Embed Size (px)
Citation preview

Hernandez 1
Dexmedetomidine for Alcohol Withdrawal Syndrome: Should we add it to the tab?
Lauren Hernandez, Pharm.D. PGY2 Critical Care Pharmacy Resident
University Health System, San Antonio, TX Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy
Pharmacotherapy Education and Research Center, University of Texas Health Science Center at San Antonio
September 20, 2013
Learning Objectives
1. Describe the pathophysiology and neurotransmitters involved with alcohol withdrawal
2. Identify characteristics, timing, and severity of clinical manifestations
3. Define the current pharmacologic options and strategies for treatment
4. Evaluate the role of dexmedetomidine to treat alcohol withdrawal

Hernandez 2
Alcohol-Related Epidemiology
I. More than 50% of Americans (>12 years old) drink alcohol1,2
A. Binge drinking > 4 to 5 drinks on one occasion: 23%
B. Heavy drinking > 1 to 2 drinks per day on average: 6.5%
C. Alcohol use disorders3
i. Abuse: drinking pattern leading to physical and psychological harm
ii. Dependence: cravings, alcohol withdrawal after cessation, and tolerance
II. Alcohol-related morbidity and mortality3,4,5
A. 1.2 million emergency room visits a year
B. 40% of intensive care unit (ICU) admissions related to alcohol abuse
C. 80,000 deaths per year
D. Estimated economic cost $200 billion per year
III. Alcohol withdrawal syndrome (AWS) morbidity and mortality1,4
A. Develops in 8% of hospital admissions
i. One-third require ICU admission
ii. Higher prevalence in trauma patients
B. ICU complications6
i. 30% require mechanical ventilation
ii. Infections
iii. Increased ICU length of stay
C. Mortality
i. Increases three-fold in post-surgical and trauma patients
ii. Decreased from 50% to 10% since first recognition of syndrome
Alcohol Withdrawal Syndrome (AWS)
I. Pathophysiology A. Main central nervous system (CNS) neurotransmitters (NT) affected
1,3,7
i. Inhibitory NT: gamma-aminobutyric acid (GABA) binds to GABAA receptor ii. Excitatory NT: glutamate binds to N-methyl-d-aspartate (NMDA) receptor
De
B. Sympathetic nervous system4,8,9
i. Norepinephrine (NE) levels increased
1. Desensitization of alpha-2 receptor
2. Increased corticotropin-releasing hormone
ii. Resulting autonomic hyperactivity
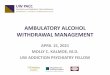
Acute exposure ↑ GABA activation
↓ glutamate activation
Chronic exposure↓GABA levels
↓ GABAA receptors & sensitivity↑ NMDA receptors
Abrupt cessation↑Glutamate binding to
NMDA receptors↓GABA binding to GABAA receptors
↓ Level of consciousness ↓ Cognition
Tolerance ↑Alcohol required for same effects
Brain hyperexcitability Results in AWS
Figure 1. Pathophysiology of alcohol withdrawal

Hernandez 3
C. Dopaminergic activity4,10
i. Increased dopamine levels
ii. Possible role in hallucinations and delirium tremens (DT)
D. Electrolyte disturbances4
i. Magnesium blocks NMDA receptors
ii. Hypomagnesemia linked to risk of seizures and cardiac arrhythmias
E. Kindling hypothesis8,11
i. Each period of alcohol cessation causes an intense excitatory CNS process
ii. Altered transmission of GABA, glutamate and NE in neurons
iii. Withdrawal symptoms become more severe with repeated occurrences of withdrawal
iv. Continual alterations in NTs increase risk for seizures and DTs
II. Diagnosis and clinical manifestations A. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
12
Table 1. Criteria for alcohol withdrawal
A. Cessation of (or reduction in) alcohol use that has been heavy and prolonged B. Two (or more) of the following, developing within several hours to a few days after criterion A
1. Autonomic hyperactivity (e.g. sweating or pulse rate >100 beats/min) 2. Increased hand tremor 3. Insomnia 4. Nausea or vomiting 5. Transient visual, tactile, or auditory hallucinations or illusions 6. Psychomotor agitation 7. Anxiety 8. Grand tonic-clonic seizures
C. The signs or symptoms in criterion B cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
D. The signs or symptoms are not attributable to another medical condition and are not better explained by another mental disorder, including intoxication or withdrawal from another substance
B. Clinical manifestation timeline1
Autonomic Hyperactivity Diaphoresis Nausea Vomiting Anxiety Tremor Agitation Tachycardia
Hallucinations Visual Tactile Less common: Auditory Lasts: 1-6 days 30% of patients
Withdrawal Seizures Generalized tonic-clonic May occur as early as 2 hours 10% of patients
Delirium Tremens or Alcohol Withdrawal Delirium Disorientation (delirium) Agitation Hallucinations Tachycardia Hypertension Fever Lasts up to 7 days 5% of patients
Figure 2. Alcohol withdrawal symptoms timeline1

Hernandez 4
III. Screening and assessment severity tools
A. Screening for unhealthy alcohol use3,13
i. CAGE questionnaire13
1. Four questions to assess cut down, annoyance, guilt, eye opener
2. Validated tool in non-ICUs to detect alcoholism and risk of AWS
3. ICU data limited and does not predict severity or outcome13
ii. Single screening questions determining quantity and frequency of heavy drinking days
iii. Prior episodes of alcohol withdrawal
B. Assessment severity tools used in AWS4,6,13,14
i. Scoring symptoms assess severity, progression and assist in management
ii. Clinical Institute of Withdrawal Assessment for Alcohol (CIWA-Ar) (Appendix A.)14
1. Developed for non-ICU patients and not validated in ICU patients
2. Includes 10 items requiring patient participation
3. CIWA-Ar > 10 warrants management and reassessment a. Score 10 -18 correlates with moderate to severe
b. Score >20 consistent with severe
iii. CIWA-Ar studied in ICU setting 13
1. CIWA-Ar >20 used as trigger for therapy and reflected severe AWS
2. Mechanically-ventilated patients often excluded
3. Variable target CIWA-Ar scores and assessment intervals
iv. Validated ICU sedation scales used in AWS studies (Appendix A.)13
1. Included mechanically ventilated patients
2. Riker Sedation-Agitation Scale (SAS)
a. Score >5 triggered pharmacologic therapy with target goal 3 to 4
b. Assessment intervals varied from every hour to every 4 hours
3. Richmond Agitation-Sedation Scale (RASS)
a. Used to titrate pharmacologic therapy to goal 0 to -1
v. Confusion Assessment Method-ICU (CAM-ICU) (Appendix A.)
1. Validated tool to detect delirium but not used solely to manage AWS
IV. Risk factors3,13
Figure 3. Risk factors for severe course of AWS
Severe Course of AWS
Prior Alcohol -Related Seizures
Alcohol Dependence
Prior AWSSeizures
and/or DTs
CIWA >20
Comorbid Medical Conditions

Hernandez 5
Management of AWS
I. Goals of therapy1
A. Alleviate symptoms B. Prevent progression of symptoms C. Treat underlying comorbidities D. Minimize sedation and respiratory suppression
II. Supportive care1,4
A. Fluid resuscitation
i. Fluid losses and intravascular volume depletion commonly observed B. Nutritional supplementation
6
i. Patients have inadequate nutritional intake and severe malnutrition ii. Thiamine
iii. Folic acid iv. Multi-vitamin
III. Benzodiazepines1,6
A. First-line therapy1,15
B. Mechanism of action (MOA)1
i. GABAA receptor agonist and glycine-mimetic effects
ii. Pharmacologic properties
1. Sedative
2. Anticonvulsant
3. Anxiolytic
4. Muscle relaxant
iii. Unfavorable adverse effects
1. Respiratory depression
2. Cardiovascular instability
C. Efficacy 15,16,17
i. Reduce development of alcohol withdrawal delirium
ii. Decrease seizure incidence and recurrent seizures
iii. No evidence to support one benzodiazepine over another
Table 2. Available benzodiazepine pharmacokinetics4,18
Generic (Brand) Equivalent Dose (mg)
Routes of Administration
Onset of Action (min)
Half-life (hours)
Hepatic Metabolism/ Active Metabolite
Chlordiazepoxide (Librium®)
25 Oral 30-120 7-28 CYP enzymes Active metabolite
Lorazepam (Ativan®)
1 Oral, IM, IV, continuous infusion
15-20 8-15 Conjugation
Midazolam (Versed®)
2 Oral, IM, IV, continuous infusion
2-5 3-11 CYP enzymes Active metabolite
Diazepam (Valium®)
5 Oral, IM, IV 2-5 20-120 CYP enzymes Active metabolite
IM: intramuscular, IV: intravenous

Hernandez 6
D. Symptom-triggered vs fixed-schedule doses1,6
i. Benzodiazepines originally administered in fixed-scheduled doses
1. Predetermined dosing taper for 3 to 5 days for all patients
ii. Symptom-triggered directed by CIWA-Ar protocol allows for individualized therapy1,19
iii. Daeppen et al. randomized 117 alcohol dependent patients in a treatment facility19
1. Symptom-triggered (CIWA>8: administer dose; target score <8) vs fixed-dose
2. Results: 39% symptom-triggered received medications vs 100%, ↓treatment
duration, and six- fold less oxazepam use
iv. Spies et al. randomized 44 patients with AWS after ICU admission20
1. Continuous infusion therapy group (ITG) vs bolus therapy group (BTG) targeting
CIWA-Ar (CIWA-Ar >20 trigger for therapy)
2. BTG ↓ benzodiazepine amount used
3. ITG ↑ AWS duration, mechanical ventilation, pneumonia, ICU stay
v. Symptom-triggered benefits in non-ICU patients are similar to ICU; limitations on
severity scale validity may make it difficult to implement20,21
IV. Anticonvulsants1,10
A. Carbamazepine
i. MOA: Limit influx of sodium ions and other unknown mechanisms
ii. Better than placebo and equally effective to lorazepam for mild to moderate AWS
B. Valproic acid
i. MOA: Increase availability of GABA or enhance GABA action
ii. Compared to placebo decreased benzodiazepine use for symptom control in mild AWS
V. Antipsychotics1,6
A. Haloperidol, phenothiazines (i.e. chlorpromazine)
B. MOA: Dopamine antagonists
C. Adjunctive to benzodiazepines for symptom control; limited comparative studies
D. Undesirable effects
i. Decrease seizure threshold
ii. Increased risk of delirium with haloperidol
iii. QT prolongation
VI. Ethanol1,6
A. Use dates back to pre-benzodiazepine management
B. Primarily used in surgical services and as a prophylaxis measure
C. Controversial issues
i. Efficacy
ii. Dosing and administration
iii. Complications
VII. Adrenergic agents1,4
A. Control autonomic hyperactivity
B. Beta-blockers1,4
i. Can help to reduce tachycardia and hypertension
ii. Delirium found to be potential side effect of use
C. Alpha-2 agonist: clonidine8
i. MOA: Inhibits NE release from presynaptic neurons
ii. Clonidine comparative studies8,22-25

Hernandez 7
Table 3. Clonidine for AWS22-25
Author (N) Patients Intervention Results
Baumgartner et al.
22
61 Alcohol dependent Excluded- seizure history
Clonidine 0.2-0.6mg/day vs Chlordiazepoxide 50-150mg/day X 4 days Adjunct meds: APAP
Clonidine favored ↓ Alcohol withdrawal scale (p<0.02) ↓Mean SBP, HR (p<0.01, p<0.001) No differences HARS, RR, diaphoresis, restlessness
Robinson et al.
23
32 Detox unit Excluded- major AWS, seizure history
Clonidine 0.3-0.9mg/day vs chlormethiazole 1000-3000mg/day X 4 days Adjunct meds: None
8 study withdrawals: clonidine group (p=0.002) Reasons: seizures, hallucinations, orthostatic hypotension
Adinoff B.24
25 Alcohol dependent Excluded- seizure history
Clonidine 0.1mg, diazepam 10mg, alprazolam 1mg, or placebo for CIWA-Ar >10, every hour until CIWA-Ar <5 or 8 doses
Alprazolam favored Fewer doses vs clonidine (p<0.04) ↓CIWA-Ar vs clonidine (p<0.03)
Spies et al.25
159 Trauma ICU Alcohol dependent
IV bolus, then infusion to target CIWA-Ar<10 Flunitrazepam/clonidine (FC) vs chlormethiazole/haloperidol (CH) vs flunitrazepam/haloperidol (FH)
CH group ↑ MV duration (p=0.03) FC group ↓PNA (p=0.040) ↑bradycardia, 1
st-degree AV block,
hypotension (p=0.005) *p<0.05 Abbreviations: APAP: acetaminophen; SBP: systolic blood pressure; HR: heart rate; HARS: Hamilton anxiety rating scale; RR: respiratory rate; ICU: intensive care unit; IV: intravenous; MV: mechanical ventilation; PNA: pneumonia. Alcohol withdrawal scale = BP, HR, RR, tremor, diaphoresis, restlessness.
iii. Summary of trials8
1. Study design included randomized, double-blind or rater-blind
2. ↓ BP and HR were benefits from clonidine on alcohol withdrawal symptoms
3. Clonidine monotherapy associated with significant seizure occurrence
4. Severe bradycardia complication with IV clonidine therapy
iv. Place in therapy8
1. Adjunct to benzodiazepine therapy for control of sympathetic symptoms
2. Higher doses to achieve control resulted in greater risk for adverse effects
D. Barbiturates1,6
i. MOA: GABA-A agonist, weak NMDA inhibitor
ii. Adjunctive agent to benzodiazepine
1. Gold et al.26
studied a strategy for patients resistant to benzodiazepines
a. Persistent agitation for 1 hour after ↑ diazepam doses to 100-150mg
b. Phenobarbital added in ↑ doses (65, 130, 260mg) to control agitation
c. Need for mechanical ventilation ↓ compared to pre-strategy group
iii. Adverse effects
1. Respiratory depression
2. Hypotension
E. Propofol1,6
i. MOA: GABAA agonist and NMDA antagonist
ii. Adjunctive agent to benzodiazepine
1. Gold et al.26
gave bolus or continuous infusion if agitation persisted with
escalating doses of diazepam and phenobarbital
2. McCowan et al.27
reported successful treatment with propofol continuous
infusion in four DTs cases with limited response to high dose benzodiazepines
3. Both studies with continuous infusion required mechanical ventilation

Hernandez 8
iii. Adverse effects
1. Respiratory depression
2. Hypotension
3. Hypertriglyceridemia
4. Propofol infusion syndrome with prolonged high doses
F. Benzodiazepine resistant alcohol withdrawal (RAW)1,28
i. Large doses of benzodiazepines needed for withdrawal symptoms or DTs
ii. Hack et al.28
defined diazepam doses >50 mg in 1 hour or >200mg in 3 hours as
suggestive criteria for RAW
iii. Mechanism for resistance
1. Downregulation and decreased function of GABAA receptors
2. Level of resistance dependent on individual’s receptor dysregulation
iv. Complications26
1. 47% require intubation due to need for alternative sedatives
2. Increased length of stay
3. Increased risk for infections
v. Alternative sedative options26,27
1. Phenobarbital
2. Propofol
Dexmedetomidine (Precedex®)
I. MOA29,30
A. Selective central alpha-2 receptor agonist
B. Binds to pre- and post-synaptic adrenergic neurons in the central nervous system (CNS)
i. Pre-synaptic: prevents release of norepinephrine from synaptic vesicles
ii. Post-synaptic: inhibits sympathetic activation
C. Dose-dependent alpha-2 selectivity
II. Pharmacological effects29,30
A. CNS
i. Sedation
1. High density of alpha-2 receptors in locus coeruleus
a. Predominant noradrenergic nucleus in brain
b. Modulator of alertness
2. Cooperative sedation
a. Allows for easy awakening
b. Facilitates routine patient assessment
ii. Analgesia
1. Mechanism not fully understood
2. Activation at supraspinal and spinal sites reduces nociceptive transmission
B. Cardiovascular
i. Initial transient increase in blood pressure resulting in reduced heart rate
1. Occurs within first 10 minutes of infusion
2. Associated with loading dose
ii. Subsequently, blood pressure decreases 10-20% from baseline and heart rate stabilizes
1. Effect of inhibition of central sympathetic outflow
2. Decreased norephinephrine release

Hernandez 9
C. Respiratory
i. No inhibition of respiratory drive
ii. Additive effects on respiratory function in combination with anesthetics, sedatives,
hypnotics, and opioids
III. Pharmacokinetics29,30
A. Onset: 15-30 minutes
B. Distribution: rapid, steady-state volume of distribution: 118 L
C. Metabolism
i. t ½ : 2 hours; severe hepatic impairment ↓ clearance
ii. Hepatic glucuronidation and CYP450 enzymes
D. Excretion: 95% urinary
IV. Indications29
A. Approved in 1999 by Food and Drug Administration (FDA)
i. ICU sedation
1. Intubated and mechanically ventilated patients in ICU; not to exceed 24 hours
2. Continuously infused prior to, during, and post extubation; not necessary to
discontinue prior to extubation
ii. Procedural sedation
1. Nonintubated patients prior to and/or during surgical or other procedures
V. Distinguishing features from clonidine6,29,30
A. More effective sedative and analgesic
B. Increased specificity for alpha-2 receptor
i. 8 times more potent
C. Shorter half-life (2-3 vs 12-24 hours)
D. Greater titratability
Understanding the Potential for Dexmedetomidine in AWS 1,6,31
I. Agitation and autonomic hyperactivity control is essential in severe AWS and DTs
II. Benzodiazepine monotherapy may be insufficient for control1
A. Patient specific factors
B. Resistant alcohol withdrawal
i. Complications
1. Mechanical ventilation
2. Increase ICU stay
3. Increase infection
III. Drawbacks to alternative sedative therapy
A. Risk for respiratory depression requiring mechanical ventilation
B. Hemodynamic instability
IV. Dexmedetomidine
A. Provides sedation and decreases autonomic activity
B. No effect on respiratory function

Hernandez 10
Role of Dexmedetomidine in AWS
I. Case reports for treatment of alcohol withdrawal32,33
Table 4. DEX for treatment of alcohol withdrawal 32,33
Case 1 Case 2
Alcohol abuse history Severe alcohol dependence Previous AWS admissions, convulsions Last drink 3 days prior
Chronic alcohol abuse Previous AWS admissions Last drink 24 hour prior
Symptoms Convulsions, hallucinations, tremor, diaphoresis, delirium
Agitated, disoriented, combative, tremors, possible DTs,
Admission General ward ICU General ward ICU
Initial treatment First 48 hours: Diazepam 360mg, Haloperidol 12.5mg Thiamine 200mg
Oxazepam 30mg twice daily, Thiamine 100mg IV daily, Phenytoin ICU:↑ BZD dose, midazolam CI
DEX initiation/dose On admission to ICU Load: 0.5mcg/kg; CI 0.175 mcg/kg/hour
31 hours after hospital admission CI 0.2-0.7mcg/kg/hour
Adjunctive medications Diazepam 15mg/day, Haloperidol 5mg/day Midazolam CI
Symptom improvement Within 2 hours, ↓ symptoms, HR, restraints removed
Immediate, ↓ in tremor, confusion, agitation, ↓midazolam infusion rate
DEX duration 15.5 hours 39 hours (25 hours monotherapy)
DEX: dexmedetomidine; BZD: benzodiazepine; CI: continuous infusion
A. Take home points i. Significant alcohol history and possible DT presentations
ii. Dexmedetomidine initiated as symptoms worsened and benzodiazepine increased iii. Rapidly improved symptoms, restraint removal, HR, ↓ benzodiazepine dose
II. Abstracts 34-35
Table 5. Abstracts evaluating safety and efficacy of DEX for AWS34-35
Jacob S et al. 200834
Dailey RW et al. 201135
Study design Case series in ICU of 4 patients Case series in ICU of 10 patients
Airway intervention 2/4 prior to DEX None prior to DEX
Symptoms and severity Delirium, RASS 2 to 4, RAW, CIWA-Ar 20-30, Severe AWS or AWD, CIWA-Ar 26
Initial treatment Pt 1 & 2 CI midazolam 15-25mg/hour Pt 3 & 4 lorazepam 2-4mg every 1-2 hours
Diazepam 13mg/hour
DEX initiation Imminent intubation, facilitate extubation Not mentioned
DEX dose 0.2-0.7mcg/kg/hour Mean 0.7mcg/kg/hour (range 0.1-1.5)
DEX duration 24-29 hours Median 50 hours (range 7-206 hours)
Adjunctive meds No, benzodiazepine stopped Diazepam
Endpoints RASS score -1 to -2, CIWA-Ar <5 Extubation (2/2) 5 & 22 hours after drip Avoided intubation (2/2) No additional benzodiazepine, no seizures
↓ CIWA-Ar to 13* ↓diazepam to 3mg/hour* No intubation needed
Hemodynamics ↓BP, HR, no significant effects noted 5/10 SBP <100mmHg, 2/10 DEX held
*p <0.05; DEX: dexmedetomidine; AWD: alcohol withdrawal delirium; LOS: length of stay; PNA: pneumonia
A. Take home points
i. Severe AWS defined by CIWA-Ar, delirium, or RAW
ii. Dexmedetomidine ↓CIWA-Ar, RASS, HR, BP, benzodiazepine dosing, and possibly
facilitated extubation and prevented intubation
iii. Dexmedetomidine alone and adjunctive to benzodiazepines, no seizures reported
iv. Hypotension is a safety concern with dexmedetomidine

Hernandez 11
III. Review of published retrospective and prospective studies36-38
Table 6. Tolonen J, Rossinen J, Alho H, Harjola VP. Dexmedetomidine in addition to benzodiazepine-based sedation in patients with alcohol withdrawal delirium. Eur J Emerg Med 2012;[Epub ahead of print].
Objective Report safety and efficacy of DEX in patients classified with alcohol withdrawal delirium (AWD)
Study Design
Multi-center prospective study CAM-ICU and RASS performed daily Medications: diazepam, lorazepam, and/or haloperidol orally and/or IV to target RASS of zero;
thiamine 100mg daily for 3 days Delirium was defined as resolved when both RASS and CAM-ICU returned to normal DEX initiated at discretion of physician based on hospital sedation protocol
o Additionally, if standard benzodiazepine-based treatment failed or o Directly if it was obvious at admission that large amounts of benzodiazepines or
haloperidol were not tolerated
Patients Inclusion o Adult patients with AWD defined by CAM-ICU
Exclusion o Pregnancy, invasive ventilator support at admission
Statistics Data expressed as mean and standard deviation
Results Baseline characteristics o 18 patients were enrolled (male = 15, female =3), mean age 53.9 years o PMH and current diagnosis included CVD, ICH, RA, asthma, epilepsy, pancreatitis,
depression, bipolar, alcohol dementia, delirium Alcohol withdrawal treatment
o DEX initiation from admission ranged from day 1 to day 3 (majority day 1) o DEX mean max rate 1.5 mcg/kg/hour (SD 1.2); mean duration 23.9 hours (SD 18.4) o Mean cumulative dose (mg): diazepam 193.6 (SD 165.8), lorazepam 9.3 (SD 8.6),
haloperidol 26.5 (SD 25) AWS symptoms
o Mean (SD) admission RASS 1.1 (1.8), DEX start 1.4 (1.5), 24 hours from DEX start 0.3 (1.4) o Time to delirium resolution mean (SD): 3.8 (1.3) days
No patients were intubated Mean (SD) length of stay in ICU 7.1 (2.7) days, in hospital 12.1 (4.5) days Two patients required subsequent rehabilitation One patient died due to acute pancreatitis not related to DEX therapy
Authors Conclusion
DEX can be safe and effective for severe AWD refractory or intolerant to conventional therapy Escalation of therapy to anesthesia and intubation is avoided
Critique Retrospective study with no comparison or control group AWD diagnosed by CAM-ICU solely, with no mention of patients’ alcohol use history Refractory/intolerant to therapy not quantified and decided by physician RASS not validated for AWS and significance of improvement prior to and after DEX not reported Hemodynamic parameters to measure efficacy and safety not collected or reported
DEX: dexmedetomidine; CVD: cardiovascular disease; ICH: intracranial hemorrhage; RA: rheumatoid arthritis
A. Take home points
i. Patients with delirium defined by CAM-ICU but no clear distinction between delirium
caused by alcohol withdrawal or other factors (i.e. ICU)
ii. Adjunctive dexmedetomidine improved sedation and possibly avoided intubation
iii. Delirium resolution due to correction of underlying cause or environmental factors
iv. Safety of dexmedetomidine cannot be determined

Hernandez 12
Table 7. DeMuro JP, Botros DG, Wirkowski E, Hanna AF. Use of dexmedetomidine for the treatment of alcohol withdrawal syndrome in critically ill patients: a retrospective case series. J Anesth 2012;26:601-605.
Objective Report on the use of DEX in patients for AWS
Study Design
Retrospective case series of a 55-adult bed ICU at a single center Institution protocol
o DEX initiated for AWS starting at 0.1 mcg/kg/hour, titrating rapidly to target HR <100 bpm, Ramsay scale of 2, with maximum dose of 1.2 mcg/kg/hour
o Adjunctive medications: Lorazepam 2 mg IV every 6 hours, haloperidol if needed for agitation, and beta-blockers (metoprolol 5 mg IV every 6 hours)
o If no response, extra dose of lorazepam followed by continuous infusion started o If above not adequate, patient intubated and DEX switched to propofol infusion
DEX and benzodiazepines were used at discretion of intensivist
Patients
Inclusion o Adult ICU patients receiving DEX in a 12-month period o Patients that received DEX for AWS diagnosed by DSM-IV
Statistics Hemodynamic parameters prior and 4 hours after DEX compared using Student’s t test
Results Baseline characteristics o 10 patients were identified (all male), mean age 53.6 years, mostly post-operative o Alcohol abuse (9 defined as heavy)and 60% were agitated within 48 hours of admission o Documented ICH in three patients; head trauma followed by seizure in 1 patient
Alcohol withdrawal treatment o DEX no loading dose; mean dose 0.63 mcg/kg/hour (range 0.2-1.2 mcg/kg/hour);
mean duration 92.7 hours (range 13-247 hours) o DEX alone (n=3); DEX plus intermittent benzodiazepine (n=7) o Antipsychotics: 70% of patients (haloperidol most common) o Beta-blockers: all patients
AWS symptoms improved in 1-2 hours o Mean duration of AWS 106.7 hours o No seizures or deaths reported
Failure of DEX to control severe agitation (n=3) o DEX discontinued, propofol in addition to lorazepam or midazolam started
No significant change in vital signs were observed 4 hours after DEX infusion started o HR decreased by 10.5%, MAP by 2.8%, RPP by 12.8% o No bradycardia requiring discontinuation of DEX
Mechanical ventilation required in 3 patients for mean of 5.3 days Average ICU LOS 9.3 days and hospital LOS 14.2 days
Authors Conclusion
DEX is effective and safe in combination with other agents to control AWS symptoms except in severe cases
Lack of early response at max doses of DEX signals failure of the drug to control AWS DEX allowed lower doses of other agents to be used Not using a bolus dose, hypotension and bradycardia avoided
Critique Retrospective study No alcohol withdrawal scale to quantify severity DEX initiation at physician discretion using hospital protocol applicable to all patients with AWS No record of benzodiazepine requirements prior and after starting Variety of patients including ICH which could have an effect on agitation and hemodynamics
DEX: dexmedetomidine; RPP: rate-pressure product=SBP X HR; ICH: intracranial hemorrhage; LOS: length of stay
B. Take home points
i. Patients had alcohol abuse history with AWS ranging in severity requiring ICU care
ii. Adjunctive dexmedetomdine ↓agitation within 1-2 hours, HR, BP, RPP
iii. May not be successful in all AWS patients especially severe
iv. HR and BP affected by combination dexmedetomidine and beta-blockers

Hernandez 13
Table 8. Rayner SG, Weinert CR, Peng H, Jepsen S, Broccard AF, Study Institution. Dexmedetomidine as adjunct treatment for severe alcohol withdrawal in the ICU. Ann Intensive Care 2012;2:12.
Objective Report use of DEX for benzodiazepine-refractory AWS
Study Design
Single-center retrospective analysis of a 23-bed mixed medical-surgical-neuroscience ICU Alcohol withdrawal protocol
o Standard physician orders (i.e. vitamin, electrolyte, and IV fluid therapy) o Nursing-administered alcohol withdrawal severity assessment protocol
10 parameters consisting of vital signs, physical and behavioral findings Ranges of total points linked to dosing ranges of IV or oral lorazepam
o Standing order for IV haloperidol 2mg per hour for severe agitation or hallucinations DEX addition was intensivist driven and with no specific protocol
Patients
Inclusion o ICU patients with ICD9-code for alcohol withdrawal during hospitalization o DEX used solely for management of alcohol withdrawal
Exclusion o Severe comorbid disease: CNS trauma, CVA, end-stage metastatic cancer, severe sepsis
Statistics Compared group means 24 hours before to means for first 24hours of DEX therapy Two-tailed t test to compare group means with p<0.05 defined as significant
Results Baseline characteristics: 20 patients (male = 19, female = 1), mean age 44.9 years Mean DEX dose 0.53 mcg/kg/hour (5 patients received load ) Mean duration of DEX therapy 49.1 hours
Table 5a. 24 hours prior compared to first 24 hours of DEX therapy
Parameter 24 hours prior First 24 hours of DEX Difference (% Decrease)
Alcohol withdrawal scoring* 9 7.1 1.9 (21.1)
Benzodiazepine dose (mg)* 52.7 20.3 32.4 (61.5)
Haloperidol dose (mg)* 12 6.4 5.6 (46.7)
HR (mmHg)* 102.8 79.3 23.4 (22.8)
SBP (mmHg)* 140.2 126.7 13.5 (9.6)
*p<0.05; reported values as means
One required intubation (excluded from analysis) 13 hours after start of DEX Mean length of ICU 98.5 hours; all survived to hospital discharge Adverse effects
o DEX discontinued in one patient due to two 9-second asystolic pauses o Non-significant increases in bradycardia and systolic hypotension
Authors Conclusion
Adjunct therapy with DEX in severe alcohol withdrawal patients led to reductions in benzodiazepine dosing, alcohol withdrawal score, and HR and BP within a few hours of DEX initiation and sustained for 24 hours
Critique Retrospective study DEX initiation at physician discretion Validity of alcohol withdrawal scoring system and lack of defining severity of score Benzodiazepine-refractory not defined as inclusion criteria Oral and IV beta-blockers administered could affect hemodynamic parameters
DEX: dexmedetomidine
C. Take home points
i. AWS ICU patients with mean lorazepam dose 52.7mg in 24hours
ii. Adjunctive dexmedetomidine ↓ severity score, haloperidol and benzodiazepine dosing
within 4 hours
iii. HR and BP affected by combination of dexmedetomidine and adjunctive beta-blockers
iv. Dexmedetomidine discontinuation required in one patient due to asystolic pauses

Hernandez 14
0%
10%
20%
30%
40%
50%
60% DEX (n=244)
Midazolam(n=122)
Summary of evidence32-38
I. Limited to case reports, case series, retrospective and prospective studies
A. Pre-and post-dexmedetomidine data
B. No studies were compared to a non-dexmedetomidine group
II. Patients studied
A. Majority non-intubated
B. AWS (severity not always quantified)
i. Severe alcohol withdrawal defined by CIWA >20
ii. AWD or DTs
iii. Benzodiazepine-refractory (lorazepam 52.7 mg/24 hours)
iv. RAW (lorazepam 4-40mg/2 hours)
III. Dexmedetomidine initiation, dosing and duration highly variable
A. Initiation varied, not defined and at physician discretion
B. Load was not common; continuous infusion ranged from 0.1-1.5mcg/kg/hour
C. Duration ranged from 15.5-206 hours
IV. Additional medications for AWS included benzodiazepines, antipyschotics, and beta-blockers
V. Efficacy and safety outcomes
A. Rapid decrease in symptoms, CIWA-Ar and RASS scores in most patients
B. No seizures reported
C. Significant reduction in benzodiazepines and haloperidol use
D. Possible avoidance of intubation and facilitation of extubation
E. Hypotension and bradycardia reported
Safety Concerns for Dexmedetomidine
I. Hemodynamic stability29,39
A. Most reported side effects: hypotension and bradycardia
i. ICU controlled trial compared to midazolam for sedation >24 hours duration
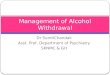
B. Tan et al.40
meta-analysis compared dexmedetomidine to other sedatives and analgesics in ICU
i. No significant difference in risk of hypotension
ii. Significant increase in risk of bradycardia requiring intervention
1. Loading dose
2. Maintenance doses >0.7mcg/kg/h
Hypotension Hypotension Intervention
Bradycardia* Bradycardia Intervention
Figure 4. Hypotension and bradycardia occurrence
*p<0.05

Hernandez 15
II. Hepatic impairment
A. 10-15% of people with alcoholism develop cirrhosis41
B. Manufacturer recommendations for hepatic impairment29
i. May be necessary to consider dose reduction
ii. Severe impairment: mean clearance value is half that observed in healthy people
C. Pharmacokinetic population study showed42
i. Correlation between high levels of AST and bilirubin and decreased clearance
ii. Changes in hepatic blood flow and cardiac output more likely to affect clearance due to
high extraction ratio of dexmedetomidine
Cost Considerations of Dexmedetomidine: Who’s picking up the tab?
I. Cost of dexmedetomidine43
A. Average wholesale price per 400mcg/100ml vial: $190.00
i. 24 hour infusion 0.2-1.2mcg/kg/hour for 70kg patient: $190.00-$957.60
B. Compared to midazolam = ~$40 per day
II. Potential cost associated with AWS and ICU admission44
A. Trauma patients with AWS compared to those without AWS
i. ICU LOS differed significantly: 7.58 days (AWS) vs 3.30 days (no AWS)
ii. Reported mean ventilator days for AWS patients was 6.79 days
B. Gold et al.23
compared intubated vs non-intubated patients with severe AWS and DTs
i. 47% required intubation after ICU admission
ii. ICU LOS: intubated patients (5.6 days) vs non-intubated patients (3.4 days)
iii. Pneumonia rates significantly differed: intubated (42%) vs non-intubated (21%)
C. ICU cost room and board only per day: $2480
D. Mechanical ventilation: initial intubation $1295, followed by $952 per day
III. No current cost comparison for dexmedetomidine for the treatment of AWS
Summary and Recommendations
I. Management in the critically ill setting A. Severe alcohol withdrawal characterized by
1
i. Profound agitation
ii. Autonomic hyperactivity
iii. Alcohol withdrawal seizures and delirium
B. Lack of validated measurement tool for ICU patients especially mechanically ventilated
i. Options studied in ICU patients CIWA-Ar, SAS, RASS
C. Benzodiazepines standard of care to prevent delirium and seizures1,16
i. RAW requires ↑ sedation and is associated with a ~40% mechanical ventilation rate23
ii. Alternative sedation options: phenobarbital, propofol, dexmedetomidine
Table 9. Pharmacologic properties of agents used for severe AWS
Medication Sedative Anxiolytic Anticonvulsant Respiratory Depression
Hemodynamic Effects
Benzodiazepine X X X X X
Propofol X X X X X
Phenobarbital X X X X X
Dexmedetomidine X X X

Hernandez 16
II. Review of dexmedetomidine for severe alcohol withdrawal
A. Clinical outcomes and efficacy
i. Limited data on clinical outcomes (i.e. mechanical ventilation, ICU length of stay)
ii. Case series comparing pre- and post-dexmedetomidine show rapid response
1. Improved CIWA-Ar score or institution derived AWS score
2. Decrease in blood pressure and heart rate
3. Reduction in benzodiazepines and haloperidol usage
iii. Proposed benefits: Avoid mechanical ventilation and facilitate extubation
B. Safety
i. No anticonvulsant properties and seizure protection not established
ii. Hypotension and bradycardia most common adverse effects
iii. Safe dosing and adverse effects in severe hepatic impairment not studied
C. Cost
i. Substantially more costly compared to alternatives
ii. Difficult to assess cost-effectiveness for this indication with no outcomes data
III. Algorithm to identify patients that may benefit with dexmedetomidine
1. Obtain baseline severity score (i.e. CIWA-Ar preferred, RASS, SAS)
2. Assess symptom control with BZD-trigger therapy RAW: Persistent symptom severity after cumulative doses
of diazepam >200mg over first 3-4 hours Persistent symptoms assessed by CIWA-Ar >20, RASS, SASS worsening, vital sign abnormalities
Continue BZD-trigger therapy Consider DEX (consider ↑BP ↑HR) or
Phenobarbital
DEX dosing guide No load. Start: 0.2mcg/kg/hour, then titrate
CIWA-Ar <10, RASS 0 to -1, SAS 3 to 4, normal vitals Max 1.2mcg/kg/hour
Monitoring Efficacy: CIWA-Ar, RASS, SAS, vitals, BZD dose
At 24 hours from DEX, if above increased = DC DEX and initiate CI BZD and/or propofol
Safety: DC DEX if HR <50bpm, SBP <90 mmHg
Intubated
Duration DEX up to 48 hours
Continue BZD therapy Consider adding
Propofol continuous infusion start 5mcg/kg/min Titrate to 50mcg/kg/min; target RASS 0 to -1, SAS 3 to 4
Monitoring: RASS, SAS, vitals TG levels @ baseline, 72 hours later
↓Rate, if SBP <90mmHg
Not going to intubate and does not meet RAW: continue BZD trigger therapy
Imminent Intubation

Hernandez 17
References
1. Sarff M, Gold JA. Alcohol withdrawal syndromes in the intensive care unit. Crit Care Med 2010;38:S494-S501.
2. Kanny D, Liu Y, Brewer RD, Garvin WS, Balluz L. Vital signs: Binge drinking prevalence, frequency, and intensity
among adults – United States, 2010. MMWR 2012;61:14–19.
3. Moss M, Burnham EL. Alcohol abuse in the critically ill patient. Lancet 2006;368:2231-2242.
4. Carlson RW, Kumar N, Wong-Mckinstry ES, et al. Alcohol withdrawal syndrome. Crit Care Clin 2012;28:549-
585.
5. Bouchery EE, Harwood HJ, Sacks JJ, Simon CJ, Brewer RD. Economic costs of excessive alcohol consumption in
the United States, 2006. Am J Prev Med 2011;41:516–524.
6. Awissi DK, Lebrun G, Fagnan M, Skrobik Y. Alcohol, nicotine, and iatrogenic withdrawals in the ICU. Crit Care
Med 2013;41:S57-S68.
7. Stehman CR, Mycyk MB. A rational approach to the treatment of alcohol withdrawal in the ED. Am J Emerg
Med 2013;31:734-742.
8. Muzyk AJ, Fowler JA, Norwood DK, Chillpko A. Role of α2-agonists in the treatment of acute alcohol
withdrawal. Ann Pharmacother 2011;45:649-657.
9. Linnoila MA, Mefford IM, Nutt D, Adinoff B. Alcohol withdrawal and noradrenergic function. Ann Intern Med
1987;107:875-889.
10. McKeon A, Frye M, Delanty N. The alcohol withdrawal syndrome. J Neurol Neurosurg Psychiatry 2008;79:854-
862.
11. Bayard M, Mcintyre J, Hill KR, Woodside J. Alcohol withdrawal syndrome. Am Fam Phyician 2004;16:1443-
1450.
12. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA, American Psychiatric
Association, 2013. Web. [access date: 1 June 2013]. dsm.psychiatryonline.org
13. Awissi DK, Lebrun G, Coursin DB, Riker RR, Skrobik Y. Alcohol withdrawal and delirium tremens in the critically
ill: a systematic review and commentary. Intensive Care Med 2013;39:16-30.
14. Sullivan JT, Sykora K, Schneiderman J, Naranjo CA, Sellers EM. Assessment of alcohol withdrawal: the revised
Clinical Institute Withdrawal Assessment for Alcohol scale (CIWA-Ar). Br J Addict 1989;84:1353-1357.
15. Kaim SC, Klett CJ, Rothfeld B. Treatment of acute alcohol withdrawal state: A comparison of four drugs. Amer J
Psychiat 1969;125:L54-60.
16. D’Onofrio G, Rathlev NK, Ulrich AS, Fish S, Freedland ES. Lorazepam for the prevention of recurrent seizures
related to alcohol. N Engl J Med 1999;340:915-919.
17. Amato L, Minozzi S, Vecchi S, Davoli M. Benzodiazepines for alcohol withdrawal. Cochrane Database Syst Rev
2010;3:CD005063.
18. Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the management of pain, agitation, and
delirium in adult patients in the intensive care unit. Crit Care Med 2013;41:263-306.
19. Daeppen JB, Gache P, Landry U, Sekera E, Schweizer V. Symptom-triggered vs fixed-schedule doses of
benzodiazepine for alcohol withdrawal. A randomized treatment trial. Arch Intern Med 2002; 162:1117-1121.
20. Spies CD, Otter HE, Huske B, et al. Alcohol withdrawal severity is decreased by symptom-orientated adjusted
bolus therapy in the ICU Intensive Care Med 2003;29:2230-2238.
21. DeCarolis D, Rice KL, Ho L, Willenbring ML, Cassaro S. Symptom-driven lorazepam protocol for treatment of
severe alcohol withdrawal delirium in the intensive care unit Pharmacotherapy. 2007;27:510-518.
22. Baumgartner GR, Rowen RC. Clonidine vs chlordiazepoxide in the management of acute alcohol withdrawal
syndrome. Arch Intern Med 1987;147:1223-1226.
23. Robinson BJ, Robinson GM, Maling TJ, Johnson RH. Is clonidine useful in the treatment of alcohol withdrawal?
Alcohol Clin Exp Res 1989;13:95-98.

Hernandez 18
24. Adinoff B. Double-blind study of alprazolam, diazepam, clonidine, and placebo in the alcohol withdrawal
syndrome: preliminary findings. Alcohol Clin Exp Res 1994;18:873-878.
25. Spies CD, Dubisz N, Neumann T, et al. Therapy of alcohol withdrawal syndrome in the intensive care unit
patients following trauma: results of a prospective randomized trial. Crit Care Med 1996;24:414-22.
26. Gold JA, Rimal B, Nolan A et al. A strategy of escalating doses of benzodiazepines and Phenobarbital
administration reduces the need for mechanical ventilation in delirium tremens. Crit Care Med 2007;35:724-
730.
27. McCowan C, Marik P. Refractory delirium tremens treated with propofol: A case series. Crit Care Med
2000;28:1781-1784.
28. Hack JB, Hoffmann RS, Nelson LS. Resistant alcohol withdrawal: does an unexpectedly large sedative
requirement identify these patients early? J Med Toxicol 2006;2:55-60.
29. Dexmedetomidine (Precedex®) Package Insert. Hospira, Inc. 2010.
30. Gertler R, Brown HC, Mitchell DH, Silvius EN. Dexmedetomidine: a novel sedative-analgesic agent. Proc (Bayl
Univ Med Cent). 2001;14:13-21.
31. MacLaren R, Krisl JC, Cochrane RE, Mueller SW. A case-based approach to the practical application of
dexmedetomidine in critically ill adults. Pharmacotherapy 2013;33:165-186.
32. Rovasalo A, Tohmo H, Aantaa R, Kettunen E, Palojoki R. Dexmedetomidine as an adjuvant in the treatment of
alcohol withdrawal delirium: a case report. Gen Hosp Psychiatry 2006; 28:362-363.
33. Darrouj J, Puri N, Prince E, Lomonaco A, Spevetz A, Gerber DR. Dexmedetomidine infusion as adjunctive
therapy to benzodiazepines for acute alcohol withdrawal. Ann Pharmacother 2008;42:1703-1705.
34. Jacob S, Karczewski, Smith H, Khan A, Nanchal R. Novel use of dexmedetomidine in 4 adults with resistant
alcohol withdrawal in the ICU. Crit Care Med 2008;36:A185.
35. Dailey RW, Leatherman JW, Sprenkle MD. Dexmedetomidine in the management of alcohol withdrawal and
alcohol withdrawal delirium. Am J Respir Crit Care Med 2011;183:A3164.
36. Tolonen J, Rossinen J, Alho H, Harjola VP. Dexmedetomidine in addition to benzodiazepine-based sedation in
patients with alcohol withdrawal delirium. Eur J Emerg Med 2012;[Epub ahead of print].
37. DeMuro JP, Botros DG, Wirkowski E, Hanna AF. Use of dexmedetomidine for the treatment of alcohol
withdrawal syndrome in critically ill patients: a retrospective case series. J Anesth 2012;26:601-605.
38. Rayner SG, Weinert CR, Peng H, Jepsen S, Broccard AF, Study Institution. Dexmedetomidine as adjunct
treatment for severe alcohol withdrawal in the ICU. Ann Intensive Care 2012;2:12.
39. Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a
randomized trial. JAMA 2009;489-499.
40. Tan JA, Ho KM. Use of dexmedetomidine as a sedative and analgesic agent in critically ill adult patients: a
meta-analysis. Intensive Care Med 2010;36:926-939.
41. Mann RE, Smart RG, Govoni R. Epidemiology of alcoholic liver disease. National Institute on Alcoholism Abuse
and Alcoholism. http://pubs.niaaa.nih.gov/publications/arh27-3/209-219.htm. Accessed 14 Sept 2013.
42. Valitalo PA, Ahtola-Satila T, Wighton A, Sarapohja T, Pohjanjousi P, Garratt C. Population pharmacokinetics of
dexmedetomidine in critically ill patients. Clin Drug Investig 2013;33:579-587.
43. Guinter JR, Kristeller JL. Prolonged infusions of dexmedetomidine in critically ill patients. Am J Health-Syst
Pharm 2010;67:1246-1253.
44. Bard MR, Goettler CE, Toschlog EA, et al. Alcohol withdrawal syndrome: turning minor injuries into a major
problem. J Trauma 2006;61:1441-46.

Hernandez 19
Appendix A. Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar) Patient____________________________________ Date___________________________Time_______
Pulse or heart rate taken for one minute_________________________Blood pressure_______________
NAUSEA AND VOMITING – Ask “Do you feel sick to your stomach? Have you vomited?” Observation. 0 No nausea and no vomiting 1 mild nausea with no vomiting 2 3 4 intermiitent nausea with dry heaves 5 6 7 constant nausea, frequent dry heaves and vomiting
TACTILE DISTURBANCES – Ask “Have you any itching, pins, and needles sensations, any burning, any numbness, or do you feel bugs crawling on your skin?” Observation. 0 none 1 very mild itching, pins and needles, burning or numbness 2 mild itching, pins and needles, burning or numbness 3 moderate itching, pins and needles, burning or numbness 4 moderately severe hallucinations 5 severe hallucinations 6 extremely severe hallucinations 7 continuous hallucinations
TREMOR – Arms extended and fingers spread apart. Observation. 0 no tremor 1 not visible, but can be felt fingertip to fingertip 2 3 4 moderate, with patient’s arm extended 5 6 7 severe, even with arms not extended
AUDITORY DISTURBANCES – Ask “Are you more aware of sounds around you? Are they harsh? Do they frighten you? Are you hearing anything that is disturbing to you? Are you hearing things you know are not there?” Observation. 0 not present 1 very mild harshness or ability to frighten 2 mild harshness or ability to frighten 3 moderate harshness or ability to frighten 4 moderately severe hallucinations 5 severe hallucinations 6 extremely severe hallucinations 7 continuous hallucinations
PAROXYSMAL SWEATS – Observation. 0 no sweat visible 1 barely perceptible sweating, palms most 2 3 4 beads of sweat obvious on forehead 5 6 7 drenching sweats
VISUAL DISTURBANCES – Ask “Does the light appear to be too bright? Is its color different? Does it hurt your eyes? Are you seeing anything that is disturbing to you? Are you seeing things you know are not there?” Observation. 0 Not present 1 very mild sensitivity 2 mild sensitivity 3 moderate sensitivity 4 moderately severe hallucinations 5 severe hallucinations 6 extremely severe hallucinations 7 continuous hallucinations
ANXIETY – Ask “Do you feel nervous?” Observation. 0 no anxiety, at ease 1 mild anxious 2 3 4 moderately anxious, or guarded, so anxiety is inferred 5 6 7 equivalent to acute panic states as seen in severe delirium or acute schizophrenic reactions
HEADACHE, FULLNESS IN HEAD – Ask “Does your head feel different? Does it feel like there is a band around your head?” do not rate for dizziness or lightheadedness. Otherwise, rate severity. 0 not present 1 very mild 2 mild 3 moderate 4 moderately severe 5 severe 6 very severe 7 extremely severe
AGITATION – Observation. 0 normal activity 1 somewhat more than normal activity 2 3 4 moderately fidgety and restless 5 6 7 paces back and forth during most of the interview, or constantly thrashes about
ORIENTATION AND CLOUDING OF SENSORIUM – Ask “What day is this? Where are you? Who am I?” 0 oriented and can do serial additions 1 cannot do serial additions or is uncertain about date 2 disoriented for date by no more than 2 calendar days 3 disoriented for date by more than 2 calendar days 4 disoriented for place/or person Patients scoring <10 do not usually need additional medication for withdrawal. TOTAL CIWA-Ar Score ___________________ Maximum possible score 67
Sullivan JT, Sykora K, Schneiderman J, Naranjo CA, Sellers EM. Assessment of alcohol withdrawal: the revised Clinical Institute Withdrawal Assessment for Alcohol scale (CIWA-Ar). Br J Addict 1989;84:1353-1357.

Hernandez 20
Richmond Agitation Sedation Scale (RASS) CAM-ICU
If RASS is > -3 proceed to CAM-ICU 1. Acute change or fluctuating course of mental status AND 2. Inattention (S A V E A H A A R T test: >2 errors) AND 3 or 4 3. Altered levels of consciousness (RAAS anything but zero CAM-ICU Poistive) 4. Disorganized thinking (I,e. Will a stone float on water? Etc.) if yes, CAM-ICU Positive http://www.mc.vanderbilt.edu/icudelirium/docs/CAM_ICU_flowsheet.pdf
Riker Sedation Agitation Scale
+4 Combative Combative, violent, immediate danger to staff
+3 Very agitated Pulls to remove tubes or catheters: aggressive
+2 Agitated Frequent non-purposeful movement, fights ventilator
+1 Restless Anxious, apprehensive, movements not aggressive
0 Alert & calm Spontaneously pays attention to caregiver
-1 Drowsy Not fully alert, but has sustained awakening to voice (eye opening & contact >10 sec)
-2 Light sedation Briefly awakens to voice (eyes open & contact <10 sec)
-3 Moderate sedation
Movement or eye opening to voice (no eye contact)
-4 Deep sedation No response to voice, but movement or eye opening (to physical stimulation)
-5 Unarousable No response to voice or physical stimulation
http://www.mc.vanderbilt.edu/icudelirium/docs/RASS.pdf
7 Dangerous agitation
Pulling ET tube, remove catheters, climbing over bedrail, striking at staff, thrashing side to side
6 Very agitated Requiring restraint and frequent verbal reminding of limits, biting ETT
5 Agitated Anxious or physically agitated, calms to verbal instruction
4 Calm & cooperative
Calm, easily arousable, follows commands
3 Sedated Difficult to arouse but awakens to verbal stimuli or gentle shaking, follows simple commands but drifts off again
2 Very sedated Aroused to physical stimuli but does not communicate or follow commands, may move spontaneously
1 Unarousable Minimal or no response to noxious stimuli, does not communicate or follow commands
http://www.mc.vanderbilt.edu/icudelirium/docs/SAS.pdf