Embed Size (px)
Citation preview

Transplant Immunology 22 (2010) 110–114
Contents lists available at ScienceDirect
Transplant Immunology
j ourna l homepage: www.e lsev ie r.com/ locate / t r im
Detection of plasma cells, C4d deposits and donor-specific antibodies on sequentialgraft biopsies of renal transplant recipients with chronic dysfunction
Laurent Martin a,e,⁎, Céline Charon-Barra a, Olivier Bocrie e, Fredy Guignier b,e, Philippe D'Athis d,Guillaume Dautin b,e, Mathilde Funes de la Vega a, Eve Justrabo a,e, Gérard Rifle c,e, Christiane Mousson c,e
a Department of Pathology, PTB, 2 rue Angélique Ducoudray 21070 Dijon, Franceb Laboratory of Tissue Typing, Etablissement Français du Sang Bourgogne/Franche Comté, PTB, 2 rue Angélique Ducoudray 21070 Dijon, Francec Department of Nephrology-Intensive Care and Transplantation, University Hospital, 2 boulevard de Lattre de Tassigny 21034 Dijon, Franced Department of Biostatistic, School of Medicine, 7 boulevard Jeanne d'Arc 21079 Dijon, Francee IFR 100 Santé STIC, School of Medicine, 7 boulevard Jeanne d'Arc 21079 Dijon, France
⁎ Corresponding author. Service d'Anatomie PatholoDucoudray, 21070 Dijon Cedex, France. Tel.: +33 380 2
E-mail address: [email protected] (L. M
0966-3274/$ – see front matter © 2009 Elsevier B.V. Adoi:10.1016/j.trim.2009.11.001
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 4 August 2009Received in revised form 29 October 2009Accepted 2 November 2009Keywords:Kidney transplantationChronic allograft rejectionAnti-HLA antibodiesComplementC4d depositsPlasma cells
Background: In order to look for a relationship between humoral mechanisms of rejection and chronicallograft dysfunction, plasma cells, C4d deposits and donor-specific antibodies (DSA) were simultaneouslysought on serial biopsies of kidney allograft recipients.Patients and methods: Ten recipients with chronic dysfunction (G1) and 8 recipients with long-term normalgraft function (G2) were included. Biopsies and serums were sampled at early graft dysfunction (T1),between 8 months and 2 years (T2) and after the third year following transplantation (T3).Results: In G1, plasma cells represented 12.3% (T1), 8.2% (T2) and 14.1% (T3) of mononuclear cells. The meanpercentage of plasma cells was 11.6% in G1 versus 0.4% in G2 (pb0.05). A progressive rise in C4d depositswas seen in G1, from 25% at T1 to 80% at T3. Donor-specific antibodies were identified in at least one serumsample of 60% of the patients in G1 and 12.5% of the patients in G2 (p=0.012), whereas donor-specificantibodies were eluted from at least one biopsy of 50% of the patients in G1 and 12.5% of the patients in G2
(p=0.03). In G1, C4d deposits were significantly associated with plasma cells (p=0.0012) and anti-HLA Absin serum samples and/or eluates (p=0.026).Conclusion: This study shows that plasma cells, DSA and C4d are associated in renal transplants developingchronic rejection.© 2009 Elsevier B.V. All rights reserved.
1. Introduction
The role of the humoral immune response occurring after kidneytransplantation has long been underestimated. Nevertheless, the latestmeetings in Banff have updated this point: acute humoral rejectionwasintroduced in 2001 [1] and chronic humoral rejection in 2005 [2]. In fact,increasing evidence suggests that allo and even autoantibodies couldplay a significant role in the development of chronic allograft rejection[3–5]. Donor-specific antibodies (DSA) and C4d deposits alongperitubular capillaries (CPT) are looked upon as the gold standard foridentification of donor-specific humoral response after kidney trans-plantation. Acutehumoral lesions include glomerulitis, capillaritis, acutetubular necrosis and/or fibrinoid necrosis of the wall of arteries, whichcould lead to interstitial fibrosis/tubular atrophy (IF/TA), capillary lossand/or transplant glomerulopathy. The antibodies are produced byplasma cells located mainly in the bone marrow and/or in lymphoid
gique, PTB, 2, rue Angélique95 714; fax: +33 380 295 717.artin).
ll rights reserved.
organs [6]. These cells can also reach inflammatory sites or could beproduced in situ by cells originating from tertiary lymphoid follicles [7].
2. Objective
Previousreportssuggest that themainactorsof thehumoralalloimmuneresponse, especially DSA, could be preferentially found in the graft ratherthan in the circulation [5,8], suggesting that testing for antibodies in serumsamples alone underestimates their frequency. Therefore, we haveconducted a retrospective study in order to look for a relationship betweentissue and blood markers of a humoral immune response, i.e. plasma cells,C4d deposits and DSA in serial serums and eluates from recipientsexperiencing chronic allograft dysfunction and/or late graft loss.
3. Material and methods
3.1. Patients
Eighteen kidney allograft recipients were included in this retro-spective study because they had simultaneous sequential transplant

Table 1Time after grafting (months) and serum creatinine level (mg/l) at sampling for patientsof group 1 with chronic dysfunction and patients of group 2 without graft dysfunction.
Group 1 (n=10) Group 2 (n=8) p
Time after grafting (T1) 2.84±1.86 4.24±5.78 nsAvailable serum 9 5Available biopsies (frozen) 8 (4) 5 (4)Serum creatinine level (mg/l) 17.5±5.83 19.6±10.6⁎ ns
Time after grafting (T2) 12.7±2.8 19.7±6.34 nsAvailable serum 10 5Available biopsies (frozen) 10 (6) 7 (4)Serum creatinine level (mg/l) 17.8±8.1 11.3±2.72 0.031
Time after grafting (T3) 50.7±27.2 62.8±21.1 nsAvailable serum 10 5Available biopsies (frozen) 10 (10) 5 (5)Serum creatinine level (mg/l) 25.5±14.1 10.7±2.59 0.032
Samples (biopsies of the transplants and serum) were taken before the 6th month (T1),between 8 months and 2 years (T2) and after the third year (T3). p values marked as“ns” are not significant. Data in bold correspond to groups 1 to 8 biopsies of thetransplant and samples from 2 transplantectomies and in groups 2 to 5 biopsies of thetransplant.*Only two recipients had early allograft dysfunction.
111L. Martin et al. / Transplant Immunology 22 (2010) 110–114
biopsieswith orwithout final graft removal and investigations for DSAboth in serum samples and in transplant biopsies. All patients receivedkidney transplants from deceased donors. In all cases, the immuno-suppressive protocol included induction therapy with anti-thymocyteglobulins (Sangstat, Lyon, France), and either a conventional double-therapy regimen with prednisone and azathioprine (Aza) or a triple-therapy regimen that consisted of ciclosporine or tacrolimus, predni-sone and Aza or mycophenolate mofetil (MMF). Acute rejections (AR)were defined as an increase in serum creatinine level of at least 50%and/or a decrease in glomerularfiltration rate of at least 25% associatedwith lesions on transplant biopsies consistent with rejection. Acutehumoral rejection was diagnosed when the following criteria wereencountered: diffuse C4d deposits and DSA in the blood sample and/orin an eluate of the transplant biopsy. All AR were treated withmethylprednisolone pulses. Steroid resistant AR episodes wererescued with OKT3® and/or plasma exchange and cyclophosphamidein resistant AHR. Clinical data on patients were obtained by reviewingmedical records. Data gathered included donor and recipient char-acteristics (age at transplantation, gender, HLA typing, and PanelReactive Abs before grafting) and post-transplantation data (delayedgraft function, AR, cytomegalovirus infection, high blood pressure,time from transplantation to sampling, serum creatinine level atsampling, and immunosuppressive drugs). During the follow-up,protocol biopsies were performed at around 1, 2 and 4 years post-transplant; in addition biopsies by cause were performed whenrequired; heavy proteinuria, acute or progressive renal failure, andsuspicion of recurrence of initial nephropathy.
According to clinical and pathological data, patients were dividedinto two groups: patients with progressive impairment of renalfunction (group 1, n=10) and patients with normal renal function,i.e. creatinine clearance ≥60 ml/mn−1/1.73 m2 and proteinuria≤0.5 g/day (group 2, n=8). All recipients were followed for atleast one year after transplantation (range: 17 to 145 months; mean:61.6±37.7 months). During the follow-up, transplant biopsies wereeither protocol biopsies or biopsies for acute or progressiveworsening of renal function. Biopsies were performed before the6th month in all cases for dysfunction (early samples, T1), withineight months and 2 years (intermediate samples, T2) and after thethird year after grafting (late samples, T3). For T2 and T3 samples,biopsies included in the study were never performed for acuteworsening of renal function, but sometimes they were performedslightly earlier than the time provided for protocol biopsy, because ofa decrease in renal function or increasing proteinuria. Some protocolbiopsies are missing because the material was inadequate or thepatient refused. Serum samples were collected at the time oftransplant biopsies and/or at least once a year. Biopsies (frozen andformalin-fixed) and serum samples available at each time point aresummarized in Table 1. In addition, 2 transplants removed 35 and51 months after transplantation in group 1were used as late biopsies.
3.2. Methods
3.2.1. Pathological evaluationThe biopsies were fixed in Dubosq-Brazil and paraffin embedded
for routine light microscopic evaluation. Serial sections were preparedand stained with hematoxylin, eosin and saffron, periodic acid Schiff,methanamine silver and trichrome stains. Lesions were gradedaccording to the latest Banff classification [1,2]. To determine theproportion of plasma cells, infiltrating mononuclear cells werecounted by two expert pathologists (LM and MFV) in serial fields athigh magnification with an optical grid on hematoxylin eosin andsaffron stain. At least five hundredmononucleated cells were counted.Routine immunofluorescence studies were performed only on frozensections by using polyclonal Abs (Dako, Glostrup, Denmark) to α(Dako F0204, 1/20), γ (Dako F0202, 1/30) and μ (Dako F0203, 1/30)heavy chains, C1q (Dako F0251, 1/50), C3 (Dako F0201, 1/50), C4
(Dako F0169, 1/20), fibrinogen (Dako F0111, 1/20) and albumin(Dako F0117, 1/20). C4d (Quidel, A213, 1/100, Santa Clara, CA) wasdetected with an indirect immunofluorescence technique in allavailable frozen biopsies. Sections were scored at high magnification(×400) for staining in PTC without knowledge of the clinical andpathological data. Sections of acute humoral rejection with diffusedeposits of C4d on PTC and DSA in the serum were used as positivecontrol.
3.2.2. Screening and identification of donor-specific antibodies in eluatesand serums
Antibodies were isolated from available frozen transplant biopsies,including transplantectomies, with a commercial acid elution kit(ELUKIT II, Gamma Biochemicals Inc., Houston TX) according to apreviously described protocol [8–10]. Briefly, each biopsywas washedand minced, the 1000 g sediment was eluted with the solution ofelution at room temperature for 15 min and the supernate wasremoved and neutralized with buffer solution before testing. Class Iand class II anti-HLA Abs were detected in eluates and serums withFlowPRA beads (FL12-60, One Lambda Canoga Park, CA) as previouslydescribed [8]. The specificity of anti-HLA Abs was assessed withFlowPRA beads coated with specific class I or class II HLA antigens(FL1-SP and FL2-SP, One Lambda Canoga Park, CA). When thespecificity of anti-HLA Abs could not be assigned with the FlowPRAtest, flow cytometric cross-match (Xm) was performed in duplicatewith donor lymphocytes using a three-color fluorescence technique toconfirm the donor specificity [11].
3.2.3. Statistical analysisStatistical analysis was conducted with TRIOMPHE software
developed at the Biostatistics Department of Dijon UniversityHospital taking into account the fact that the series of samples wassmall and incomplete: quantitative data were studied with theMann–Whitney test and qualitative data with Fisher's exact test. Theresults were considered significant if the degree of significancesatisfied pb0.05.
4. Results
4.1. Patients and samples
Time from transplantation to sampling and serum creatinine level at sampling areshown in Table 1. Forty-four formalin-fixed biopsies and 33 frozen biopsies, including 2samples coming from transplantectomies, were analysed. The cortex and the medullawere represented in only 7 frozen biopsies (21%). The characteristics of donors,recipients and post-transplantation events were not statistically different between

Table 2Pre- and post-transplant characteristics of recipients of groups 1 with late chronicdysfunction and recipients of group 2 without dysfunction of the graft.
Group 1 (n=10) Group 2 (n=8) p
Pre-transplant characteristicsGender (donor) (M/F) 7/3 6/2 nsAge (recipient) 50.3±3.58 54.4±2.22 nsGender (recipient) (M/F) 8/2 3/5 nsNephropathy (GN/PK/others) 2/3/5 3/2/3 nsPRA (%) 8.2±14.3 23.3±41.2 nshemodialysis time (months) 16.5±10.6 40.5±33.6 0.002Cold ischemia time (h) 27.8±6.5 27.1±12.1 ns
Post-transplant characteristicsFollow-up (months) 50.7±27.2 62.3±21.1 nsDelayed graft function 2/10 (20%) 2/8 (25%) nsEarly graft dysfunction (AR) 9/10 (6) 3/8 (2) 0.038CMV infection 3/10 (30%) 1/8 (12.5%) nsHigh blood pressure 7/10 (70%) 5/8 (62.5%) nsHypercholesterolemia 3/10 (30%) 3/8 (37.5%) ns
PRAmeans Panel Reactive Antibodies (percentage of positive cells). AR: acute rejection,GN: glomerulonephritis, PK: dominant polycystic kidney disease. p values marked as“ns” are not significant.
112 L. Martin et al. / Transplant Immunology 22 (2010) 110–114
groups, except for a longer duration of hemodialysis in group 2 and a higher incidenceof AR in group 1 (Table 2).
4.2. Pathological data
4.2.1. IF/TANo IF/TA was seen on early biopsies in both groups or in intermediate and late
biopsies in group 2. In group 1, intermediate transplant biopsies showed IF/TA in 4cases (40%), one being associated with de novo membranous glomerulonephritis. Latebiopsies of 8 still functioning grafts and transplantectomies from the 2 other recipientsshowed extensive IF/TA. In 8 cases, C4d deposits along peritubular capillaries and/orDSA associated with IF/TA indicated a humoral chronic rejection.
4.2.2. Acute rejectionEarly renal allograft dysfunction occurred in 9 out of 10 recipients in group 1 and 3
out of 8 recipients in group 2. According to the Banff classification, 6 biopsies in group 1,and 2 biopsies in group 2 showed lymphocyte-mediated AR (type 1A or 1B) orborderline lesions. In 1 case in group 1, the association of C4d deposits with lymphocyteinfiltrate was in favour of a humoral component in the rejection process. No acutelymphocyte-mediated vascular rejections or acute humoral rejections were detected.
4.2.3. Plasma cellsIn early biopsies, plasma cells (Fig. 1) were associated with borderline lesions and
lymphocyte-mediated rejection (mean proportion of inflammatory cells: 12.4% ingroup 1 versus 0.4% in group 2). Plasma cells were seen in 5 intermediate biopsies fromgroup 1 (8.2% of inflammatory cells), showing IF/TA (n=4) or AR (n=1). Two
Fig. 1. Plasma cell-rich infiltrate on an intermediate transplant biopsy of a recipientfrom group 1. Plasma cells are located in the connective tissue and are not dysmorphic(HES).
intermediate biopsies from group 2 also had few plasma cells (0.7% of inflammatorycells). Plasma cells were detected in 8 late biopsies from group 1 (14.1% ofinflammatory cells) and two late biopsies from group 2 (0.2% of inflammatory cells).The mean proportion of plasma cells seen on biopsies from group 1 was 11.6% (range 0to 53.9% of inflammatory cells) whereas the proportion of these cells was always b2%on biopsies in group 2. In group 1, the median proportion of plasma cells on biopsieswas 6.5% of mononuclear inflammatory cells. Eight recipients in group 1 had at leastone biopsy with a higher proportion of plasma cells.
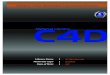
4.2.4. C4dIn group 1, C4d was detected in 25% of early biopsies (1/4 frozen biopsies), in 60%
(3/5 frozen biopsies) of intermediate biopsies and 80% (8/10 frozen biopsies) of latebiopsies (Fig. 2). No C4d deposits were seen at any time on biopsies from group 2. Onlyone case with de novo membranous glomerulopathy showed significant deposits ofother complement components or immunoglobulins.
4.3. Donor-specific antibodies in eluates and serums
In group 1, DSA were detected in 11% of early serums (1/9), in 60% of intermediateserums (6/10) and 10% of late serums (1/10). Anti-HLA Abs were detected in 8/10 lateeluates from group 1 but their donor specificity could be assigned in only five cases. Inthe other three cases, donor lymphocytes were not available.
DSA were eluted from only one early frozen biopsy of one recipient in group 2 whoexperienced early allograft dysfunction with borderline acute rejection. No anti-HLAAbs were found in any other serums or eluates from group 2.
4.4. Association of plasma cells, C4d and DSA
Among the 8 recipients in group 1 with plasma cells on their biopsies, 6 had C4ddeposits and/or DSA after grafting. The last two patients had no C4d deposits or anti-HLA Abs. Two recipients with DSA and/or C4d deposits had fewer than 6.5% of plasmacells on their biopsies. In late samples, all biopsies with more than 6.5% of plasma cellsamong infiltrating mononuclear cells had C4d deposits and anti-HLA Abs in the eluates.In group 1, diffuse deposits of C4d on peritubular capillaries were significantlyassociated with plasma cells (p=0.0012) and anti-HLA Abs in the serum samples and/or eluates (p=0.026). In total, six recipients of group 1 had plasma cell on at least onetransplant biopsy associated with C4d deposits and/or DSA. Two other recipients ingroup 1 showed C4d and/or DSA without plasma cell-rich infiltrate. Plasma cellsdetected on the transplant biopsies of the last 2 recipients were not associated with C4dor DSA. No statistical relationship between items of the Banff schema (tubulitis,inflammation, and glomerulitis) and plasma cells, C4d or anti-HLA Abs was found.Table 3 summarizes the results in groups 1 and 2.
5. Discussion
This retrospective and longitudinal study was limited to threeparameters potentially involved in humoral response after kidneytransplantation. Plasma cells, diffuse C4d staining of PTC and DSAwere detected on serial biopsies of recipients with chronic dysfunc-tion and compared to a control group with normal renal function.
Fig. 2. Diffuse linear deposits of C4d on peritubular capillaries seen on an intermediatetransplant biopsy of a recipient from group 1.

Table 3Plasma cells, C4d, anti-HLA antibodies and donor-specific antibodies at each time pointin samples from recipients of group 1 with chronic dysfunction and recipients of group2 with minimal changes and normal long-term graft function.
Group 1 (n=10) Group 2 (n=8) p
% of plasma cells(number of positive cases)T1 12.4 (6/8) 0.4 (1/4) b0.05T2 8.2 (6/9) 0.7 (2/5)T3 14.1 (8/10) 0.3 (2/5)
C4d positive casesT1 ¼ (25%) 0/4 (0%) 0.012T2 3/5 (60%) 0/3 (0%)T3 8/10 (80%) 0/5 (0%)
Anti-HLA positive eluatesT1 (DSA) 0/4 (0/4) 2/4 (1/4) 0.03T2 (DSA) 0/5 (0/5) 0/3 (0/3)T3 (DSA) 8/10 (5/10) 2/5 (0/5)
Anti-HLA positive serumsT1 (DSA) 2/9 (1/9) 0/3 (0/3) 0.012T2 (DSA) 6/10 (6/10) 0/8 (0/8)T3 (DSA) 5/10 (1/10) 0/8 (0/8)
Anti-HLA positive cases 8/10 (80%) 1/8 (12.5%) 0.036T1 (DSA) 3/9 (1/9) 2/8 (1/8)T2 (DSA) 6/10 (6/10) 0/8 (0/8)T3 (DSA) 8/10 (7/10) 2/8 (0/8)
113L. Martin et al. / Transplant Immunology 22 (2010) 110–114
Today, diffuse C4d staining of PTC on transplant biopsies isregarded as a reliable marker of acute and chronic humoral responses[12–17]. C4d and more recently C3d deposits have been shown to bein situ markers of complement activation and are poor predictorfactors of graft survival [18,19]. In our study, diffuse and linear C4ddeposits on PTC were only seen in recipients developing further IF/TA.Moreover, the percentage of C4d positive biopsies in group 1progressively increased over time to reach 80% in the last period offollow-up when all patients had extensive IF/TA. The humoralcomponent associated with AR detected on early biospies is probablyunderestimated because C4d staining could not be performed for allpatients.
Detection of plasma cells among infiltrating mononuclear cells isnot common during rejection. Plasma cell-rich acute rejection hasalready been reported and seems to be related to a poor prognosis[20–23], but the persistent presence of plasma cells among infiltratingmononuclear cells on serial kidney transplant biopsies has never beenreported. Recently, Xu et al., in an analysis of 40 explanted grafts,found that 57.5% of the grafts had CD138+ plasma cells and 32.5% hadboth CD138+ plasma cells and diffuse C4d deposits [24]. C4ddeposition and CD138+ plasma cell infiltrate were statisticallyrelated (p=0.038). These data suggest that plasma cells can bepresent in kidney transplants in the absence of acute rejectionepisodes and associated with chronic allograft damage. In our study, ifwe consider the median proportion of plasma cells in biopsies ofgroup 1 (i.e.: 6.5%), 8 recipients had at least one biopsy with a highernumber of plasma cells. Early transplant biopsies with plasma cellsshowed mainly lymphocyte-mediated AR or borderline lesions, andlater IF/TA with C4d deposits in 8 cases, which is indicative of chronichumoral rejection. In these recipients, the percentage of plasma cellsremained constant on intermediate and late biopsies. In contrast, ingroup 2, there were few inflammatory cells on transplant biopsies andthe mean proportion of plasma cells was always less than 1%. At thethree time points, the average proportion of plasma cells was higheron the biopsies in group 1 than in group 2, suggesting that these cellsplay a role in the physiopathology of chronic humoral rejection. Thesignificant association of plasma cells with C4d deposits and anti-HLAAbs suggests that intra-graft plasma cells might be a source of Abs.This hypothesis is corroborated in animal models, by the demonstra-tion of the possible production of donor-specific anti-MHC Abs by
plasma cells in the graft [7]. However, studies of the expression of Bcell-associated transcripts and immunoglobulin transcripts in renalallograft biopsies suggest that B cells and plasma cells could berecruited/retained in allografts as a non-specific feature of inflamma-tion rather than part of the alloimmune response and depend on thetime of the biopsy [25]. This study was based on biopsies for cause. Itwas not related to DSA and did not concern sequential biopsies.
Flow cytometry was chosen to detect and identify IgG anti-HLAAbs because it is a sensitive method that, unlike complementdependent cytotoxic assay, does not require complement fixation.The use of beads coated with specific class I or class II HLA antigensrules out the fixation of autoantibodies and makes it possible todetermine the specificity of anti-HLA Abs in the same test.Furthermore, as the volumes of elution were extremely low (lessthan 100 µl), other sensitive and modern methods like ELISA assaycould not be used because eluate volumes were not large enough. In aprevious study [8], DSA were eluted from 60 to 70% of renaltransplants removed after irreversible graft failure. However, wecould not determine whether or not DSA fixed onto the transplant atthe time of transplantectomy were the cause, the consequence or acofactor of IF/TA [26]. In this trial, 70% of group 1 patients had anti-HLA in serum or eluates whereas only 12.5% of group 2 patients hadsuch Abs. This significant difference between the two groups is inagreement with other studies in the kidney, lung, liver, heart andcornea grafts [4,5,27]. The low rate of detection of DSA in our eluatescould be explained, in part, by the absence of medulla in a majority ofthe biopsies [10]. The identification of IgG DSA in our eluates and/orserum samples corroborates previous studies, which found aprevalence of IgG-producing plasma cells in chronic rejection [28]or plasma cell-rich acute rejection [20]. The statistically significantrelationship between C4d deposits on PTC and DSA in serum samplesobserved in this study was also mentioned by Mauiyyedi et al. [17]: itsuggests that anti-HLA Abs may be the cause of the activation of thecomplement pathway in the microcirculation of kidney transplantsleading to capillary loss. It is also noticeable that one recipient ofgroup 2 had DSA in the early eluate. Complete recovery was observedafter treatment of the rejection episode. We still do not know whysuch Abs are not deleterious for the graft. They might be inhibited byeither anti-idiotypic Abs [29], graft released soluble antigens [30] oraccommodation [31].
In conclusion, with the caution justified by the limited number ofpatients included in this preliminary report, our study supports thefact that humoral markers increase over time in renal transplantsduring chronic rejection [2] and shows a relationship between in situactors of humoral response: plasma cells, C4d deposits and donor-specific anti-HLA antibodies. It does not rule out the possibility thatantibodies to other antigens may be implicated in such a process [5].The detection of plasma cells on early biopsies (more than 6.5% ofmononucleated cells in our study) with lymphocyte-mediatedrejection (borderline or type 1) may be predictive of furtheroccurrence of IF/TA even though no C4d deposits or DSA are initiallypresent. These results must be confirmed by further studies involvingof greater number of patients. Thus, the detection of plasma cells onearly transplant biopsies, in the absence of pathology-producingtissue plasmocytosis, could lead to modifications in the immunosup-pressive regimen to include drugs that inhibit the B cell response inorder to limit IF/TA and prolong graft survival [32–35].
Acknowledgements
We thankMartine Rondeau, Nadine Rodet, Jeanne-Lise Heydenreichand Sébastien Rudier for their expert technical assistance in flowcytometric assays and Martine Goiset for her secretarial assistance incompiling this manuscript.
This work was supported in part by a grant from the FondationTransplantation (Strasbourg, France).

114 L. Martin et al. / Transplant Immunology 22 (2010) 110–114
References
[1] Racusen LC, Colvin RB, Solez K, Mihatsch MJ, Halloran PF, Campbell PM, et al.Antibody-mediated rejection criteria— an addition to the Banff 97 classification ofrenal allograft rejection. Am J Transplant 2003;3:708–14.
[2] Solez K, Colvin RB, Racusen LC, Sis B, Halloran PF, Birk PE, et al. Banff '05 meetingreport: differential diagnosis of chronic allograft injury and elimination of chronicallograft nephropathy (‘CAN’). Am J Transplant 2007;7:518–26.
[3] McKenna RM, Takemoto S, Terasaki PI. Anti-HLA antibodies after solid organtransplantation. Transplantation 2000;69:319–26.
[4] Terasaki PI. Humoral theory of transplantation. Am J Transplant 2003;3:665–73.[5] Rifle G, Mousson C, Martin L, Guignier F, Hajji K. Donor-specific antibodies in
allograft rejection: clinical and experimental data. Transplantation 2005;79:S14–8.
[6] Stegall MD, Dean PG, Gloor J. Mechanisms of alloantibody production in sensitizedrenal allograft recipients. Am J Transplant 2009;9:998–1005.
[7] Thaunat O, Field AC, Dai J, Louedec L, Patey N, BlochMF, et al. Lymphoid neogenesisin chronic rejection: evidence for a local humoral alloimmune response. Proc NatlAcad Sc USA 2005;102:14723–8.
[8] Martin L, Guignier F, Mousson C, Rageot D, Justrabo E, Rifle G. Detection of donor-specific anti-HLA antibodies with flow cytometry in eluates and serums from renaltransplant recipients with chronic allograft nephropathy. Transplantation 2003;76:395–400.
[9] Martin L, Guignier F, Bocrie O, D'Athis P, Rageot D, Rifle G, et al. Detection of anti-HLA antibodies by flow cytometry in eluates from needle core biopsies of renaltransplant recipients with chronic allograft nephropathy. Transplantation 2005;79:1459–61.
[10] Bocrie O, Hussein Aly AA, Guignier F, Funes de la Vega M, Rifle G, Mousson C, et al.Distribution of donor-specific antibodies in the cortex and the medulla of renaltransplants with chronic allograft nephropathy. Transplant Immunol 2007;17:227–9.
[11] Bray RA. Flow cytometry cross-matching for solid organ transplantation. MethodsCell Biol 1994;41:103–19.
[12] Feucht HE, Felbert E, Gokel MJ, Hillebrand G, Nattermann U, Brockmeyer C, et al.Vascular deposition of complement—split products in kidney allografts with cell-mediated rejection. Clin Exp Immunol 1991;86:464–70.
[13] Feucht HE, Schneeberg H, Hillebrand G, Burkhardt K, Weiss M, Riethmuller G, et al.Capillary deposition of C4d complement fragment and early renal graft loss.Kidney Int 1993;43:1333–8.
[14] Collins AB, Schneeberger EE, Pascual MA, Saidman SL, Williams WW, Tolkoff-Rubin N, et al. Complement activation in acute humoral renal allograft rejection:diagnostic significance of C4d deposits in peritubular capillaries. J Am Soc Nephrol1999;10:2208–14.
[15] Crespo M, Pascual M, Tolkoff-Rubin N, Mauiyyedi S, Collins AB, Fitzpatrick D, et al.Acute humoral rejection in renal allograft recipients. I. Incidence, serology andclinical characteristics. Transplantation 2001;71:652–8.
[16] Mauiyyedi S, CrespoM, Collins AB, Schneeberger EE, Pascual MA, Saidman SL, et al.Acute humoral rejection in kidney transplantation: II. morphology, immunopa-thology and pathologic classification. J Am Soc Nephrol 2002;13:779–87.
[17] Mauiyyedi S, Della Pelle P, Saidman A, Collins AB, Pascual M, Tolkoff-Rubin NE, et al.Chronichumoral rejection: identificationof antibody-mediated chronic renal allograftrejection by C4d deposits in peritubular capillaries. J Am Soc Nephrol 2001;12:574–82.
[18] Herzenberg AM, Gill JS, Djurdjev O, Magil AB. C4d deposition in acute rejection:an independent long-term prognostic factor. J Am Soc Nephrol 2002;13:234–41.
[19] Kuypers DR, Lerut E, Evenepoel P, Maes B, Vanrenterghem Y, Van Damme B. C3ddeposition in peritubular capillaries indicates a variant of acute renal allograftrejection characterized by aworse clinical outcome. Transplantation 2003;76:102–8.
[20] Charney DA, Nadasdy T, Lo WH, Racusen LC. Plasma cell-rich acute renal allograftrejection. Transplantation 1999;68:791–7.
[21] Meehan SM, Domer P, Josephson M, Donoghue M, Sadhu A, Ho LT, et al. Theclinical and pathologic implications of plasmacytic infiltrates in percutaneousrenal allograft biopsies. Hum Pathol 2001;32:205–15.
[22] Desvaux D, Le Gouvello S, Pastural M, Abtahi M, Suberbielle C, Boeri N, et al. Acuterenal allograft rejections with major-interstitial oedema and plasma cell-richinfiltrates: high gamma-interferon expression and poor clinical outcome. NephrolDial Transplant 2004;19:933–9.
[23] Gartner V, Eigentler TK, Viebhan R. Plasma cell-rich rejection processes in renaltransplantation: morphology and prognostic relevance. Transplantation 2006;81:986–91.
[24] Xu X, Shi B, Cai M, Han Y, Wang Q, Xu L, et al. A retrospective study of plasma cellinfiltrates in explanted renal allografts. Transplant Proc 2008;40:1366–70.
[25] Einecke G, Reeve J, Mengel M, Sis B, Bunnag S, Mueller TF, Halloran PF. Expressionof B cell and immunoglobulin transcripts is a feature of inflammation in lateallografts. Am J Transplant 2008;8:1434–43.
[26] Cramer DV, Shirwan H. The importance of humoral immune responses in chronicrejection. Transplantation Rev 1998;12:166–76.
[27] Lachmann N, Terasaki P, Budde K, Liefeldt L, Kalh A, Reinke P, et al. Anti-humanleukocyte antigen and donor-specific antibodies detected by luminex post-transplant serve as biomarkers for chronic rejection of renal allografts.Transplantation 2009;87:1505–13.
[28] Nadasdy T, Krenacs T, Kalmar KN, Csajbok E, Boda K, Ormos J. Importance ofplasma cells in the infiltrate of renal allografts. An immunohistochemical study.Pathol Res Pract 1991;187:178–83.
[29] Suciu-Foca N, Reed E, D'Agati VD, Ho E, Cohen DJ, Benvenisty AI, et al. Soluble HLAantigens, anti-HLA antibodies, and antiidiotypic antibodies in the circulation ofrenal transplant recipients. Transplantation 1991;51:593–601.
[30] Piazza A, Torlone N, Valeri M, Poggi E, Monaco PI, Provenzani L, et al. Antidonor-HLA antibodies and soluble HLA antigens after kidney transplant. Transplant Proc1993;25:3279–80.
[31] Jindra PT, Zhang X, Mulder A, Claas F, Veale J, Jin YP, et al. Anti-HLA antibodies caninduce endothelial cell survival or proliferation depending on their concentration.Transplantation 2006;82:S33–5.
[32] Theruvath TP, Saidman SL, Mauiyyedi S, Delmonico FL, Williams WW, Tolkoff-Rubin N, et al. Control of anti-donor antibody production with tacrolimus andmycophenolate mofetil in renal allograft recipients with chronic rejection.Transplantation 2001;72:77–83.
[33] Nickeleit V, Zeiler M, Gudat F, Thiel G, Mihatsch MJ. Detection of the complementdegradation product C4d in renal allografts: diagnostic and therapeutic implica-tions. J Am Soc Nephrol 2002;13:242–51.
[34] Snanoudj R, Beaudreuil S, Arzouk N, de Preneuf H, Durrbach A, Charpentier B.Immunological strategies targeting B cells inorgan grafting. Transplantation 2005;79:S33–6.
[35] Everly MJ, Everly JJ, Susskind B, Brailey P, Arend LJ, Alloway RR, et al. Bortezomibprovides effective therapy for antibody- and cell-mediated acute rejection.Transplantation 2008;86:1754–61.