Embed Size (px)
Citation preview

Acta Medica Scandinavica. Vol. CXXII, fasc. I. 1945.
Determination of Vitamin B1 in the Blood from Healthy and Diseased Persons.
The Phycomyces Method.
I ~ E T E H M I X A T I O N OF V I T A M I N I N THE D1,OOD F R O M l I E . \ L T H Y E T C . 39
however, b w n difficult to develop, since the concentration of vita- min n, in the body fluids is so small. Several chemical methods have nevertheless bcen drvcloped for this purpose - but nearly all of thcni arc encumbered with so many errors, or are so difficult to carry out, that so far the data collected have kleen very lirnittd. It is especially difficult to detern-ine the vitamin R, content of the blood; less difficult is the deterruination in urine which, therefore, has boon subject t o nunirrous investigations tha t have furnished considerable inforniation regarding the vitamin I$ excretion.
IVhen ~e are tlenliny \vith sueh small amounts of substance, a biological assay - assuming i t has t h e necessary sensitivity and specificity - should he more advantageous than chemical melhods. M’hcn Schopfer and Jung (1937) inli.oductd the Phycomyces me- thod it found widespread use in the invcstigation of the vitainin B, co!itent of Ihc blood.
The author of the present paper decided to investigate further what one might -expect from this inctliod [Rang (1045)l and, more- ov(’r, on thv basis of a relatively largc material to gain some infor- niation regarding the actual vitainin U, contcnt of the blood in healthy and direased persons.
The most i m l m t a n t result of thc critical exainination of the nicthod was that blood was fount1 to kontain other substances besides vitamin B, \vliich influence tho growth of Phycomyces- substances for which i t so far had hen impossible to develop a satis- factory met hod of corrcction. Several attempts (Hang 1942, 1944) gave uncertain, others (Sinclnir 1939) erroneous rcsults.
The data obtained by the I’hycomyces method should therefore be accepted n.i th considerable reservation. H o w v t ~ r , tlierc arr sevcrnl favourablc facts tha t must not be ignored:
1) Vitamin 13, is a grontli-proinoting substance for Phyconiyccs. 2) Exwpt ing biotin, no other known growth substances sewn
to influence t h c growth of I’hycomyces. 3) T h c constitutional specificity of vitamin B, in the case of
I’hycomyccs is considerable. 4) I-sperinicnts on animals have shown t h a t thc vitamin R,
contcnt of t he blood and of the organs is considcrablylo\~eriri B,- avitaiitinolic anirrials than in normal animals [Schopfer and Jung (1938), hlciklejohn (1937). c lc . ]
4 0 11. 0. n . \ \ c ;
.-I) Clinical data include several observations o f lo\\ vitainin Bl values, determined by the Phycomyces neth hod, accompanying clinically niaiiifest vitamin HI deficiency (Laitrent and Sin- clair (1938), Lehniann and Sielsen (1939), Pannckoek-jl’estcn- burg and van Vecn (1940), Sinclair (1 WI), Odin and Ixhinann
6) The vitamin R, values in blood found by the prcscnt and by other investigators, using the Phycomyces method, show good agrocincnt with values found by other methods. One may espe- cially point lo the agreemrnt between rcsults obtained by the c.oc.arboxylase activation niethod [Goodhart and Sinclair (193(1), Schlenk, Lindberg and Tingstam (1940), Goodhart and Sinclair
7) Intravcnous injection of vitaiiiin B, into an individual cau- ses an inimcdiate rise i n the vitamin Ell content of the blood, detcr- minctl by the Phyeomyccs method; the risc is a little dclayctl n-hcn the injection is intramuscular or intracutaneous.
Thus, in spite of the difficulties rnentioncd, one should still bti justified in expecting results from a large number of assays of vita- niin Hl i n the blood. \Yhen i t is s t : i td in thv folloaing that a w r - tain number of iiiicrogranis of vitamin R, per 100 nil of blood has beon found hy the I’hyconiyces method, thc expression should pcr1i:ips be accepted v i l l i some reservation. It might bc better to speak of the 1-csu1ts of the I’hycomyces method in terms of ))vita- i i i i n B, indicators)) or )>vitaniin H, cqiiivalmts)).
The material dealt with i n the present investigation falls within two groups: I . Sornial individuals, 11. Pativnts with various dis-
I . The mwnial inaferialo cornprism 38 persons aged 1!)-70 years, with vitamin H, valiics i n the blood ranging from 5.7 t o l l . - j inicrograms per 100 1111. S o difference i n this respect has been found between the two xcxc’s (18 men and 20 women), nor any rliffcrcnce bctwecn the vitamin 13, valiic-s i n the older and in the younger age-groups. The blood s a m ~ ~ l e (obtained as venous blood frorii the cubital vcin with potassium osalatc BS anti-co:igulant) \\.as iai4her secured while t h c person was fasting or 2- 4 hours after a breakfast that did not contain much vitamin 13,. .I statistical investigation o f the values showed that the mon-fasling)) \wre not higher than the ofastingo ones. Tlie distribution of t h e niatcrial
(1940)].
( 1 91 O)].
t’ases.

D t T E R M I \ A T l O h O F V I I 4 M I A B1 I N THt. B L O O D F R O V H E A L T H Y E T C . 41
was found to be asymmetrical, but becanic normal when the vita- niin B, values were plotted logarithmically as abscissae. Hence it was possible to calculate the mean and the standard deviation:
log mean was 0.8985, corresponding to 7.9 micrograms per 100 ml. Thc standard devialion was 0.0960, which, using the ))5 leveln1, gave the extreme values:
1.0943-12.4 micrograins/per 100 nil 0.7028- 5.0 0.8985 7:. 2.02 . 0.0969 =
1.160 1 - 14.5 H
0.63G9- 4.3 0.8985 4 2.70. 0.09G9 =
11. The / ~ ~ f i e n f s fall within two groups: a) a large number of patients suffering from various diseases; most of these patients have only been cxamined as rquirctl in according \vith their diseas- es and symptoms, and not with the view of looking for special signs of vitamin n, deficiency. A11 wtw patients admitted to 1)epartment I 1 1 of the Kommunehospital, Copenhagen. b) 11 smaller number of patients who - besides the general clinical examination suggest- ed by their particular disease - were subjected to a more detailed examination, taking into account any possible symptoms of vita- min B, deficiency, with a rather careful study of their dietary habits. 'Ihe patients in thi4 group were partly froiii Department 111 of the Ihmniunehospital (included in the above mentioned group), and partly from ))Dc Gamlcs By)), Copcnhngen.
a ) The large g o u p included as many patients as it was possible to subject to determinations of the vitamin B, content of the blood, without selection and without special regard to their disease. l'hc object was to investigate how often a reduced vitamin B, content of thc blood was to be found in an ordinary, mixed number of patients from a special medical department. In practically all cases the blood sampling was done on the first niorning the patient spent in the hospital, and always whilr the patient was fasting.
In this manner vitamin Bl determinations in the blood were carried out in the case of 587 different patients in the course of 1 year. (I t should be added, that the material datcs from a period
1 See R. A. Fisher, rSLatistica1 Nethods for liesearch Workerso.

Table 1. Distribution of 5S7 patieiit\ rrrording to the vit:imiri B, \:ilue i i i the hIi.od
(micrograms per 100 ml).
prior t o tlic intrbduclion of food restrictions in Jknniark) , C;::q; of lht, patients \vcrc i w n , 37 76 nomcn. ?':iblc 1 shows thr. dist.ribri- tion of thc inalcrial according l o t l w vitairiin valuc~ in t l i v hlood.
T h c various investigators who have dealt witti the question arc not in cclniplctc agreement as to lhc normal vitamin H I content of I Iic blond as dctcrniincd by the Phyconiyccs nicthod. Lc'Iiiii:iiiii : i t id Nielscn (I%!)) put thc limits 31 7--14 micrograms per 100 nil, bnbrd on a niatcrial comprising 36 ~ i i v n and 30 women, \vliilc Otlin and Lchiii:inn (19.11) in 10 healthy p r s o n s likc\vise found thc limits to bc i-1.1 micrograms per 100 n i l of hlood. Lchiiiann (privatr c~otiiiriu~iic.atic!~i) is of the opinion, Iio\vcvvr. t l i a t t h e l o v w limit of 7 rnicrogranis pcr 100 nil of blood is too high, and that it should be G..i triicrograins instcad. In 47 niale and 20 fcirialc Iic~althy p ~ s o n s Sinclair (1039) finds 8- 15, or oii tlw nvtmgc. 10.6 micro- grains pcr 1 0 0 1111 of blood. I I c rt.gar(ls a valuc of 7.0 iiiicrograiiih per per 100 1111 2s pat hologically I o ~ v . €'annt.k~ick-\~cstent,urfi and van Yecn (19.10) rvgtnrd .5.S iiiicrogratiis y r 100 nil as tliv lo\\cst limit for t h e vit:iniin I$ content of the blootl. though i r i G out of 90 hcalthy,peIsons they found 5.5 microgrnIiis per 100 1111. or t8vt.n Icss. Elowlantls and \\'ilkinsoit (1038) found t l i c vitaiiiin HI colitcnt o f t h r blood from hcallliy pt'rsons to 1 x 3 G.5---16.5 iiric~rograiii~ pcr 100 1111.
'I'ht. nornial values found by t h c b present autlior S W I I I to lie so I i iwha t loner tlian Ihosc j u s t iiirntioncd: no c.xplanation can be givcn for this tliscrcpancy. ;\iiiong t tic 3S Iicalthy pc~soi is , 5.7 niicrogrnnis per 100 nil was the lowest valiic ohscIvc't1. If applying
D E T E R M I N A T I O N O F V I T A M I N Ill I N THE BLOOD FItOM H E A L T H Y ETC. 43
the 05 o/o levcls (see above) as a criterion for t he extreme values, the lower liniit is found to be 5.0, whilc t he stricter ))I. 04, levelo leads to a lower liniit of 4.3 micrograms pcr 100 nil of blood. It was now found tha t among the 587 patients examined, the vitamin n, con- tent of the blood was less than 5.0 niicrograms per 100 nil in 65 cases (or 11.1 yo) and less than 4 . 3 micrograms per 100 ml in 27
An attempt is iriadc to t.lucidatc the question :xi to \vhich diseas- cis are associated with subnormal vitamin U, content of the blood: It is known tha t various diseases and conditions arc associat- ed with an increased vitamin B, rcquirrment. Jollifft. (193‘3) presents the following, exccllent schedule:
cases (4.6 %).
Fnclors incrctrsiny Ihr uilaniin B, reqirirrmenl.
I. Increase in total mcfatolism. ;l. Abnormal activity, as associated with
1. Prolongcd slrcwuous activity 2. Ikliriuni 3. Manic deprcssivc psychosis, manic type.
1. ‘I‘ubcrculosis 2. Typhoid 3. Rlalaria.
C. Hypcrthyroidisni D. Pregnancy E. Rapid growth.
U. F e v t ~ , rspt~ial ly of long duration, as i n
11. Furrlly assiniilalion A. Diarrhea, especially of long duration, as i 11
I . Ulcerative and m u m i s colitis 2. Intestinal parasite5 3. Intestinal tuberculosis 4. Sp l i t ’
I3. Gaslrointesti na1 fistulac C . Iliseasrs of liver or gall bladclt~r D. .\chlorhydria E. Carcinoma of s to~nuch

4 4 II. 0 . B \ \ I ;
I I I. lncrensetl encrclion ..I. Polyuria, as in
1. Uncontrolled diabetes nicllitus 2. Di.3betc.s insipidus 3 . 1,ong continued excessive fluid intake, as i i i urinary
tract infcctions 13. L.;ictation.
If the states and diseases inentionctl may lead to vitamin 1 4 deficiency, and this dcficic,nry is reflectecl in a reduced vitamin 131 content of thl: blood, one should expcct t ha t the vitamin l3, v:ilucs in the blood of patients suffcring from the diseascs nientionrtl. :IS
a wliolr, would bc lower than in healthy persons, and tha t t h y fell helo\\- thc noiwal lowor liniit more f r q i ( ~ n t 1 y thaii i n p:itierits suf- fering frorii diseases not assumed t o influence tlw T3, requircrncnt.
I n order l o investigate this qut.stion. the. niaterial has bccn di- vided into a nuniher of groups according to diseaw, s c ~ 'I'ahlvs Tables 2 and 3.
'l'nblcs 2 .arid 3 show that both in the investigation of l l i c ire- qutncy of subnornial vitamin HI values in the blood in tliffcrent groups of cli:ieasrs, and in the statistical evaluation of possiblee differences i n the distribution of thr vitamin B1 values in, on the one liantl, tliflerent groups of diseases, and, on t he other, the normal niatcrial, ~ v e f i n d a number of diseascs where a supposed vitaiiiin l3,deficicncy seerns.to he rcflectcd in low values for t h e vitaniin 13, in the blood.
I t shoiild hc said a t once, ;IS d s o shown by t h e tahlcbs, Lliat 1 1 1 ~ siiiii of the cases i n which t l ic tliseascs are supposed to be associated n.ith vitamin H, tlcficiency cxccrds thc total number of patic~nts suffering from these diseases -- the explanation bring that i t often happens that one and the saiiw patient suffers froiii sevt,ral of tlic. diseases mentioned. For c.s:tniplc, t l ic sarrie person mag suffer from achlorliytlria arid chronic alcoliolisni.
valucs i i i thv I ~ l o o t l are considerably more freclutwt in paticnts xitli the diagnosis nnial- nutrition)) t h a n i n the p:rtit.nls suffering from diseases wliich are not believed to be nssociated with vitamin H1 deficiency. Table 3 slio\vs, moreover, t ha t the distribution of the vitainin B, values for thc p t i c n t s \vith malnutrition differs significantly froill t ha t
'l'able 2 shows tha t subnornial vitamin
D E T E R M I S A T I O S O F V I T A M I N B~ IS T H E BI .OOLI F R O I I H E A I . T H Y E T C . 45
I . Diseasrs not believec associated with vitatilit 131 tlrfiricanry . . . . . . . . .
- - . - - - .. -. . . - . - -
2 . .\l;ilnutrition . . . . . . . . . 3. I'ts. on prot'racted tlicst o
with defer1 ivc tliet:ir! habits . . . . . . . . . . . . . . .
1. (:hronic nlcoholism . . . .-). hrhlorliydria . . . . . . . . . 6. 3Ialignant timior i n di
grslivc tract . . . . . . . . . 5. 1)iarrhv.n of long duratioi 8. Gastrocnt crostomiar seq 9. Increased mc~tabolisri
due to various caiiscs . 10. Niimrrou!, yomilings . 11. Cachexia after disease
other than lliow untlrr 1
12. Diseases (11 liver ani bile duct . . . . . . . . . . . . .
'I'o t a1
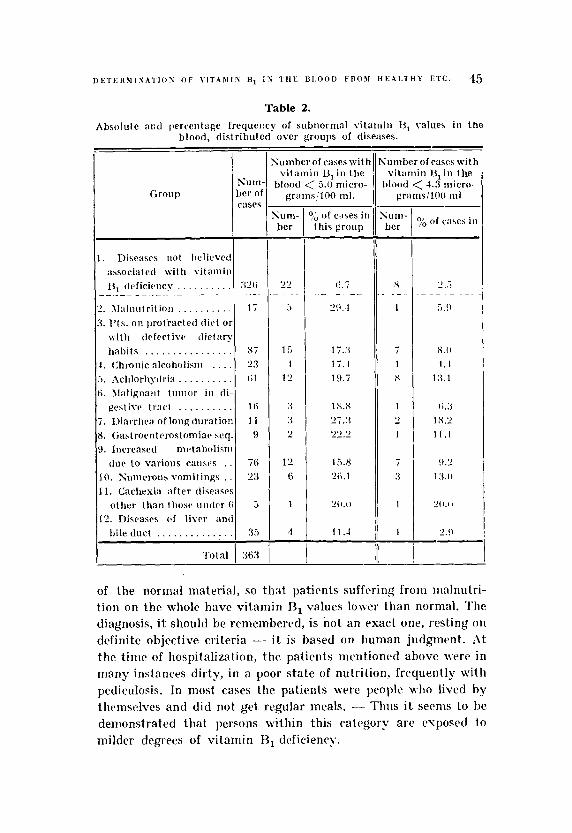
Table 2.
blood, distributed over groups of diseases. Absolute m c l percentege frequetlry of subnormal vitamin lj1 values i n the
Group
<umber of cases with vitamin HI i n the
blood < 5.1) micro- gratns!lOO ml.
ium- ber
of cases in this group
li.7
29. I - - _ _
17.3 1 i . 1 I9 . i
1 X . S 27.3 22,'
15.8 2li.l
2ll.(l
1 1 .-I
-- :umberofraseswith vitamin 13, i n the
ilootl < 4 .3 micro- granis/lOO nil - Cum- ber -
x
1
- I
1 s
1 2 1
7 :3
1
1
yo of case5 i n
of the normal material, so that patients suffering from nialnutri- tion on the whole have vitamin n, values lover than normal. ?'hr diagnosis, i t should be remembered, is not an exact one, resting on definite objective criteria - it is based on human judgment. At t h r tintr of hospitalization, thr patients mentioned above \{ere i n many imtances dirty, i n a poor state of nutrition, frcquently with pediculosis. In most ca4es the patirnts were people who lived by themst~lves and did not get regular meals. - - Thus it seems to he demonstrated that persons within this category are c\rposrd to milder degrees of vitamin €3, dcficiency.
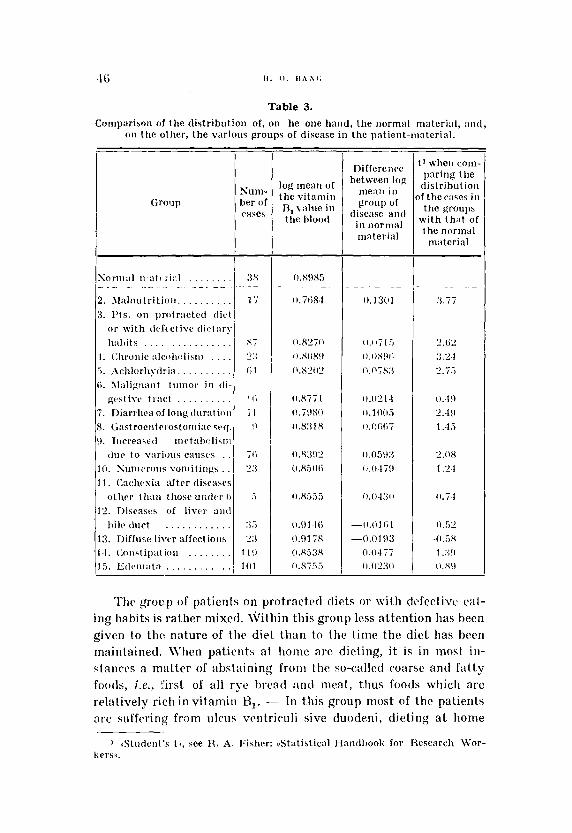
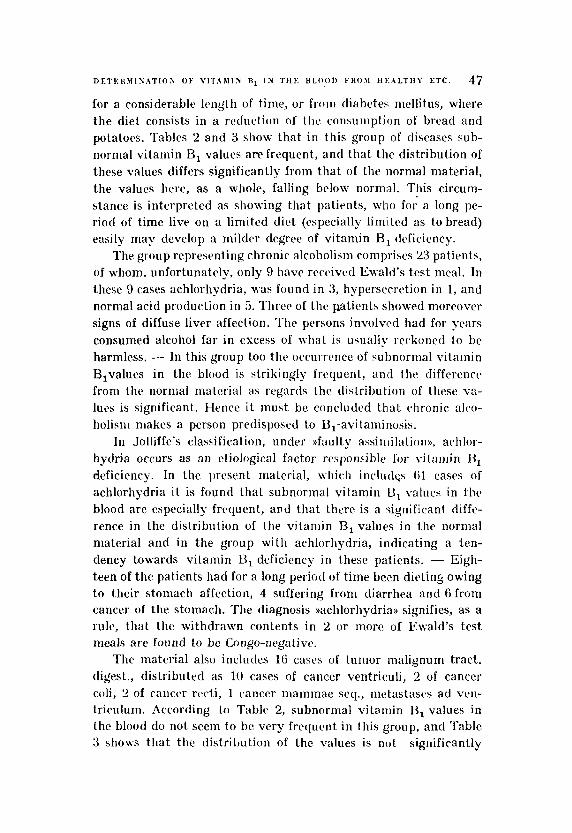
Table 3.
on the other, t h e various groups of disease in the patient-material. Comparison of the distribution of, on he one hand, the iiormal materi:il, a n d ,
Group
Sor1li:rl wat t ri::l . . . . . . . .
2. ~ I a l i i u t r i t i o ~ i . . . . . . . . . . 3. I'is. on protracted t l i c . 1
o r wi th tlcfcclivt. tli(,l:u'y lialiit s . . . . . . . . . . . . . . .
1. (:tirunic alcoliolisiti , , . . 5. ~\cl~Ior l iydri ; i . . . . . . . . . . (i. 3l;ilipn:int tumor i n t l i -
gest ivc tract . . . . . . . . . . 7. Diarrhea of long tltiratioti 8. C;:istroeritriastonliar z r q . 0. Ttirreasetl mc~tahclisrii
(luc to v:irious caiises 10. Suiiioroiis vonliting\ . . 1 1 . (:achcsi:i af ter tliseaws
otl i r r t l i i tn tliow uiitlc,r li 12. Diseases of livcr aiitl
hilr tluct . . 13. Diffuse l i \ w xffectioiis 14 . Cniistipatioii . . . . . . . . 1.5. E ~ I ~ . I I I ; I t R
.. . - . . - . . - - . - -
. . , . . , . , , . , .
log mean of the vi tamin R, v:~lue in the hlood
Difference between log
menii i l l
group of disease a i i t l
in iiormal material
t' when corn- par ing the distrihution
)f thec:iwF in t h e groups
wi th tha t of the normal
inaterial
The group of patients on protractrd diets or with clc4ectivc cal - ing habits is rather mixed. \Vitliin this group less attention has been given 1 0 thc nature of the d i d than to the lime the diet has heen maintained. \\'hen patients at home are dieting, it is in most i n - stances n matter of abstaining from the so-called coarse and fatty foods, i.e., ' k l of d l rye bread and Incat, thus foods which are relntively rich in vitamin B,. - In this group most of the patients arc. suffering from ulcus vcntriculi sive tluodrni, dieting a t home
D E T E H Y I N A T I O A O F VIT.\BIIN B1 I N T H E B L O O D F R O > I H € : A L T l l Y ETC. 47
for a considerable Iengtli of tinie, or from diabetes mcllitus, where the diet consists in a reduction of thc consumption of bread and potatoes. Tables 2 and 3 show that in this group of diseases suh- normal vitamin B, values arc frequent, and that the distribution of these values differs significantly from that of the normal material, the values hcre, as a whole, falling below normal. This circum- stance is interpreted as showing that patients, who for a long pe- riod of time live on a limited diet (especially limited as to bread) easily may develop a milder degree of vitamin H, dcficiency.
The gIoup representing chronic alcoholism comprises 23 patients, of whom. unfortunately, only 9 have reccived Ewald’s test meal. In these 9 cases achlorhydria, was found in 3, liyperscclrtion in 1, and normal acid production i n 5. lhrec of the patients showed moreover signs of diffuse liver affection. The persons involvcd had for years consumed alcohol far in excess of what is usually reckoned to be harmless. - I n this group too tlw occurrc’rice of subnormal vitamin B,values in the blood is strikingly frcquenl, and the differencc from the riorriial matcrial as rcBgards the distribution of these va- lucs is significant. Hence it must be concluded that chronic alco- liolis~it makes a person predisposed to B,-avitaminosis.
In Jolliffe’s classification, under ))faulty assimilation)), aelilor- hydria occurs as an etiological factor responzible for vil:inrin 13, deficiency. In the present material, which inclridcs 61 cases of achlorhydria it is found that subnormal vitamin B, values in Ilic blood are especially frcqucnt, and that Lhcre is a significant diffc- rence in the distribution of the vitamin B, values in the normal material and in the group with achlorhydria, indicating a tcn- dency towards vitamin I), deficiency i r i these patients. - Eigh- teen of the patients had for a long period of time been dieting owing to their stomach affection, 4 suffering from diarrhea and 6 from cancer of the stomach. The diagnosis ))aclilorhydriav signifies, as a rule, that thc withdrawn contents in 2 or more of Ewald’s test meals arc found to be Congo-neg a t ’ IVC.
The material also includes 16 casc’s of tumor malignum tract. digest., distributed as 10 cases of cancer ventriculi, 2 of cancer coli, 2 of caiicer r c 4 , 1 cancer inammae seq., mctastasc>s ad ven- trirulum. According to Table 2, subnormal vitamin U, values in the blood do not seem to he very frequent in this group, and Table 3 shows that the dis t r iht ion of the values is not significantly

48 11. 0. n . \ s c .
different from that found i n tlie normal material. Of tlir 10 cases of cancer of the stomach, G showed inacidity, 1 normal acidity, and in the remaining 3 no Ewald’s test meal was tried. - That thc group docs not show definite signs of vitamin €3, deficicwry is sonicwlial surprising when considering tha t aclilorhydria so frv- qucntly accompanies these diseases. T h t w is nothing strarigc i n thr circumstance that tumors i n the colon or tlie rc.ctuin do not :if-
fcct the absorption of vitamin R, to any noticeable degree, but one should cixpect that stomach cancers had this rffect. The occur- rence of 3 subnornial (i.e. < 5.0 micrograms per 100 nil) vitamin 131 values in the blood is probably more than one can explain as purely chancc phenomena. Whvn t h e distribution of the vita- min 1 3 1 values found does not diffcr significantly from t ha l of t l i c
normal material, i t is pwliaps tluc tci thc o ~ ~ u r r v ~ i c c of a couple oT especially high vitamin I $ values (onv of thrni 18.9 microgr:ims pvr 100 1111 of blood), \vhic.li Iinturally affects a niatcrial of siic.11
liinilcd sizlt. l’lir rcwlts lead to the conclusion tha t tlicrc. weins t o hc a certain slight tendency towards vitamin H I dcficiency i n thr?cb patients, hut t l i c available data furnish no definitc proof.
I<lrvcn patients suffered from protracted diarrheas, and ‘I’ablrs 2 and 3 show that t h e vitnniin l3, deficicnq in some of tlicse pati- ents \\as roflccttvl i n a frcqucnt occurrcnw of subnormal vitamin 131 values i n t h r blood ir i comparison with t l i t values of the normal rnatcrial. 111 one case tlic diarrhea had lasted only 8 days, hut du- ring 1li:it time t h r patient had evacuation 15 times daily. Tlit, re- maining cases involved diarrheas which had lasted one or sevcr:il riionths. ‘rl~rrc of tlie 11 patients had, owing to the diarrhea, been diet ing for some length of time. *hr figures f o u n d thus indicate t h a t in diseases with protracted diarrhea vitamin H, tlcficiency may occur due to reduced absorption of this vitamin.
In Jolliffe’s classification, gastroiritcstinal fistula(’ figurc a s a factor t ha t may increase the vitamin R , requirement. Such fistulae arc raw, however a t any rate, those associatcd with the ripper part of th,;. gastrointestinal tract. ‘fhe material includes only 9 caws with conditions resulting froiii anastoriiotic operation of the stomach or the small intestine. In all instances the opvration was onc t o several ycars old. X-ray examination indicated tha t in most of the cases the anastomosis functioned satisfactorily. Three of t hc patients were on diet owing to the stomach affection. Table 2
D E T E H M I N I T I O X O F V I T A M I S B1 19 T H E BI.001) F R O M H C A L T H Y E T C . 49
shows that subnormal vitaniin I3, values were rather frequent in this group, bu t Table 3shows that the distribution of the vitamin B, values in the case of these patients is not significantly different froni that of the normal material.
Under the heading ))faulty assimilation)) of the vitamin H, Jol- liffe also mentions diseases of liver or gall bladder. Odin and Ixh- mann (1041) found a slight reduction of the vitamin 13, content of the blood in 11 out of 23 cases of acute hepatitis. l 'he present mate- rial includes 35 cases of diseased liver and bile duct, distributed as 10 cases of acute hepatitis, 13 cases of chronic, diffuse liver affect- ion like cirrhosis of the liver, chronic hepatitis, steatosis hepatis; in one ieterus gravis was observed as a result of occlusion of duc- tus choledochus, in 6, different cases of gallstone, and in 5, meta- stases to the liver from various inalignant tumors (including 2 cases of cancer of the stomach). Tables 2 and 3 show that siibror- ma1 vitaniin B, values in the blood in patients belong to this group are not exccptionally frequent, and that the distribution of the vitamin €3, valoes is not significantly different from that of the normal material. Nor do the patients with diffusc liver affections, i.e., the above 35 cases minus the, cases with gallstone, obstructive jaundice, and cancer metastases, seem to show signs of vitamin B, deficiency.
I t is known tha t increased metabolism gives rise to increased vitamin B, requirement. The present material includes 76 cases of increased mctabolism due to various causes. There are two groups: Hyperthyroidism (5 cases) and fever (71 cases). Ehch case of fever of a t lest 38" C, which has lagted for not less than 4 days before the sampling of the blood for thc vitamin R, assay, is included within this group. One might perhaps think that the groupshould be confined to include eases where the fever had lasted more than 4 days, bu t the experience gained froni the first vitaniin €3, detcr- minations in patients of this kind led to the adoption of this time limit, since i t was not unusual to find reduced values a t that stage in a febrile disease. Observations from experinicntally pro- dued B, avitaminoses i n human beings have shown, too, that the first symptoms of vitamin B, deficiency may occur a t an early stage [ Jolliffe, Goodhart and Cline (1939)l. 'Lhc febrile diseases here considered are pneunionias, undulant fevcr, rheuniatie fever, febrile infectious diseases of the urinary duct, and phlebitis. - I t 4 Acla med. scandinar?. Vol. C X X I I .
50 H . 0. UAS(.
should be pointed out that the vitamin B, deficiency observed in the case of febrile diseases hardly is due solely to the increase in metabolism which accompanies the fever. The anorexia, which in many instances accompanies the febrile disease, is undoubtedly of considerable importance in this connection. - ('The 5 cases of hyperthyroidism have not been dealt with separately because the number is so low.) - Tables 2 and 3 show that not only do the subnormal vitamin B, values seeni to be frequent in the patients belonging to this group, but the distribution of the values found in this group is significantly different from that of the normal material. Tlie findings indicate that the febrile diseases, even when of short duration, may give rise to vitamin U , deficiency.
There n.;is some reason to assuine that cacliectic patienls sub finern oitae had a low vitamin 1 j l content of the blood. The present nialerial includes 5 cascs of cachexia not duc to nialignaiit tuniors in the gastrointestinal tract. I n the 5 patients, a subnornial Jita- min 13, valul? occurs only once; the distribution of n ' l 5values is not significantly different from that of the nornial material.
Finally, inention is niadc of 3 group of patients who Iiave in common t h a t they havc suffered for some time froin repeated vomitings -- an affection \vhich one might expect to (:ausc' vita- min U l deficiency if the vornitings are sufficiently intense. The group includes 24 patients, in most instalices suffering froin diseases of the stomach (iilcus juxtapyloriuni, pylorostcnosis, cancer veiitricLli), hut also other diseases may be rcsponsiblc, e q . , iicphro- sclerosis with uremia, Nb. Alertiere, diverticuluni oesophagi. - Subnormal \ d u e s for vilamin U, in. the blood ai'e rather frequent, but the statistical comparison bctwecn values of this gIoup and those from the nornial material shows no significant difference.
In the foregoing inention has been nmdc of the vitamin 13, f in- dings i n the blood of patients suffering from a series of diseases whwc i t \vtl:j to be expected, more or Irss, that vitainin defi- ciency would occur. Table 2 shows, however, that subnormal vitamin B, values also are found in patients suffering from other diseases. We shall briefly review these cases. .Is mcn- tioned, of Ihe 326 patients suffering from diseases which one would not ordinarily associatc with vitamin n, deficiency, 22 (or 0.7 l /o) showed vitamin H, values < 5.0 micrograms per 100 ml, and 8 (or 2.5 yo) values < -1.3 micrograms per 100 ml. For com-
~ E T E R % l I \ A T I O \ O F V I T A > l l \ R 1 I \ 1 I i K U l . 0 0 1 ~ F I I O N I l ~ A L T 1 1 Y ETC. 51
parison with these figures it may be mentioned that of the 261 patients suffering from sonic disease which according to the litera- ture might be expected to be associated with vitamin t3 , deficiency, 43 (or 16.5 %) showed vitamin R, values < 5.0 niicrograms per 100 ml, and 20 (or 7.7 yo) values < 4.3 micrograms per 100 1111. Accord- ingly, the probability of finding a subnormal amount of vitamin €3, in thc blood is more than twjce as large jn the patients suffering from diseases which are known to be associated with vitamin B, deficiency as it is in patients with diseases ot.hers than those men t io nea .
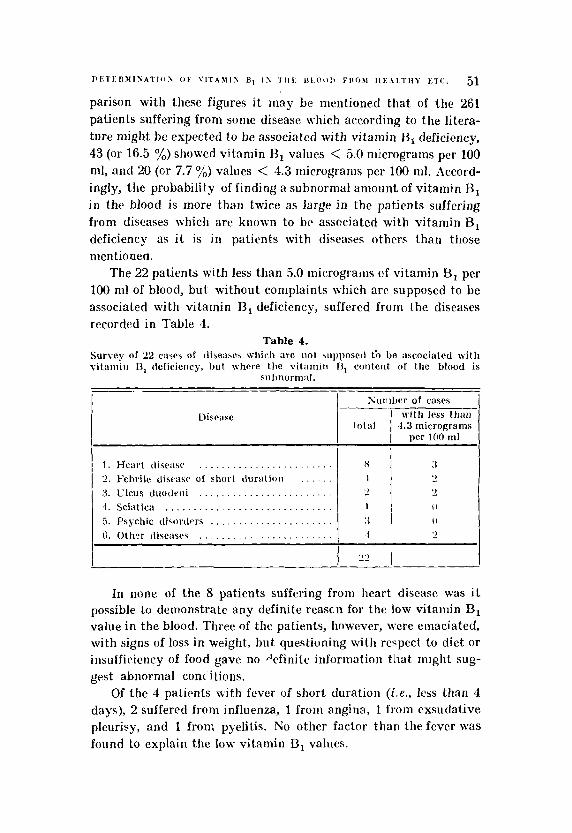
The 22 patients with less than 5.0 microgram of vitamin B, per 100 ml of blood, but withcut complaints which arc supposed to be associated with vitamin R, deficiency, suffered froni the diseases recorded in Table 4.
Table 4. Survey of "2 cases of dise:iaes wliich are not suyposcd th be ascociated with vitanlin 13, tlcficiericy, but where the vit;umili N, content of the blood is
subnorm:il. ___.
Disease
1 . Heart tliwise . . . . . . . . . . . . . . . . . . . . . . . . 2. lcbri lr cliscasr of short tluration . . . . . . 3. Clcus duotleiii 1. Sciatica . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5. Psychic disorders . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . .
Sumber of cases with less than
total 4.3 micrograms per 100 ml
___.
H :I 1 - ) - > - > 1 0
3 0
In none of the 8 patients suffering from heart disease was i t possible to demonstrate any definite reascii for the low vitainin Bl value in the blood. Three of the patients, however, were emaciated, with signs of loss in weight, but questioning with respect to diet or insuffiriency of food gave no +finite information tha t might sug- gest abnormal coil( itions.
Of the 4 patients with fever of short duration (Le., less than 4 days), 2 suffered froni influenza, 1 froni angina, 1 from exsudative pleurisy, and 1 from pyelitis. No other factor than the fever was found to explain the low vitamin 13, values.

52 Ii. 0. B A N G
Two patients with low vitamin B, content of the blood suffered from duodenal ulcers, but neither of them had been dieting a t home. One was rather underweight. ?\'either suffered from vomiting.
Three patients with subnormal vitainiri B, values in the blood suffered frorri psychic disorders, in 2 of them in the form ol* mer- vousnesso, in 1 the form of hysterics. Two of them showed loss of weight prior to admission.
))Other diseases)) (Table 4) which were accompanicd by subnur- ma1 vitamin H, values in the blood were the following: Tltrom- bosis cerebrj (l), urolithiasis, cystitis (I), arthrosis coxac e t gen. (l), and bronchitis chron. (1) In none of the cases was i t possible to find anything to account for the low value. - Summing up, i t may he said that in the 22 patients suffering from diseases not known nor bdievetl to be associated with vitamin B, deficiency, subnor- mal values were found for the vitamin 13, conlent of the blood, without it being possible to find any definite oxplanation of the fact. In sonie of the cases onc mjght perhaps have sonic idea of the cause (loss in weight, fever of short duration, storiiach disease), but nothing definite can he said on the basis of thc information avai 1 ah Ic .
\Ve shall now consider the qucstion \vhcther subnormal vita- min ll1 values in the blood are associated with any definite symp- toms. Let i t be said a t once tliat the niateriul unfortunately does riot include any cases of manifest l~eribcri. - - Sone of thc patients suf- fered from cdemata tha t could not be attributed to other diseasths, nor showed heart symptoms that could not as nell be imagined to have another c.tiology than vitariiin €3, deficiency, nor symptoms of polyneuritis as sevcrc :is those described in the c : ~ w of oriental bwiberi. If any of the patients showed syinptoiiis associated with subnormal vitaniin U, of the blood, it should be t h t w cague, rwn characteristic syriiptoiiis which are common for a number of different diseases, but which, from experimentally produced vita- min B, dr,ficiency in h u m m beings, are known to be duc. Lo a mild degree of vitamin B, dcficiency. 1-Iere we have in mind such symp- loiris as f:itigue, milder parcsihesja, loss of appeti le, insomnia, ctc. If one were to make an investigation of the presence of this kind of syniptonis in the various patients considered, i t would be re- quired tliat the ordinary, clinical examination of the patient upon admission bc suppleniented by a questioning and examination

D E T E R M I T A T I O S OF V l T A M l Y HI IN T H E RLOOD F R O M IIEALTIIY ETC. 53
with particular respect to these symptoms. In the present mate- rial this has only been don(. in a minor number of cases, which w l l be considered later in the paper. At this place we shall Iiierely mentioned a few special symptoms which the available data make it possible to investigate.
I t was mentioned abo\-e that a symptom like etleniata was not found in any case where i t could not be explained on the basis of the primary disease . - heart disease, kidney disease, ctc. Hut since i t could not be denied a priori tha t vitamin H , deficiency perhaps might be a contributive cause in the appearance of the edcmata, especially in diseases of the heart, it was investigated whether pati- ents with edemata had a vitamin B, content of the blood which was definitely lower than that found in healthy pcrsons. The results are recorded in Table 3. It is seen that the vitamin HI values for the patients with edemata are not significantly different from those found in the normal niaterial. This tloes not, liowcvcr, permit us to concludc definitely that a reduced vitamin 13, content of the blood may not play a r61e i n some cases of edeina1.a.
Constipation is another symptom which perhaps might be accounted for nuniericnlly on the basis of the available inaterial. Various authors have mentioned constipation as a symptom of vitamin H, deficiency [Shiniazono (1'327) in oriental beriberi, Elsoni (1933) and Williams, Mason, \\:ilder and Sliiitli (1940), the latter in experinlentally produced vitamin Ei, deficiency in human beings). -- In the present investigation a count has been made of the patients suffcring from constipation, and the vitamin B, content of the blood of these patients has been noted. The result is found in Table 3. 1\ comparison with the distribu- tion of the values in the normal. inaterial shows no significant difference.
In the ordinary clinical examination of the patients only slight attention has been given to all the other symptoms of vitamin H I deficiency - cspccially the many different neurological symptoms - so that i t is impossible from the available data to calculate the frequency of these symptoms in relation to the vitamin B, content of the blood. I t is here necessary to confine oneself to a general estimate which is arrived a t by a study of the numerous records. This estimate seems to show that reduced vitamin B, values are not accompanied by symptoms which ordinar~lg are associated
54 H . 0. I I A S G
with beriberi. Thus it seems that in all instances i t is a question of latent cases of vitamin R, dcficiency, as i n the case of other viin- mins, especially vitamin C
b. As mentioned in t hc foregoing, a small number of paticnts in whom the vitamin B, content of the blood was determined, were not only subjected t o t he usual clinical examination, h u t also to a supplementary exaniination, aimed at possihle syrnptonis of H,-nvitaniino.;is: moreover, their dietary history \\.as taltcn into account. - - This osinall rtiatcrialo conipriscs 53 patients, of whom 31 are from Department 111 of the Il;omniuneIiospital, while the remaining 22 ,711 are froin the infirmary of i d k Ganiles By)). In order to get as niany cast's as possible with suhnorinal vitamin H , values in the blood, patients have hccn sc~lectrtl - e s p ~ i a l l y aniong those frort- elk Ganiles I3go - \vho orit' \\.otild rixpect, knowing their disexie, t o have lo\\. vitainin R, valucs in tlie blood, e.y., pati- ents with cancer of tlie sfoiiia,.li. l l i c result of this selection is tha l the mziterial includes 11 patients with less than (5.0 niicrograrns of vitamin B, per 100 in1 of blood, and 7 with less than 4.3 nlicro- grams per 100 1111 of blood.
These patients have been questioned in detail regarding sub- jective synlptoms and daily diet. AIoreover, they liavc been rarcfully examined Tor B,-avilaniinotic syniptoiiis. They have hecn ques- tioned as t o social environment, especially as whetlier they liave been unemployed or have been living alone. I t is possible on tlie basis of tlie informations to get an idea of the vitamin H, provi- sion. On the basis of data collected [Hang (19.14)] i t is possible to estimatc that on I l i r average about '75 yo o f thc vitaniin I%, intake per day has its origin in bread (cercals), p(Jtatocs and milk. 'l'lie procedure in dealing with the informalion obtained from t h e pati- ents has been as follows: First the vitamin 13, content o f t h c w tliwe basic foods is calculated; by multiplying the result by 4/3 one arri- ves a t the estimated daily vitamin B, intake. This is then coniparcd to the assunled vitamin 13, requirenirnt, estiniaied according 10 Ege (1940). Since the requirement is dependent on the magnitude of t l i c met.Ibolism, tlie lnttcr is cstiinated n i th the aid of tables prepared by Faber and Norgaard (19X3). ?'tic dcgrcc of tlie vita- rnin 13, provision is now ealrnlated according t o the forniula:
vitamin HI intakc vitainin B, requiremen'
x 100. It is obvious that this coniputa-
D E T E I O I I \ \ T I O S OF V I T 4 M I S l j l IS T I I E B 1 . 0 0 1 I F R O M H E A I . T H Y ET(:. 55 Microgram
B, per 100 ml
I I I I ; I c
. ‘1 1 I
Degree of provision
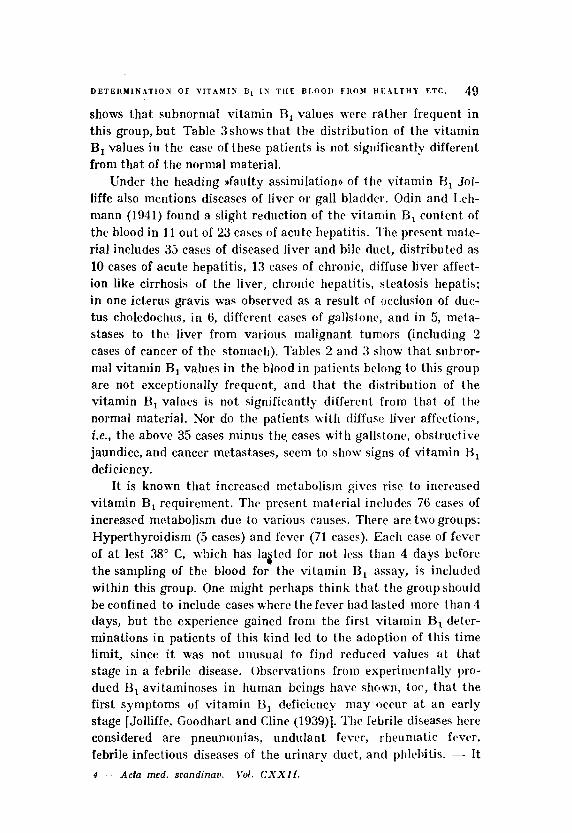
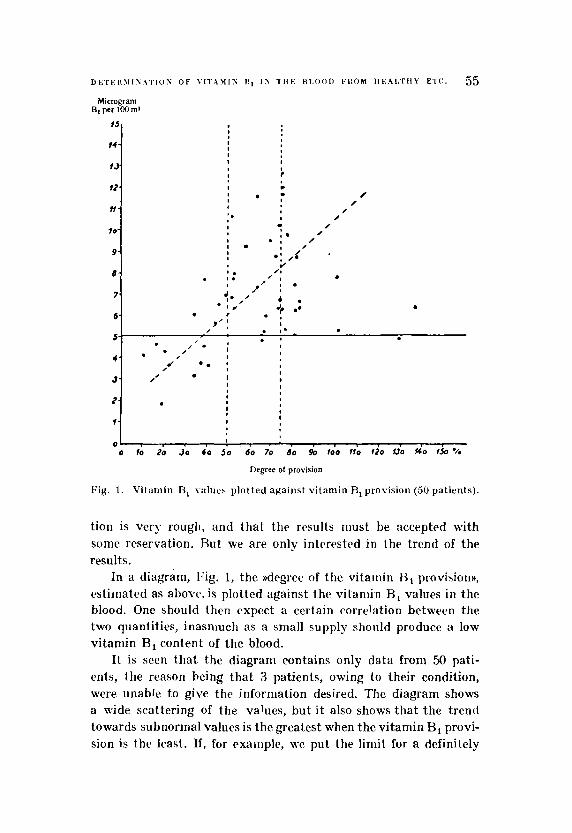
Fig. 1. Vitamin I3, w l u c s plotted against vitamin R, provision (50 patients).
tion is very rough, and tha t the results must be accepted with some reservation. Rut we are only intrrested in the trend of the results.
provision)), estimated as al)orc, is plotted against the vitamin H , values i n the blood. One should then expect a certain correlation between the two quantities, inasniuch as a small supply should produce a low vitamin B, content of the blood.
I t is seen that the diagram contains only data from 50 pati- ents, the reason being that 3 patients, owing to their condition, were unable to give the information desired. The diagram shows a wide scattering of the values, but i t also shows tha t the trend towards subnorinal values is the greatest when the vitamin B, provi- sion is the least. If, for exainplc, we put the limit for a definitely
In a diagram, Fig. 1, the ))degree of the vitairiin

56 H. t ) . B \ S t i
insufficient vitainin B, provision a t 50 yo, i t is scrn that 10 out of the 1.5 observed vitamin €3, values (01 67 yo) with a vitainin n, pro- vision below the one just stat'ed correspond to subnornnl vitamin €3, values in the blood. The zone with thc vitamin H, provision %-- 74 yo is regarded as having doubtful significance. The ratio between the subnormal and the total number of vitamin R, v' '1 1 ues within this zone is 1: 17, or 6 yo. The vitamin B, provision of 75 yo over is regarded as being in all probability sufficicnt; the observed vitamin B, values in this part of the diagram are distributed with 1 subnormal and a total of 18 values, the subnormal one therefore representing 6 yo. - ~ - - .\n attenipt has been made to trace a straight line through the diagram which, roughly, \\-auld satisfy the points. The line, however, should not- be accepted as a niathe- matical expression for the correlntion - it only shows the trend in the distribution of the points.
The paticnts concerned have also been quvstionctl :IS to the presence or absence of a number of symptoms \vhich niust be sup- posed to be more or less indicative of I<,-a\itaniinosis. For cxaiiiple, the patient M a s asked whether there had been any loss of appetite, loss in weight, depression or onervousntsss. functional dyspnoea, palpitations, angina pectoris-like cases, vdcniatn, cramps in the calf of the I t g weakness and ))nervous pains)) in the cxtremitics, constipation, vomiting, diarrhea.
The physical exmiination has dealt especially with neurological phenoniena, and confincd to thc most readily ohstwed symploms. I t has 'morec'ver been investigated whether the patients sufferetl from any cardiovascular changes or sho\ved signs of H,-avitarnino- sis, especially pellagra (Jr arihoflax inosis.
Of the 11 patients with subnormal vitamin I3,values, 4 suffered from cancer ventriculi, 1 from cancer oesophagi, anti 1 from cnnccr capi tis pancreatis. The rernaindt.r were dtbilitated, senile, arterio- sclerotic patients with very slight appetite.. l+3nally, 1 suffered from quinine poisoning. The patients with noriiial vitamin L3, con- tent of the k,lood suffered from a variety of diseases, of short or long duration.
As the main result i t may be stated a t once that the various symptoms listed above (including those usually associated with t i - tamin B, deficiency) 011 the whole were not found i n the patients wjth subnornial vitamin B, values. A t any rate, the symptoms were
D E T E R M I S A T I O S O F V I T A M I S B1 IS T H E I i L O O D F R O M H E A L T H Y ETC 57
not more frequent here than in the patients with normal vitamin B, values. Most of the symptoms, it is understood, are symptoms which occasionally or frequently accompany a number of diseases which have nothing to do with vitamin B, deficiency, e.q., symp- toms like fatigue, milder depressive states, anorexia, loss in weight, constip%tion, etc. Hence i t is inipossible to account, numerically, for the frequency of most of the symptoms in the two groups. A few may be pointed out, however, as apparently inore frequent in the group with subnormal vitaniin €3, values in the blood: Anorexia was observed in 8 of the 11 patients with subnormal values, or in 73 yo, while in the 42 patients with normal values tlie symptom cwm-red only 11 times, or in 26 yo of the cases. This coincides with the extremely poor dietary history of the patients with the subnormal vitamin I3, values in the blood. Add to this, that 7 out of the 11 (64 yo) and 15 out of the 42 patients (36'y0) with, respecti- vely, subnormal and normal values had suffered a loss in weight during the period prior to the vitamin B, assay. AIildcr states of depression were observed in 4 out of the 11 (28 7,) and in 5 out of the 42 (12 %) patients with, respectively, subnormal and normal vitamin B, values. Symptoms of disturbances of the circulation, or of edemata, were not more frequent in the paticnts with subnor- mal values. Likewise, there secmed to be no difference in thc inci- dence of the various subjective neurological symptonis in the two groups.
As far as the physical exaiiiination was concerned, none of the looked - for symptoms seemed to be more frequently observed in the patients with subnormal vitamin B, values than in the patients with normal values. In most instances the neurological examination gave rather negative results, and if changes like weak or absent tendon reflexes or the like were observed, they wwc eithcr isolated findings, or could be explained by tlie general debility of the patient.
Atrophy of the lingual papillae was observed more frequently in the patients with subnormal vitamin H, values, namely i n 7out of 11 against 7 out of 42, or in 64 yo against 17 yo.
N o electrocardiographic changes were observed tha t could not be explained by the presence of other affections, especially arte- riosclerosis.
The conclusion from the findings just described must there- fore be that a subnormal vitamin B, content of the blood, detrr-
58 H. 0. B A S C
mined by the I’hyconiyces method, in most cases is not arcom- panied by symptoms which one ordinarily assorintt.s with vita- min B, deficiency, and that the symptoins observed along with the subnormal vitamin B, content of the blood are so vagiic ant1 non-cliaractwistic that they cannot be used in rctting off a Bl- hypovitaminotic condition from 0thr.r states of i l l health. € h e we must rrly upon a rediicrd vitamin R , content of lhr blood (or the urine,). In tliese cases, as i n the case of vitamin C dcfiriency, one has to sptlak of a lafenf uiluniin B , delicirncy. Such latent vita- min 13, deficiencyis a not unusual finding in connection with a num- bcir of diseases wd ich etiologically or patliogrnically have 1 ) w n associated with B,-avitarninosis, but it also s e e m to :icconipany diseases which apparently have notliing to do with vitamin f 3 , deficiency.
Summary.
The decline in the vitamin If, provision during t l ic last century makes it desirable to investigate the vitainin H , contcnt of the body fluids. The I’hycomtyces rnefhod has in another paper by thc present author been subjected to a critical cvaluntion.
I h c prcwnt paptir discusses the results of B Scrirs of vitamin R , assays of t h e blood of normal persons and of paticrits suffering from various diseases. ’I’hc vitamin n, values in thr blood of t l i c normal persons show normal distribution if plotted IogarithIiiically as abscissae. l‘lie mean value of the vitamin B, contcnt of the h o d froni these 38 individuals is 7.1) micrograms per 100 nil.
The rn:itc,rial comprising the patients falls into t\\o groups, one of 587 and one of 53 patients. The latter have been more thoroughly examined tIian the former with respect to possible syniptonis of vitamin U, deficiency, and records h a w been obtained of their dietary history.
In the ))large material>) the vitamin H I valuo in the blood of thesr 587 non-selected patients is subnormal in 6.5, o r 11.1 %), if the lower limit is put a t 5.0 micrograins, and in 27, or 4.6 06, i f t tw lower limit is put at 4.3 niicrogranis per 100 rill of blood. 3lort.- over, that a series CJf different diseases arc aecompied by a strik- ingly frequent occurrence of subnorinal vitamin I3, values, and that these v:ilues for the vitamin 13, i n the blood i n these diseases
- .

D E T I R M I h A 7 I t N 0 1 VI’TAMI? B, I N T H E BLOOD k R O \ I H F A L T E Y ETC 59
are found to be significantly lower than in the wormal materiala. The following diseases are involved: hlalnutrition, diseases caused by prolonged dieting, chronic alcoholism, achlorhydria, diseases with protracted diarrhea, and increased metabolism due to fever.
The paper finally mentions the special exammation of the above mentioned mna 1 material)) (53 patients). I1 is shown that, on the basis of a rough estimate of the vitamin B, intake through the diet, together with an evaluation of the requirement, soiiie correlation is found to exist between the rdegree of the vitamin B, provisiono and the vitamin 13) values in the blood.
The symptoms, which are generally rtwgniLed as those of vitamin 13, deficiency, are not found to accompany subnormal vitamin B, values in the blood. It is therefore necessary to speak of a lalenf vitamin 11, deficiency, which is a not unusual finding i n a number of disease\.
Bibliography.
I . Rang, Jl. 0.: 1:geskr. f . Largvr 104: 572, 19.12. - 2. Rang, H . 0.: Dispirta’ts, Ksberihavii 194.1. - 3. Bang, H. 0.: Xcta med. Scarid. 120: 447, 19.45. - 4. Ege, R . : Ernzriugslzrc, Ksbenhapn 1940. .- 5. Elsom, K . 0.: J . Clirt. Investigation 14; 40, 1935. - 6. F’kbcr, A. & A. Xorgaard: Haand- bok i Diictetik, K0bt:nhavn 1033. - 7. Goodhart, €3. & H. Ivl. Sinclair: Biochem. J . 33: 1099, 1939. - 8 . Goodhart, R . & 11. 31. Sinclair: J. Biol. Chem. 132: 11, 19.10. - 9. Jolliffe, N.: Hull. Xew York Acnd. Mcd. 15: 469, 1939. - 10. Jolliffe, X., R . Goodhart, Dennis & , I . Cline: Am. J . M. Sc. 198; 198, 1939. - 11. Laurent, L. 1’. 13. & H. M. Sinclair: 1,ancet 1: 1045, 1938. - 12. Lchmann, J . 8r 11. E. Nielsen: So rd . Med. 1: 289, 1939. - 13. Meiklejohn, -4. P.: Riochem. J . 31: 1441, 1937. -- 1 4 . Odirt, M. & J. Lemartn: Acta Ined. Scarid. Suppl. 123: 390, 1941. - 15. Panrit!koek- Westenhurg, S. J . E. & A. van Y w n : . I . A. 31. A. 115: 1494, 1:&1(1. - lti. Howlands, E. h. 8r J . F. Wilkirisori: &it. 11. d . 2 : 878, 1938. - 17. Schlcnk, IJ. 13. I h d h r r g 8: S. Tingstarn: \’it. u . Ilorrnone 2: 51, 1!)42. - 18. Schopfcr, W. 11. & A. Jung: \’:c Congrrs international technique et chimique dcs induslries agricoles. Schrwt~rtingue 1937 p. 21. - 19. Schopfrr, W. 11. & A. Juiig: Zeitschr. f . Yilantiitforsch. 7: 143, 1938. - 20. Shimazono: Berlin 1927. - 21. Sinclair, H. 31.: Riochcm. J . 3 3 : 2027, 1939. - 22. Williarns, R . D., €1. 1,. &fason, 13. H. Wilder B. B. F. Smith: Arch. I n t . I\fcd. 66: 7x5. 1940.