Embed Size (px)
Citation preview

CLINICAL REVIEW
Dermoscopy of pigmented skin lesions
Ralph Peter Braun, MD,a Harold S. Rabinovitz, MD,b Margaret Oliviero, ARNP, MSN,b
Alfred W. Kopf, MD,c and Jean-Hilaire Saurat, MDa
Geneva, Switzerland; Miami, Florida; and New York, New York
Dermoscopy is an in vivo method for the early diagnosis of malignant melanoma and the differentialdiagnosis of pigmented lesions of the skin. It has been shown to increase diagnostic accuracy over clinicalvisual inspection in the hands of experienced physicians. This article is a review of the principles ofdermoscopy as well as recent technological developments. ( J Am Acad Dermatol 2005;52:109-21.)
In the last two decades a rising incidence ofmalignant melanoma has been observed.1-7
Because of a lack of adequate therapies formetastatic melanoma, the best treatment currentlyis still early diagnosis and prompt surgical excision ofthe primary cancer.5,7 Dermoscopy (also known asepiluminescence microscopy, dermatoscopy, andamplified surface microscopy) is an in vivo method,that has been reported to be a useful tool for the earlyrecognition of malignant melanoma.8-11 The perfor-mance of dermoscopy has been investigated bymany authors. Its use increases diagnostic accuracybetween 5% and 30% over clinical visual inspection,depending on the type of skin lesion and experienceof the physician.12-16 This was confirmed by recentevidence-based publications and based on a meta-analysis of the literature.17,18 This article is a review ofthe principles of dermoscopy as well as recenttechnological developments.
From the Pigmented Skin Lesion Unit, Department of Dermatol-
ogy, University Hospital Genevaa; Skin and Cancer Associates,
Plantation, Fla, and Department of Dermatology, University of
Miami School of Medicineb; and The Ronald O. Perelman
Department of Dermatology, New York University School of
Medicine.c
Funding sources: The work of Dr Braun has been supported by the
Swiss Cancer League. Dr Kopf has the following funding
sources: The Ronald O. Perelman Department of Dermatology,
New York University School of Medicine, Joseph H. Hazen
Foundation, Mary and Emanuel Rosenthal Foundation, Kaplan
Comprehensive Cancer Center (Cancer Center Support Core
Grant No. 5P30-CA-16087), Blair O. Rogers Medical Research
Fund, The Rahr Family Foundation, and Stravros S. Niarchos
Foundation Fund of the Skin Cancer Foundation.
Conflict of interest: None.
Accepted for publication November 9, 2001.
Reprint requests: R. P. Braun, MD, Department of Dermatology,
University Hospital Geneva, 24, rue Micheli-du-Crest, CH—
1211Geneva 14, Switzerland. E-mail: [email protected].
0190-9622/$30.00
ª 2005 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2001.11.001
HISTORY OF DERMOSCOPYSkin surface microscopy started in 1663 with
Kolhaus who investigated the small vessels in thenailfold with the help of a microscope.11,19 In 1878,Abbe described the use of immersion oil in lightmicroscopy 20 and this principle was transferred toskin surface microscopy by the German dermatolo-gist, Unna, in 1893.21 He introduced the term‘‘diascopy’’ and described the use of immersion oiland a glass spatula for the interpretation of lichenplanus and for the evaluation of the infiltrate in lupuserythematosus. The term ‘‘dermatoscopy’’ was in-troduced in 1920 by the German dermatologistJohann Saphier who published a series of commu-nications using a new diagnostic tool resemblinga binocular microscope with a built-in light sourcefor the examination of the skin.22-25 He used this newtool in various indications and did some interestingmorphological observations on anatomical struc-tures of the skin which indicated the high perfor-mance of his equipment. Skin surface microscopywas further developed in the United States byGoldman in the 1950s. He published a series ofinteresting articles on new devices on what he called‘‘Dermoscopy.’’26-29 He was the first dermatologist touse this new technique for the evaluation of pig-mented skin lesions. In 1971, Rona MacKie30 clearlyidentified, for the first time, the advantage of surfacemicroscopy for the improvement of preoperativediagnosis of pigmented skin lesions and for thedifferential diagnosis of benign versus malignantlesions. These investigations were continued mainlyin Europe by several Austrian and German groups.The first Consensus Conference on Skin SurfaceMicroscopy was held in 1989 in Hamburg31 and theConsensus Netmeeting on Dermoscopy, which washeld in 2001 in Rome32 (http://www.dermoscopy.org), was the first international meeting of itskind. Today dermoscopy has become a routinetechnique in Europe and is gaining acceptance inother countries.
109

J AM ACAD DERMATOL
JANUARY 2005
110 Braun et al
Table I. Vascular architecture of pigmented skin lesions according to Kreusch and Koch57
Morphological aspect Type of pathology
Tree-like vessels Thick, arborizing vessels, superficial Pigmented BCC of any type (discrete insuperficial BCCs)
Corona vessels ‘‘Surround’’ the tumor Sebaceous gland hyperplasiaThinner than tree-like vesselsLess curved than tree-like vessels
Comma-shaped vessels Short, strong, curved, Dermal neviLocated on the tumorShort distance, parallel to skin surface
Point vessels Short capillary loops Thin malignant melanomasDense packed red points Epithelial tumors such as actinic keratosis,
Bowen’s disease, etc (short vertical height)Not in the holes of the pigment networkHairpin vessels Long capillary loops of thicker tumors at the
borderThick melanomas
Whitish halo in tumors with keratin SCC keratoacanthoma, seborrheic keratosis
BCC, Basal cell carcinoma; SCC, squamous cell carcinoma.
PHYSICAL ASPECTSLight is either reflected, dispersed, or absorbed by
the stratum corneum because of its refraction indexand its optical density, which is different from air.33
Thus, deeper underlying structures cannot be ade-quately visualized. However, when various immer-sion liquids are used, they render the skin surfacetranslucent and reduce the reflection, so that un-derlying structures are readily visible. The applica-tion of a glass plate flattens the skin surface andprovides an even surface. Optical magnification isused for examination. Taken together, these opticalmeans allow the visualization of certain epidermal,dermo-epidermal, and dermal structures.
MATERIAL FOR DERMOSCOPYDermoscopy requires optical magnification and
liquid immersion. This can be performed with verysimple, inexpensive equipment.34,35 Specially de-signed handheld devices with 10 to 20 times magni-fication are commercially available (Dermatoscope[Heine AG]; DermoGenius Basic [RodenstockPrazisionsoptik]; Episcope [Welch-Allyn]; DermLite[3Gen, LLC]). Photographic documentation can beperformed with a dermoscopic attachment to a stan-dard camera (Dermaphot, Heine, AG) which can beused also with some digital cameras. Most recently,digital cameras have been designed that are attachedto computers. This allows easy storage, retrieval, andfollow-up of pigmented skin lesions. For dermatol-ogists with less experience in dermoscopy, some ofthe systems may offer the possibility of computer-assisted diagnosis for malignant melanoma or forconsulting an expert through telemedicine.
DERMOSCOPIC CRITERIAColors
The use of dermoscopy allows the identificationof many different structures and colors, not seen bythe naked eye.
Colors play an important role in dermoscopy.Common colors are light brown, dark brown, black,blue, blue-gray, red, yellow, and white. The mostimportant chromophore in melanocytic neoplasms ismelanin.11,13,36 The color of melanin essentiallydepends on its localization in the skin. The colorblack is due to melanin located in the stratumcorneum and the upper epidermis, light to darkbrown in the epidermis, gray to gray-blue in thepapillary dermis and steel-blue in the reticulardermis.11,13 The color blue occurs when there ismelanin localized within the deeper parts of the skinbecause the portions of visible light with shorterwavelengths (blue-violet end of spectrum) are moredispersed than portions with longer wavelengths(red end of visible spectrum).37,38 The color red isassociated with an increased number or dilatation ofblood vessels, trauma, or neovascularization. Thecolor white is often caused by regression and/orscarring.11
Dermoscopic structuresIn this context we will use the nomenclature as
proposed by the recent Consensus Netmeeting (heldin Rome in 2001) with some revisions32:
Pigment network. The pigment network isa grid-like (honeycomb-like) network consistingof pigmented ‘‘lines’’ and hypopigmented‘‘holes.’’11,13,36,37,39 The anatomic basis of the

J AM ACAD DERMATOL
VOLUME 52, NUMBER 1
Braun et al 111
pigment network is either melanin pigment inkeratinocytes, or in melanocytes along the dermoe-pidermal junction.40 The reticulation (network) rep-resents the rete ridge pattern of the epidermis.41-43
The relatively hypomelanotic holes in the networkcorrespond to tips of the dermal papillae and theoverlying suprapapillary plates of the epider-mis.13,36,37
The pigment network can be either typical oratypical. A typical network is relatively uniform,regularly meshed, homogeneous in color, and usu-ally thinning out at the periphery.36,39,44 An atypicalnetwork is nonuniform, with darker and/or broad-ened lines and ‘‘holes’’ that are heterogeneous inarea and shape. The lines are often hyperpigmentedand may end abruptly at the periphery.36,39,44
If the rete ridges are short or less pigmented, thepigment network may not be visible. Areas devoid ofany network (but without signs of regression) arecalled ‘‘structureless areas.’’11,45
Dots. Dots are small, round structures less than0.1 mm in diameter, which may be black, brown,gray, or blue-gray.11,13,32,36 Black dots are caused bypigment accumulation in the stratum corneum and inthe upper part of the epidermis.11,37,42,46 Brown dotsrepresent focal melanin accumulations at the der-moepidermal junction.47 Gray-blue granules (pep-pering) are caused by tiny melanin structures in thepapillary dermis. Gray-blue or blue granules are dueto loose melanin, fine melanin particles or melanin‘‘dust’’ in melanophages or free in the deep papillaryor reticular dermis.11,37,42,46
Globules. Globules are symmetrical, round tooval, well-demarcated structures that may be brown,black, or red.11,13,32,36 They have a diameter which isusually larger than 0.1 mm and correspond to nestsof pigmented benign or malignant melanocytes,clumps of melanin, and/or melanophages situated
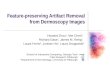
Fig 1. Two-step procedure for the classification of pig-mented skin lesions. Adapted from Argenziano G et al.J Am Acad Dermatol 2003;48:679-93.32
usually in the lower epidermis, at the dermoepider-mal junction, or in the papillary dermis.11,37,42,46
Both dots and globules may occur in benign aswell as in malignant melanocytic proliferations. Inbenign lesions, they are rather regular in size andshape and quite evenly distributed (frequently in thecenter of a lesion).32,36 In melanomas they tend tovary in size and shape and are frequently found inthe periphery of lesions.32,36,48
Branched streaks. Branched streaks are anexpressionof an alteredpigmentednetwork inwhichthe network becomes disrupted or broken up.11,32,45
Their pathological correlations are remnants of pig-mented rete ridges and bridging nests of melanocyticcells within the epidermis and papillary dermis.11
Radial streaming. Radial streaming appears asradially and asymmetrically arranged, parallel linearextensions at the periphery of a lesion.13,49 Histo-logically, they represent confluent pigmented junc-tional nests of pigmented melanocytes.13,36
Pseudopods. Pseudopods represent fingerlikeprojections of dark pigment (brown to black) at theperiphery of the lesion.13,49,50 They may have smallknobs at their tips, and are either connected to thepigment network or directly connected to the tumorbody.13,50 They correspond as well to intraepidermalor junctional confluent radial nests of melano-cytes.13,50 Menzies et al49 found pseudopods to beone of the most specific features of superficialspreading melanoma.
Streaks. ‘‘Streaks’’ is a term used by someauthors interchangeably with radial streaming or
Fig 2. Algorithm for the determination of melanocyticversus nonmelanocytic lesions according to the proposi-tion of the Board of the Consensus Netmeeting. Adaptedfrom Argenziano G et al. J Am Acad Dermatol 2003;48:679-93.32

J AM ACAD DERMATOL
JANUARY 2005
112 Braun et al
Fig 3. A, Macroscopic picture of a superficial spreading malignant melanoma (Breslowthickness 0.52 mm; Clark level II). B, Dermoscopy of A shows (atypical) pigment network andbranched streaks and can therefore be considered a melanocytic lesion.
Fig 4. A, Macroscopic picture of a blue nevus. B, Dermoscopy of A shows steel-blue areas (nopigment network, no aggregated globules, no branched streaks).
Fig 6. A, Macroscopic picture of a seborrheic keratosis. B, Dermoscopy of A shows comedo-like openings and multiple milia-like cysts.
Fig 5. A, Macroscopic picture of a seborrheic keratosis. B, Dermoscopy of A shows comedo-like openings (a), multiple milia-like cysts (b), and fissures (c).

J AM ACAD DERMATOL
VOLUME 52, NUMBER 1
Braun et al 113
Fig 8. A, Macroscopic picture of a basal cell carcinoma. B, Dermoscopy of A shows multiplespoke wheel areas.
Fig 7. A, Macroscopic picture of a basal cell carcinoma. B, Dermoscopy of A shows mapleleafelike areas, ovoid nests, and arborized telangiectasia.
Fig 9. A, Macroscopic picture of an angioma. B, Dermoscopy of A shows red lagoons.
pseudopods. This is because both these structureshave the same histopathological correlation.11,37,42,46
Streaks can be irregular, when they are unevenlydistributed (malignant melanoma), or regular (sym-metrical radial arrangement over the entire lesion).The latter is particularly found in the pigmentedspindle cell nevi (Reed’s nevi).51-53
Structureless areas. Structureless areas repre-sent areas devoid of any discernible structures (eg,globules, network). They tend to be hypopig-mented, which is due to the absence of pigment ordiminution of pigment intensity within a pigmentedskin lesion.11
Blotches. A blotch (also called black lamella bysome authors) is caused by a large concentration of
melanin pigment localized throughout the epidermisand/or dermis visually obscuring the underlyingstructures.41-43,46
Regression pattern. Regression appears aswhite scar-like depigmentation (lighter than the sur-rounding skin) or ‘‘peppering’’ (speckled multipleblue-gray granules within a hypopigmented area).Histologically, regression shows fibrosis, loss of pig-mentation, epidermal thinning, effacement of the reteridges, and melanin granules free in the dermis or inmelanophages scattered in the papillary dermis.43,46
Blue-white veil. Blue-white veil is an irregu-lar, indistinct, confluent blue pigmentation withan overlying white, ground-glass haze.13,32 Thepigmentation cannot occupy the entire lesion.

J AM ACAD DERMATOL
JANUARY 2005
114 Braun et al
Table II. Pattern analysis according to Pehamberger et al39 (modified)
Lentigo simplex Junctional nevus Compound nevus Dermal nevus Blue nevus
Regular pigmentnetwork withoutinterruptions
Regular pigmentnetwork withoutinterruptions
Regular pigmentnetwork withoutinterruptions
No criteria formelanocytic lesion
Steel-blue areas
Regular border, thinsout at periphery
Regular border, thinsout at periphery
Regular border, thinsout at periphery
No pigment network No pigment network
Black dots over gridsof pigmentnetwork
Heterogeneous holesof pigmentnetwork
Heterogeneous holesof pigmentnetwork
Brown globules lll-defined
Brown-black globulesat center of thelesion
Brown globules Brown globules Homogeneouscolors
White veils arepossible
Homogeneous colors Homogeneous colors Symmetric papularappearance
‘‘Pseudonetwork’’ No pseudonetwork
All criteria formelanocytic lesionpossible
‘‘Comma’’-shapedblood vessels
Color heterogeneitypossible
Histopathologically this corresponds to an aggrega-tion of heavily pigmented cells or melanin in thedermis (blue color) in combination with a compactorthokeratosis.13,32,36,43,46,54
Vascular pattern. Pigmented skin lesions mayhave dermoscopically visible vascular patterns,which include ‘‘comma vessels,’’ ‘‘point vessels,’’‘‘tree-like vessels,’’ ‘‘wreath-like vessels,’’ and ‘‘hair-pin-like vessels’’ (Table I).55-57 Atypical vascularpatterns may include linear, dotted, or globular redstructures irregularly distributed within the le-sion.32,36,58,59 Some of the vascular patterns may becaused by neovascularization. For the evaluation ofvascular patterns, there has to be as little pressure aspossible on the lesion during examination becauseotherwise the vessels are simply compressed andwill not be visible. The use of ultrasound gel forimmersion helps to reduce the pressure necessaryfor the best evaluation of the skin lesion.57
Milia-like cysts. Milia-like cysts are round whit-ish or yellowish structures which are mainly seen inseborrheic keratosis.* They correspond to intraepi-dermal keratin-filled cysts and may also be seen incongenital nevi as well as in some papillomatousmelanocytic nevi. At times, milia-like cysts arepigmented, and thus, can resemble globules.
*References 8, 11, 13, 32, 36, 37, 49, 55, 60-63.Comedo-like openings (crypts, pseudofollic-
ular openings). Comedo-like openings (with‘‘blackhead-like plugs’’) are mainly seen in sebor-rheic keratoses or in some rare cases in papilloma-tous melanocytic nevi.y The keratin-filled invaginationsof the epidermis correspond to the comedo-likestructures histopathologically.
yReferences 8, 11, 13, 32, 36, 37, 49, 55, 60-64.Fissures and ridges (‘‘brain-like appear-
ance’’). Fissures are irregular, linear keratin-filleddepressions, commonly seen in seborrheic kerato-ses.63 They may also be seen in melanocytic neviwith congenital patterns and in some dermal mela-nocytic nevi. Multiple fissures might give a ‘‘brain-like appearance’’ to the lesion.32,36,63,65 This patternhas also been named ‘‘gyri and sulci’’ or ‘‘mountainand valley pattern’’ by some authors.11
Fingerprint-like structures. Some flat sebor-rheic keratoses (also known as solar lentigines) canshow tiny ridges running parallel and producinga pattern that resembles fingerprints.11,32,65,66
Moth-eaten border. Some flat seborrheic kera-toses (mainly on the face) have a concave borderso that the pigment ends with a curved structure,which has been compared to a moth-eaten gar-ment.11,13,32,63,65,66
Leaf-like areas. Leaf-like areas (maple leafelikeareas) are seen as brown to gray-blue discretebulbous blobs, sometimes forming a leaf-like pat-tern.* Their distribution reminds one of the shapeof finger pads. In absence of a pigment network,they are suggestive of pigmented basal cell car-cinoma.11,32,67
*References 8, 9, 11, 13, 32, 36, 37, 39, 55, 65,67, 68.
Spoke wheelelike structures. Spoke wheelelike structures are well-circumscribed, brown togray-blue-brown, radial projections meeting ata darker brown central hub.11,32,67 In the absenceof a pigment network, they are highly suggestive ofbasal cell carcinoma.

J AM ACAD DERMATOL
VOLUME 52, NUMBER 1
Braun et al 115
Table III. ABCD rule of dermoscopy according to Stoiz et al (modified)11,45
Points Weight factor Subscore range
Asymmetry Complete symmetry 0 1.3 0-2.6Asymmetry in 1 axis 1Asymmetry in 2 axis 2
Border 8 segments, 1 point for abrupt cut-off of pigment 0-8 0.1 0-0.8Color 1 point for each color: 1-6 0.5 0.5-3.0
WhiteRedLight brownDark brownBlackBlue-gray
Differential structures 1 point for every structure: 1-5 0.5 0.5-2.5Pigment networkStructureless areasDotsGlobulesStreaks
Total score range: 1.0-8.9
Table II. Cont’d
Malignant melanoma Atypical (Clark) nevus Angioma Seborrheic keratosis Pigmented BCC
Heterogeneous(colors andstructures)
Irregular pigmentnetwork withinterruptions
No features ofmelanocytic lesion
No features formelanocytic lesion
No features formelanocytic lesion
Asymmetry (colorsand structures)
Heterogeneous holes No pigment network Pigment networkusually absent
Maple-leafelikepigmentation
Irregular pigmentnetwork
Irregular border Red, red-blue, orred-black lagoons,( globules, saccules)
Milia-like cysts Telangiectasia
Irregular border withabrupt peripheralmargin
Heterogeneity ofcolors
Abrupt border cut-off Pseudofollicularopenings,comedo-likeopenings (plugs)
Tree-like bloodvessels
Structureless areas Gray-white veil Rough surface ‘‘Dirty’’ gray-brown togray-black colors
Gray-blue or red-roseveils
Absence of primarycriteria formalignantmelanoma
Abrupt border cut-off
Red Opaque gray-browncolors
Pseudopods/radialstreaming
Point and hairpinvessels
Large blue-gray ovoid nests. Ovoid nests arelarge, well-circumscribed, confluent or near-con-fluent, pigmented ovoid areas, larger than glob-ules, and not intimately connected to a pigmentedtumor body.11,32,67 When a network is absent,ovoid nests are highly suggestive of basal cellcarcinoma.
Multiple blue-gray globules. Multiple blue-gray globules are round, well-circumscribed struc-tures that are, in the absence of a pigment network,highly suggestive of basal cell carcinoma.11,32,67
They have to be differentiated from multiple blue-gray dots (which correspond to melanophages andmelanin dust).

J AM ACAD DERMATOL
JANUARY 2005
116 Braun et al
DIFFERENTIAL DIAGNOSIS OFPIGMENTED LESIONS OF THE SKIN
There are many publications on the subject of thedifferential diagnosis of pigmented lesions of theskin. The 5 algorithms most commonly used arepattern analysis8,39,62; the ABCD rule of dermo-scopy11,45,70; the 7-point checklist32,36,44; theMenzies method13,32,49; and the revised patternanalysis.71
The Board of the Consensus Netmeeting agreedon a two-step procedure for the classification ofpigmented lesions of the skin (Fig 1). A similarapproach has been proposed by other authors inthe past.
The first step is the differentiation betweena melanocytic and a nonmelanocytic lesion. Forthis decision, the algorithm in Fig 2 is used.
Are aggregated globules, pigment network,branched streaks (Fig 3), homogeneous blue pig-mentation (blue nevus: Fig 4), or a parallel pattern(palms, soles, and mucosa) visible? If this is the case,the lesion should be considered as a melanocyticlesion (Fig 3). If not, the lesion should be evaluatedfor the presence of comedo-like plugs, multiplemilia-like cysts, and comedo-like openings, irregularcrypts, light brown fingerprint-like structures, or‘‘fissures and ridges’’ (brain-like appearance) pat-tern. If so, the lesion is suggestive of a seborrheickeratosis (Figs 5 and 6). If not, the lesion has to beevaluated for the presence of arborizing bloodvessels (telangiectasia), leaf-like areas, large blue-gray ovoid nests, multiple blue-gray globules, spokewheel areas, or ulceration. If present, the lesion issuggestive of basal cell carcinoma (Figs 7 and 8). Ifnot, one has to look for red or red-blue (to black)lagoons. If these structures are present, the lesionshould be considered a hemangioma (Fig 9) or anangiokeratoma. If all the preceding questions wereanswered with ‘‘no,’’ the lesion should still beconsidered to be a melanocytic lesion.
Table IV. The 7-point checklist according toArgenziano et al44
Criteria 7-point score
Major criteriaAtypical pigment network 2Blue-white veil 2Atypical vascular pattern 2
Minor criteriaIrregular streaks 1Irregular pigmentation 1Irregular dots/globules 1Regression structures 1
Once the lesion is identified to be of melanocyticorigin, the decision has to be made if the melanocyticlesion is benign, suspect, or malignant. To accom-plish this, 4 different approaches are the mostcommonly used.
Pattern analysis (Pehamberger et al)Pattern recognition has historically been used by
clinicians and histopathologists to differentiate be-nign lesions from malignant neoplasms. A similarprocess has been found useful with dermoscopy,and has been termed ‘‘pattern analysis.’’ It allowsdistinction between benign and malignant growthfeatures. It was described by Pehamberger andcolleagues based on the analysis of more than 7000pigmented skin lesions.8,39,62 Table II shows thetypical patterns of some common, pigmented skinlesions using pattern analysis.
ABCD rule of dermatoscopy (Stolz et al)The ABCD rule of dermatoscopy, described by
Stolz et al in 1993 was based on an analysis of 157pigmented skin lesions.11,70 The complete ABCDrule is explained in Table III.
For the evaluation of asymmetry, the lesion isdivided into 4 segments (2 perpendicular axes). Theaxes are oriented so that the lowest asymmetry isobtained. For asymmetry in both axes, a value of 2 isobtained. To calculate the subscore, the value of eachABCD category has to be multiplied by the corre-sponding weight factor. To obtain the total scorevalue, the different ABCD subscores have to beadded.
The total score ranges from 1 to 8.9. A lesion witha total score greater than 5.45 should be consideredas melanoma. A lesion with a total score of 4.75or less can be considered as benign. A lesion witha score value between 4.75 and 5.45 should be
Table V. ‘‘The Menzies Method’’ according toMenzies et al13,49
Negative featuresPoint and axial symmetry of pigmentationPresence of a single color
Positive featuresBlue-white veilMultiple brown dotsPseudopodsRadial streamingScar-like depigmentationPeripheral black dots-globulesMultiple colors (5 or 6)Multiple blue/gray dotsBroadened network

J AM ACAD DERMATOL
VOLUME 52, NUMBER 1
Braun et al 117
Table VI. Pattern of benign and malignant lesions
Benign Malignant
Dots Centrally located or situated right on thenetwork
Unevenly distributed and scattered focally atthe periphery
Globules Uniform in size, shape, and color, symmetricallylocated at the periphery, centrally located, oruniform throughout the lesion as in acobblestone pattern
Globules that are unevenly distributed andwhen reddish are highly suggestive ofmelanoma
Streaks Radial streaming or pseudopods tend to besymmetrical and uniform at the periphery
Radial streaming or pseudopods tend to befocal and irregular at periphery
Blue-white veil Tends to be centrally located Tends to be asymmetrically located or diffusealmost over entire lesion
Blotch Centrally located or may be diffusehyperpigmented area that extends almost toperiphery of the lesion
Asymmetrically located or there are oftenmultiple asymmetrical blotches
Network Typical network that consists of light to darkuniform pigmented lines andhypopigmented holes
Atypical network that may be nonuniform withblack/brown or gray thickened lines andholes of different sizes and shapes
Network borders Either fades into the periphery or issymmetrically sharp
Focally sharp
considered ‘‘suspicious’’ and should therefore bemonitored closely or removed.11,70
7-point checklistIn 1998 Argenziano and colleagues described a 7-
point checklist based on the analysis of 342 pig-mented skin lesions.32,36,44 They distinguish 3 majorcriteria and 4 minor criteria (Table IV). Each majorcriterion has a score of 2 points while each minorcriterion has a score of 1 point. A minimum totalscore of 3 is required for the diagnosis of malignantmelanoma.
Menzies methodIn the Menzies method13,32,49 for diagnosing
melanoma, both of the following negative featuresmust not be found: a single color (tan, dark brown,gray, black, blue, and red, but white is not consid-ered) and ‘‘point and axial symmetry of pigmenta-tion’’ (refers to pattern symmetry around any axisthrough the center of the lesion). This does notrequire the lesion to have symmetry of shape.Additionally, at least one positive feature must befound (Table V).
Exceptions to the algorithmsThe ABCD rule is not applicable for pigmented
lesions on the palms, soles, or face.11 Palms and soleshave a particular anatomy which is characterized bymarked orthokeratosis and the presence of sulci andgyri. The sweat ducts join the surface at the summitsof the gyri.11,32 A classification of 10 differentdermoscopy patterns on the palms and soles hasbeen proposed by Saida et al.72
The face has a very particular anatomic architec-ture especially concerning the dermoepidermaljunction where rete ridges are shorter. That is whyfacial lesions often do not exhibit a regular pigmentnetwork. Dermoscopy shows a broadened pigmentreticulation which is called a ‘‘pseudonetwork.’’ Thisdoes not correspond to the projection of pigmentedrete ridges. It is due to a homogeneous pigmentationwhich is interrupted by the surface openings of theadnexal structures.11,66,73
The differential diagnosis of a pseudonetwork issolar lentigo, seborrheic keratosis, lentigo simplex,melanoma in situ, lichen planuselike keratosis, andpigmented actinic keratosis.11,66,73 These lesionsare often difficult to distinguish dermoscopically.However, when there are multiple colors anda broadened, thickened, and irregular ‘‘pseudonet-work,’’ melanoma is often the diagnosis suggested.Other, more specific characteristics include an ‘‘an-nular granular’’ or ‘‘rhomboidal pattern.’’11,66,73
Revised pattern analysisThe overall general appearance of color, architec-
tural order, symmetry of pattern, and homogeneity(CASH) are important components in distinguishingthese two groups. Benign melanocytic lesions tendto have few colors, architectural order, symmetry ofpattern, or homogeneity. Malignant melanoma oftenhas many colors and much architectural disorder,asymmetry of pattern, and heterogeneity.
The reticular pattern or network pattern is themost common global feature in melanocytic lesions.This pattern represents the junctional component

J AM ACAD DERMATOL
JANUARY 2005
118 Braun et al
of a melanocytic nevus (Clark nevus, dysplasticnevus).32,36,71
Another pattern is the so-called globular pattern.It is characterized by the presence of numerous‘‘aggregated globules.’’ This pattern is commonlyseen in a congenital nevus, superficial type.32,36,71
The cobblestone pattern is very similar to theglobular pattern but is composed of closer aggre-gated globules, which are somehow angulated, re-sembling cobblestones.
The homogeneous pattern appears as diffusepigmentation, which might be brown, gray-blue,gray-black, or reddish black.32,36,71 No pigmentnetwork or any other distinctive dermoscopy struc-ture is found. An example is the homogeneous steel-blue color seen in blue nevi.
The so-called starburst pattern is characterized bythe presence of streaks in a radial arrangement,which is visible at the periphery of the lesion.32,36,71
This pattern is commonly seen in Reed nevi or Spitznevi.
The parallel pattern is exclusively found on thepalms and soles due to the particular anatomy ofthese areas.32,36,71
The combination of 3 or more distinctive dermo-scopic structures (ie, network, dots, and globules aswell diffuse areas of hyperpigmentation and hypo-pigmentation) within a given lesion is called multi-component pattern.32,36,71 This pattern is highlysuggestive of melanoma, but might be observed insome cases in acquired melanocytic nevi and con-genital nevi.
The term ‘‘lesions with indeterminate patterns’’are dermoscopic patterns that can be seen in bothbenign and malignant pigmented lesions. Clinicallyand dermoscopically, one cannot make a distinctionbetween whether they are melanomas or atypicalnevi.
In addition to the global features already men-tioned, the local features (dermoscopic structuressuch as the pigment network, dots, and globules, etc)are important to evaluate melanocytic lesions(Table VI).
PERSPECTIVESBecause computer hardware has become user-
friendly and more affordable, digital dermoscopywill become more integrated into the clinical setting.The currently available digital dermoscopic systemsalready have an acceptable picture quality whichcomes close to a photograph.74 Digital images offerthe possibility of computer storage and retrieval ofdermoscopic images and patient data.48,75-78 Somesystems even offer the potential of ‘‘computer-assisted diagnosis.’’79-94 Because diagnostic accuracy
with dermoscopy has been shown to depend on theexperience of the dermatologist, such objectivesystems might help less-experienced dermatologistsin the future.
Another expanding field is teledermoscopy. Atthe beginning of the digital dermoscopic era, tele-dermoscopy was used between experts to exchangedifficult or interesting images. The development ofnew electronic media and the evolution of theInternet will have an important impact as the in-frastructure becomes available to almost everyone,and the exchange is now easy to perform. Recentstudies were able to show the feasibility and impor-tance of teledermoscopy.95-98 This was recently usedin a Consensus Netmeeting on Dermoscopy held inRome during the first World57,69 Congress on Der-moscopy (http://www.dermoscopy.org).32
We thank Dr G. Argenziano, Dr J. Kreusch, Professor S.Menzies, Professor H. Pehamberger, and Professor W.Stolz for their suggestions and their permission for thereproductions. We also thank Dr S. Rabinovitz for her helpduring the entire editing process and for her valuablesuggestions.
REFERENCES
1. Rigel DS, Friedman RJ, Kopf AW. The incidence of malignant
melanoma in the United States: Issues as we approach the
21st century. J Am Acad Dermatol 1996;34:839-47.
2. Rigel DS, Friedman RJ, Kopf AW. Lifetime risk for development
of skin cancer in the U.S. population: current estimate is now 1
in 5. J Am Acad Dermatol 1996;35:1012-3.
3. Landis SH, Murray T, Bolden S, Wingo PA. Cancer statistics,
1999. CA Cancer J Clin 1999;49:8-31.
4. Landis SH, Murray T, Bolden S, Wingo PA. Cancer statistics,
1998. CA Cancer J Clin 1998;48:6-29.
5. Rigel DS, Carucci JA. Malignant melanoma: prevention, early
detection, and treatment in the 21st century. CA Cancer J Clin
2000;50:215-36.
6. Burton RC. Malignant melanoma in the year 2000. CA Cancer
J Clin 2000;50:209-13.
7. Rigel DS. Malignant melanoma: perspectives on incidence and
its effects on awareness, diagnosis, and treatment. CA Cancer
J Clin 1996;46:195-8.
8. Pehamberger H, Binder M, Steiner A, Wolff K. In vivo
epiluminescence microscopy: improvement of early diagnosis
of melanoma. J Invest Dermatol 1993;100:356S-62S.
9. Soyer HP, Argenziano G, Chimenti S, Ruocco V. Dermoscopy of
pigmented skin lesions. Eur J Dermatol 2001;11:270-6.
10. Soyer HP, Argenziano G, Talamini R, Chimenti S. Is dermoscopy
useful for the diagnosis of melanoma? Arch Dermatol
2001;137:1361-3.
11. Stolz W, Braun-Falco O, Bilek P, Landthaler M, Burgdorf WHC,
Cognetta AB. Color alas of drmatoscopy. 2nd ed. Berlin:
Blackwell Wissenschafts-Verlag; 2002.
12. Mayer J. Systematic review of the diagnostic accuracy of
dermatoscopy in detecting malignant melanoma. Med J Aust
1997;167:206-10.
13. Menzies SW, Crotty KA, Ingvar C, McCarthy WH. An atlas of
surface microscopy of pigmented skin lesions. Sydney:
McGraw-Hill Book Company; 2003.

J AM ACAD DERMATOL
VOLUME 52, NUMBER 1
Braun et al 119
14. Binder M, Schwarz M, Winkler A, Steiner A, Kaider A, Wolff K,
et al. Epiluminescence microscopy. A useful tool for the di-
agnosis of pigmented skin lesions for formally trained
dermatologists. Arch Dermatol 1995;131:286-91.
15. Binder M, Puespoeck-Schwarz M, Steiner A, Kittler H, Muellner
M, Wolff K, et al. Epiluminescence microscopy of small
pigmented skin lesions: short-term formal training improves
the diagnostic performance of dermatologists. J Am Acad
Dermatol 1997;36:197-202.
16. Westerhoff K, McCarthy WH, Menzies SW. Increase in the
sensitivity for melanoma diagnosis by primary care physicians
using skin surface microscopy. Br J Dermatol 2000;143:
1016-20.
17. Bafounta ML, Beauchet A, Aegerter P, Saiag P. Is dermoscopy
(epiluminescence microscopy) useful for the diagnosis of
melanoma? Results of a meta-analysis using techniques
adapted to the evaluation of diagnostic tests. Arch Dermatol
2001;137:1343-50.
18. Kittler H, Pehamberger H, Wolff K, Binder M. Diagnostic
accuracy of dermoscopy. Lancet Oncol 2002;3:159-65.
19. Gilje O, O’Leary PA, Baldes EY. Capillary microscopic examina-
tion in skin siease. Arch Dermatol 1958;68:136-45.
20. Diepgen P. Geschichte der Medizin. Berlin: De Gruyter; 1965.
21. Unna P. Die Diaskopie der Hautkrankheiten. Berl Klin Wochen
1885;42:1016-21.
22. Saphier J. Die Dermatoskopie. I. Mitteilung. Arch Dermatol
Syphiol 1920;128:1-19.
23. Saphier J. Die Dermatoskopie. II. Mitteilung. Arch Dermatol
Syphiol 1921;132:69-86.
24. Saphier J. Die Dermatoskopie. IV. Mitteilung. Arch Dermatol
Syphiol 1921;136:149-58.
25. Saphier J. Die Dermatoskopie. III. Mitteilung. Arch Dermatol
Syphiol 2002;134:314-22.
26. Goldman L. Some investigative studies of pigmented nevi
with cutaneous microscopy. J Invest Dermatol 1951;16:407-26.
27. Goldman L. Clinical studies in microscopy of the skin at
moderate magnification. Arch Dermatol 1957;75:345-60.
28. Goldman L. A simple portable skin microscope for surface
microscopy. Arch Dermatol 1958;78:246-7.
29. Goldman L. Direct skin microscopy as an aid in the early
diagnosis of precancer and cancer of the skin in the elderly.
J Am Geriatr Soc 1980;28:337-40.
30. MacKie RM. An aid to the preoperative assessment of
pigmented lesions of the skin. Br J Dermatol 1971;85:232-8.
31. Bahmer FA, Fritsch P, Kreusch J, Pehamberger H, Rohrer C,
Schindera I, et al. Diagnostische Kriterien in der Auflichtsmik-
roskopie. Konsensus-Treffen der Arbeitsgruppe Analytische
Morphologie der Arbeitsgemeinschaft Dermatologische For-
schung, 17November1989 inHamburg.Hautarzt 1990;41:513-4.
32. Argenziano G, Soyer HP, Chimenti S, Talamini R, Corona R, Sera
F, et al. Dermoscopy of pigmented skin lesions: results of
a consensus meeting via the Internet. J Am Acad Dermatol
2003;48:679-93.
33. Anderson RR, Parrish JA. The optics of human skin. J Invest
Dermatol 1981;77:13-9.
34. Braun RP, Saurat JH, Krischer J. Diagnostic pearl: unmagnified
diascopy for large pigmented lesions reveals features similar
to those of epiluminescence microscopy. J Am Acad Dermatol
1999;41:765-6.
35. Bahmer FA, Rohrer C. Rapid and simple macrophotography of
the skin. Br J Dermatol 1986;114:135-6.
36. Argenziano G, Soyer HP, De Giorgi V, Piccolo D, Carli P, Delfino
M, et al. Dermoscopy: a tutorial. 1st ed. Milano: EDRA; 2000.
37. Kenet RO, Kang S, Kenet BJ, Fitzpatrick TB, Sober AJ, Barnhill
RL. Clinical diagnosis of pigmented lesions using digital
epiluminescence microscopy. Grading protocol and atlas.
Arch Dermatol 1993;129:157-74.
38. Reisfeld PL. Blue in the skin. J Am Acad Dermatol 2000;42:
597-605.
39. Pehamberger H, Steiner A, Wolff K. In vivo epiluminescence
microscopy of pigmented skin lesions. I. Pattern analysis of
pigmented skin lesions. J Am Acad Dermatol 1987;17:571-83.
40. Krischer J, Skaria A, Guillod J, Lemonnier E, Salomon D, Braun
R, et al. Epiluminescent light microscopy of melanocytic
lesions after dermoepidermal split. Dermatology 1997;
195:108-11.
41. Massi D, De Giorgi V, Soyer HP. Histopathologic correlates of
dermoscopic criteria. Dermatol Clin 2001;19:259-68.
42. Soyer HP, Kenet RO, Wolf IH, Kenet BJ, Cerroni L. Clinicopath-
ological correlation of pigmented skin lesions using dermo-
scopy. Eur J Dermatol 2000;10:22-8.
43. Yadav S, Vossaert KA, Kopf AW, Silverman M, Grin-Jorgensen
C. Histopathologic correlates of structures seen on dermo-
scopy (epiluminescence microscopy). Am J Dermatopathol
1993;15:297-305.
44. Argenziano G, Fabbrocini G, Carli P, De Giorgi V, Sammarco E,
Delfino M. Epiluminescence microscopy for the diagnosis of
doubtful melanocytic skin lesions. Comparison of the ABCD
rule of dermatoscopy and a new 7-point checklist based on
pattern analysis. Arch Dermatol 1998;134:1563-70.
45. Nachbar F, Stolz W, Merkle T, Cognetta AB, Vogt T, Landthaler
M, et al. The ABCD rule of dermatoscopy: high prospective
value in the diagnosis of doubtful melanocytic skin lesions.
J Am Acad Dermatol 1994;30:551-9.
46. Soyer HP, Smolle J, Hodl S, Pachernegg H, Kerl H. Surface
microscopy: a new approach to the diagnosis of cutaneous
pigmented tumors. Am J Dermatopathol 1989;11:1-10.
47. Guillod JF, Skaria AM, Salomon D, Saurat JH. Epiluminescence
videomicroscopy: black dots and brown globules revisited by
stripping the stratum corneum. J Am Acad Dermatol
1997;36:371-7.
48. Kittler H, Seltenheim M, Dawid M, Pehamberger H, Wolff K,
Binder M. Frequency and characteristics of enlarging common
melanocytic nevi. Arch Dermatol 2000;136:316-20.
49. Menzies SW, Ingvar C, McCarthy WH. A sensitivity and
specificity analysis of the surface microscopy features of
invasive melanoma. Melanoma Res 1996;6:55-62.
50. Menzies SW, Crotty KA, McCarthy WH. The morphologic
criteria of the pseudopod in surface microscopy. Arch
Dermatol 1995;131:436-40.
51. Argenziano G, Scalvenzi M, Staibano S, Brunetti B, Piccolo D,
Delfino M, et al. Dermatoscopic pitfalls in differentiating
pigmented Spitz naevi from cutaneous melanomas. Br J
Dermatol 1999;141:788-93.
52. Argenziano G, Soyer HP, Ferrara G, Piccolo D, Hofmann-
Wellenhof R, Peris K, et al. Superficial black network: an
additional dermoscopic clue for the diagnosis of pigmented
spindle and/or epithelioid cell nevus. Dermatology 2001;
203:333-5.
53. Steiner A, Pehamberger H, Binder M, Wolff K. Pigmented Spitz
nevi: improvement of the diagnostic accuracy by epilumines-
cence microscopy. J Am Acad Dermatol 1992;27:697-701.
54. Massi D, De Giorgi V, Carli P, Santucci M. Diagnostic
significance of the blue hue in dermoscopy of melanocytic
lesions: a dermoscopic-pathologic study. Am J Dermatopathol
2001;23:463-9.
55. Kreusch J, Rassner G. Auflichtmikroskopie pigmentierter
Hauttumoren. Stuttgart: Thieme; 1991.
56. Kreusch J, Rassner G, Trahn C, Pietsch-Breitfeld B, Henke D,
Selbmann HK. Epiluminescent microscopy: a score of

J AM ACAD DERMATOL
JANUARY 2005
120 Braun et al
morphological features to identify malignant melanoma.
Pigment Cell Res 1992:295-8.
57. Kreusch J, Koch F. Auflichtmikroskopische Charakterisierung
von Gefassmustern in Hauttumoren. Hautarzt 1996;47:264-72.
58. Argenziano G, Fabbrocini G, Carli P, De Giorgi V, Delfino M.
Epiluminescence microscopy: criteria of cutaneous melanoma
progression. J Am Acad Dermatol 1997;37:68-74.
59. Argenziano G, Fabbrocini G, Carli P, De Giorgi V, Delfino M.
Clinical and dermatoscopic criteria for the preoperative
evaluation of cutaneous melanoma thickness. J Am Acad
Dermatol 1999;40:61-8.
60. Argenyi ZB. Dermoscopy (epiluminescence microscopy) of
pigmented skin lesions. Current status and evolving trends.
Dermatol Clin 1997;15:79-95.
61. Carli P, De Giorgi V, Soyer HP, Stante M, Mannone F, Giannotti
B. Dermatoscopy in the diagnosis of pigmented skin lesions:
a new semiology for the dermatologist. J Eur Acad Dermatol
Venereol 2000;14:353-69.
62. Steiner A, Pehamberger H, Wolff K. In vivo epiluminescence
microscopy of pigmented skin lesions. II. Diagnosis of small
pigmented skin lesions and early detection of malignant
melanoma. J Am Acad Dermatol 1987;17:584-91.
63. Braun RP, Rabinovitz H, Krischer J, Kreusch J, Oliviero M, Naldi
L, et al. Dermoscopy of pigmented seborrheic keratosis. Arch
Dermatol 2002;138:1556-60.
64. Provost N, Kopf AW, Rabinovitz HS, Oliviero MC, Toussaint S,
Kamino HH. Globulelike dermoscopic structures in pigmented
seborrheic keratosis. Arch Dermatol 1997;133:540-1.
65. Braun RP, Rabinovitz H, Oliviero M, Kopf AW, Saurat JH,
Thomas L. Dermatoscopy of pigmented lesions. Ann Dermatol
Venereol 2002;129:187-202.
66. Schiffner R, Schiffner-Rohe J, Vogt T, Landthaler M, Wlotzke U,
Cognetta AB, et al. Improvement of early recognition of
lentigo maligna using dermatoscopy. J Am Acad Dermatol
2000;42:25-32.
67. Menzies SW, Westerhoff K, Rabinovitz H, Kopf AW, McCarthy
WH, Katz B. Surface microscopy of pigmented basal cell
carcinoma. Arch Dermatol 2000;136:1012-6.
68. Soyer HP, Argenziano G, Ruocco V, Chimenti S. Dermoscopy of
pigmented skin lesions (Part II). Eur J Dermatol 2001;11:
483-98.
69. Wang SQ, Katz B, Rabinovitz H, Kopf AW, Oliviero M. Lessons
on dermoscopy #4. Poorly defined pigmented lesion. Di-
agnosis: pigmented BCC. Dermatol Surg 2000;26:605-6.
70. Stolz W, Riemann A, Cognetta AB, Pillet L, Abmayr W, Holzel D,
et al. ABCD rule of Dermatoscopy: a new practical method for
early recognition of malignant melanoma. Eur J Dermatol
1994;4:521-7.
71. Braun RP, Rabinovitz H, Oliviero M, Kopf AW, Saurat JH.
Pattern analysis: a two step procedure for the dermoscopic
diagnosis of melanoma. Clin Dermatol 2002;20:236-9.
72. Saida T, Oguchi S, Ishihara Y. In vivo observation of magnified
features of pigmented lesions on volar skin using video
macroscope. Usefulness of epiluminescence techniques in
clinical diagnosis. Arch Dermatol 1995;131:298-304.
73. Cognetta AB Jr, Stolz W, Katz B, Tullos J, Gossain S. Dermato-
scopy of lentigo maligna. Dermatol Clin 2001;19:307-18.
74. Kittler H, Seltenheim M, Pehamberger H, Wolff K, Binder M.
Diagnostic informativeness of compressed digital epilumines-
cence microscopy images of pigmented skin lesions com-
pared with photographs. Melanoma Res 1998;8:255-60.
75. Braun RP, Lemonnier E, Guillod J, Skaria A, Salomon D, Saurat
JH. Two types of pattern modification detected on the follow-
up of benign melanocytic skin lesions by digitized epilumi-
nescence microscopy. Melanoma Res 1998;8:431-7.
76. Kittler H, Pehamberger H, Wolff K, Binder M. Follow-up of
melanocytic skin lesions with digital epiluminescence micros-
copy: patterns of modifications observed in early melanoma,
atypical nevi, and common nevi. J Am Acad Dermatol
2000;43:467-76.
77. Menzies SW, Gutenev A, Avramidis M, Batrac A, McCarthy WH.
Short-termdigital surfacemicroscopicmonitoring of atypical or
changing melanocytic lesions. Arch Dermatol 2001;137:1583-9.
78. Stolz W, Schiffner R, Pillet L, Vogt T, Harms H, Schindewolf T,
et al. Improvement of monitoring of melanocytic skin lesions
with the use of a computerized acquisition and surveillance
unit with a skin surface microscopic television camera. J Am
Acad Dermatol 1996;35:202-7.
79. Binder M, Steiner A, Schwarz M, Knollmayer S, Wolff K,
Pehamberger H. Application of an artificial neural network in
epiluminescence microscopy pattern analysis of pigmented
skin lesions: a pilot study. Br J Dermatol 1994;130:460-5.
80. Binder M, Kittler H, Seeber A, Steiner A, Pehamberger H, Wolff
K. Epiluminescence microscopy-based classification of pig-
mented skin lesions using computerized image analysis and
an artificial neural network. Melanoma Res 1998;8:261-6.
81. Binder M, Kittler H, Dreiseitl S, Ganster H, Wolff K, Peham-
berger H. Computer-aided epiluminescence microscopy of
pigmented skin lesions: the value of clinical data for the
classification process. Melanoma Res 2000;10:556-61.
82. Day GR, Barbour RH. Automated melanoma diagnosis: where
are we at? Skin Res Technol 2000;6:1-5.
83. Debeir O, Decaestecker C, Pasteels JL, Salmon I, Kiss R, Van
Ham P. Computer-assisted analysis of epiluminescence mi-
croscopy images of pigmented skin lesions. Cytometry
1999;37:255-66.
84. Elbaum M, Kopf AW, Rabinovitz HS, Langley RG, Kamino H,
Mihm MC Jr, et al. Automatic differentiation of melanoma
from melanocytic nevi with multispectral digital dermoscopy:
a feasibility study. J Am Acad Dermatol 2001;44:207-18.
85. Fleming MG, Steger C, Zhang J, Gao J, Cognetta AB, Pollak I,
et al. Techniques for a structural analysis of dermatoscopic
imagery. Comput Med Imaging Graph 1998;22:375-89.
86. Gutenev A, Skladnev VN, Varvel D. Acquisition-time image
quality control in digital dermatoscopy of skin lesions. Comput
Med Imaging Graph 2001;25:495-9.
87. Gutkowicz-Krusin D, Elbaum M, Jacobs A, Keem S, Kopf AW,
Kamino H, et al. Precision of automatic measurements of
pigmented skin lesion parameters with a MelaFind(TM) mul-
tispectral digital dermoscope. Melanoma Res 2000;10:563-70.
88. Menzies SW. Automated epiluminescence microscopy: human
vs machine in the diagnosis of melanoma. Arch Dermatol
1999;135:1538-40.
89. Moncrieff M, Cotton S, Claridge E, Hall P. Spectrophotometric
intracutaneous analysis: a new technique for imaging pig-
mented skin lesions. Br J Dermatol 2002;146:448-57.
90. Murali A, Stoecker WV, Moss RH. Detection of solid pigment in
dermatoscopy images using texture analysis. Skin Res Technol
2000;6:193-8.
91. Rubegni P, Ferrari A, Cevenini G, Piccolo D, Burroni M, Perotti
R, et al. Differentiation between pigmented Spitz naevus and
melanoma by digital dermoscopy and stepwise logistic
discriminant analysis. Melanoma Res 2001;11:37-44.
92. Schmid P. Segmentation of digitized dermatoscopic images
by two-dimensional color clustering. IEEE Trans Med Imaging
1999;18:164-71.
93. Smolle J. Computer recognition of skin structures using
discriminant and cluster analysis. Skin Res Technol 2000;6:58-63.
94. Stoecker WV, Moss RH. Digital imaging in dermatology.
Comput Med Imaging Graph 1992;16:145-50.

J AM ACAD DERMATOL
VOLUME 52, NUMBER 1
Braun et al 121
95. Braun RP, Meier M, Pelloni F, Ramelet AA, Schilling M,
Tapernoux B, et al. Teledermatoscopy in Switzerland: a pre-
liminary evaluation. J Am Acad Dermatol 2000;42:770-5.
96. Piccolo D, Smolle J, Argenziano G, Wolf IH, Braun R, Cerroni L,
et al. Teledermoscopy—results of a multicentre study on 43
pigmented skin lesions. J Telemed Telecare 2000;6:132-7.
97. Piccolo D, Smolle J, Wolf IH, Peris K, Hofmann-Wellenhof R,
Dell’Eva G, et al. Face-to-face diagnosis vs telediagnosis of
pigmented skin tumors: a teledermoscopic study. Arch Der-
matol 1999;135:1467-71.
98. Provost N, Kopf AW, Rabinovitz HS, Stolz W, DeDavid M, Wasti
Q, et al. Comparison of conventional photographs and tele-
phonically transmitted compressed digitized images of mela-
nomas and dysplastic nevi. Dermatology 1998;196:299-304.
ADDITIONAL READING
1. Argenziano G, Soyer HP, De Giorgi V, Piccolo D, Carli P, et al.
Dermoscopy: A tutorial. 1st ed. Milan: EDRA; 2000.
2. Menzies SW, Crotty KA, Ingvar C, McCarthy WH. An atlas of
surface microscopy of pigmented lesions. Sydney: McGraw-Hill
Company; 1996.
3. Stolz W, Braun-Falco O, Bilek P, Landthaler M, Burgdorf WHC,
Cognetta AB. Color atlas of dermatoscopy. 2nd ed. Berlin:
Blackwell Wessenschafts-Verlag; 2002.
4. Soyer HP, Argenziano G, Chimenti S, Rabinovitz HS, Stolz W,
Kopf AW, et al. Dermoscopy of pigmented lesions. Milan: EDRA;
2001.
5. Rabinovitz HS, Cognetta AB. Dermatologic clinics. Philadelphia
(PA): WB Saunders; 2001.
6. Johr R, Soyer HP, Argenziano G, Hofmann-Wellenhof R,
Scalvenzi M. Dermoscopy: The essentials. London: Mosby; 2004.
8. Marghoob AA, Braun RP, Kopf AW. Atlas of dermoscopy.
London: Taylor & Francis; 2005.
9. Malvehy J, Puig S. Principles of dermoscopy. Barcelona: CEGE
Editors; 2002.