Embed Size (px)
Citation preview


DermatophytesInfection
Description:
Dermatophytosis (tinea or ringworm) of the scalp, glabrous skin, and nails is caused by a closely related group of fungi known as dermatophytes which have the ability to utilise keratin as a nutrient source, i.e. they have a unique enzymatic capacity [keratinase].
The disease process in dermatophytosis is unique for two reasons: Firstly, no living tissue is invaded the keratinised stratum corneum is simply colonised. However, the presence of the fungus and its metabolic products usually induces an allergic and inflammatory eczematous response in the host. The type and severity of the host response is often related to the species and strain of dermatophyte causing the infection. Secondly, the dermatophytes are the only fungi that have a dependency on human or animal infection for the survival and dissemination of their species.

Enzyme production and release by the parasitic phase of pathogenic fungi appear to be involved in the pathogenesis of systemic mycoses, as they are closely related to invasion and tissue damage caused by fungi.

Mycoses: diseases cause by fungi
• Superficial • Cutaneous• Subcutaneous • Systemic • Opportunistic

• Clinical manifestations:
• The common anthropophilic species are primarily parasitic on man (Table 1). They are unable to colonise other animals and they have no other environmental sources. On the other hand, geophilic species normally inhabit the soil where they are believed to decompose keratinaceous debris.
• Some species may cause infections in animals and man following contact with soil. Zoophilic species are primarily parasitic on animals and infections may be transmitted to humans following contact with the animal host
• Zoophilic infections usually elicit a strong host response and on the skin where contact with the infective animal has occurred ie arms, legs, body or face.
• Table 1. Ecology of Common Human Dermatophyte Species.
Species Natural habitat
Incidence
Epidermophyton floccosum Humans Common
Trichophyton rubrum Humans Very Common
Trichophyton interdigitale Humans Very Common
Trichophyton tonsurans Humans Common
Trichophyton violaceum Humans Less Common
Trichophyton concentricum Humans Rare*
Trichophyton schoenleinii Humans Rare*
Trichophyton soudanense Humans Rare*
Microsporum audouinii Humans Less Common*
Microsporum ferrugineum Humans Less Common*

• Tinea pedis• Infections by anthropophilic dermatophytes are usually caused by
the shedding of skin scales containing viable infectious hyphal elements [arthroconidia] of the fungus. Desquamated skin scales may remain infectious in the environment for months or years. Therefore transmission may take place by indirect contact long after the infective debris has been shed.
• Substrates like carpet and matting that hold skin scales make excellent vectors. Thus, transmission of dermatophytes like Trichophyton rubrum, T. interdigitale and Epidermophyton floccosum is usually via the feet. In this site infections are often chronic and may remain subclinical for many years only to become apparent when spread to another site, usually the groin or skin.
• It is important to recognize that the toe web spaces are the major reservoir on the human body for these fungi and therefore it is not practical to treat infections at other sites without concomitant treatment of the toe web spaces. This is essential if a "cure" is to be achieved. It should also be recognized that individuals with chronic or subclinical toe web infections are carriers and represent a public health risk to the general population, in that they are constantly shedding infectious skin scales.
• Tinea pedis caused by T. rubrum. Sub-clinical infection (left) showing mild maceration under the little toe and more severe infection showing extensive maceration of all toe web spaces
•
• Tinea is transmitted via the feet by desquamated skin scales in substrates like carpet and matting.

• Tinea cruris• Tinea cruris refers to dermatophytosis of the proximal medial thighs,
preum and buttocks. It occurs more commonly in males and is usually due to spread of the fungus from the feet. Thus the usual causative agents are T. rubrum, T. interdigitale and E. floccosum.
•Tinea of the groin showing typical erythematous lesions on the inner thighs .
•Tinea of the buttocks caused by T. rubrum granular strain .
•
• Tinea of the buttocks caused by T. rubrum downy strain.

• Tinea unguium (dermatophyte onychomycosis)
• Trichophyton rubrum and T. interdigitale are the dominant dermatophyte species involved. In countries like Australia, UK and USA the incidence of dermatophyte onychomycosis has been estimated to be about 3% of the population, increasing up to 5% in the elderly, with some subgroups such as miners, servicemen and sportsmen etc having an incidence of up to 20% due to the use of communal showers and changing rooms.
• It is important to stress that only 50% of dystrophic nails have a fungal etiology, therefore it is essential to establish a correct laboratory diagnosis by either microscopy and/or culture, before treating a patient with a systemic antifungal agent.
•
• Tinea of the nails caused by T. rubrum.• Dermatophyte onychomycosis may be classified into two main
types; (1) superficial white onychomycosis in which invasion is restricted to patches or pits on the surface of the nail; and (2) invasive, subungaul dermatophytosis in which the lateral, distal or proximal edges of the nail are first involved, followed by establishment of the infection beneath the nail plate. Distal subungual onychomycosis is the most common form of dermatophyte onychomycosis. The fungus invades the distal nail bed causing hyperkeratosis of the nail bed with eventual onycholysis, and thickening of the nail plate.

As the name suggests, lateral subungual onychomycosis begins at the lateral edge of the nail and often spreads to involve the entire nail bed and nail plate. In proximal subungual onychomycosis, the fungus invades under the cuticle and infects the proximal rather than the distal nail bed causing yellowish-white spots which slowly invade the lunula and then the nail plate.

• Tinea corporis • Tinea corporis refers to dermatophytosis of the glabrous skin and
may be caused by anthrophophilic species such as T. rubrum usually by spread from another body site or by geophilic and zoophilic species such as M. gypseum and M. canis following contact with either contaminated soil or an animal host.
•
• Tinea corporis caused by T. rubrum in Australian Aborigines living near Darwin in the Northern Territory.
•
• Tinea capitis and corporis caused by M. canis following contact with infectious kittens .
•
•
• Tinea of the beard "Tinea barbae" caused by T. rubrum .•

• Tinea capitis • Tinea capitis refers to dermatophytosis of the scalp. Three types of
in vivo hair invasion are recognised:• 1. Ectothrix invasion is characterised by the development of
arthroconidia on the outside of the hair shaft. The cuticle of the hair is destroyed and infected hairs usually fluoresce a bright greenish yellow colour under Wood's ultraviolet light. Common agents include M. canis, M. gypseum, T. equinum and T. verrucosum.
• 2. Endothrix hair invasion is characterised by the development of arthroconidia within the hair shaft only. The cuticle of the hair remains intact and infected hairs do not fluoresce under Wood's ultraviolet light. All endothrix producing agents are anthropophilic eg T. tonsurans and T. violaceum.
• 3. Favus usually caused by T. schoenleinii, produces favus-like crusts or scutula and corresponding hair loss.
• Tinea capitis showing extensive hair loss caused by M. canis. .
•
• "Kerion" lesion caused by M. canis. •
•
• Endothrix tinea capitis (left) caused by T. tonsurans and "black dot" tinea capitis (right) caused by T. violaceum.

• Laboratory diagnosis • Clinical Material • Skin Scrapings, nail scrapings and epilated hairs. For a laboratory
diagnosis, clinicians should be aware of the need to generate an adequate amount of suitable clinical material. Unfortunately many specimens submitted are either of an inadequate amount or are not appropriate to make a definitive diagnosis. The laboratory needs enough specimen to perform both microscopy and culture. Routine turn around times for direct microscopy should be less than 24 hours, however culture may take several weeks.
• In patients with suspected dermatophytosis of skin [tinea or ringworm] any ointments or other local applications present should first be removed with an alcowipe. Using a blunt scalpel, tweezers, or a bone curette, firmly scrape the lesion, particularly at the advancing border. In cases of vesicular tinea pedis, the tops of any fresh vesicles should be removed as the fungus is often plentiful in the roof of the vesicle.
• In patients with suspected dermatophytosis of nails [onychomycosis] the nail should be pared and scraped using a blunt scalpel until the crumbling white degenerating portion is reached. Any white keratin debris beneath the free edge of the nail should also be collected.
• Skin and nail specimens may be scraped directly onto special black cards which make it easier to see how much material has been collected and provide ideal conditions for transportation to the laboratory.
•
• Black collection cards showing a suitable amount of nail material for a good sample.
• It must be stressed that up to 30% of suspicious material collected from nail specimens may be negative by either direct microscopy or culture. A positive microscopy result showing fungal hyphae and/or arthroconidia is generally sufficient for the diagnosis of dermatophytosis, but gives no indication as to the species of fungus involved. Culture is often more reliable and permits the species of fungus involved to be accurately identified. Repeat collections should always be considered in cases of suspected dermatophytosis with negative laboratory reports.

• Direct Microscopy • Skin Scrapings, nail scrapings and epilated hairs should be examined
using 10% KOH and Parker ink or calcofluor white mounts.
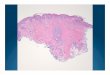
•KOH mount of infected skin scales (left) and nail material (right) showing typical dermatophyte hyphae breaking up into arthroconidia.
•
• KOH mount of infected hairs showing "small spored" ectothrix invasion by M. canis and "large spored" ectothrix invasion by M. gypseum.
•KOH mount of an infected hair showing an endothrix invasion caused by T. tonsurans.

• Culture • Specimens should be inoculated onto primary isolation media, like
Sabouraud's dextrose agar containing cycloheximide (actidione) and incubated at 26-28C for 4 weeks. The growth of any dermatophyte is significant.
•
• Mixed culture of T. violaceum and T. tonsurans from a case of endothrix Tinea capitis in an Australian Aborigine.
• Serology • Not required for diagnosis. • Identification • Characteristic clinical, microscopic and culture features. See
descriptions of individual species for details. • Causative agents:• Epidermophyton floccosum, Microsporum audouinii,
Microsporum canis, Microsporum canis var. disortum, Microsporum cookei, Microsporum equinum, Microsporum ferrugineum, Microsporum fulvum, Microsporum gallinae, Microsporum gypseum, Microsporum nanum, Microsporum persicolor, Microsporum sp., Trichophyton concentricum, Trichophyton equinum, Trichophyton mentagrophyes var. nodulare, Trichophyton mentagrophytes var. erinacei, Trichophyton mentagrophytes var. interdigitale, Trichophyton mentagrophytes var. mentagrophytes, Trichophyton mentagrophytes var. quinckeanum, Trichophyton rubrum, Trichophyton rubrum downy strain, Trichophyton rubrum granular strain, Trichophyton schoenleinii, Trichophyton soudanense, Trichophyton sp., Trichophyton tonsurans, Trichophyton verrucosum, Trichophyton violaceum

• Management • Treatment of dermatophytosis is often dependant on the clinical
setting. For instance uncomplicated single cutaneous lesions can be adequately treated with a topical antifungal agent, however topical treatment of scalp and nail infections is often ineffective and systemic therapy is usually needed to cure these conditions. Chronic or widespread dermatophyte infections, acute inflammatory tinea and "Moccasin" or dry type T. rubrum infection involving the sole and dorsum of the foot usually also require systemic therapy. Ideally, mycological confirmation of the clinical diagnosis should be gained before systemic antifungal treatment is commenced. Oral treatment options for dermatophytosis are listed below (Table 2).
• Table 2. Oral treatment options for cutaneous fungal infections.
Infection Recommended Alternative
Tinea unguium[Onychomycosis]
Terbinafine 250 mg/day6 weeks for finger nails,12 weeks for toe nails.
Itraconazole 200 mg/day/3-5 months or 400 mg/day for one week per month for 3-4 consecutive months. Fluconazole 150-300 mg/ wk until cure [6-12 months].Griseofulvin 500-1000 mg/day until cure [12-18 months].
Tinea capitisGriseofulvin 500mg/day[not less than 10 mg/kg/day]until cure [6-8 weeks].
Terbinafine 250 mg/day/4 wks.Itraconazole 100 mg/day/4wks. Fluconazole 100 mg/day/4 wks
Tinea corporis
Griseofulvin 500 mg/day untilcure [4-6 weeks], often combined with a topicalimidazole agent.
Terbinafine 250 mg/day for 2-4 weeks.Itraconazole 100 mg/day for 15 days or 200 mg/day for 1week.Fluconazole 150-300 mg/week for 4 weeks.
Tinea cruris Griseofulvin 500 mg/dayuntil cure [4-6 weeks].
Terbinafine 250 mg/day for 2-4 weeks.Itraconazole 100 mg/day for 15 days or 200 mg/day for 1week.Fluconazole 150-300 mg/week for 4 weeks.
Tinea pedis Griseofulvin 500mg/dayuntil cure [4-6 weeks].
Terbinafine 250 mg/day for 2-4 weeks.Itraconazole 100 mg/day for 15 days or 200 mg/day for 1week.Fluconazole 150-300 mg/week for 4 weeks.
Chronic and/orwidespreadnon-responsivetinea.
Terbinafine 250 mg/dayfor 4-6 weeks.
Itraconazole 200 mg/day for 4-6 weeks.Griseofulvin 500-1000 mg/day until cure [3-6 months].