterized by circulating IgG autoantibodies thatbind to the surface of the keratinocytes. This results in theloss of cohesion between the epidermal cells (acantholy-sis), while cells in the basement membrane remainintact.57 Clinically, this means that blisters form within inthe epidermal layer of the skin.
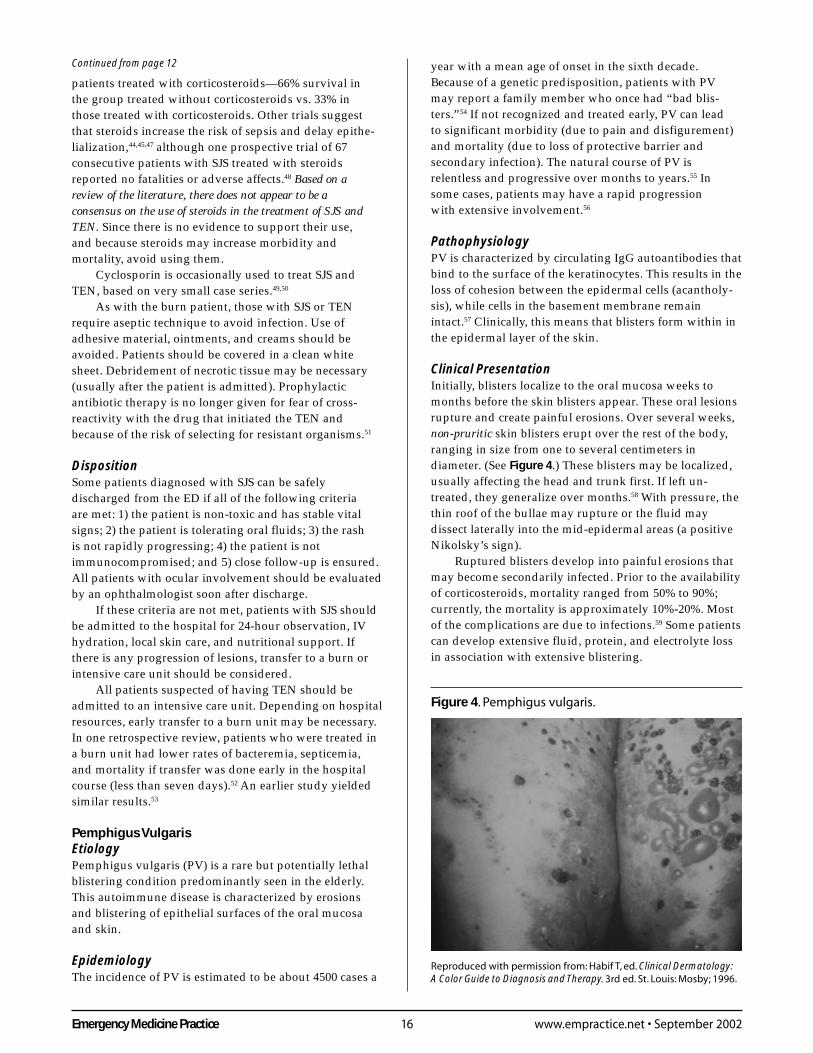
Clinical PresentationInitially, blisters localize to the oral mucosa weeks tomonths before the skin blisters appear. These oral lesionsrupture and create painful erosions. Over several weeks,non-pruritic skin blisters erupt over the rest of the body,ranging in size from one to several centimeters indiameter. (See Figure 4.) These blisters may be localized,usually affecting the head and trunk first. If left un-treated, they generalize over months.58 With pressure, thethin roof of the bullae may rupture or the fluid maydissect laterally into the mid-epidermal areas (a positiveNikolsky’s sign).
Ruptured blisters develop into painful erosions thatmay become secondarily infected. Prior to the availabilityof corticosteroids, mortality ranged from 50% to 90%;currently, the mortality is approximately 10%-20%. Mostof the complications are due to infections.59 Some patientscan develop extensive fluid, protein, and electrolyte lossin association with extensive blistering.
Continued from page 12
Reproduced with permission from: Habif T, ed. Clinical Dermatology:A Color Guide to Diagnosis and Therapy. 3rd ed. St. Louis: Mosby; 1996.
Figure 4. Pemphigus vulgaris.
17 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
DiagnosisThe diagnosis of PV is made by biopsy of the skinadjacent to the blister. Light microscopy will showintraepidermal blister, acantholysis of the epidermal cell,and a slight eosinophilic infiltrate. Direct immunofluores-cence demonstrates IgG on the surface of keratinocytes.Circulating autoantibodies can be found in 80%-90% ofPV patients.60
For the emergency physician, the skin biopsy andimmunofluorescence may not be practical. Therefore, theemergency physician must act based on the clinicalscenario—for example, an elderly patient who complainsof oral blisters for a few months and now has generalizedvesicles on the body. In the case of SJS or TEN, bullouslesions progress faster, the patient will look more toxic,and he or she may have recently taken a suspect drug.
TreatmentA low daily dose of prednisone (1 mg/kg/d) is the initialtreatment for cutaneous PV.54 Steroids are given untilremission (defined as a state of no new blisters for oneweek). If new lesions appear after 1-2 weeks of treatment,the dose of prednisone is increased.61
In general, begin the first dose of prednisone (1 mg/kg PO or IV) in the ED after consultation with a derma-tologist. (Alternatively, the dermatologist can beginsteroids as indicated if close follow-up is ensured.) Mostcases of PV can be treated at home as long as the patientis not toxic-appearing and has only a few blisters.54 Adermatologist should see the patient within days. Theconsultant can then perform an outpatient biopsy andadjust corticosteroids as indicated.
Patients with extensive blisters, erosions of the skin,or who are toxic-looking should be admitted. Once in thehospital, they can be monitored and treated for fluid orelectrolyte imbalances and observed for potentialinfection. If there are overt signs of infection in the ED,start antibiotics immediately.
Petechial/Purpuric Rashes
Certain petechial eruptions are among the most rapidlyfatal of the rashes. Prompt and accurate diagnosis andproper treatment may be life-saving, especially inpatients with meningococcal disease or Rocky Mountainspotted fever.
EtiologyThere are many causes of petechial rashes. It may beeasier to separate petechial rashes into bacterial, viral,and non-infectious causes. (See Table 11.) Whilepetechial rashes caused by bacteria are usually themost lethal, they are potentially treatable. Viral causesinclude Epstein-Barr virus, rubella, hepatitis B,and enteroviruses. Enteroviruses (e.g., echo 9 andcoxsackie 9) more commonly occur in summer and fallseasons. Affected patients may have disseminatedpetechial rash and aseptic meningitis, mimickingmeningococcal disease.9
General ApproachFirst, consider isolating the patient with a rapidlyprogressive petechial rash who looks ill and has a fever.In such cases, the examiner should wear a fitted respira-tory mask until meningococcemia can be ruled out. As arule, whenever confronted with a petechial rash, considerthe worst-case scenario—that is, meningococcemia andRocky Mountain spotted fever—as both of these diseasescan be rapidly progressive and fatal if not treatedaggressively. (See the Clinical Pathway on page 15,“Evaluating The Petechial Rash.”) It is prudent torapidly (and empirically) treat the ill-appearingpatient for these conditions, especially if the work-upwill take several hours.
HistoryIn a patient with petechiae, it is important to elicit anysick contacts (especially those with meningococcemia).Patients with viral infections may have upper respiratoryillnesses, body aches, and fever. It is also important toelicit a travel history. Dengue fever should be suspectedfor those who have traveled to Central or South America(although recent outbreaks have erupted in Puerto Rico,Hawaii, and the South Pacific). The petechial/purpuricrash will appear in about 30%-50% of patients and willmaterialize a few days after initial symptoms of malaise,cough, and fever.62 Rocky Mountain spotted fever isassociated with tick bites and is most often acquired in
Table 11. Causes Of Petechial/Purpuric Rashes.
Bacterial• Meningococcal disease• Rocky Mountain spotted fever• Gonococcemia• Pneumococcal sepsis• Haemophilus influenzae sepsis• Rat bite fevers (Spirillum minor and Streptobacillus
moniliformis)• Epidemic typhus
Viral• Dengue• Hemorrhagic fevers (Ebola, Lassa, etc.)• Enteroviral infections• Epstein-Barr virus• Rubella• Hepatitis B
Noninfectious• Coughing, sneezing, strangulation, Valsalva (mostly
petechiae in face or above nipple line)• Thrombocytopenia• Idiopathic thrombocytopenic purpura• Thrombotic thrombocytopenic purpura• Vasculitis (Henoch-Schönlein purpura, hypersensitivity)• Systemic lupus erythematosus
Adapted from: Schlossberg D. Fever and rash. Infect Dis Clin North Am1996;10:101-110.

Emergency Medicine Practice 18 www.empractice.net • September 2002
rural parts of the central and eastern United States.Ask the patient regarding a history of thrombocy-
topenia, systemic lupus erythematosus, scurvy, or HIVdisease. HIV patients are prone to idiopathic thrombocy-topenia purpura (ITP) and thrombotic thrombocytopenicpurpura (TTP).
On physical examination, determine whether thepurpura are palpable. Palpable purpura is seen invasculitis due to Henoch-Schönlein purpura, essentialmixed cryoglobulinemia, hypersensitivity vasculitis,and secondary vasculitis from connective tissue disease.63
Note the location of the petechiae. Coughing, sneezing,and other Valsalva maneuvers will produce petechiaelimited to above the nipple line—a finding especiallylikely in children. In one study, no febrile child withpetechiae limited to above the nipple line hadinvasive disease.64
General Diagnostic TestsIn toxic-appearing patients, draw a CBC with platelets,blood cultures, chemistries, and PT/PTT. These tests mayhelp to determine if the patient has multi-organ failureand/or disseminated intravascular coagulopathy.Consider thrombotic thrombocytopenic purpura in apatient with petechiae, mental status change, renalinsufficiency, hemolysis, and thrombocytopenia.
Order a urine assay to look for casts, red bloodcells, and protein (as glomerulonephritis is seen withHenoch-Schönlein purpura).65 A lumbar punctureshould be performed on those who have fever,headache, or meningeal signs. Additional tests thatmay aid in the diagnosis include hepatitis B andhepatitis C antibodies, an HIV test, an antinuclearantibody test, and a skin biopsy. If you are not surewhether meningococcemia or Rocky Mountain spottedfever is the cause of the rash in a toxic-appearingpatient, then a biopsy of the petechial/purpuric lesionfor Gram’s staining may be helpful. (A simpler solution isto give antibiotics that will cover both diagnoses—thatis, ceftriaxone plus doxycycline—and let the consultantworry about further diagnostic testing.)
General TreatmentsAdminister antibiotics as soon as possible for suspectedmeningococcemia or Rocky Mountain spotted fever: IVceftriaxone (Rocephin) 2 g for meningococcemia anddoxycycline 100 mg IV for suspected Rocky Mountainspotted fever. Give these antibiotics before the results oftests return if the patient is ill-appearing or the rash isprogressing rapidly. Be aggressive with IV fluids in toxicand hypotensive patients; pressors may be necessary.
MeningococcemiaAcute meningococcemia and meningococcal meningitisare caused by Neisseria meningitidis, an encapsulatedgram-negative diplococcus.66 Most cases of meningococ-cemia begin with colonization of the nasopharynx andthen progress to systemic invasion, ultimately leading to
bacteremia, then sepsis and/or CNS invasion. Untreated,meningococcemia is invariably fatal. Even with prompttreatment, the mortality rate is about 10%-20%.67
There are about 3000 cases of meningococcal diseaseper year in the United States; about 50% of these involvemeningitis.68 Most cases occur sporadically, but outbreaksarise in crowded environs such as dormitories or militarysettings.69 Most cases develop during the winter andspring months. Children from 6 months to 1 year of ageare at highest risk, followed by adults under 20 years.Persons with complement deficiencies, protein C&Sdeficiency, or who are asplenic are at higher risk than therest of the population.67
Clinical PresentationThe incubation period varies from two to 10 days, but thedisease usually begins 3-4 days after exposure. Symp-toms usually begin with an upper respiratory infection.The patient can have fever, chills, malaise, myalgias,headaches, nausea, and vomiting. A rash is seen in morethan 70% of people with meningococcemia.70 Petechiae,which develop on the wrist and ankles, are the first signof impending septicemia. At this stage, the rash may bemistaken for Rocky Mountain spotted fever. The pete-chiae then spread to the rest of the body, becomingconfluent and eventually developing into purpuricmacules. This process can be very rapid—with as little as12 hours between onset of fever until death.67
In certain people, the rash of meningococcemia canalso be described as faint pink macules or erythematouspapules in addition to the classic petechiae and purpuriclesions.71 Some petechiae may appear “smudged,” andthe purpura can appear “gun metal gray” in the center.Look for signs of meningeal irritation—neck soreness orstiffness, photophobia, and headaches.
The clinical manifestations of meningococcemia arethose of septic shock, with acute renal failure, hypoxia,hypotension, multi-organ failure, and disseminatedintravascular coagulopathy. This fulminating septicemiais termed Waterhouse-Friderichsen syndrome, accompa-nied by hemorrhagic destruction of the adrenal glands.
Early diagnosis and treatment are crucial. Thediagnosis of meningococcemia must rest on clinicalfindings and is confirmed by positive cultures of the skinor blood. In meningococcal sepsis, a Gram’s stain of askin biopsy specimen is significantly more sensitive(72%) than Gram’s-stained cerebrospinal fluid (22%).Also, a Gram’s-stained punch biopsy can be positive upto 45 hours after antibiotics, compared to 13 hours forblood cultures.19 Patients should only have a punchbiopsy when blood cultures results are negative forsuspected N. meningitidis and a definitive diagnosis needsto be made. This decision is usually in the hands of theconsultant and not the emergency physician.
TreatmentIn cases where the organism has not yet been identified,ceftriaxone (2 g q12h) is the initial antibiotic of choice to

19 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
cover the most common bacterial causes of purpuricdisease: N. meningitidis, H. influenzae, and S. pneumoniae.Once a definitive diagnosis of N. meningitidis is made inthe hospitalized patient, ceftriaxone can be continued orthe patient can be switched to IV penicillin G (4 millionunits q4h). An alternative regimen is ampicillin (2 g q6h);for those who are penicillin-allergic, ceftriaxone (2 gq12h) or cefotaxime can be used. In cases of severepenicillin allergy, IV chloramphenicol 4 g/d is indi-cated.72 Supportive care involving IV fluids is crucial inthe patient with overt or incipient shock. Patients withsuspected meningococcemia should be admitted to anisolation room.
Close contacts, such as daycare center personnel,household members, or ED personnel who have been incontact with the patient’s oral secretions should receiveantibiotic prophylaxis. Others who should receiveprophylaxis include those with prolonged contact (for atleast 4 hours in the week before onset of illness). In thecase of healthcare workers, prophylaxis is indicated forthose involved with intubation, nasotracheal suctioning,or resuscitation efforts. (A housekeeper who inadvert-ently walks into an isolation room to change the garbagebag does not need prophylaxis.) The recommendation forprophylaxis is a single dose of ciprofloxacin 500 mg PO.An alternative is rifampin 600 mg q12h PO for two daysor ceftriaxone 250 mg IM.73
Rocky Mountain Spotted FeverRocky Mountain spotted fever (RMSF) is an acuteinfectious disease caused by Rickettsia rickettsii, anobligate intracellular coccobacillus. This organism istransmitted by the bites of several species of ticks, mostlyDermacentor variabilis (American dog tick) in the easternUnited States and Dermacentor andersoni (Rocky Mountainwood tick) in the western United States. The term “RockyMountain” spotted fever is misleading because themajority of the cases occur in the eastern part of theUnited States (although the first cases were described inIdaho and Montana).66,74
There are about 1000 cases of RMSF a year, most ofwhich occur between April and September, when theticks are most active. However, cases have been reportedyear-round. The mortality rate for the untreated exceeds30%.71,75 Risk factors for mortality include delay intreatment and advanced age.76
It is thought that the tick must be attached for aprolonged period (hours) in order for the rickettsii to bereleased into the bloodstream; however, a tick bite isrecalled in only 50% of patients.77 After the tick bite, theR. rickettsii organism disseminates into the bloodstreamand invades the endothelium of blood vessels. Theresulting vasculitis produces the characteristic rash ofpetechiae, hemorrhage, and edema.
Clinical PresentationThe rash typically appears on the fourth day after the bite(range, 1-15 days), erupting first on the wrist and ankles.
Subsequently, the rash spreads centrally to the trunk andproximal extremities.78 The rash begins as reddishmacules that blanch with pressure, eventually becomingpetechial and purpuric. (See Figure 5.) In approximately10%-15% of the cases, a rash does not appear (producing“spotless” fever).75 In darker-skinned people, the rashmay be difficult to see, which may contribute to thehigher mortality rate in blacks (16%) as compared towhites (3%).71,79 Most patients with RMSF complain offever, headaches, myalgias, and malaise.74 Pain in thecalves and abdomen is common. In severe cases ofRMSF, multiple organs can be involved. CNS involve-ment may range from headaches (very common) tocoma and even seizures. Disseminated intravascularcoagulopathy is a predictor for mortality. Third spacingof fluids and concomitant edema, hypoalbuminemia,and hypovolemia may occur secondary to increasedcapillary permeability. In severe cases, the syndromeof inappropriate secretion of antidiuretic hormone canproduce hyponatremia.80
The diagnosis of RMSF is empiric and is initially based onclinical and epidemiologic findings. Serologic testing will benegative in the acute period.81 As a general rule, a patientwith a history of possible tick exposure in an endemicarea during the months of April to September whopresents with fever, headaches, and a rash should betreated for RMSF. Unfortunately, this triad of fever, rash,and a history of tick bite is found in only 60%-70% ofpatients on initial examination.75 Serologic testing isconfirmatory about two weeks after the tick bite butgenerally unnecessary.82 The Weil-Felix agglutinationtest is no longer used because of its low sensitivityand specificity.78,83
TreatmentThe recommended treatment for RMSF in adults isdoxycycline 100 mg BID PO or IV for seven days orfor two days after temperature has normalized.
Reproduced with permission from: Habif T, ed. Clinical Dermatology:A Color Guide to Diagnosis and Therapy. 3rd ed. St. Louis: Mosby; 1996.
Figure 5. Rocky Mountain spotted fever.

Emergency Medicine Practice 20 www.empractice.net • September 2002
While chloramphenicol is also active against therickettsia, doxycycline is associated with fewerfatalities.84 In the past, doxycycline was not often used inchildren under 8 years because of the presumed risk ofdental staining that occurs with tetracycline, a relateddrug. For this reason, some physicians prescribe chloram-phenicol for young children in whom RMSF is suspected.However, a number of authorities strongly recommenddoxycycline even in children under 8, arguing for itsdocumented effectiveness, broad margin of safety,minimal risk of dental staining, and convenient dosingschedule.85 Evidence suggests that the short courses ofdoxycycline used to treat RMSF do not cause clinicallysignificant staining of teeth.86 The recommended treat-ment for pregnant women is chloramphenicol 500 mgQID PO or IV for seven days or for two days after thetemperature has normalized.87,88
Patients who receive antirickettsial therapy withinfive days of symptom onset are significantly less likely
to die than those who receive treatment after the fifthday (6.5% vs 22.9%; P < 0.03).81 The need for hospitaliza-tion depends on the severity of the illness. Long-termsequelae from severe illness due to RMSF includehearing loss, peripheral neuropathy, bladder andbowel incontinence, and cerebellar, vestibular, andmotor dysfunction.89 Lifelong immunity appears todevelop after infection.80
Henoch-Schönlein Purpura“Numerous smaller, and larger, dark red, or bluish, round
patches are especially noticed on the legs and feet, while theupper portions of the body are free, or present but a few specks.They are not changed by pressure....The purpura in these cases
was always combined with colic, tenderness of the colon,vomiting, intestinal hemorrhage, and, with one exception, with
rheumatic pains, with swelling of the joints being less con-stant.”—Eduard Heinrich Henoch, Lectures on Diseases ofChildren: A Handbook for Physicians and Students, 1882
Ten Pitfalls To Avoid1. “I didn’t think Mr. Smith had Rocky Mountain spotted
fever—he had no rash!”
Well, he had “Rocky Mountain spotless fever.”
Approximately 10%-15% of people diagnosed with
RMSF have no rash. It can be fatal to presume otherwise.
The index of suspicion should be high in individuals
with fever, headache, myalgias, and possible tick exposure
from April to September. Treat liberally and empirically
with doxycycline.
2. “That elderly fellow kept returning to the ED with mouth
sores and complained it was painful to eat. I referred him to
his dentist.”
Well, you neglected to check out the rest of his body for
lesions or ask about personal or family history of bullous
diseases. This patient had pemphigus vulgaris. Early
treatment can significantly improve outcome.
3. “I thought that alcoholic, drug-abusing homeless person
was seeking narcotics. He kept on saying he had severe
pain in his leg, but I didn’t see any physical signs that
anything was wrong. He was probably drunk.”
Pain out of proportion to physical examination in a “toxic”
person should raise suspicion for early necrotizing fasciitis.
This patient was toxic with altered mental status—not
drunk. History of alcohol abuse, diabetes, peripheral
vascular disease, and a debilitated state are all risk factors
for necrotizing fasciitis.
4. “I thought the patient might have had cellulitis of his face
and chest. He had fever and lymphadenopathy, so I started
him on IV penicillin G. He got worse, developing
hepatitis and nephritis. Then his skin began to exfoliate
for no reason.”
There was a reason. You neglected to elicit that he had self-
medicated with his girlfriend’s “antibiotic pill” for a sore
throat. This pill turned out to be penicillin VK. Facial swelling
and erythema without pain in a person with
lymphadenopathy and a diffuse body erythema should
raise suspicion for a hypersensitivity syndrome.
5. “I didn’t think about antibiotic prophylaxis for his
dorm mates.”
You did a splendid job in quickly diagnosing and treating
the index case of meningococcemia, but you neglected to
prophylax his roommates with ciprofloxacin or rifampin.
Now two other students have contracted meningitis.
6. “I diagnosed the patient with Stevens-Johnson syndrome
because he came in with denuded skin and lesions of the
mouth, eyes, and rectum. I put silver sulfadiazene on the
denuded areas, but he got worse.”
Drugs are usually the inciting agent in SJS and TEN. This
patient was started on sulfonamides the week he
developed symptoms. You should have stopped the drug
(and not given silver sulfadiazene) as soon as the diagnosis
of SJS was considered.
7. “I thought the patient might have TEN because she had a
really bad rash that was sloughing off and fever. It was 3:00
a.m. and I didn’t want to wake up the dermatologist, so I
Continued on page 21

21 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
Henoch-Schönlein purpura is a vasculitis that primarilyaffects children. It is a constellation of cutaneous pur-pura, arthritis, abdominal pain, gastrointestinal bleeding,and nephritis. Immunoglobulin A (IgA) plays an impor-tant role in the development of this syndrome.90 Patientspresent with palpable purpura on the legs and buttocksand often complain of joint pain. Abdominal pain is alsocommon, and some children go on to develop intussus-ception. Nephritis occurs in 40% of patients, usuallyassociated with gross or microscopic hematuria andfrequently proteinuria.
Henoch-Schönlein purpura is an acute, self-limiteddisease of approximately one month’s duration. Corticos-teroids are effective in treating the arthritis and abdomi-nal pain.91,92 Consult a specialist if nephritis is suspected.
Diffuse Erythematous Rashes
The differential diagnosis for diffuse erythematous rashes
is broad. Some of these diagnoses are not immediatelylife-threatening, such as a viral exanthema, staphylococ-cal scalded skin syndrome, and Kawasaki disease. Othersare rapidly lethal, such as the toxic shock syndromes(TSS) and necrotizing fasciitis.
Staphylococcal Toxic Shock SyndromeAnd Streptococcal Toxic Shock SyndromeFor the purposes of this article, staphylococcal toxicshock syndrome (TSS) and streptococcal toxic shocksyndrome (STSS) will be discussed together, sincethey are similar in etiology, clinical presentation,and treatment.
EtiologyTSS and STSS are exotoxin-mediated diseases withdramatic clinical presentations. First described by Todd etal in 1978, TSS is characterized by fever, rash, mucousmembrane involvement, and hypotension. Initially, toxic
just started the steroids in the ED. I admitted the patient
to the floor and figured the dermatologist could see her
in the morning.”
This emergency physician made two big mistakes: 1) He
should have called the on-call dermatologist. 2) The patient
should have been admitted to the ICU. Retrospective
studies have shown that steroids may increase the rate
of morbidity and mortality of patients with TEN. Steroids
are generally not given for TEN and should only be given
in consultation with a dermatologist. Patients with TEN
should be treated like burn patients and admitted either
to a burn unit or an ICU setting. The mortality rate from
TEN is 25%-30%.
8. “The patient came in complaining of severe leg pain and
malaise. He was febrile and hypotensive but responded to
fluids and acetaminophen. I diagnosed him with cellulitis,
started him on cefazolin, and admitted him to the floor. I
had no idea he would deteriorate so quickly and require
transfer to the ICU.”
This patient had streptococcal toxic shock syndrome.
STSS often presents with pain out of proportion to
physical exam findings. About 80% of patients with
STSS have an associated soft-tissue infection, and
60% develop bacteremia. The emergency physician
must have a high index of suspicion for STSS when
patients present with a soft-tissue infection or injury,
high fever, and hypotension. IV penicillin combined
with clindamycin is the initial treatment of choice.
Get a surgical consult if there is suspicion of a
necrotizing infection.
Ten Pitfalls To Avoid (continued)
9. “She was 68 years old and had a high fever and a red
rash on her trunk. She said she had decreased energy
and myalgias for the past few days with low-grade
fever. She had a past medical history of hypertension.
I thought she had a viral syndrome and sent her home
with follow-up with her primary care physician the
next day.”
This patient’s rash worsened, and when she went to her
primary care physician the next day, the patient was found
to have a high fever, hypotension, and upon admission to
the hospital she had increased BUN/Cr, CPK, and bilirubin.
The patient had a nosebleed approximately one week prior
to presentation that required nasal packing. The emergency
physician failed to obtain this history. She was admitted to
the hospital with the diagnosis of staphylococcal toxic
shock syndrome.
10. “I suspected meningococcemia from the start. It takes
time to get blood and urine cultures. I also needed to get a
CT before I did the lumbar puncture. Plus, the nurses
couldn’t find a vein to stick.”
This child arrested before antibiotics were ever given. When
you suspect meningococcemia, set a timer. If the cultures,
bloodwork, lumbar puncture, etc., are not done by 30
minutes, give the antibiotics anyway (the lesions can be
biopsied and successfully Gram’s-stained the next day—
and the cerebrospinal fluid will not be sterilized for hours).
Can’t get a peripheral IV or a central line? If you can’t get
access within a reasonable time, consider IM or
intraosseous antibiotics for the first dose and give the IV
dose as soon as a line is established. ▲
Emergency Medicine Practice 22 www.empractice.net • September 2002
shock syndrome was thought to be associated only withstaphylococcal infection, but it has since been found to beassociated with streptococcal infection as well.93
PathophysiologyTSS is caused by colonization of toxin-producing strainsof S. aureus. The systemic manifestations of the illnessarise from a staphylococcal toxin and other mediators.
Unlike TSS, STSS is caused by a local tissueinvasion of the infecting organism S. pyogenes (groupA Streptococcus). Unlike TSS, a bacteremia ensues.94
EpidemiologyWhen TSS was first discovered, 85%-90% of the caseswere in young, healthy women who used hyper-absor-bent tampons, which resulted in vaginal colonization oftoxin-producing strains of S. aureus.95 Increased patientand physician awareness, along with removal of thesetampons from the market, has decreased the incidence ofTSS in menstruating women. Currently, TSS occurs in allage groups but still occurs more commonly in women.96
Up to 45% of cases of TSS are non-menstrual.97 Non-menstrual cases of TSS occur with abscesses, bursitis,surgical wounds, indwelling foreign bodies such as nasalpacking, and in post-partum patients.98-101
In STSS, most patients are 20-50 years old,78 and 80%of patients have an associated soft-tissue infection orminor skin trauma.94 In contrast to TSS, where bloodcultures are usually sterile, more than 60% of patientswith STSS develop bacteremia.102
Morbidity And MortalityEven though most individuals who are susceptible to
STSS tend to be young and healthy, the morbidity andmortality are higher in STSS than TSS.103 Patients developprofound shock, renal failure, sepsis, and adult respira-tory distress syndrome. The overall mortality is 30%, andmortality rates can reach 80% in the elderly.104-106 Between1990 and 1994, 29 cases of STSS were reported in childrenup to 14 years of age, and five of these children died.107
The mortality rate for TSS is 2%-5%.108
Clinical PresentationPatients report a prodrome of low-grade fever, malaise,myalgias, and vomiting.109 Symptoms may occur within2-3 days of tampon use, soft-tissue infection, or within aweek of other inciting factors.110
The onset of the major symptoms of TSS and STSS(high fever, rash, and hypotension) begins abruptly afterthe prodrome. Hypotension develops rapidly, leading totissue ischemia and subsequent multisystem involve-ment. An endotoxin-induced vasculitis contributes to thesystemic failure.
Rash is a characteristic feature of TSS and usuallydevelops 1-3 days after other major symptoms. The rashis a diffuse, non-pruritic, blanching, and macular erythro-derma. It generally erupts on the trunk, where it remainsmost prominent, although scattered erythematouspapules may coexist. If the patient is thrombocytopenic,purpura may develop. The initial rash may be subtle oreven overlooked (especially in dark-skinned individuals)and generally resolves in 3-5 days. Half of patientsdevelop a pruritic, diffuse, maculopapular eruption,usually on the hands and feet.78 If the patient survives theinitial episode of TSS, full-thickness desquamation of thepalms and soles occurs 5-12 days after the onset of
Cost-Effective Strategies For Patients With Rashes1. Discharge appropriately.
Patients with erythema multiforme minor and major, and
even some with Stevens-Johnson syndrome, can be
discharged home with timely follow-up.
Caveat: Patients who are discharged should return
immediately for any worsening of their rash or if they
start to feel worse. Individuals with significant epithelial
loss, the very young or very old, and those with
comorbidities or no follow-up require admission to the
hospital. Those with TEN require intensive care and
possibly transfer to a burn unit.
2. Limit laboratory studies.
The diagnosis of most rashes is clinical. If the patient is not ill-
appearing, most patients with rash will not require
bloodwork. Confused about a rash? Get out a book or talk to
a consultant instead of ordering gazillions of tests that will
only further muddy the waters.
Caveat: Certain patients will require laboratory evaluation,
including those who are ill-appearing (and especially if
they have petechiae). In such patients, a CBC, with special
attention to the platelet count, is useful. Order a VDRL for
those with a papulosquamous rash, particularly if it
involves the palms or soles.
3. Do a good physical examination.
Nothing will provide as much “bang for the buck” as a superb
physical examination. While the best way to examine a rash is
to take a naked patient out into the afternoon sun, this is not
always practical. At least make sure every patient is in a gown
and touch the rash. Does the patient have palpable purpura
or a positive Nikolsky’s sign? If there are “spots,” do they
blanch? Always look in the mouth and at the eyes, as well as
the palms and soles; if erythema mulitforme or Stevens-
Johnson syndrome is possible, look at the genitalia and
rectum as well. ▲
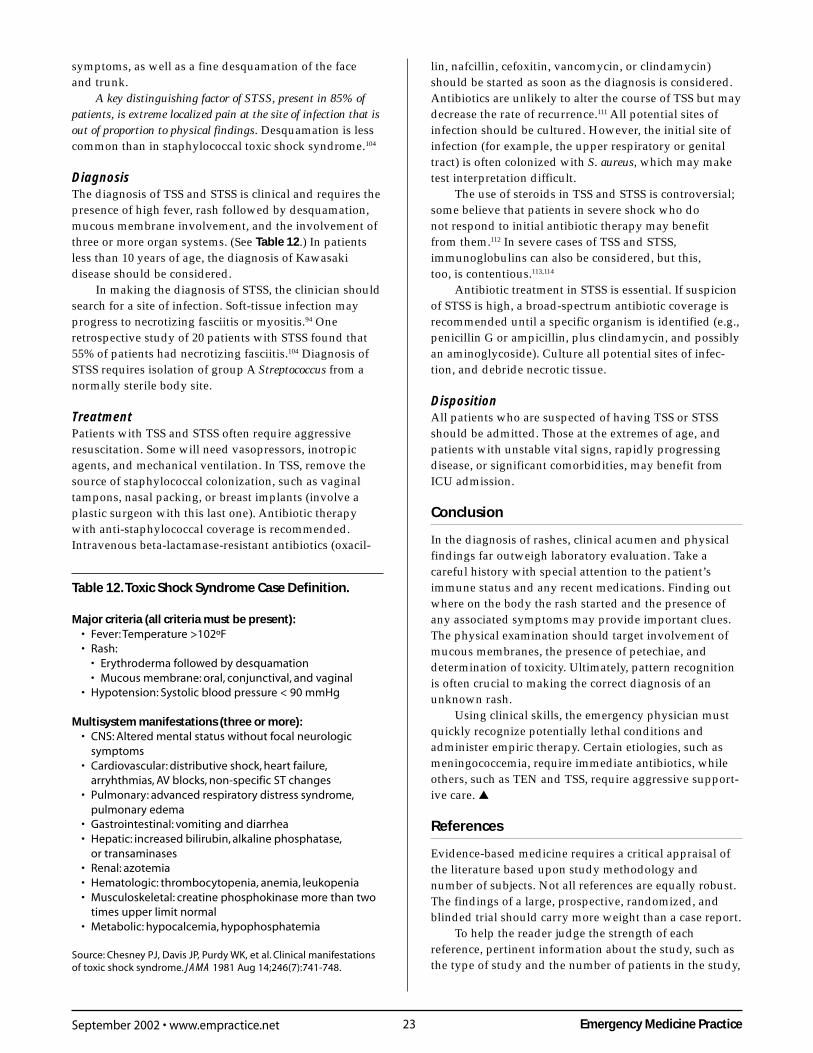
23 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
symptoms, as well as a fine desquamation of the faceand trunk.
A key distinguishing factor of STSS, present in 85% ofpatients, is extreme localized pain at the site of infection that isout of proportion to physical findings. Desquamation is lesscommon than in staphylococcal toxic shock syndrome.104
DiagnosisThe diagnosis of TSS and STSS is clinical and requires thepresence of high fever, rash followed by desquamation,mucous membrane involvement, and the involvement ofthree or more organ systems. (See Table 12.) In patientsless than 10 years of age, the diagnosis of Kawasakidisease should be considered.
In making the diagnosis of STSS, the clinician shouldsearch for a site of infection. Soft-tissue infection mayprogress to necrotizing fasciitis or myositis.94 Oneretrospective study of 20 patients with STSS found that55% of patients had necrotizing fasciitis.104 Diagnosis ofSTSS requires isolation of group A Streptococcus from anormally sterile body site.
TreatmentPatients with TSS and STSS often require aggressiveresuscitation. Some will need vasopressors, inotropicagents, and mechanical ventilation. In TSS, remove thesource of staphylococcal colonization, such as vaginaltampons, nasal packing, or breast implants (involve aplastic surgeon with this last one). Antibiotic therapywith anti-staphylococcal coverage is recommended.Intravenous beta-lactamase-resistant antibiotics (oxacil-
lin, nafcillin, cefoxitin, vancomycin, or clindamycin)should be started as soon as the diagnosis is considered.Antibiotics are unlikely to alter the course of TSS but maydecrease the rate of recurrence.111 All potential sites ofinfection should be cultured. However, the initial site ofinfection (for example, the upper respiratory or genitaltract) is often colonized with S. aureus, which may maketest interpretation difficult.
The use of steroids in TSS and STSS is controversial;some believe that patients in severe shock who donot respond to initial antibiotic therapy may benefitfrom them.112 In severe cases of TSS and STSS,immunoglobulins can also be considered, but this,too, is contentious.113,114
Antibiotic treatment in STSS is essential. If suspicionof STSS is high, a broad-spectrum antibiotic coverage isrecommended until a specific organism is identified (e.g.,penicillin G or ampicillin, plus clindamycin, and possiblyan aminoglycoside). Culture all potential sites of infec-tion, and debride necrotic tissue.
DispositionAll patients who are suspected of having TSS or STSSshould be admitted. Those at the extremes of age, andpatients with unstable vital signs, rapidly progressingdisease, or significant comorbidities, may benefit fromICU admission.
Conclusion
In the diagnosis of rashes, clinical acumen and physicalfindings far outweigh laboratory evaluation. Take acareful history with special attention to the patient’simmune status and any recent medications. Finding outwhere on the body the rash started and the presence ofany associated symptoms may provide important clues.The physical examination should target involvement ofmucous membranes, the presence of petechiae, anddetermination of toxicity. Ultimately, pattern recognitionis often crucial to making the correct diagnosis of anunknown rash.
Using clinical skills, the emergency physician mustquickly recognize potentially lethal conditions andadminister empiric therapy. Certain etiologies, such asmeningococcemia, require immediate antibiotics, whileothers, such as TEN and TSS, require aggressive support-ive care. ▲
References
Evidence-based medicine requires a critical appraisal ofthe literature based upon study methodology andnumber of subjects. Not all references are equally robust.The findings of a large, prospective, randomized, andblinded trial should carry more weight than a case report.
To help the reader judge the strength of eachreference, pertinent information about the study, such asthe type of study and the number of patients in the study,
Table 12. Toxic Shock Syndrome Case Definition.
Major criteria (all criteria must be present):• Fever: Temperature >102ºF• Rash:
• Erythroderma followed by desquamation• Mucous membrane: oral, conjunctival, and vaginal
• Hypotension: Systolic blood pressure < 90 mmHg
Multisystem manifestations (three or more):• CNS: Altered mental status without focal neurologic
symptoms• Cardiovascular: distributive shock, heart failure,
arryhthmias, AV blocks, non-specific ST changes• Pulmonary: advanced respiratory distress syndrome,
pulmonary edema• Gastrointestinal: vomiting and diarrhea• Hepatic: increased bilirubin, alkaline phosphatase,
or transaminases• Renal: azotemia• Hematologic: thrombocytopenia, anemia, leukopenia• Musculoskeletal: creatine phosphokinase more than two
times upper limit normal• Metabolic: hypocalcemia, hypophosphatemia
Source: Chesney PJ, Davis JP, Purdy WK, et al. Clinical manifestationsof toxic shock syndrome. JAMA 1981 Aug 14;246(7):741-748.
Emergency Medicine Practice 24 www.empractice.net • September 2002
will be included in bold type following the reference,where available. In addition, the most informativereferences cited in the paper, as determined by theauthors, will be noted by an asterisk (*) next to thenumber of the reference.
1.* Drake LA, Dinehart SM, Farmer ER, et al. Guidelines ofcare for cutaneous adverse drug reactions. AmericanAcademy of Dermatology. J Am Acad Dermatol 1996Sep;35(3 Pt 1):458-461. (Practice guideline)
2.* Shivaram V, Christoph RA, Hayden GF. Skin disordersencountered in a pediatric emergency department.Pediatr Emerg Care 1993 Aug;9(4):202-204. (Retrospective;1381 visits)
3. Feldman SR, Fleischer AB Jr, McConnell RC. Mostcommon dermatologic problems identified by internists,1990-1994. Arch Intern Med 1998 Apr 13;158(7):726-730. (Retrospective)
4. Lynch P. Dermatology for the House Officer. Baltimore:Williams & Wilkins; 1987. (Textbook)
5.* Lynch PJ, Edminster SC. Dermatology for thenondermatologist: a problem-oriented system. Ann EmergMed 1984 Aug;13(8):603-606. (Descriptive review)
6. No authors listed. Immunization of Health-Care Workers:Recommendations of the Advisory Committee on Immuni-zation Practices (ACIP) and the Hospital Infection ControlPractices Advisory Committee (HICPAC). MMWR MorbMortal Wkly Rep 1997 Dec 26;46(RR-18):1-42. (Guideline)
7.* Spach DH, Liles WC, Campbell GL, et al. Tick-bornediseases in the United States. N Engl J Med 1993 Sep23;329(13):936-947. (Review)
8.* Roujeau JC, Stern RS. Severe adverse cutaneous reactionsto drugs. N Engl J Med 1994 Nov 10;331(19):1272-1285. (Review)
9.* Schlossberg D. Fever and rash. Infect Dis Clin North Am1996 Mar;10(1):101-110. (Review)
10. Millikan LE. Treating pruritus. What’s new in safe reliefof symptoms? Postgrad Med 1996 Jan;99(1):173-176,179-184. (Review)
11. Nadelman RB, Wormser GP. Lyme borreliosis. Lancet 1998Aug 15;352(9127):557-565. (Review)
12. Raviglione MC, Pablos-Mendez A, Battan R. Clinicalfeatures and management of severe dermatologicalreactions to drugs. Drug Saf 1990 Jan;5(1):39-64. (Review)
13. Vervloet D, Durham S. Adverse reactions to drugs. BMJ1998 May 16;316(7143):1511-1514. (Review)
14. Fitzpatrick TB, Johnson RA, Wolff K, et al, eds. Color Atlasand Synopsis of Clinical Dermatology: Common and SeriousDiseases. 4th ed. New York: McGraw-Hill, 2001. (Textbook)
15.* McKinnon HD Jr, Howard T. Evaluating the febrilepatient with a rash. Am Fam Physician 2000 Aug15;62(4):804-816. (Review)
16. Bunikis J, Barbour AG. Laboratory testing for suspectedLyme disease. Med Clin North Am 2002 Mar;86(2):311-340. (Review)
17. Nikkels AF, Debrus S, Sadzot-Delvaux C, et al.Immunohistochemical identification of varicella-zostervirus gene 63-encoded protein (IE63) and late (gE) proteinon smears and cutaneous biopsies: implications fordiagnostic use. J Med Virol 1995 Dec;47(4):342-347.(Comparative; 66 skin sections)
18. Achar S. Principles of skin biopsies for the family physi-cian. Am Fam Physician 1996 Dec;54(8):2411-2418. (Review)
19. van Deuren M, van Dijke BJ, Koopman RJ, et al. Rapid
diagnosis of acute meningococcal infections by needleaspiration or biopsy of skin lesions. BMJ 1993 May8;306(6887):1229-1232. (Retrospective; 51 patients)
20. Edlow JA. Lyme disease and related tick-borne illnesses.Ann Emerg Med 1999 Jun;33(6):680-693. (Review)
21.* Levin S, Goodman LJ. An approach to acute fever andrash (AFR) in the adult. Curr Clin Top Infect Dis 1995;15:19-75. (Review)
22.* Roujeau JC, Kelly JP, Naldi L, et al. Medication use andthe risk of Stevens-Johnson syndrome or toxic epidermalnecrolysis. N Engl J Med 1995 Dec 14;333(24):1600-1607.(Multicenter, case-control; 245 SJS/TEN patients,1147 controls)
23. Rieder MJ, Shear NH, Kanee A, et al. Prominence of slowacetylator phenotype among patients with sulfonamidehypersensitivity reactions. Clin Pharmacol Ther 1991Jan;49(1):13-17. (Case-control; 21 patients)
24. Garcia-Doval I, LeCleach L, Bocquet H, et al. Toxicepidermal necrolysis and Stevens-Johnson syndrome: doesearly withdrawal of causative drugs decrease the risk ofdeath? Arch Dermatol 2000 Mar;136(3):323-327. (Observa-tional; 203 patients)
25. Bigby M, Stern RS, Arndt KA. Allergic cutaneous reactionsto drugs. Prim Care 1989 Sep;16(3):713-727. (Review)
26. Roujeau JC. Treatment of severe drug eruptions. J Dermatol1999 Nov;26(11):718-722. (Review)
27. Klein PA, Clark RA. An evidence-based review of theefficacy of antihistamines in relieving pruritus in atopicdermatitis. Arch Dermatol 1999 Dec;135(12):1522-1525.(Review; 16 studies)
28.* Bastuji-Garin S, Rzany B, Stern RS, et al. Clinicalclassification of cases of toxic epidermal necrolysis,Stevens-Johnson syndrome, and erythema multiforme.Arch Dermatol 1993 Jan;129(1):92-96. (Prospective, case-control; 28 cases)
29.* Roujeau JC. The spectrum of Stevens-Johnson syndromeand toxic epidermal necrolysis: a clinical classification.J Invest Dermatol 1994 Jun;102(6):28S-30S. (Review,consensus classification)
30. Assier H, Bastuji-Garin S, Revuz J, et al. Erythemamultiforme with mucous membrane involvement andStevens-Johnson syndrome are clinically different disorderswith distinct causes. Arch Dermatol 1995 May;131(5):539-543. (Retrospective; 76 patients)
31. Paquet P, Pierard GE. Erythema multiforme and toxicepidermal necrolysis: a comparative study. Am JDermatopathol 1997 Apr;19(2):127-132. (Comparative study,17 specimens)
32. Power WJ, Ghoraishi M, Merayo-Lloves J, et al. Analysisof the acute ophthalmic manifestations of the erythemamultiforme/Stevens-Johnson syndrome/toxic epidermalnecrolysis disease spectrum. Ophthalmology 1995Nov;102(11):1669-1676. (Multicenter, retrospective;366 patients)
33. Kakourou T, Klontza D, Soteropoulou F, et al. Corticoster-oid treatment of erythema multiforme major (Stevens-Johnson syndrome) in children. Eur J Pediatr 1997Feb;156(2):90-93. (Prospective, randomized controlledtrial; 16 patients)
34. Renfro L, Grant-Kels JM, Feder HM Jr, et al. Controversy:are systemic steroids indicated in the treatment of erythemamultiforme? Pediatr Dermatol 1989 Mar;6(1):43-50. (Review,case report; 3 patients)
35. Ting HC, Adam BA. Erythema multiforme—response to
25 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
corticosteroid. Dermatologica 1984;169(4):175-178. (Retro-spective; 25 patients)
36. Rasmussen JE. Erythema multiforme in children. Responseto treatment with systemic corticosteroids. Br J Dermatol1976 Aug;95(2):181-186. (Retrospective; 32 patients)
37. Guillaume JC, Roujeau JC, Revuz J, et al. The culprit drugsin 87 cases of toxic epidermal necrolysis (Lyell’s syndrome).Arch Dermatol 1987 Sep;123(9):1166-1170. (Retrospective;87 patients)
38.* Wolkenstein P, Revuz J. Toxic epidermal necrolysis.Dermatol Clin 2000 Jul;18(3):485-495, ix. (Review)
39. Wolkenstein P, Carriere V, Charue D, et al. A slowacetylator genotype is a risk factor for sulphonamide-induced toxic epidermal necrolysis and Stevens-Johnson syndrome. Pharmacogenetics 1995 Aug;5(4):255-258. (Comparative)
40. Wolkenstein P, Tan C, Lecoeur S, et al. Covalent bindingof carbamazepine reactive metabolites to P450isoforms present in the skin. Chem Biol Interact 1998May 1;113(1):39-50.
41. Saiag P, Caumes E, Chosidow O, et al. Drug-inducedtoxic epidermal necrolysis (Lyell syndrome) in patientsinfected with the human immunodeficiency virus. J AmAcad Dermatol 1992 Apr;26(4):567-574. (Retrospective;80 patients)
42.* Revuz J, Penso D, Roujeau JC, et al. Toxic epidermalnecrolysis. Clinical findings and prognosis factors in 87patients. Arch Dermatol 1987 Sep;123(9):1160-1165. (Retro-spective; 87 patients)
43. Bastuji-Garin S, Zahedi M, Guillaume JC, et al. Toxicepidermal necrolysis (Lyell syndrome) in 77 elderlypatients. Age Ageing 1993 Nov;22(6):450-456. (Retrospec-tive; 77 patients)
44. Halebian PH, Corder VJ, Madden MR, et al. Improved burncenter survival of patients with toxic epidermal necrolysismanaged without corticosteroids. Ann Surg 1986Nov;204(5):503-512. (Comparative; 30 patients)
45. Roujeau JC, Chosidow O, Saiag P, et al. Toxic epidermalnecrolysis (Lyell syndrome). J Am Acad Dermatol 1990Dec;23(6 Pt 1):1039-1058. (Review)
46. Meneux E, Wolkenstein P, Haddad B, et al. Vulvovaginalinvolvement in toxic epidermal necrolysis: a retrospectivestudy of 40 cases. Obstet Gynecol 1998 Feb;91(2):283-287.(Retrospective; 40 patients)
47. Rohrer TE, Ahmed AR. Toxic epidermal necrolysis. Int JDermatol 1991 Jul;30(7):457-466. (Review)
48. Tripathi A, Ditto AM, Grammer LC, et al. Corticosteroidtherapy in an additional 13 cases of Stevens-Johnsonsyndrome: a total series of 67 cases. Allergy Asthma Proc2000 Mar;21(2):101-105. (Prospective; 67 patients)
49. Hewitt J, Ormerod AD. Toxic epidermal necrolysis treatedwith cyclosporin. Clin Exp Dermatol 1992 Jul;17(4):264-265.(Case report)
50. Renfro L, Grant-Kels JM, Daman LA. Drug-induced toxicepidermal necrolysis treated with cyclosporin. Int JDermatol 1989 Sep;28(7):441-444. (Case report)
51.* Fine JD. Management of acquired bullous skin diseases. NEngl J Med 1995 Nov 30;333(22):1475-1484. (Review)
52. McGee T, Munster A. Toxic epidermal necrolysis syndrome:mortality rate reduced with early referral to regional burncenter. Plast Reconstr Surg 1998 Sep;102(4):1018-1022.(Retrospective; 36 patients)
53. Heimbach DM, Engrav LH, Marvin JA, et al. Toxicepidermal necrolysis. A step forward in treatment. JAMA
1987 Apr 24;257(16):2171-2175. (Prospective; 19 patients)54. Camisa C, Warner M. Treatment of pemphigus. Dermatol
Nurs 1998 Apr;10(2):115-118, 123-131. (Review)55. Nousari HC, Anhalt GJ. Pemphigus and bullous pemphig-
oid. Lancet 1999 Aug 21;354(9179):667-672. (Review)56. Korman NJ. Pemphigus. Dermatol Clin 1990 Oct;8(4):689-
700. (Review)57. Korman N. Pemphigus. J Am Acad Dermatol 1988
Jun;18(6):1219-1238. (Review)58. Seidenbaum M, David M, Sandbank M. The course
and prognosis of pemphigus. A review of 115 patients.Int J Dermatol 1988 Oct;27(8):580-584. (Follow-up study;115 patients)
59. Rosenberg FR, Sanders S, Nelson CT. Pemphigus: a 20-yearreview of 107 patients treated with corticosteroids. ArchDermatol 1976 Jul;112(7):962-970. (Retrospective;107 patients)
60. Sams WM Jr, Gammon WR. Mechanism of lesion produc-tion in pemphigus and pemphigoid. J Am Acad Dermatol1982 Apr;6(4 Pt 1):431-452. (Review)
61. Lever WF, Schaumburg-Lever G. Treatment of pemphigusvulgaris. Results obtained in 84 patients between 1961 and1982. Arch Dermatol 1984 Jan;120(1):44-47. (Retrospective;84 patients)
62.* Wilson ME. Skin problems in the traveler. Infect Dis ClinNorth Am 1998 Jun;12(2):471-488. (Review)
63. Blanco R, Martinez-Taboada VM, Rodriguez-Valverde V, etal. Cutaneous vasculitis in children and adults. Associateddiseases and etiologic factors in 303 patients. Medicine(Baltimore) 1998 Nov;77(6):403-418. (Review, retrospective;303 patients)
64.* Baker RC, Seguin JH, Leslie N, et al. Fever and petechiae inchildren. Pediatrics 1989 Dec;84(6):1051-1055. (Prospective,observational; 190 children)
65. Gibson LE. Cutaneous vasculitis: approach to diagnosisand systemic associations. Mayo Clin Proc 1990Feb;65(2):221-229. (Review)
66. Levinson W, Jawetz E. Medical Microbiology andImmunobiology. 6th ed. New York: Lange Medical/McGrawHill; 2000. (Textbook)
67. Kirsch EA, Barton RP, Kitchen L, et al. Pathophysiology,treatment and outcome of meningococcemia: a review andrecent experience. Pediatr Infect Dis J 1996 Nov;15(11):967-978; quiz 979. (Review)
68. Rosenstein NE, Perkins BA, Stephens DS, et al. Thechanging epidemiology of meningococcal disease in theUnited States, 1992-1996. J Infect Dis 1999 Dec;180(6):1894-1901. (Population surveillance)
69. Stephens DS, Hajjeh RA, Baughman WS, et al. Sporadicmeningococcal disease in adults: results of a 5-yearpopulation-based study. Ann Intern Med 1995 Dec15;123(12):937-940. (Prospective; 132 patients)
70. Wong VK, Hitchcock W, Mason WH. Meningococcalinfections in children: a review of 100 cases. Pediatr InfectDis J 1989 Apr;8(4):224-227. (Review, retrospective;100 patients)
71. Habif TP, Habie TP. Clinical Dermatology: A Color Guideto Diagnosis and Therapy. 3rd ed. St. Louis: Mosby.1996. (Textbook)
72. Wispelwey B, Tunkel AR, Scheld WM. Bacterialmeningitis in adults. Infect Dis Clin North Am 1990Dec;4(4):645-659. (Review)
73. No authors listed. Immunization of Health-Care Workers:Recommendations of the Advisory Committee on Immuni-
Emergency Medicine Practice 26 www.empractice.net • September 2002
zation Practices (ACIP) and the Hospital Infection ControlPractices Advisory Committee (HICPAC). MMWR MorbMortal Wkly Rep 1997 Dec 26;46(RR-18):1-42. (Guideline)
74. Weber DJ, Walker DH. Rocky Mountain spotted fever. InfectDis Clin North Am 1991 Mar;5(1):19-35. (Review)
75. Spach DH, Liles WC, Campbell GL, et al. Tick-bornediseases in the United States. N Engl J Med 1993 Sep23;329(13):936-947. (Review)
76. Dalton MJ, Clarke MJ, Holman RC, et al. National surveil-lance for Rocky Mountain spotted fever, 1981-1992:epidemiologic summary and evaluation of risk factors forfatal outcome. Am J Trop Med Hyg 1995 May;52(5):405-413.(Population surveillance; 7650 patients)
77.* Kirk JL, Fine DP, Sexton DJ, et al. Rocky Mountain spottedfever. A clinical review based on 48 confirmed cases, 1943-1986. Medicine (Baltimore) 1990 Jan;69(1):35-45. (Review,retrospective; 48 patients)
78. Drage LA. Life-threatening rashes: dermatologic signs offour infectious diseases. Mayo Clin Proc 1999 Jan;74(1):68-72. (Review)
79. No authors listed. Current trends in Rocky Mountainspotted fever—United States, 1990. MMWR MorbMortal Wkly Rep 1991 July 12:40(27);451-453, 459.(Epidemiologic data)
80. Petri WA Jr. Tick-borne diseases. Am Fam Physician 1988Jun;37(6):95-104. (Review)
81. Kirkland KB, Wilkinson WE, Sexton DJ. Therapeuticdelay and mortality in cases of Rocky Mountain spottedfever. Clin Infect Dis 1995 May;20(5):1118-1121.(Retrospective cohort)
82. Kostman JR. Laboratory diagnosis of rickettsial diseases.Clin Dermatol 1996 May;14(3):301-306. (Review)
83. Kaplan JE, Schonberger LB. The sensitivity of variousserologic tests in the diagnosis of Rocky Mountain spottedfever. Am J Trop Med Hyg 1986 Jul;35(4):840-844. (Compara-tive; 4141 cases)
84. Holman RC, Paddock CD, Curns AT, et al. Analysis of riskfactors for fatal Rocky Mountain Spotted Fever: evidencefor superiority of tetracyclines for therapy. J Infect Dis 2001Dec 1;184(11):1437-1444. (Comparative; 6388 patients)
85. Cale DF, McCarthy MW. Treatment of Rocky Mountainspotted fever in children. Ann Pharmacother 1997Apr;31(4):492-494. (Review)
86. Lochary ME, Lockhart PB, Williams WT Jr. Doxycyclineand staining of permanent teeth. Pediatr Infect Dis J 1998May;17(5):429-431. (Retrospective)
87. Stallings SP. Rocky Mountain spotted fever and pregnancy:a case report and review of the literature. Obstet GynecolSurv 2001 Jan;56(1):37-42. (Review, case report)
88. Thorner AR, Walker DH, Petri WA Jr. Rocky mountainspotted fever. Clin Infect Dis 1998 Dec;27(6):1353-1359; quiz1360. (Review)
89. Archibald LK, Sexton DJ. Long-term sequelae of RockyMountain spotted fever. Clin Infect Dis 1995 May;20(5):1122-1125. (Follow-up study; 25 patients)
90. Saulsbury FT. Henoch-Schönlein purpura. Curr OpinRheumatol 2001 Jan;13(1):35-40. (Review)
91. Rosenblum ND, Winter HS. Steroid effects on the course ofabdominal pain in children with Henoch-Schonleinpurpura. Pediatrics 1987 Jun;79(6):1018-1021. (Comparative)
92.* Saulsbury FT. Henoch-Schönlein purpura in children.Report of 100 patients and review of the literature. Medicine(Baltimore) 1999 Nov;78(6):395-409. (Review, retrospective;100 patients)
93. Todd J, Fishaut M, Kapral F, et al. Toxic-shock syndromeassociated with phage-group-I Staphylococci. Lancet 1978Nov 25;2(8100):1116-1118. (Case report; 7 patients)
94.* Wolf JE, Rabinowitz LG. Streptococcal toxic shock-likesyndrome. Arch Dermatol 1995 Jan;131(1):73-77. (Review)
95. Broome CV. Epidemiology of toxic shock syndrome in theUnited States: overview. Rev Infect Dis 1989 Jan;11 Suppl1:S14-S21. (Review)
96. Manders SM. Toxin-mediated streptococcal and staphylo-coccal disease. J Am Acad Dermatol 1998 Sep;39(3):383-398;quiz 399-400. (Review)
97. Herzer CM. Toxic shock syndrome: broadening thedifferential diagnosis. J Am Board Fam Pract 2001Mar;14(2):131-136. (Review, case report)
98. Reingold AL, Hargrett NT, Dan BB, et al. Nonmenstrualtoxic shock syndrome: a review of 130 cases. Ann InternMed 1982 Jun;96(6 Pt 2):871-874. (Retrospective; 130 cases)
99. Andrews MM, Parent EM, Barry M, et al. Recurrentnonmenstrual toxic shock syndrome: clinical manifesta-tions, diagnosis, and treatment. Clin Infect Dis 2001 May15;32(10):1470-1479. (Review, case report; 3 patients)
100. Arnold J, Lucarelli M, Cutrona AF, et al. Toxic shocksyndrome originating from the foot. J Foot Ankle Surg 2001Nov;40(6):411-413. (Case report)
101. Davis D, Gash-Kim TL, Heffernan EJ. Toxic shocksyndrome: case report of a postpartum female and aliterature review. J Emerg Med 1998 Jul;16(4):607-614.(Review, case report)
102. Stevens DL. The toxic shock syndromes. Infect Dis ClinNorth Am 1996 Dec;10(4):727-746. (Review)
103. Chesney PJ. Clinical aspects and spectrum of illness of toxicshock syndrome: overview. Rev Infect Dis 1989 Jan;11 Suppl1:S1-S7. (Review)
104.*Stevens DL, Tanner MH, Winship J, et al. Severe group Astreptococcal infections associated with a toxic shock-likesyndrome and scarlet fever toxin A. N Engl J Med 1989 Jul6;321(1):1-7. (Retrospective; 20 patients)
105. Stevens DL. Invasive group A streptococcus infections. ClinInfect Dis 1992 Jan;14(1):2-11. (Review)
106. Davies HD, McGeer A, Schwartz B, et al. Invasive group Astreptococcal infections in Ontario, Canada. Ontario GroupA Streptococcal Study Group. N Engl J Med 1996 Aug22;335(8):547-554. (Population surveillance; 323 patients)
107. Conway E. Streptococcal toxic shock: A race against time.Contemp Pediat (Res Ed) 1995;2:5-10. (Review)
108. Gannon T. Dermatologic emergencies. When earlyrecognition can be lifesaving. Postgrad Med 1994Jul;96(1):67-70, 73-75, 79 passim. (Review)
109. Wright SW, Trott AT. Toxic shock syndrome: a review. AnnEmerg Med 1988 Mar;17(3):268-273. (Review)
110. Kain KC, Schulzer M, Chow AW. Clinical spectrum ofnonmenstrual toxic shock syndrome (TSS): comparisonwith menstrual TSS by multivariate discriminant analyses.Clin Infect Dis 1993 Jan;16(1):100-106. (Comparative;45 patients)
111. Norman GR, Rosenthal D, Brooks LR, et al. The develop-ment of expertise in dermatology. Arch Dermatol 1989Aug;125(8):1063-1068. (Comparative)
112. Todd JK, Ressman M, Caston SA, et al. Corticosteroidtherapy for patients with toxic shock syndrome. JAMA1984 Dec 28;252(24):3399-3402. (Comparative, retrospec-tive; 45 patients)
113. Todd JK. Therapy of toxic shock syndrome. Drugs 1990Jun;39(6):856-861. (Review)
27 Emergency Medicine PracticeSeptember 2002 • www.empractice.net
114. Barry W, Hudgins L, Donta ST, et al. Intravenous immuno-globulin therapy for toxic shock syndrome. JAMA 1992 Jun24;267(24):3315-3316. (Case report)
Physician CME Questions
33. When triaging patients with rashes, any ofthe following would qualify the patient ashigh-risk except:a. abnormal vital signs.b. altered mental status.c. a localized rash that does not progress.d. potential airway compromise.e. a petechial rash.
34. The most common cause of pruritus is:a. scabies.b. lymphomas.c. an acute allergic reaction.d. poison ivy.e. dry skin.
35. Recent travel can be associated with all of thefollowing life-threatening rashes except:a. toxic epidermal necrolysis.b. Rocky Mountain spotted fever.c. Lyme disease.d. hemorrhagic fevers.
36. Oral ulcers or blisters can imply a serious systemicreaction, such as Stevens-Johnson syndrome orpemphigus vulgaris.a. Trueb. False
37. A patient who presents with a rash and fever:a. should receive a full, head-to-toe examination.b. only requires a skin examination.c. should receive acetaminophen for presumed
viral syndrome.d. is considered low-risk unless he or she also has
difficulty breathing.
38. When performing the skin examination, theemergency physician should evaluate:a. the type of lesion.b. the shape of the individual lesion.c. the arrangement of multiple lesions.d. the pattern of the rash.e. all of the above.
39. Patients who are not toxic or febrile and who havea rash that appears benign should receive:a. a CBC.b. a CBC, chemistry panel, and liver function tests.c. a Gram’s stain.d. a punch biopsy.e. none of the above.
40. Maculopapular rashes:a. are the most common types of rash.b. have the broadest differential diagnosis.c. are usually seen with viral illnesses, bacterial
infection, drug reactions, and other immune-related syndromes.
d. should prompt questions about sick contacts,travel, and new medications.
e. all of the above.
41. Appropriate treatment of cutaneous drug reactionsinclude all of the following except:a. removing the offending drug.b. a short course of steroids.c. diphenhydramine to alleviate pruritus.d. non-sedating antihistamines (instead of diphen-
hydramine if sedation would be a problem) toalleviate pruritus.
42. A target lesion is typically associated with:a. erythema multiforme.b. pemphigus vulgaris.c. Rocky Mountain spotted fever.d. toxic shock syndrome.
43. Which of the following would be theproper disposition of the patient witherythema multiforme?a. immediate admission to the ICU.b. discharge home with a two-week course
of prednisone.c. discharge home with antihistamines and
analgesia for symptomatic relief as needed.d. admission for a day of observation.
44. Diseases that produce diffuse erythematous rashesinclude all of the following except:a. staphylococcal scalded skin syndrome.b. toxic epidermal necrolysis.c. Kawasaki disease.d. the toxic shock syndromes.e. necrotizing fasciitis.
45. Antibiotic prophylaxis for all close contacts ofpatients with meningococcemia, including house-hold members and medical personnel in contactwith respiratory droplets, is mandatory.a. Trueb. False
46. Henoch-Schönlein purpura:a. rarely affects children.b. is a constellation of cutaneous purpura,
arthritis, abdominal pain, gastrointestinalbleeding, and nephritis.
c. requires hospital admission.d. treatment should include antibiotics and
not corticosteroids.
Emergency Medicine Practice 28 www.empractice.net • September 2002
Emergency Medicine Practice is not affiliated with anypharmaceutical firm or medical device manufacturer.
Class I• Always acceptable, safe• Definitely useful• Proven in both efficacy and
effectiveness
Level of Evidence:• One or more large prospective
studies are present (withrare exceptions)
• High-quality meta-analyses• Study results consistently
positive and compelling
Class II• Safe, acceptable• Probably useful
Level of Evidence:• Generally higher levels
of evidence• Non-randomized or retrospec-
tive studies: historic, cohort, orcase-control studies
• Less robust RCTs• Results consistently positive
Class III• May be acceptable• Possibly useful• Considered optional or
alternative treatments
Level of Evidence:• Generally lower or intermediate
levels of evidence
• Case series, animal studies,consensus panels
• Occasionally positive results
Indeterminate• Continuing area of research• No recommendations until
further research
Level of Evidence:• Evidence not available• Higher studies in progress• Results inconsistent,
contradictory• Results not compelling
Significantly modified from: TheEmergency Cardiovascular CareCommittees of the American HeartAssociation and representativesfrom the resuscitation councils ofILCOR: How to Develop Evidence-Based Guidelines for EmergencyCardiac Care: Quality of Evidenceand Classes of Recommendations;also: Anonymous. Guidelines forcardiopulmonary resuscitation andemergency cardiac care. EmergencyCardiac Care Committee andSubcommittees, American HeartAssociation. Part IX. Ensuringeffectiveness of community-wideemergency cardiac care. JAMA1992;268(16):2289-2295.
Class Of Evidence Definitions
Each action in the clinical pathways section of Emergency Medicine Practicereceives an alpha-numerical score based on the following definitions.
Direct all editorial or subscription-related questions to EB Practice, LLC: 1-800-249-5770 • Fax: 1-770-500-1316 • Non-U.S. subscribers, call: 1-678-366-7933
EB Practice, LLC • 305 Windlake Court • Alpharetta, GA 30022E-mail: [email protected] • Web Site: http://www.empractice.net
Emergency Medicine Practice (ISSN 1524-1971) is published monthly (12 times per year) by EB Practice, LLC, 305 Windlake Court, Alpharetta, GA 30022. Opinions expressed are not necessarilythose of this publication. Mention of products or services does not constitute endorsement. This publication is intended as a general guide and is intended to supplement, rather thansubstitute, professional judgment. It covers a highly technical and complex subject and should not be used for making specific medical decisions. The materials contained herein are notintended to establish policy, procedure, or standard of care. Emergency Medicine Practice is a trademark of EB Practice, LLC. Copyright 2002 EB Practice, LLC. All rights reserved. No part of thispublication may be reproduced in any format without written consent of EB Practice, LLC. Subscription price: $249, U.S. funds. (Call for international shipping prices.)
Publisher: Robert Williford. Executive Editor: Heidi Frost.
Physician CME InformationThis CME enduring material is sponsored by Mount Sinai School of Medicine andhas been planned and implemented in accordance with the Essentials andStandards of the Accreditation Council for Continuing Medical Education. Creditmay be obtained by reading each issue and completing the printed post-testsadministered in December and June or online single-issue post-testsadministered at www.empractice.net.
Target Audience: This enduring material is designed for emergency medicinephysicians.
Needs Assessment: The need for this educational activity was determined by asurvey of medical staff, including the editorial board of this publication; reviewof morbidity and mortality data from the CDC, AHA, NCHS, and ACEP; andevaluation of prior activities for emergency physicians.
Date of Original Release: This issue of Emergency Medicine Practice was publishedSeptember 1, 2002. This activity is eligible for CME credit through September1, 2005. The latest review of this material was August 7, 2002.
Discussion of Investigational Information: As part of the newsletter, faculty maybe presenting investigational information about pharmaceutical products thatis outside Food and Drug Administration approved labeling. Informationpresented as part of this activity is intended solely as continuing medicaleducation and is not intended to promote off-label use of any pharmaceuticalproduct. Disclosure of Off-Label Usage: This issue of Emergency Medicine Practicediscusses the use of doxycycline in young children with Rocky Mountainspotted fever. Although it is not approved for this use, clinical studies indicate itis safe and effective for this condition. (See text.)
Faculty Disclosure: In compliance with all ACCME Essentials, Standards, andGuidelines, all faculty for this CME activity were asked to complete a fulldisclosure statement. The information received is as follows: Dr. Nguyen, Dr.Freedman, Dr. Burke, and Dr. Playe report no significant financial interest orother relationship with the manufacturer(s) of any commercial product(s)discussed in this educational presentation.
Accreditation: Mount Sinai School of Medicine is accredited by the AccreditationCouncil for Continuing Medical Education to sponsor continuing medicaleducation for physicians.
Credit Designation: Mount Sinai School of Medicine designates this educationalactivity for up to 4 hours of Category 1 credit toward the AMA Physician’sRecognition Award. Each physician should claim only those hours of creditactually spent in the educational activity. Emergency Medicine Practice is approvedby the American College of Emergency Physicians for 48 hours of ACEP Category1 credit (per annual subscription). Emergency Medicine Practice has been reviewedand is acceptable for up to 48 Prescribed credit hours by the American Academyof Family Physicians. Emergency Medicine Practice has been approved for 48Category 2B credit hours by the American Osteopathic Association.
Earning Credit: Two Convenient Methods• Print Subscription Semester Program: Physicians with current and valid
licenses in the United States who read all CME articles during eachEmergency Medicine Practice six-month testing period, complete the post-test and the CME Evaluation Form distributed with the December and Juneissues, and return it according to the published instructions are eligible forup to 4 hours of Category 1 credit toward the AMA Physician’s RecognitionAward (PRA) for each issue. You must complete both the post-test and CMEEvaluation Form to receive credit. Results will be kept confidential. CMEcertificates will be delivered to each participant scoring higher than 70%.
• Online Single-Issue Program: Physicians with current and valid licenses inthe United States who read this Emergency Medicine Practice CME articleand complete the online post-test and CME Evaluation Form atwww.empractice.net are eligible for up to 4 hours of Category 1 credittoward the AMA Physician’s Recognition Award (PRA). You must completeboth the post-test and CME Evaluation Form to receive credit. Results willbe kept confidential. CME certificates may be printed directly from the Website to each participant scoring higher than 70%.
47. Which of the following is/are a risk factor(s)associated with toxic shock syndrome?a. Soft-tissue infectionb. Surgical woundsc. Indwelling foreign bodies such as
nasal packingd. Use of hyper-absorbent tamponse. All of the above
48. All of the following are true of petechial/purpuric rashes except:a. They can be due to viral, bacterial, or
non-infectious causes.b. They include some of the most rapidly
lethal rashes.c. They are usually caused by toxic
shock syndrome.d. They should be presumed to be caused
by Rocky Mountain spotted fever ormeningococcal disease until ruled out.