Embed Size (px)
Citation preview

1341
Vancomycin and histamine releaseSiR,—Your April 28 editorial (p 1006) suggests that Hl receptorantagonists may provide protection from the anaphylactoid orpseudoallergic type of reaction in some patients receivingvancomycin.An alternative and perhaps simpler approach where anti-gram-
positive therapy is needed would be to use the glycopeptideantibiotic teicoplanin. Teicoplanin has antibacterial activity similarto that of vancomycin and is effective in the treatment of variousgram-positive infections. Importantly the incidence of cross-
reactivity between vancomycin and teicoplanin seems low. Twelvepatients who had anaphylactoid reactions to vancomycin weresuccessfully treated with teicoplanin without evidence of cross-reactivity.1-3 McElrath et al4 recorded cross-reactivity in an opiateabuser with staphylococcal endocarditis. There has been only onereport of an anaphylactoid reaction in a patient receivingteicoplanin.5This experience suggests that teicoplanin is well tolerated in
patients with vancomycin sensitivity. It is noteworthy that
anaphylactoid reactions occur even when the chromatographicallypurified form of vancomycin is used and when the drug is given as aslow 2-h intravenous infusion, as recommended by themanufacturers. Teicoplanin may therefore provide a safealternative to vancomycin in the treatment of infection associatedwith sensitive gram-positive organisms.Magnetic Resonance Research Centreand Department of Haematology,
Liverpool University,Liverpool L69 3BX, UK STEPHEN R. SMITH
1. Smith SR, Cheesbrough JS, Makris M, Davies JM. Teicoplanin administration inpatients experiencing reactions to vancomycin. J Antimicrob Ther 1989; 23: 810-12.
2. Van Laethem Y, Goossens H, Cran S, Butzler JP, Clumesk N. Teichomycin in severemethicillin resistant gram positive septicaemia. (Twenty-fourth InterscienceConference on Antimicrobial Agents and Chemotherapy, Washington DC, 8-10October.) Washington, DC: American Society for Microbiology, 1984, abstract1219: 306.
3. Schlemmer B, Falkman H, Boudjada A, Jacob L, LeGall JR. Teicoplanin for patientsallergic to vancomycin. N Engl J Med 1988; 318: 1127-28.
4. McElrath MJ, Goldberg D, Neu HC. Allergic cross-reactivity of teicoplanin andvancomycin. Lancet 1986; i: 47.
5. Lewis P, Garaud J, Parenti F. A multicentre open clinical trial of infections caused bygram-positive bacteria. J Antimicrob Ther 1988; 21 (suppl A): 61-67.
Diabetes mortality in a tertiary referralhospital in India
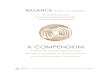
SIR,-A cross-sectional analysis of hospital records of the All IndiaInstitute of Medical Sciences (AIIMS) from 1977 to 19871 led tothe identification of 580 "diabetic deaths" (all ages). 11 patients hadchildhood onset (under 20 years of age) and 20 had onset of diabetesat age 21-30. Ketoacidosis accounted for 91 % and 25% of diabetesdeaths, respectively; most deaths were at or soon after the diagnosisof diabetes (table).
In a cohort of patients with childhood onset diabetes beingfollowed up at the AIIMS diabetic clinic diabetes duration was 1-3months in 26%,4-12 months in 24%, 1-5 years in 27%, 6-10 yearsin 13%, and greater than 10 years in only 9%.To the best of our knowledge this is the first report of childhood
diabetes mortality data from India: the prognosis remains
alarmingly dismal. Ketoacidosis, a preventable and treatable
condition, accounted for 91 % of deaths, usually at the time of orwithin a few months of the diabetes being diagnosed.
PROFILE OF DIABETES DEATHS
Figures m Italic type show diabetes duration in years at time of death. Frequency ofhypertension 0% and 40% in the childhood and youth onset group, respectively.CAD=coronary artery disease; CRF = chronic renal disease; other includes chronicvascular disease and infection.
Possibly, in the Indian health scene, only a very few children withdiabetes survive long enough for the chronic complications todevelop. In the United States deaths in childhood onset diabetes areusually caused by coronary heart disease (48%) or renal failure(31%), and 90% of children surviving 20 years of diabetes, 77% 30years, and 46% 40 years.2
Departments of Paediatricsand Endocrinology, Metabolism, and Diabetes,
All India Institute of Medical Sciences,Diabetes Foundation (India),New Delhi 110029, India
ANJU VIRMANIP. USHABALAP. V. RAO
1. Virmani A, Ushabala P, Rao PV. Mortality in IDDM observed in a tertiary referralhospital in India. Diabetes Bull 1989; 9 (suppl 1): 18-19.
2. Christlieb AR, Warram JH, Krolewski AS, et al. Hypertension: the major risk factor injuvenile-onset insulin-dependent diabetes. Diabetes 1981; 30 (suppl 2): 90.
Diabetes in Asian children
SiR,—Two medicolegal reports on death due to undiagnoseddiabetes in children (March 10, p 595; March 17, p 652) call to mindtwo fatalities in children whose referral to hospital was delayedbecause diabetes had not been recognised as the cause for theirsymptoms. Both came from Asian families. On contacting thegeneral practitioners concerned we found a widely held belief thattrue insulin-dependent diabetes is rare in Asians.’We have studied in detail the prevalence of insulin-dependent
diabetes in 20 267 Asian and 44 268 white children below the age of15 in Leicestershire. The prevalence (per 1000) for Asians is 0-54and for whites 0-99 (relative risk 055, 95% confidence interval0-3-11). This rate for Asians is higher than that recorded in otherFar and Middle Eastern populations in which methodologicallystringent prevalence studies have been done. In Japan and Israel theprevalence rates of insulin-dependent diabetes in children are 0-06and 0 16, respectively.2 Insulin-treated diabetes was rare in theyoung adult Asian indirectly suggesting an increased prevalence ofinsulin-dependent diabetes in Asian children after migration to theUK.4
Diabetes Research,Leicester General Hospital,Leicester LE5 4PW, UK
A. SAMANTAA. C. BURDEN
J. R. HEARNSHAWP. G. F. SWIFT
1. Samanta A, Burden AC, Jones GR, et al. Prevalence of insulin-dependent diabetes inAsian children. Diabetic Med 1987; 4: 65-67.
2. Knowleski AS, Warram JH. Epidemiology of diabetes mellitus. In: Marble A, KrallLP, Bradley RF, Christlieb AR, Soeldner JS, eds. Joslin’s diabetes mellitus.Philadelphia: Lea & Febiger, 1985.
3. Chaudhuri KR, Samanta A, Burden AC. Prevalence of insulin-treated diabetesmellitus: differences between whites and (Indian) Asians in the UK. Diabetic Med1989; 6 (suppl 2): 21A.
4. Burden AC, Hearnshaw JR, Swift PGF. Childhood diabetes: an increasing incidence.Diabetic Med 1989; 6: 334-36.
Nutrition and hip fractureSIR,-Dr Delmi and colleagues (April 28, p 1013) suggest thatmalnutrition may be an important determinant of the incidence ofand complications from hip fractures in the elderly, and theyprovide evidence for a more favourable clinical outcome in patientsgiven nutritional supplements. However, the only evidence for animprovement in nutritional status is an increase in serum albumin,but this responded in the normal manner of a negative acute-phaseprotein and I question the evidence for malnutrition in thesepatients.The biochemical evidence given for malnutrition is based on
serum concentrations of retinol binding protein (RBP), vitamin A,carotene, and 25-hydroxycholecalciferol (250HD) for which themeans were reported to be below normal. Many 250HD valueswere indeed low but this probably reflects the lifestyle of thesepatients before their injury since most vitamin D is obtained fromendogenous synthesis in response to sunlight. For the other indicesthe means were not below normal. The normal range for RBP is20-2-5 pmol/1 (40-50 mg/1) and for retinol it is above 0-7 umol/1