Embed Size (px)
Citation preview
1 | P a g e
DIABETES INTEGRATED CARE PATHWAYS
Preliminary Review of Best Practices
Selection of successful good practices of integrated care pathways (‘ICP’)
The list of good practices of integrated care pathways were selected from sources that are available
in the public domain. The main source used was the publication of the European Innovation
Partnership on Active and Health Ageing: A Compilation of Good Practices (Nov 2013) (‘EIP’). Aside
from demonstrating improvement of health outcomes, best practices were evaluated in relation to
the following process and outcomes indicators as listed below:
Process indicators:
Involvement of public authorities
Involvement of other stakeholders
Multidisciplinary teams
Patient stratification
Patient involvement
M-health tools
E-health tools
Outcome indicators:
Hospitalization
Cost saving
Satisfaction of patients
Satisfaction of HCP
Process indicators
Involvement of public authorities
To evaluate involvement of public authorities, we checked 1) whether a local authority was involved
in the coordination and/or organization of the integrated care pathway (‘pathway) and 2) whether
the implementation of care pathways was financially supported by a public authority.
Involvement of private stakeholders
To evaluate involvement of private stakeholders we checked whether other non-state organizations
were involved in the implementation or evaluation of the pathways.
Multidisciplinary teams
To evaluate the involvement of multidisciplinary teams in the implementation of care pathways, we
assessed whether health care professionals (‘HCPs’) from both primary and secondary care from
different fields were actively and systematically engaged in the pathway.
Patient stratification
To evaluate whether ICPs were based on risk stratification, we checked whether risk groups were
identified and reached out to for preventative reasons.
2 | P a g e
Patient involvement
To evaluate whether patients were involved in the design and implementation of the ICPs, we
checked whether patient representatives were involved in an advisory capacity at any stage of the
process (design, implementation, evaluation).
M-health tool
To evaluate whether the care pathway was supported by m-health solutions, we checked whether
there were any m-health tools used within the delivery of health care allowing the transmission of
health data from patients to healthcare professionals by use of mobile devices.
E-health tools
To evaluate whether other ICT solutions were used within the pathway, we checked whether other
eHealth tools were used, including tele monitoring tools and other electronic information tools such
as electronic prescriptions and electronic health records.
Outcome indicators
To evaluate the cost-effectiveness of the ICPs, we have also set outcome indicators to evaluate the
results achieved through the provision of goods and services. These were quantified according to:
Decrease of hospitalization
Cost savings related to treatment of acute episodes, use of healthcare facilities, sick leave
and absenteeism
Satisfaction of patients captured in evaluation forms
Satisfaction of HCPs captured in evaluation forms
Based on the abovementioned methodology, ten case studies were benchmarked (table 1) and
analyzed (case study profiles). The case study section also includes remarks on key take-aways
contributing to the success of each best practice.
3 | P a g e
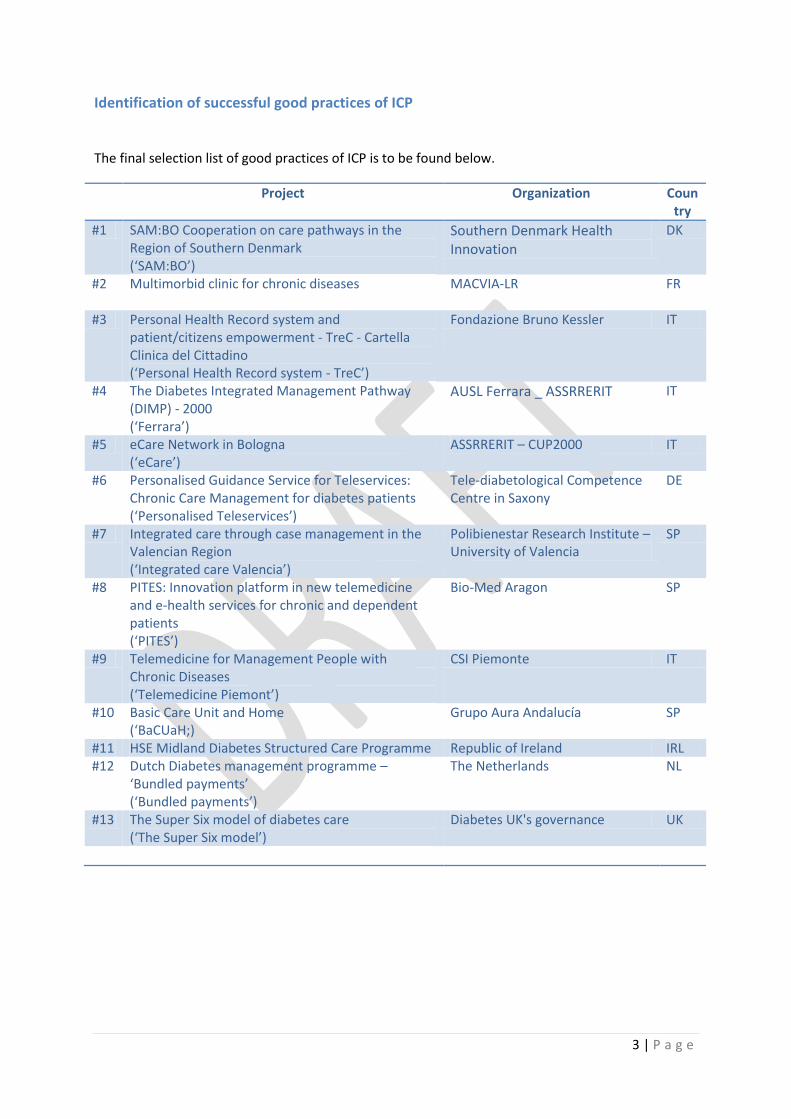
Identification of successful good practices of ICP
The final selection list of good practices of ICP is to be found below.
Project Organization Country
#1 SAM:BO Cooperation on care pathways in the Region of Southern Denmark (‘SAM:BO’)
Southern Denmark Health Innovation
DK
#2 Multimorbid clinic for chronic diseases
MACVIA-LR FR
#3 Personal Health Record system and patient/citizens empowerment - TreC - Cartella Clinica del Cittadino (‘Personal Health Record system - TreC’)
Fondazione Bruno Kessler IT
#4 The Diabetes Integrated Management Pathway (DIMP) - 2000 (‘Ferrara’)
AUSL Ferrara _ ASSRRERIT IT
#5 eCare Network in Bologna (‘eCare’)
ASSRRERIT – CUP2000 IT
#6 Personalised Guidance Service for Teleservices: Chronic Care Management for diabetes patients (‘Personalised Teleservices’)
Tele-diabetological Competence Centre in Saxony
DE
#7 Integrated care through case management in the Valencian Region (‘Integrated care Valencia’)
Polibienestar Research Institute – University of Valencia
SP
#8 PITES: Innovation platform in new telemedicine and e-health services for chronic and dependent patients (‘PITES’)
Bio-Med Aragon SP
#9 Telemedicine for Management People with Chronic Diseases (‘Telemedicine Piemont’)
CSI Piemonte IT
#10 Basic Care Unit and Home (‘BaCUaH;)
Grupo Aura Andalucía SP
#11 HSE Midland Diabetes Structured Care Programme Republic of Ireland IRL #12 Dutch Diabetes management programme –
‘Bundled payments’ (‘Bundled payments’)
The Netherlands NL
#13 The Super Six model of diabetes care (‘The Super Six model’)
Diabetes UK's governance UK
4 | P a g e
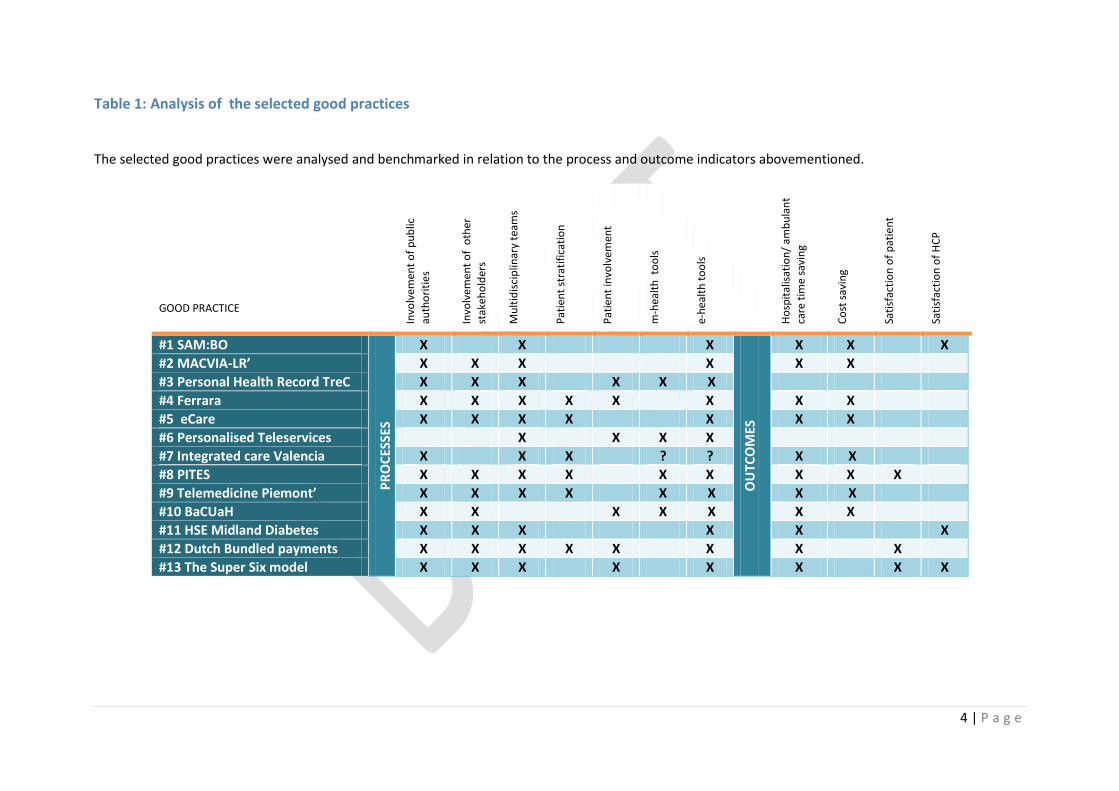
Table 1: Analysis of the selected good practices
The selected good practices were analysed and benchmarked in relation to the process and outcome indicators abovementioned.
GOOD PRACTICE
Invo
lvem
ent
of
pu
blic
auth
ori
tie
s
Invo
lvem
ent
of
oth
er
stak
eho
lder
s
Mu
ltid
isci
plin
ary
team
s
Pat
ien
t st
rati
fica
tio
n
Pat
ien
t in
volv
emen
t
m-h
ealt
h t
oo
ls
e-h
ealt
h t
oo
ls
Ho
spit
alis
atio
n/
amb
ula
nt
care
tim
e sa
vin
g
Co
st s
avin
g
Sati
sfac
tio
n o
f p
atie
nt
Sati
sfac
tio
n o
f H
CP
#1 SAM:BO
PR
OC
ESSE
S
X X X
OU
TCO
MES
X X X
#2 MACVIA-LR’ X X X X X X
#3 Personal Health Record TreC X X X X X X
#4 Ferrara X X X X X X X X
#5 eCare X X X X X X X
#6 Personalised Teleservices X X X X
#7 Integrated care Valencia X X X ? ? X X
#8 PITES X X X X X X X X X
#9 Telemedicine Piemont’ X X X X X X X X
#10 BaCUaH X X X X X X X
#11 HSE Midland Diabetes X X X X X X
#12 Dutch Bundled payments X X X X X X X X
#13 The Super Six model X X X X X X X X
5 | P a g e
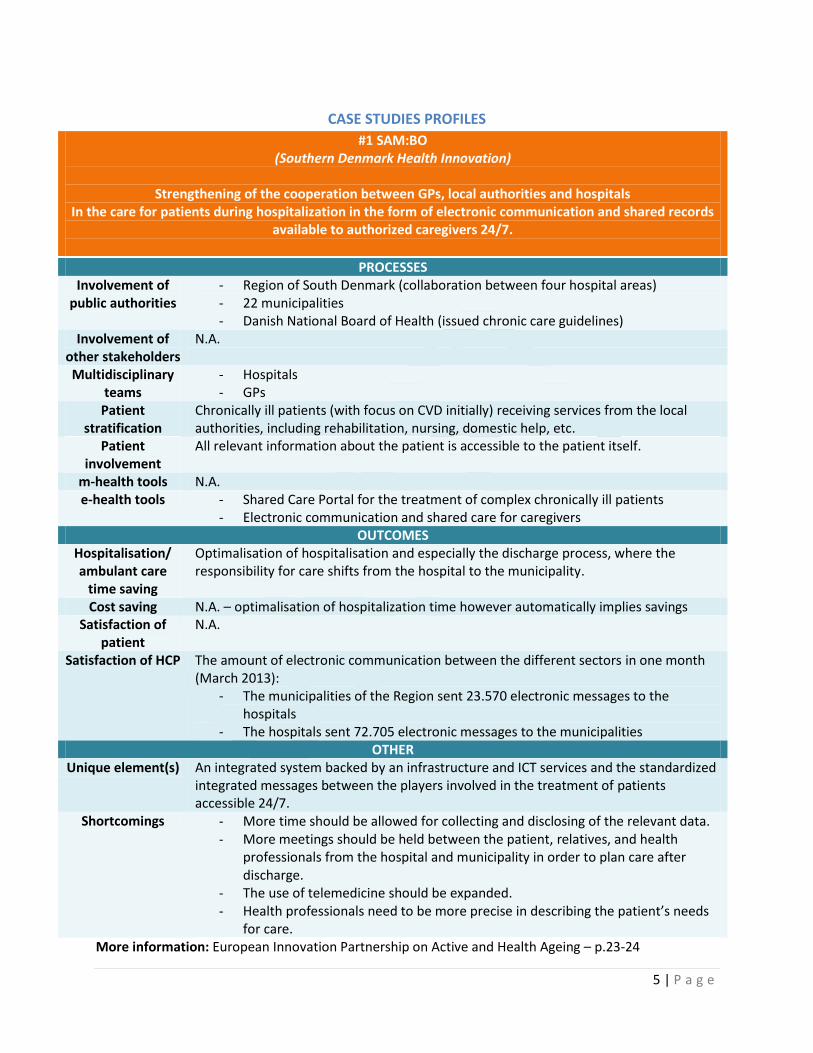
CASE STUDIES PROFILES
#1 SAM:BO (Southern Denmark Health Innovation)
Strengthening of the cooperation between GPs, local authorities and hospitals
In the care for patients during hospitalization in the form of electronic communication and shared records available to authorized caregivers 24/7.
PROCESSES Involvement of
public authorities - Region of South Denmark (collaboration between four hospital areas) - 22 municipalities - Danish National Board of Health (issued chronic care guidelines)
Involvement of other stakeholders
N.A.
Multidisciplinary teams
- Hospitals - GPs
Patient stratification
Chronically ill patients (with focus on CVD initially) receiving services from the local authorities, including rehabilitation, nursing, domestic help, etc.
Patient involvement
All relevant information about the patient is accessible to the patient itself.
m-health tools N.A. e-health tools - Shared Care Portal for the treatment of complex chronically ill patients
- Electronic communication and shared care for caregivers OUTCOMES
Hospitalisation/ ambulant care
time saving
Optimalisation of hospitalisation and especially the discharge process, where the responsibility for care shifts from the hospital to the municipality.
Cost saving N.A. – optimalisation of hospitalization time however automatically implies savings Satisfaction of
patient N.A.
Satisfaction of HCP The amount of electronic communication between the different sectors in one month (March 2013):
- The municipalities of the Region sent 23.570 electronic messages to the hospitals
- The hospitals sent 72.705 electronic messages to the municipalities OTHER
Unique element(s) An integrated system backed by an infrastructure and ICT services and the standardized integrated messages between the players involved in the treatment of patients accessible 24/7.
Shortcomings - More time should be allowed for collecting and disclosing of the relevant data. - More meetings should be held between the patient, relatives, and health
professionals from the hospital and municipality in order to plan care after discharge.
- The use of telemedicine should be expanded. - Health professionals need to be more precise in describing the patient’s needs
for care. More information: European Innovation Partnership on Active and Health Ageing – p.23-24
6 | P a g e
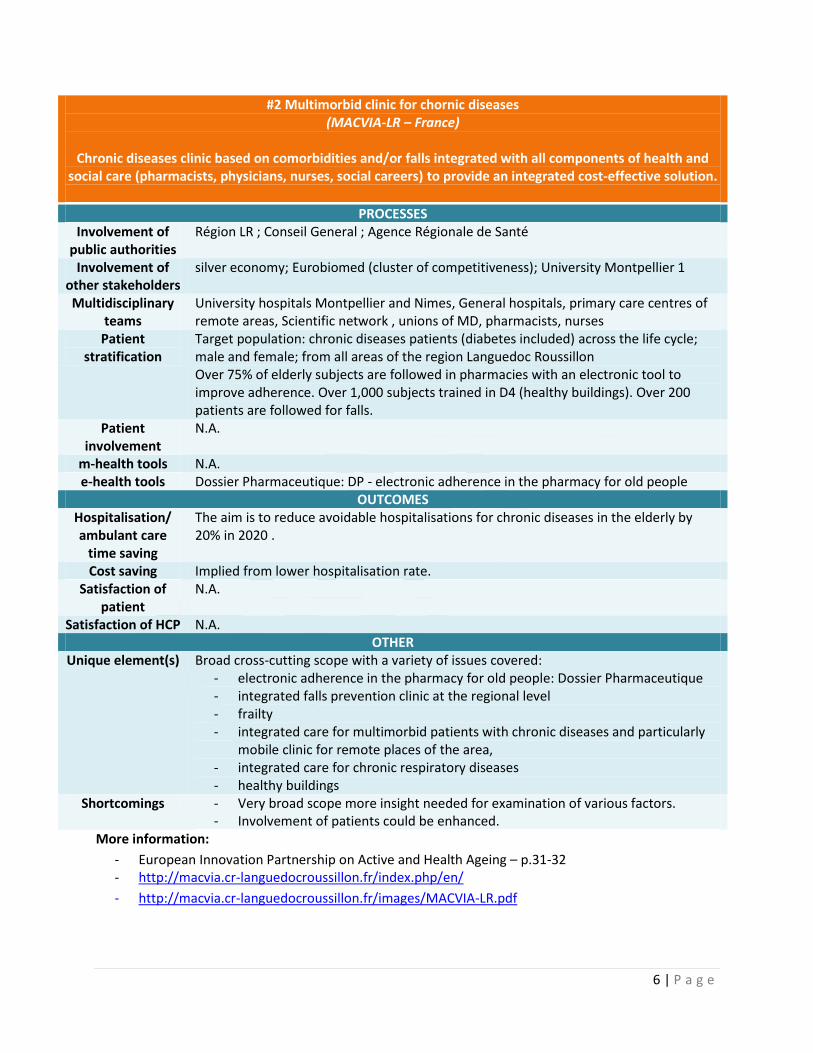
#2 Multimorbid clinic for chornic diseases (MACVIA-LR – France)
Chronic diseases clinic based on comorbidities and/or falls integrated with all components of health and
social care (pharmacists, physicians, nurses, social careers) to provide an integrated cost-effective solution.
PROCESSES Involvement of
public authorities Région LR ; Conseil General ; Agence Régionale de Santé
Involvement of other stakeholders
silver economy; Eurobiomed (cluster of competitiveness); University Montpellier 1
Multidisciplinary teams
University hospitals Montpellier and Nimes, General hospitals, primary care centres of remote areas, Scientific network , unions of MD, pharmacists, nurses
Patient stratification
Target population: chronic diseases patients (diabetes included) across the life cycle; male and female; from all areas of the region Languedoc Roussillon Over 75% of elderly subjects are followed in pharmacies with an electronic tool to improve adherence. Over 1,000 subjects trained in D4 (healthy buildings). Over 200 patients are followed for falls.
Patient involvement
N.A.
m-health tools N.A. e-health tools Dossier Pharmaceutique: DP - electronic adherence in the pharmacy for old people
OUTCOMES Hospitalisation/ ambulant care
time saving
The aim is to reduce avoidable hospitalisations for chronic diseases in the elderly by 20% in 2020 .
Cost saving Implied from lower hospitalisation rate. Satisfaction of
patient N.A.
Satisfaction of HCP N.A. OTHER
Unique element(s) Broad cross-cutting scope with a variety of issues covered: - electronic adherence in the pharmacy for old people: Dossier Pharmaceutique - integrated falls prevention clinic at the regional level - frailty - integrated care for multimorbid patients with chronic diseases and particularly
mobile clinic for remote places of the area, - integrated care for chronic respiratory diseases - healthy buildings
Shortcomings - Very broad scope more insight needed for examination of various factors. - Involvement of patients could be enhanced.
More information:
- European Innovation Partnership on Active and Health Ageing – p.31-32 - http://macvia.cr-languedocroussillon.fr/index.php/en/
- http://macvia.cr-languedocroussillon.fr/images/MACVIA-LR.pdf
7 | P a g e
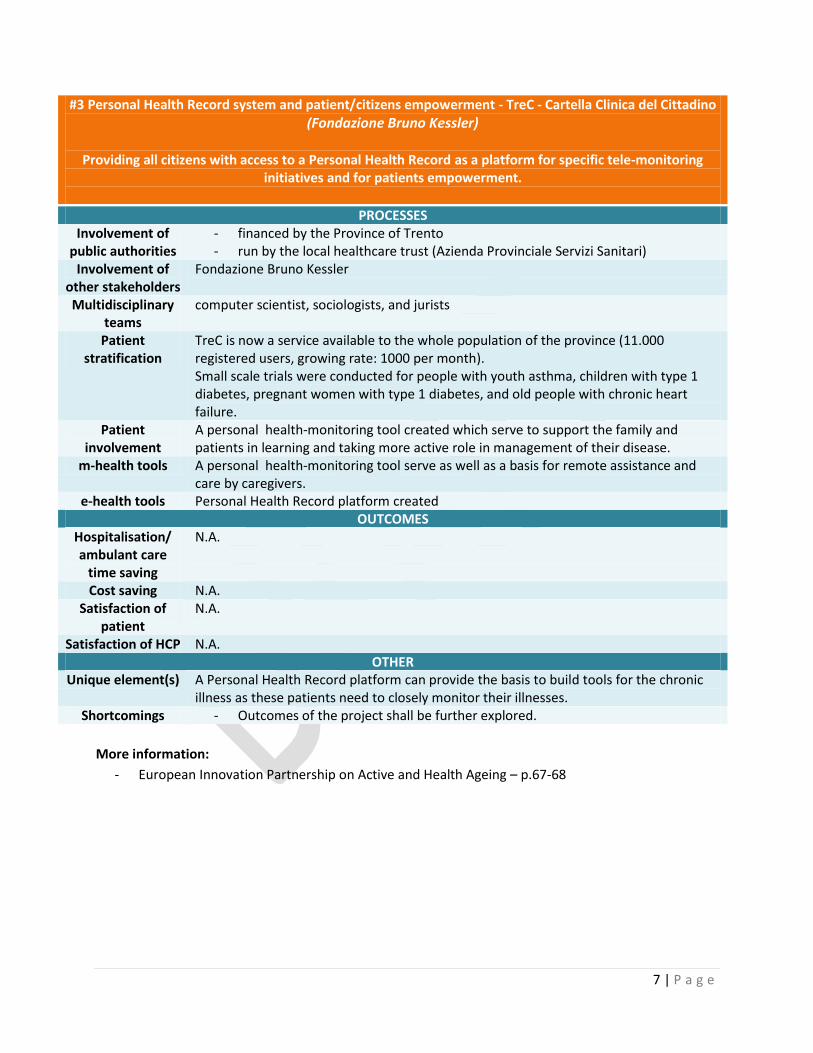
#3 Personal Health Record system and patient/citizens empowerment - TreC - Cartella Clinica del Cittadino
(Fondazione Bruno Kessler)
Providing all citizens with access to a Personal Health Record as a platform for specific tele-monitoring initiatives and for patients empowerment.
PROCESSES Involvement of
public authorities - financed by the Province of Trento - run by the local healthcare trust (Azienda Provinciale Servizi Sanitari)
Involvement of other stakeholders
Fondazione Bruno Kessler
Multidisciplinary teams
computer scientist, sociologists, and jurists
Patient stratification
TreC is now a service available to the whole population of the province (11.000 registered users, growing rate: 1000 per month). Small scale trials were conducted for people with youth asthma, children with type 1 diabetes, pregnant women with type 1 diabetes, and old people with chronic heart failure.
Patient involvement
A personal health-monitoring tool created which serve to support the family and patients in learning and taking more active role in management of their disease.
m-health tools A personal health-monitoring tool serve as well as a basis for remote assistance and care by caregivers.
e-health tools Personal Health Record platform created OUTCOMES
Hospitalisation/ ambulant care
time saving
N.A.
Cost saving N.A. Satisfaction of
patient N.A.
Satisfaction of HCP N.A. OTHER
Unique element(s) A Personal Health Record platform can provide the basis to build tools for the chronic illness as these patients need to closely monitor their illnesses.
Shortcomings - Outcomes of the project shall be further explored.
More information:
- European Innovation Partnership on Active and Health Ageing – p.67-68
8 | P a g e
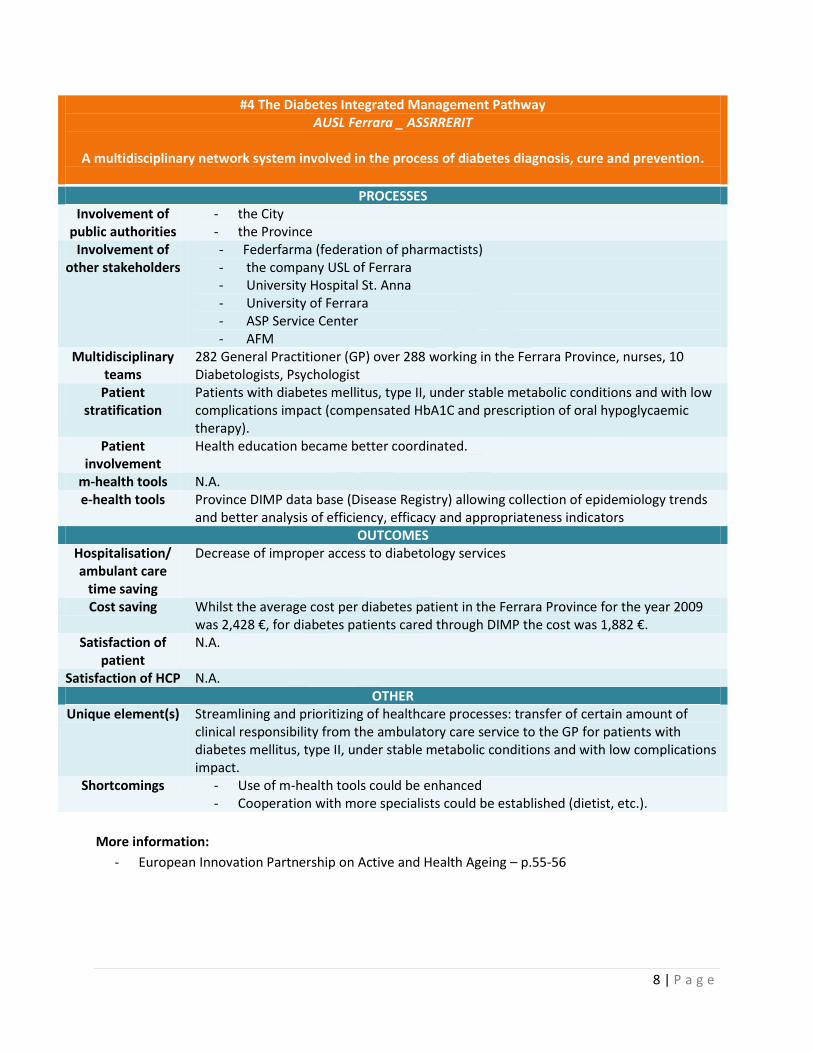
#4 The Diabetes Integrated Management Pathway AUSL Ferrara _ ASSRRERIT
A multidisciplinary network system involved in the process of diabetes diagnosis, cure and prevention.
PROCESSES Involvement of
public authorities - the City - the Province
Involvement of other stakeholders
- Federfarma (federation of pharmactists) - the company USL of Ferrara - University Hospital St. Anna - University of Ferrara - ASP Service Center - AFM
Multidisciplinary teams
282 General Practitioner (GP) over 288 working in the Ferrara Province, nurses, 10 Diabetologists, Psychologist
Patient stratification
Patients with diabetes mellitus, type II, under stable metabolic conditions and with low complications impact (compensated HbA1C and prescription of oral hypoglycaemic therapy).
Patient involvement
Health education became better coordinated.
m-health tools N.A. e-health tools Province DIMP data base (Disease Registry) allowing collection of epidemiology trends
and better analysis of efficiency, efficacy and appropriateness indicators OUTCOMES
Hospitalisation/ ambulant care
time saving
Decrease of improper access to diabetology services
Cost saving Whilst the average cost per diabetes patient in the Ferrara Province for the year 2009 was 2,428 €, for diabetes patients cared through DIMP the cost was 1,882 €.
Satisfaction of patient
N.A.
Satisfaction of HCP N.A. OTHER
Unique element(s) Streamlining and prioritizing of healthcare processes: transfer of certain amount of clinical responsibility from the ambulatory care service to the GP for patients with diabetes mellitus, type II, under stable metabolic conditions and with low complications impact.
Shortcomings - Use of m-health tools could be enhanced - Cooperation with more specialists could be established (dietist, etc.).
More information:
- European Innovation Partnership on Active and Health Ageing – p.55-56
9 | P a g e
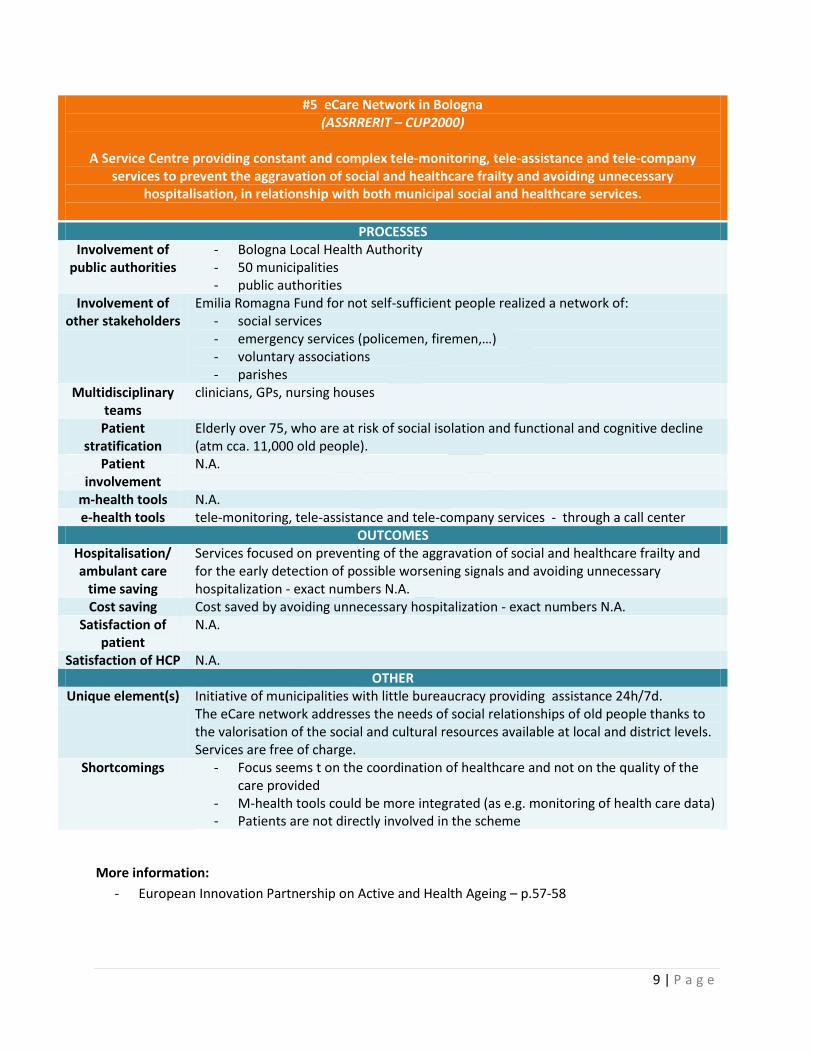
#5 eCare Network in Bologna (ASSRRERIT – CUP2000)
A Service Centre providing constant and complex tele-monitoring, tele-assistance and tele-company
services to prevent the aggravation of social and healthcare frailty and avoiding unnecessary hospitalisation, in relationship with both municipal social and healthcare services.
PROCESSES Involvement of
public authorities - Bologna Local Health Authority - 50 municipalities - public authorities
Involvement of other stakeholders
Emilia Romagna Fund for not self-sufficient people realized a network of: - social services - emergency services (policemen, firemen,…) - voluntary associations - parishes
Multidisciplinary teams
clinicians, GPs, nursing houses
Patient stratification
Elderly over 75, who are at risk of social isolation and functional and cognitive decline (atm cca. 11,000 old people).
Patient involvement
N.A.
m-health tools N.A. e-health tools tele-monitoring, tele-assistance and tele-company services - through a call center
OUTCOMES Hospitalisation/ ambulant care
time saving
Services focused on preventing of the aggravation of social and healthcare frailty and for the early detection of possible worsening signals and avoiding unnecessary hospitalization - exact numbers N.A.
Cost saving Cost saved by avoiding unnecessary hospitalization - exact numbers N.A. Satisfaction of
patient N.A.
Satisfaction of HCP N.A. OTHER
Unique element(s) Initiative of municipalities with little bureaucracy providing assistance 24h/7d. The eCare network addresses the needs of social relationships of old people thanks to the valorisation of the social and cultural resources available at local and district levels. Services are free of charge.
Shortcomings - Focus seems t on the coordination of healthcare and not on the quality of the care provided
- M-health tools could be more integrated (as e.g. monitoring of health care data) - Patients are not directly involved in the scheme
More information:
- European Innovation Partnership on Active and Health Ageing – p.57-58
10 | P a g e
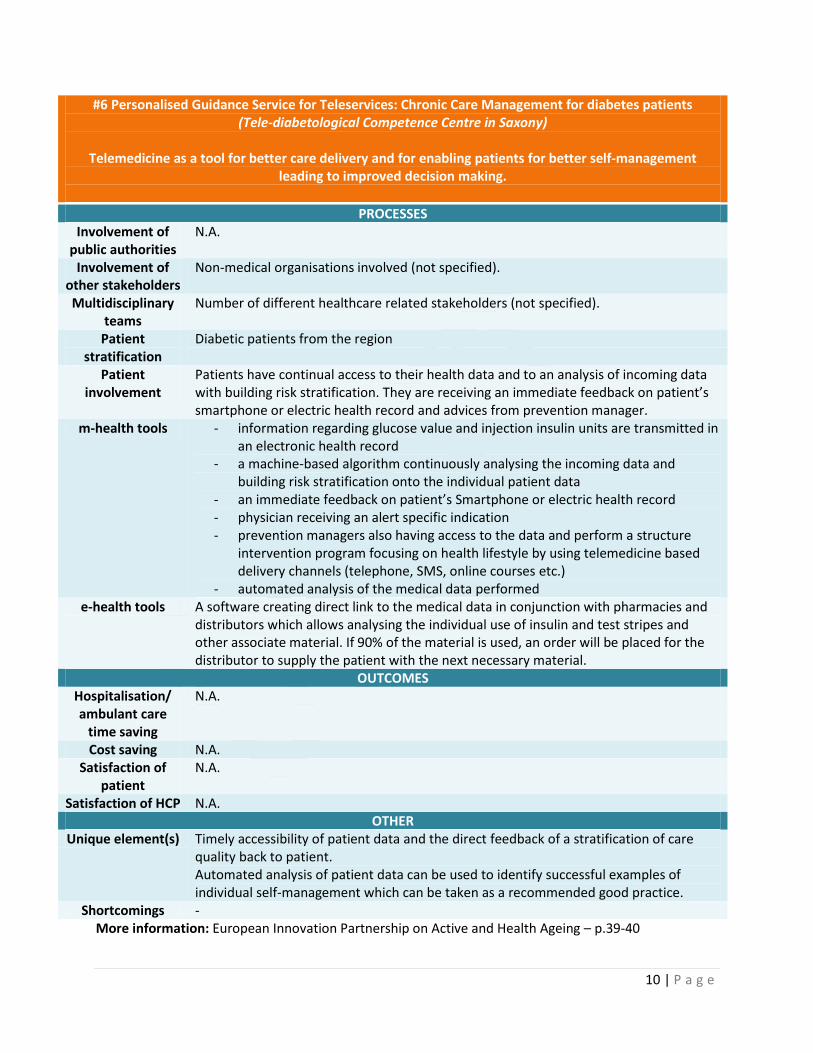
#6 Personalised Guidance Service for Teleservices: Chronic Care Management for diabetes patients (Tele-diabetological Competence Centre in Saxony)
Telemedicine as a tool for better care delivery and for enabling patients for better self-management
leading to improved decision making.
PROCESSES Involvement of
public authorities N.A.
Involvement of other stakeholders
Non-medical organisations involved (not specified).
Multidisciplinary teams
Number of different healthcare related stakeholders (not specified).
Patient stratification
Diabetic patients from the region
Patient involvement
Patients have continual access to their health data and to an analysis of incoming data with building risk stratification. They are receiving an immediate feedback on patient’s smartphone or electric health record and advices from prevention manager.
m-health tools - information regarding glucose value and injection insulin units are transmitted in an electronic health record
- a machine-based algorithm continuously analysing the incoming data and building risk stratification onto the individual patient data
- an immediate feedback on patient’s Smartphone or electric health record - physician receiving an alert specific indication - prevention managers also having access to the data and perform a structure
intervention program focusing on health lifestyle by using telemedicine based delivery channels (telephone, SMS, online courses etc.)
- automated analysis of the medical data performed e-health tools A software creating direct link to the medical data in conjunction with pharmacies and
distributors which allows analysing the individual use of insulin and test stripes and other associate material. If 90% of the material is used, an order will be placed for the distributor to supply the patient with the next necessary material.
OUTCOMES Hospitalisation/ ambulant care
time saving
N.A.
Cost saving N.A. Satisfaction of
patient N.A.
Satisfaction of HCP N.A. OTHER
Unique element(s) Timely accessibility of patient data and the direct feedback of a stratification of care quality back to patient. Automated analysis of patient data can be used to identify successful examples of individual self-management which can be taken as a recommended good practice.
Shortcomings - More information: European Innovation Partnership on Active and Health Ageing – p.39-40
11 | P a g e
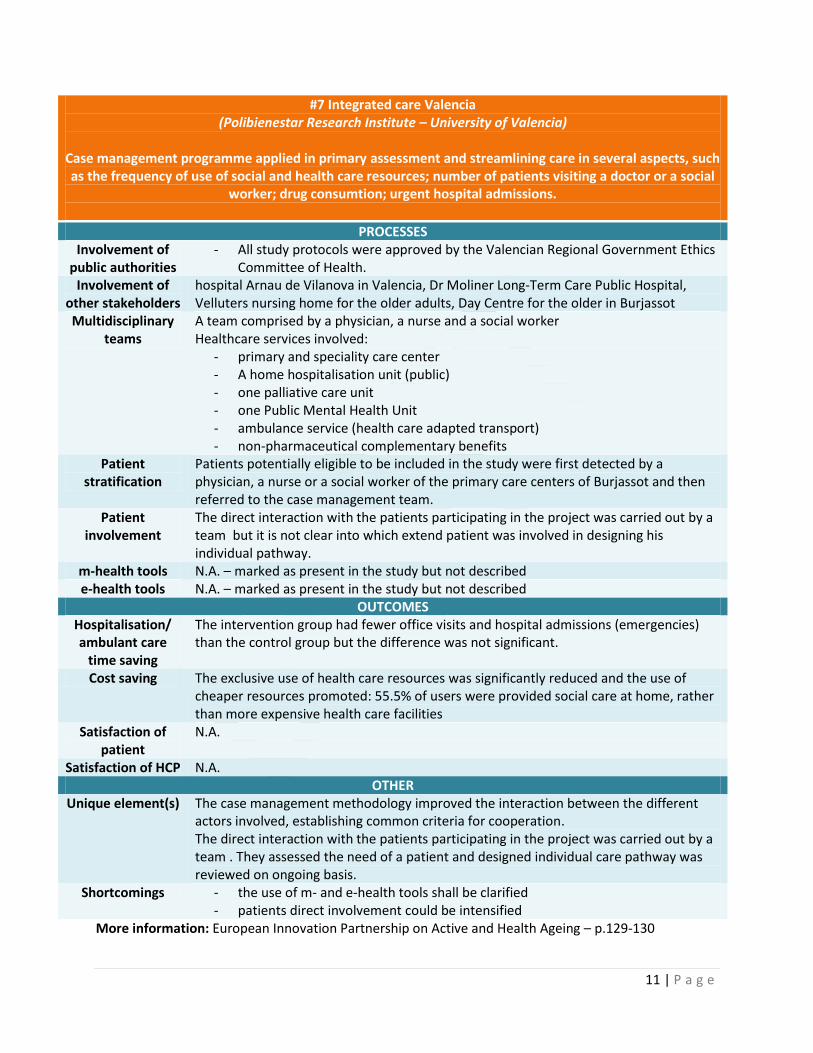
#7 Integrated care Valencia (Polibienestar Research Institute – University of Valencia)
Case management programme applied in primary assessment and streamlining care in several aspects, such as the frequency of use of social and health care resources; number of patients visiting a doctor or a social
worker; drug consumtion; urgent hospital admissions.
PROCESSES Involvement of
public authorities - All study protocols were approved by the Valencian Regional Government Ethics
Committee of Health. Involvement of
other stakeholders hospital Arnau de Vilanova in Valencia, Dr Moliner Long-Term Care Public Hospital, Velluters nursing home for the older adults, Day Centre for the older in Burjassot
Multidisciplinary teams
A team comprised by a physician, a nurse and a social worker Healthcare services involved:
- primary and speciality care center - A home hospitalisation unit (public) - one palliative care unit - one Public Mental Health Unit - ambulance service (health care adapted transport) - non-pharmaceutical complementary benefits
Patient stratification
Patients potentially eligible to be included in the study were first detected by a physician, a nurse or a social worker of the primary care centers of Burjassot and then referred to the case management team.
Patient involvement
The direct interaction with the patients participating in the project was carried out by a team but it is not clear into which extend patient was involved in designing his individual pathway.
m-health tools N.A. – marked as present in the study but not described e-health tools N.A. – marked as present in the study but not described
OUTCOMES Hospitalisation/ ambulant care
time saving
The intervention group had fewer office visits and hospital admissions (emergencies) than the control group but the difference was not significant.
Cost saving The exclusive use of health care resources was significantly reduced and the use of cheaper resources promoted: 55.5% of users were provided social care at home, rather than more expensive health care facilities
Satisfaction of patient
N.A.
Satisfaction of HCP N.A. OTHER
Unique element(s) The case management methodology improved the interaction between the different actors involved, establishing common criteria for cooperation. The direct interaction with the patients participating in the project was carried out by a team . They assessed the need of a patient and designed individual care pathway was reviewed on ongoing basis.
Shortcomings - the use of m- and e-health tools shall be clarified - patients direct involvement could be intensified
More information: European Innovation Partnership on Active and Health Ageing – p.129-130
12 | P a g e
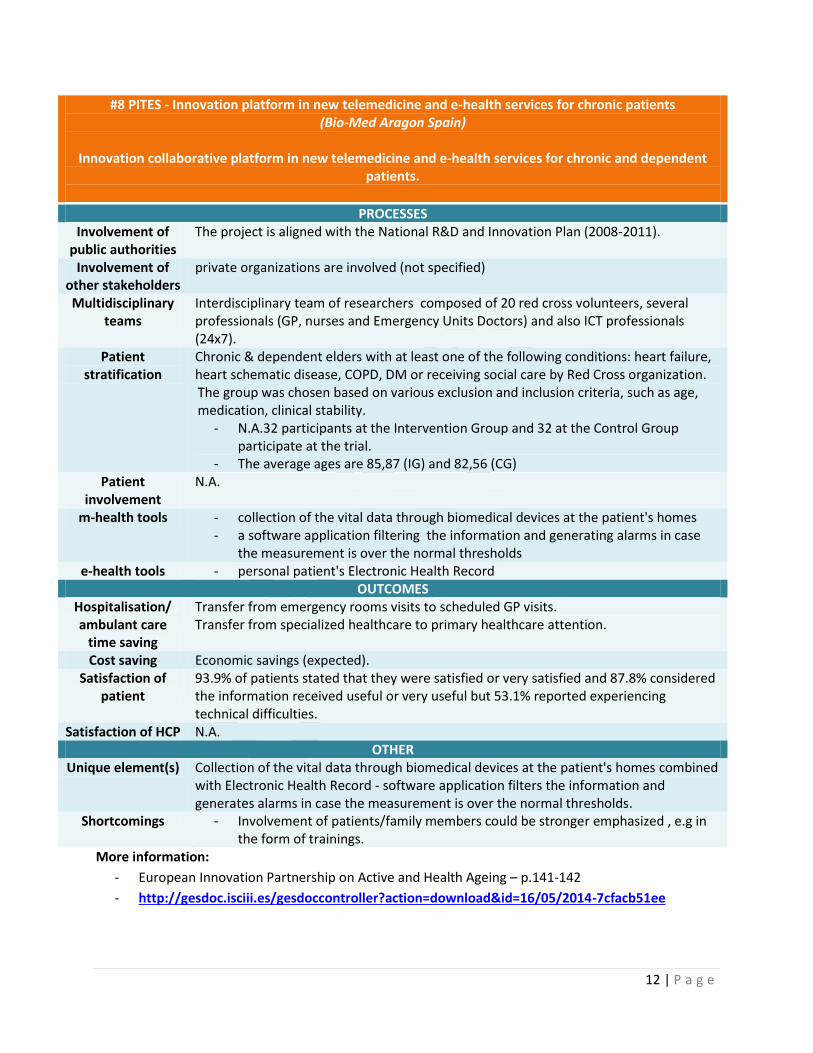
#8 PITES - Innovation platform in new telemedicine and e-health services for chronic patients (Bio-Med Aragon Spain)
Innovation collaborative platform in new telemedicine and e-health services for chronic and dependent
patients.
PROCESSES Involvement of
public authorities The project is aligned with the National R&D and Innovation Plan (2008-2011).
Involvement of
other stakeholders private organizations are involved (not specified)
Multidisciplinary teams
Interdisciplinary team of researchers composed of 20 red cross volunteers, several professionals (GP, nurses and Emergency Units Doctors) and also ICT professionals (24x7).
Patient stratification
Chronic & dependent elders with at least one of the following conditions: heart failure, heart schematic disease, COPD, DM or receiving social care by Red Cross organization. The group was chosen based on various exclusion and inclusion criteria, such as age, medication, clinical stability.
- N.A.32 participants at the Intervention Group and 32 at the Control Group participate at the trial.
- The average ages are 85,87 (IG) and 82,56 (CG) Patient
involvement N.A.
m-health tools - collection of the vital data through biomedical devices at the patient's homes - a software application filtering the information and generating alarms in case
the measurement is over the normal thresholds e-health tools - personal patient's Electronic Health Record
OUTCOMES Hospitalisation/ ambulant care
time saving
Transfer from emergency rooms visits to scheduled GP visits. Transfer from specialized healthcare to primary healthcare attention.
Cost saving Economic savings (expected). Satisfaction of
patient 93.9% of patients stated that they were satisfied or very satisfied and 87.8% considered the information received useful or very useful but 53.1% reported experiencing technical difficulties.
Satisfaction of HCP N.A. OTHER
Unique element(s) Collection of the vital data through biomedical devices at the patient's homes combined with Electronic Health Record - software application filters the information and generates alarms in case the measurement is over the normal thresholds.
Shortcomings - Involvement of patients/family members could be stronger emphasized , e.g in the form of trainings.
More information:
- European Innovation Partnership on Active and Health Ageing – p.141-142
- http://gesdoc.isciii.es/gesdoccontroller?action=download&id=16/05/2014-7cfacb51ee
13 | P a g e
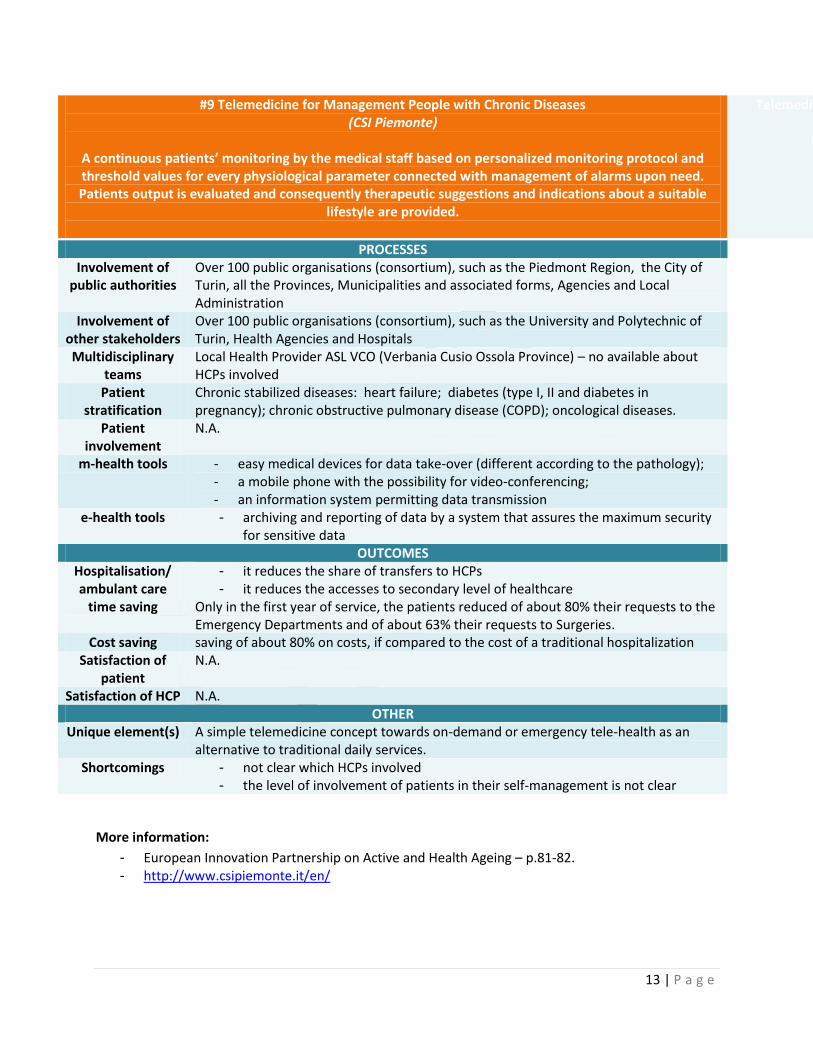
#9 Telemedicine for Management People with Chronic Diseases (CSI Piemonte)
A continuous patients’ monitoring by the medical staff based on personalized monitoring protocol and threshold values for every physiological parameter connected with management of alarms upon need. Patients output is evaluated and consequently therapeutic suggestions and indications about a suitable
lifestyle are provided.
Telemedicine for Management People with Chronic Diseases
(‘Telemedicine Piemont’)
PROCESSES Involvement of
public authorities Over 100 public organisations (consortium), such as the Piedmont Region, the City of Turin, all the Provinces, Municipalities and associated forms, Agencies and Local Administration
Involvement of other stakeholders
Over 100 public organisations (consortium), such as the University and Polytechnic of Turin, Health Agencies and Hospitals
Multidisciplinary teams
Local Health Provider ASL VCO (Verbania Cusio Ossola Province) – no available about HCPs involved
Patient stratification
Chronic stabilized diseases: heart failure; diabetes (type I, II and diabetes in pregnancy); chronic obstructive pulmonary disease (COPD); oncological diseases.
Patient involvement
N.A.
m-health tools - easy medical devices for data take-over (different according to the pathology); - a mobile phone with the possibility for video-conferencing; - an information system permitting data transmission
e-health tools - archiving and reporting of data by a system that assures the maximum security for sensitive data
OUTCOMES Hospitalisation/ ambulant care
time saving
- it reduces the share of transfers to HCPs - it reduces the accesses to secondary level of healthcare
Only in the first year of service, the patients reduced of about 80% their requests to the Emergency Departments and of about 63% their requests to Surgeries.
Cost saving saving of about 80% on costs, if compared to the cost of a traditional hospitalization Satisfaction of
patient N.A.
Satisfaction of HCP N.A. OTHER
Unique element(s) A simple telemedicine concept towards on-demand or emergency tele-health as an alternative to traditional daily services.
Shortcomings - not clear which HCPs involved - the level of involvement of patients in their self-management is not clear
More information:
- European Innovation Partnership on Active and Health Ageing – p.81-82. - http://www.csipiemonte.it/en/
14 | P a g e
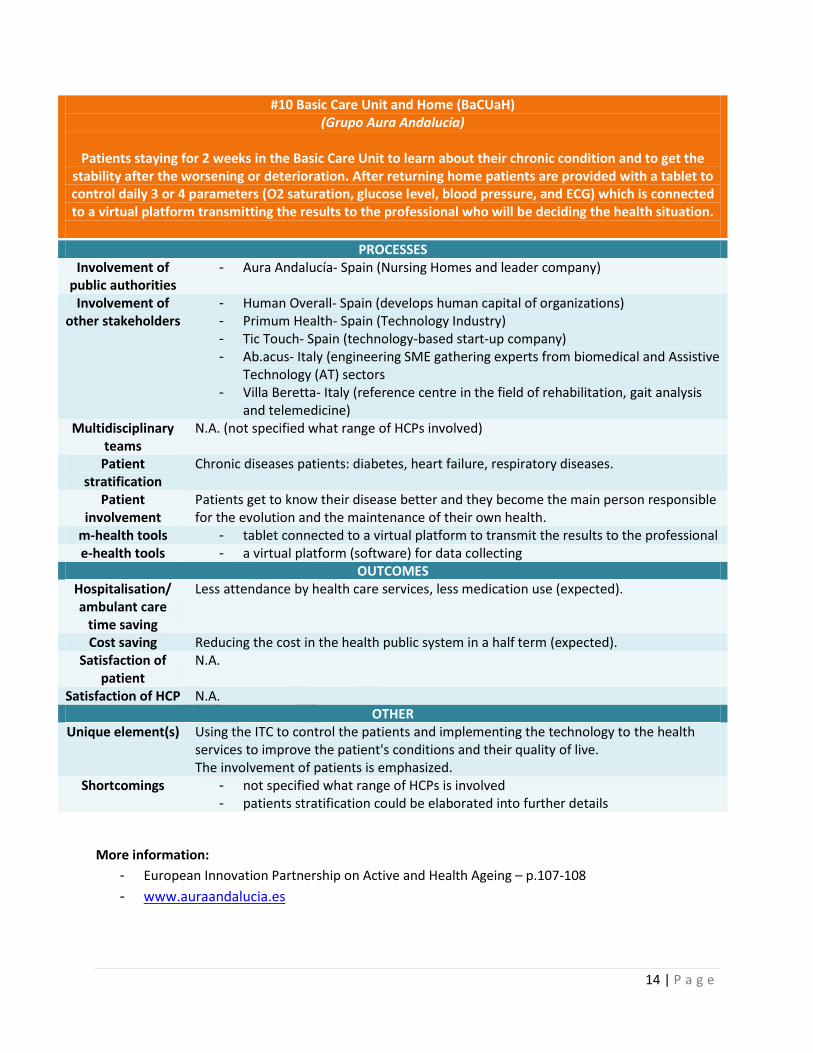
#10 Basic Care Unit and Home (BaCUaH) (Grupo Aura Andalucía)
Patients staying for 2 weeks in the Basic Care Unit to learn about their chronic condition and to get the
stability after the worsening or deterioration. After returning home patients are provided with a tablet to control daily 3 or 4 parameters (O2 saturation, glucose level, blood pressure, and ECG) which is connected to a virtual platform transmitting the results to the professional who will be deciding the health situation.
PROCESSES Involvement of
public authorities - Aura Andalucía- Spain (Nursing Homes and leader company)
Involvement of other stakeholders
- Human Overall- Spain (develops human capital of organizations) - Primum Health- Spain (Technology Industry) - Tic Touch- Spain (technology-based start-up company) - Ab.acus- Italy (engineering SME gathering experts from biomedical and Assistive
Technology (AT) sectors - Villa Beretta- Italy (reference centre in the field of rehabilitation, gait analysis
and telemedicine) Multidisciplinary
teams N.A. (not specified what range of HCPs involved)
Patient stratification
Chronic diseases patients: diabetes, heart failure, respiratory diseases.
Patient involvement
Patients get to know their disease better and they become the main person responsible for the evolution and the maintenance of their own health.
m-health tools - tablet connected to a virtual platform to transmit the results to the professional e-health tools - a virtual platform (software) for data collecting
OUTCOMES Hospitalisation/ ambulant care
time saving
Less attendance by health care services, less medication use (expected).
Cost saving Reducing the cost in the health public system in a half term (expected). Satisfaction of
patient N.A.
Satisfaction of HCP N.A. OTHER
Unique element(s) Using the ITC to control the patients and implementing the technology to the health services to improve the patient's conditions and their quality of live. The involvement of patients is emphasized.
Shortcomings - not specified what range of HCPs is involved - patients stratification could be elaborated into further details
More information:
- European Innovation Partnership on Active and Health Ageing – p.107-108
- www.auraandalucia.es
15 | P a g e
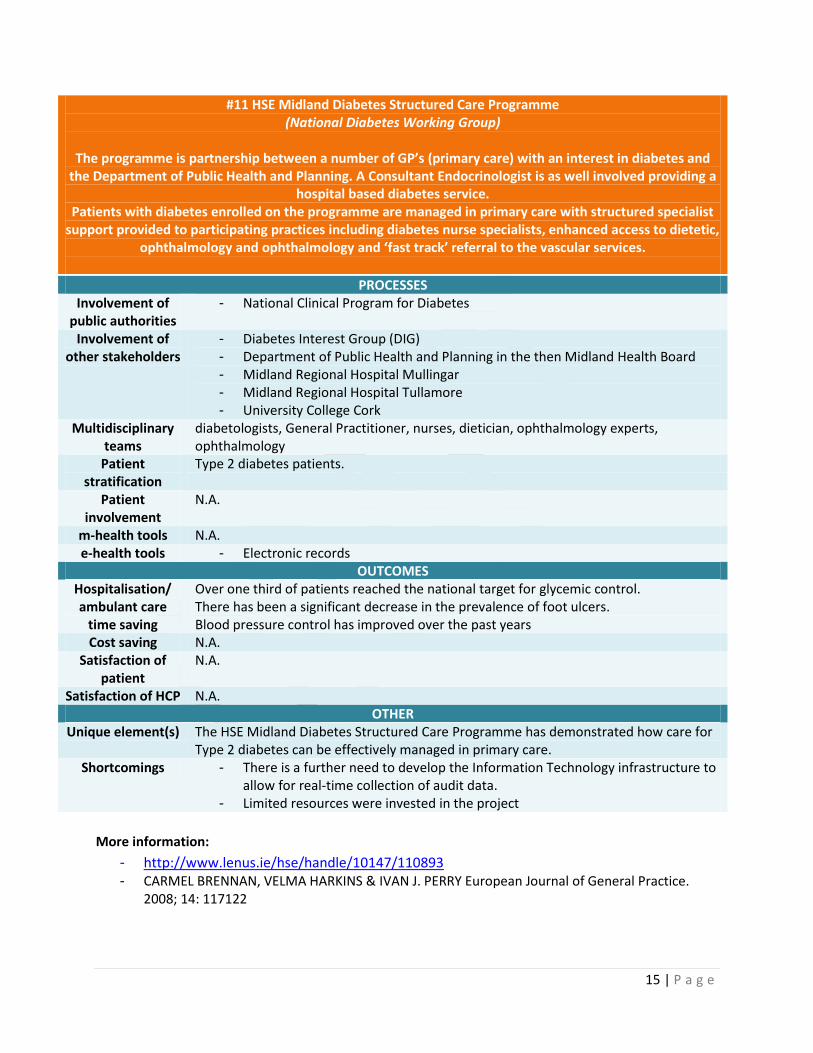
#11 HSE Midland Diabetes Structured Care Programme (National Diabetes Working Group)
The programme is partnership between a number of GP’s (primary care) with an interest in diabetes and
the Department of Public Health and Planning. A Consultant Endocrinologist is as well involved providing a hospital based diabetes service.
Patients with diabetes enrolled on the programme are managed in primary care with structured specialist support provided to participating practices including diabetes nurse specialists, enhanced access to dietetic,
ophthalmology and ophthalmology and ‘fast track’ referral to the vascular services.
PROCESSES Involvement of
public authorities - National Clinical Program for Diabetes
Involvement of other stakeholders
- Diabetes Interest Group (DIG) - Department of Public Health and Planning in the then Midland Health Board - Midland Regional Hospital Mullingar - Midland Regional Hospital Tullamore - University College Cork
Multidisciplinary teams
diabetologists, General Practitioner, nurses, dietician, ophthalmology experts, ophthalmology
Patient stratification
Type 2 diabetes patients.
Patient involvement
N.A.
m-health tools N.A. e-health tools - Electronic records
OUTCOMES Hospitalisation/ ambulant care
time saving
Over one third of patients reached the national target for glycemic control. There has been a significant decrease in the prevalence of foot ulcers. Blood pressure control has improved over the past years
Cost saving N.A. Satisfaction of
patient N.A.
Satisfaction of HCP N.A. OTHER
Unique element(s) The HSE Midland Diabetes Structured Care Programme has demonstrated how care for Type 2 diabetes can be effectively managed in primary care.
Shortcomings - There is a further need to develop the Information Technology infrastructure to allow for real-time collection of audit data.
- Limited resources were invested in the project
More information:
- http://www.lenus.ie/hse/handle/10147/110893 - CARMEL BRENNAN, VELMA HARKINS & IVAN J. PERRY European Journal of General Practice.
2008; 14: 117122
16 | P a g e
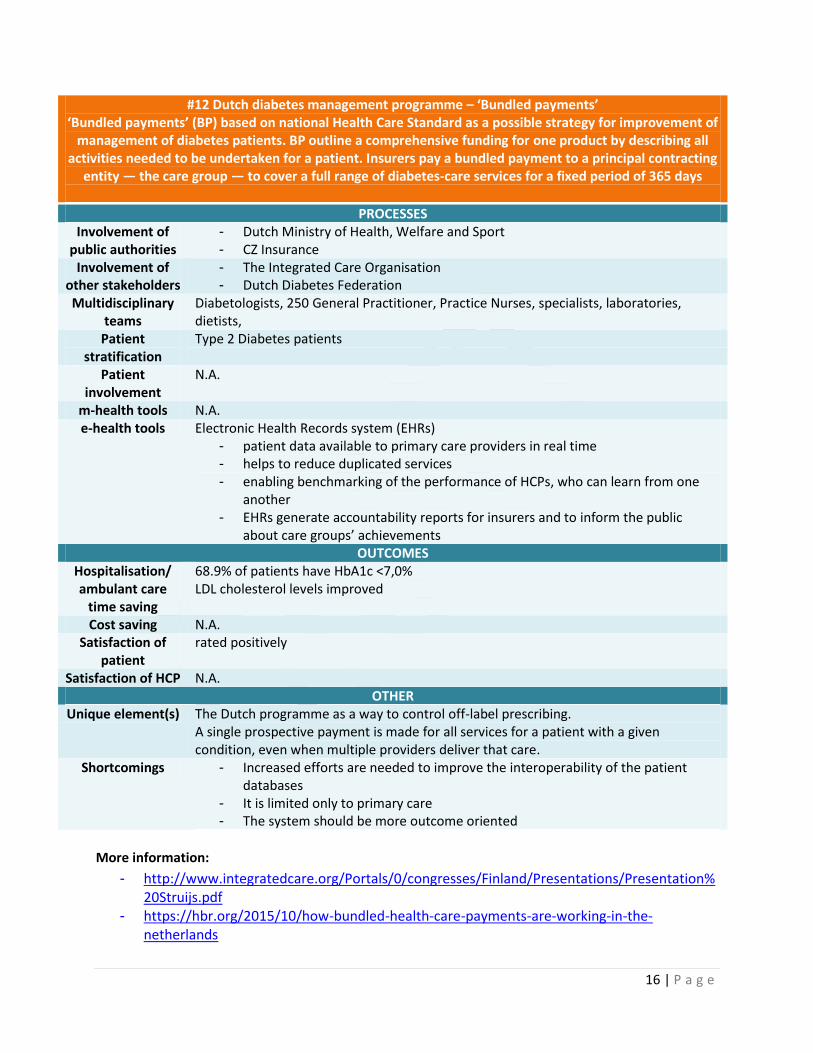
#12 Dutch diabetes management programme – ‘Bundled payments’ ‘Bundled payments’ (BP) based on national Health Care Standard as a possible strategy for improvement of
management of diabetes patients. BP outline a comprehensive funding for one product by describing all activities needed to be undertaken for a patient. Insurers pay a bundled payment to a principal contracting
entity — the care group — to cover a full range of diabetes-care services for a fixed period of 365 days
PROCESSES Involvement of
public authorities - Dutch Ministry of Health, Welfare and Sport - CZ Insurance
Involvement of other stakeholders
- The Integrated Care Organisation - Dutch Diabetes Federation
Multidisciplinary teams
Diabetologists, 250 General Practitioner, Practice Nurses, specialists, laboratories, dietists,
Patient stratification
Type 2 Diabetes patients
Patient involvement
N.A.
m-health tools N.A. e-health tools Electronic Health Records system (EHRs)
- patient data available to primary care providers in real time - helps to reduce duplicated services - enabling benchmarking of the performance of HCPs, who can learn from one
another - EHRs generate accountability reports for insurers and to inform the public
about care groups’ achievements OUTCOMES
Hospitalisation/ ambulant care
time saving
68.9% of patients have HbA1c <7,0% LDL cholesterol levels improved
Cost saving N.A. Satisfaction of
patient rated positively
Satisfaction of HCP N.A. OTHER
Unique element(s) The Dutch programme as a way to control off-label prescribing. A single prospective payment is made for all services for a patient with a given condition, even when multiple providers deliver that care.
Shortcomings - Increased efforts are needed to improve the interoperability of the patient databases
- It is limited only to primary care - The system should be more outcome oriented
More information:
- http://www.integratedcare.org/Portals/0/congresses/Finland/Presentations/Presentation%20Struijs.pdf
- https://hbr.org/2015/10/how-bundled-health-care-payments-are-working-in-the-netherlands
17 | P a g e
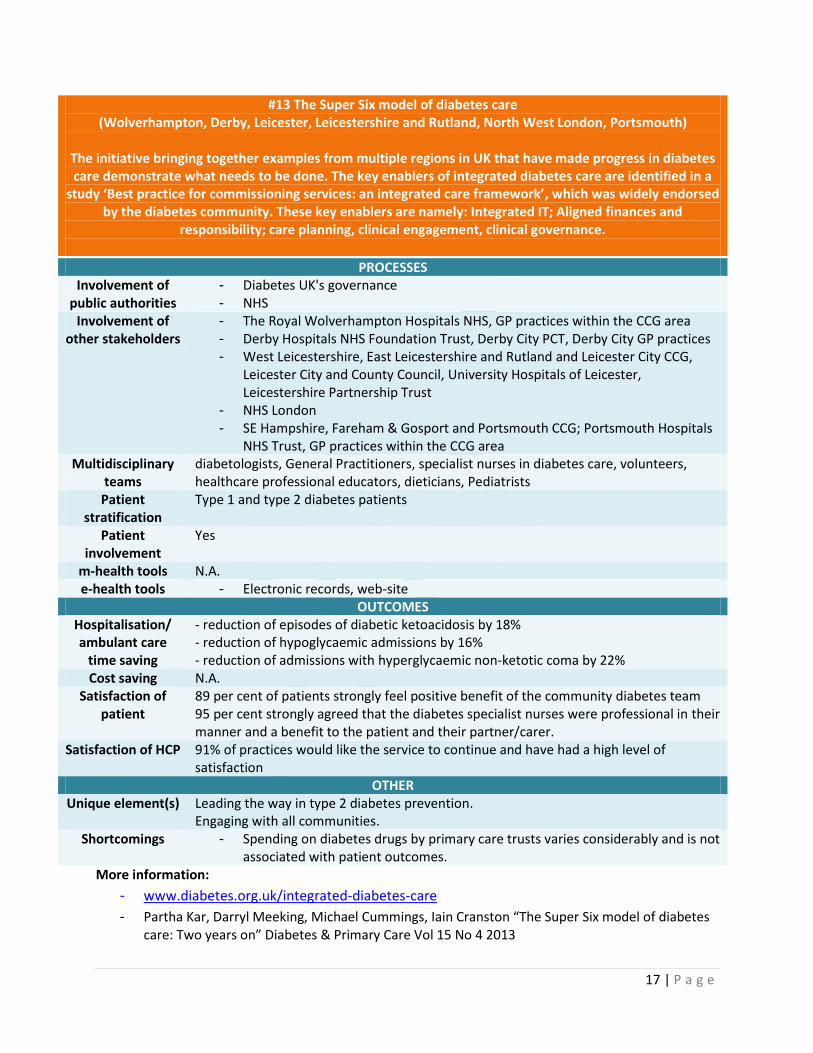
#13 The Super Six model of diabetes care (Wolverhampton, Derby, Leicester, Leicestershire and Rutland, North West London, Portsmouth)
The initiative bringing together examples from multiple regions in UK that have made progress in diabetes care demonstrate what needs to be done. The key enablers of integrated diabetes care are identified in a
study ‘Best practice for commissioning services: an integrated care framework’, which was widely endorsed by the diabetes community. These key enablers are namely: Integrated IT; Aligned finances and
responsibility; care planning, clinical engagement, clinical governance.
PROCESSES Involvement of
public authorities - Diabetes UK's governance - NHS
Involvement of other stakeholders
- The Royal Wolverhampton Hospitals NHS, GP practices within the CCG area - Derby Hospitals NHS Foundation Trust, Derby City PCT, Derby City GP practices - West Leicestershire, East Leicestershire and Rutland and Leicester City CCG,
Leicester City and County Council, University Hospitals of Leicester, Leicestershire Partnership Trust
- NHS London - SE Hampshire, Fareham & Gosport and Portsmouth CCG; Portsmouth Hospitals
NHS Trust, GP practices within the CCG area Multidisciplinary
teams diabetologists, General Practitioners, specialist nurses in diabetes care, volunteers, healthcare professional educators, dieticians, Pediatrists
Patient stratification
Type 1 and type 2 diabetes patients
Patient involvement
Yes
m-health tools N.A. e-health tools - Electronic records, web-site
OUTCOMES Hospitalisation/ ambulant care
time saving
- reduction of episodes of diabetic ketoacidosis by 18% - reduction of hypoglycaemic admissions by 16% - reduction of admissions with hyperglycaemic non-ketotic coma by 22%
Cost saving N.A. Satisfaction of
patient 89 per cent of patients strongly feel positive benefit of the community diabetes team 95 per cent strongly agreed that the diabetes specialist nurses were professional in their manner and a benefit to the patient and their partner/carer.
Satisfaction of HCP 91% of practices would like the service to continue and have had a high level of satisfaction
OTHER Unique element(s) Leading the way in type 2 diabetes prevention.
Engaging with all communities. Shortcomings - Spending on diabetes drugs by primary care trusts varies considerably and is not
associated with patient outcomes. More information:
- www.diabetes.org.uk/integrated-diabetes-care
- Partha Kar, Darryl Meeking, Michael Cummings, Iain Cranston “The Super Six model of diabetes care: Two years on” Diabetes & Primary Care Vol 15 No 4 2013





























