Embed Size (px)
Citation preview

Development and Testing of the Helex Septal Occluder, aNew Expanded Polytetrafluoroethylene Atrial Septal
Defect Occlusion SystemEvan M. Zahn, MD; Neil Wilson, MD; Warren Cutright, DVM; Larry A. Latson, MD
Background—A variety of transcatheter atrial septal defect (ASD) occluders are currently in use around the world.Although for the most part effective, all of these devices lack features that would be desirable in a “perfect” device. TheHelex septal occluder is a new type of device designed to improve the results of transcatheter ASD closure. This studywas designed to examine the effectiveness and safety of this occluder in an animal model.
Methods and Results—The Helex was implanted into 24 dogs with surgically created ASDs. Procedural details focusingon deployment, removal, and early closure rates were examined. Follow-up consisted of sequential transesophagealechocardiography and fluoroscopy as well as epicardial contrast echocardiography and angiography at the time of death.Specimens were examined grossly and histologically, and devices were tested for metal fatigue. All animals hadsuccessful ASD closure. Implantation was uncomplicated (mean fluoroscopy time 11.7 minutes), and removal orrepositioning was always possible. Closure rate as judged by transesophageal echocardiography was 88% initially and100% at 2-week follow-up. Devices rapidly became infiltrated with connective tissue without inflammation and wereendothelialized over time. There were no instances of thromboembolism. A single wire-frame fracture occurredsecondary to a prototype delivery system malfunction.
Conclusions—The Helex septal occluder proved safe and effective for ASD closure. Several advantages over currentlyavailable devices were evident in this model. Controlled prospective clinical trials are needed.(Circulation. 2001;104:711-716.)
Key Words: heart septal defectsn catheterizationn pediatricsn shunts
Since the 1970s, investigators have been searching forimproved techniques to achieve transcatheter closure of
atrial septal defects (ASDs).1 Although a number of deviceshave undergone investigation, the ideal device does notexist.2–8 Such a prosthesis would be simple to implant andeasy to remove, provide 100% closure, maintain a low profileon the atrial septum, have an atraumatic contour, and becomposed of materials with proven mechanical integrity andlong-term biocompatibility. In 1995, we began to design anocclusion system that would incorporate these features. Thisstudy reports the results of tests of this new device in ananimal model.
MethodsDevice and Delivery SystemThe Helex occluder is composed of a single piece of nickel-titanium(nitinol) wire with a patch of microporous expanded polytetrafluo-roethylene (ePTFE; W.L. Gore & Associates, Inc) attached along itslength. The superelastic property of nitinol is used to form the wireframe into 2 equal-size opposing disks that bridge and occlude theseptal defect (Figure 1). The wire frame is easily visible with
fluoroscopy and contains 3 clearly marked “eyelets” that facilitateproper placement. The occluder is fixed in place by a unique lockingmechanism that passes through the center of the device from the leftto the right atrial disk, thereby securing it in place. The ePTFE isspecially designed to facilitate rapid cell penetration, thereby pro-moting rapid tissue ingrowth, resulting in permanent defect closureand device stability.
The delivery system is a coaxial catheter assembly consisting of a9F preshaped outer delivery catheter, an inner 6F control catheterused for deployment and/or withdrawal of the device, and a centralmandrel used to configure the device and deploy the lockingmechanism (Figure 2). An ePTFE retention suture anchored to the tipof the control catheter loops through the right atrial eyelet and isexteriorized to the operator. This suture allows for removal of thedevice after complete deployment and release from the catheterdelivery system if desired.
Delivery ProcedureThe occluder comes premounted on the delivery system. Afterirrigation with heparinized saline, the system is introduced through astandard 9F femoral venous sheath. The delivery catheter is designedto facilitate direct passage across the ASD, obviating the need forplacement of a guidewire and delivery sheath in the left atrium(Figure 3). Once positioned in the left atrium, incremental advance-
Received November 6, 2000; revision received April 17, 2001; accepted April 17, 2001.From the Department of Cardiology, Miami Children’s Hospital, Miami, Fla (E.M.Z.); the Department of Cardiology, Royal Hospital for Sick Children,
Glasgow, Scotland (N.W.); W.L. Gore and Associates, Flagstaff, Ariz (W.C.); and the Department of Pediatric Cardiology, The Cleveland ClinicFoundation, Cleveland, Ohio (L.A.L.).
Correspondence to Evan M. Zahn, MD, Miami Children’s Hospital, Suite 104, 3200 SW 60th Court, Miami, FL 33155. E-mail [email protected]© 2001 American Heart Association, Inc.
Circulation is available at http://www.circulationaha.org
711
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from
ment of the control catheter and retraction of the mandrel result inconstitution of the left atrial disk. The appearance of the center eyeletmarks the completion of left atrial disk deployment. Gentle retractionof the entire system then results in apposition of this disk to the atrialseptum. The right atrial disk is then delivered in a similar fashion.Before the device is locked in place, repeated repositioning of eitherdisk and/or complete device removal via the delivery catheter ispossible. Withdrawal of the mandrel into the control catheter resultsin deployment of the lock and separation of the device from thecatheter. Once this occurs, the device and atrial septum are free of alldistortion associated with the delivery system, and a true assessmentof device position and leak status can be made. Even at this late stageof delivery, if device removal is desired, traction on the retentionsuture unlocks the device and allows it to be withdrawn back into thedelivery catheter. If the result is acceptable, however, the retentionsuture is removed, completing the procedure.
Animal ImplantationsImplantations were performed in 24 mature dogs cared for inaccordance with the “Position of the American Heart Association onResearch Animal Use.” Before this study, extensive laboratory andcomputer analysis of all device and delivery system components wasperformed. Animals were given oxymorphone (0.05 mg/kg SC) andatropine (0.04 mg/kg IM) before the induction of general anesthesiawith diazepam (0.2 mg/kg IV) and ketamine (5 to 10 mg/kg IV) andwere maintained with isoflurane and vecuronium (0.1 mg/kg IV).Septal defects were created surgically via a left lateral thoracotomy.A 6-mm punch was passed via a purse-string suture from the left tothe right atrium as previously described by Das et al.8 Defect creationwas followed by device closure from a right femoral venousapproach. Preclosure evaluation consisted of transesophageal colorDoppler echocardiography (TEE), left atrial angiography, and staticballoon sizing (Nitinol Medical Technologies). During the studyperiod, devices were available in 15-, 20-, and 25-mm diameters.After device placement, results were assessed by TEE and right atrialangiography. Antiplatelet therapy (aspirin 81 mg/d) began 2 daysbefore the procedure and continued until the dog was euthanized orfor a maximum of 6 months. Animals received heparin 100 U/kg IV
and antibiotic prophylaxis (cefazolin 22 to 44 mg/kg IV) during theprocedure.
Follow-Up and ExplantsTEE and fluoroscopy were performed 2 weeks after implantation andmonthly thereafter. Animals were euthanized at 1, 3, 6, or 12 monthsafter implantation. At the time of device explantation, TEE wasperformed, followed by lateral thoracotomy and placement of alarge-bore catheter into the left atrium. Epicardial color Doppler andbubble contrast echocardiography (left and right atrial injections) andright and left atrial angiography were then performed. Heart, lungs,brain, and kidneys were examined grossly and microscopically forevidence of thromboemboli.
ResultsImplantationTwenty-six dogs (mean weight 23.6 kg) were used for thestudy. Two died after ASD creation before catheterization.Twenty-three of the remaining 24 animals had left-to-rightshunting at the atrial level demonstrated by TEE after thesurgical procedure. In 1, no ASD was identified, and atransseptal puncture and static dilation of the atrial septumwere used to create a defect. Mean static and balloon-sizeddefect diameters were 7.962.3 and 10.462.4 mm, respec-tively. In 23 of 24, the ASD was crossed with the deliverysystem alone. For the animal that required transseptal punc-ture, a guidewire and long sheath were used to cross the ASD.
Device placement was successful in all animals, andrepositioning of the device was always possible before lockdeployment. Mean fluoroscopy time for single device implan-tations was 11.766.2 minutes. There were 4 instances ofdevice removal (withdrawal of the deployed device back intothe delivery catheter before lock deployment) and 3 instances
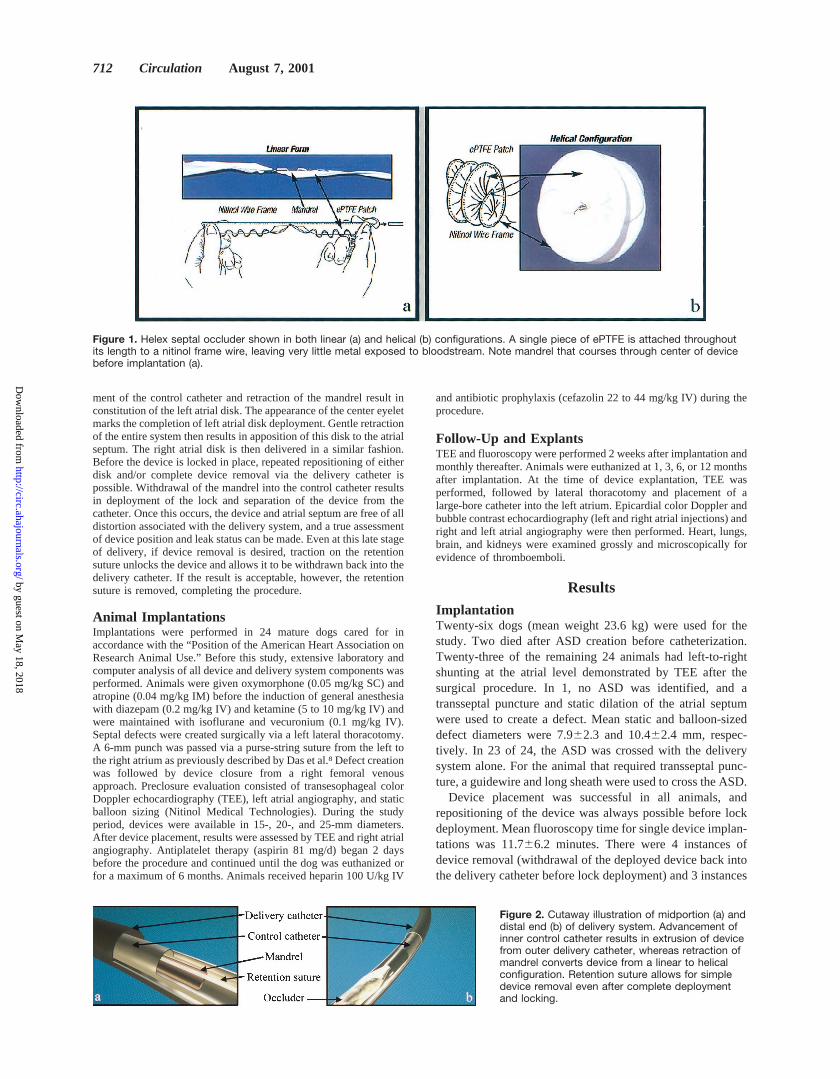
Figure 1. Helex septal occluder shown in both linear (a) and helical (b) configurations. A single piece of ePTFE is attached throughoutits length to a nitinol frame wire, leaving very little metal exposed to bloodstream. Note mandrel that courses through center of devicebefore implantation (a).
Figure 2. Cutaway illustration of midportion (a) anddistal end (b) of delivery system. Advancement ofinner control catheter results in extrusion of devicefrom outer delivery catheter, whereas retraction ofmandrel converts device from a linear to helicalconfiguration. Retention suture allows for simpledevice removal even after complete deploymentand locking.
712 Circulation August 7, 2001
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from
of device retrieval (snare-assisted recapture of a completelyreleased device). Indications for removal or retrieval includedprototype delivery system failure (n54), operator error(n52), or a combination of both (n51). Delivery systemfailure was a result of high friction between the mandrel andthe control catheter that resulted in poor coordination of thedeployment sequence. All 3 instances requiring snare-assistedremoval occurred early in the study and involved failure ofthe suture retrieval cord related to the friction issue men-tioned above. After this design issue was addressed, thisproblem disappeared. Retrieval was performed with a com-mercially available Amplatz gooseneck snare (Microvena)and was achieved without incident in the aorta and right andleft atria. The helical design and smooth contour of the devicemade snare capture and removal through the bloodstreameasy and atraumatic.
Efficacy–Closure RateTwenty-one animals (88%) had immediate complete ASDclosure as determined by TEE and right atrial angiography.Three were noted to have trivial residual shunts immediatelyafter device placement. At 2-week follow-up, all had com-plete ASD closure as judged by TEE. One animal wassubsequently found to have a 2- to 3-mm residual shunt seenonly with left atrial angiography and epicardial contrastechocardiography before euthanasia 3 months after implan-tation. No other animal had evidence of a residual shunt byangiography, TEE, epicardial contrast echocardiography, orautopsy examination (Figure 4). The overall complete closurerate was 95%, with 1 small residual shunt that was notdetectable by standard noninvasive imaging methods.
Device Performance and AppearanceBecause of the relatively small chamber size and prominentcrista terminalis found in the canine heart, 11 of 24 devices
had a somewhat flared, rather than parallel, appearanceimmediately after implantation. Interestingly, follow-up flu-oroscopy demonstrated progressive realignment of the disksin 7 of these animals, resulting in a parallel orientation of thedisks over time. This phenomenon suggests that the nitinolframe adapted to the unfavorable topography of the crowdedatria in this model for a period of time after implantation.
In 1 case, the flared disk appearance became more pro-nounced with time. A fracture of the wire frame was detected120 days after implantation. A review of the procedure andexamination of the frame at explantation suggested that the
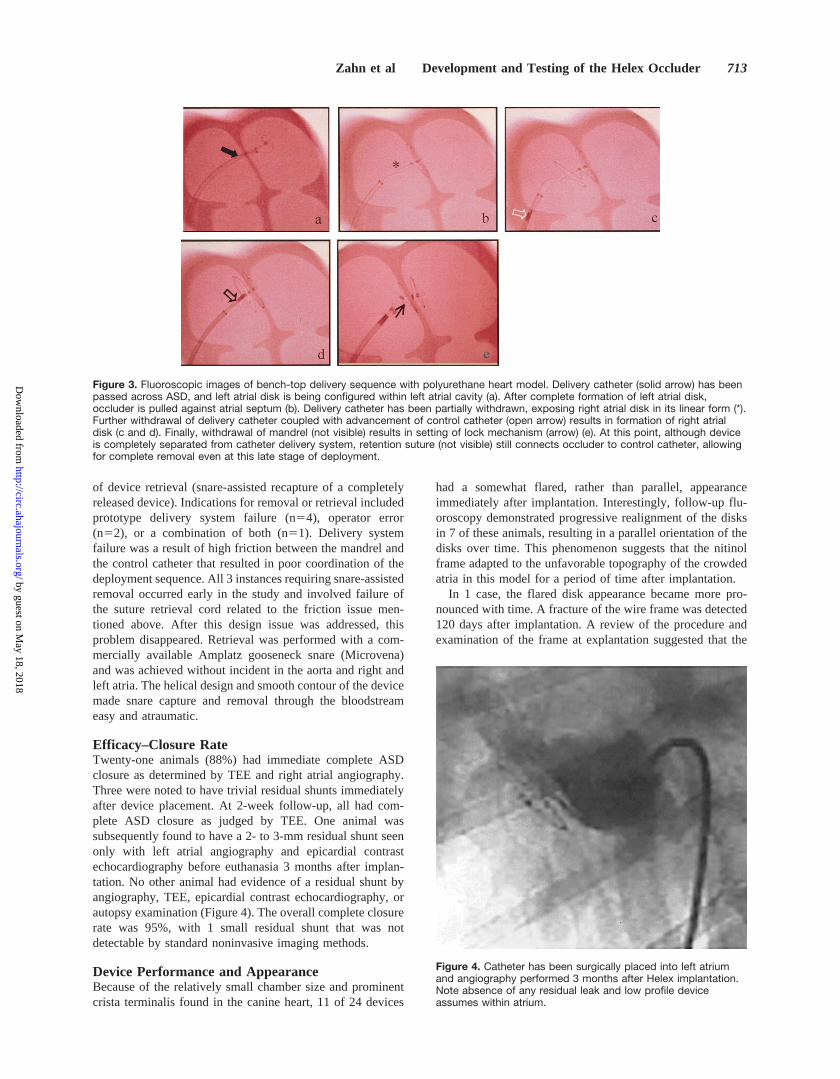
Figure 3. Fluoroscopic images of bench-top delivery sequence with polyurethane heart model. Delivery catheter (solid arrow) has beenpassed across ASD, and left atrial disk is being configured within left atrial cavity (a). After complete formation of left atrial disk,occluder is pulled against atrial septum (b). Delivery catheter has been partially withdrawn, exposing right atrial disk in its linear form (*).Further withdrawal of delivery catheter coupled with advancement of control catheter (open arrow) results in formation of right atrialdisk (c and d). Finally, withdrawal of mandrel (not visible) results in setting of lock mechanism (arrow) (e). At this point, although deviceis completely separated from catheter delivery system, retention suture (not visible) still connects occluder to control catheter, allowingfor complete removal even at this late stage of deployment.
Figure 4. Catheter has been surgically placed into left atriumand angiography performed 3 months after Helex implantation.Note absence of any residual leak and low profile deviceassumes within atrium.
Zahn et al Development and Testing of the Helex Occluder 713
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

fracture was secondary to kinking of the device within thedelivery catheter before implantation, coupled with the largesize (25 mm) of the device for the small canine atrium. Thiscombination led to excessive stress forces placed on the wireframe that exceeded the known tolerance limits, resulting infracture. Importantly, at explantation, there was neither anyevidence of thrombosis on the device surface nor microscopicevidence of distant thromboembolism. There was no residualleak, and the device posed no threat to the surroundingcardiac structures.
Device Mechanical Integrity TestingAfter enzymatic digestion of the atrial septum, scanningelectron microscopy was performed examining the nitinolframe for evidence of excessive wear or fatigue (Figure 5).Other than the fractured device discussed previously, wefound no evidence of wear or fatigue at any time afterimplantation.
Nickel AssayFive tissue samples were obtained from 8 dogs (3 testsamples in close proximity to the device and 2 controlsamples obtained.1 cm from the device perimeter) and
analyzed for nickel content at 3-, 6-, and 12-month intervalswith inductively coupled plasma/mass spectrometry. Analysiswas performed with a split ANOVA plot. No statisticaldifference was found between test and control samples takenat any time interval (the lower test limit was 0.025 ppm), norwas any difference between the average nickel concentrationsfound at 3, 6, or 12 months.
PathologyPathological examination of the heart and distal organs wasperformed at 1, 3, 6, and 12 months after implantation.Microscopic evaluation was performed on the organs of alldogs at each time frame and on the devices of 5 dogs at 1month, 1 dog at 3 months, 4 dogs at 6 months, and 3 dogs at12 months after placement. Devices used for mechanicalintegrity testing were not available for microscopicevaluation.
There was no gross evidence of thrombosis on the devicesurface or within any of the cardiac chambers at any timeafter implantation (Figure 6). At 1 and 6 months, resolvingmicrothrombi were observed on the surface of each device.Microthrombi were not visible grossly, occurred in lownumbers, and appeared to be part of the healing process.Microthrombi were not visible at 1-year follow-up. In noanimal was there any gross or microscopic evidence of new orold thromboembolism in the brain, lungs, or kidney.
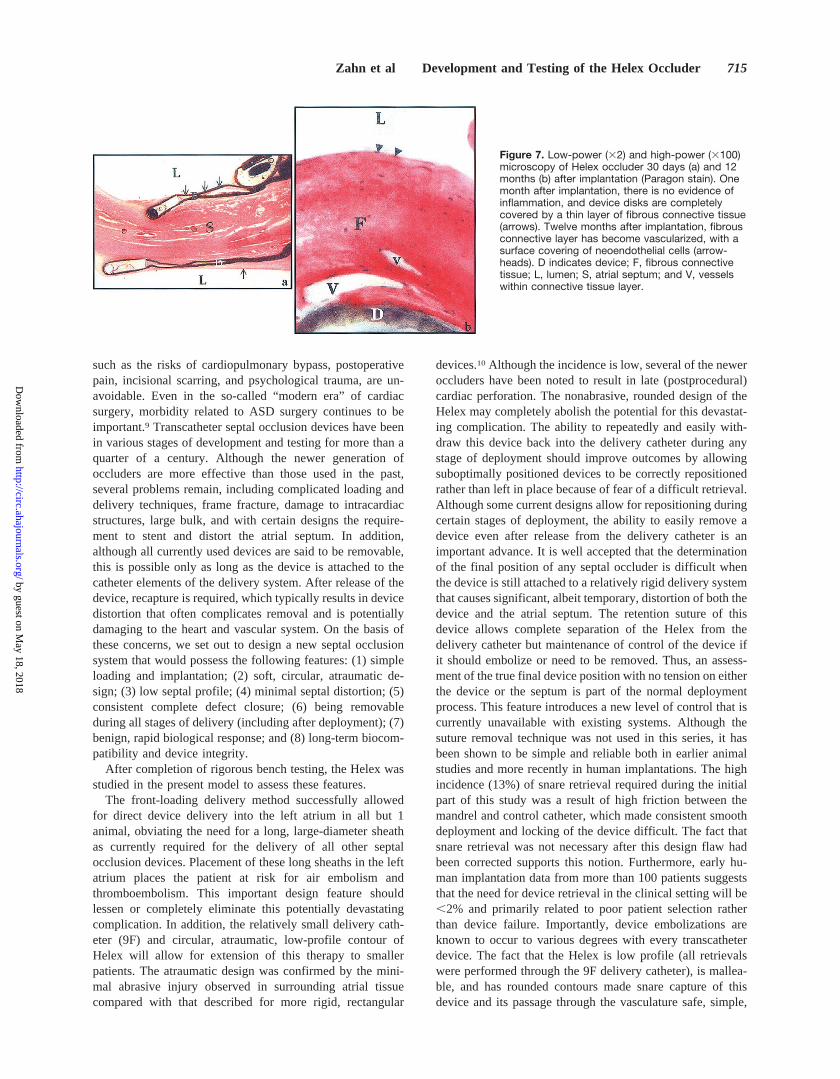
By 1 month after implantation, all devices were nearlycompletely covered by a thin layer of fibrous connectivetissue that deeply infiltrated the interstices of the ePTFE(Figure 7). A layer of spindle-shaped endothelium-like cellscovered the luminal surfaces of the device. Areas not coveredby fibrous connective tissue were generally located at themargins of the device, associated with areas of separationbetween the device and the septal surface. These areasappeared to be a result of the topography and small size of thedog atrium. Further development and maturation of thedevice covering was observed over time. At 6-month follow-up, 2 small nodules of fibrous connective tissue were attachedto the atrial septum, immediately adjacent to a device in 1dog. They appeared to be the result of the device marginabrading the septum. Similar nodules were observed in 2 dogsat 1-year follow-up. All nodules were firmly adherent to themyocardium and were of no hemodynamic significance.
DiscussionCardiac surgery is a relatively safe and time-tested methodfor closing secundum atrial septal defects. As with all opensurgical procedures, however, certain aspects of this therapy,
Figure 5. Scanning electron microscopy (3100) of an explanteddevice after enzymatic digestion to remove tissue. No evidenceof metal wear was observed.
Figure 6. Gross examination of right atrial disk 1month (a) and left atrial disk 1 year (b) after implan-tation. Device assumes a low profile and is exten-sively adhered to septum. There is no evidence ofthrombosis on device surface or within surroundingchamber.
714 Circulation August 7, 2001
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from
such as the risks of cardiopulmonary bypass, postoperativepain, incisional scarring, and psychological trauma, are un-avoidable. Even in the so-called “modern era” of cardiacsurgery, morbidity related to ASD surgery continues to beimportant.9 Transcatheter septal occlusion devices have beenin various stages of development and testing for more than aquarter of a century. Although the newer generation ofoccluders are more effective than those used in the past,several problems remain, including complicated loading anddelivery techniques, frame fracture, damage to intracardiacstructures, large bulk, and with certain designs the require-ment to stent and distort the atrial septum. In addition,although all currently used devices are said to be removable,this is possible only as long as the device is attached to thecatheter elements of the delivery system. After release of thedevice, recapture is required, which typically results in devicedistortion that often complicates removal and is potentiallydamaging to the heart and vascular system. On the basis ofthese concerns, we set out to design a new septal occlusionsystem that would possess the following features: (1) simpleloading and implantation; (2) soft, circular, atraumatic de-sign; (3) low septal profile; (4) minimal septal distortion; (5)consistent complete defect closure; (6) being removableduring all stages of delivery (including after deployment); (7)benign, rapid biological response; and (8) long-term biocom-patibility and device integrity.
After completion of rigorous bench testing, the Helex wasstudied in the present model to assess these features.
The front-loading delivery method successfully allowedfor direct device delivery into the left atrium in all but 1animal, obviating the need for a long, large-diameter sheathas currently required for the delivery of all other septalocclusion devices. Placement of these long sheaths in the leftatrium places the patient at risk for air embolism andthromboembolism. This important design feature shouldlessen or completely eliminate this potentially devastatingcomplication. In addition, the relatively small delivery cath-eter (9F) and circular, atraumatic, low-profile contour ofHelex will allow for extension of this therapy to smallerpatients. The atraumatic design was confirmed by the mini-mal abrasive injury observed in surrounding atrial tissuecompared with that described for more rigid, rectangular
devices.10 Although the incidence is low, several of the neweroccluders have been noted to result in late (postprocedural)cardiac perforation. The nonabrasive, rounded design of theHelex may completely abolish the potential for this devastat-ing complication. The ability to repeatedly and easily with-draw this device back into the delivery catheter during anystage of deployment should improve outcomes by allowingsuboptimally positioned devices to be correctly repositionedrather than left in place because of fear of a difficult retrieval.Although some current designs allow for repositioning duringcertain stages of deployment, the ability to easily remove adevice even after release from the delivery catheter is animportant advance. It is well accepted that the determinationof the final position of any septal occluder is difficult whenthe device is still attached to a relatively rigid delivery systemthat causes significant, albeit temporary, distortion of both thedevice and the atrial septum. The retention suture of thisdevice allows complete separation of the Helex from thedelivery catheter but maintenance of control of the device ifit should embolize or need to be removed. Thus, an assess-ment of the true final device position with no tension on eitherthe device or the septum is part of the normal deploymentprocess. This feature introduces a new level of control that iscurrently unavailable with existing systems. Although thesuture removal technique was not used in this series, it hasbeen shown to be simple and reliable both in earlier animalstudies and more recently in human implantations. The highincidence (13%) of snare retrieval required during the initialpart of this study was a result of high friction between themandrel and control catheter, which made consistent smoothdeployment and locking of the device difficult. The fact thatsnare retrieval was not necessary after this design flaw hadbeen corrected supports this notion. Furthermore, early hu-man implantation data from more than 100 patients suggeststhat the need for device retrieval in the clinical setting will be,2% and primarily related to poor patient selection ratherthan device failure. Importantly, device embolizations areknown to occur to various degrees with every transcatheterdevice. The fact that the Helex is low profile (all retrievalswere performed through the 9F delivery catheter), is mallea-ble, and has rounded contours made snare capture of thisdevice and its passage through the vasculature safe, simple,
Figure 7. Low-power (32) and high-power (3100)microscopy of Helex occluder 30 days (a) and 12months (b) after implantation (Paragon stain). Onemonth after implantation, there is no evidence ofinflammation, and device disks are completelycovered by a thin layer of fibrous connective tissue(arrows). Twelve months after implantation, fibrousconnective layer has become vascularized, with asurface covering of neoendothelial cells (arrow-heads). D indicates device; F, fibrous connectivetissue; L, lumen; S, atrial septum; and V, vesselswithin connective tissue layer.
Zahn et al Development and Testing of the Helex Occluder 715
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

and atraumatic. These same characteristics may allow forsuccessful ASD closure with smaller device/defect ratios,thereby further extending the age and size of patients inwhom it may be used. Although not specifically addressed inthis study, it appears that device/defect ratio as small as 1.5:1to 1.6:1 may be ideal with this device. Coupled with theminimalist design, the amount of implanted material associ-ated with Helex ASD closure will be considerably less thanwith other devices. Although implantation of large, bulkydevices into growing children has not proved to be hazardous,intuitively one would think the less intravascular materialimplanted the better. Although the Helex possesses a nickel-titanium frame, the small amount of metal is nearly com-pletely covered by ePTFE. The normal levels of nickel foundin adjacent tissue during this study suggest that nickelleaching will not be a problem with this device. The lack ofany evidence of thromboembolic events, early appearance ofa benign tissue response, and neoendothelial covering of thedevice support long-term biocompatibility. Furthermore, themajor component of the Helex, ePTFE, has been used incardiac surgery for decades and has a proven record of safetyand durability. Although a single instance of wire fracturewas observed, it appears to have been related to excessiveforces placed on that particular device as a result of a faultyprototype delivery system coupled with oversizing of thedevice for the small canine atrium. If the delivery system ismodified and the device properly sized, frame fracturesshould not occur. The initial nonparallel appearance of thedisks in 46% of the implantations reflects the malleablenature of this low-profile device, which can adapt to varyingatrial topography compared with more rigid devices, whichmust distort the atrial septum and surrounding structures toassume their designed configurations. The ability to adjust tothe atrial terrain is most likely advantageous. For example, inthe common case involving absence of the anterior/superiorseptal rim, where the posterior wall of the aorta composes thismargin of the ASD, the Helex disks can splay around theaorta, providing atraumatic, improved closure rates. Finally,the high closure rates observed both initially and in follow-upsuggest that the Helex occluder is very effective for completeearly closure of secundum ASD, thus predicting a very lowrequirement for reintervention of any kind.
Study LimitationsThe canine atrial anatomy differs significantly from that ofhumans, which makes it an imperfect model. The right atriumpossesses a very prominent crista terminalis, and the septalsurfaces on both sides are quite small compared with thehuman (even that of a small child). This resulted in less direct
contact between the device and septal surface than we expectwill occur in the human heart. Surgically created atrial septaldefects cannot duplicate the noncircular shape and variableposition of secundum atrial septal defects seen in humans. Inparticular, we were unable to assess device performancewhen a portion of the defect rim is deficient.
ConclusionsThe new Helex occluder appears to offer a number ofadvantages over currently existing transcatheter occlusiondevices. The ease of implantation, atraumatic design, highclosure rate, simple removal technique, and compatible bio-logical profile shown in this animal study suggest that thisdevice will be a useful addition to the therapy alreadyavailable for treatment of ASD. The data reported heresupport the initiation of multicenter controlled human clinicaltrials.
AcknowledgmentsThis work was funded by a grant from W.L. Gore and Associates,Flagstaff, Ariz. We wish to thank Dena Anderson, DVM; NickMacri, DVM, MS, PhD; Melanie Manning, DVM; Nitin Salunke,PhD; and Paul Sawyer, MS for their invaluable contributions to thiswork.
References1. King TD, Thompson SL, Steiner C, et al. Secundum atrial septal defect:
non-operative closure during cardiac catheterization.JAMA. 1976;235:2506–2509.
2. Rao PS, Sideris EB, Hausdorf G, et al. International experience withsecundum atrial septal defect occlusion by the buttoned device.AmHeart J. 1994;128:1022–1035.
3. O’Laughlin MP. Catheter closure of secundum atrial septal defects.TexHeart Inst J. 1997;24:287–292.
4. Hausdorf G, Schneider M, Fink C, et al. Transcatheter closure of atrialseptal defects within the oval fossa: medium-term results in childrenusing the “ASDOS”-technique.Cardiol Young. 1998;8:462–471.
5. Masura J, Gavora P, Formanek A, et al. Transcatheter closure ofsecundum atrial septal defects using the new self-centering amplatzerseptal occluder: initial human experience.Cathet Cardiovasc Diagn.1997;42:388–393.
6. Prieto LR, Foreman CK, Cheatham JP, et al. Intermediate-term outcomeof transcatheter secundum atrial septal defect closure using the Bardclamshell septal umbrella.Am J Cardiol. 1996;78:1310–1312.
7. Sievert H, Babic UU, Ensslen R, et al. Transcatheter closure of large atrialseptal defects with the Babic system.Cathet Cardiovasc Diagn. 1995;36:232–240.
8. Das GS, Voss G, Jarvis G, et al. Experimental atrial septal defect closurewith a new, transcatheter, self-centering device.Circulation. 1993;88(4 pt1):1754–1764.
9. Galal MO, Wobst A, Hatle HL, et al. Peri-operative complications fol-lowing surgical closure of atrial septal defect type II in 232 patients: abaseline study.Eur Heart J. 1994;15:1381–1384.
10. Kuhn MA, Latson LA, Cheatham JP. Biological response to Bardclamshell septal occluders in the canine heart.Circulation. 1996;93:1459–1463.
716 Circulation August 7, 2001
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

Evan M. Zahn, Neil Wilson, Warren Cutright and Larry A. LatsonAtrial Septal Defect Occlusion System
Development and Testing of the Helex Septal Occluder, a New Expanded Polytetrafluoroethylene
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2001 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/hc3301.092792
2001;104:711-716Circulation.
http://circ.ahajournals.org/content/104/6/711Wide Web at:
The online version of this article, along with updated information and services, is located on the World
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe middle column of the Web page under Services. Further information about this process is available in thethe online version of the published article for which permission is being requested is located, click Request Permissions in
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. OnceCirculation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from












![Post Traumatic Ventricular Septal Defect Closure Using an … · ensure survival [3].In this procedure, an Ampletzer VSD Occluder has usually been employed [4], or occasionally, an](https://img.pdfslide.net/doc/110x75/602593159134b37e87220abe/post-traumatic-ventricular-septal-defect-closure-using-an-ensure-survival-3in.jpg)














