Embed Size (px)
Citation preview
Utilizing the Utilizing the
Adult Alcohol Withdrawal Adult Alcohol Withdrawal
Syndrome Order formSyndrome Order form& &
CIWA-Ar toolCIWA-Ar tool
Prepared by Buffalo General Hospital Departments of Pharmacy and Prepared by Buffalo General Hospital Departments of Pharmacy and Clinical EducationClinical Education
April 2010
Alcohol Withdrawal Syndrome (AWS)
Definition: discontinuation or reduction of prolonged, heavy alcohol use that results in minor or major withdrawal symptoms.
Minor withdrawal symptoms include: tremor, hypertension, diaphoresis and tachycardia.
Symptoms can occur within 6-12 hours from last drink.
Serious withdrawal complications include: seizures and delirium tremens (DTs).
Symptoms can occur within 48-96 hours from last drink.
Severity of symptoms is related to amount of alcohol intake and duration of patient’s recent drinking habit.
Clinical Institute Withdrawal Assessment for Alcohol Scale, revised (CIWA-Ar)
This assessment scale: Objectively assessesObjectively assesses patients for the development of acute
alcohol withdrawal. Has well-documentedwell-documented reliability and validity. Is a 10-item scale that assesses the severity of withdrawal. Serves as a basis for prescribing medication managementbasis for prescribing medication management.
CIWA-ArThis 10-item scale can be located in 2 places:On the back of the order form (requires addition calculation)
or by using an online CIWA-Ar calculator that can be placed on a computer
desktop.
The 10 items to be assessed are:Nausea & vomiting Visual disturbancesHeadache, fullness in head AgitationParoxysmal sweats Tactile disturbancesAuditory disturbances TremorAnxiety Orientation & clouding
of sensorium
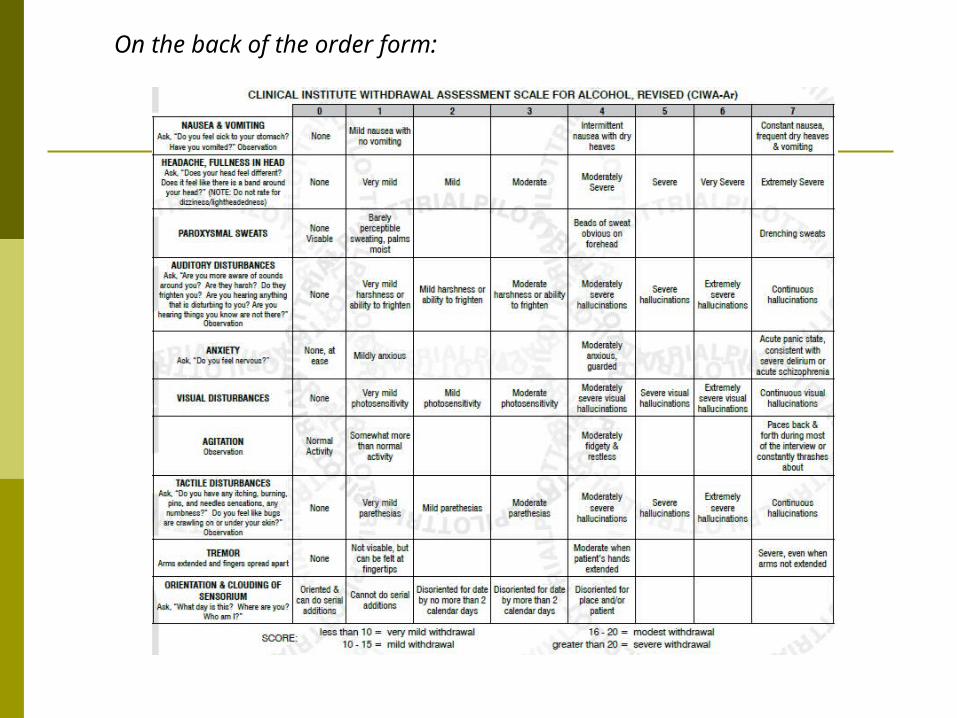
On the back of the order form:
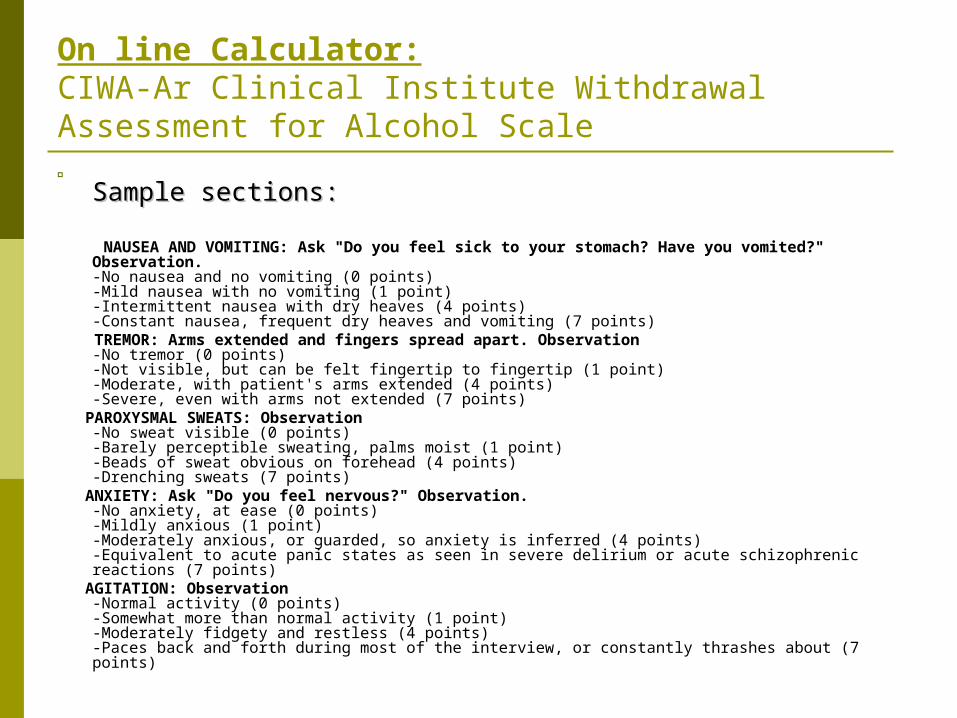
On line Calculator: CIWA-Ar Clinical Institute Withdrawal Assessment for Alcohol Scale
Sample sections: Sample sections:
NAUSEA AND VOMITING: Ask "Do you feel sick to your stomach? Have you vomited?" Observation. -No nausea and no vomiting (0 points)-Mild nausea with no vomiting (1 point)-Intermittent nausea with dry heaves (4 points)-Constant nausea, frequent dry heaves and vomiting (7 points)
TREMOR: Arms extended and fingers spread apart. Observation -No tremor (0 points)-Not visible, but can be felt fingertip to fingertip (1 point)-Moderate, with patient's arms extended (4 points)-Severe, even with arms not extended (7 points)
PAROXYSMAL SWEATS: Observation -No sweat visible (0 points)-Barely perceptible sweating, palms moist (1 point)-Beads of sweat obvious on forehead (4 points)-Drenching sweats (7 points)
ANXIETY: Ask "Do you feel nervous?" Observation. -No anxiety, at ease (0 points)-Mildly anxious (1 point)-Moderately anxious, or guarded, so anxiety is inferred (4 points)-Equivalent to acute panic states as seen in severe delirium or acute schizophrenic reactions (7 points)
AGITATION: Observation -Normal activity (0 points)-Somewhat more than normal activity (1 point)-Moderately fidgety and restless (4 points)-Paces back and forth during most of the interview, or constantly thrashes about (7 points)
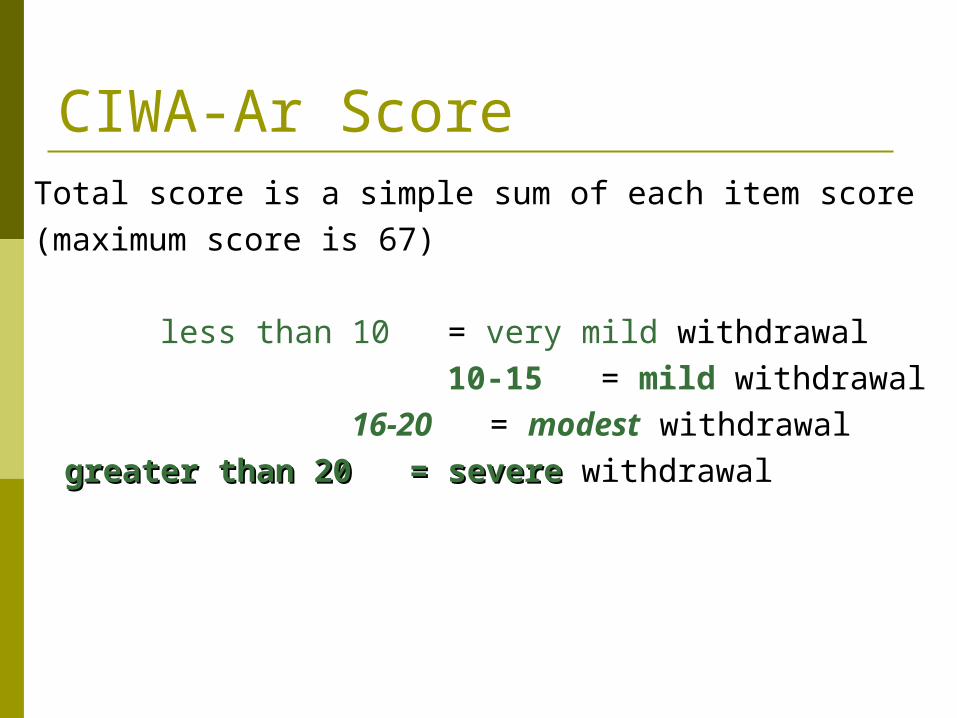
CIWA-Ar ScoreTotal score is a simple sum of each item score(maximum score is 67)
less than 10 = very mild withdrawal 10-15 = mild withdrawal
16-20 = modest withdrawal
greater than 20 = severegreater than 20 = severe withdrawal
Adult Alcohol Withdrawal Adult Alcohol Withdrawal Syndrome OrdersSyndrome Orders
A new form developed to incorporate the CIWA-Ar assessment scale as well as physician orders to manage the patient’s
alcohol withdrawal safely
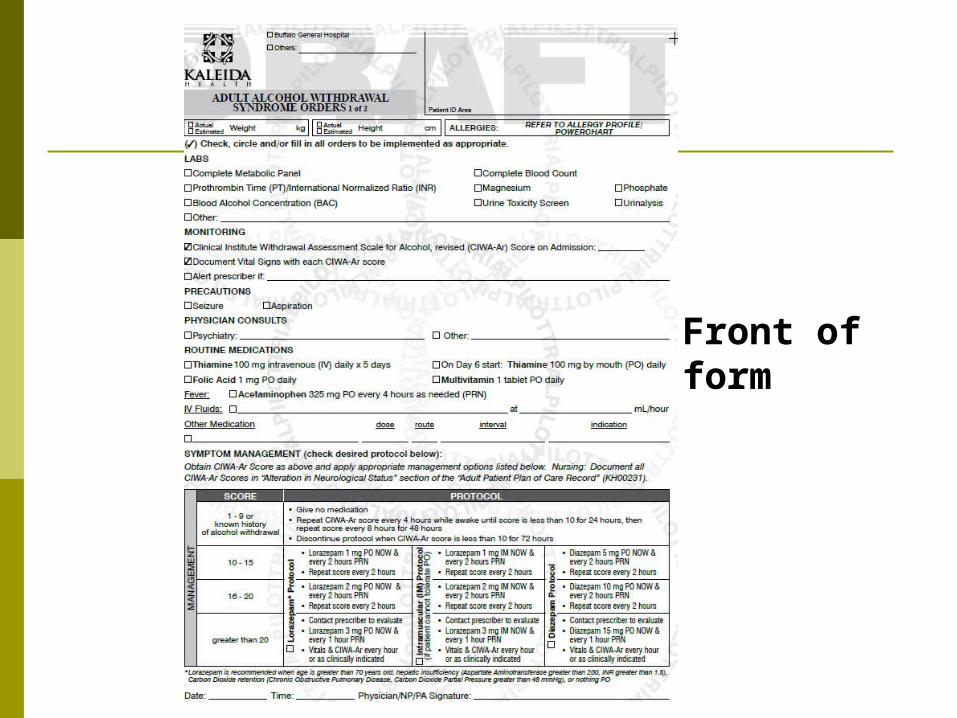
Front of form
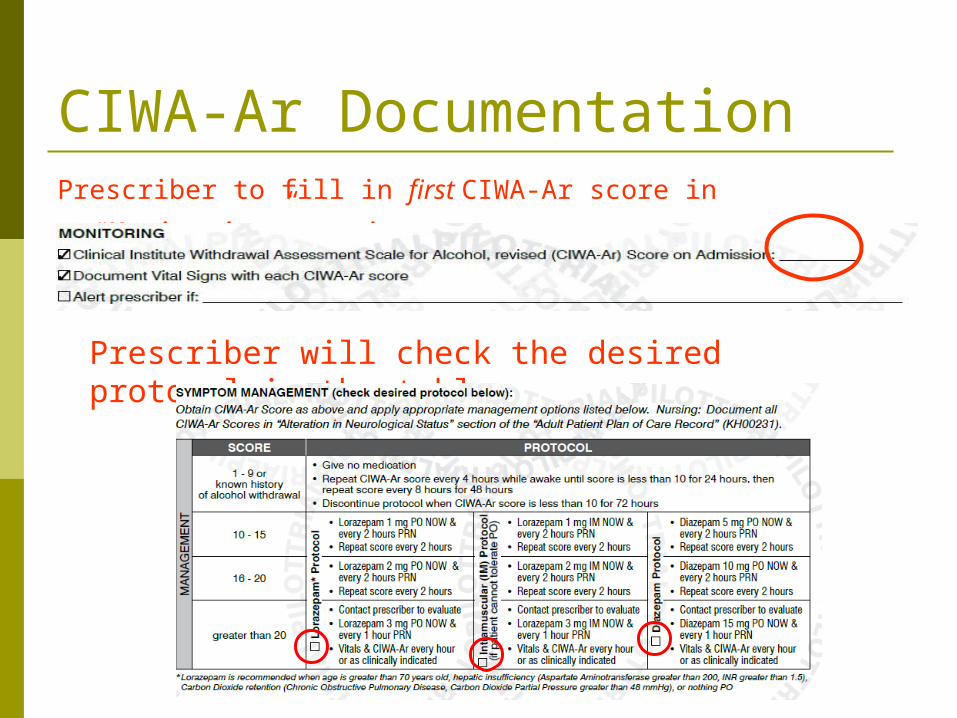
CIWA-Ar DocumentationPrescriber to fill in first CIWA-Ar score in “Monitoring” section.
Prescriber will check the desired protocol in the table.
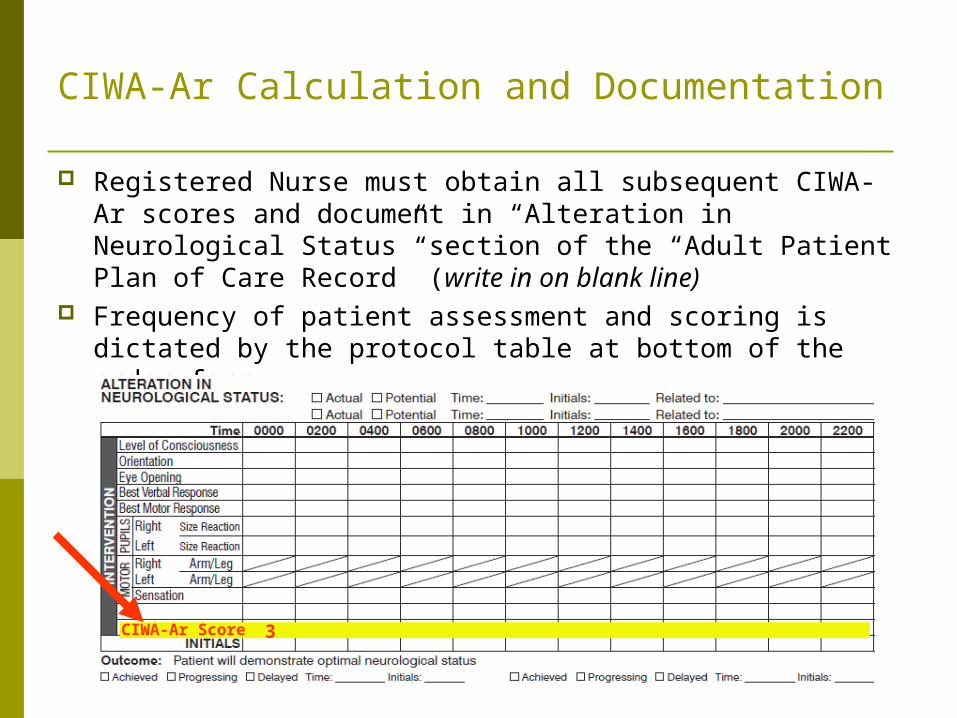
CIWA-Ar Calculation and Documentation
Registered Nurse must obtain all subsequent CIWA-Ar scores and document in “Alteration in Neurological Status” section of the “Adult Patient Plan of Care Record” (write in on blank line)
Frequency of patient assessment and scoring is dictated by the protocol table at bottom of the order form.
CIWA-Ar Score 3
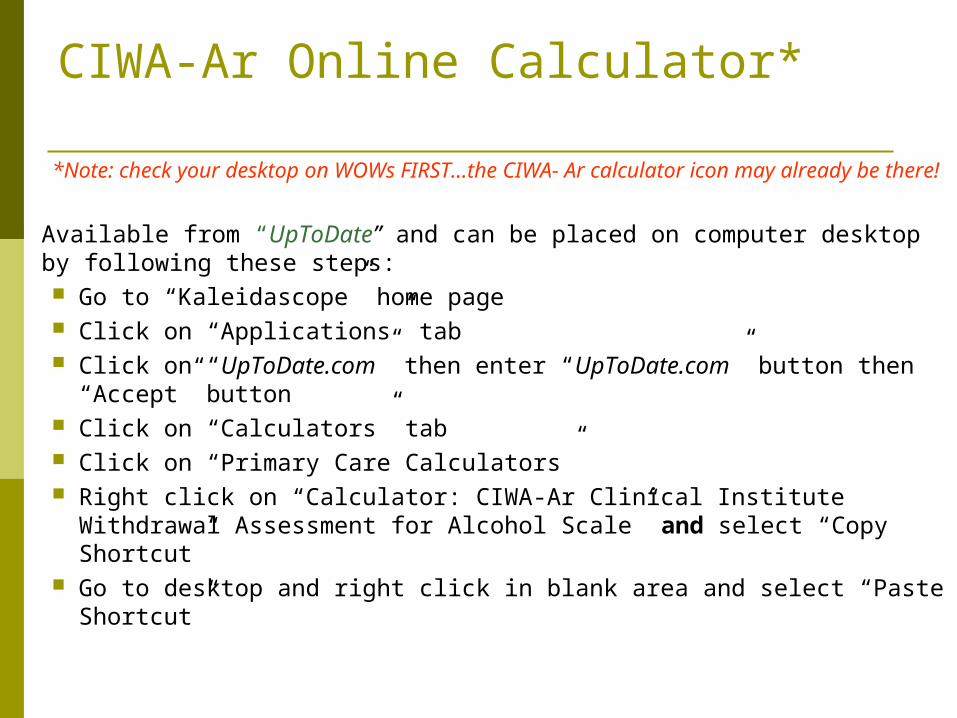
CIWA-Ar Online Calculator*
*Note: check your desktop on WOWs FIRST…the CIWA- Ar calculator icon may already be there!
Available from “UpToDate” and can be placed on computer desktop by following these steps: Go to “Kaleidascope” home page Click on “Applications” tab Click on “UpToDate.com” then enter “UpToDate.com” button
then “Accept” button Click on “Calculators” tab Click on “Primary Care Calculators” Right click on “Calculator: CIWA-Ar Clinical Institute Withdrawal
Assessment for Alcohol Scale” and select “Copy Shortcut” Go to desktop and right click in blank area and select “Paste
Shortcut”
Frequency of AssessingCIWA-Ar Score
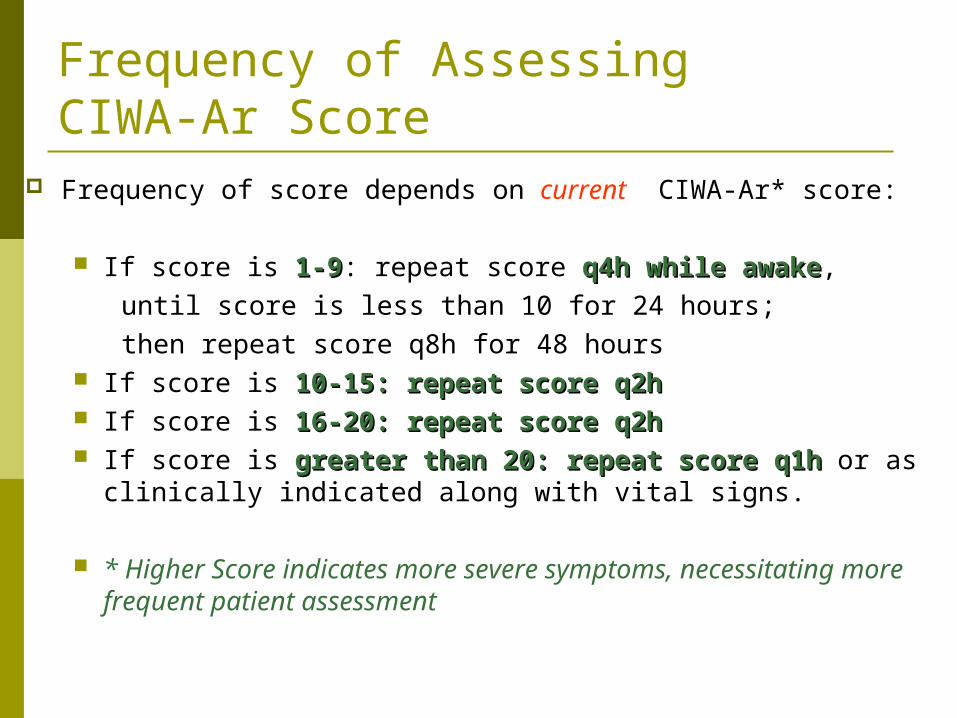
Frequency of score depends on current CIWA-Ar* score:
If score is 1-91-9: repeat score q4h while awakeq4h while awake, until score is less than 10 for 24 hours; then repeat score q8h for 48 hours If score is 10-15: repeat score q2h10-15: repeat score q2h If score is 16-20: repeat score q2h16-20: repeat score q2h If score is greater than 20: repeat score q1hgreater than 20: repeat score q1h or as
clinically indicated along with vital signs.
* Higher Score indicates more severe symptoms, necessitating more frequent patient assessment
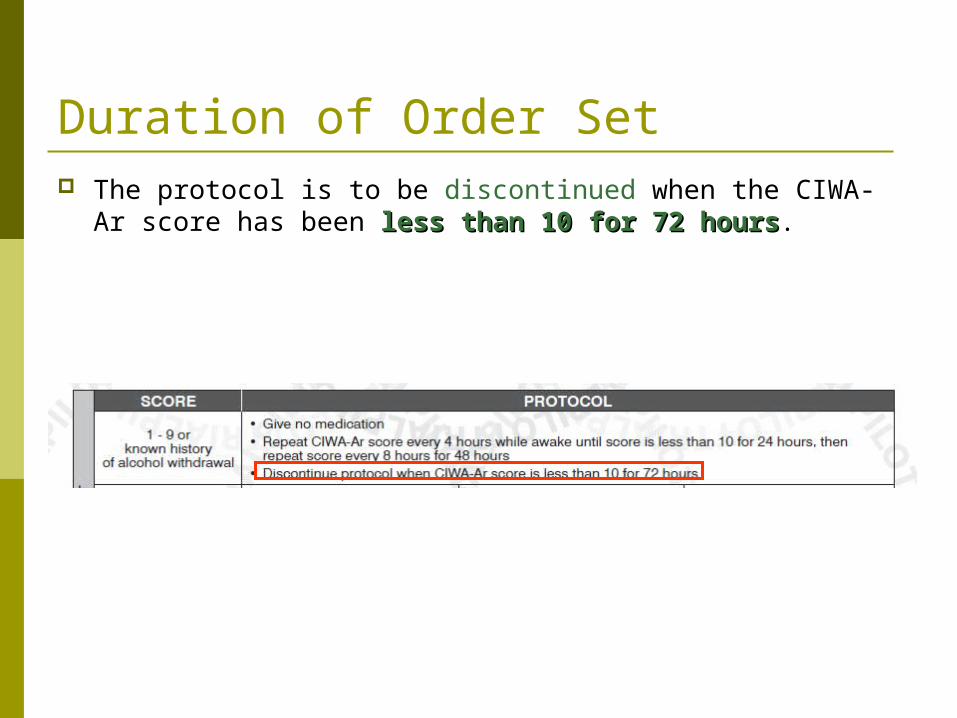
Duration of Order Set The protocol is to be discontinued when the CIWA-Ar score
has been less than 10 for 72 hoursless than 10 for 72 hours.
Scenario 1-Introduction
A 47 year old male is admitted with diagnosis of cellulitis. The Adult Alcohol Withdrawal Syndrome Orders were initiated- and the
Lorazepam protocol was selected based on his symptoms and history.
Patient Assessment:• is awake, alert & oriented X 3• complains of being a little nauseous but has not vomited• has a very mild headache• feels a little anxious
The patient does not have:• any visual, auditory or tactile disturbances; • paroxysmal sweats• agitation • or• tremors.
The patient states he drinks approximately 2-3 beers/day.
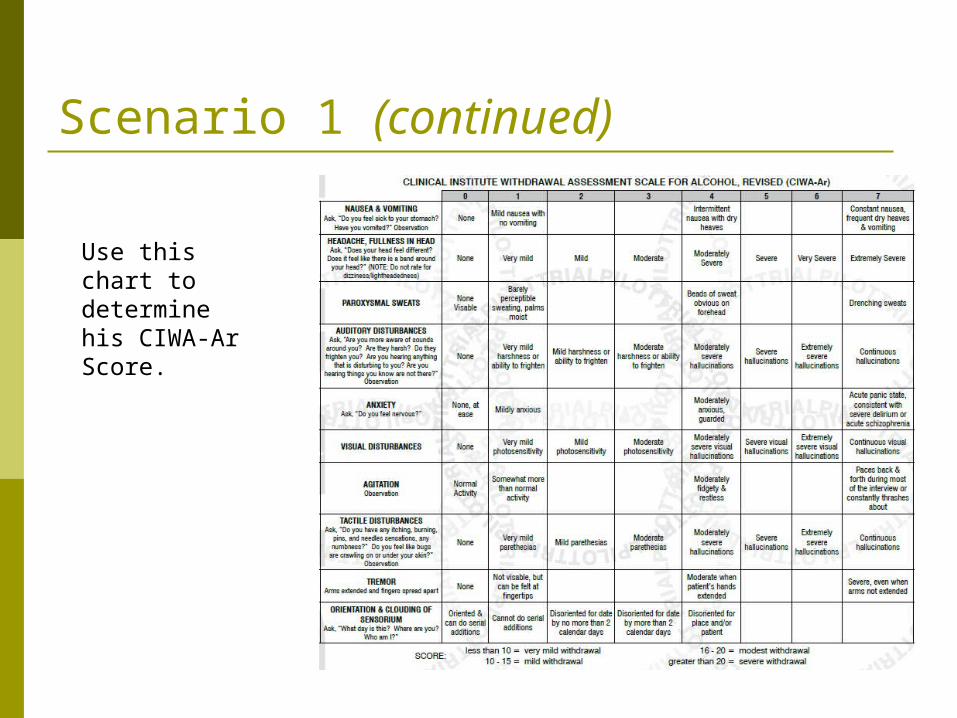
Scenario 1 (continued)
Use this chart to determine his CIWA-Ar Score.
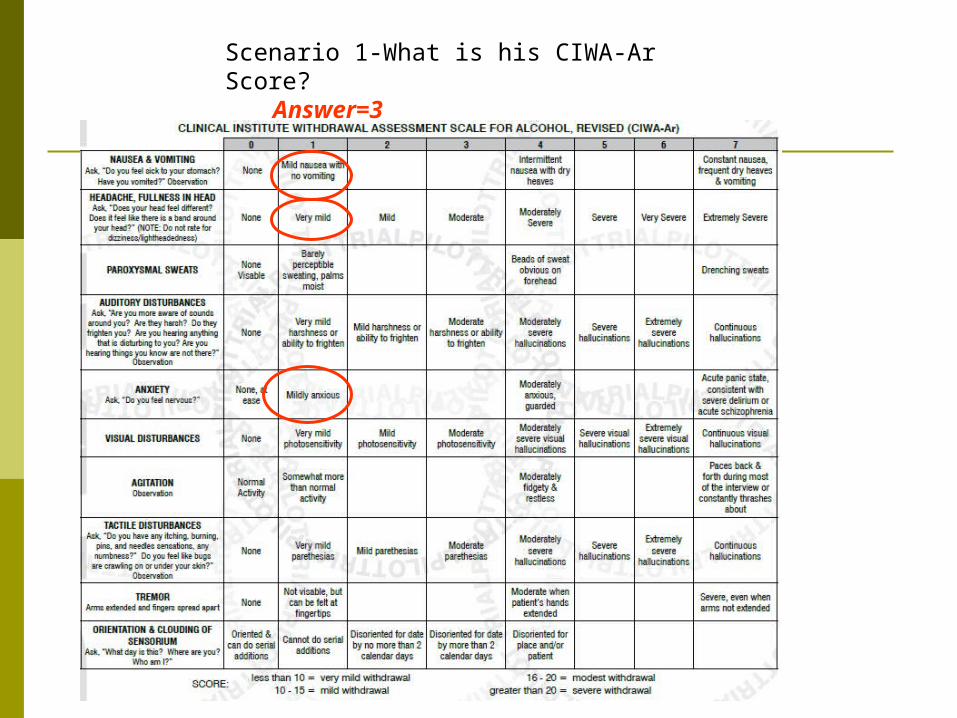
Scenario 1-What is his CIWA-Ar Score? Answer=3
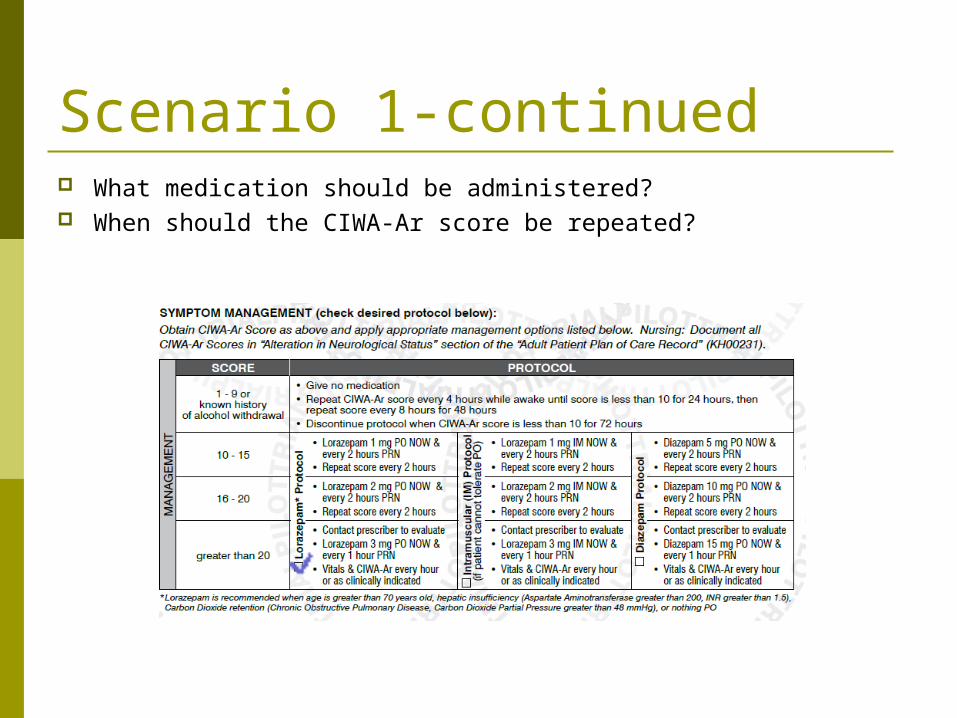
Scenario 1-continued What medication should be administered? When should the CIWA-Ar score be repeated?
Scenario 1 answers What is his CIWA-Ar Score?
3
What medication should he receive?No medication necessary
When should the CIWA-Ar Score be repeated?Every 4 hours while awake
Scenario 2
8 hours later the patient is still awake, alert & oriented x 3 and has the following: Intermittent nausea with dry heaves Moderate headache Sweat seen on forehead Moderately anxious Moderately fidgety Severe tremors even without arms being
extended
Patient does not have auditory, visual or tactile disturbances

Scenario 2-continued
What is the patient’s CIWA-Ar score now?
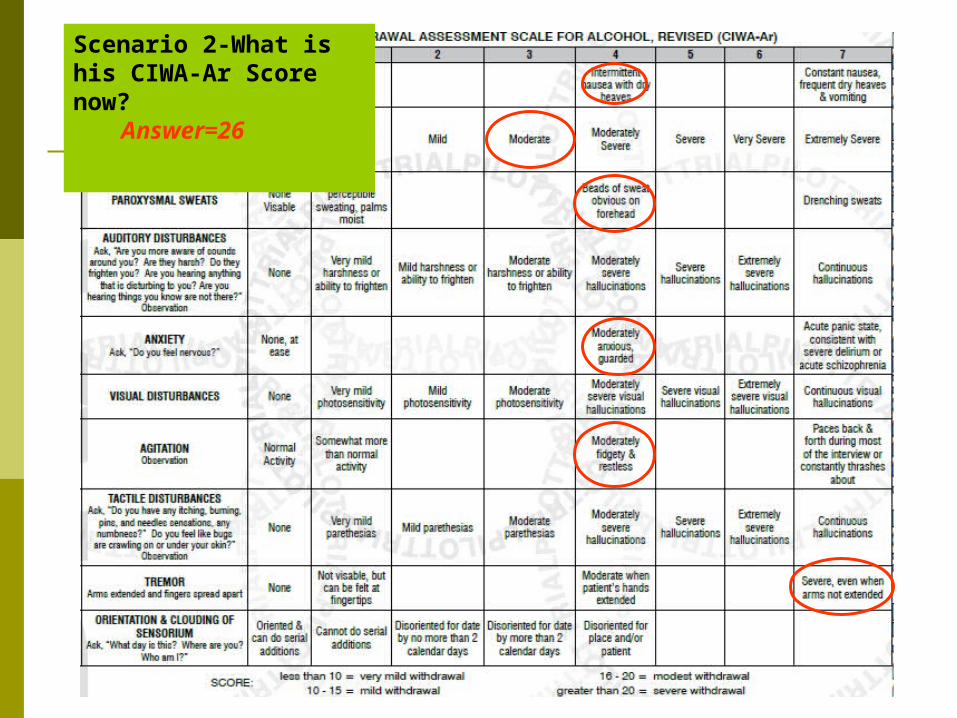
Scenario 2-What is his CIWA-Ar Score now?
Answer=26
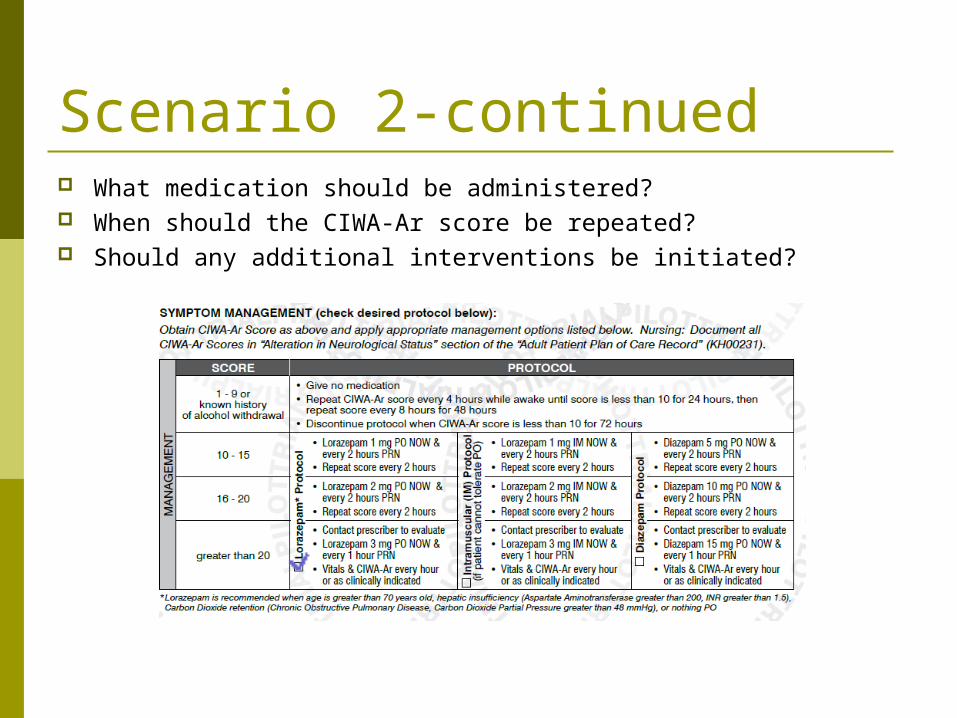
Scenario 2-continued What medication should be administered? When should the CIWA-Ar score be repeated? Should any additional interventions be initiated?
Scenario 2 (answers) What is his CIWA-Ar Score now?
26 What medication should he receive?
Lorazepam 3mg po NOW and every 1 hour as needed
When should the CIWA-Ar Score be repeated?Every hour along with vital signs
Should any additional interventions be initiated?Yes, contact prescriber to evaluate; document
assessment and interventions in patient’s chart
Conclusion The CIWA-Ar scale is a very useful tool to:
Measure severity of withdrawal symptoms Guide medication administration based on
severity of symptoms Assure patient safety during withdrawal





























