Embed Size (px)
Citation preview

Development and Use of Neighborhood Health Analysis:Residential Mobility in Context
Katie Murray, The Providence PlanThe Urban Institute April 24, 2003

Why Investigate Residential Mobility?
Known levels of mobility in Providence student population – annual snapshot, at least 1 in 4 students stays in Providence but changes residence
Health Dept. perspective: challenges of serving urban mobile populations
Neighborhood strengthening agendas: strategies that will serve mobile families
Prior research confirms impacts of residential mobility on learning and performance. Minimal research of impact on childhood health outcomes
Opportunity to access unique Health Dept. data set for address tracking

What is the extent of childhood residential mobility in RI?
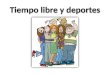
Residential Mobility among Providence Public School Students, 1987-2001
n=57,642
53%
23%
12%
7%
3% 3%
0 moves 1 move 2 moves 3 moves 4 moves 5-11moves
Residential Mobility among Children in KidsNet System, 1997-2001 births
n=65,795
66%
22%
7%
3%1% <1%
0 moves 1 move 2 moves 3 moves 4 moves 5-7moves

HEALTH, 1997-2001
Residential mobility impacts whether a child receives continuous care from the same primary care provider.
Residential Mobility and Childhood Health Outcomes
Residential Mobility and Number of Different Primary Care Providers
84%
77% 76%74%
16%
20%23% 24%
26%
80%
0 moves 1 move 2 moves 3 moves 4+ moves
1 provider
2 or more providers

Residential Mobility and Childhood Health Outcomes
Children in mobile families have less contact with any primary care provider than other children. Most notable among children less than 2 years old.
Residential mobility does not affect whether a child received the required 2 blood lead screenings by age 3.
Children born to teens, single women, women with low levels of education or income, and women who received inadequate prenatal care are most likely to experience mobility at a young age.
Two-thirds of mobile children were identified as “development risk positive” at birth by RI Department of Health.

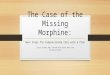
Residential Mobility and Educational Outcomes Students in mobile households are 2-4 times more likely to repeat at least one grade than students who don’t move.
Providence School Dept, 1987-2001
13%
39%
47%
55%
61%
73%
26%
No moves 1 move 2 moves 3 moves 4 moves 5 moves 6+ moves
Students that repeated at least one grade by number of moves

Residential Mobility and Educational Outcomes
Children in residentially stable households are twice as likely to meet the required standards in tests of reading and math than mobile children.
Residential mobility correlate with absenteeism – students who moved missed an average of 19 days of school compared to 13 days for students who did not move.

19
29
34
2928
36 3521
22
23
27
3126
25
32
22
23
2522
23
2520
614
16
30N/A
33
24
11
24
33
30N/A
16
146
20 25
23
22 25
23
22
32
25
2631
27
23
22
213536
2829
34
29
1213
17
3718
15
3
7
2
10 11
8
4
5
9
Early childhood mobility
Early childhood and student residential mobility
Student mobility
Shading denotes tracts where mobility exceeded 1SD of city average:
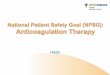
Census Tracts More than One Standard Deviation above the City Average in Residential Mobility
Census Tracts with High Rates of Residential Mobility
Census tracts with extreme residential mobility also exhibited high crime and poverty rates, below average property values, and poor indicators of maternal and child health.

24
21
23
27 30N/A
33
32
31
34
35
28 29
20
18
1716
151
22
19
13
14
12
3
2
5
64
7
8
36
37
26
25
9
1110
Census Tracts More than One Standard Deviation above the City Average in Selected Areas of Child Health and Neighborhood Well-Being
0123
456*7
Cumulative factors where tract exceeds 1 SD of city average
*Note: no tract exceeded the city average in six areas
As measured by 15 indicators of well-being
Residential Mobility Student Early Childhood Maternal & Child HealthLess than 12 years of educationTeen birthsDelayed prenatal careInsufficient prenatal visitsLow birth weightBlood lead exposure CrimePart I violentPart I property IncomeMedian family income Property CharacteristicsVacant dwelling unitsRenter occupancy rates
Most Distressed Tracts

Next Steps
Phase II: Modeling and analysis with local social epidemiologist
Parent Consultants to have discussions with parents – why do they move?
Tie efforts for outreach to neighborhood based Community Health Centers
Tie into existing family strengthening agendas: Making Connections and Ready to Learn Providence
Revisit developmental risk criteria or more strategically use the criteria to target mothers/newborns needing service

Full Report at www.provplan.org