Embed Size (px)
Citation preview
Fframwaith GwasanaethCenedlaethol ar gyfer
Diabetes yng Nghymru
Strategaeth Gyflawni
GWELLA IECHYD YNG NGHYMRU
National Service Frameworkfor Diabetes in Wales
Delivery Strategy
IMPROVING HEALTH IN WALES
National Service Fram
ework for D
iabetes in Wales: D
elivery Strategy
Ffra
mw
aith
Gw
asan
aeth
Cen
edla
etho
l ar
gyfe
r D
iabe
tes
yng
Ngh
ymru
: Stra
tega
eth
Gyf
law
ni

© Crown copyright 2003Typeset by Text Processing Services
ISBN 0 7504 3136 3Designed by CartoGraphic Services G/600/02-03
March 2003INA - 15 - 02 - 533
© Hawlfraint y Goron 2003Cysodwyd gan y Gwasanaethau Prosesu Testun
ISBN 0 7504 3156 3Cynlluniwyd gan CartoGraffeg G/600/02-03
Mawrth 2003INA - 15 - 02 - 533
Improving Health in Wales
National Service Framework for Diabetes in Wales: Delivery Strategy
A national framework within which healthprofessionals, people living with diabetes and
communities can work together to improve diabetesservices in Wales.
Further copies of this document are available from
Health Services Policy and DevelopmentWelsh Assembly GovernmentCathays ParkCardiffCF10 3NQ
Tel: 029 2082 5519
The National Assembly for Wales Internet site at www.wales.gov.uk
Contents
Page
Foreword 1
Executive summary 3
Chapter 1 Setting the Scene 5
Chapter 2 Introduction to the Diabetes NSF for Wales 12
Chapter 3 Action and Structures to support Implementation 16
Chapter 4 Implementation and Action Plans 27
Annex 1 Summary of report - Information Management and Technology subgroup report 61
Annex 2 Clinical Terminology Support for the Diabetes National Service Framework 66
Annex 3 Health Promotion / Prevention Programmes 81
Annex 4 Summary of Market Research Wales Focus Groups 83
Annex 5 Training and Education 85
Annex 6 Summary of report -Patient Education and Support subgroup report 87
Annex 7 Summary of the Having Your Say Conference report 92
Annex 8 Membership of Implementation Group 93
Annex 9 Membership of the Project Board 94
Annex 10 References 95


Foreword
The recent Audit Commission ‘Service Review ofDiabetes in Wales’ - Primary Care Survey, indicates thatthe total number of people with diagnosed diabetes inWales is about 3.5% of the population, with thepossibility of as many as 50,000 people undiagnosed.The number of those affected by diabetes is predicted todouble worldwide, rising to at least 5% of the world
population by the year 20101, largely as a result of lifestyle factors, poordiet and lack of physical activity. This figure may already have been reachedin Wales.
Diabetes can have a significant impact on the quality of life of individuals,their families, friends, carers and the wider society. The emotional andsocial effects are often underestimated. If diabetes is poorly controlled orundetected, complications ensue, possibly resulting in heart attacks, strokes,foot ulcers, amputation of lower limbs, renal failure, nerve damage andblindness. In Wales, the prevalence of diabetes, and its complications, ishigher amongst people from some minority ethnic groups and those who aresocially disadvantaged.
Research has shown that better management of diabetes significantlyreduces the risk of developing complications. For example eye screening todetect diabetic retinopathy can reduce the incidence of blindness by half.The All Wales Diabetic Retinopathy Screening Programme will be asignificant advance in diabetes management in Wales.
There are many areas of good practice and good quality services acrossWales. We want to see good practice developed in all areas, therebyreducing the inequalities in health care. Everyone with diabetes deservesaccess to high quality care and support.
The Diabetes National Service Framework standards were launched inWales in April 2002. The Delivery Strategy is the foundation for theplanning and implementation of the standards and developing partnershipswith people with diabetes. Helping and supporting people to manage theircare in this way can reduce disability and life expectancy can be increased.
The NSF is a ten-year plan, and sets out national objectives against whichNHS performance can be judged. It offers local health services theopportunity to produce and disseminate implementation plans, and sets
1
targets, which will result in improved services and high quality care andsupport for all those with diabetes, their families, friends and carersthroughout Wales.
I would like to thank all those who have been involved in developing theDiabetes NSF Delivery Strategy, which offers the vision of the future ofdiabetes care in Wales.
Jane HuttMinister for Health and Social Services
2
Executive Summary
The Diabetes National Service Framework for Wales: Standards documentwas published in April 2002 and provides a vision of diabetes serviceswhich:
• leads to fewer people developing diabetes and improved care forpeople known to have diabetes
• is developed in partnership with health care staff, centred aroundthe needs of people with diabetes, equitable, integrated andfocused on delivering the best outcomes for the person with diabetes
• offers care that is structured and pro-active providing people andtheir carers with the support they need to manage their owncondition
• is encapsulated in standards, key interventions and implications forservice planning
The key elements proposed in the Delivery Strategy are:
• setting up local diabetes networks or similarly robust mechanism,strengthening joint partnerships between Local Health Boards andLocal Diabetes Service Advisory Groups
• reviewing the Audit Commission Baseline Service Review reports,establishing and promulgating local implementation arrangementsto achieve the standards
• putting in place registers and clinical management systemspublished with the Delivery Strategy (Annex 2)
• All Wales Diabetes Retinopathy Screening Service
• participating in comparative local and national audit
• dedicated education and advice for people with diabetes
• ensuring that staff working with people with diabetes engage incontinuous professional development and updating in diabeteseducation
3

The Delivery Strategy offers a framework for the NHS to build capacity to:
• put in place building blocks for the NHS to reach the NationalService Framework targets over the next ten years.
• deliver the national targets.
4

Chapter 1
Setting the Scene
What is diabetes?
Diabetes* is a chronic and progressive condition that impacts upon almostevery aspect of life. It can affect infants, children, young people and adultsof all ages, and is becoming more common. Whilst diabetes can result in illhealth, disability and even in premature death, these can often be preventedor delayed by effective self-management, education and high-quality care.About 9%2 of acute sector NHS costs are spent on diabetes and themanagement of its complications. Diabetes can also have a significantimpact on the families or carers of people with diabetes and considerationof their needs is also paramount. Diabetes comprises a group of disorderswith many different causes, all of which are characterised by a raised bloodglucose level. This is the result of a lack of the hormone insulin and/or thebody’s inability to utilise it.
There are two main types of diabetes: Type 1 diabetes andType 2 diabetes.
Type 1 diabetes:
In people with Type 1 diabetes, the pancreas is no longer able to produceinsulin because the insulin-producing ß-cells cells have been destroyed by thebody's immune system. Without insulin to move glucose from thebloodstream to the body's cells, glucose builds up in the blood and isexcreted in the urine. Type 1 diabetes develops most frequently in children,young people and young adults. About 15% of people with diabetes haveType 1 diabetes. Symptoms can include increased or excessive thirst,passing urine frequently – particularly during the night, often resulting inenuresis - (bed-wetting, especially in children), weight loss despite increasedappetite, tiredness and blurred vision.
Type 1 diabetes is usually diagnosed as a result of the presence of acombination of characteristic symptoms plus an elevated blood glucoselevel. People with Type 1 diabetes need daily injections of insulin to survive.Failure to take insulin can result in hyperglycaemia, and eventually diabeticketoacidosis**. If too much insulin is injected relative to diet and physical
5
* In this document the term diabetes refers to diabetes mellitus** Diabetic ketoacidosis is potentially a life threatening complication of diabetes caused by aninadequate concentration of insulin in the blood for the body’s requirements
activity levels, this can lead to hypoglycaemia (very low blood glucose). Bothhyperglycaemia and hypoglycaemia can lead to coma and, if untreated,death.
To prevent short and long term complications, people with diabetes need tomaintain their blood glucose within certain limits, which will requireadjustments in their diet, activity and lifestyle.
Type 2 diabetes:
About 85% of people with diabetes have Type 2 diabetes, which in manycases could either have been prevented or its onset delayed. In Type 2diabetes, the pancreas ß-cells are not able to produce sufficient insulin forthe body’s needs, or the body is unable to properly utilise insulin produced(insulin resistance). Type 2 diabetes is most commonly diagnosed in adultsover the age of 40, and many may have a close relative who has diabetes,although increasingly it is appearing in children and young adults.Symptoms usually appear more gradually than in the case of Type 1diabetes, and diabetes may not be diagnosed for some years. The majorityof people with Type 2 diabetes are overweight or obese and do not takeenough exercise. The most significant modifiable risk factor for Type 2diabetes is to tackle overweight and obesity. These issues will therefore needto be central to local health prevention and promotion strategies.Establishing control of diabetes, including weight and activity managementas well as control of blood glucose, blood pressure and lipids will contributeto better outcomes. Of particular concern, Type 2 diabetes, previouslyconsidered an adult condition, is now increasingly being seen in overweightchildren, who could face very serious health consequences in the long term.
The National Institute for Clinical Excellence will be publishing guidelines onType 1 and Type 2 diabetes as well as a series of appraisals which will alsobe applicable in Wales. Details can be found at www.nice.org.uk
Complications of Diabetes
People with diabetes are more at risk of complications if they experience anyof the following: prolonged hyperglycaemia, hypertension or dyslipidaemia.These manifestations of the condition can result in small (microvascular) orlarge (macrovascular) blood vessel damage. This small or large vesseldamage manifests itself by reducing the blood supply to essential organs.
6
The microvascular complications are:
Diabetic retinopathy: Damage to the eyes, which can lead to visual impairment and blindness.Diabetes is the leading cause of blindness in people of working age.3
Diabetic nephropathy: Damage to the kidney, which can lead to progressive renal failure. Diabetesis the leading cause of renal failure, accounting for more than one in sixpeople starting renal replacement therapy.4
Diabetic neuropathy: Damage to the nerves supplying the lower limbs can lead to loss of sensationin the feet, thereby predisposing to the development of foot ulcers, sometimesrequiring lower limb amputation5. Diabetes is the second commonest causeof lower limb amputation.6 Damage to other nerves can lead to a variety ofsymptoms, including postural hypotension, gustatory (abnormal) sweating,gastrointestinal problems (such as diarrhoea), difficulties with bladderemptying and erectile dysfunction (impotence).
The macrovascular complications are:
Coronary heart disease:Which can include angina, acute myocardial infarction (heart attack) andheart failure. Mortality rates from coronary heart disease are up to five timeshigher for people with diabetes.7
Cerebrovascular disease:Strokes and transient ischaemic attacks can occur when the vessels supplyingthe brain/brainstem become damaged. Stroke is three times more frequentin people with diabetes.8
Peripheral vascular disease:Damage to the blood vessels supplying the legs resulting in poor circulation.Affected people may experience pain in the calves and are sixteen timesmore likely, than a person without diabetes, to require amputation of lowerlimbs.9
7
Other Complications of Diabetes
Complications during pregnancy and birth: Diabetes, if not wellcontrolled during pre-conception or in pregnancy, can result in an increasedrisk of congenital malformation of the foetus, intrauterine death ormacrosomia (heavy birth weight) babies. Babies born to mothers withdiabetes are also more likely to require neo-natal care.10 11 12
Cataracts, which are twice as common in people with diabetes and occurabout 10 years earlier than in people who do not have diabetes.
Infections, particularly affecting the urinary tract and the skin.
Dental, periodontal gum disease (which can significantly affect glycaemiccontrol) is commoner in people with diabetes.
Soft tissue conditions, such as frozen shoulder and trigger finger.
Skin conditions, some of which are specific to people with diabetes.
Mental health problems, including depression and eating disorders.
THE IMPACT AND COST OF DIABETES
As a life-long condition, diabetes can have a profound impact on lifestyle,relationships, work, income, health, well being and life expectancy. It has amajor impact on the physical, psychological and material well being ofindividuals, their families and carers, as well as on health and socialservices:
• Life expectancy is reduced, on average, by more than 20 years inpeople with Type 1 diabetes and by up to 10 years in people withType 2 diabetes.13
• Diabetes incurs significant direct personal costs for people withdiabetes, including costs associated with managing their diabetes.The average cost in 1999 was estimated to be £802 per year pluslost earnings.
• The presence of diabetic complications increases personalexpenditure three-fold, and doubles the chance of the person withdiabetes requiring a carer.14
8
Diabetes also has a significant impact on health and social services:
• Around 9% of acute sector NHS costs spent on diabetes andmanagement of its complications.15
• People with diabetes are twice as likely to be admitted to hospitalas the general population and, once admitted, are likely to have alength of stay that is up to twice the average.16
• The presence of diabetic complications increases NHS costs morethan five-fold. People with diabetes are five times more likely toneed hospital admission.
• One in 20 people with diabetes incurs social services costs and, forthese people, the average annual costs were £2,450 in 1999, andare likely to have increased since then. More than three-quarters ofthese costs were associated with residential and nursing care, whilehome help services accounted for a further one fifth. The presenceof complications increased social services costs four-fold.17
Diabetes does not affect everyone equally
Significant inequalities exist in the risk of developing diabetes, in access tohealth services, the quality of those services, and in health outcomes,particularly with regard to Type 2 diabetes.
Type 2 diabetes is up to six times more common in people of South Asian(Indian, Pakistani and Bangladeshi) descent and up to three times morecommon in those of African and African-Caribbean descent, compared withthe white population. It is also more common in people of Chinese descent.18
The prevalence of diabetes rises steeply with age: one in 20 people over theage of 65 in the UK has diabetes and in people over the age of 85 yearsthis rises to one in five. The diagnosis of diabetes may be delayed in olderpeople, with symptoms being wrongly attributed to ageing. Older peoplemay experience discrimination in the degree of active management offeredcompared with younger people, this is clearly unacceptable. 19
9
Type 2 diabetes is more prevalent among less affluent populations. Those inthe most deprived fifth of the population are one-and-a-half times more likelythan average to have diabetes at any given age.20 Both mortality andmorbidity are increased by socio-economic deprivation. Morbidity resultingfrom diabetes complications is three-and-a-half times higher in social class 5than social class I.21
Socially excluded groups – including those in custodial settings, refugeesand asylum seekers, people with learning disabilities or mental healthproblems and people who reside in Nursing or Residential Care Homes –may be more prone to the complications of diabetes and receive poorerquality care. Also, the number of people at high risk of diabetes and thosewith diabetes in the hard-to-reach groups are over-represented in the prisonpopulation. Close partnership working between the prison health care teamand the local NHS specialist diabetes service is essential.22
The frequency of diabetes is higher in men than women. However, womenwith diabetes are at relatively greater risk of dying than men.
Risk may accumulate if an individual belongs to more than oneof these groups
Our developing understanding of diabetes
The last hundred years have seen significant advances in our understandingof diabetes, and our capacity to treat it and enable people to live longer andhealthier lives. Today, with the support of high-quality health care, peoplewith diabetes have the potential to live long lives, free of the devastatingcomplications suffered by previous generations. The St. Vincent Declaration,ratified by the World Health Organisation’s Regional Committee for Europein 1991, set aspirations and goals for reducing the impact of diabetes. Sincethen, there have been significant developments, including:
• Evidence that the onset of Type 2 diabetes can be delayed or evenprevented.
• Evidence that tight control of blood glucose and blood pressureincreases life expectancy and improves quality of life for people withboth Type 1 and Type 2 diabetes, by reducing the risks of thedevelopment of the complications of diabetes.
10

• Evidence that supported self-care improves outcomes, with thediabetes specialist nurse playing a key role.
• New and improved therapies.
• Effective organisation, involving a register, recall system and reviewfor people with diabetes.
11
Chapter 2
Introduction to the Diabetes National ServiceFramework (NSF) for Wales
The Assembly is looking to develop a coherent programme of NationalService Frameworks (NSFs) that must take account of the wider priorities forimproving health in Wales working in partnership with the Department ofHealth and other key partners on underpinning programmes to supportdelivery.
The NSF programme was established to define standards and servicemodels, together with milestones and performance managementarrangements for implementation, to improve service quality and tacklevariations in care. It sets out a ten-year programme of change to deliver firstclass care and support for children and adults with diabetes.
The NSF has been developed as two documents:
1. The 12 NSF Standards, published in April 2002, showing the level ofdiabetes care that we need to reach. The Standards were informed by theadvice of an External Reference Group, and set out the aims, standards,rationales and key interventions, together with the implications forplanning services.
2. The Delivery Strategy will assist in identifying how the Standards can bebest implemented. It offers a systematic programme of reform providing aclear direction and scope for local priorities across Wales, enabling localstaff to build upon existing good practice as well as closing any gaps inservice provision.
In keeping with the principles of Improving Health in Wales23 and BetterHealth, Better Wales, the primary goal is to enable the person with diabetes,or those at risk of developing diabetes, to manage their own lifestyle anddiabetes, through support and structured education as well as drugs andtreatments. Evidence suggests that a partnership between the person withdiabetes and their clinical and support team can improve outcomes andquality of life. Delivering this vision and embedding these principles inpractice requires staff throughout the NHS to understand the experience ofpeople with diabetes and diabetes care, and to recognise the expertise ofpeople who live with diabetes.
12
A Diabetes NSF Implementation Group (External Reference Group) was setup in Wales in 2001 to steer the development of the National ServiceFramework. It was a multi-agency, multi-professional group, includingpatients and carers. The Group worked with a wide range of stakeholdersand advised on the production of the Standards Document, Baseline Reviewand Delivery Strategy. Workshops, focus groups and conferences were heldto inform this process. The Project Board substituted the ImplementationGroup in January 2003, bringing together the External and InternalReference Groups.
In 2001, the Welsh Assembly Government identified the importance oftaking forward initiatives in preparation for the Diabetes NSF. One million-pound was allocated to LHGs and Trusts for a period of three years.£250,000 a year funded national projects on an All Wales basis to assistwith the development of the Delivery Strategy.
A NSF Officer was funded by the Welsh Assembly to work in partnershipwith Diabetes UK Cymru to help engage the views of people living withdiabetes in supporting the delivery of the NSF.
The Delivery Strategy identifies the key actions needed, based on researchevidence commissioned to help inform the process, and the views andexperiences of people with diabetes. The Baseline Review undertaken by theAudit Commission24, Market Research Wales Focus Group work and thereport of the Health Services Ombudsman25 have all informed thedevelopment of this NSF. More details are provided on the Diabetes NSFweb page, www.wales.nhs.uk (click on Subject Index, Health and NationalService Framework).
This NSF aims to "empower people with diabetes through skills,knowledge and access to services to manage their owndiabetes, with support, and fulfil their potential to live longlives free of the complications that can accompany diabetes".
To achieve this, NSF implementation needs to be:
• Person-centred: empowering the individual to adopt a healthylifestyle and to manage their own diabetes, through education andsupport which recognises the importance of lifestyle, culture andreligion, and where necessary, tackles the adverse impact ofmaterial disadvantage and social exclusion.
13
• Developed in partnership: ensuring goals and the respectiveresponsibilities of the individual and the diabetes team are agreedand clearly set out in a regularly reviewed care plan.
• Equitable: ensuring that services are planned to meet the needs ofthe population, including specific groups within the population, andare appropriate to individuals’ needs.
• Integrated: drawing on the knowledge and skills of health andsocial care professionals across a multidisciplinary diabetes healthcare team, including primary care, social care, the voluntary sectorand specialist services, and maximising the quality of life forindividuals by empowering staff to deliver, evaluate and measurecare.
• Targeted: narrowing the inequalities gap by targeting groups withthe greatest health needs; minimising the risk of developing diabetesand its complications.
Links with other strategies
The NSF for Diabetes builds on other healthcare priorities:
The Welsh NSF for coronary heart disease (CHD) Tackling CoronaryHeart Disease in Wales: Implementing Through Evidence: Thereis considerable overlap between CHD and diabetes. Preventing or delayingthe onset of diabetes and good management of diabetes will contribute tothe achievement of the goals of the Implementing Through Evidencedocument.
Renal Services: Diabetes is a major cause of end-stage renal failure, andof the need for dialysis and kidney transplant. Improving the care of peoplewith diabetes will reduce the development and progression of renal disease,potentially reducing the number of people who develop end-stage renalfailure, and therefore helping to realise the aims of the proposed Renal NSFfor Wales.
Children: Diabetes can affect children of all ages. Developing services thatput children and young people with diabetes at the centre of care, andsupport them through the transition to adult services, will provide a model forthe forthcoming Children’s National Service Framework.
14
Older People: The prevalence of diabetes increases with age. Poorlycontrolled diabetes increases the risk of hospital admission and prolongslength of stay. This NSF will help contribute to further work being undertakenon older people through the Older People’s NSF.
Welsh Language Act 1993
In the context of Wales, the provision of a quality service involves havingdue regard to the provision of care in Welsh and English (and otherlanguages) according to the wishes of the patient. Organisations arereminded of their responsibilities under their Welsh Language Schemes totreat English and Welsh on the basis of equality in their dealings with thepublic in this context. Even when not explicitly stated, these requirementsneed to be applied to all aspects of service planning and delivery outlinedin the document.
This discipline offers a vehicle to also give consideration to the needs ofthose who speak other languages. This is particularly relevant given the highprevalence of diabetes in certain minority ethnic communities in Wales andthe UK as a whole.
15
Chapter 3
Actions and structures to supportImplementation
The context for Implementation
In November 2001 the Minister for Health and Social Services announcedthe structural changes to deliver the renewal of the NHS in Wales set out inImproving Health in Wales - A Plan for the NHS with its partners.23
The five Health Authorities in Wales were abolished in April 2003 and astatutory Local Health Board (LHB) established in each local authority area.LHBs provide the building blocks of the new NHS in Wales, becoming thelead organisations in assessing need, planning and securing health servicesand improving health. They work in partnership with communities and leadthe NHS contribution to work jointly with local government and otherpartners. There is a duty placed on each Local Health Board and LocalAuthority to work together to develop and implement a strategy for health,social care and well being for people in the area. This will include agreeingjoint investment priorities and the joint planning of interface services, basedon a joint assessment of need.
LHBs, Local Authorities, NHS Trusts and the voluntary sector will worktogether to ensure joined-up, and where appropriate, integratedcommissioning arrangements for hospital and community services withinlocal authority areas. There will be some 14 local partnerships throughoutWales linking LHBs, local authorities and NHS Trusts, to secure the bestpossible range and quality of services through effective value for moneycommissioning.
In addition to securing tertiary services, the Specialist Services Commissionfor Wales will be strengthened to provide dedicated guidance, support andfacilitation more generally in relation to acute services commissioning. It willalso provide advice to the NHS in Wales in relation to more specialisedsecondary and regional services commissioning. NHS Trusts will continueto provide services, working within delivery agreements.
There will be a strengthening of the NHS Directorate within the NationalAssembly, both in the area of strategic planning and in the operational arm
16
of the organisation. This includes the establishment of three RegionalAssembly Offices in North, Mid and West and South Wales, ensuring thatconcerted effort at national and local levels will deliver local services toprovide national standards of care.
The NHS Directorate will focus on supporting the delivery of the health andwell-being agenda set out in the NHS Plan for Wales. An ImplementationProgramme sets out actions and milestones required to ensure that theundertakings in the NHS Plan for Wales be delivered.
Workforce Planning
Workforce planning data is collected annually from NHS Trusts and LHBs inWales and used to inform the commissioning of centrally funded educationand training for healthcare professional staff. The numbers of training placescommissioned each year directly relate to the number of newly qualified staffthe NHS forecasts it will require. The workforce planning process is basedon identified need rather than on affordability.
An all staff, all Wales approach is taken when dealing with workforce issuesin Wales. The All Wales Workforce Development Steering Group, chairedby the Director of NHS Wales, has been established to support the servicein filling its current vacancies and increasing staffing levels in line with thestaffing targets set in October 2002. Sub Groups have also been set up tosupport the Steering Group. A NSF and Clinical Networks sub group is oneof these and is to be established in the near future. Workforce issues relatingto the Diabetes NSF will be dealt with through this mechanism.
The workforce planning process collects data on Endocrinology andDiabetes Mellitus (Consultants, Associate Specialists and Staff Grades). Datais collected on all staff groups who have an input into diabetes care,including nurses, Allied Health Professionals (including dieticians), ClinicalScientists and also staff in Primary Care. This information, however, is notbroken down into care specific categories.
Research and Development
A review of the current and future research on Diabetes in the UnitedKingdom "Current and Future Research on Diabetes, A Review for theDepartment of Health and the Medical Research Council" has beenpublished with the English delivery Strategy for Diabetes and is available on
17
the Department of Health’s web-site. The review was conducted by anAdvisory Committee and informed by an open public consultation organisedin conjunction with Diabetes UK.
A key theme from the review highlights opportunities for translating thebiomedical science research into clinical and public health practice. TheWelsh Assembly Government will be considering how best to take thisforward in the context of the research and development strategy for healthand social care.
Local action to support planning
Improving Health in Wales sets out clearly, how all parts of the NHSwill work together to develop partnerships that lead to improved patient-centred services. Building upon the experience of CHD, cancer and otherareas, this section describes the organisational steps the LHBs should take toassist Diabetes NSF implementation. They should ensure that mechanismsare in place that:
• engage all stakeholders, including clinical and other staff,managers, people living with diabetes, local authorities, thevoluntary sector and the independent/private sector.
• work across traditional service boundaries.
• have clear lines of accountability.
Realising these three principles and building on the Audit Commissionreports, the LHBs will produce local implementation plans.
Many parts of Wales already have Local Diabetes Advisory Groups(LDSAGs) that have membership from key stakeholders, including healthcareprofessionals, managers, voluntary sector, people with diabetes and theircarers. They have always championed a patient-centred approachencouraging the involvement of people with diabetes in planning localservices. Where LDSAGs already exist and operate successfully, LHBs maychoose to develop them as a mechanism for local Diabetes NSFimplementation. Where they do not currently exist or operate successfully,LHBs will need to establish groups with multi-stakeholder input as part of theimplementation process. The role of these local implementation groups (orLDSAGs) should include;
18
• development of a local plan for diabetes care and prevention, withspecific locally agreed objectives and targets.
• advising on the development of a service specification and protocolsto meet identified needs.
• developing systems to facilitate the achievement of the targets andof user satisfaction.
• monitoring and auditing the quality of the service against the targetsand standards set.
• developing a local information system to assist in this process andidentify shortfalls.
• links between the deliverers and receivers of care.
The involvement of people living with diabetes in LDSAGs (or equivalent) willneed to be facilitated by adequate training and support.
Each LDSAG will require a user reference group of people living withdiabetes, supported by the NHS locally. This will require modest investmentto facilitate meetings, including provision of a suitable venue, lightrefreshments and secretarial/administrative support. It is envisaged that inmany cases, but not exclusively, a NHS Trust and the LHB(s) area(s) it serveswill form the basis of the Group.
Evaluating Performance
As with all strategies and frameworks it will be important to ensure that therecommendations contained in the Diabetes NSF bring about thechanges/outcomes needed and envisaged. An essential part of the NSFdevelopment process will therefore be the agreement and implementation of:
• outcome measures – to ensure that the results expected from theimplementation of the NSF are achieved by the procedures andprocesses put in place.
• performance indicators – to ensure that on-going improvementand progress is achieved in line with agreed annual targets.
19
Minimum Standards and Continuous Improvement
As referred to above there is a need to set measures and targets with dueregard to the Performance Improvement Frameworks under which health andsocial care organisations and professionals operate.
The priorities and requirements of the Welsh Assembly Government for theNHS in Wales for 2003-2004, issued in January 2003 (WHC (2003) 01),set a precedent for the establishment of minimum standards – targets thatmust be achieved by all health organisations and are hence absolutestandards; and continuous improvement targets that contain an expectationthat substantial and demonstrable progress will be made towards them i.e.quantifiable and substantial improvement over the financial year in theseareas. Attention should be paid to this approach in the setting of NSFrelated measures and targets.
The emphasis in the SaFF (Service and Financial Framework) round will beon re-engineering and innovation, incorporating changes in clinicalpractice, which will streamline pathways of care and create more efficient,high quality and cost effective services. There will also be a focus on themanagement of demand and capacity across the health system. Theallocation of funds to LHGs made available, by the Minister in 2001, forprojects relating to the NSF, continues until March 2004.
The Audit Commission identified that funding for diabetes servicesthroughout Wales was difficult to identify, as historically, it has emanatedfrom the ‘general medical purse’. The financial requirements forimplementation of the Diabetes NSF will be identified by each LHB/LDSAGduring planning of the service developments required to attain the objectivesof the Standards. The Audit Commission reports issued to each LHB willassist in the planning process and will then be reflected in the SaFF process.The pace of development over the ten-year period will need to be consideredalongside available funding and will have to be phased accordingly.
Clinical Audit
A clinical information report has been produced to support this DeliveryStrategy. This will assist the production of information, including appropriateREAD coding, audit framework, and guidelines on how to use them,replicating the requirements of the quality indicators within the new GMScontract (See Annex 2).
20

In the future, national clinical audit developments will be steered by theOffice for Information on Health Care Performance being established withinthe Commission for Health Audit and Improvement (CHAI). The Office willbe responsible for assessing performance (including clinical andperformance indicators), national clinical audits and national surveys ofpatients and staff.
As part of this work, the Office will set out criteria against which nationalclinical audits will be assessed. It will endorse national clinical audits thatconform to the criteria and may provide support to enable existing audits notmeeting these criteria to do so.
Professional education and training
Ongoing continuing professional development and training should underpinthe NSF Delivery Strategy. This will take a variety of forms to suit the trainingneeds identified. Currently opportunities exist to undertake courses indiabetes management for continuing professional development that is at theheart of continuous quality improvement.(See Education and Training –Annex 5.)
Regular and ongoing training of healthcare professionals involved indiabetes care – particularly those in primary care, where most people’sdiabetes is managed should include: -
• Risk factors for diabetes:- the potential for preventing diabetesthrough the modification of risk factors and interventions that areeffective in managing weight, treating blood pressure andcholesterol and encouraging physical activity.
• Knowledge of screening issues:- identifying those at high riskof diabetes and knowledge of signs and symptoms of diabetes.
• Diagnosis and examination:- including the identification of thecomplications of diabetes.
• Clinical management:- including the management of diabetesand its complications associated conditions and cardiovascular riskfactors.
21
• The provision of education and support for people withdiabetes (to include their family and carers):- including theability to impart the necessary knowledge, motivation, andbehaviour change and self-care skills. These skills will enable peoplewith diabetes to take responsibility for their own healthcare, andequip them with an understanding of the emotional and socialproblems likely to be faced by people with diabetes.
• Management of diabetes emergencies:- awareness of thelocal services available and what to do in the event of anemergency.
• Record keeping:- i.e. the maintenance of adequate diabetesrecords, a diabetes register, a call/recall system via patient lists andthe use of hand held records.
• Cultural awareness training and management ofvulnerable groups:- this is particularly relevant given the highprevalence of diabetes in certain minority ethnic communities inWales and the particular challenges in delivering diabetes servicesto these groups.
Sufficient time and funding should be allocated by LHBs and Trusts to enableall relevant professionals to undertake training, including validated andaccredited courses. Regular updating is also important to ensure that staffare aware of improvements and changes in diabetes management,treatment regimes, and techniques. This may include study days organisedby in-house training facilitators, clinicians, specialist nurses or by the localNHS or education provider, single profession study days/courses toenhance development within the profession, Practice and PersonalDevelopment Planning and non accredited courses.
There is also a role for people with diabetes in educating healthcareprofessionals about the condition, to help develop a better understanding ofthe patients’ perspective and appreciate patients’ expertise.
Education and training for professionals should include the wide range ofstaff likely to come into contact with people with diabetes, including localauthority staff such as teachers, leisure centre staff, social care staff and NHSDirect. This could be facilitated via local authority involvement in LHBs.
22
Education and support of people living with diabetes
It is also beneficial for family members or carers to be encouraged andwelcomed to attend the educational sessions, as their understanding of thecondition and support of the person with diabetes is of great importance.
The Diabetes NSF aims to empower people living with diabetes, thereforeinitial and ongoing education and information are all-important. The aim ofsuch education and information is to facilitate and support self-management,and it needs to be available at the time of diagnosis and also later on. Ad-hoc information is an important element of this, as are structured educationprogrammes. See Diabetes UK website for examples of good practice atwww.diabetes.org.uk and the Welsh Assembly Government Diabetes NSFwebsite at www.wales.gov.uk.
Support, as distinct from education, of people living with diabetes is alsoimportant. Such support could include counselling and/or psychologicalsupport, and access to self-help groups and other forms of peer support.Healthcare professionals’ training needs to include training in supportingpeople living with diabetes, communication and listening skills. Voluntaryorganisations should also be recognised for the vital role that they playacross Wales.
Patient and Public Involvement
A key requirement of ‘Improving Health in Wales’ (Chapter 3) is to ensurethat patients and the public are fully involved in the design, delivery andmonitoring of health services. The overall benefits include better outcomes ofhealth care, increased patient satisfaction, more responsive and costeffective health care services, and a general strengthening of publicconfidence in the NHS. This commitment ensures that every NHS Trust andLHG, produced for the first time, from 2002, annual action plans setting outproposals for patient involvement and patient focus. This was supported bythe Assembly through the production of ‘Signposts – A practical guide topublic and patient involvement in Wales’. The introduction of the ‘ExpertPatient’ Programme and the strengthening of the role of Community HealthCouncils (CHC) in their support of patients, now includes the provision ofpatient advocates across the 9 CHC ‘federation’ areas of Wales.
23
Expert Patient Programme – Pilot Programmes(Wales)
Expert Patient Programmes26 (EPP) also known as self managementprogrammes are about providing training and education to develop theconfidence and motivation of people to use their own skills and knowledgeto take effective control over living with a chronic illness. Two pilot projectsestablished in Gwynedd and Swansea LHBs, will provide an opportunity totest this in a rural and urban setting. The LHB structure provides a basis forclose partnership working with local health, social care, voluntaryorganisations, community groups and community health councils.
The schemes will establish local arrangements to support development of anEPP so that it is possible to focus on the needs of local people and theircommunities. The EPP pilots commenced in March 2003 and will run for 12months. It will be important to learn lessons from these schemes before anyconsideration is given to the way forward in terms of wider application.
Primary care contracts
Implementation of the Diabetes NSF in primary care is expected to takeplace in the context of the proposed new General Medical Services (GMS)contract. This is being negotiated between the NHS Confederation and theBMA General Practitioners’ Committee. The new GMS contract frameworkagreement makes clear that new work would be recognised and rewardedin a number of ways. The contract currently being negotiated envisages theprovision of essential, additional and enhanced services.
In addition, the contract provides for an optional quality and outcomesframework, which would attract additional remuneration. Within the clinicaldomain of the quality and outcomes framework sits a series of evidencebased quality indicators specific to diabetes.
All Wales Diabetic Retinopathy Screening Programme
"The aim of the All Wales Diabetes Retinopathy ScreeningProgramme, is that by 2005 a minimum of 80% of people withdiabetes to be offered screening, rising to 100% offered by theend of 2006".
24

This programme was launched in July 2002 as part of the All Wales EyeCare Initiative Programme, which includes the Low Vision Aids, and EyeHealth Examination programmes. These are important developments forWales and have direct relevance to the implementation of the Diabetes NSF.It is expected that contact details (i.e. patient lists) taken from the practicebased diabetes registers will assist with call and recall for appointments forretinal screening. People with diabetes will be offered screening with digitalcameras, for the early detection (and treatment if required) of diabeticretinopathy as part of a systematic programme that meets nationalstandards. Specific services will be developed to meet the needs of the hardto reach groups such as the housebound, and develop links with the ethnicgroups to encourage uptake.
Optometrists who are accredited within the Wales Eye Care Initiative willcontinue to provide the diabetic retinopathy co-management of the personwith diabetes and link into the DRSS – underpinning and supporting thescheme.
Clinical Governance
Quality Care and Clinical Excellence outlined our ten-year plan forimproving the quality of health services in Wales. This was followed by theclinical governance guidance contained in WHC (99) 54. Clinicalgovernance is a framework through which NHS organisations areaccountable for continuously improving the quality of their services andsafeguarding the standards of care by creating an environment in whichclinical care will flourish.
The key components of clinical governance are patient involvement, riskmanagement, clinical audit, staffing and staff management, education andtraining, clinical effectiveness, use of information and strategic capacity.Trust boards and LHBs support and monitor the development of each of theclinical governance components to continuously improve patient care.
NSFs are based on the best available evidence of clinical effectiveness, andthey set explicit standards (targets) to achieve consistency and high qualitycare for specific medical conditions.
The Diabetes NSF has clear standards, key actions and targets for achievingbest practice and improving the patient’s experience of care. Progress willbe monitored through the clinical governance framework, particularlythrough clinical audit and through patient involvement in evaluation.
25

Accountability for Delivery
Each LHB will need to establish a system of auditing the management ofpeople with diabetes. The audit must include levels of compliance with thelocally agreed patient pathways and protocols. The audit should beundertaken jointly by primary and secondary care. The LHB and Trust shouldpublish the results as a joint annual report in partnership with the LDSAG (orequivalent) and submit it to the Assembly. Progress will be monitored as partof the wider monitoring of the NHS under the SaFF. Implementation of theDiabetes NSF will be subject to review by the Commission for HealthcareAudit and Improvement (CHAI), after its establishment in 2004.
26
Chapter 4
Implementation and Action Plans
Twelve Evidence Based Standards for ImprovingServices for People Living with Diabetes in Wales
Standard 1The NHS will develop, implement and monitor strategies to reduce the riskof developing Type 2 diabetes in the population as a whole and to reducethe inequalities in the risk of developing Type 2 diabetes.
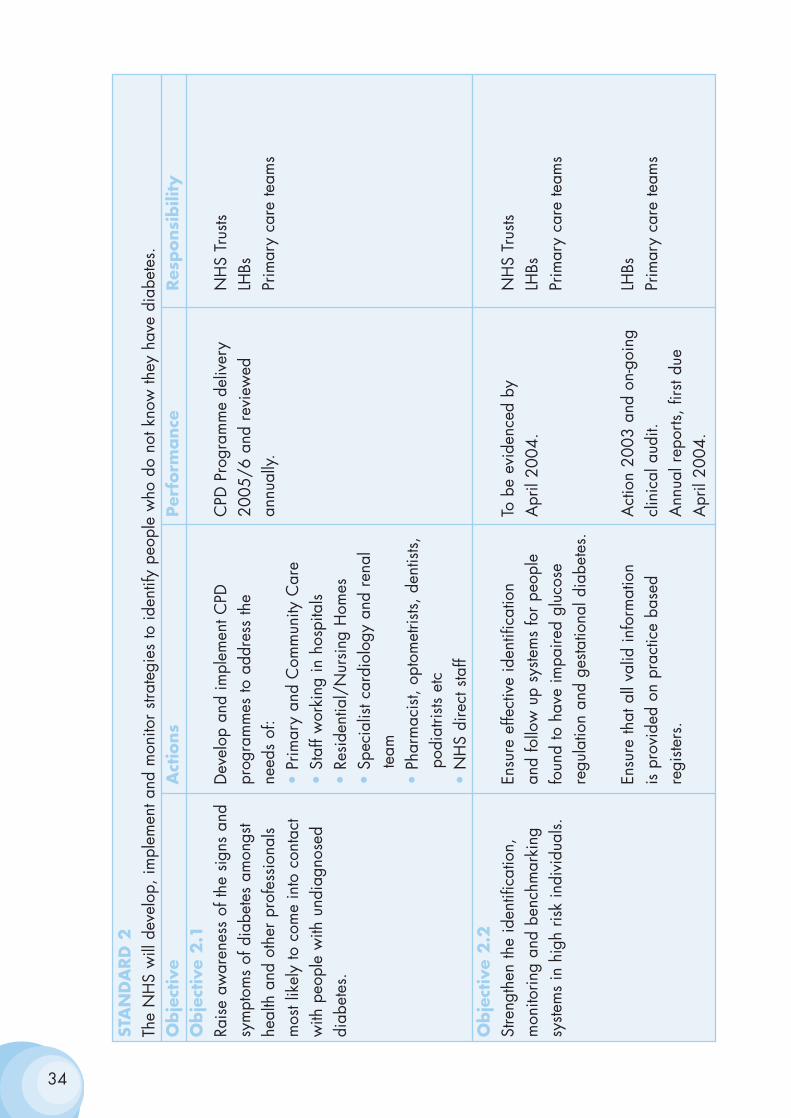
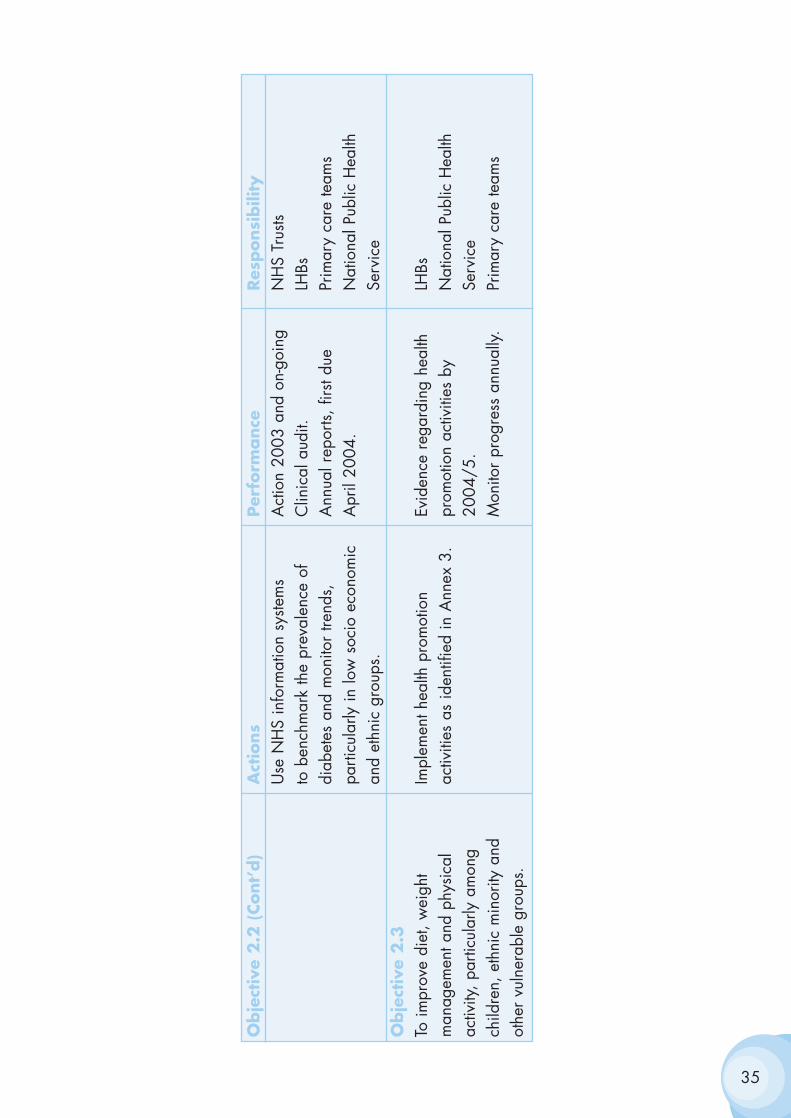
Standard 2The NHS will develop, implement and monitor strategies to identify peoplewho do not know they have diabetes.
Standard 3All children, young people and adults with diabetes will receive a service,which encourages partnership in decision-making, supports them inmanaging their diabetes and helps them to adopt and maintain a healthylifestyle. This will be reflected in an agreed and shared care plan in anappropriate format and language. Where appropriate, parents and carersshould be fully engaged in this process.
Standard 4All adults with diabetes will receive high-quality care throughout theirlifetime, including support to optimise the control of their blood glucose,blood pressure and other risk factors for developing the complications ofdiabetes.
Standard 5All children and young people with diabetes will receive consistently high-quality care and they, with their families and others involved in their day-to-day care, will be supported to optimise the control of their blood glucoseand their physical, psychological, intellectual, educational and socialdevelopment.
Standard 6All young people with diabetes will experience a smooth transition of carefrom paediatric diabetes services to adult diabetes services, whether hospital
27
or community-based, either directly or via a young people’s clinic. Thetransition will be organised in partnership with each individual and at anage appropriate to and agreed with them.
Standard 7The NHS will develop, implement and monitor agreed protocols for rapidand effective treatment of diabetic emergencies by appropriately trainedhealth care professionals. Protocols will include the management of acutecomplications and procedures to minimise the risk of recurrence.
Standard 8All children, young people and adults with diabetes admitted to hospital, forwhatever reason, will receive effective care of their diabetes. Whereverpossible, they will continue to be involved in decisions concerning themanagement of their diabetes.
Standard 9The NHS will develop, implement and monitor policies that seek to empowerand support women with pre-existing diabetes and those who developdiabetes during pregnancy to optimise the outcomes of their pregnancy.
Standard 10All young people and adults with diabetes will receive regular surveillancefor the long-term complications of diabetes.
Standard 11The NHS will develop, implement and monitor agreed protocols and systemsof care to ensure that all people who develop long-term complications ofdiabetes receive timely, appropriate and effective investigation andtreatment to reduce their risk of disability and premature death.
Standard 12All people with diabetes requiring multi-agency support will receiveintegrated health and social care.
28
Implementation of Standard 1
Standard 1
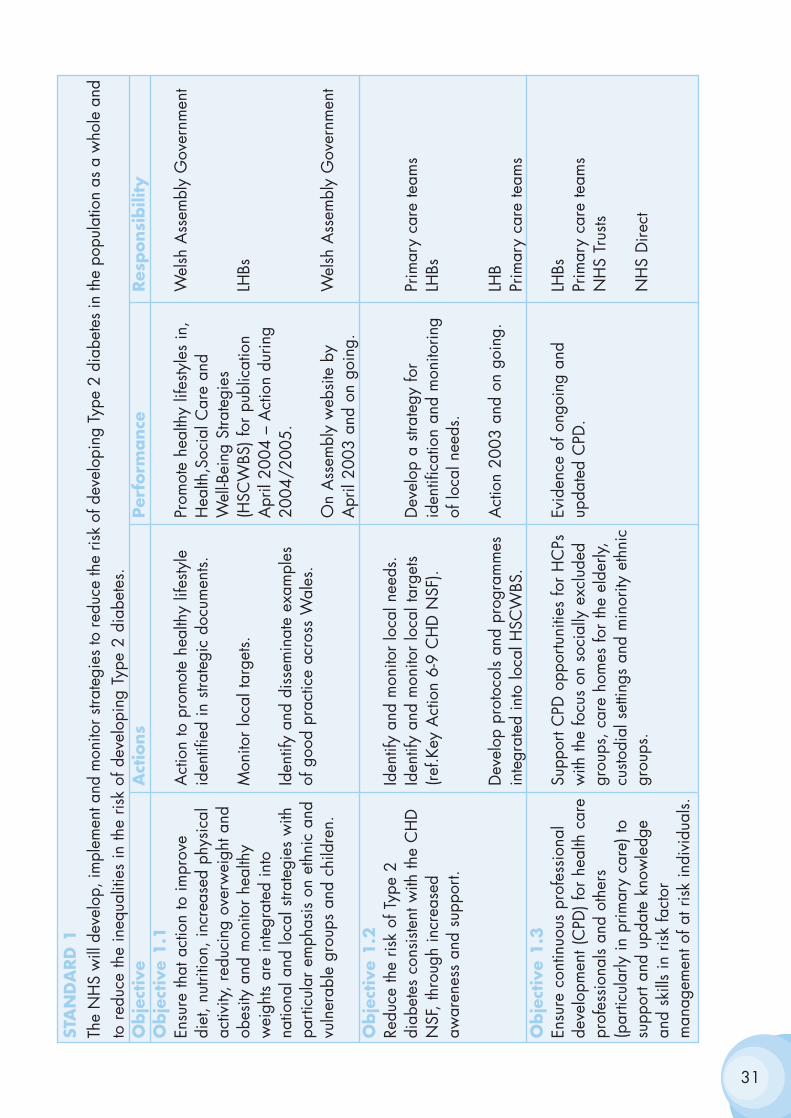
The NHS will develop, implement and monitor strategies to reduce the riskof developing Type 2 diabetes in the population as a whole and to reducethe inequalities in the risk of developing Type 2 diabetes.
AIM
To reduce the number of people who develop Type 2 diabetes.
RATIONALE
1. The number of people with Type 2 diabetes is rising, with an increasingnumber of young people being diagnosed. Some risk factors for developingdiabetes (such as family history, increasing age and ethnic origin) are non-modifiable. However, other risk factors (such as being overweight or obese,having an adverse distribution of body fat and being physically inactive) aremodifiable and need to be the focus of prevention strategies.
2. The increase in Type 2 diabetes mirrors the increase in the proportionof people, including children and young people, who are either overweightor obese. Excessive body weight reduces the body's ability to respond toinsulin and is therefore a risk factor for Type 2 diabetes. Approximately onein five adults is now obese (defined as a body mass index >30 kg/m2) andtwo in five are overweight (defined as a body mass index 25-30 kg/m2).The body's distribution of fat is also important. Excess fat stored around thewaist, referred to as central obesity, is also a risk factor for diabetes,whatever the body mass index.
3. Regular physical activity lowers the risk of developing Type 2 diabetesby increasing insulin sensitivity. This reduction in risk of diabetes isindependent of body weight. Physical activity rates are low across the entireadult population - around six in ten men and seven in ten women are notsufficiently physically active. Rates of inactivity are higher among olderpeople and in some minority ethnic communities.
29

4. Multi-agency action is required to reduce the numbers of people whoare physically inactive, overweight and obese, by promoting a balanceddiet and physical activity across the population. In order to have the greatestimpact action must start in childhood. These interventions will also contributeto a reduction in the number of people who develop coronary heart disease(CHD). Both Type 2 diabetes and CHD are more common in people of SouthAsian, African and African-Caribbean descent, and initiatives must includeelements developed with, and appropriate for, these communities.
5. Action is also needed to help those who are already overweight orobese to lose weight, and people who are physically inactive to increasetheir levels of physical activity. There is clear evidence that individuals whohave impaired glucose tolerance can reduce their risk of developing Type 2 diabetes if they are helped to eat a balanced diet, lose weight andincrease their physical activity levels.
30
31
STA
ND
ARD
1Th
e N
HS
will
dev
elop
, im
plem
ent a
nd m
onito
r stra
tegi
es to
redu
ce th
e ris
k of
dev
elop
ing
Type
2 d
iabe
tes
in th
e po
pula
tion
as a
who
le a
ndto
red
uce
the
ineq
ualit
ies
in th
e ris
k of
dev
elop
ing
Type
2 d
iabe
tes.
Obje
ctiv
e A
ctio
ns
Per
form
ance
Res
ponsi
bili
tyO
bje
ctiv
e 1.1
Ensu
re th
at a
ctio
n to
impr
ove
Act
ion
to p
rom
ote
heal
thy
lifes
tyle
Pr
omot
e he
alth
y lif
esty
les
in,
Wel
sh A
ssem
bly
Gov
ernm
ent
diet
, nut
ritio
n, in
crea
sed
phys
ical
id
entif
ied
in s
trate
gic
docu
men
ts.
Hea
lth,S
ocia
l Car
e an
d ac
tivity
, red
ucin
g ov
erw
eigh
t and
W
ell-B
eing
Stra
tegi
es
obes
ity a
nd m
onito
r he
alth
y M
onito
r lo
cal t
arge
ts.(H
SCW
BS) f
or p
ublic
atio
n LH
Bsw
eigh
ts ar
e in
tegr
ated
into
A
pril
2004
– A
ctio
n du
ring
natio
nal a
nd lo
cal s
trate
gies
with
Id
entif
y an
d di
ssem
inat
e ex
ampl
es
2004
/200
5.pa
rticu
lar
emph
asis
on
ethn
ic a
nd
of g
ood
prac
tice
acro
ss W
ales
.vu
lner
able
gro
ups
and
child
ren.
On
Ass
embl
y w
ebsi
te b
y W
elsh
Ass
embl
y G
over
nmen
tA
pril
2003
and
on
goin
g.O
bje
ctiv
e 1.2
Redu
ce th
e ris
k of
Typ
e 2
Iden
tify
and
mon
itor
loca
l nee
ds.
diab
etes
con
siste
nt w
ith th
e C
HD
Id
entif
y an
d m
onito
r lo
cal t
arge
ts D
evel
op a
stra
tegy
for
Prim
ary
care
team
sN
SF, t
hrou
gh in
crea
sed
(ref.K
ey A
ctio
n 6-
9 C
HD
NSF
).id
entif
icat
ion
and
mon
itorin
g LH
Bsaw
aren
ess
and
supp
ort.
of lo
cal n
eeds
.
Dev
elop
pro
toco
ls an
d pr
ogra
mm
es
Act
ion
2003
and
on
goin
g.LH
Bin
tegr
ated
into
loca
l HSC
WBS
.Pr
imar
y ca
re te
ams
Obje
ctiv
e 1.3
Ensu
re c
ontin
uous
pro
fess
iona
l Su
ppor
t CPD
opp
ortu
nitie
s fo
r H
CPs
Ev
iden
ce o
f ong
oing
and
LH
Bsde
velo
pmen
t (C
PD) f
or h
ealth
car
e w
ith th
e fo
cus
on s
ocia
lly e
xclu
ded
upda
ted
CPD
.Pr
imar
y ca
re te
ams
prof
essi
onal
s an
d ot
hers
grou
ps, c
are
hom
es fo
r th
e el
derly
, N
HS
Trus
ts (p
artic
ular
ly in
prim
ary
care
) to
custo
dial
set
tings
and
min
ority
eth
nic
supp
ort a
nd u
pdat
e kn
owle
dge
grou
ps.
NH
S D
irect
and
skill
s in
ris
k fa
ctor
m
anag
emen
t of a
t ris
k in
divi
dual
s.
The Implementation of standard 2
Standard 2
The NHS will develop, implement and monitor strategies to identify peoplewho do not know they have diabetes.
AIM
To ensure that people with diabetes are identified as early as possible.
RATIONALE
1. Many people are unaware that they have diabetes, either because theyhave no symptoms, or because they ascribe symptoms such as tiredness andlethargy, to stresses and strains of everyday life. Health care professionalsmay also misinterpret the symptoms of diabetes when people first describetheir symptoms to them.
2. The rapid onset of Type 1 diabetes means that only a small proportionof people remain undiagnosed for any length of time. Children and youngpeople with Type 1 diabetes can become ill very quickly and some developsuch high blood glucose levels before they are diagnosed that they presentwith diabetic ketoacidosis (DKA). The earlier diagnosis of Type 1 diabetescould prevent some of the deaths resulting from DKA. Type 2 diabetes maybe present for many years before diagnosis and nearly half of thoseidentified as having Type 2 diabetes already have complications such asdiabetic retinopathy, diabetic neuropathy or cardiovascular disease.
3. Raising awareness of the symptoms and signs of diabetes among thepublic, particularly among sub-groups of the population at risk of developingdiabetes, and among health professionals, can help to ensure that peoplewith symptoms and/or signs of diabetes are identified as early as possible.
4. Some individuals are known to be at increased risk of developing Type2 diabetes, including people who have been found previously to haveimpaired glucose regulation (impaired glucose tolerance and/or impairedfasting glycaemia) and women who have a history of gestational diabetes.For these people, follow up and regular testing can lead to the earlierdiagnosis of diabetes in those who go on to develop the condition. Adviceand support to reduce their risk of developing diabetes, and information to
32
help them recognise the symptoms and signs of diabetes should complementthis.
5. People who have multiple risk factors for diabetes – such as familyhistory, ethnic background, obesity, increasing age – also need advice andsupport to reduce their risk of developing diabetes and information about thesymptoms and signs of diabetes. In addition, opportunistic screening (testingfor diabetes when people are in contact with health services for anotherreason) will identify some people who do not know that they have thecondition.
33
34
STA
ND
ARD
2Th
e N
HS
will
dev
elop
, im
plem
ent a
nd m
onito
r str
ateg
ies
to id
entif
y pe
ople
who
do
not k
now
they
hav
e di
abet
es.
Obje
ctiv
eA
ctio
ns
Per
form
ance
Res
ponsi
bili
tyO
bje
ctiv
e 2.1
Rais
e aw
aren
ess
of th
e si
gns
and
Dev
elop
and
impl
emen
t CPD
C
PD P
rogr
amm
e de
liver
y N
HS
Trus
tssy
mpt
oms
of d
iabe
tes
amon
gst
prog
ram
mes
to a
ddre
ss th
e 20
05/6
and
rev
iew
ed
LHBs
heal
th a
nd o
ther
pro
fess
iona
ls ne
eds
of:
annu
ally.
Prim
ary
care
team
sm
ost l
ikel
y to
com
e in
to c
onta
ct
•Pr
imar
y an
d C
omm
unity
Car
ew
ith p
eopl
e w
ith u
ndia
gnos
ed
•St
aff w
orki
ng in
hos
pita
lsdi
abet
es.
•Re
side
ntia
l/N
ursi
ng H
omes
•Sp
ecia
list c
ardi
olog
y an
d re
nal
team
•Ph
arm
acis
t, op
tom
etris
ts, d
entis
ts,
podi
atris
ts et
c•
NH
S di
rect
sta
ff O
bje
ctiv
e 2.2
Stre
ngth
en th
e id
entif
icat
ion,
En
sure
effe
ctiv
e id
entif
icat
ion
To b
e ev
iden
ced
by
NH
S Tr
usts
mon
itorin
g an
d be
nchm
arki
ng
and
follo
w u
p sy
stem
s fo
r pe
ople
A
pril
2004
.LH
Bssy
stem
s in
hig
h ris
k in
divi
dual
s.fo
und
to h
ave
impa
ired
gluc
ose
Prim
ary
care
team
sre
gula
tion
and
gesta
tiona
l dia
bete
s.
Ensu
re th
at a
ll va
lid in
form
atio
n A
ctio
n 20
03 a
nd o
n-go
ing
LHBs
is p
rovi
ded
on p
ract
ice
base
d cl
inic
al a
udit.
Pr
imar
y ca
re te
ams
regi
sters
.A
nnua
l rep
orts,
firs
t due
A
pril
2004
.
35
Obje
ctiv
e 2.2
(Cont’
d)
Act
ions
Per
form
ance
Res
ponsi
bili
tyU
se N
HS
info
rmat
ion
syste
ms
Act
ion
2003
and
on-
goin
gN
HS
Trus
tsto
ben
chm
ark
the
prev
alen
ce o
f C
linic
al a
udit.
LHBs
diab
etes
and
mon
itor
trend
s,
Ann
ual r
epor
ts, fi
rst d
ue
Prim
ary
care
team
spa
rticu
larly
in lo
w s
ocio
eco
nom
ic
Apr
il 20
04.
Nat
iona
l Pub
lic H
ealth
an
d et
hnic
gro
ups.
Serv
ice
Obje
ctiv
e 2.3
To im
prov
e di
et, w
eigh
t Im
plem
ent h
ealth
pro
mot
ion
Evid
ence
reg
ardi
ng h
ealth
LH
Bsm
anag
emen
t and
phy
sica
l ac
tiviti
es a
s id
entif
ied
in A
nnex
3.
prom
otio
n ac
tiviti
es b
y N
atio
nal P
ublic
Hea
lth
activ
ity, p
artic
ular
ly a
mon
g 20
04/5
.Se
rvic
ech
ildre
n, e
thni
c m
inor
ity a
nd
Mon
itor
prog
ress
ann
ually
.Pr
imar
y ca
re te
ams
othe
r vu
lner
able
gro
ups.
Implementation of Standard 3
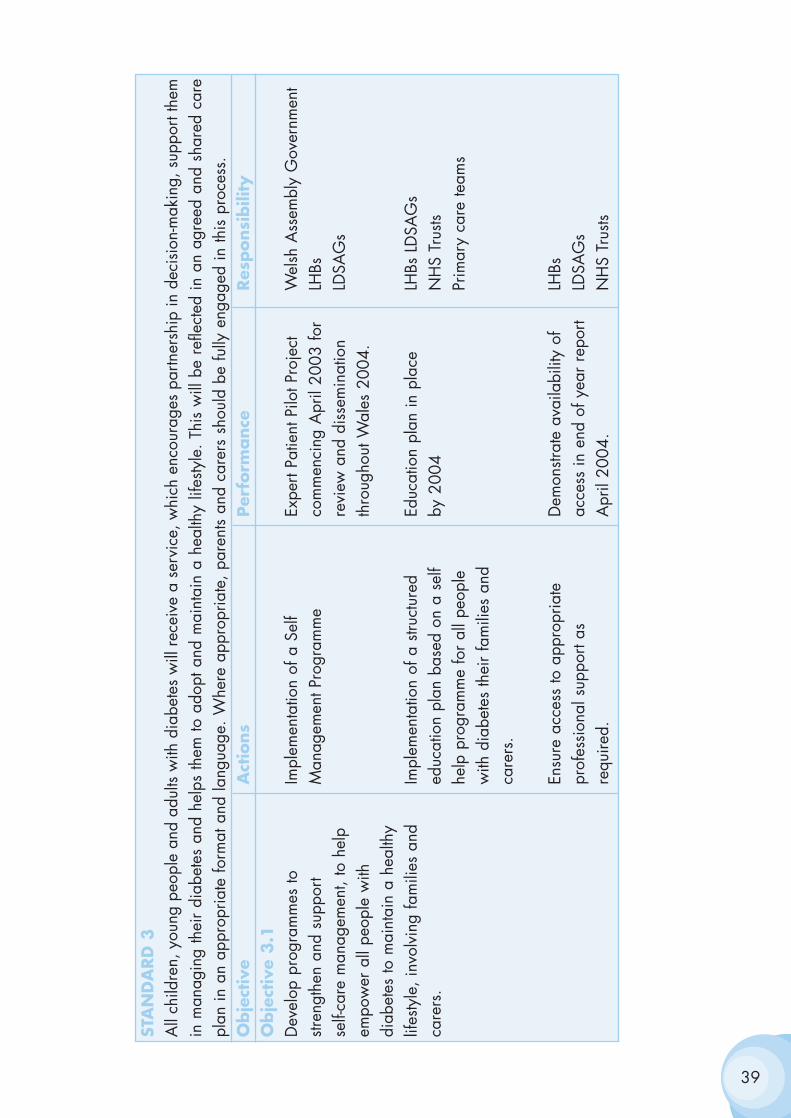
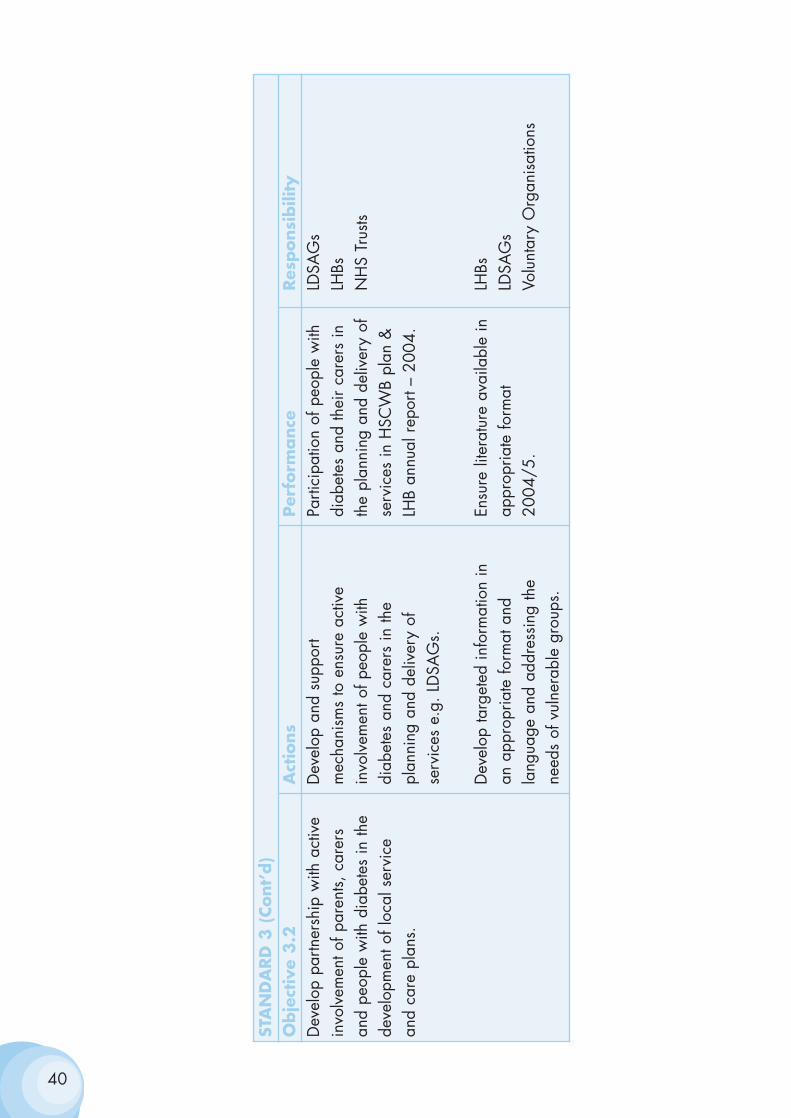
Standard 3
All children, young people and adults with diabetes will receive a servicethat encourages partnership in decision-making, supports them in managingtheir diabetes and helps them to adopt and maintain a healthy lifestyle. Thiswill be reflected in an agreed and shared care plan in an appropriate formatand language. Where appropriate, parents and carers should be fullyengaged in this process.
AIM
To ensure that people with diabetes are empowered to enhance theirpersonal control over the day-to-day management of their diabetes in a waythat enables them to experience the best possible quality of life.
RATIONALE
1. Users of the NHS should have choice, voice and control over whathappens to them at each step of their care. Empowering people with long-term conditions in their relationships with health and other professionalsenables them to assert control over their lives, build confidence and be activepartners in their care.
2. The Expert Patient Taskforce noted that, although people have needsspecific to their individual disease, they also have a core of commonrequirements, for example:
• knowing how to recognise and act upon symptoms
• dealing with acute attacks or exacerbation’s of the disease
• making the most effective use of medicines and treatment
• understanding the implications of medical advice
• establishing a stable pattern of sleep and rest and dealing withfatigue
• accessing social and other services
36
• managing work and the resources of employment services
• accessing chosen leisure activities
• developing strategies to deal with the psychological consequencesof illness
• learning to cope with other people’s response to their chronic illness.
3. Diabetes is a chronic life-long condition that impacts upon almost everyaspect of life. Living with diabetes is not easy. Medication is usually self-administered, whilst lifestyle changes involving diet and physical activityrequire commitment and active involvement. Those with Type 1 diabeteshave to balance the risks of hypoglycaemia against the longer-term risks ofhyperglycaemia. Those with Type 2 diabetes usually need to make changesin their lifestyle, but this can be difficult to do if the individual does not feelill or the impact of not doing so does not have immediate repercussions.
4. People who take on greater responsibility for the management of theirdiabetes have been shown to have reduced blood glucose levels, with noincrease in severe hypoglycaemic attacks, a marked improvement in qualityof life and a significant increase in satisfaction with treatment. However, fora range of reasons, a significant proportion of people with diabetes do notunderstand key elements of their diabetes care.
5. Additionally, a diagnosis of diabetes can lead to poor psychologicaladjustment, including self-blame and denial, which can create barriers toeffective self-management. The diagnosis can also create or reinforce asense of low self-esteem and induce resistance and depression. While thehealth benefits of self-management and care are clear, a commitment to theperson with diabetes having choice, voice and control over what happensto them means that this must be balanced with their autonomy in choosinghow they live their lives with diabetes. The health professional’s role is toensure that people can develop an understanding of and receive informationabout, the risks and consequences of the choice being made.
6. The provision of information, education and psychological support thatfacilitates self-management is therefore the cornerstone of diabetes care.People with diabetes need the knowledge, skills and motivation to assesstheir risks, to understand what they will gain from changing their behaviouror lifestyle and to act on that understanding by engaging in appropriatebehaviours. Other beneficial factors include:
37
• A family and social environment that supports change: families andcommunities provide both the practical support and a framework forthe individual’s beliefs.
• The tools to support behaviour, for example, affordable healthierfood options both at home and in the workplace.
• Active involvement in negotiating, agreeing and owning goals.
• Knowledge to understand the consequences of different choices andto enable action.
38
39
STA
ND
ARD
3A
ll ch
ildre
n, y
oung
peo
ple
and
adul
ts w
ith d
iabe
tes
will
rece
ive
a se
rvic
e, w
hich
enc
oura
ges
partn
ersh
ip in
dec
isio
n-m
akin
g, s
uppo
rt th
emin
man
agin
g th
eir
diab
etes
and
hel
ps th
em to
ado
pt a
nd m
aint
ain
a he
alth
y lif
esty
le.
This
will
be
refle
cted
in a
n ag
reed
and
sha
red
care
plan
in a
n ap
prop
riate
form
at a
nd la
ngua
ge. W
here
app
ropr
iate
, par
ents
and
care
rs s
houl
d be
fully
eng
aged
in th
is p
roce
ss.
Obje
ctiv
eA
ctio
ns
Per
form
ance
Res
ponsi
bili
tyO
bje
ctiv
e 3.1
Dev
elop
pro
gram
mes
to
Impl
emen
tatio
n of
a S
elf
Expe
rt Pa
tient
Pilo
t Pro
ject
W
elsh
Ass
embl
y G
over
nmen
t str
engt
hen
and
supp
ort
Man
agem
ent P
rogr
amm
eco
mm
enci
ng A
pril
2003
for
LHBs
self-
care
man
agem
ent,
to h
elp
revi
ew a
nd d
isse
min
atio
n LD
SAG
sem
pow
er a
ll pe
ople
with
th
roug
hout
Wal
es 2
004.
diab
etes
to m
aint
ain
a he
alth
y lif
esty
le, i
nvol
ving
fam
ilies
and
Im
plem
enta
tion
of a
stru
ctur
ed
Educ
atio
n pl
an in
pla
ce
LHBs
LD
SAG
sca
rers
.ed
ucat
ion
plan
bas
ed o
n a
self
by 2
004
NH
S Tr
usts
help
pro
gram
me
for
all p
eopl
e Pr
imar
y ca
re te
ams
with
dia
bete
s th
eir
fam
ilies
and
ca
rers
.
Ensu
re a
cces
s to
app
ropr
iate
D
emon
strat
e av
aila
bilit
y of
LH
Bspr
ofes
sion
al s
uppo
rt as
ac
cess
in e
nd o
f yea
r re
port
LDSA
Gs
requ
ired.
Apr
il 20
04.
NH
S Tr
usts
40
STA
ND
ARD
3 (
Cont’
d)
Obje
ctiv
e 3.2
Act
ions
Per
form
ance
Res
ponsi
bili
tyD
evel
op p
artn
ersh
ip w
ith a
ctiv
e D
evel
op a
nd s
uppo
rt Pa
rtici
patio
n of
peo
ple
with
LD
SAG
sin
volv
emen
t of p
aren
ts, c
arer
s m
echa
nism
s to
ens
ure
activ
e di
abet
es a
nd th
eir
care
rs in
LH
Bsan
d pe
ople
with
dia
bete
s in
the
invo
lvem
ent o
f peo
ple
with
th
e pl
anni
ng a
nd d
eliv
ery
of
NH
S Tr
usts
deve
lopm
ent o
f loc
al s
ervi
ce
diab
etes
and
car
ers
in th
e se
rvic
es in
HSC
WB
plan
&
and
care
pla
ns.
plan
ning
and
del
iver
y of
LH
B an
nual
rep
ort –
200
4.se
rvic
es e
.g. L
DSA
Gs.
Dev
elop
targ
eted
info
rmat
ion
in
Ensu
re li
tera
ture
ava
ilabl
e in
LH
Bsan
app
ropr
iate
form
at a
nd
appr
opria
te fo
rmat
LDSA
Gs
lang
uage
and
add
ress
ing
the
2004
/5.
Volu
ntar
y O
rgan
isat
ions
need
s of
vul
nera
ble
grou
ps.
The Implementation of Standard 4
Standard 4
All adults with diabetes will receive high-quality care throughout theirlifetime, including support to optimise the control of their blood glucose,blood pressure and other risk factors for developing the complications ofdiabetes.
AIM
To maximise the quality of life of all people with diabetes and to reduce theirrisk of developing the long-term complications of diabetes.
RATIONALE
1. For most people with diabetes, coming to terms with their lifelongcondition will be challenging. They may grieve for the loss of earlieridentities as a ‘healthy person’ and will need to adjust to the fact that theyhave a long-term condition, the treatment of which may involve fundamentalchanges in their lifestyle if they are to reduce their risk of developing long-term complications. Key to this will be their ability to control their bloodglucose, and where necessary, to reduce their blood pressure. The treatmentand care required will vary as people’s length of time living with diabetesincreases and as they negotiate major life events.
2. There is robust evidence that meticulous blood glucose control canprevent or delay the onset of microvascular complications. It may alsoreduce the risk of developing cardiovascular disease. However, this requireseffort and dedication on the part of the person with diabetes and the healthprofessionals working with them. For people with Type 1 Diabetes, insulin isthe mainstay of blood glucose management and is essential for survival. Forpeople with newly diagnosed Type 2 diabetes, the majority of whom areoverweight, weight loss and increased physical activity are the firstintervention, followed by the addition of medication, as appropriate.
3. Up to 70% of adults with Type 2 diabetes have raised blood pressureand more than 70% have raised cholesterol levels. Both increase the risk ofdeveloping cardiovascular disease as well as microvascular complications.Pre-menopausal women with diabetes do not have the same protectionagainst coronary heart disease as other pre-menopausal women. High
41

blood pressure control improves health outcomes in people with Type 2diabetes. Results for people with Type 2 diabetes who participated in trialsto assess the effectiveness of lipid-lowering therapy suggest that a reductionin cholesterol levels may also reduce their risk of cardiovascular events.Stopping smoking is one of the most effective ways of reducing the risk ofdeveloping cardiovascular disease and also reduces the risk of developingmicrovascular complications.
4. Structured diabetes care programmes, which include the provision ofregular recall and review of people with diabetes, including those inresidential/nursing care homes and custodial settings, can improve thequality of diabetes care and result in better glycaemic control and quality oflife, reductions in cardiovascular risk factors, lower rates of long-termcomplications and lower mortality rates. This is particularly so whencombined with interventions targeted at the health professionals providingdiabetes care, such as reminders to undertake annual reviews, the provisionof guidelines and the opportunity to participate in continuing education.
42
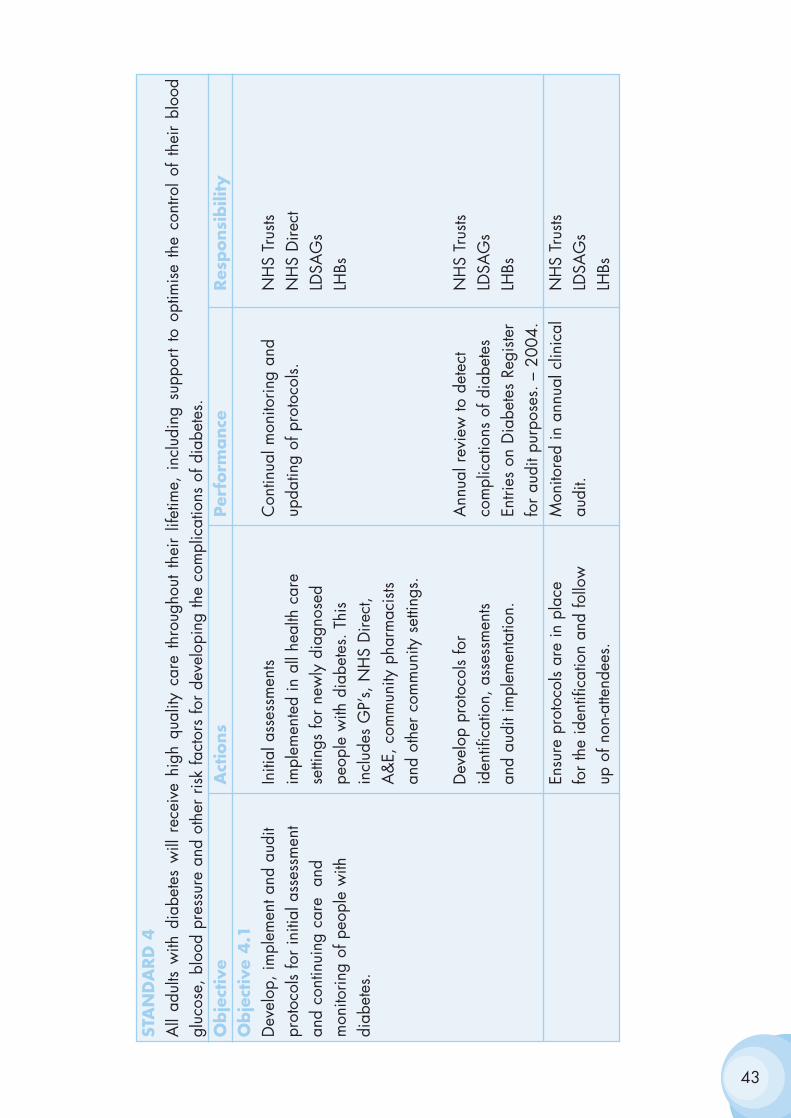
43
STA
ND
ARD
4A
ll ad
ults
with
dia
bete
s w
ill r
ecei
ve h
igh
qual
ity c
are
thro
ugho
ut t
heir
lifet
ime,
inc
ludi
ng s
uppo
rt to
opt
imis
e th
e co
ntro
l of
the
ir bl
ood
gluc
ose,
blo
od p
ress
ure
and
othe
r ris
k fa
ctor
s fo
r de
velo
ping
the
com
plic
atio
ns o
f dia
bete
s.O
bje
ctiv
eA
ctio
ns
Per
form
ance
Res
ponsi
bili
tyO
bje
ctiv
e 4.1
Dev
elop
, im
plem
ent a
nd a
udit
Initi
al a
sses
smen
ts C
ontin
ual m
onito
ring
and
NH
S Tr
usts
prot
ocol
s fo
r in
itial
ass
essm
ent
impl
emen
ted
in a
ll he
alth
car
eup
datin
g of
pro
toco
ls.N
HS
Dire
ctan
d co
ntin
uing
car
e a
nd
setti
ngs
for
new
ly d
iagn
osed
LD
SAG
sm
onito
ring
of p
eopl
e w
ith
peop
le w
ith d
iabe
tes.
Thi
s LH
Bsdi
abet
es.
incl
udes
GP’
s, N
HS
Dire
ct,
A&
E, c
omm
unity
pha
rmac
ists
and
othe
r co
mm
unity
set
tings
.
Dev
elop
pro
toco
ls fo
r A
nnua
l rev
iew
to d
etec
t N
HS
Trus
ts id
entif
icat
ion,
ass
essm
ents
com
plic
atio
ns o
f dia
bete
s LD
SAG
san
d au
dit i
mpl
emen
tatio
n.En
tries
on
Dia
bete
s Re
giste
r LH
Bsfo
r au
dit p
urpo
ses.
– 2
004.
Ensu
re p
roto
cols
are
in p
lace
M
onito
red
in a
nnua
l clin
ical
N
HS
Trus
tsfo
r th
e id
entif
icat
ion
and
follo
w
audi
t. LD
SAG
s up
of n
on-a
ttend
ees.
LHBs
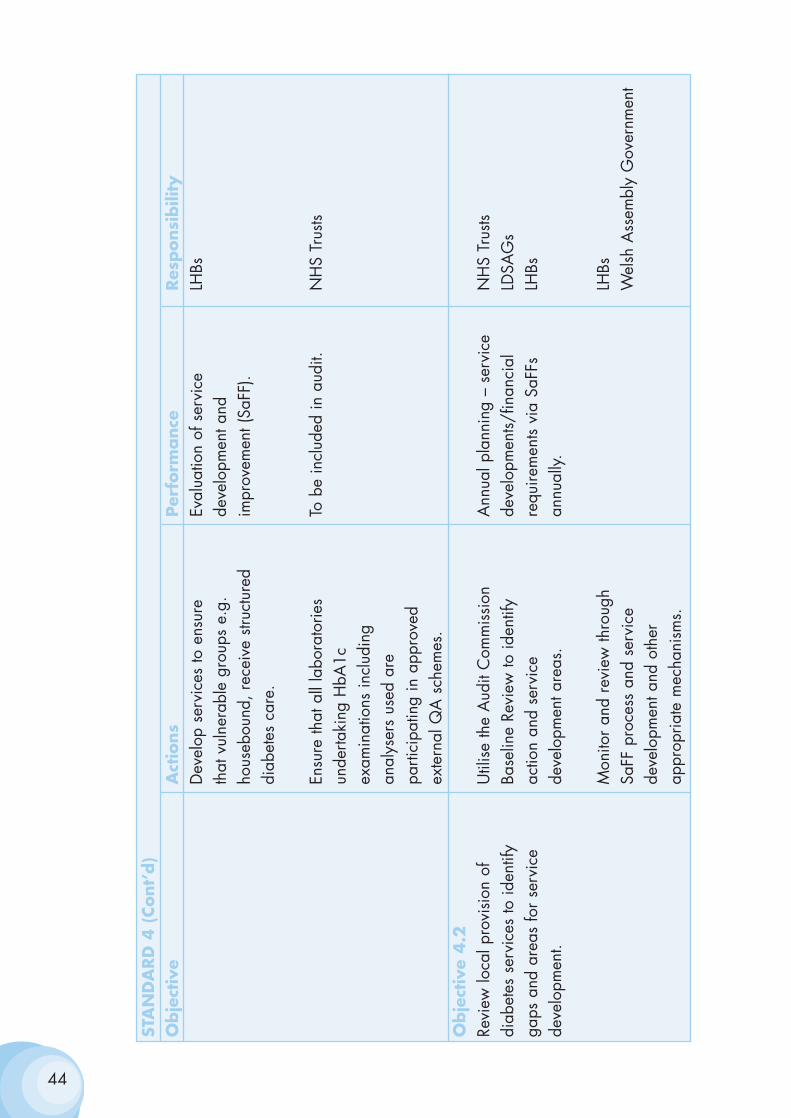
44
STA
ND
ARD
4 (
Cont’
d)
Obje
ctiv
e A
ctio
ns
Per
form
ance
Res
ponsi
bili
tyD
evel
op s
ervi
ces
to e
nsur
e Ev
alua
tion
of s
ervi
ce
LHBs
that
vul
nera
ble
grou
ps e
.g.
deve
lopm
ent a
nd
hous
ebou
nd, r
ecei
ve s
truct
ured
im
prov
emen
t (Sa
FF).
diab
etes
car
e.
Ensu
re th
at a
ll la
bora
torie
s To
be
incl
uded
in a
udit.
NH
S Tr
usts
unde
rtaki
ng H
bA1c
ex
amin
atio
ns in
clud
ing
anal
yser
s us
ed a
re
parti
cipa
ting
in a
ppro
ved
exte
rnal
QA
sch
emes
.O
bje
ctiv
e 4.2
Revi
ew lo
cal p
rovi
sion
of
Util
ise
the
Aud
it C
omm
issi
on
Ann
ual p
lann
ing
– se
rvic
e N
HS
Trus
tsdi
abet
es s
ervi
ces
to id
entif
y Ba
selin
e Re
view
to id
entif
y de
velo
pmen
ts/fin
anci
al
LDSA
Gs
gaps
and
are
as fo
r se
rvic
e ac
tion
and
serv
ice
requ
irem
ents
via
SaFF
s LH
Bsde
velo
pmen
t.de
velo
pmen
t are
as.
annu
ally.
Mon
itor
and
revi
ew th
roug
h LH
BsSa
FF p
roce
ss a
nd s
ervi
ce
Wel
sh A
ssem
bly
Gov
ernm
ent
deve
lopm
ent a
nd o
ther
ap
prop
riate
mec
hani
sms.
Implementing standards 5 & 6
Standard 5
All children and young people with diabetes will receive consistently highquality care and they, with their families and others involved in their day-to-day care, will be supported to optimise the control of their blood glucoseand their physical, psychological, intellectual, educational and socialdevelopment.
Standard 6
All young people with diabetes will experience a smooth transition of carefrom paediatric diabetes services to adult diabetes services, whether hospitalor community-based, either directly or via a young people's clinic. Thetransition will be organised in partnership with each individual and at anage appropriate to and agreed with them.
AIM
To ensure that the special needs of children and young people with diabetesare recognised and met, thereby ensuring that, when they enter adulthood,they are in the best of health and able to manage their own day-to-daydiabetes care effectively.
RATIONALE
1. Children and young people with diabetes are subject to all the normalpressures and pleasures of physical, emotional and social development.Their needs as an individual within a family or family system, and the roleof their parent or carer and siblings in sustaining them from initial diagnosisthrough childhood to independence, are key. Those who develop Type 1diabetes require lifelong insulin replacement therapy, which will need to beregularly adjusted as they grow. Good glucose control is essential for normalgrowth and development and to avoid the acute and long-term complicationsof diabetes. The optimisation of diabetes control is also important for theirintellectual and educational attainment. While physical maturity will belargely complete by the late teens, young people continue forming theiridentities into early adulthood. During this period, they face unique pressuresto conform to social, cultural and sexual norms, which may challenge theirability to manage their diabetes.
45
2. There has been a steady rise in the incidence of diabetes in childrenand young people in recent decades. The majority of children and youngpeople with diabetes have Type 1 diabetes and the risk of developing Type1 diabetes is similar for all ethnic groups. However, Type 2 diabetes is alsoincreasingly being diagnosed in young people, particularly in those fromminority ethnic groups. Maturity onset diabetes of the young (MODY) andtheir rare genetic disorders of insulin metabolism may also be diagnosed inchildren and young people. People who develop diabetes in childhood canhave a reduced life expectancy – their lifespan may be reduced by as muchas 20 years - and many develop the long-term complications of diabetes,such as nephropathy and retinopathy, before they reach middle age.
3. Parents of young children with diabetes need to be actively involved inthe day-to-day diabetes management of their children. Others such as staffin nurseries and schools will also be involved in the day-to-day care ofchildren and young people with diabetes.
4. Children and young people with diabetes need the support of a healthservice not only expert in child health and diabetes, but also able to supportthem through the transitions from childhood through adolescence toadulthood. Diabetes is often more difficult to control during the teenageyears and in early adult life due both to hormonal changes of puberty andto the emotional roller coaster that often characterises adolescence. Youngpeople have higher rates of diabetic emergencies and death rates aresignificantly higher than in young people without diabetes. Greater effort isrequired to ensure effective diabetes control at this time than at any otherstage of life both by health professionals and by young people themselves.
5. The transfer of young people from paediatric diabetes services toservices for adults with diabetes often occurs at a sensitive time for theindividual concerned, both personally and from the point of view of theirdiabetes. Many find the culture change unacceptable and non-attendancerates at adult diabetes clinics are often higher in young people and youngadults. Care can also become disjointed and young people can feelunsupported. This may be exacerbated when young people leave home andadopt more mobile lifestyles.
6. The forthcoming Children’s National Service Framework will identifyissues relevant to the delivery of all children’s services. The Children’sNational Service Framework will complement the National ServiceFramework for Diabetes.
46
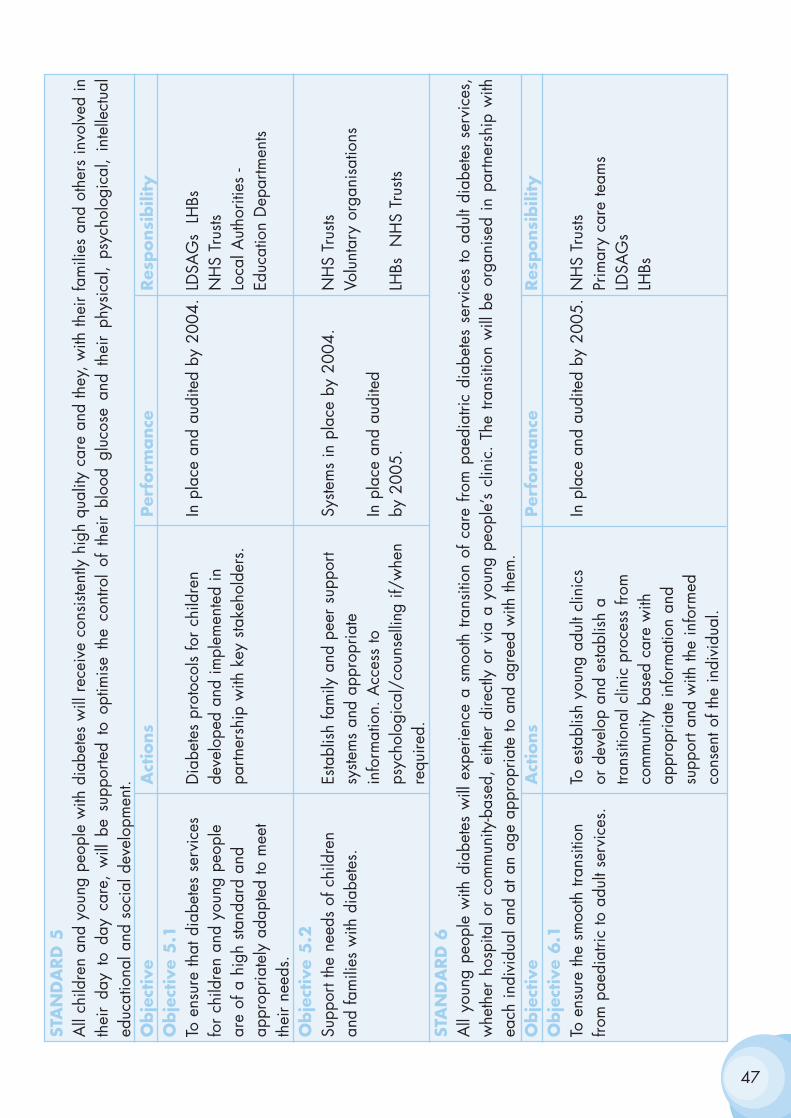
47
STA
ND
ARD
5A
ll ch
ildre
n an
d yo
ung
peop
le w
ith d
iabe
tes
will
rec
eive
con
siste
ntly
hig
h qu
ality
car
e an
d th
ey,
with
thei
r fa
mili
es a
nd o
ther
s in
volv
ed in
thei
r da
y to
day
car
e, w
ill b
e su
ppor
ted
to o
ptim
ise
the
cont
rol
of t
heir
bloo
d gl
ucos
e an
d th
eir
phys
ical
, ps
ycho
logi
cal,
inte
llect
ual
educ
atio
nal a
nd s
ocia
l dev
elop
men
t.O
bje
ctiv
eA
ctio
ns
Per
form
ance
Res
ponsi
bili
tyO
bje
ctiv
e 5
.1To
ens
ure
that
dia
bete
s se
rvic
es
Dia
bete
s pr
otoc
ols
for
child
ren
In p
lace
and
aud
ited
by 2
004.
LDSA
Gs
LH
Bsfo
r ch
ildre
n an
d yo
ung
peop
le
deve
lope
d an
d im
plem
ente
d in
N
HS
Trus
tsar
e of
a h
igh
stand
ard
and
partn
ersh
ip w
ith k
ey s
take
hold
ers.
Loca
l Aut
horit
ies
-ap
prop
riate
ly a
dapt
ed to
mee
t Ed
ucat
ion
Dep
artm
ents
thei
r ne
eds.
Obje
ctiv
e 5
.2Su
ppor
t the
nee
ds o
f chi
ldre
n Es
tabl
ish
fam
ily a
nd p
eer
supp
ort
Syste
ms
in p
lace
by
2004
.N
HS
Trus
tsan
d fa
mili
es w
ith d
iabe
tes.
syste
ms
and
appr
opria
te
Volu
ntar
y or
gani
satio
nsin
form
atio
n. A
cces
s to
In
pla
ce a
nd a
udite
d ps
ycho
logi
cal/
coun
selli
ng if
/whe
n by
200
5.LH
Bs
NH
S Tr
usts
requ
ired.
STA
ND
ARD
6A
ll yo
ung
peop
le w
ith d
iabe
tes
will
exp
erie
nce
a sm
ooth
tran
sitio
n of
car
e fro
m p
aedi
atric
dia
bete
s se
rvic
es to
adu
lt di
abet
es s
ervi
ces,
whe
ther
hos
pita
l or
com
mun
ity-b
ased
, ei
ther
dire
ctly
or
via
a yo
ung
peop
le’s
clin
ic.
The
trans
ition
will
be
orga
nise
d in
par
tner
ship
with
each
indi
vidu
al a
nd a
t an
age
appr
opria
te to
and
agr
eed
with
them
.O
bje
ctiv
eA
ctio
ns
Per
form
ance
Res
ponsi
bili
tyO
bje
ctiv
e 6.1
To e
nsur
e th
e sm
ooth
tran
sitio
n To
esta
blis
h yo
ung
adul
t clin
ics
In p
lace
and
aud
ited
by 2
005.
NH
S Tr
usts
from
pae
diat
ric to
adu
lt se
rvic
es.
or d
evel
op a
nd e
stabl
ish
a Pr
imar
y ca
re te
ams
trans
ition
al c
linic
pro
cess
from
LD
SAG
sco
mm
unity
bas
ed c
are
with
LH
Bsap
prop
riate
info
rmat
ion
and
supp
ort a
nd w
ith th
e in
form
ed
cons
ent o
f the
indi
vidu
al.
Implementing Standard 7
Standard 7
The NHS will develop, implement and monitor agreed protocols for rapidand effective treatment of diabetic emergencies by appropriately trainedhealthcare professionals.
AIM
To minimise the impact of the acute complications of diabetes on people withdiabetes.
RATIONALE
1. The acute complications of diabetes include diabetic ketoacidosis(DKA) and hyperosmolar non-ketotic syndrome (HONK), both of which arecharacterised by very high blood glucose levels resulting from a severe lackof insulin; and hypoglycaemia, when the blood glucose level falls too low.Children and young people with diabetes and their carers need to be alertto the dangers of these potentially life-threatening situations. They need toknow how these emergencies can be prevented and how to detect andrespond rapidly to the early signs of an emergency. Health professionalsalso need to know how to respond.
2. The prevalence of the acute complications of diabetes can be reducedthrough education of people with diabetes and all ‘front line’ healthprofessionals about how to avert hypoglycaemic episodes and how toprevent DKA and HONK.
3. DKA is an avoidable, potentially life-threatening complication ofdiabetes and is caused by an inadequate concentration of insulin in theblood. As a result, the cells in the body are unable to use glucose as anenergy source and have to rely on the body’s fat reserves. Blood glucoselevels rise, as do the by-products of fat metabolism (ketone bodies). The lattercauses the blood to become more acidic than usual. About a quarter ofcases of DKA occur in people with newly presenting Type 1 diabetes, inthose with previously diagnosed diabetes, insulin omission, infection andother severe acute illness, such as myocardial infarction or pnuemonia, arethe main precipitating causes.
48
4. DKA may lead to drowsiness or coma. People who develop DKArequire urgent hospital treatment. DKA continues to be a prominent cause ofdeath in people with diabetes, particularly in children and young people.And carries a high risk of neurological damage and death.
5. HONK is a life-threatening condition, which mainly occurs in olderpeople with Type 2 diabetes. In about a third of cases HONK is the firstmanifestation of Type 2 diabetes.
The blood glucose rises to a very high level but acidosis does not develop.Severe dehydration can result. Mortality from HONK is high, with reporteddeath rates as high as 58%.
6. Hypoglycaemia is a common side effect of treatment with insulin andcan also occur in people with Type 2 diabetes treated with some types oforal hypoglycaemic drugs, (e.g. long-acting sulphonylureas). Irregular ormissed meals, exercise and alcohol consumption can predispose tohypoglycaemia. The brain is dependent on a continuous supply of glucoseas its main energy source and, when blood glucose levels fall below acritical level, brain function is affected. This can lead to confusion, fits andcoma and can, on occasion, be fatal.
7. The risk of severe hypoglycaemia, defined as hypoglycaemia requiringthe help of others to reverse it, may be higher in people receiving intensiveinsulin therapy. Fear of hypoglycaemia can be a major obstacle to theachievement of the blood glucose levels required to prevent the long-termcomplications of diabetes. Repeated episodes of hypoglycaemia mayseriously impair quality of life. For example, it may restrict educational andemployment opportunities and ability to drive, as well as participation insports and social activities. Although severe hypoglycaemia does not appearto cause long-term impairment of brain function in adults, it may result inneuropsychological impairment in children particularly in younger children.All steps should therefore be taken to prevent severe recurrenthypoglycaemia in young children with diabetes, particularly those under fiveyears of age.
49
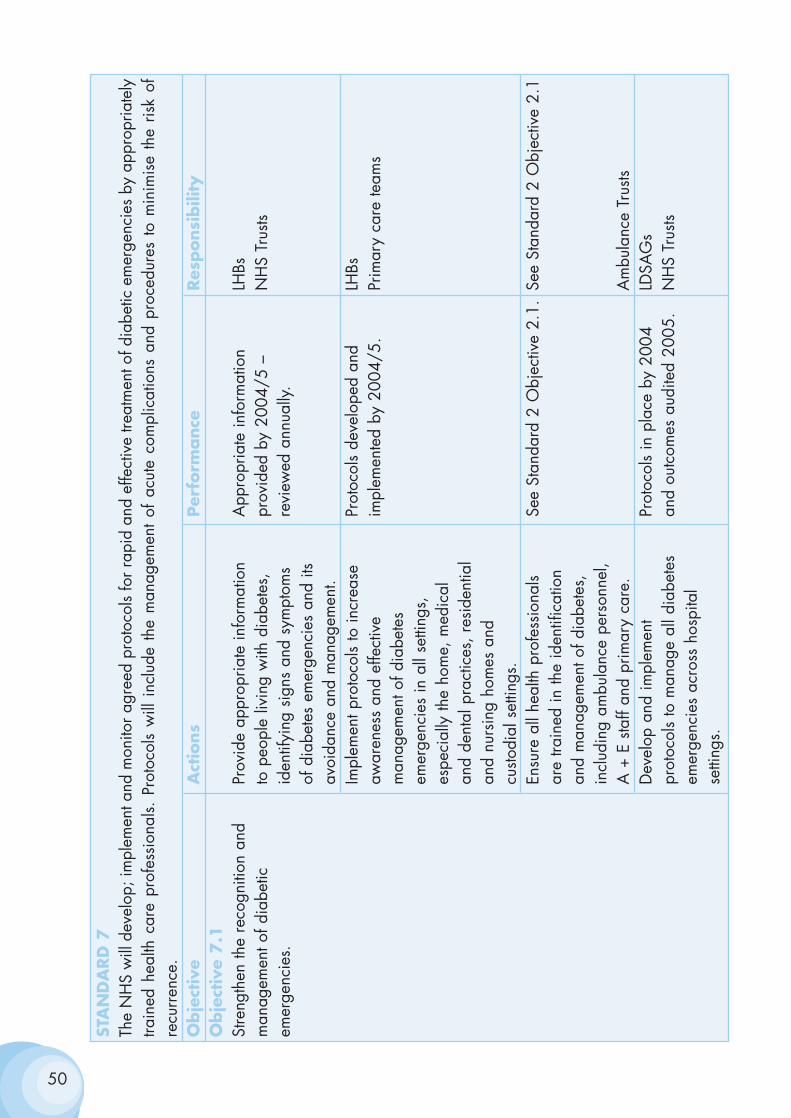
50
STA
ND
ARD
7Th
e N
HS
will
dev
elop
; im
plem
ent a
nd m
onito
r agr
eed
prot
ocol
s fo
r rap
id a
nd e
ffect
ive
treat
men
t of d
iabe
tic e
mer
genc
ies
by a
ppro
pria
tely
train
ed h
ealth
car
e pr
ofes
sion
als.
Pro
toco
ls w
ill i
nclu
de t
he m
anag
emen
t of
acu
te c
ompl
icat
ions
and
pro
cedu
res
to m
inim
ise
the
risk
ofre
curr
ence
.O
bje
ctiv
eA
ctio
ns
Per
form
ance
Res
ponsi
bili
tyO
bje
ctiv
e 7.1
Stre
ngth
en th
e re
cogn
ition
and
Pr
ovid
e ap
prop
riate
info
rmat
ion
App
ropr
iate
info
rmat
ion
LHBs
man
agem
ent o
f dia
betic
to
peo
ple
livin
g w
ith d
iabe
tes,
pr
ovid
ed b
y 20
04/5
–
NH
S Tr
usts
emer
genc
ies.
iden
tifyi
ng s
igns
and
sym
ptom
s re
view
ed a
nnua
lly.
of d
iabe
tes
emer
genc
ies
and
its
avoi
danc
e an
d m
anag
emen
t.Im
plem
ent p
roto
cols
to in
crea
se
Prot
ocol
s de
velo
ped
and
LHBs
awar
enes
s an
d ef
fect
ive
impl
emen
ted
by 2
004/
5.Pr
imar
y ca
re te
ams
m
anag
emen
t of d
iabe
tes
emer
genc
ies
in a
ll se
tting
s,
espe
cial
ly th
e ho
me,
med
ical
an
d de
ntal
pra
ctic
es, r
esid
entia
l an
d nu
rsin
g ho
mes
and
cu
stodi
al s
ettin
gs.
Ensu
re a
ll he
alth
pro
fess
iona
ls Se
e St
anda
rd 2
Obj
ectiv
e 2.
1.Se
e St
anda
rd 2
Obj
ectiv
e 2.
1ar
e tra
ined
in th
e id
entif
icat
ion
and
man
agem
ent o
f dia
bete
s,
incl
udin
g am
bula
nce
pers
onne
l, A
+ E
sta
ff an
d pr
imar
y ca
re.
Am
bula
nce
Trus
tsD
evel
op a
nd im
plem
ent
Prot
ocol
s in
pla
ce b
y 20
04
LDSA
Gs
prot
ocol
s to
man
age
all d
iabe
tes
and
outc
omes
aud
ited
2005
.N
HS
Trus
tsem
erge
ncie
s ac
ross
hos
pita
l se
tting
s.
Implementing Standard 8
Standard 8
All children, young people and adults with diabetes admitted to hospital, forwhatever reason, will receive effective care of their diabetes. Whereverpossible, they will continue to be involved in decisions concerning themanagement of their diabetes.
AIM
To ensure good quality consistent care is provided for people with diabeteswhenever they are admitted to hospital.
RATIONALE
1. People with diabetes are admitted to hospital twice as often and staytwice as long as those without diabetes. They occupy one in ten acutehospital beds.
2. They also frequently describe poor experiences of inpatient care,particularly in relation to:
• Inadequate knowledge of diabetes among hospital staff
• Inappropriate amounts and timings of food and inappropriatetimings of medication
• The lack of information provided
• Delays in discharge resulting from their diabetes, especially whendiabetes was not the original reason for their admission
• Inadequate opportunity to discuss issues with specialist nursingteam.
3. Timely liaison with the diabetes team can both prevent the need fordiabetes-related admission and, where hospital admission is unavoidable,prevent complications during admission and delayed discharge.
51
4. The employment of a specialist nurse to oversee the diabetesmanagement of people with diabetes during their admission to hospital canreduce their length of stay, arrangements then being made for specialistnurses to continue care in the community in relation to discharge planning,thereby releasing bed space. Patients are also more knowledgeable about,and satisfied with, care provided in this way.
5. Surgery in people with diabetes is associated with increased clinicalrisk. This can be reduced by adherence to locally agreed evidence-basedguidelines for the management of people with diabetes during surgicalprocedures.
52
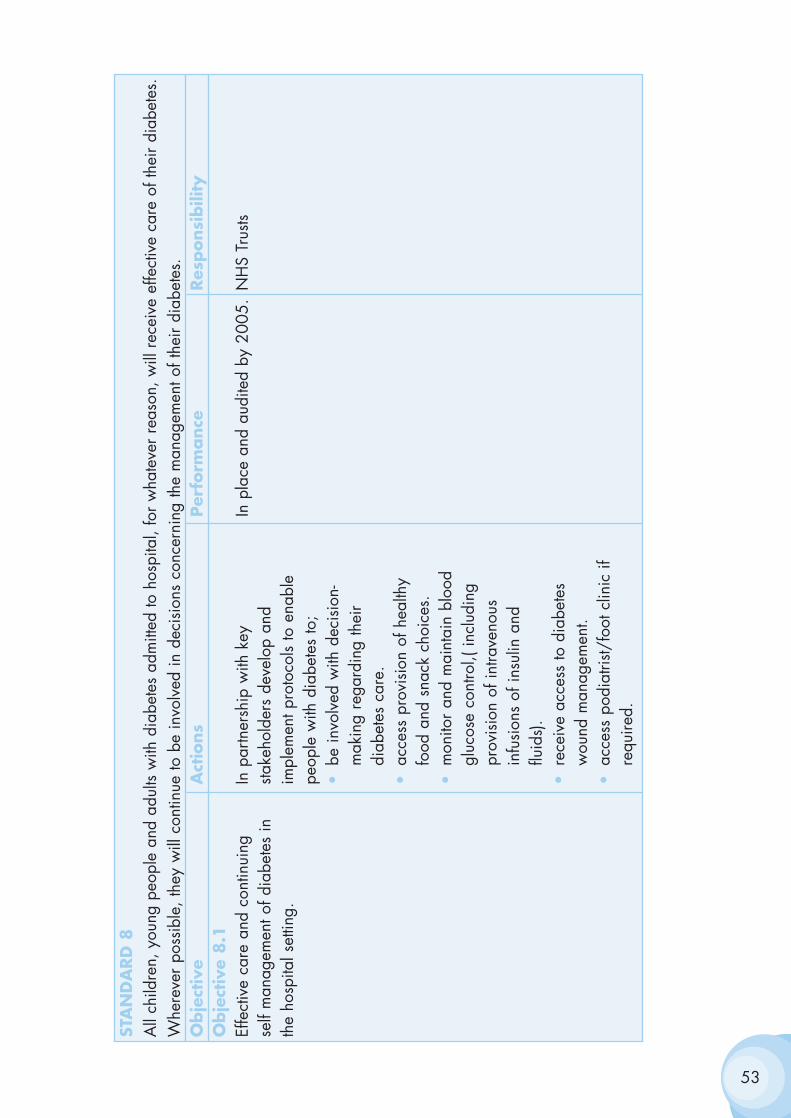
53
STA
ND
ARD
8A
ll ch
ildre
n, y
oung
peo
ple
and
adul
ts w
ith d
iabe
tes
adm
itted
to h
ospi
tal,
for
wha
teve
r re
ason
, will
rec
eive
effe
ctiv
e ca
re o
f the
ir di
abet
es.
Whe
reve
r po
ssib
le, t
hey
will
con
tinue
to b
e in
volv
ed in
dec
isio
ns c
once
rnin
g th
e m
anag
emen
t of t
heir
diab
etes
.O
bje
ctiv
eA
ctio
ns
Per
form
ance
Res
ponsi
bili
tyO
bje
ctiv
e 8.1
Effe
ctiv
e ca
re a
nd c
ontin
uing
In
par
tner
ship
with
key
In
pla
ce a
nd a
udite
d by
200
5.N
HS
Trus
tsse
lf m
anag
emen
t of d
iabe
tes
in
stake
hold
ers
deve
lop
and
the
hosp
ital s
ettin
g.im
plem
ent p
roto
cols
to e
nabl
e pe
ople
with
dia
bete
s to
;•
be in
volv
ed w
ith d
ecis
ion-
mak
ing
rega
rdin
g th
eir
diab
etes
car
e.•
acce
ss p
rovi
sion
of h
ealth
y fo
od a
nd s
nack
cho
ices
.•
mon
itor
and
mai
ntai
n bl
ood
gluc
ose
cont
rol,(
incl
udin
g pr
ovis
ion
of in
trave
nous
in
fusi
ons
of in
sulin
and
flu
ids)
.•
rece
ive
acce
ss to
dia
bete
s w
ound
man
agem
ent.
•ac
cess
pod
iatri
st/fo
ot c
linic
if
requ
ired.
54
Obje
ctiv
e 8.1
(Cont’
d)
Act
ions
Per
form
ance
Res
ponsi
bili
ty•
have
thei
r in
vesti
gatio
ns
man
aged
or
oper
ativ
e pr
oced
ures
app
ropr
iate
ly
timed
.•
have
thei
r di
ffere
nt c
ultu
ral
and
relig
ious
nee
ds m
et,
incl
udin
g ac
cess
to
appr
opria
te fo
od c
hoic
es.
•re
ceiv
e or
al h
ypog
lyca
emic
m
edic
atio
n /
insu
lin
appr
opria
tely
tim
ed in
re
latio
n to
mea
ls.•
acce
ss c
lear
info
rmat
ion
abou
t the
man
agem
ent o
f th
eir
diab
etes
dur
ing
hosp
ital
stay
and
afte
r di
scha
rge.
•lia
ison
with
the
Dia
bete
s Te
am.
•ac
cess
die
tetic
adv
ice.
•re
ceiv
e fo
llow
-up
on
disc
harg
e fro
m h
ospi
tal.
Educ
atio
n an
d up
datin
g of
war
d Pr
ogra
mm
e in
pla
ce b
y 20
04N
HS
Trus
tsba
sed
nurs
ing
staff
and
juni
or
med
ical
sta
ff
Implementation of standard 9
Standard 9
The NHS will develop, implement and monitor policies that seek to empowerand support women with pre-existing diabetes and those who developdiabetes during pregnancy to optimise the outcomes of their pregnancy.
AIM
To achieve a good outcome and experience of pregnancy and childbirth forwomen with pre-existing diabetes and for those who develop diabetes inpregnancy.
RATIONALE
1. The aim of maternity care is to ensure that all pregnant women have apositive experience of pregnancy and childbirth and receive care thatpromotes their physical health and psychological well being and optimisesthe health of their baby. Although some women’s experience of a‘medicalised’ and high-intervention labour and delivery can be a negativeor frightening one, this need not be the case if they and their partner areinvolved in decision-making and kept fully informed.
2. Diabetes is the most common pre-existing medical disordercomplicating pregnancy in the UK. Approximately one pregnant woman in250 has pre-existing diabetes. This is associated with increased risks forboth mother and baby.
3. Women with pre-existing diabetes are much more likely to lose theirbaby than women who do not have diabetes, either during pregnancy as aresult of a miscarriage or an intrauterine death, or after birth. In the UKperinatal mortality rates amongst the babies of mothers with diabetes are upto five times higher than in the general population. Congenital malformationsare the main cause of this high perinatal mortality. These result fromabnormal foetal development during the six weeks following conception.Later in pregnancy, the main risks to the baby are excessive foetal growth(macrosomia), which can result in damage to both the baby and the motherduring delivery. The main risk to the baby after delivery is hypoglycaemia.These risks can be reduced if near-normal blood glucose levels are achievedbefore and around the time of conception, throughout pregnancy and duringlabour.
55
4. Pregnancy results in increasing insulin resistance and if more insulindoes not match this hyperglycaemia ensues. However, intensified glucosecontrol can also increase the risk of hypoglycaemia. Pregnancy can alsoresult in the progression, if present, of diabetic retinopathy and diabeticnephropathy.
5. Women with pre-existing diabetic nephropathy also have an increasedrisk of pre-eclampsia, hypertensive disease of pregnancy and placentalinsufficiency. Maternal deaths in women with diabetes are now, thankfully,rare but do still occur occasionally.
6. Outcomes can be improved if women with pre-existing diabetes aresupported to plan their pregnancies and to optimise their blood glucosecontrol before and throughout their pregnancies. They should receive closemonitoring and specialist care pre-pregnancy and throughout pregnancyand childbirth.
7. Between 2 and 12 percent of women develop gestational diabetes,which is more common in women from minority ethnic groups. These womenare more likely to have large-for-date babies, a risk that can be reduced byreducing maternal hyperglycaemia. Women whose blood glucose levelsrevert to normal after delivery have an increased risk of developing Type 2diabetes later in life. They can reduce this risk by increasing their physicalactivity levels, eating a balanced diet and avoiding excessive weight gain.As they are significantly at risk of developing Type 2 diabetes they shouldreceive routine follow up and attend for annual review.
56
57
STA
ND
ARD
9Th
e N
HS
will
dev
elop
, im
plem
ent a
nd m
onito
r pol
icie
s th
at s
eek
to e
mpo
wer
and
sup
port
wom
en w
ith p
re-e
xisti
ng d
iabe
tes
and
thos
e w
hode
velo
p di
abet
es d
urin
g pr
egna
ncy
to o
ptim
ise
the
outc
omes
of t
heir
preg
nanc
y.
Obje
ctiv
eA
ctio
ns
Per
form
ance
Res
ponsi
bili
tyO
bje
ctiv
e 9.1
Ensu
re e
ffect
ive
man
agem
ent o
f D
evel
op a
nd p
ilot p
roto
cols
for
LHBs
preg
nant
wom
en w
ith d
iabe
tes.
effe
ctiv
e di
abet
es
In p
lace
and
aud
ited
by 2
005.
NH
S Tr
usts
man
agem
ent p
re c
once
ptio
n,
Prim
ary
care
team
sin
tra p
artu
m, p
ost p
artu
m a
nd
durin
g pr
egna
ncy.
Revi
ew lo
cal p
olic
ies
for
the
LHB
dete
ctio
n an
d m
anag
emen
t of
Aud
it by
200
5.N
HS
Trus
tsge
statio
nal d
iabe
tes
in
preg
nant
wom
en a
nd p
ost
partu
m fo
llow
up.
Atte
nd fo
r an
nual
rev
iew
.
Implementing standards 10, 11 and 12
Standard 10
All young people and adults with diabetes will receive regular surveillanceand screening for the long-term complications of diabetes.
Standard 11
The NHS will develop, implement and monitor agreed protocols and systemsof care to ensure that all people who develop long-term complications ofdiabetes receive timely, appropriate and effective investigation andtreatment to reduce their risk of disability and premature death.
Standard 12
All people with diabetes requiring multi-agency support will receiveintegrated health and social care.
AIM
To minimise the impact of the long-term complications of diabetes by earlydetection and effective treatment and by maximising the quality of life ofthose who develop long-term complications.
RATIONALE
1. People with diabetes are at risk of developing the microvascularcomplications of diabetes: diabetic retinopathy (damage to the eyes),diabetic nephropathy (damage to the kidneys) and diabetic neuropathy(damage to the nerves). They are also at increased risk of developingcardiovascular disease, including coronary heart disease, stroke andperipheral vascular disease.
2. The impact of the microvascular complications can be reduced ifdiabetes is detected and treated at an early stage.
3. Early detection of sight threatening diabetic retinopathy andtreatment with laser therapy can prevent visual impairment. The quality of lifeof those who develop visual impairment can be improved by access to lowvision aids, information, and psychological support and appropriate welfarebenefits. People with diabetes are also entitled to free eye examinationthrough the General Opthalmic Services.
58

4. Angiotensin converting enzyme (ACE) inhibitors can delay the onset ofdiabetic nephropathy in people with diabetes who are found to havemicroalbumuria. Tight control of raised blood pressure, as well as tightcontrol of blood glucose levels, can significantly reduce the rate ofprogression of diabetic nephropathy.
5. Diabetic foot problems are the most frequent manifestation of diabeticneuropathy. Foot ulceration and lower limb amputation can be reduced ifpeople who have sensory neuropathy affecting their feet are identified andoffered foot care education, podiatry and, where required protectivefootwear. Examination of the feet should be included in annual review.Prompt treatment of foot ulcers can reduce the risk of amputation. For thosewho require amputation, their rehabilitation can be optimised through theprovision of care by integrated, multidisciplinary, rehabilitation, prostheticand social support teams.
6. People with diabetes who develop cardiovascular disease can benefitfrom secondary prevention measures already recommended for the generalpopulation in "Tackling Coronary Heart Disease in Wales: implementingthrough evidence" including treatment with low dose aspirin, ß blockers andlipid-lowering agents. In addition, outcomes for people with Type 2 diabeteswho have a heart attack are improved if they are treated with intensiveinsulin therapy.
7. Regular surveillance for, and effective management of, other conditionsthat occur more commonly in people with diabetes, such as depression anderectile dysfunction, can reduce the impact of these conditions on the qualityof life of people with diabetes.
59
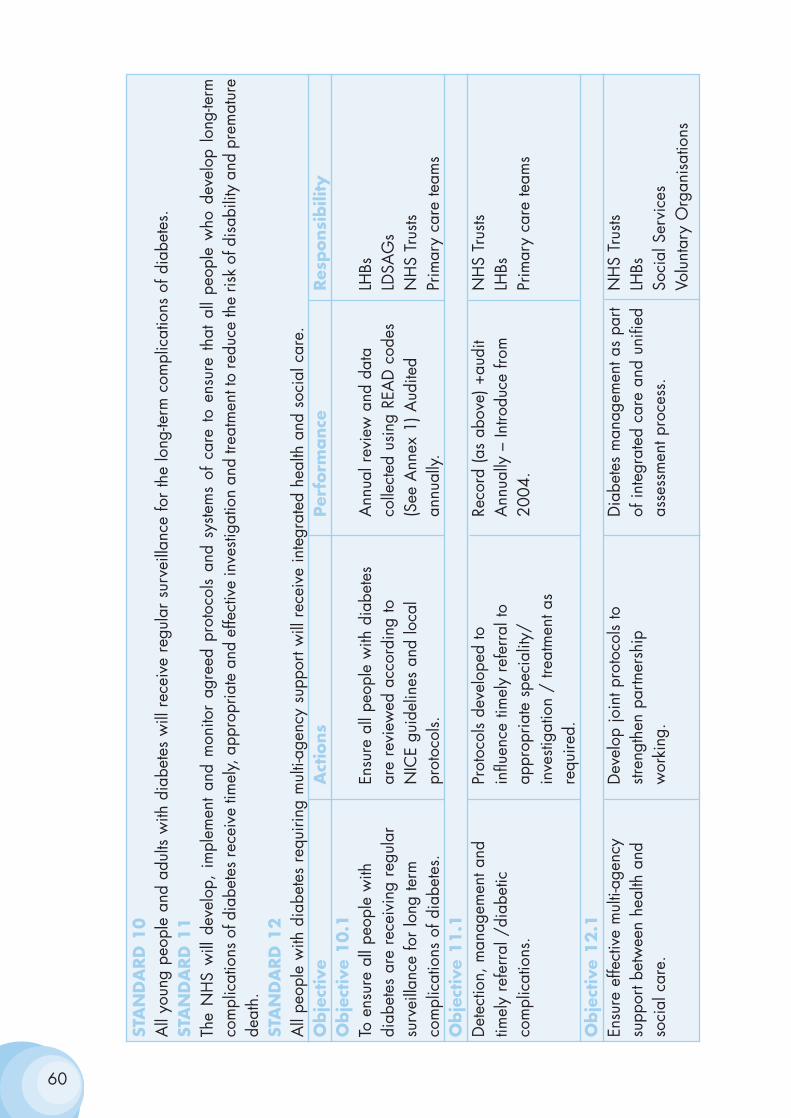
60
STA
ND
ARD
10
All
youn
g pe
ople
and
adu
lts w
ith d
iabe
tes
will
rec
eive
reg
ular
sur
veill
ance
for
the
long
-term
com
plic
atio
ns o
f dia
bete
s.ST
AN
DA
RD
11
The
NH
S w
ill d
evel
op,
impl
emen
t an
d m
onito
r ag
reed
pro
toco
ls an
d sy
stem
s of
car
e to
ens
ure
that
all
peop
le w
ho d
evel
op l
ong-
term
com
plic
atio
ns o
f dia
bete
s re
ceiv
e tim
ely,
app
ropr
iate
and
effe
ctiv
e in
vesti
gatio
n an
d tre
atm
ent t
o re
duce
the
risk
of d
isab
ility
and
pre
mat
ure
deat
h.ST
AN
DA
RD
12
All
peop
le w
ith d
iabe
tes
requ
iring
mul
ti-ag
ency
sup
port
will
rec
eive
inte
grat
ed h
ealth
and
soc
ial c
are.
O
bje
ctiv
eA
ctio
ns
Per
form
ance
Res
ponsi
bili
tyO
bje
ctiv
e 10.1
To e
nsur
e al
l peo
ple
with
En
sure
all
peop
le w
ith d
iabe
tes
Ann
ual r
evie
w a
nd d
ata
LHBs
diab
etes
are
rec
eivi
ng r
egul
ar
are
revi
ewed
acc
ordi
ng to
co
llect
ed u
sing
REA
D c
odes
LDSA
Gs
surv
eilla
nce
for
long
term
N
ICE
guid
elin
es a
nd lo
cal
(See
Ann
ex 1
) Aud
ited
NH
S Tr
usts
com
plic
atio
ns o
f dia
bete
s.pr
otoc
ols.
annu
ally.
Prim
ary
care
team
sO
bje
ctiv
e 11.1
Det
ectio
n, m
anag
emen
t and
Pr
otoc
ols
deve
lope
d to
Re
cord
(as
abov
e) +
audi
tN
HS
Trus
tstim
ely
refe
rral
/di
abet
ic
influ
ence
tim
ely
refe
rral
to
Ann
ually
– In
trodu
ce fr
om
LHBs
com
plic
atio
ns.
appr
opria
te s
peci
ality
/ 20
04.
Prim
ary
care
team
sin
vesti
gatio
n /
treat
men
t as
requ
ired.
Obje
ctiv
e 12.1
Ensu
re e
ffect
ive
mul
ti-ag
ency
D
evel
op jo
int p
roto
cols
to
Dia
bete
s m
anag
emen
t as
part
NH
S Tr
usts
su
ppor
t bet
wee
n he
alth
and
str
engt
hen
partn
ersh
ip
of in
tegr
ated
car
e an
d un
ified
LH
Bsso
cial
car
e.w
orki
ng.
asse
ssm
ent p
roce
ss.
Soci
al S
ervi
ces
Volu
ntar
y O
rgan
isat
ions
Annex 1
Summary of Report – InformationManagement and Technology Sub-Group
The NSF on Diabetes
"National Service Frameworks (NSFs) are being developed to addressvariations in standards of care and to achieve greater consistency in theavailability and quality of services, by putting in place mechanisms whichwill enable best care to be provided to all."
As outlined in the NHS Wales White Paper "Quality Care and ClinicalExcellence", National Service Frameworks provide a systematic approach todriving up standards to improve quality across health care sectors, inpartnership with social care and other organisations. They:
• set national standards and define service models for a service orcare group;
• put in place programmes to support implementation.
The English NSF on Diabetes aims to "establish performance measuresagainst which progress within agreed timescales would bemeasured………and to have a systematic approach to the detection of thelong-term complications of diabetes with regular, planned review anddelivery initially prioritised to the highest risk groups."
In order to be able to develop the service to our people withdiabetes and be able to monitor progress, (and in due course,outcomes), the establishment of a meaningful informationsystem is essential.
Most clinical data in the NHS is gathered inefficiently and in anunstandardised, unstructured manner. Consequently it is difficult to accessand not useable as worthwhile information. Diabetes is no exception. Whatis more, in the light of current evidence, caring for the person with diabeteshas become multifaceted and mutiprofessional. There is also the culture ofmore information for patients and empowerment for them to take a moreactive role in their care plans.
61
In order for such a complex system of care to work effectively and efficiently,there should be a method of information flow where each individual careprovider can be able to contribute and have access to ‘fit for purpose’information at the point of care.
The King’s Fund suggests that diabetes management should be a primarycare led service, with seamless integration with secondary and tertiary careprovider. Thus, a shared record, in which the interventions of ConsultantPhysicians, GPs, hospital, community and practice nurses and Allied HealthProfessionals, are recorded would not only support shared care andfacilitate teamwork, but also: -
• Enable the creation of a patient profile.
• Eliminate inappropriate, duplication of procedures.
• Identify any change in the patient's condition to provide moreappropriate and quicker change in management.
• Use the skills of a clinical team to provide an optimum service atminimum cost and inconvenience to patient and care provider.
• Enable comparable information on clinical quality to be derived tosupport clinical audit, clinical governance and performancemanagement purposes.
Whilst recognising that clinical data has special problems, and not least thatof confidentiality, it is imperative that in order to maximise the usefulness ofthese data, common standards in inputting should be defined and any suchstandard should try and anticipate future augmentation. We would thenhave the ability to access large amounts of information of individual patientsand aggregates and have reliable comparative data. Research activitiesand more appropriate use of resources could develop almost as by-productsof service, which could have considerable benefits to the process of qualityGP commissioning. Thus, we could:
• develop accurate population based information systems for peoplewith diabetes
• develop structured programmes for the systematic reviews ofpatients and keep up to date records
62
• develop systematic programmes to monitor and audit processes andoutcomes and recall patients for regular review
• ensure access to podiatrists and dieticians, when carrying outannual reviews with patients
• ensure provision of support and education to hospital andcommunity staff, and work with them to develop guidelines forreferral and management of people with diabetes
• ensure that staff, particularly GPs and practice nurses, are well-trained and kept up to date with new developments
• support clinical audit, clinical governance and performancemanagement purposes.
The patient with diabetes should be offered:-
1. An annual review.
2. A regular follow-up programme.
3. Regular specialist investigation when appropriate.
4. An open and quick referral to a "problem clinic" run by a consultant.
Along the lines suggested by the English NSF, a core underpinning datasetto support a person with diabetes in managing their care should beestablished. The dataset will cover key risk factors, processes, intermediateoutcomes and final outcomes, and support information that the person withdiabetes or the carer, can hold, understand and act upon.
A suggested pro-forma for an annual review dataset is included in Figure 1. Supporting information, held in the generic patient record, wouldinclude patient identifiers, ethnicity, family history and lifestyle profile.
63
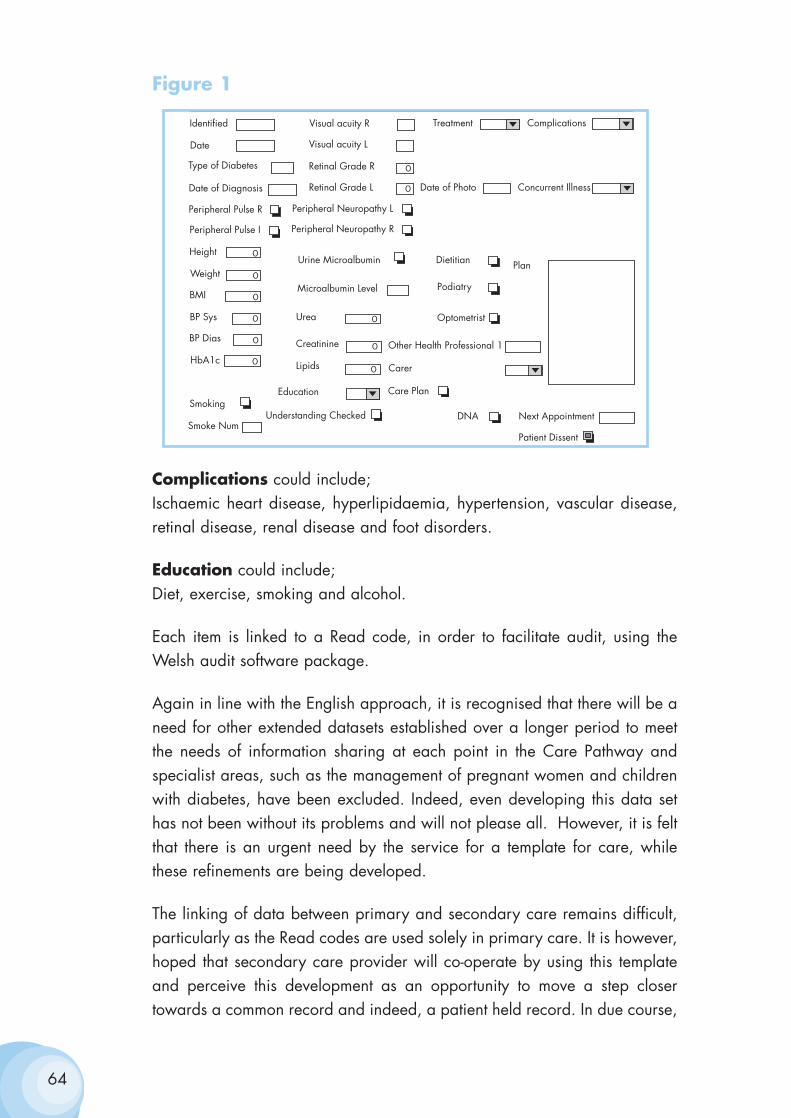
Figure 1
Complications could include;Ischaemic heart disease, hyperlipidaemia, hypertension, vascular disease,retinal disease, renal disease and foot disorders.
Education could include;Diet, exercise, smoking and alcohol.
Each item is linked to a Read code, in order to facilitate audit, using theWelsh audit software package.
Again in line with the English approach, it is recognised that there will be aneed for other extended datasets established over a longer period to meetthe needs of information sharing at each point in the Care Pathway andspecialist areas, such as the management of pregnant women and childrenwith diabetes, have been excluded. Indeed, even developing this data sethas not been without its problems and will not please all. However, it is feltthat there is an urgent need by the service for a template for care, whilethese refinements are being developed.
The linking of data between primary and secondary care remains difficult,particularly as the Read codes are used solely in primary care. It is however,hoped that secondary care provider will co-operate by using this templateand perceive this development as an opportunity to move a step closertowards a common record and indeed, a patient held record. In due course,
64
Identified
Date
Visual acuity R
Visual acuity L
Retinal Grade RType of Diabetes
Date of Diagnosis Retinal Grade L Date of Photo
Treatment Complications
Concurrent Illness
Peripheral Pulse R
Peripheral Pulse I
Peripheral Neuropathy L
Peripheral Neuropathy R
Height
Weight
BMI
BP Sys
BP Dias
HbA1c
Urine Microalbumin
Microalbumin Level
Urea
Creatinine
Lipids
Dietitian
Podiatry
Optometrist
Other Health Professional 1
Carer
SmokingEducation Care Plan
Smoke NumUnderstanding Checked DNA Next Appointment
Patient Dissent
Plan0
0
0
0
0
0
0
0
0
0
0
double entry and other investigations will become less common, reducingexpense and inconvenience to patients.
We have also worked with the ICT Foundation Programme for GeneralMedical Practices, which has developed:
(1) an Education, Training and Development (ETD) Framework
(2) a Data Quality Initiative (DQI)
These support its aim of improving data quality and the use of clinicalinformation systems to support the delivery of patient care. Both the ETDframework and DQI are intrinsically linked to supporting clinical priorities,in particular the delivery of the Diabetes NSF.
To conclude, this template is seen as the foundation stone for appropriatedata management and the development of useful information for the care ofthe patient with diabetes. It will also serve as an audit tool and assistpractices to achieve quality payment if the new GP contract is accepted. Thedata set will be linked to that of heart disease, which it is anticipated, willalso have an all Wales template in the near future. It is recognised that thisinformation package is only the beginning of an evolving process and it issuggested that the process be reviewed at intervals.
65
Annex 2
Clinical Terminology Support for the DiabetesNational Service Framework
In order to support high quality care for those at risk and those withconfirmed diabetes, it is essential to create and maintain consistent andcomprehensive patient centred clinical records. This process is facilitatedwithin general practice by the widespread use of sophisticated electronicclinical systems.
The Diabetes National Service Framework outlines twelve evidence basedStandards for implementation in Wales. Associated with these twelveStandards are a number of Key Actions that are to be monitored locally andwhere appropriate reported on nationally.
In order to be able to show that these key actions have been completedand/or monitored it is necessary to collect some basic, patient centred, dataon the clinical system in a structured and consistent way. It is clearlyimportant to ensure that these data items support and are a by-product of theday-to-day clinical management of the patient and not an additional‘information burden’ on the clinician.
As all of the GP clinical systems incorporate the Read Codes these data itemsare based on Read Code terms and their associated codes for each of theversions, GP 4 Byte, Version 2 and Clinical Terms Version 3.
Work is currently ongoing to develop a number of Read Code lists to supportthe clinical management of people with diabetes. The creation of ‘virtualregisters’ within the Clinical Management System will enable consistent calland recall of those at risk, and those with confirmed diabetes and a numberof lists to support high quality clinical audit. This work is being supportedby and receiving feedback from the appropriate clinical professional bodies.
Clinical system suppliers are being consulted to ensure that these lists can beimplemented in a way that makes data capture simple and consistent and tosupport the implementation of the clinical audit queries.
66
Two lists of Read Code terms are recommended as being appropriate to useas the target group of lifestyles, conditions and disorders that fall within theremit of the twelve Standards.
• The first short list (List A) forms the basis of the list or register ofpatients within the Clinical Management system. They would beused to support call and recall of patients and constitute the basepopulation for clinical audit.
• The second more comprehensive list (List B) enables more detailedclinical audit and would serve to provide sufficient information tosupport clinical governance requirements.
A guiding principle employed in deriving these lists is that the clinical termsshould be used prospectively and forms a natural part of the informationcollected to support the day-to-day clinical management of the patient. It is,therefore, proposed that clinicians should use these lifestyle and clinicaldiagnostic groups in the following circumstances:
• At the time of new patient registration to record lifestyle, andprevious and current medical problems relating to diabetes.
• For existing practice patients when they present with featuressuggestive of diabetes.
• To review the diagnostic coding of those patients with known risk oractual diabetes who present for review or repeat prescriptions.
• To review lifestyle and clinical diagnostic coding of patientsidentified from a practice audit.
• This list of Read Codes has been provided for Read Code 4Byte andVersion 2. Clinical Terms Version 3 (CTV3) Read Code lists areavailable and may be obtained from the ICT Foundation Programmefor General Medical Practices. Telephone number 01792 607434,e-mail: [email protected]
• At the time of publication a small number of required clinical termsand codes were found to be absent from the March 2003 releaseof Read Codes. Application has been made to the NHS InformationAuthority to have these added in the next release and an update listwill be circulated in due course.
67

It is intended that the lists developed should be dynamic and keep pace withthe services requirements, evolving clinical guidelines and the ability ofsuppliers to support good quality user interfaces.
68
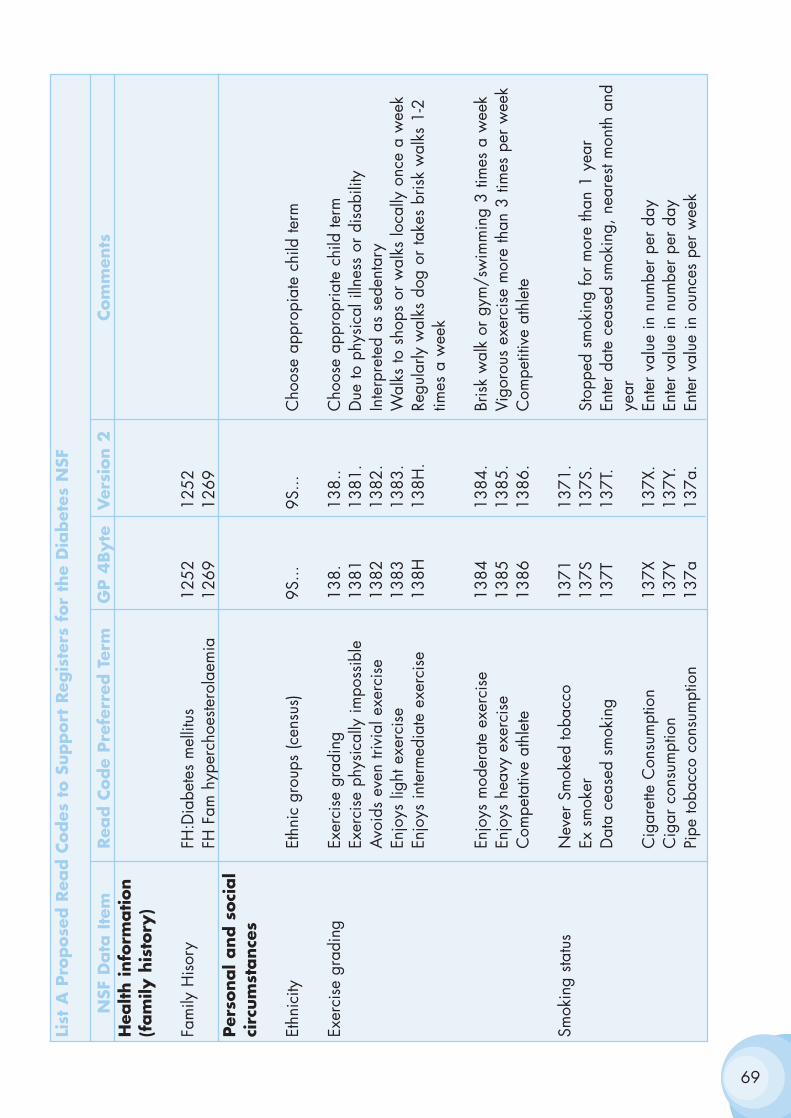
69
List
A P
ropose
d R
ead C
odes
to S
upport
Reg
iste
rs f
or
the
Dia
bet
es N
SF
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsH
ealth info
rmation
(fam
ily h
isto
ry)
Fam
ily H
isor
yFH
:Dia
bete
s m
ellit
us12
5212
52FH
Fam
hyp
erch
oeste
rola
emia
1269
1269
Per
sonal and s
oci
al
circ
um
stance
s
Ethn
icity
Ethn
ic g
roup
s (c
ensu
s)9S
...9S
...C
hoos
e ap
prop
iate
chi
ld te
rm
Exer
cise
gra
ding
Exer
cise
gra
ding
138.
138.
.C
hoos
e ap
prop
riate
chi
ld te
rmEx
erci
se p
hysi
cally
impo
ssib
le13
8113
81.
Due
to p
hysi
cal i
llnes
s or
dis
abili
tyA
void
s ev
en tr
ivia
l exe
rcis
e13
8213
82.
Inte
rpre
ted
as s
eden
tary
Enjo
ys li
ght e
xerc
ise
1383
1383
.W
alks
to s
hops
or
wal
ks lo
cally
onc
e a
wee
kEn
joys
inte
rmed
iate
exe
rcis
e13
8H13
8H.
Regu
larly
wal
ks d
og o
r ta
kes
bris
k w
alks
1-2
tim
es a
wee
k
Enjo
ys m
oder
ate
exer
cise
1384
1384
.Br
isk
wal
k or
gym
/sw
imm
ing
3 tim
es a
wee
kEn
joys
hea
vy e
xerc
ise
1385
1385
.Vi
goro
us e
xerc
ise
mor
e th
an 3
tim
es p
er w
eek
Com
peta
tive
athl
ete
1386
1386
.C
ompe
titiv
e at
hlet
e
Smok
ing
statu
sN
ever
Sm
oked
toba
cco
1371
1371
.Ex
sm
oker
137S
137S
.St
oppe
d sm
okin
g fo
r m
ore
than
1 y
ear
Dat
a ce
ased
sm
okin
g13
7T13
7T.
Ente
r da
te c
ease
d sm
okin
g, n
eare
st m
onth
and
ye
arC
igar
ette
Con
sum
ptio
n13
7X13
7X.
Ente
r va
lue
in n
umbe
r pe
r da
yC
igar
con
sum
ptio
n13
7Y13
7Y.
Ente
r va
lue
in n
umbe
r pe
r da
yPi
pe to
bacc
o co
nsum
ptio
n13
7a13
7a.
Ente
r va
lue
in o
unce
s pe
r w
eek
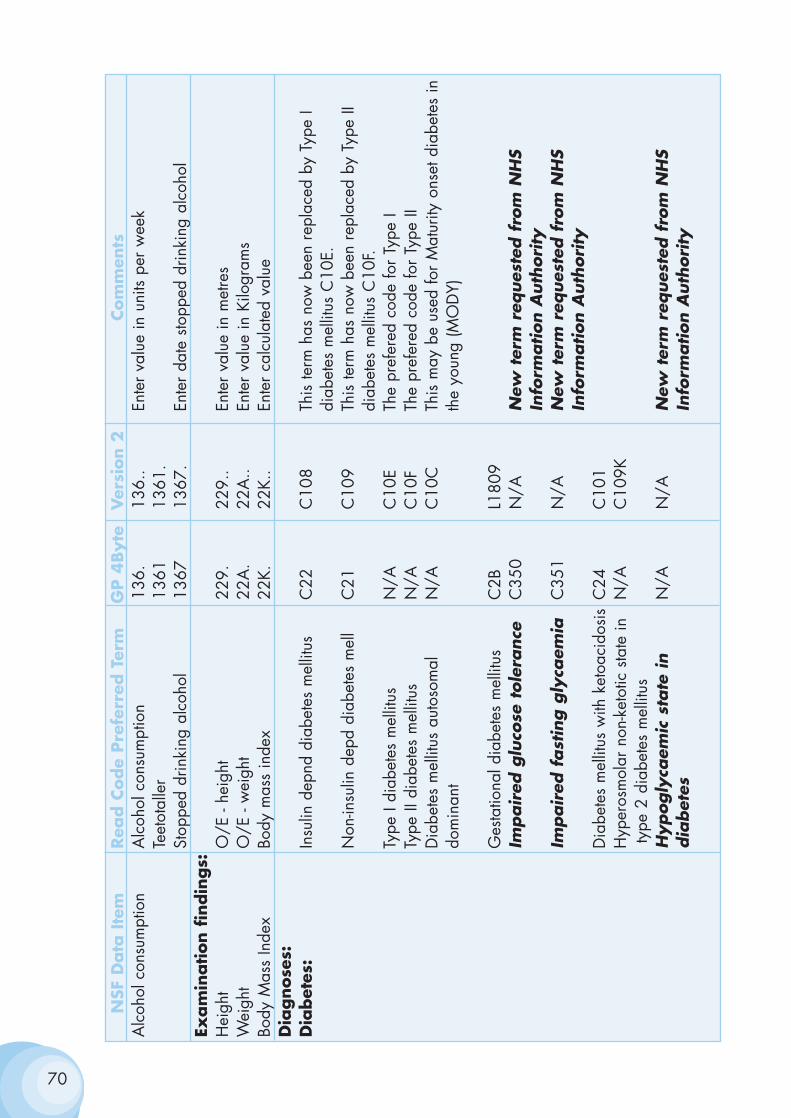
70
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsA
lcoh
ol c
onsu
mpt
ion
Alc
ohol
con
sum
ptio
n13
6.13
6..
Ente
r va
lue
in u
nits
per
wee
kTe
etot
alle
r13
6113
61.
Stop
ped
drin
king
alc
ohol
1367
1367
.En
ter
date
sto
pped
drin
king
alc
ohol
Exam
ination f
indin
gs:
Hei
ght
O/E
- he
ight
229.
229.
.En
ter
valu
e in
met
res
Wei
ght
O/E
- w
eigh
t22
A.
22A
..En
ter
valu
e in
Kilo
gram
sBo
dy M
ass
Inde
xBo
dy m
ass
inde
x22
K.22
K..
Ente
r ca
lcul
ated
val
ueD
iagnose
s:D
iabet
es:
Insu
lin d
epnd
dia
bete
s m
ellit
usC
22C
108
This
term
has
now
bee
n re
plac
ed b
y Ty
pe I
diab
etes
mel
litus
C10
E.N
on-in
sulin
dep
d di
abet
es m
ell
C21
C10
9Th
is te
rm h
as n
ow b
een
repl
aced
by
Type
II
diab
etes
mel
litus
C10
F.Ty
pe I
diab
etes
mel
litus
N/A
C10
ETh
e pr
efer
ed c
ode
for
Type
ITy
pe II
dia
bete
s m
ellit
usN
/AC
10F
The
pref
ered
cod
e fo
r Ty
pe II
Dia
bete
s m
ellit
us a
utos
omal
N
/AC
10C
This
may
be
used
for
Mat
urity
ons
et d
iabe
tes
indo
min
ant
the
youn
g (M
OD
Y)
Ges
tatio
nal d
iabe
tes
mel
litus
C2B
L180
9Im
pair
ed g
luco
se t
ole
rance
C35
0N
/AN
ew t
erm
req
ues
ted f
rom
NH
S In
form
ation A
uth
ori
tyIm
pair
ed f
ast
ing g
lyca
emia
C35
1N
/AN
ew t
erm
req
ues
ted f
rom
NH
S In
form
ation A
uth
ori
tyD
iabe
tes
mel
litus
with
ket
oaci
dosi
sC
24C
101
Hyp
eros
mol
ar n
on-k
etot
ic s
tate
inN
/AC
109K
type
2 d
iabe
tes
mel
litus
Hypogly
caem
ic s
tate
in
N/A
N/A
New
ter
m r
eques
ted f
rom
NH
S dia
bet
esIn
form
ation A
uth
ori
ty
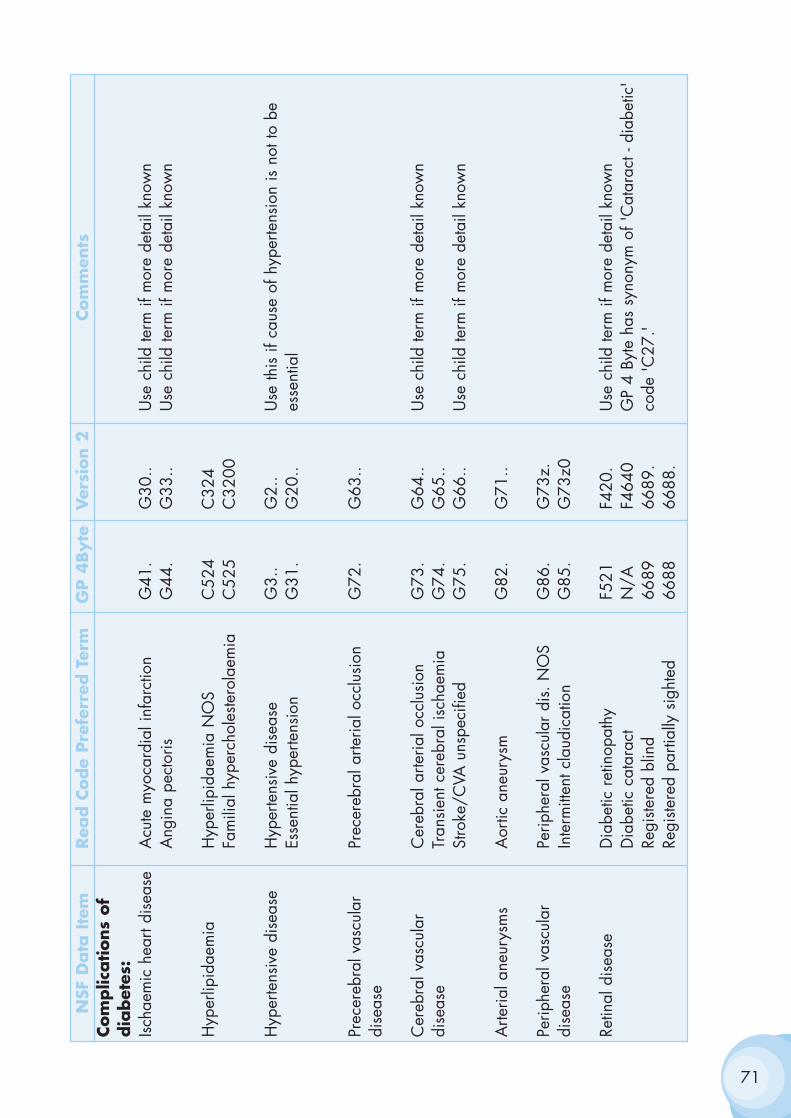
71
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsCom
plic
ations
of
dia
bet
es:
Ischa
emic
hea
rt di
seas
eA
cute
myo
card
ial i
nfar
ctio
nG
41.
G30
..U
se c
hild
term
if m
ore
deta
il kn
own
Ang
ina
pect
oris
G44
.G
33..
Use
chi
ld te
rm if
mor
e de
tail
know
n
Hyp
erlip
idae
mia
Hyp
erlip
idae
mia
NO
SC
524
C32
4Fa
mili
al h
yper
chol
este
rola
emia
C52
5C
3200
Hyp
erte
nsiv
e di
seas
eH
yper
tens
ive
dise
ase
G3.
.G
2..
Use
this
if c
ause
of h
yper
tens
ion
is n
ot to
be
Esse
ntia
l hyp
erte
nsio
nG
31.
G20
..es
sent
ial
Prec
ereb
ral v
ascu
lar
Prec
ereb
ral a
rteria
l occ
lusi
onG
72.
G63
..di
seas
e
Cer
ebra
l vas
cula
r C
ereb
ral a
rteria
l occ
lusi
onG
73.
G64
..U
se c
hild
term
if m
ore
deta
il kn
own
dise
ase
Tran
sien
t cer
ebra
l isc
haem
iaG
74.
G65
..St
roke
/CVA
uns
peci
fied
G75
.G
66..
Use
chi
ld te
rm if
mor
e de
tail
know
n
Arte
rial a
neur
ysm
sA
ortic
ane
urys
mG
82.
G71
..
Perip
hera
l vas
cula
r Pe
riphe
ral v
ascu
lar
dis.
NO
SG
86.
G73
z.di
seas
eIn
term
itten
t cla
udic
atio
nG
85.
G73
z0
Retin
al d
isea
seD
iabe
tic r
etin
opat
hyF5
21F4
20.
Use
chi
ld te
rm if
mor
e de
tail
know
nD
iabe
tic c
atar
act
N/A
F464
0G
P 4
Byte
has
syn
onym
of '
Cat
arac
t - d
iabe
tic'
Regi
stere
d bl
ind
6689
6689
.co
de 'C
27.'
Regi
stere
d pa
rtial
ly s
ight
ed66
8866
88.
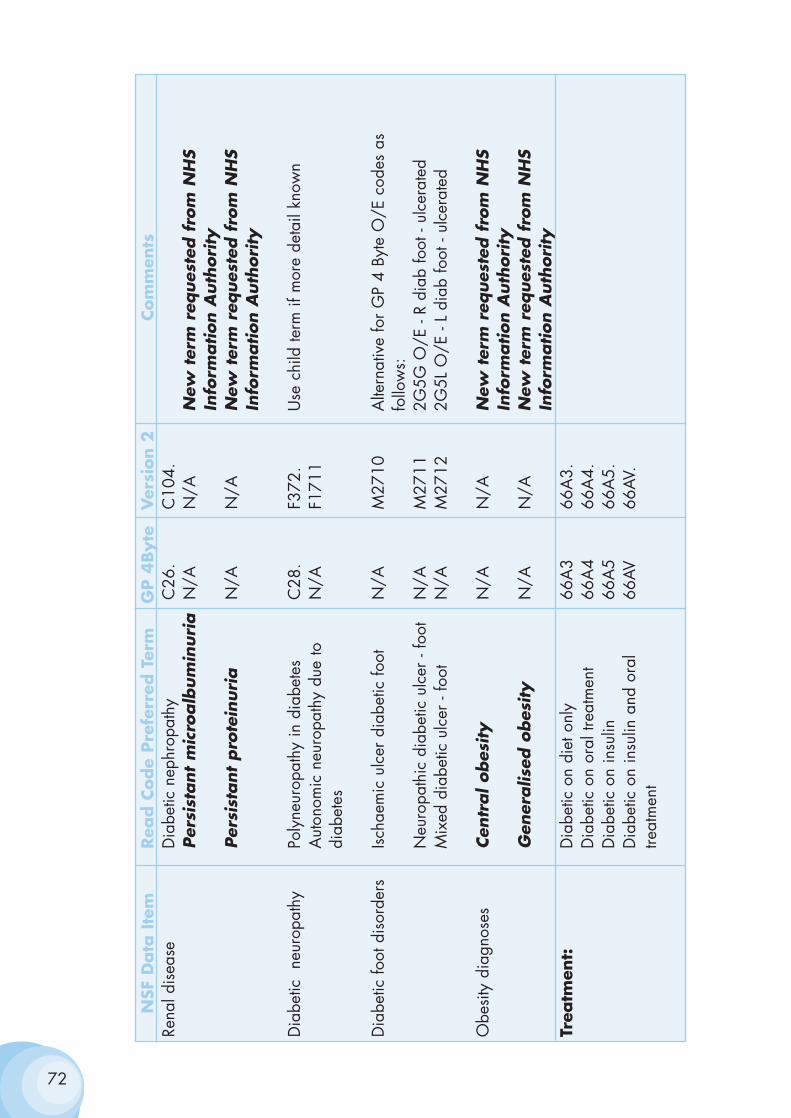
72
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsRe
nal d
isea
seD
iabe
tic n
ephr
opat
hyC
26.
C10
4.Per
sist
ant
mic
roalb
um
inuri
aN
/AN
/AN
ew t
erm
req
ues
ted f
rom
NH
SIn
form
ation A
uth
ori
tyPer
sist
ant
pro
tein
uri
aN
/AN
/AN
ew t
erm
req
ues
ted f
rom
NH
SIn
form
ation A
uth
ori
ty
Dia
betic
ne
urop
athy
Poly
neur
opat
hy in
dia
bete
sC
28.
F372
.U
se c
hild
term
if m
ore
deta
il kn
own
Aut
onom
ic n
euro
path
y du
e to
N
/AF1
711
diab
etes
Dia
betic
foot
dis
orde
rsIsc
haem
ic u
lcer
dia
betic
foot
N/A
M27
10A
ltern
ativ
e fo
r G
P 4
Byte
O/E
cod
es a
s fo
llow
s:N
euro
path
ic d
iabe
tic u
lcer
- fo
otN
/AM
2711
2G5G
O/E
- R
diab
foot
- ul
cera
ted
Mix
ed d
iabe
tic u
lcer
- fo
otN
/AM
2712
2G5L
O/E
- L
diab
foot
- ul
cera
ted
Obe
sity
dia
gnos
esCen
tral obes
ity
N/A
N/A
New
ter
m r
eques
ted f
rom
NH
SIn
form
ation A
uth
ori
tyG
ener
alis
ed o
bes
ity
N/A
N/A
New
ter
m r
eques
ted f
rom
NH
SIn
form
ation A
uth
ori
tyTr
eatm
ent:
Dia
betic
on
diet
onl
y66
A3
66A
3.D
iabe
tic o
n or
al tr
eatm
ent
66A
466
A4.
Dia
betic
on
insu
lin66
A5
66A
5.D
iabe
tic o
n in
sulin
and
ora
l66
AV66
AV.
treat
men
t
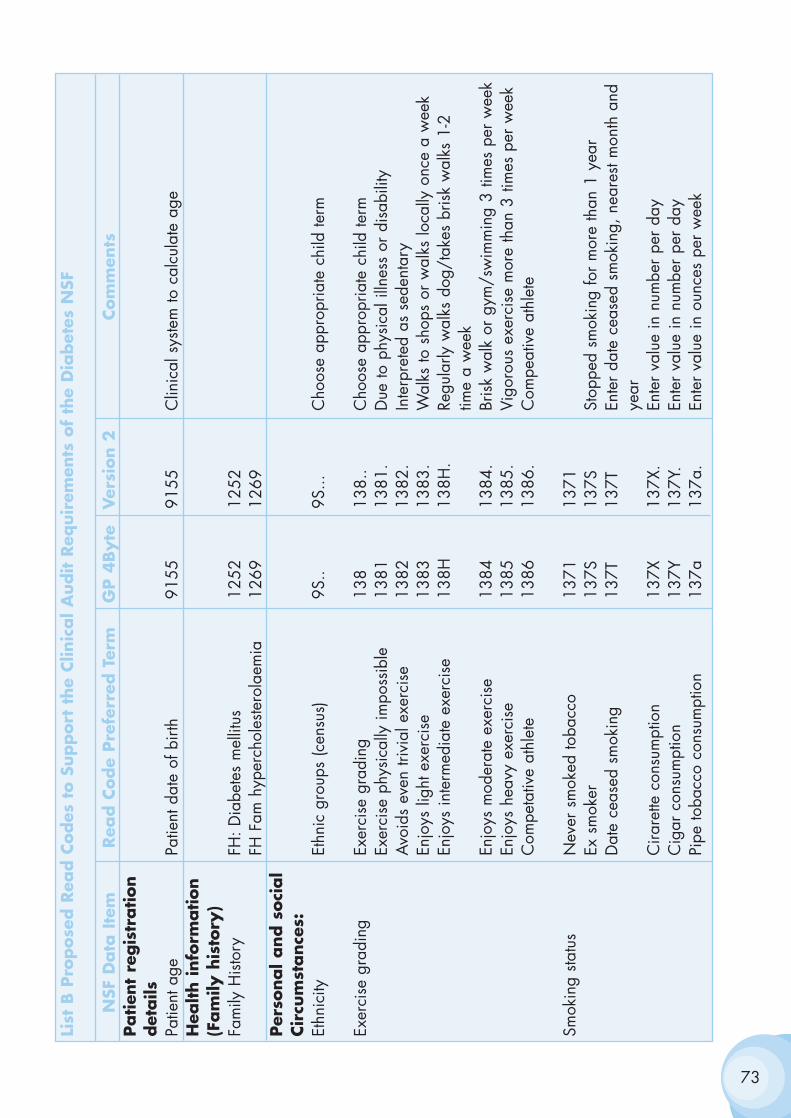
73
List
B P
ropose
d R
ead C
odes
to S
upport
the
Clin
ical A
udit R
equir
emen
ts o
f th
e D
iabet
es N
SF
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsPatien
t re
gis
tration
det
ails
Patie
nt a
gePa
tient
dat
e of
birt
h91
5591
55C
linic
al s
yste
m to
cal
cula
te a
geH
ealth info
rmation
(Fam
ily h
isto
ry)
Fam
ily H
isto
ryFH
: Dia
bete
s m
ellit
us12
5212
52FH
Fam
hyp
erch
oles
tero
laem
ia12
6912
69Per
sonal and s
oci
al
Cir
cum
stance
s:Et
hnic
ityEt
hnic
gro
ups
(cen
sus)
9S..
9S...
Cho
ose
appr
opria
te c
hild
term
Exer
cise
gra
ding
Exer
cise
gra
ding
138
138.
.C
hoos
e ap
prop
riate
chi
ld te
rmEx
erci
se p
hysi
cally
impo
ssib
le13
8113
81.
Due
to p
hysi
cal i
llnes
s or
dis
abili
tyA
void
s ev
en tr
ivia
l exe
rcis
e13
8213
82.
Inte
rpre
ted
as s
eden
tary
Enjo
ys li
ght e
xerc
ise
1383
1383
.W
alks
to s
hops
or
wal
ks lo
cally
onc
e a
wee
kEn
joys
inte
rmed
iate
exe
rcis
e13
8H13
8H.
Regu
larly
wal
ks d
og/t
akes
bris
k w
alks
1-2
time
a w
eek
Enjo
ys m
oder
ate
exer
cise
1384
1384
.Br
isk
wal
k or
gym
/sw
imm
ing
3 tim
es p
er w
eek
Enjo
ys h
eavy
exe
rcis
e13
8513
85.
Vigo
rous
exe
rcis
e m
ore
than
3 ti
mes
per
wee
kC
ompe
tativ
e at
hlet
e13
8613
86.
Com
peat
ive
athl
ete
Smok
ing
statu
sN
ever
sm
oked
toba
cco
1371
1371
Ex s
mok
er13
7S13
7SSt
oppe
d sm
okin
g fo
r m
ore
than
1 y
ear
Dat
e ce
ased
sm
okin
g13
7T13
7TEn
ter
date
cea
sed
smok
ing,
nea
rest
mon
th a
nd
year
Cira
rette
con
sum
ptio
n13
7X13
7X.
Ente
r va
lue
in n
umbe
r pe
r da
yC
igar
con
sum
ptio
n13
7Y13
7Y.
Ente
r va
lue
in n
umbe
r pe
r da
yPi
pe to
bacc
o co
nsum
ptio
n13
7a13
7a.
Ente
r va
lue
in o
unce
s pe
r w
eek
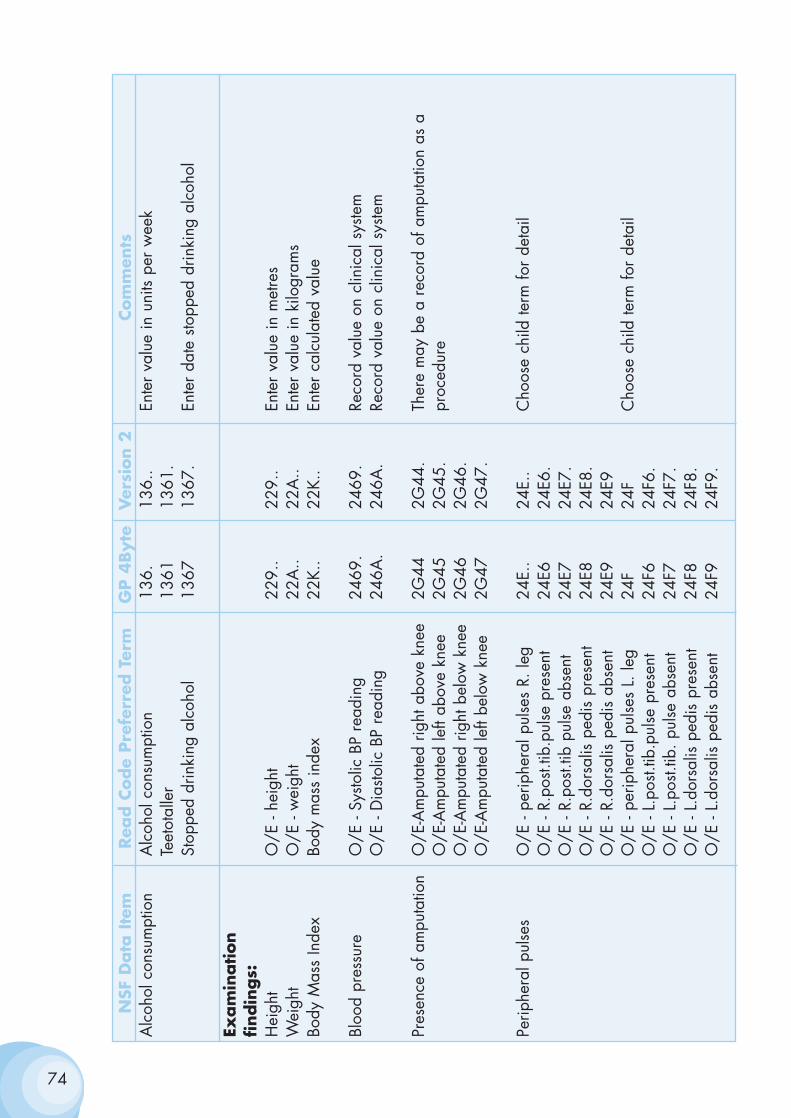
74
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsA
lcoh
ol c
onsu
mpt
ion
Alc
ohol
con
sum
ptio
n13
6.13
6..
Ente
r va
lue
in u
nits
per
wee
kTe
etot
alle
r13
6113
61.
Stop
ped
drin
king
alc
ohol
1367
1367
.En
ter
date
sto
pped
drin
king
alc
ohol
Exam
ination
findin
gs:
Hei
ght
O/E
- he
ight
229.
.22
9..
Ente
r va
lue
in m
etre
sW
eigh
tO
/E -
wei
ght
22A
..22
A..
Ente
r va
lue
in k
ilogr
ams
Body
Mas
s In
dex
Body
mas
s in
dex
22K.
.22
K..
Ente
r ca
lcul
ated
val
ue
Bloo
d pr
essu
reO
/E -
Systo
lic B
P re
adin
g24
69.
2469
.Re
cord
val
ue o
n cl
inic
al s
yste
mO
/E -
Dia
stolic
BP
read
ing
246A
.24
6A.
Reco
rd v
alue
on
clin
ical
sys
tem
Pres
ence
of a
mpu
tatio
nO
/E-A
mpu
tate
d rig
ht a
bove
kne
e2G
442G
44.
Ther
e m
ay b
e a
reco
rd o
f am
puta
tion
as a
O
/E-A
mpu
tate
d le
ft ab
ove
knee
2G45
2G45
.pr
oced
ure
O/E
-Am
puta
ted
right
bel
ow k
nee
2G46
2G46
.O
/E-A
mpu
tate
d le
ft be
low
kne
e2G
472G
47.
Perip
hera
l pul
ses
O/E
- pe
riphe
ral p
ulse
s R.
leg
24E.
.24
E..
Cho
ose
child
term
for
deta
ilO
/E -
R.po
st.tib
.pul
se p
rese
nt24
E624
E6.
O/E
- R.
post.
tib p
ulse
abs
ent
24E7
24E7
.O
/E -
R.do
rsal
is p
edis
pre
sent
24E8
24E8
.O
/E -
R.do
rsal
is p
edis
abs
ent
24E9
24E9
O/E
- pe
riphe
ral p
ulse
s L.
leg
24F
24F
Cho
ose
child
term
for
deta
ilO
/E -
L.po
st.tib
.pul
se p
rese
nt24
F624
F6.
O/E
- L.
post.
tib. p
ulse
abs
ent
24F7
24F7
.O
/E -
L.do
rsal
is p
edis
pre
sent
24F8
24F8
.O
/E -
L.do
rsal
is p
edis
abs
ent
24F9
24F9
.
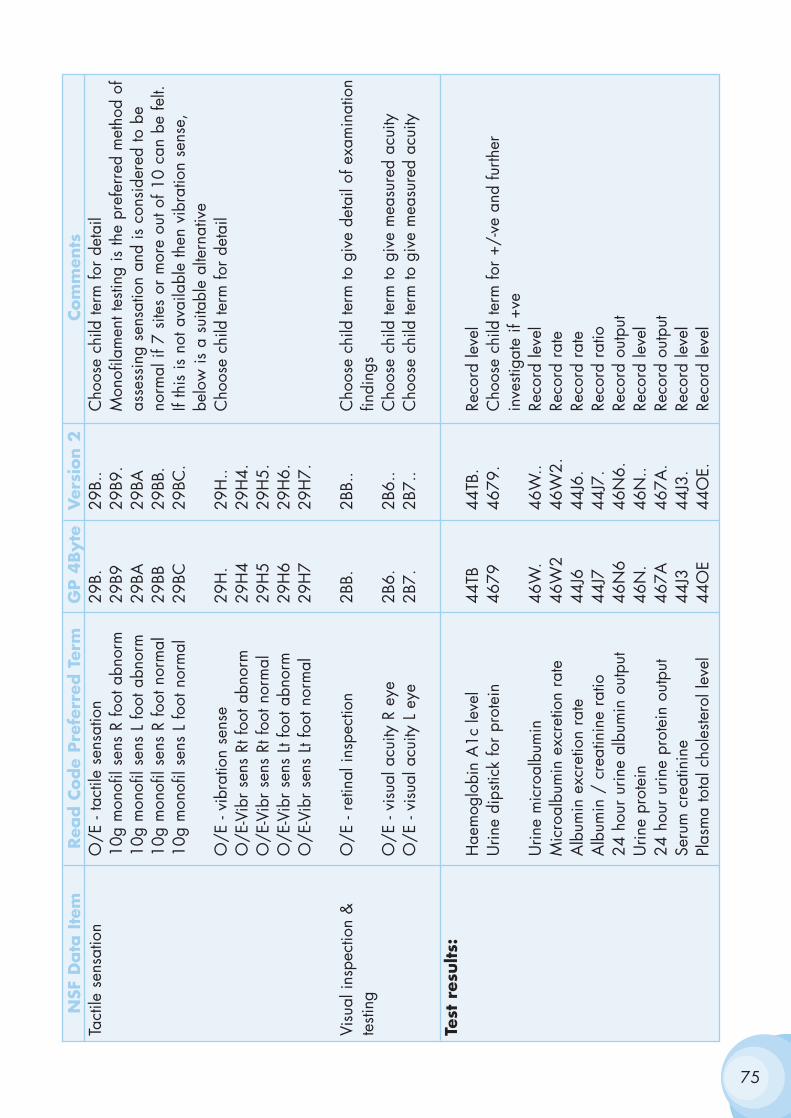
75
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsTa
ctile
sen
satio
nO
/E -
tact
ile s
ensa
tion
29B.
29B.
.C
hoos
e ch
ild te
rm fo
r de
tail
10g
mon
ofil
sens
R fo
ot a
bnor
m29
B929
B9.
Mon
ofila
men
t tes
ting
is th
e pr
efer
red
met
hod
of10
g m
onof
il se
ns L
foot
abn
orm
29BA
29BA
asse
ssin
g se
nsat
ion
and
is c
onsi
dere
d to
be
10g
mon
ofil
sens
R fo
ot n
orm
al29
BB29
BB.
norm
al if
7 s
ites
or m
ore
out o
f 10
can
be fe
lt.10
g m
onof
il se
ns L
foot
nor
mal
29BC
29BC
.If
this
is n
ot a
vaila
ble
then
vib
ratio
n se
nse,
be
low
is a
sui
tabl
e al
tern
ativ
eO
/E -
vibr
atio
n se
nse
29H
.29
H..
Cho
ose
child
term
for
deta
ilO
/E-V
ibr
sens
Rt f
oot a
bnor
m29
H4
29H
4.O
/E-V
ibr
sens
Rt f
oot n
orm
al29
H5
29H
5.O
/E-V
ibr
sens
Lt f
oot a
bnor
m29
H6
29H
6.O
/E-V
ibr
sens
Lt f
oot n
orm
al29
H7
29H
7.
Visu
al in
spec
tion
&
O/E
- re
tinal
insp
ectio
n2B
B.2B
B..
Cho
ose
child
term
to g
ive
deta
il of
exa
min
atio
nte
sting
findi
ngs
O/E
- vi
sual
acu
ity R
eye
2B6.
2B6.
.C
hoos
e ch
ild te
rm to
giv
e m
easu
red
acui
tyO
/E -
visu
al a
cuity
L e
ye2B
7.2B
7..
Cho
ose
child
term
to g
ive
mea
sure
d ac
uity
Test
res
ults:
Hae
mog
lobi
n A
1c le
vel
44TB
44TB
.Re
cord
leve
lU
rine
dips
tick
for
prot
ein
4679
4679
.C
hoos
e ch
ild te
rm fo
r +/
-ve
and
furth
er
inve
stiga
te if
+ve
Urin
e m
icro
albu
min
46W
.46
W..
Reco
rd le
vel
Mic
roal
bum
in e
xcre
tion
rate
46W
246
W2.
Reco
rd r
ate
Alb
umin
exc
retio
n ra
te44
J644
J6.
Reco
rd r
ate
Alb
umin
/ c
reat
inin
e ra
tio44
J744
J7.
Reco
rd r
atio
24 h
our
urin
e al
bum
in o
utpu
t46
N6
46N
6.Re
cord
out
put
Urin
e pr
otei
n46
N.
46N
..Re
cord
leve
l24
hou
r ur
ine
prot
ein
outp
ut46
7A46
7A.
Reco
rd o
utpu
tSe
rum
cre
atin
ine
44J3
44J3
.Re
cord
leve
lPl
asm
a to
tal c
hole
stero
l lev
el44
OE
44O
E.Re
cord
leve
l
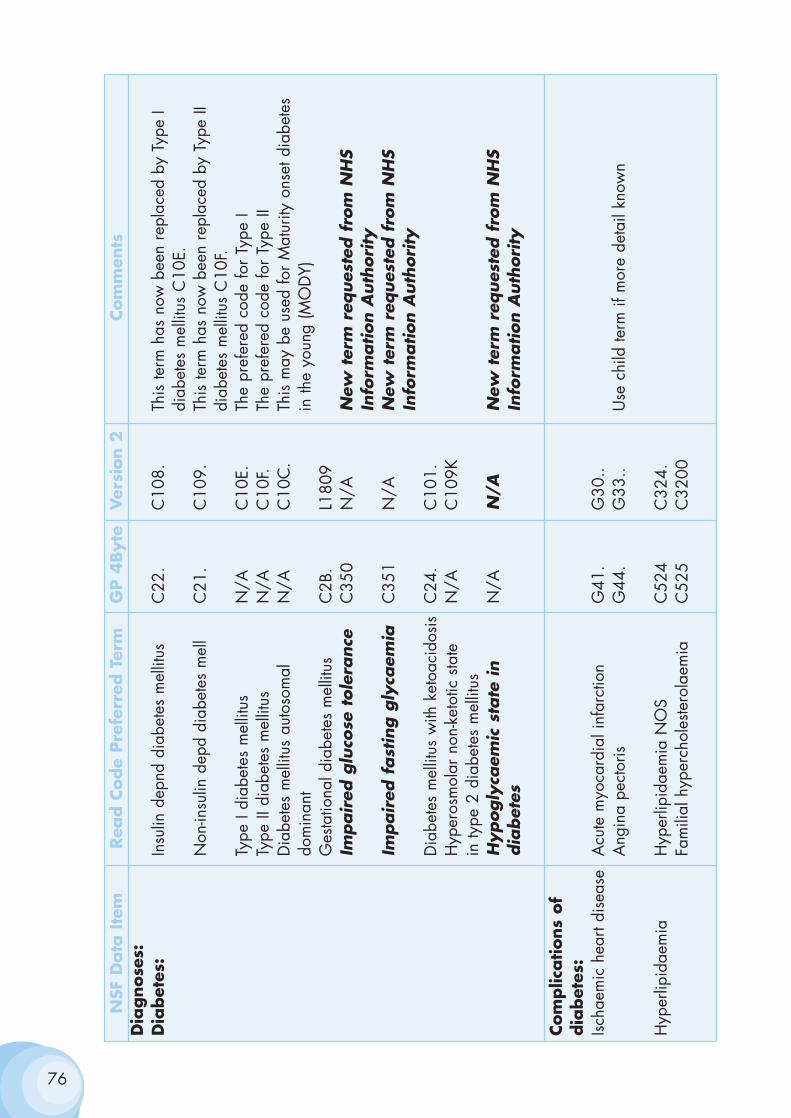
76
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsD
iagnose
s:D
iabet
es:
Insu
lin d
epnd
dia
bete
s m
ellit
usC
22.
C10
8.Th
is te
rm h
as n
ow b
een
repl
aced
by
Type
I di
abet
es m
ellit
us C
10E.
Non
-insu
lin d
epd
diab
etes
mel
lC
21.
C10
9.Th
is te
rm h
as n
ow b
een
repl
aced
by
Type
II
diab
etes
mel
litus
C10
F.Ty
pe I
diab
etes
mel
litus
N/A
C10
E.Th
e pr
efer
ed c
ode
for
Type
ITy
pe II
dia
bete
s m
ellit
usN
/AC
10F.
The
pref
ered
cod
e fo
r Ty
pe II
Dia
bete
s m
ellit
us a
utos
omal
N/A
C10
C.
This
may
be
used
for
Mat
urity
ons
et d
iabe
tes
dom
inan
tin
the
youn
g (M
OD
Y)G
esta
tiona
l dia
bete
s m
ellit
usC
2B.
L180
9Im
pair
ed g
luco
se t
ole
rance
C35
0N
/AN
ew t
erm
req
ues
ted f
rom
NH
S In
form
ation A
uth
ori
tyIm
pair
ed f
ast
ing g
lyca
emia
C35
1N
/AN
ew t
erm
req
ues
ted f
rom
NH
S In
form
ation A
uth
ori
tyD
iabe
tes
mel
litus
with
ket
oaci
dosi
sC
24.
C10
1.H
yper
osm
olar
non
-ket
otic
sta
te
N/A
C10
9Kin
type
2 d
iabe
tes
mel
litus
Hypogly
caem
ic s
tate
in
N/A
N/A
New
ter
m r
eques
ted f
rom
NH
S dia
bet
esIn
form
ation A
uth
ori
ty
Com
plic
ations
of
dia
bet
es:
Ischa
emic
hea
rt di
seas
eA
cute
myo
card
ial i
nfar
ctio
nG
41.
G30
..A
ngin
a pe
ctor
isG
44.
G33
..U
se c
hild
term
if m
ore
deta
il kn
own
Hyp
erlip
idae
mia
Hyp
erlip
idae
mia
NO
SC
524
C32
4.Fa
mili
al h
yper
chol
este
rola
emia
C52
5C
3200
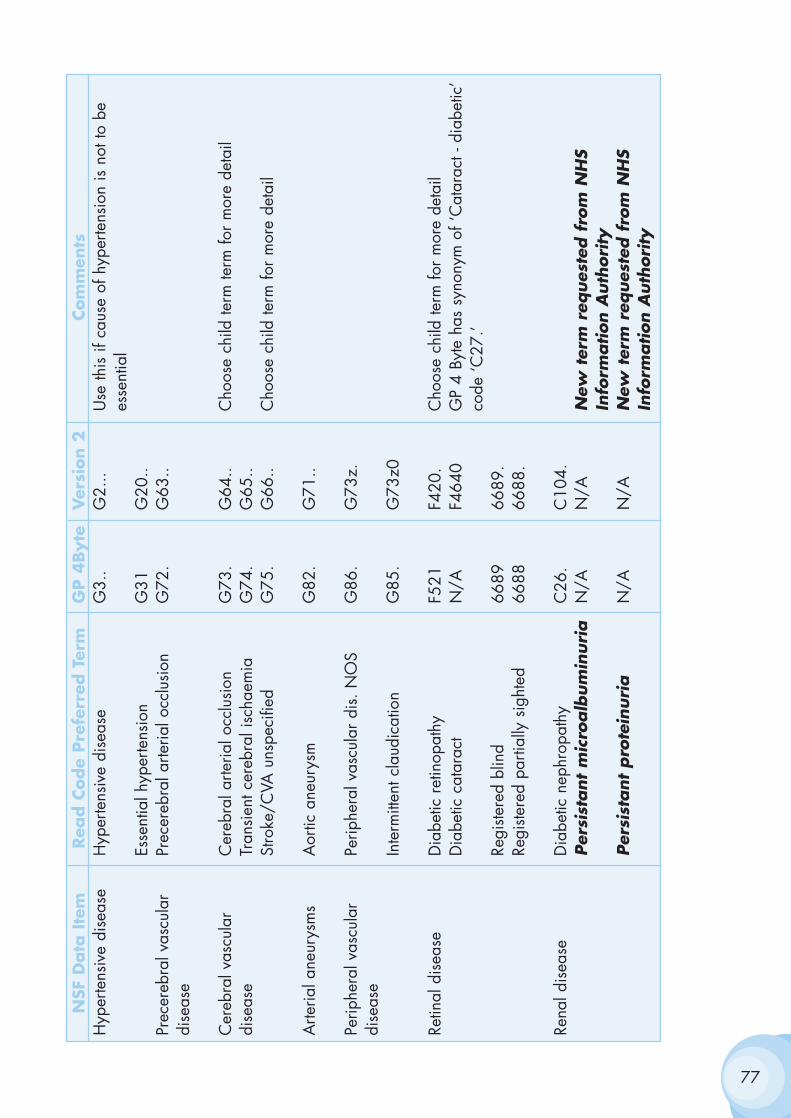
77
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsH
yper
tens
ive
dise
ase
Hyp
erte
nsiv
e di
seas
eG
3..
G2.
..U
se th
is if
cau
se o
f hyp
erte
nsio
n is
not
to b
e es
sent
ial
Esse
ntia
l hyp
erte
nsio
nG
31G
20..
Prec
ereb
ral v
ascu
lar
Prec
ereb
ral a
rteria
l occ
lusi
onG
72.
G63
..di
seas
e
Cer
ebra
l vas
cula
r C
ereb
ral a
rteria
l occ
lusi
onG
73.
G64
..C
hoos
e ch
ild te
rm te
rm fo
r m
ore
deta
ildi
seas
eTr
ansi
ent c
ereb
ral i
scha
emia
G74
.G
65..
Stro
ke/C
VA u
nspe
cifie
dG
75.
G66
..C
hoos
e ch
ild te
rm fo
r m
ore
deta
il
Arte
rial a
neur
ysm
sA
ortic
ane
urys
mG
82.
G71
..
Perip
hera
l vas
cula
r Pe
riphe
ral v
ascu
lar
dis.
NO
SG
86.
G73
z.di
seas
eIn
term
itten
t cla
udic
atio
nG
85.
G73
z0
Retin
al d
isea
seD
iabe
tic r
etin
opat
hyF5
21F4
20.
Cho
ose
child
term
for
mor
e de
tail
Dia
betic
cat
arac
tN
/AF4
640
GP
4 By
te h
as s
ynon
ym o
f ‘C
atar
act -
dia
betic
’co
de ‘C
27.’
Regi
stere
d bl
ind
6689
6689
.Re
giste
red
parti
ally
sig
hted
6688
6688
.
Rena
l dis
ease
Dia
betic
nep
hrop
athy
C26
.C
104.
Per
sist
ant
mic
roalb
um
inuri
aN
/AN
/AN
ew t
erm
req
ues
ted f
rom
NH
S In
form
ation A
uth
ori
tyPer
sist
ant
pro
tein
uri
aN
/AN
/AN
ew t
erm
req
ues
ted f
rom
NH
S In
form
ation A
uth
ori
ty
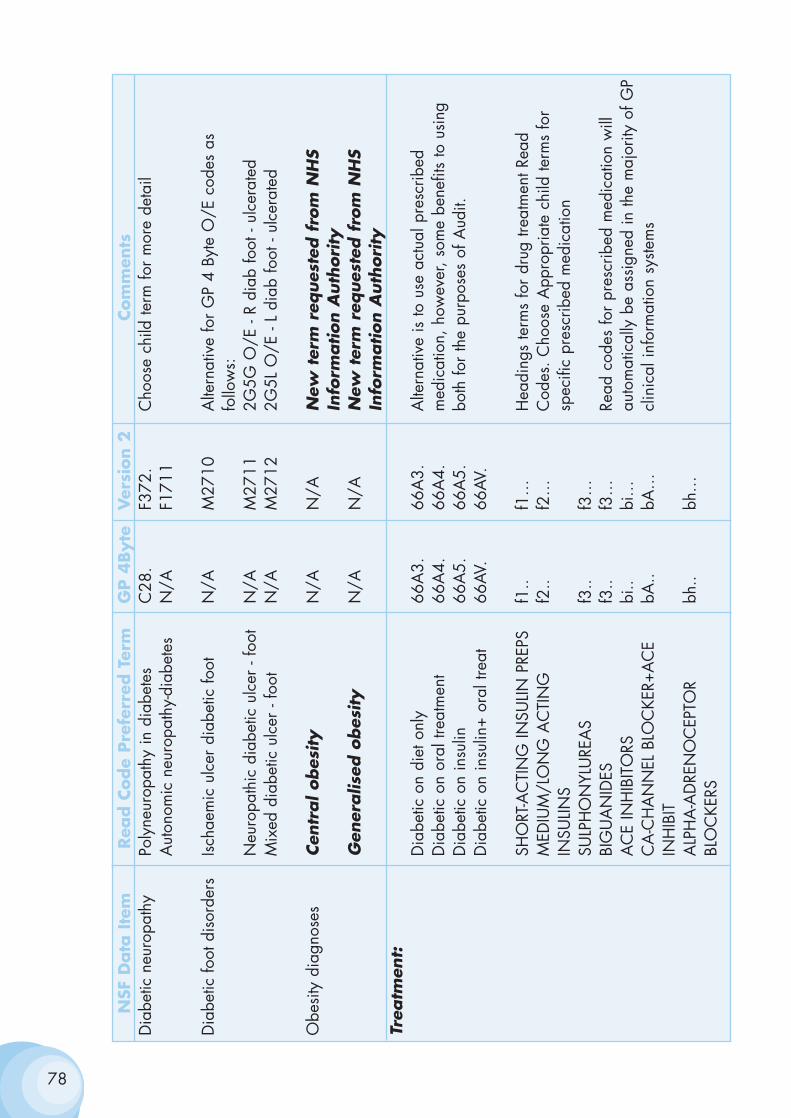
78
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsD
iabe
tic n
euro
path
yPo
lyne
urop
athy
in d
iabe
tes
C28
.F3
72.
Cho
ose
child
term
for
mor
e de
tail
Aut
onom
ic n
euro
path
y-di
abet
esN
/AF1
711
Dia
betic
foot
dis
orde
rsIsc
haem
ic u
lcer
dia
betic
foot
N/A
M27
10A
ltern
ativ
e fo
r G
P 4
Byte
O/E
cod
es a
s fo
llow
s:N
euro
path
ic d
iabe
tic u
lcer
- fo
otN
/AM
2711
2G5G
O/E
- R
diab
foot
- ul
cera
ted
Mix
ed d
iabe
tic u
lcer
- fo
otN
/AM
2712
2G5L
O/E
- L
diab
foot
- ul
cera
ted
Obe
sity
dia
gnos
esCen
tral obes
ity
N/A
N/A
New
ter
m r
eques
ted f
rom
NH
S In
form
ation A
uth
ori
tyG
ener
alis
ed o
bes
ity
N/A
N/A
New
ter
m r
eques
ted f
rom
NH
SIn
form
ation A
uth
ori
tyTr
eatm
ent:
Dia
betic
on
diet
onl
y66
A3.
66A
3.A
ltern
ativ
e is
to u
se a
ctua
l pre
scrib
ed
Dia
betic
on
oral
trea
tmen
t66
A4.
66A
4.m
edic
atio
n, h
owev
er, s
ome
bene
fits
to u
sing
D
iabe
tic o
n in
sulin
66A
5.66
A5.
both
for
the
purp
oses
of A
udit.
Dia
betic
on
insu
lin+
oral
trea
t66
AV.
66AV
.
SHO
RT-A
CTI
NG
INSU
LIN P
REPS
f1..
f1…
Hea
ding
s te
rms
for
drug
trea
tmen
t Rea
d M
EDIU
M/L
ON
G A
CTI
NG
f2
..f2
…C
odes
. Cho
ose
App
ropr
iate
chi
ld te
rms
for
INSU
LINS
spec
ific
pres
crib
ed m
edic
atio
nSU
LPH
ON
YLU
REA
Sf3
..f3
…BI
GU
AN
IDES
f3..
f3…
Read
cod
es fo
r pr
escr
ibed
med
icat
ion
will
A
CE
INH
IBIT
ORS
bi..
bi…
auto
mat
ical
ly b
e as
sign
ed in
the
maj
ority
of G
P C
A-C
HA
NN
EL B
LOC
KER+
AC
E bA
..bA
…cl
inic
al in
form
atio
n sy
stem
sIN
HIB
ITA
LPH
A-A
DRE
NO
CEP
TOR
bh..
bh…
BLO
CKE
RS
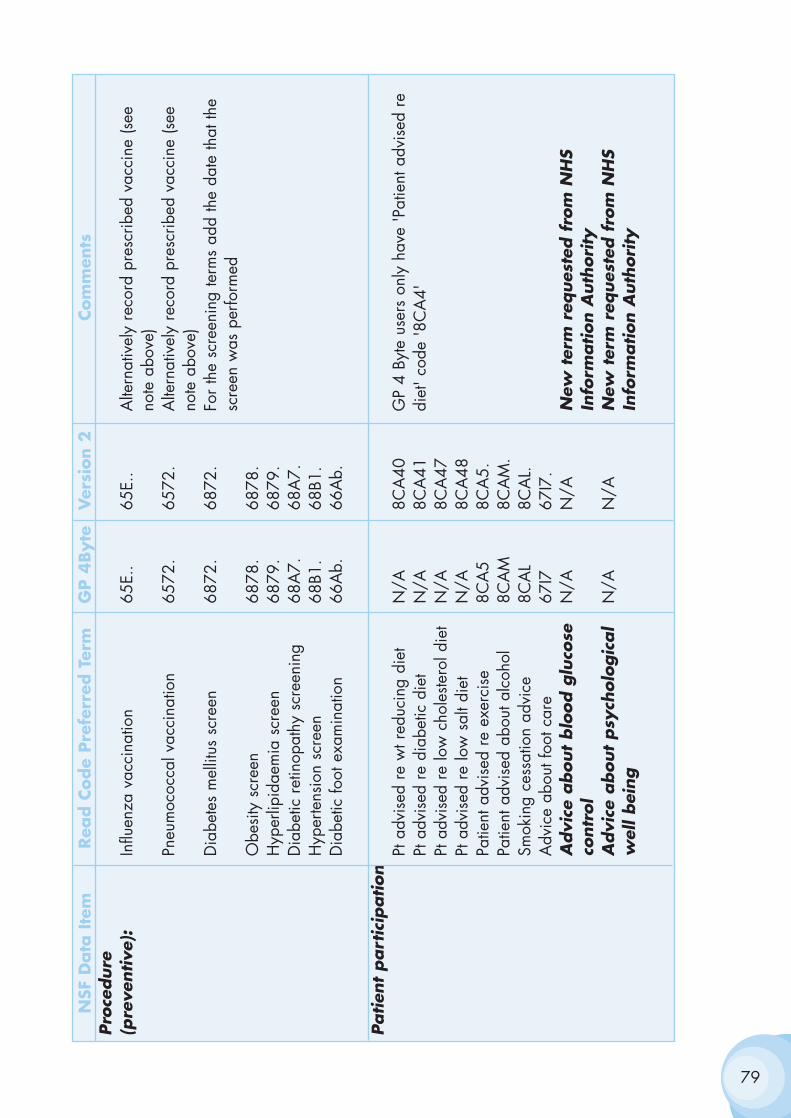
79
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsPro
cedure
(p
reve
ntive
):In
fluen
za v
acci
natio
n65
E..
65E.
.A
ltern
ativ
ely
reco
rd p
resc
ribed
vac
cine
(see
no
te a
bove
)Pn
eum
ococ
cal v
acci
natio
n65
72.
6572
.A
ltern
ativ
ely
reco
rd p
resc
ribed
vac
cine
(see
no
te a
bove
)D
iabe
tes
mel
litus
scr
een
6872
.68
72.
For
the
scre
enin
g te
rms
add
the
date
that
the
scre
en w
as p
erfo
rmed
Obe
sity
scr
een
6878
.68
78.
Hyp
erlip
idae
mia
scr
een
6879
.68
79.
Dia
betic
ret
inop
athy
scr
eeni
ng68
A7.
68A
7.H
yper
tens
ion
scre
en68
B1.
68B1
.D
iabe
tic fo
ot e
xam
inat
ion
66A
b.66
Ab.
Patien
t part
icip
ation
Pt a
dvis
ed r
e w
t red
ucin
g di
etN
/A8C
A40
GP
4 By
te u
sers
onl
y ha
ve 'P
atie
nt a
dvis
ed r
e Pt
adv
ised
re
diab
etic
die
tN
/A8C
A41
diet
' cod
e '8
CA
4'Pt
adv
ised
re
low
cho
leste
rol d
iet
N/A
8CA
47Pt
adv
ised
re
low
sal
t die
tN
/A8C
A48
Patie
nt a
dvis
ed r
e ex
erci
se8C
A5
8CA
5.Pa
tient
adv
ised
abo
ut a
lcoh
ol8C
AM
8CA
M.
Smok
ing
cess
atio
n ad
vice
8CA
L8C
AL.
Adv
ice
abou
t foo
t car
e67
I767
I7.
Advi
ce a
bout
blo
od g
luco
se
N/A
N/A
New
ter
m r
eques
ted f
rom
NH
S co
ntr
ol
Info
rmation A
uth
ori
tyA
dvi
ce a
bout
psy
cholo
gic
al
N/A
N/A
New
ter
m r
eques
ted f
rom
NH
Sw
ell bei
ng
Info
rmation A
uth
ori
ty
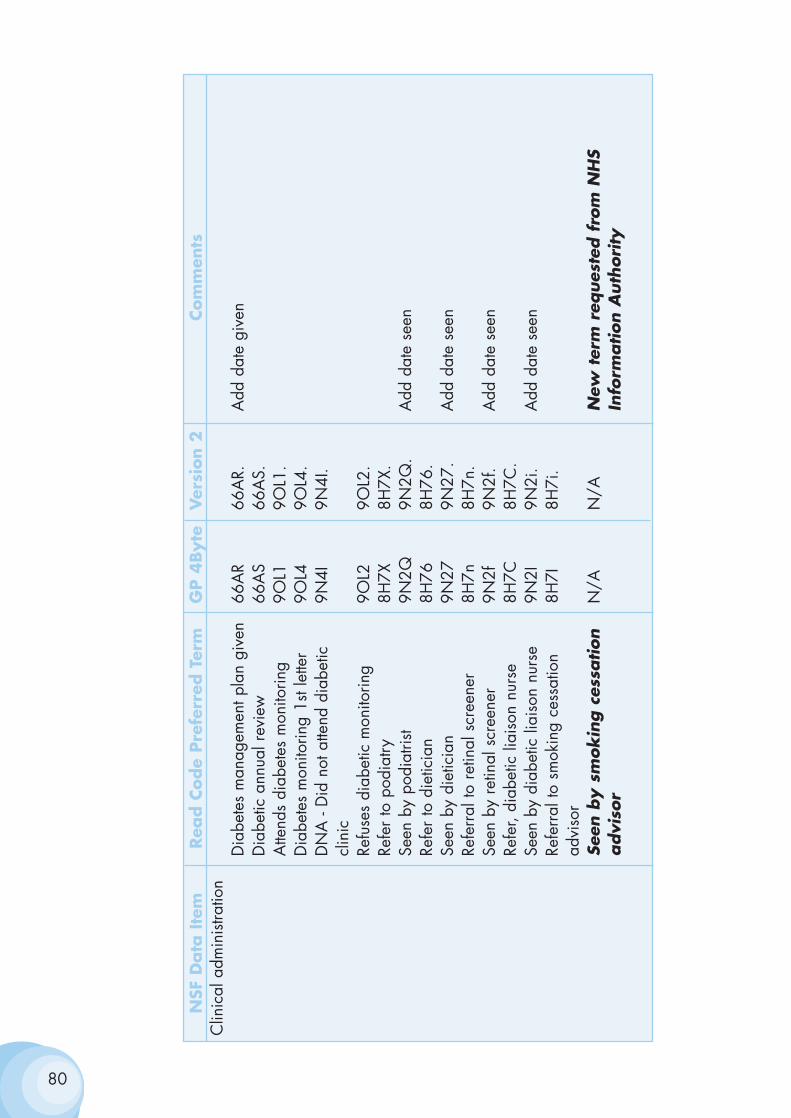
80
NSF
Data
Ite
mRea
d C
ode
Pre
ferr
ed T
erm
GP 4
Byte
Ver
sion 2
Com
men
tsC
linic
al a
dmin
istra
tion
Dia
bete
s m
anag
emen
t pla
n gi
ven
66A
R66
AR.
Add
dat
e gi
ven
Dia
betic
ann
ual r
evie
w66
AS
66A
S.A
ttend
s di
abet
es m
onito
ring
9OL1
9OL1
.D
iabe
tes
mon
itorin
g 1s
t let
ter
9OL4
9OL4
.D
NA
- D
id n
ot a
ttend
dia
betic
9N
4I9N
4I.
clin
icRe
fuse
s di
abet
ic m
onito
ring
9OL2
9OL2
.Re
fer
to p
odia
try8H
7X8H
7X.
Seen
by
podi
atris
t9N
2Q9N
2Q.
Add
dat
e se
enRe
fer
to d
ietic
ian
8H76
8H76
.Se
en b
y di
etic
ian
9N27
9N27
.A
dd d
ate
seen
Refe
rral
to r
etin
al s
cree
ner
8H7n
8H7n
.Se
en b
y re
tinal
scr
eene
r9N
2f9N
2f.
Add
dat
e se
enRe
fer,
diab
etic
liai
son
nurs
e8H
7C8H
7C.
Seen
by
diab
etic
liai
son
nurs
e9N
2I9N
2i.
Add
dat
e se
enRe
ferr
al to
sm
okin
g ce
ssat
ion
8H7I
8H7i
.ad
viso
rSe
en b
y s
mok
ing c
essa
tion
N/A
N/A
New
ter
m r
eques
ted f
rom
NH
S advi
sor
Info
rmation A
uth
ori
ty
Annex 3
Health Promotion Activity To Prevent Diabetes
Recommended activity
Obesity and physical inactivity are major risk factors for Type 2 diabetes.There is also clear evidence that individuals who have impaired glucosetolerance can reduce their risk of developing Type 2 diabetes if they eat abalanced diet, lose weight and increase their physical activity levels.
Promoting healthy eating and physical activity
A number of Welsh Assembly Government initiatives are currently beingimplemented to encourage a healthier diet and increase physical activitylevels:
• The "Food and Well Being" strategy and action plan, developed incollaboration by the Food Standards Agency Wales and the WelshAssembly Government, was launched on 13 February 2003. Thedocument outlines the actions required by key players to improve thediet of all people in Wales, but particularly those groups most likelyto be affected by inequalities in diet and health. Seminars tosupport the implementation of the strategy are being held in May 2003.
• The Community Food initiative launched in October 2000 (smallgrants scheme for projects that actively promote healthy eatingamong disadvantaged and vulnerable groups).
• Action to improve the nutrition of school-aged children through theWelsh Network of Healthy School Schemes, including fruit tuck shopschemes and breakfast clubs.
• Implementation of the Assembly Government’s Healthy LifestylesAction Plan, which aims to increase levels of physical activity inWales. The public consultation on the Action Plan ended on 31 January 2003, and the final version will be launched in latespring 2003.
81
• Development and distribution to all primary schools in Wales of "TheClass Moves!", an educational resource which provides aprogramme to enable children and teachers to discover thepleasures of movement and the benefits of relaxation.
• Inequalities in Health Fund (IHF) projects with a healthy eatingand/or physical activity component. (IHF funding is currentlytargeted at reducing coronary heart disease, but CHD preventioninitiatives also address diabetes and cancer prevention aims).
Smoking prevention and cessation
As well as increasing the risk of heart disease and lung and other cancers,smoking greatly increases the risk of developing complications fromdiabetes. The Welsh Assembly Government has a comprehensive nationalsmoking prevention and cessation programme in place. Current activitytargeted at discouraging young people from smoking includes:
• development and distribution of new education materials ontobacco for primary school children
• support for Smokebugs clubs for primary school children
• participation by Welsh schools in the Smoke-Free Class Competition
• development of Tobacco Action Groups in secondary schools.
Action being taken by the Assembly to help smokers who want to give upincludes:
• Continuing support for local smoking cessation services
• Smoking cessation training for primary care professionals
• Piloting adolescent smoking cessation projects
• Provision of a smokers’ helpline, and a mass media campaign topromote awareness of the helpline.
82
Annex 4
Summary of Market Research Wales FocusGroup
When looked at as a set of Standards, they were generally very wellreceived by both users and providers. Many participating in the research,especially users, found them quite hard to grasp as a document, however,and most of the issues arising emerged from the general discussion aroundtheir views of the service rather than the Standards themselves (even thoughthese issues were linked to the Standards).
The main priorities for action agreed by both providers and users alike wereStandards 1 and 2. Even though the whole set of 12 Standards were allperceived as being vital to the care of people with diabetes, Standards 1and 2 were viewed as the most important as it is these two that will be mostbeneficial in terms of identifying and controlling the condition. The two issuesof identification and prevention, need to be achieved through:
• raising awareness
• educating health professionals, people with diabetes and thegeneral public
• patient empowerment
• regular checks of high risk groups
• screening of people with diabetes for long-term complications.
The following were perceived as being the next most important priorities:
• the transition of adolescents from paediatric to adult care
• the standardisation of service across Wales
• the integration of primary and secondary care
• the surveillance of long-term complications
In addition to the above, some views on gaps to current service provisionwere very group specific, particularly the language and culture barriers to
83

service cited by ethnic minorities. Both providers and ethnic minorities withdiabetes thought they were receiving very sub-standard care whencompared to the rest of the population.
Other than the ethnic communities, the overall current level of service wasperceived to be very good, especially the service given by DiabeticSpecialist Nurses. Users, as well as providers, felt the Standards werealready being striven for in the service they were receiving, even though theyhad not been previously formalised, and the reasons they were not beingachieved linked to the lack of resources (staff) and funding. In order for theStandards to be achieved successfully both users and providers felt thatadditional staff resources and funding had to be provided, and that theachievement of the Standards would have to be carefully monitored(therefore requiring the appropriate procedures to be put in place).
84
Annex 5
Summary of Report - Training and EducationSub-Group
AIM
The aim of the group was to advise the Implementation Group and WelshAssembly on training and education issues for health care professionalsrelating to the implementation of the Diabetes National Service Frameworkin Wales.
The group was multi-professional with representation from primary andsecondary care, PAMS, academic establishments, people with diabetes,voluntary sector and representatives from departments within the WelshAssembly. Three meetings were held and members of the group alsoarranged an additional meeting at Llangammarch Wells. It was identifiedthat priority must be given to a structured education plan, which involves allhealth care professionals involved with diabetes care particularly those inprimary care.
Key Recommendations
1. Establish a Diabetes Education Steering Group.
The Welsh School of Medicine would appear to be the most likely focal pointof this group although representation from primary care health professionalswill be vital.
2. Wales should be independent in training.
At present, for most educational courses in diabetes, individuals in Walesare required to access courses in England. For the delivery of a Welsh NSFit is vital that a Welsh educational framework is in existence.
3. Further education needs to be patient centred and take into account theexperiences of people with diabetes in Wales.
4. If education is to take advantage of potential partnerships with thepharmaceutical industry clear guidelines must be established by theAssembly and made widely available. This would overcome the existinguncertainty and confusion.
85

5. It is unlikely that any one course or type of delivery will suit all groupsof health care professionals. Consideration must be given to bothmultidisciplinary and more traditional uni-professional courses. Coursedelivery must examine the potential benefits of residential, satellite anddistance learning. The needs of different professional groups and differentlocalities will need to be addressed.
86
Annex 6
Summary of Report – Patient and Educationand Support Sub-Group
Introduction
The Implementation Group identified patient education and support as animportant aspect to be considered for the delivery of the Diabetes NationalService Framework.
Aim
To advise the Implementation Group and Welsh Assembly on patienteducation and support issues relating to the implementation of the DiabetesNational Service Framework in Wales.
Objectives
• To develop a menu for patient education, and support and establishmethods of clinical, emotional and psychological supportprofessional that will underpin the Delivery Strategy.
• To advise on the use of any available monies for patient training andeducation in the area of diabetes in 2003/04 as part of the statedphased approach to the delivery of the Diabetes NSF in Wales.
• To comment on patient education and issues arising out of theStandards document.
• To assist the Audit Commission commissioned to carry out thebaseline review in Wales.
• To establish guidelines for the working relationship between theNHS and pharmaceutical industry that can be used by thoseworking to develop patient training and education and supportstrategies as part of the implementation of the NSF.
87
• To communicate back to the Implementation Group and otherrelevant groups. The Chair to deliver a final report to theImplementation Group with recommendations for theimplementation of the NSF.
• To consider hard to reach groups, and develop strategies for raisingawareness with the public, professionals and people with diabetes.
Membership
Membership was multi-disciplinary and included people with diabetes andcarers.
It was also geographically spread to reflect the needs of all parts of Wales.Membership included relevant members of the Implementation Group andInternal Reference Group in the Assembly.
Issues
• What models of education are available: which are the best onesand how can people be directed to the best ones.
• Working with the pharmaceutical industry.
Diabetes is a life-long condition that will have impact on every part of aperson with diabetes’ life, therefore it is vitally important that people withdiabetes have access to a structured education programme that is culturallyappropriate and individualised.
Self-management of diabetes is the cornerstone of diabetes care and this willreduce the risks of the associated complications of diabetes, which areknown to reduce life expectancy and quality of life.
Recommendations:
1. Patient Education
All people with diabetes should receive a structured and ongoingprogramme of education that is language and culturally appropriate and isindividualised. This needs to be multi-disciplinary and based on local needs.
88
2. Education for Children
Children to have access to:
• professional education programmes which will include support forteachers and nurses.
• psychology and/or counselling service.
• 24-hour helpline for children and families with diabetes.
• appropriate literature that is standardised and consistent.
3. Funding
Education must be resourced, evaluated and monitored. Local HealthBoards will need to allocate money for this.
Some initiatives they could spend it on are:
• Raising awareness of the risk factors and those people who are ata higher risk of developing diabetes.
• Support and self-management programmes such as the Peer SupportProgramme (Merthyr LHG) Chronic Disease Self-ManagementProgramme, 3D Programme (Diabetes UK Scheme for NewlyDiagnosed).
4. Residential/Nursing Homes
• Training issues will need to be addressed by the Care StandardsInspectorate. Social Services need to be involved in the training.All people with diabetes in residential/nursing homes should haveequitable access to services.
5. Patient held records
• People with diabetes should be involved in the design of theserecords and they will need to be piloted in Wales. Patient heldrecords should be integrated with IT.
89
6. Patient/Public Involvement
• Patient involvement needs to be targeted at as wide an audience ofpeople with diabetes as soon as possible.
• LDSAG needs to be associated with the Local Health Board.
• Patient involvement must be properly resourced.
• Annual review of public/patient involvement to be sent to WelshAssembly Government.
• People with diabetes should be involved in the planning of diabetesservices.
7. Working with the Pharmaceutical Industry
• The Welsh Assembly Government needs to issue guidelines to LHBs.
• Any literature produced should involve people with diabetes in itsdesign and also involve RNIB, Diabetes UK, Wales Council for theBlind and British Heart Foundation.
8. Clinical, emotional and psychological support
• All people with diabetes should have access to psychology and/orcounselling service.
• All people with diabetes should have access to intensive educationprogrammes, peer support, chronic disease managementprogrammes and voluntary organisations.
Patient education, support and empowerment programmes should includehard to reach groups. Strategies for raising the awareness of diabetes issuesto the public, professionals and people with diabetes should be developed.
9. Hard to reach groups
• Education needs to be provided to minority ethnic communities in anappropriate language and taking into account their religious andcultural needs.
90
• People who develop sight problems as a result of their diabetesneed to have access to information that is provided in appropriatesize of font and access to mobility training and social services.
• All people with diabetes who are in prisons need equal access todiabetes services and education.
10. Health Promotion
• The sub-group felt that Health Promotion should raise awareness ofrisk factors and prevention.
• The group felt that a further sub group needed to be set up to takethis issue forward.
Conclusion
Patient education and support services should be a key deliverable of thediabetes NSF and in order for this to be achievable dedicated long termfunding will need to be available.
91
Annex 7
Summary of the ‘Having Your Say’ ConferenceReport
This conference took place in September 2002 in Llandrindod Wells, andgave people living with diabetes from across Wales a chance to voice theirviews on diabetes services.
The National Service Framework is a 10-year plan, and all at the conferencewere aware that changes and developments take time and investment.People living with diabetes grasped the opportunity provided by theconference to have their say, and to welcome developments to date andshowed they were keen to contribute to future developments in Wales.
Delegates expressed the hope that the Diabetes NSF Project Board set up bythe Welsh Assembly Government will support a delivery strategy that putspeople with diabetes at the centre of services. It was agreed that theimplementation services that support the NSF standards would improve thecare of people with diabetes at a time when more people are beingdiagnosed every week in Wales.
There is a great deal of support and interest amongst people living withdiabetes in the NSF and an enthusiasm for the potential development of apatient centred, modern service where people living with diabetes receiveevidence based care from knowledgeable, supportive health careprofessionals and through which they can access the support of voluntaryorganisations (when they need it).
The conference delegates wanted to see clear action in the areas of:
• Education and training for healthcare professionals and peopleliving with diabetes
• Greater awareness of diabetes and diabetes services amongsthealthcare managers/planners and politicians
• User involvement in planning
• Information about local voluntary groups/Diabetes UK and thesupport they can provide.
The full report and all action points are available on www.wales.gov.uk. 92
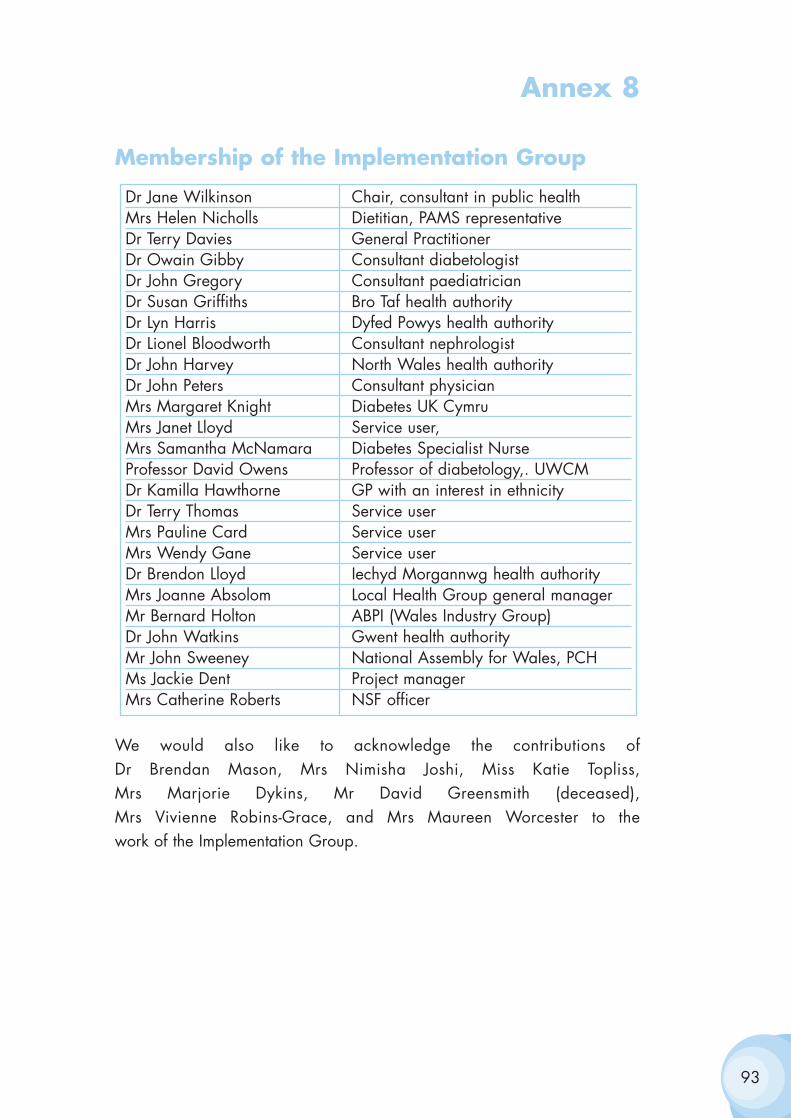
Annex 8
Membership of the Implementation Group
We would also like to acknowledge the contributions of Dr Brendan Mason, Mrs Nimisha Joshi, Miss Katie Topliss, Mrs Marjorie Dykins, Mr David Greensmith (deceased), Mrs Vivienne Robins-Grace, and Mrs Maureen Worcester to the work of the Implementation Group.
93
Dr Jane Wilkinson Chair, consultant in public healthMrs Helen Nicholls Dietitian, PAMS representativeDr Terry Davies General PractitionerDr Owain Gibby Consultant diabetologistDr John Gregory Consultant paediatricianDr Susan Griffiths Bro Taf health authorityDr Lyn Harris Dyfed Powys health authorityDr Lionel Bloodworth Consultant nephrologistDr John Harvey North Wales health authorityDr John Peters Consultant physicianMrs Margaret Knight Diabetes UK CymruMrs Janet Lloyd Service user, Mrs Samantha McNamara Diabetes Specialist NurseProfessor David Owens Professor of diabetology,. UWCMDr Kamilla Hawthorne GP with an interest in ethnicityDr Terry Thomas Service userMrs Pauline Card Service userMrs Wendy Gane Service userDr Brendon Lloyd Iechyd Morgannwg health authorityMrs Joanne Absolom Local Health Group general managerMr Bernard Holton ABPI (Wales Industry Group)Dr John Watkins Gwent health authorityMr John Sweeney National Assembly for Wales, PCHMs Jackie Dent Project managerMrs Catherine Roberts NSF officer
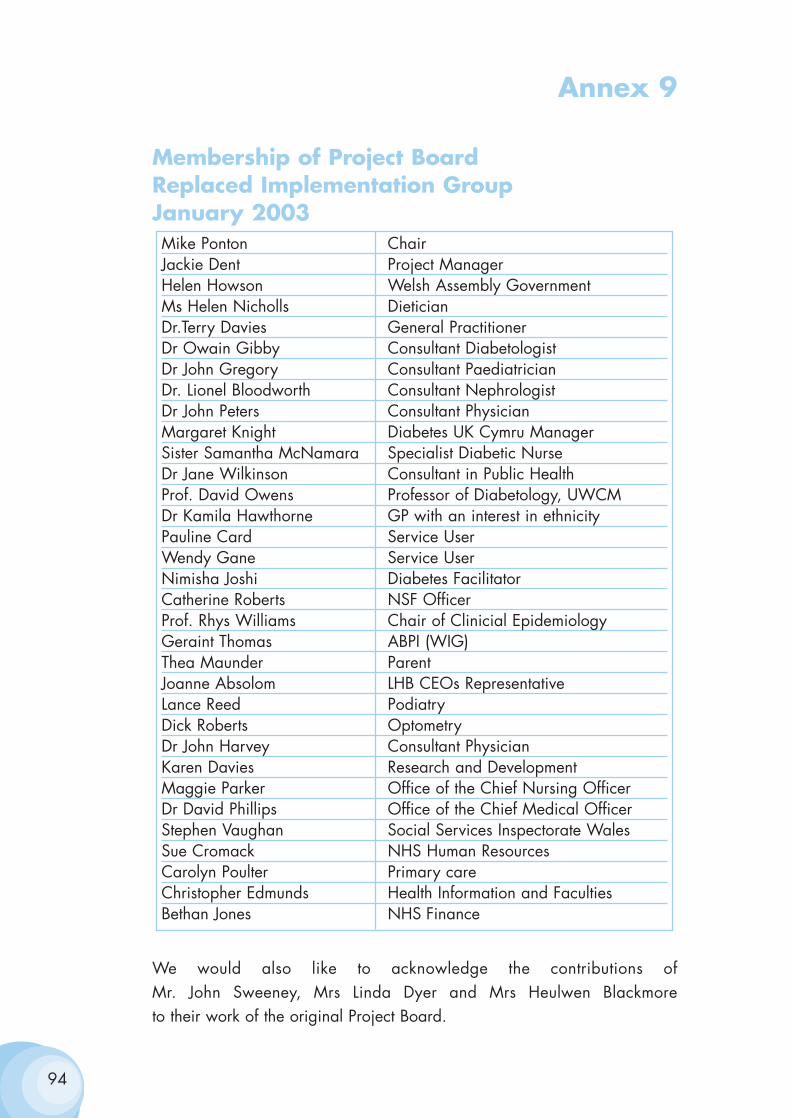
Annex 9
Membership of Project Board Replaced Implementation Group January 2003
We would also like to acknowledge the contributions of Mr. John Sweeney, Mrs Linda Dyer and Mrs Heulwen Blackmore to their work of the original Project Board.
94
Mike Ponton ChairJackie Dent Project ManagerHelen Howson Welsh Assembly GovernmentMs Helen Nicholls DieticianDr.Terry Davies General PractitionerDr Owain Gibby Consultant DiabetologistDr John Gregory Consultant PaediatricianDr. Lionel Bloodworth Consultant NephrologistDr John Peters Consultant PhysicianMargaret Knight Diabetes UK Cymru ManagerSister Samantha McNamara Specialist Diabetic NurseDr Jane Wilkinson Consultant in Public HealthProf. David Owens Professor of Diabetology, UWCMDr Kamila Hawthorne GP with an interest in ethnicityPauline Card Service UserWendy Gane Service UserNimisha Joshi Diabetes FacilitatorCatherine Roberts NSF OfficerProf. Rhys Williams Chair of Clinicial EpidemiologyGeraint Thomas ABPI (WIG)Thea Maunder ParentJoanne Absolom LHB CEOs RepresentativeLance Reed PodiatryDick Roberts OptometryDr John Harvey Consultant PhysicianKaren Davies Research and DevelopmentMaggie Parker Office of the Chief Nursing OfficerDr David Phillips Office of the Chief Medical OfficerStephen Vaughan Social Services Inspectorate WalesSue Cromack NHS Human ResourcesCarolyn Poulter Primary careChristopher Edmunds Health Information and FacultiesBethan Jones NHS Finance
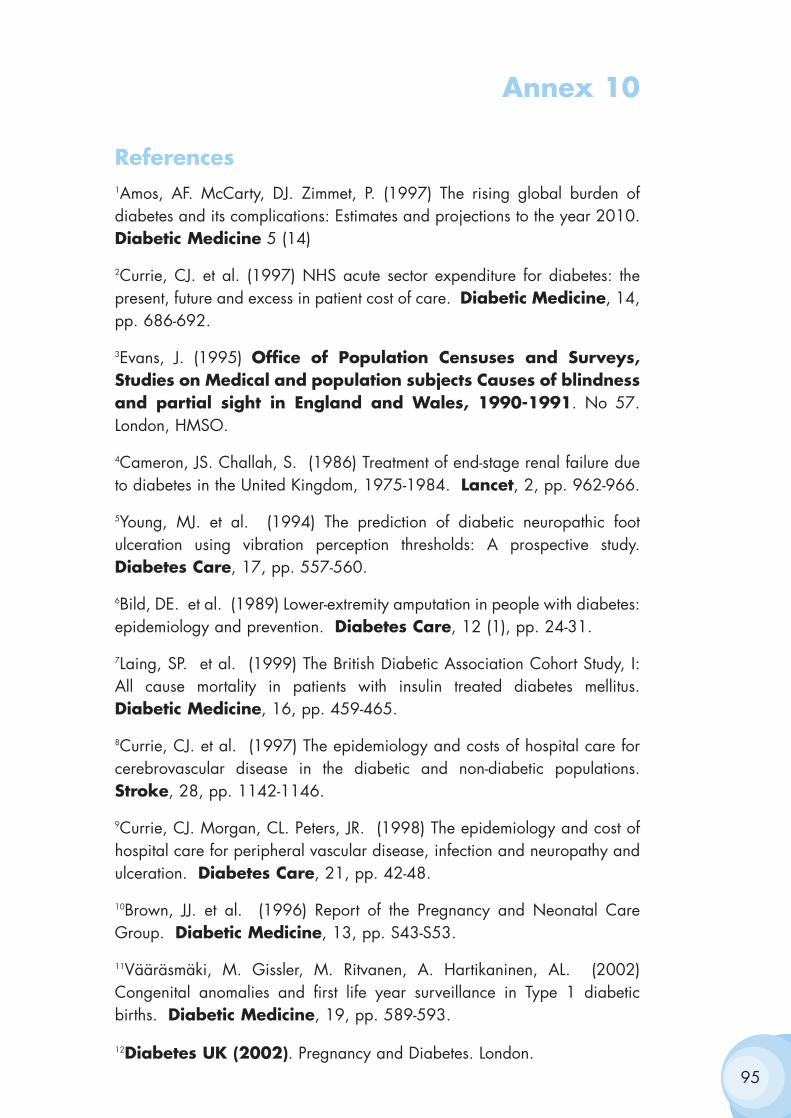
Annex 10
References1Amos, AF. McCarty, DJ. Zimmet, P. (1997) The rising global burden ofdiabetes and its complications: Estimates and projections to the year 2010.Diabetic Medicine 5 (14)
2Currie, CJ. et al. (1997) NHS acute sector expenditure for diabetes: thepresent, future and excess in patient cost of care. Diabetic Medicine, 14,pp. 686-692.
3Evans, J. (1995) Office of Population Censuses and Surveys,Studies on Medical and population subjects Causes of blindnessand partial sight in England and Wales, 1990-1991. No 57.London, HMSO.
4Cameron, JS. Challah, S. (1986) Treatment of end-stage renal failure dueto diabetes in the United Kingdom, 1975-1984. Lancet, 2, pp. 962-966.
5Young, MJ. et al. (1994) The prediction of diabetic neuropathic footulceration using vibration perception thresholds: A prospective study.Diabetes Care, 17, pp. 557-560.
6Bild, DE. et al. (1989) Lower-extremity amputation in people with diabetes:epidemiology and prevention. Diabetes Care, 12 (1), pp. 24-31.
7Laing, SP. et al. (1999) The British Diabetic Association Cohort Study, I:All cause mortality in patients with insulin treated diabetes mellitus.Diabetic Medicine, 16, pp. 459-465.
8Currie, CJ. et al. (1997) The epidemiology and costs of hospital care forcerebrovascular disease in the diabetic and non-diabetic populations.Stroke, 28, pp. 1142-1146.
9Currie, CJ. Morgan, CL. Peters, JR. (1998) The epidemiology and cost ofhospital care for peripheral vascular disease, infection and neuropathy andulceration. Diabetes Care, 21, pp. 42-48.
10Brown, JJ. et al. (1996) Report of the Pregnancy and Neonatal CareGroup. Diabetic Medicine, 13, pp. S43-S53.
11Vääräsmäki, M. Gissler, M. Ritvanen, A. Hartikaninen, AL. (2002)Congenital anomalies and first life year surveillance in Type 1 diabeticbirths. Diabetic Medicine, 19, pp. 589-593.
12Diabetes UK (2002). Pregnancy and Diabetes. London. 95
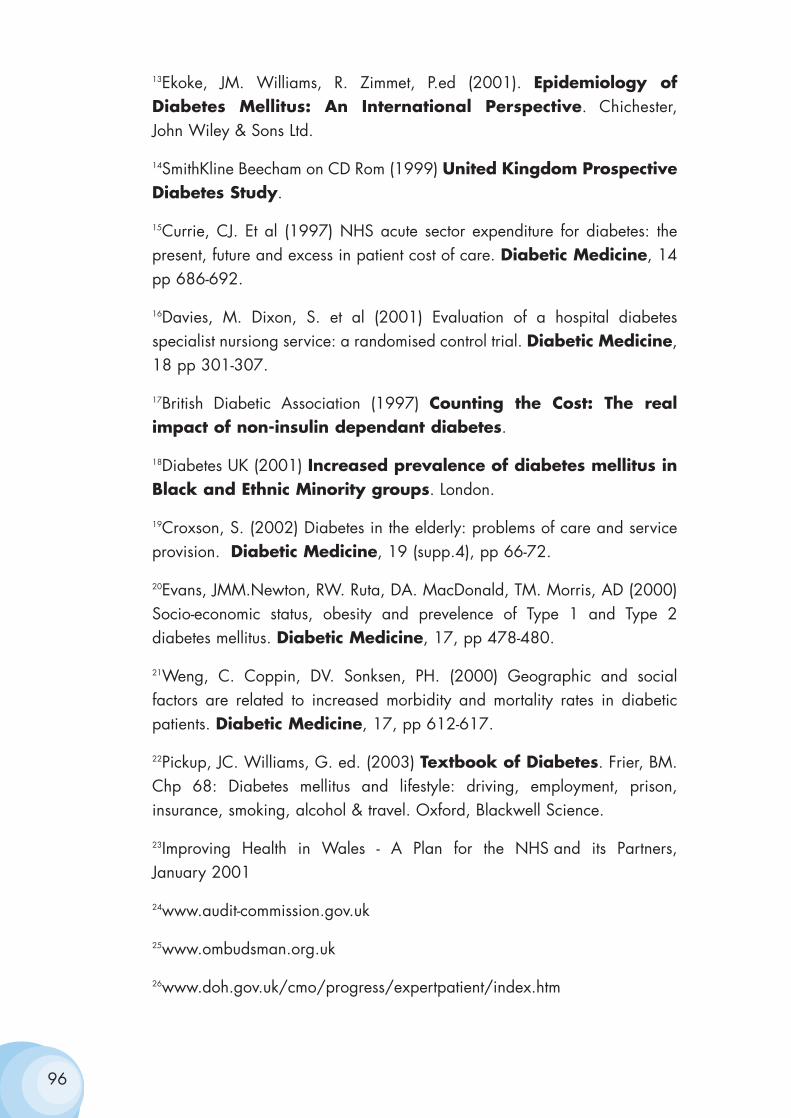
13Ekoke, JM. Williams, R. Zimmet, P.ed (2001). Epidemiology ofDiabetes Mellitus: An International Perspective. Chichester, John Wiley & Sons Ltd.
14SmithKline Beecham on CD Rom (1999) United Kingdom ProspectiveDiabetes Study.
15Currie, CJ. Et al (1997) NHS acute sector expenditure for diabetes: thepresent, future and excess in patient cost of care. Diabetic Medicine, 14pp 686-692.
16Davies, M. Dixon, S. et al (2001) Evaluation of a hospital diabetesspecialist nursiong service: a randomised control trial. Diabetic Medicine,18 pp 301-307.
17British Diabetic Association (1997) Counting the Cost: The realimpact of non-insulin dependant diabetes.
18Diabetes UK (2001) Increased prevalence of diabetes mellitus inBlack and Ethnic Minority groups. London.
19Croxson, S. (2002) Diabetes in the elderly: problems of care and serviceprovision. Diabetic Medicine, 19 (supp.4), pp 66-72.
20Evans, JMM.Newton, RW. Ruta, DA. MacDonald, TM. Morris, AD (2000)Socio-economic status, obesity and prevelence of Type 1 and Type 2diabetes mellitus. Diabetic Medicine, 17, pp 478-480.
21Weng, C. Coppin, DV. Sonksen, PH. (2000) Geographic and socialfactors are related to increased morbidity and mortality rates in diabeticpatients. Diabetic Medicine, 17, pp 612-617.
22Pickup, JC. Williams, G. ed. (2003) Textbook of Diabetes. Frier, BM.Chp 68: Diabetes mellitus and lifestyle: driving, employment, prison,insurance, smoking, alcohol & travel. Oxford, Blackwell Science.
23Improving Health in Wales - A Plan for the NHS and its Partners, January 2001
24www.audit-commission.gov.uk
25www.ombudsman.org.uk
26www.doh.gov.uk/cmo/progress/expertpatient/index.htm
96





























