Embed Size (px)
Citation preview

Diagnostic Utility of Examination of the Carotid Pulse Apex Impulse Jugular Venous Pulse
Mary Beth Fontana M.D.
Cardiovascular Medicine

Block Learning Objectives
Evaluate carotid pulse and auscultate for bruits Localize and characterize the apex impulse Identify jugular venous pulse components and assess
jugular venous pressure Describe the abnormalities of the carotid pulse, apex
impulse, and jugular venous pulse in cardiac and pericardial disease

Resources
Lilly doesn’t have specific sections on carotid pulse or apex impulse, instead describing them with some specific diagnoses.
Jugular venous pulse; Chapter 2, pp.29-30 This module summarizes the abnormalities of all 3 that
are pertinent to diagnosis

Learning Objectives
For the carotid pulse, apex impulse, jugular venous pulse be able to: Describe the normal characteristics Describe the method of examination Explain the pathophysiology causing abnormalities of
the components of each The abnormalities described are mentioned in the clinical
examination of the individual diagnoses

Carotid Pulse
Palpate between larynx and sternocleidomastoid muscle Marker of ventricular systole Rapid upstroke and slower decline

Normal Carotid Pulse
Rapid upstroke
Dicrotic notch

Abnormal Carotid Pulse
Increased volume, rapid upstrokes Sympathetic stimulation increases stroke volume and upstroke
velocity Bradycardia-larger stroke volume per beat Aortic valvular regurgitation Aging stiffens walls – flow is transmitted more rapidly which
raises systolic blood pressure and maintains the rapid upstroke

Pulsus Parvus
Reduced stroke volume Left ventricular failure Severe fixed LV outflow obstruction Blood volume depletion

Pulsus Tardus
Slow upstrokes Obstruction to flow between heart and carotid Most common is valvular aortic stenosis Turbulent flow in carotid is audible—called a BRUIT and can
cause a palpable vibration of the arterial wall – called a THRILL

Pulsus Parvus &Tardus Valvular Aortic Stenosis
Slow upstrokecarotid
ECG
Small volume

Bisferiens or Bifid Carotid
Two systolic peaks Rapid ejection of a large stroke volume as in severe aortic
valvular regurgitation. The elastic artery reverberates Initial rapid ejection followed by slow ejection in the same systole.
Seen in dynamic muscular subvalvular aortic obstruction, called hypertrophic obstructive cardiomyopathy. Only the initial spike is palpable

Bisferiens Carotid PulseAortic Regurgitation
2 systolic peaks

Bisferiens Carotid PulseHypertrophic Obstructive Cardiomyopathy
spike
dome
Dicrotic notch

Pulsus Alternans
Aortic pressure
Strong beat from larger LV diastolic volume
Weak beat from smaller LV diastolic volume
Sign of severe left ventricular failure

Paradoxical PulseSign of fluid under pressure in the pericardial space-- tamponade
inspiration15mmHg drop
Aortic pressure
Greater than 10 mmHg fall in systolic pressure with inspiration
expiration

LV Apex Impulse
Recording of the apex impulse- usually only the E is palpable
Systolic contraction of LV contacting the chest wall is palpable– the E pointA wave may be
palpable at time of S4
Rapid filling wave may be palpable at time of an S3

LV Apex Impulse
Midclavicular line 5th intercostal space in the supine and upright position
Palpable in 50% Quarter size or smaller Marker of ventricular systole Size of impulse, duration, and magnitude can be
assessed in left lateral position

Abnormal Apex
Enlarged LV - displaced toward left axilla Prominent heave- ejection of large stroke volume Sustained- Poor LV systolic function, prolongation of
ejection time from obstruction to LV outflow Double or triple apex impulses - palpable gallop(s)

Normal JVP - RA
a = atrial contraction
C=upward thrust of T valve
x =atrial relaxation, emptying
v = atrial filling with T valve closed during ventricular systole
y descent = atrial emptying in early diastole

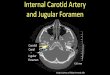
Carotid artery and internal jugular vein anatomy

JVP Examination
Elevate head 10-15 degrees to see waves and estimate pressure. If JVP visible at 45 degrees, RA pressure is abnormally high
Measure vertical distance above manubrial-sternal junction and add 5 to get RA pressure.
Time events by feeling carotid pulse on opposite side of neck; a is before carotid, v peak is after. The c is not seen
Descents are more rapid than ascents of waves
JVP normally goes down with inspiration

Elevated Jugular Venous Pressure
Increased blood volume- pregnancy, heart failure Obstruction to atrial emptying- pericardial disease,
tricuspid valve obstruction, noncompliant RV Absent wave forms- SVC obstruction Further elevation with inspiration- Kussmaul’s sign-
constrictive pericarditis

Abnormal A Wave, Attenuated Y Descent
Also seen when the RV muscle has reduced compliance
Large a wave due to stenosis of tricuspid valve
Attenuated y descent

Large V wave-tricuspid valve regurgitation
V
Y
The RA is filling from the vena cavae and from the RV during ventricular systole when the T valve should be closed. The Y descent is rapid from emptying a large volume into the RV
No a wave – loss of atrial contraction, atrial fibrillation

AV Dissociation – Cannon A waves
Atrial contraction when tricuspid valve is closed
P P
P waves and QRS’s occur independently due to complete block of conduction at the AV node
AA

RA – JVP Tamponade
20mm. Hg
Good X descent
Attenuated Y descent
Fluid under pressure in the pericardial space prevents passive ventricular filling in early diastole

JVP – RA Accentuated Y Descent Constrictive Pericarditis
y
Constriction raises RA pressure, early diastolic filling is rapid until constricting pericardium limits filling

Summary & Advice

Carotid Pulse Apex Impulse JVP Quiz

Thank you for completing this module
• I hope that I was able to teach the subject clearly.• If you have any questions, write to me:

Survey
We would appreciate your feedback on this module. Click on the button below to complete a brief survey. Your responses and comments will be shared with the module’s author, the LSI EdTech team, and LSI curriculum leaders. We will use your feedback to improve future versions of the module.
The survey is both optional and anonymous and should take less than 5 minutes to complete.
Survey





















![Cronicon OPEN ACCESS EC CLINICAL AND MEDICAL CASE … · [RSV], right internal jugular vein [RIJV], brachiocephalic arterial trunk [BCAT], left primitive carotid artery [LPCA], left](https://img.pdfslide.net/doc/110x75/60b15dff4becc74a0427c431/cronicon-open-access-ec-clinical-and-medical-case-rsv-right-internal-jugular.jpg)






