Embed Size (px)
Citation preview

Diet Behavior Change Techniquesin Type 2 Diabetes: A SystematicReview and Meta-analysisDiabetes Care 2017;40:1800–1810 | https://doi.org/10.2337/dc17-0462
OBJECTIVE
Dietary behavior is closely connected to type 2 diabetes. The purpose of this meta-analysis was to identify behavior change techniques (BCTs) and specific componentsof dietary interventions for patients with type 2 diabetes associated with changes inHbA1c and body weight.
RESEARCH DESIGN AND METHODS
The Cochrane Library, CINAHL, Embase, PubMed, PsycINFO, and Scopus databaseswere searched. Reports of randomized controlled trials published during 1975–2017that focused on changing dietary behavior were selected, and methodological rigor,use of BCTs, and fidelity and intervention features were evaluated.
RESULTS
In total, 54 studies were included, with 42 different BCTs applied and an average of7 BCTs used per study. Four BCTsd“problem solving,” “feedback on behavior,”“adding objects to the environment,” and “social comparison”dand the interven-tion feature “use of theory”were associatedwith>0.3% (3.3mmol/mol) reduction inHbA1c. Meta-analysis revealed that studies that aimed to control or change theenvironment showed a greater reduction in HbA1c of 0.5% (5.5 mmol/mol) (95%CI 20.65, 20.34), compared with 0.32% (3.5 mmol/mol) (95% CI 20.40, 20.23)for studies that aimed to change behavior. Limitations of our study were the het-erogeneity of dietary interventions and poor quality of reporting of BCTs.
CONCLUSIONS
This study provides evidence that changing the dietary environmentmay havemoreof an effect on HbA1c in adults with type 2 diabetes than changing dietary behavior.Diet interventions achieved clinically significant reductions in HbA1c, although initialreductions in body weight diminished over time. If appropriate BCTs and theory areapplied, dietary interventions may result in better glucose control.
Dietary behavior is intricately linked to type 2 diabetes and has become an increasinglycomplex phenomenon to understand and change. There is a long association betweendiet and the pathogenesis of type 2 diabetes. A recent study suggested that reducedrisk of type 2 diabetes was strongly associated with dietary factors such as greaterintake of fruit, vegetables, legumes, nuts, whole grains, and long-chain fats and a lowerintake of sugar-sweetened beverages (1), trans fat, processed/red meats, and sodiumand a moderate alcohol intake (2). Dietary factors have also been linked to the highestproportion of deaths in type 2 diabetes, stroke, and heart disease (3). There is a need toidentify factors associated with effective clinical outcomes in dietary interventions
1Physiology Department, School of Medicine,National University of Ireland Galway, Galway,Ireland2Electrical & Electronic Engineering, College ofEngineering and Informatics, National Universityof Ireland Galway, Galway, Ireland3Science Foundation of Ireland Centre for Researchin Medical Devices (CURAM), Galway, Ireland4Bariatric Medicine Service, Galway Diabetes Re-search Centre, Health Research Board ClinicalResearch Facility, Galway, Ireland5School of Health and Exercise Sciences, Facultyof Health and Social Development, The Univer-sity of British Columbia, Kelowna, British Colum-bia, Canada
Corresponding author: Leo R. Quinlan, [email protected].
Received 11March 2017 and accepted 11 August2017.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc17-0462/-/DC1.
© 2017 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
Kevin A. Cradock,1,2 Gearoid OLaighin,2,3
Francis M. Finucane,4 Rhyann McKay,5
Leo R. Quinlan,1,3 Kathleen A. Martin Ginis,5
and Heather L. Gainforth5
1800 Diabetes Care Volume 40, December 2017
META-ANALYSIS

(4–6). Identifying effective behaviorchange techniques (BCTs) in successful di-etary approaches to type 2 diabetesmanagement may help to refine andimprove the scalability of successfulapproaches to changing dietary behavior.A BCT is an observable, replicable,and irreducible component of an interven-tion designed to alter or redirect causalprocesses regulating behavior, such as“feedback” or “self-monitoring” (7). Theobjective of this systematic review andmeta-analysis was to identify dietaryBCTs, intervention features, and specificdiets associated with changes in HbA1cand body weight in type 2 diabetes.
RESEARCH DESIGN AND METHODS
This systematic review and meta-analysisfollowed a registered protocol (http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016042466). APRISMA (Preferred Reporting Items forSystematic Reviews and Meta-Analyses)checklist was created and PRISMA reviewguidelineswere followed (SupplementaryData Table S1).
Inclusion Criteria
1. Randomized controlled trials (RCTs) ofany duration using a dietary interven-tion published in peer-reviewed jour-nals between 1 January 1975 and12 April 2017 were included.
2. RCTswith a comparison armor controlgroup that constituted usual carewere included. Usual care could in-clude typical diabetes dietary treat-ment such as recommended by theAmerican Diabetes Association or car-bohydrate exchange–type diets.
3. Human participants were older than18 years of agewith clinically confirmedtype 2 diabetes at time of recruitment.
4. The primary clinical outcomemeasurewas HbA1c. However, studies report-ing HbA1c results as a secondary out-come measure were also included.
5. Randomized crossover trials were in-cluded if relevant outcome data werereported for both intervention andcontrol groups prior to subjects cross-ing over to the other diet.
Exclusion Criteria
1. RCTs of diabetes prevention or RCTs inpopulations at risk for type 2 diabetes
2. RCTs that used pharmacological agentsexclusively to treat type 2 diabetes
3. RCTs that included supervised physicalactivity
4. RCTs that targeted multiple chronicdiseases, gestational diabetes, ortype 1 diabetes
5. Studies not reported in English6. Studies that focused exclusively on
supplement or micronutrient use
Information Sources and SearchStrategyThe following databases were searchedusing a Boolean combination of keywordsandMeSH terms: Cochrane Library, CINAHL,Embase, PubMed, PsycINFO, and SCOPUS(Supplementary Data Table S2). Searchterms were developed following the pro-tocol of an earlier review (8) and using aseries of sensitivity analyses of terms,cross-checking results against identifiedreference criteria. Additional recordsidentified from other sources such as ref-erence lists of relevant reviews, studieswithmultiple intervention arms in an ear-lier review, and all included studies weresearched for additional sources. The orig-inal searchwas conducted on 22 February2016 and repeated on 12 April 2017.
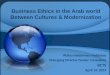
Article ScreeningArticles were initially screened by two re-search team members (K.A.C. and R.M.)based on titles and abstracts and then fulltexts of the remaining articles (see Fig. 1).A thirdmember of the review team (H.L.G.)oversaw any disagreements on search re-sults andhad thefinal sayon included stud-ies. Interrater agreement by the Cohen kfor the full-text search results was 0.82.
Article ClassificationStudies that aimed to control or change en-vironment were classified as studies whereall foodor themajorityof foodwasprovidedto participants. Studies in this categorycould also be described as studies withhigh internal validity. Studies that aimedto change behavior were classified as stud-ies where participants were instructed oreducated about diet changes by dietitiansor health care professionals; they included avariety of diets and no food was provided.Studies in this category could also be de-scribed as having high external validity.
Low-carbohydrate diets were classi-fied as studies where carbohydrate in-take of ,130 g/day was recommended(9). Low-fat diets were classified as stud-ies where dietary fat intake of,30% wasrecommended (10). High-protein dietswere classified as studies where protein
intake of.2 g/kg/daywas recommended(11).
Data Extraction ProcessData extraction was carried out by onemember of the team (K.A.C.), and rele-vant information was stored in Excel filetemplates. All data regarding HbA1c,weight loss, intervention features, BCTs,fidelity coding, and risk of bias waschecked by another member of the re-search team (R.M.). All corresponding au-thors were contacted by e-mail (wherecontact details were available, n = 50 of54) using a standardized template to re-quest additional information. The re-sponse rate was 34% (over a period of6 weeks).
Risk of Bias and Fidelity AssessmentThe Cochrane Collaboration risk of biastool was used to assess methodologicalquality (12). Assessment criteria are ap-plied to seven aspects of trials to yield anappraisal of “low risk,” “high risk,” or “un-clear risk” of bias. Studies were indepen-dently assessed by two members of thereview team for risk of bias and method-ological quality (K.A.C. and R.M.). Assess-ment results were discussed and agreedupon after the first 10 studies and againafter the first 20 studies. Interrater reli-ability was calculated and discrepancieswere discussed after each round. Treat-ment fidelity was assessed according tothe five categories proposed by Bellget al. (13). Each category and subcategorywas assigned a score of yes, no, or unclear.RCTs were independently assessed by twomembers of the review team (K.A.C. andH.L.G.) and results were discussed andassessments repeated following discus-sion of the first 10 and first 20 articles.Interrater reliability is based on the final34 studies.
Coding of Behavior ChangeTechniquesThe BCT taxonomy v1 of Michie et al. (7)was used to identify and code BCTs re-lated to diet only that were identified ineach study. A list of all 93 BCTs and theirdescriptions is available (http://www.bct-taxonomy.com) (7). A BCT was onlycoded when it was explicitly mentionedin the intervention methodology. BCTswere coded separately for interventionand control groups. A coding rubric wasdeveloped by three authors (K.A.C.,R.M., and H.L.G.) to guide the coding pro-cess (Supplementary Data Table S3). All
care.diabetesjournals.org Cradock and Associates 1801

included studies were coded indepen-dently by two authors (K.A.C. and R.M.)immediately after training in the use oftheMichie et al. taxonomy. A third mastercoder (H.L.G.) independently assessed thecoding results and arbitrated any disagree-ments. Cohen k and prevalence-adjusted
bias-adjusted k calculations were used toestablish intercoder reliability of BCTspresent and absent. A BCT must have beenused in at least three studies for inclusionin the moderator analysis (14). Bothcoders discussed coding practices and re-sults after coding the first study and again
after independently coding the remaining53 studies. All available information, in-cluding study manuals, protocols, and ear-lier methodology papers, was also used tocode each study. Rationale for classifica-tion of intervention features such as modeof delivery, provider, intensity/frequency of
Figure 1—PRISMA2009flowdiagramof search process and results. Adapted fromMoherD, LiberatiA, Tetzlaff J, AltmanDG;ThePRISMAGroup.PreferredReporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 2009;6:e1000097. For more information, visit www.prisma-statement.org.
1802 Diet Behavior Change Techniques Diabetes Care Volume 40, December 2017

intervention, andother variables included isdocumented inanearlier reviewcarriedoutby the review team (8). Intensity was de-fined as the number of total or face-to-face contacts with intervention personneland frequencywas defined as the averagenumber of weeks between contacts.
AnalysisWe defined an HbA1c reduction of$0.3%(3.3 mmol/mol) as clinically significant,which follows the precedent set by others(14,15). Meta-analyses were conductedusing RevMan (v5.3) on the primary out-come measure of HbA1c and the second-ary outcome of body weight, wheresufficient data were available. We re-corded changes in outcomes at 0–3, 3–6, 6–12, and 12–24 months. The use ofthese time points allowed a greater num-ber of studies to be included. In studiesthat reported data from multiple timepoints, we used the time point closestto the end of the intervention for analysis.Mean differences and SDs in the differ-ences for HbA1c and weight loss betweenbaseline and the different time pointswere calculated. SDs for missing datawere calculated from SE, P, and t values,where reported, using the Cochraneguidelines or were calculated using a cor-relation (method documented in an ear-lier review by this research team) (8).Correlations of 0.75 (HbA1c) and 0.98(weight loss) were used to calculate miss-ing SDs following a sensitivity analysis ofcorrelations and reported SDs. Statisticalsignificance of the moderator and meta-analyses was set at P , 0.05. In all casesthe meta-analyses used the raw meandifference and a random effects modelto calculate results. Meta-analyses werecarried out on both interventions thataimed to change behavior only and inter-ventions that aimed to change environ-ment only. Further meta-analyses werecarried out on HbA1c and weight loss at0–3, 3–6, 6–12, and 12–24months.Meta-analyses were also carried out on differ-ent diet types.
Moderator AnalysesA series of moderator analyses were car-ried out to investigate the association be-tween BCTs/intervention features andclinical outcome results (HbA1c) wherethe presence or absence of a certain BCTor intervention feature in certain studieswas associated with changes in HbA1c.The moderator analyses reported thestandardizedmeandifference inoutcomes,
usingComprehensiveMeta-Analysis (CMA)software. The random effects analysis wasused to conduct all moderator analyses.For every moderator variable (BCT and in-tervention feature), we calculated thepoint estimate, 95% CIs, Q statistic, andP value.
As a result of the large effect size ob-served in the control group, a series ofsubgroup analyses were carried out inan attempt to elucidate the true effectsize of intervention groups comparedwith control groups. Further subgroupsensitivity analyses were carried out ontrue control groups, excluding studieswhere the control group had.1 contactwith a dietitian, and an additional sub-group analysis removed studies with acontrol group reduction in HbA1c of $0.3%(3.3 mmol/mol). Moderator analyses ofBCTs associated with reductions in HbA1cwere also carried out on studies that usedinterventions aimed at changing behaviorprimarily or environment primarily and stud-ies that reported results at 3 months only.
RESULTS
Study Selection and StudyCharacteristicsThe inclusion criteria were met by 54studies (16–69). Summary characteris-tics of included studies are outlined inSupplementary Data Table S4. Averageage of participants was 57.7 6 4.7 yearsfor intervention groups and 58.1 6 5.1years for control groups. For interven-tion and control groups, respectively,mean duration of diabetes, where re-ported, was 7.6 6 3.3 years and 7.3 63.1 years, mean baseline HbA1c was8.1% (69.8 mmol/mol) 6 1% and 8.12%(69.9 mmol/mol) 6 1%, and BMI was32.1 6 4.1 kg/m2 and 31.8 6 4 kg/m2.Six of the included studies were carriedout in a community center setting, 12studies did not report the setting, onestudywas online, one studywas in a hotelsetting, and all remaining studies (n = 34)were carried out in a clinical or academicsetting. All participants in the 54 studieswere classified as having type 2 diabetes;however, diagnostic criteria for HbA1c var-iedamong includedstudies fromaminimumof 5.5% (47.4 mmol/mol) (34) to a maxi-mum of 12% (103.4 mmol/mol) (23,57).The mean percentage of dropouts perstudywas lower in the intervention groups(12.6%) than in control groups (16.4%).Studies with low–glycemic index and high-protein diets reported the lowest number
of dropouts (meanpercentageof dropouts1% and 1.8%, respectively), with mealreplacement studies reporting the high-est dropout rate (mean percentage ofdropouts 28%) (Supplementary DataTable S5).
Risk of Bias and Treatment FidelityIn the assessments of risk of bias, 63% ofthe studies were classified as “unclear,”while 34% were “low” across all sevenvariables and only 2% were classified as“high” risk of bias (Supplementary DataTables S6a and S6b). Raters agreed on78% of risk of bias assessments follow-ing initial assessment and came toagreement on the remainder throughdiscussion. Treatment fidelity resultsare documented in Supplementary DataTable S7. Overall, the reported use oftreatment fidelity strategies was verylow, with 78% assessed as having notused a treatment fidelity strategy. Themost widely used treatment fidelitystrategy was in the subcategory of“monitoring and improving enactmentof treatment skills,” where 68.5% of allstudies reported use of “ensure partici-pant use of behavioral skills.” Ratersagreed on 76.5% of assessments and re-solved remaining disagreements throughdiscussion and arbitration.
Meta-analyses of Diet InterventionsMeta-analysis of interventions that aimedto change behavior (n = 39) showed anoverall reduction in HbA1c of 0.32%(3.5 mmol/mol) (95% CI 20.40, 20.23;P , 0.00001), while interventions thataimed to change or control the environ-ment showed an overall reduction inHbA1c of 0.5% (5.5 mmol/mol) (95%CI 20.65, 20.34; P , 0.00001) (Fig. 2).Sensitivity analysis removing studies witha .0.3% (3.3 mmol/mol) reduction inHbA1c in the control group (n = 21)increased further the observed effectsize on HbA1c, with behavioral interven-tions showing a reduction of 0.32%(3.5 mmol/mol) (95% CI 20.41, 20.24;P , 0.00001) compared with 0.66%(7.3 mmol/mol) (95% CI 20.88, 20.45;P, 0.00001) for environment-controlledstudies (n = 11) (Supplementary DataTable S8).
Studies included in this review focusedon different dietary approaches: low car-bohydrate (n = 9), low fat (n = 16), highprotein (n = 5), meal replacements (n = 4),low glycemic index (n = 3), medical
care.diabetesjournals.org Cradock and Associates 1803

nutritional therapy (n = 2),Mediterranean(n = 2), and others (n = 13). There wasconsiderable heterogeneity in the dietsused in control groups. There was a“true” control group in 28 studies, whereno additional intervention support or
contact was provided. In 16 studies,American Diabetes Association or Ameri-can Heart Association guidelines were ap-plied to control groups, with varyingdegrees of intervention support pro-vided (Supplementary Data Table S9).
The duration of interventions carriedout ranged from 4 weeks to 2 years. In21 studies, there was an additional minorphysical activity component.
Studies using meal replacements andhigh-protein diets were associated with
Figure 2—Meta-analysis of studies aimed at changing dietary behavior (n = 39) (A) and studies aimed at changing dietary environment (n = 17) (B). Valuesreported in meta-analyses represent mean difference and SD of the difference in HbA1c from baseline to specific time point for intervention and controlgroups. Letter next to a study indicates a subgroup. Each figure panel provides the combinedweighted difference of all studies between intervention andcontrol groups. 95%CIs are also reported. Pedersen et al. (49)was not included as the intervention provided a portion control plate to subjects rather thana specific diet or food group. Yusof et al. (58) was not included as it did not specify the amount of food provided to subjects. IV, inverse variance.
1804 Diet Behavior Change Techniques Diabetes Care Volume 40, December 2017

the greatest reductions in HbA1c (0.56%[6.2mmol/mol] and0.5% [5.5mmol/mol],respectively). Low-carbohydrate dietsshowed a greater reduction in HbA1c(0.44% [4.8mmol/mol]) than low-fat diets(0.40% [4.4 mmol/mol]) or low–glycemicindex diets (0.09% [1 mmol/mol])(Supplementary Data Table S10).
Meta-analysis of Changes in HbA1c andBody Weight at Different Time PointsMeta-analyses showed differences inHbA1c between intervention and controlgroups at different timepoints, presentedgraphically in Fig. 3. Combining all studiesand all time points in one overall meta-analysis (n = 59, 54 studies) showed a re-duction inHbA1c of 0.35% (3.8mmol/mol)(95% CI 20.43, 20.28; P , 0.00001)(Supplementary Data Table S11). Hetero-geneity as measured by I2 was 62%, 44%,38%, and 68% at 0–3, 3–6, 6–12, and 12–24 months, respectively. Sensitivity anal-ysis comparing data at exactly 3, 6, 12, and24 months to data at 0–3, 3–6, 6–12, and12–24 months using a larger dataset (n =54) showed no significant differences.The difference in body weight loss
between intervention and control groupswas 2.34 kg (95% CI 22.99, 21.69; P ,0.00001), 2.94 kg (95% CI 23.92, 21.97;P , 0.00001), 2.27 kg (95% CI 23.32,21.21; P , 0.0001), and 2.14 kg (95%CI 23.34, 20.93; P = 0.0005) at 0–3,3–6, 6–12, and 12–24 months, respec-tively (Supplementary Data Table S12).Combining all studies and time points re-vealed a reduction in body weight of2.41 kg (95% CI 22.96, 21.86; P ,0.00001) (Supplementary Data TableS13). Heterogeneity as measured by I2
was 84%, 93%, 88%, and 27% at 0–3, 3–6, 6–12, and 12–24 months, respectively.
BCTs UsedA total of 42 distinct BCTs were applied inthe intervention groups, 7 of which werereported only once. The number of BCTsused in a single RCT ranged from3 (25,35,45) to 17 (41). The five most fre-quently occurring BCTs were “instructionon how to perform a behavior” (n = 54),“credible source” (n = 45), “self-monitoringof behavior” (n = 37), “monitoring of be-havior by others without feedback” (n =32), and “social support (unspecified)”(n = 24) (Table 1).Control group BCTs were coded sepa-
rately, and 28 different BCTs were identi-fied, with the number of BCTs used in a
single study ranging from 0 (49,60) to15 (44) (Supplementary Data Table S14).Interrater agreement as determined bythe Cohen kwas 0.7 after coding 44 stud-ies and 0.68 after all 54 studies werecoded. A breakdown by category ofBCTs used (Supplementary Data TableS15) and BCTs not used (SupplementaryData Table S16) was also carried out.
Moderator Analysis of BCTsThe original moderator analysis showedno BCTs coded for diet behavior were as-sociated with .0.3% (3.3 mmol/mol) re-duction in HbA1c (Supplementary DataTable S17). Subgroup analysis of interven-tions using only true control groupsshowed that the BCTs “social compari-son” (0.52% [5.7 mmol/mol], P = 0.012)and “feedback on behavior” (0.365%[4mmol/mol], P = 0.046) were associatedwith clinically and statistically significantreductions in HbA1c (Supplementary DataTable S18). Subgroup analysis of interven-tions excluding studieswith control grouppre- to poststudy change of .0.3%(3.3 mmol/mol) in HbA1c also showedthe BCT “feedback on behavior” (0.34%[3.7mmol/mol]) associatedwith clinicallysignificant reductions in HbA1c (Supple-mentary Data Table S19). Subgroup anal-ysis of BCTs reporting outcome changesat 3 months showed that the BCT “prob-lem solving” (0.63% [6.9 mmol/mol]) wasassociated with clinically significant re-ductions in HbA1c (Supplementary DataTable S20). Moderator analysis was notcarried out at 12 months because insuffi-cient data were available.
Subgroup analysis of interventionsaimed at changing behavior showedthat the BCTs “feedback on behavior”(0.52% [5.7 mmol/mol], P = 0.007) and“adding objects to the environment”(0.39% [4.3 mmol/mol]) were associatedwith clinically significant reductions inHbA1c (Supplementary Data Table S21).Subgroup analysis of interventions aimedat changing the dietary environmentshowed that the BCT “problem solving”(0.5% [5.5 mmol/mol]) was associatedwith a clinically significant reduction inHbA1c (Supplementary Data Table S22).
Moderator Analysis of InterventionFeaturesThe original moderator analysis showedno intervention feature was associatedwith a clinically significant reduction inHbA1c (Supplementary Data Table S23).Subgroup moderator analysis excluding
studies with control group pre- to post-study change of.0.3% (3.3mmol/mol) inHbA1c showed that the only interventionfeature associated with a clinically signif-icant reduction in HbA1c was the use of atheoretical model or framework (0.33%[3.6 mmol/mol]). Other intervention fea-tures associated with reductions in HbA1cwere a higher frequency and number ofboth total and face-to-face contacts withintervention personnel (SupplementaryData Table S23).
CONCLUSIONS
These findings suggest that changing orcontrolling dietary environmental factorsmay be more effective than strategiesto change dietary behavior in attemptingto reduce HbA1c in adults with type 2 dia-betes. High-protein diets and meal re-placement programs produced the greatestreductions in HbA1c. A clinically significantdifference in HbA1c at 0–3, 3–6, and 6–12months was reportedwhen all dietary ap-proacheswere combined inmeta-analyses.Weight loss occurred but diminished overtime. Moderator analyses identified fourBCTsd“problem solving,” “feedback onbehavior,” “adding objects to the environ-ment,” and “social comparison”dandthe intervention feature “use of theory”that were associated with clinically signif-icant reductions in HbA1c.
Diets where the environment waschanged or controlled (e.g., where all foodwas provided) were more than twice aseffective in reducingHbA1c thandiets usingbehavioral change interventions. This ob-servation was consistent when a range ofdifferent foods were provided, includinghigh-protein (29,30,48), meal replace-ment (21,27,50,57), low-carbohydrate(51,62), low-fat (51,55,63), Mediterra-nean (33), Korean traditional (35), vege-tarian (36), and partial formula or partiallow-calorie diets (52). These studies rep-resent a more internally valid approachcompared with studies aimed at changingbehavior; however, successful externallyvalid interventions are required in orderto change diet in a real-world setting. Ithas been suggested that environmentalchanges to social, built, and food environ-ments, in addition to individual behavioralchanges, are required in order to adopt ahealthy diet and lifestyle (70). Changingthe environment has been identified asone of the overall theoretical themes as-sociated with changing behavior, particu-larly in the longer term (71).
care.diabetesjournals.org Cradock and Associates 1805

Figure 3—Meta-analysis ofHbA1c at 0–3months (n =35) (A), at 3–6months (n= 26) (B), at 6–12months (n= 16) (C), and at12–24months (n=5) (D). Valuesreported in meta-analyses represent mean difference and SD of the difference in HbA1c from baseline to specific time point for intervention and controlgroups. Letter next to a study indicates a subgroup. Each figure panel provides the combinedweighted difference of all studies between intervention andcontrol groups. 95% CIs are also reported. IV, inverse variance.
1806 Diet Behavior Change Techniques Diabetes Care Volume 40, December 2017

In regard to the typeof diet, ourfindingof a modest but statistically significant re-duction in HbA1c at 3, 6, and 12 monthsneeds to be interpretedwith caution, as arange of different diets were combined inan effort to elucidate the most effectiveBCTs and intervention features. The ob-served reduction in HbA1c is greater thaninprevious reportswith fewer (n = 20) stud-ies of high-protein, low-carbohydrate,
and low–glycemic index diets. Our dataalso indicate that the use ofmeal replace-ments and high-protein diets results inthe greatest reduction in HbA1c, withlow-carbohydrate diets showing a greaterreduction in HbA1c than low-fat diets.However, meal replacement interven-tions also had the highest dropout rate,suggesting these interventions may notbe externally valid or themost acceptable
approach for participants. The averagenumber of dropouts per study was thelowest for the high-protein diets at1.8%, suggesting that it was the dietmost acceptable to participants. Theoverall meta-analysis showed an overallweight loss of 2.41 kg, with the greatestdecrease observed at 6 months (2.94 kg)but diminishing over timeda patternconsistent with previous work (4).
Table 1—BCTs most frequently occurring in studies included in meta-analysis
BCT no.* BCT label No. of studies that reported BCT
4.1 Instruction on how to perform a behavior 54
9.1 Credible source 45
2.3 Self-monitoring of behavior 37
2.1 Monitoring of behavior by others without feedback 32
3.1 Social support (unspecified) 24
1.1 Goal setting (behavior) 23
12.5 Adding objects to the environment 22
2.4 Self-monitoring of outcome(s) of behavior 15
2.5 Monitoring outcome(s) of behavior by others withoutfeedback
12
2.6 Biofeedback 12
6.1 Demonstration of the behavior 12
1.3 Goal setting (outcome) 10
1.2 Problem solving 9
8.1 Behavioral practice/rehearsal 9
2.2 Feedback on behavior 7
1.5 Review behavior goal(s) 6
3.3 Social support (emotional) 6
13.2 Framing/reframing 5
1.7 Review outcome goal(s) 4
6.2 Social comparison 4
4.2 Information about antecedents 3
12.1 Restructuring the physical environment 3
1.4 Action planning 2
1.6 Discrepancy between current behavior and goal 2
2.7 Feedback on outcome(s) of behavior 2
5.1 Information about health consequences 2
7.1 Prompts/cues 2
8.2 Behavior substitution 2
8.3 Habit formation 2
10.3 Nonspecific reward 2
10.4 Social reward 2
11.2 Reduce negative emotions 2
11.3 Conserving mental resources 2
12.2 Restructuring the social environment 2
15.3 Focus on past success 2
3.2 Social support (practical) 1
5.4 Monitoring of emotional consequences 1
8.6 Generalization of a target behavior 1
8.7 Graded tasks 1
9.2 Pros and cons 1
10.9 Self-reward 1
12.3 Avoidance/reducing exposure to cues for the behavior 1
*BCTs categorized according to BCT taxonomy v1 of Michie et al. (7).
care.diabetesjournals.org Cradock and Associates 1807

Beyond the BCT “adding objects to theenvironment,” the three other BCTs “so-cial comparison,” “feedback on behav-ior,” and “problem solving” all havestrong theoretical foundations and havebeen shown to be efficacious in otherstudies (5,8,72,73). Given that the use ofmore BCTs was not associated withgreater effectiveness, the pattern of ap-plication or fidelity of use of BCTs maybe of greater importance. Of the 93 BCTsin the taxonomy of Michie et al. (7),51 BCTs were not found in any of the54 reviewed studies. BCTs most fre-quently used came from the categories“feedback and monitoring,” “shapingknowledge,” “goals and planning,” “com-parison of behavior,” and “social sup-port.” The BCTs “behavioral contract”and “commitment” were not used inany of the included studies. The studiesreviewed focused almost exclusively onreflective motivation, suggesting thatdeployment of a wider range of BCTsneeds to be investigated in changingdietary behavior and improving HbA1c
and body weight in adults with type 2diabetes.The only intervention feature in the
moderator analysis that was associatedwith clinically significant reductions inHbA1c was the “use of theory/model” toinform interventions. Similar findingshave been reported, in which dietary be-havior interventions in cancer preventionwere more effective when informed bytheory (74). However, fidelity of the useof theory was not reported in the studiesincluded in our review or other reviews(74), and descriptions of use of theoryvaried considerably from “integrated con-cepts fromdifferent theories” (46) to “be-havior modification treatment usedprinciples from the modern learning the-ory” (37) and “group educational classeswere based on the social cognitive the-ory” (21). The social cognitive theory(75) was the only theory reported morethan once (21,46,64).Our findings might suggest that higher
frequency and greater number of con-tacts are associated with greater reduc-tions inHbA1c,which is consistentwithourprevious systematic review of combineddiet and physical activity interventions(8), although this may arise from moreintervention content being delivered.However, we cannot be sure because fi-delity was so poorly reported in almost allcategories and in all studies apart from
one subcategory of “monitoring and im-proving enactment of treatment skills,”where 68.5% of studies reported use offidelity. This subcategorywas coded “yes”when the intervention description report-ed that subjects carried out a 3- or 7-dayfood record and that it was reviewed bythe dietitian. The criteria (13) for inter-vention fidelity assessment do not takeaccount of the extent of use of each cat-egory, which is particularly relevant in as-sessing participant adherence to dietaryprograms, i.e., enactment. Low levels ofenactment make it difficult to assess theefficacy of interventions.
Thesefindings fromlarge,well-controlleddietary interventions have potentiallyimportant implications for type 2 diabe-tes management and suggest that inter-ventions aimed at changing the dietaryenvironment warrant further scrutiny. Itis impractical from a treatment perspec-tive to provide food and control the foodenvironment as a scalable solution totype 2 diabetes treatment in the com-munity. However, this finding does pro-vide evidence that changing or alteringthe food environment or using highly in-ternally valid interventions is efficacious.Providing foods at the beginning of aprogram or intervention might be an ef-fective strategy to help people managetheir diabetes, followed by instructionon how to choose, shop for, and pre-pare these foods, gradually weaningthem off of reliance on foods provided.We would suggest that future studieslook at the economic ramifications ofchanging the food environment frompolicy, marketing, and farming perspec-tives. Individual behavior change effortsmight benefit from increased aware-ness of the dietary environment and ex-ertion of greater control over one’sdietary environment. For example, the in-dividual could be guided through an auditof their current home food environment(stored food supplies) and inappropri-ate foodwould be removed to eliminatepotential impulse food consumption ofinappropriate foods. If we really wantto change diet in real-world settings,we also need to find BCTs associatedwith successful externally valid dietaryinterventions.
Future studies ought to quantify in-tervention fidelity, which would allowthe identification of more effectiveBCTs. The use of video or audio record-ings of consultations with dietitians
and other health care professionals mayhelp to better define the range of BCTsbeing deployed in any given intervention.
A strength of our study is the use ofthe most recent and comprehensive tax-onomy of behavior change techniquesavailable (7). We have provided a com-prehensive analysis of fidelity categoriesand subcategories as well as detailed sub-group meta- and moderator analyses.Limitations of our study are the heteroge-neity in the dietary interventions andthe different diagnostic criteria fortype 2 diabetes, which are likely to haveresulted in variable effects on HbA1c andweight in patients with type 2 diabetes.However, we think that this heterogene-ity in the interventions and in their effi-cacy is likely to have increased randomerror rather than bias, making our find-ings evenmore compelling. The quality ofreporting of BCTs in different studies var-ied considerably and was poor overall.This is particularly true of fidelity mea-sures, and any conclusions must be tem-pered with the recognition of significantinter- and intrastudy variability in adher-ence to intervention protocols. As studyprotocols do not always stipulate eachBCT used, BCTs are likely to have beenunderreported.
In conclusion, this systematic reviewand meta-analysis provides evidencethat changing dietary environmentmay be more important than focusingon dietary behavior in type 2 diabetestreatment. More robust reporting of con-tent, fidelity, and frequency of BCTs andintervention fidelity, as well as betteralignment of intervention design with be-havior change theory, would be helpful inrefining interventions so that they aremore efficacious.
Funding. The authors thank the Irish ResearchCouncil for Science, Engineering and Technologyfor funding this project (Project ID GOIPG/2013/873).Duality of Interest. No potential conflicts of in-terest relevant to this article were reported.AuthorContributions.K.A.C.,G.OL., F.M.F., L.R.Q.,K.A.M.G., and H.L.G. formulated the researchquestion and defined the search terms. K.A.C. car-ried out the electronic searches. K.A.C. and R.M.carried out the search process, the methodologi-cal assessment, and the BCT coding. H.L.G. guidedthe BCT coding process and acted as a mastercoder. K.A.C. and H.L.G. carried out the fidelityassessment. K.A.C. carried out the moderator analy-sis and the meta-analysis. All authors were involvedin writing and reviewing the final manuscript.
1808 Diet Behavior Change Techniques Diabetes Care Volume 40, December 2017

References1. Schulze MB, Manson JE, Ludwig DS, et al.Sugar-sweetened beverages, weight gain, and in-cidence of type 2 diabetes in young and middle-aged women. JAMA 2004;292:927–9342. Ley SH, Ardisson Korat AV, Sun Q, et al. Con-tribution of the nurses’ health studies to uncover-ing risk factors for type 2 diabetes: diet, lifestyle,biomarkers, and genetics. Am J Public Health2016;106:1624–16303. Micha R, Pe~nalvo JL, Cudhea F, Imamura F,Rehm CD, Mozaffarian D. Association betweendietary factors and mortality from heart disease,stroke, and type 2 diabetes in the United States.JAMA 2017;317:912–9244. Dansinger ML, Tatsioni A, Wong JB, Chung M,Balk EM.Meta-analysis: the effect of dietary coun-seling for weight loss. Ann Intern Med 2007;147:41–505. Lara J, Hobbs N, Moynihan PJ, et al. Effective-ness of dietary interventions among adults ofretirement age: a systematic review and meta-analysis of randomized controlled trials. BMCMed 2014;12:606. Dombrowski SU, Sniehotta FF, Avenell A,JohnstonM,MacLennanG,Araujo-SoaresV. Iden-tifying active ingredients in complex behaviouralinterventions for obese adults with obesity-related co-morbidities or additional risk factorsfor co-morbidities: a systematic review. HealthPsychol Rev 2012;6:7–327. Michie S, RichardsonM, JohnstonM, et al. Thebehavior change technique taxonomy (v1) of93 hierarchically clustered techniques: buildingan international consensus for the reporting ofbehavior change interventions. Ann Behav Med2013;46:81–958. Cradock KA, OLaighin G, Finucane FM,Gainforth HL, Quinlan LR, Martin Ginis KA. Behav-iour change techniques targeting both diet andphysical activity in type 2 diabetes: a systematicreview and meta-analysis. Int J Behav Nutr PhysAct 2017;14:189. Accurso A, Bernstein RK, Dahlqvist A, et al. Di-etary carbohydrate restriction in type 2 diabetesmellitus and metabolic syndrome: time for a crit-ical appraisal. Nutr Metab (Lond) 2008;5:910. Hu T, Mills KT, Yao L, et al. Effects of low-carbohydrate diets versus low-fat diets on meta-bolic risk factors: a meta-analysis of randomizedcontrolled clinical trials. Am J Epidemiol 2012;176(Suppl. 7):S44–S5411. Antonio J, Peacock CA, EllerbroekA, FromhoffB, Silver T. The effects of consuming a high proteindiet (4.4 g/kg/d) on body composition in resistance-trained individuals. J Int Soc SportsNutr 2014;11:1912. Higgins JPT, Deeks JJ (Eds.). Chapter 7: Select-ing studies and collecting data. In Cochrane Hand-book for Systematic Reviews of Interventions.Version 5.1.0 (updated March 2011) [Internet].The Cochrane Collaboration, 2011. Availablefrom http://www. handbook.cochrane.org.Accessed 13 April 201713. Bellg AJ, Borrelli B, Resnick B, et al.; Treat-ment Fidelity Workgroup of the NIH BehaviorChange Consortium. Enhancing treatment fidelityin health behavior change studies: best practicesand recommendations from the NIH BehaviorChange Consortium. Health Psychol 2004;23:443–45114. Avery L, Flynn D, van Wersch A, Sniehotta FF,Trenell MI. Changing physical activity behavior in
type 2 diabetes: a systematic review and meta-analysis of behavioral interventions. DiabetesCare 2012;35:2681–268915. Dasgupta K, Hajna S, Joseph L, Da Costa D,Christopoulos S, Gougeon R. Effects of meal prep-aration training on body weight, glycemia, andblood pressure: results of a phase 2 trial in type 2diabetes. Int J Behav Nutr Phys Act 2012;9:12516. Al-Shookri A, Khor GL, Chan YM, Loke SC, Al-Maskari M. Effectiveness of medical nutritiontreatment delivered by dietitians on glycaemicoutcomes and lipid profiles of Arab, Omani pa-tients with type 2 diabetes. Diabet Med 2012;29:236–24417. Anderson-Loftin W, Bunn BS, Sullivan P,Hussey J, Tavakoli A. Soul food light: culturallycompetent diabetes education. Diabetes Educ2005;31:555–56318. Andrews RC, Cooper AR, Montgomery AA,et al. Diet or diet plus physical activity versus usualcare in patients with newly diagnosed type 2 di-abetes: the Early ACTID randomised controlledtrial. Lancet 2011;378:129–13919. Azadbakht L, Surkan PJ, Esmaillzadeh A,Willett WC. The Dietary Approaches to Stop Hy-pertension eating plan affects C-reactive protein,coagulation abnormalities, and hepatic functiontests among type 2 diabetic patients. J Nutr2011;141:1083–108820. BarnardND,Gloede L, Cohen J, et al. A low-fatvegan diet elicits greater macronutrient changes,but is comparable in adherence and acceptability,comparedwith amore conventional diabetes dietamong individuals with type 2 diabetes. J AmDietAssoc 2009;109:263–27221. Cheskin LJ, Mitchell AM, Jhaveri AD, et al.Efficacy of meal replacements versus a standardfood-based diet for weight loss in type 2 diabetes:a controlled clinical trial. Diabetes Educ 2008;34:118–12722. Coppell KJ, Kataoka M, Williams SM,Chisholm AW, Vorgers SM, Mann JI. Nutritionalintervention in patients with type 2 diabeteswho are hyperglycaemic despite optimised drugtreatmentdLifestyle Over and Above Drugs in Di-abetes (LOADD) study: randomised controlled tri-al. BMJ 2010;341:c333723. Daly ME, Paisey R, Paisey R, et al. Short-termeffects of severe dietary carbohydrate-restrictionadvice in type 2 diabetesda randomized con-trolled trial. Diabet Med 2006;23:15–2024. Dyson PA, Beatty S, Matthews DR. A low-carbohydrate diet is more effective in reducingbody weight than healthy eating in both diabeticand non-diabetic subjects. Diabet Med 2007;24:1430–143525. Elhayany A, Lustman A, Abel R, Attal-Singer J,Vinker S. A low carbohydrate Mediterranean dietimproves cardiovascular risk factors and diabetescontrol among overweight patients with type 2diabetes mellitus: a 1-year prospective random-ized intervention study. Diabetes Obes Metab2010;12:204–20926. Evangelista LS, Heber D, Li Z, Bowerman S,HamiltonMA, FonarowGC. Reduced body weightand adiposity with a high-protein diet improvesfunctional status, lipid profiles, glycemic control,and quality of life in patients with heart failure: afeasibility study. J Cardiovasc Nurs 2009;24:207–21527. Foster GD, Borradaile KE, Vander Veur SS,et al. The effects of a commercially available
weight loss program among obese patients withtype 2 diabetes: a randomized study. PostgradMed 2009;121:113–11828. FranzMJ,MonkA, Barry B, et al. Effectivenessof medical nutrition therapy provided bydietitians in the management of non-insulin-dependent diabetes mellitus: a randomized, con-trolled clinical trial. J Am Diet Assoc 1995;95:1009–101729. Gannon MC, Nuttall FQ, Saeed A, Jordan K,Hoover H. An increase in dietary protein improvesthe blood glucose response in personswith type 2diabetes. Am J Clin Nutr 2003;78:734–74130. Gannon MC, Nuttall FQ. Effect of a high-pro-tein, low-carbohydrate diet on blood glucose con-trol in peoplewith type 2 diabetes.Diabetes2004;53:2375–238231. Goldstein T, Kark JD, Berry EM, Adler B, Ziv E,Raz I. The effect of a low carbohydrate energy-unrestricted diet on weight loss in obese type 2diabetes patientsda randomized controlled trial.e-SPEN J 2011;6:e178–e18632. Imai S, Matsuda M, Hasegawa G, et al. Asimple meal plan of ‘eating vegetables before car-bohydrate’ was more effective for achieving gly-cemic control than an exchange-based meal planin Japanese patientswith type2diabetes. Asia PacJ Clin Nutr 2011;20:161–16833. Itsiopoulos C, Brazionis L, Kaimakamis M,et al. Can the Mediterranean diet lower HbA1cin type 2 diabetes? Results from a randomizedcross-over study. Nutr Metab Cardiovasc Dis2011;21:740–74734. Jonsson T, Granfeldt Y, Ahren B, et al. Bene-ficial effects of a Paleolithic diet on cardiovascularrisk factors in type 2diabetes: a randomized cross-over pilot study. Cardiovasc Diabetol 2009;8:3535. Jung SJ, Park SH, Choi EK, et al. Beneficialeffects of Korean traditional diets in hypertensiveand type 2 diabetic patients. J Med Food 2014;17:161–17136. Kahleova H, Matoulek M, Malinska H, et al.Vegetarian diet improves insulin resistance andoxidative stress markers more than conventionaldiet in subjects with type 2 diabetes. Diabet Med2011;28:549–55937. Kaplan RM, Hartwell SL, Wilson DK, WallaceJP. Effects of diet and exercise interventions oncontrol andquality of life in non-insulin-dependentdiabetes mellitus. J Gen Intern Med 1987;2:220–22838. Kattelmann KK, Conti K, Ren C. The MedicineWheel nutrition intervention: a diabetes educa-tion study with the Cheyenne River Sioux Tribe. JAm Diet Assoc 2010;110(Suppl.):S44–S5139. Kondo K, Morino K, Nishio Y, et al. A fish-based diet intervention improves endothelialfunction in postmenopausal women with type 2diabetes mellitus: a randomized crossover trial.Metabolism 2014;63:930–94040. Koo BK, Han KA, Ahn HJ, Jung JY, Kim HC,MinKW. The effects of total energy expenditure fromall levels of physical activity vs. physical activityenergy expenditure from moderate-to-vigorousactivity on visceral fat and insulin sensitivity inobese type 2 diabetic women. Diabet Med2010;27:1088–109241. Laitinen JH, Ahola IE, Sarkkinen ES, WinbergRL, Harmaakorpi-Iivonen PA, UusitupaMI. Impactof intensified dietary therapy on energy and nu-trient intakes and fatty acid composition of serumlipids in patients with recently diagnosed
care.diabetesjournals.org Cradock and Associates 1809

non-insulin-dependent diabetes mellitus. J AmDiet Assoc 1993;93:276–28342. Liu H, Zhang M, Wu X, Wang C, Li Z. Effective-ness of a public dietitian-led diabetes nutrition inter-vention on glycemic control in a community settingin China. Asia Pac J Clin Nutr 2015;24:525–53243. Luger M, Holstein B, Schindler K, Kruschitz R,Ludvik B. Feasibility and efficacy of an isocalorichigh-protein vsstandard diet on insulin require-ment, body weight and metabolic parameters inpatients with type 2 diabetes on insulin therapy.Exp Clin Endocrinol Diabetes 2013;121:286–29444. Ma Y, Olendzki BC, Merriam PA, et al. A ran-domized clinical trial comparing low-glycemic in-dex versus ADA dietary education amongindividuals with type 2 diabetes. Nutrition 2008;24:45–5645. Mesci B, Celik S, Coksert KilicD, TekinM,OguzA. Refined carbohydrate restricted diet versusconventional diabetic diet in type 2 diabetic pa-tients treated by insulin. Acta Endocrinol (Buc)2010;6:203–20946. Miller CK, Edwards L, Kissling G, Sanville L.Nutrition education improves metabolic out-comes among older adults with diabetesmellitus:results from a randomized controlled trial. PrevMed 2002;34:252–25947. Nicholson AS, Sklar M, Barnard ND, Gore S,Sullivan R, Browning S. Toward improved man-agement of NIDDM: a randomized, controlled,pilot intervention using a lowfat, vegetarian diet.Prev Med 1999;29:87–9148. Nuttall FQ, Schweim K, Hoover H, GannonMC. Effect of the LoBAG30 diet on blood glucosecontrol in people with type 2 diabetes. Br J Nutr2008;99:511–51949. Pedersen SD, Kang J, KlineGA. Portion controlplate for weight loss in obese patients with type 2diabetes mellitus: a controlled clinical trial. ArchIntern Med 2007;167:1277–128350. Pi-Sunyer FX, Maggio CA, McCarron DA, et al.Multicenter randomized trial of a comprehensiveprepared meal program in type 2 diabetes. Dia-betes Care 1999;22:191–19751. Rock CL, Flatt SW, Pakiz B, et al. Weight loss,glycemic control, and cardiovascular disease riskfactors in response to differential diet composi-tion in a weight loss program in type 2 diabetes: arandomized controlled trial. Diabetes Care 2014;37:1573–158052. Shirai K, Saiki A, Oikawa S, et al. The effects ofpartial use of formula diet on weight reductionand metabolic variables in obese type 2 diabeticpatientsdmulticenter trial. Obes Res Clin Pract2013;7:e43–e54
53. Talib R, Ali O, Arshad F, Kadir KA. The effec-tiveness of group dietary counselling among noninsulin dependent diabetes mellitus (NIDDM) pa-tients in resettlement scheme areas in Malaysia.Asia Pac J Clin Nutr 1997;6:84–8754. Visek J, Lacigova S, Cechurova D, Rusavy Z.Comparison of a low-glycemic index vs standarddiabetic diet. Biomed Pap Med Fac Univ PalackyOlomouc Czech Repub 2014;158:112–11655. Williams KV, Mullen ML, Kelley DE, Wing RR.The effect of short periods of caloric restriction onweight loss and glycemic control in type 2 diabe-tes. Diabetes Care 1998;21:2–856. Yamada Y, Uchida J, Izumi H, et al. A non-calorie-restricted low-carbohydrate diet is effec-tive as an alternative therapy for patients withtype 2 diabetes. Intern Med 2014;53:13–1957. Yip I, Go VL, DeShields S, et al. Liquid mealreplacements and glycemic control in obesetype 2 diabetes patients. Obes Res 2001;9(Suppl.4):341S–347S58. Yusof BN, Talib RA, Kamaruddin NA, KarimNA, Chinna K, Gilbertson H. A low-GI diet is asso-ciated with a short-term improvement of glycae-mic control in Asian patientswith type 2 diabetes.Diabetes Obes Metab 2009;11:387–39659. Ziemer DC, Berkowitz KJ, Panayioto RM, et al.A simple meal plan emphasizing healthy foodchoices is as effective as an exchange-based mealplan for urban African Americans with type 2 di-abetes. Diabetes Care 2003;26:1719–172460. Bowen ME, Cavanaugh KL, Wolff K, et al. Thediabetes nutrition education study randomizedcontrolled trial: A comparative effectivenessstudy of approaches to nutrition in diabetes self-management education. Patient Educ Couns2016;99:1368–137661. Carter S, Clifton PM, Keogh JB. The effects ofintermittent compared to continuous energy re-striction on glycaemic control in type 2 diabetes; apragmatic pilot trial. Diabetes Res Clin Pract 2016;122:106–11262. Goday A, Bellido D, Sajoux I, et al. Short-termsafety, tolerability andefficacyof a very low-calorie-ketogenic diet interventional weight loss pro-gram versus hypocaloric diet in patients withtype 2 diabetes mellitus. Nutr Diabetes 2016;6:e23063. Li X, Cai X, Ma X, et al. Short- and long-termeffects of wholegrain oat intake on weight man-agement and glucolipidmetabolism in overweighttype-2 diabetics: a randomized control trial. Nu-trients 2016;8:E54964. Muchiri JW, Gericke GJ, Rheeder P. Effect of anutrition education programme on clinical status
and dietary behaviours of adults with type 2 di-abetes in a resource-limited setting in SouthAfrica: a randomised controlled trial. PublicHealthNutr 2016;19:142–15565. O’Neil PM, Miller-Kovach K, Tuerk PW, et al.Randomized controlled trial of a nationally avail-able weight control program tailored for adultswith type 2 diabetes. Obesity (Silver Spring)2016;24:2269–227766. Saslow LR, Mason AE, Kim S, et al. An onlineintervention comparing a very low-carbohy-drate ketogenic diet and lifestyle recommenda-tions versus a plate method diet in overweightindividuals with type 2 diabetes: a random-ized controlled trial. J Med Internet Res 2017;19:e3667. Sato J, KanazawaA,Makita S, et al. A random-ized controlled trial of 130 g/day low-carbohy-drate diet in type 2 diabetes with poor glycemiccontrol. Clin Nutr 2017;36:992–100068. Trico D, Filice E, Trifiro S, Natali A. Manipulat-ing the sequence of food ingestion improves gly-cemic control in type 2 diabetic patients underfree-living conditions. Nutr Diabetes 2016;6:e22669. Yang SH, Chung HK, Lee SM. Effects of activ-ity-based personalized nutrition education ondietary behaviors and blood parameters in mid-dle-aged and older type 2 diabetes Korean outpa-tients. Clin Nutr Res 2017;5:237–24870. Hu FB. Globalization of diabetes: the role ofdiet, lifestyle, and genes. Diabetes Care 2011;34:1249–125771. Kwasnicka D, Dombrowski SU, White M,Sniehotta F. Theoretical explanations for mainte-nance of behaviour change: a systematic reviewof behaviour theories. Health Psychol Rev 2016;10:277–29672. Hartmann-Boyce J, Johns DJ, Jebb SA,Aveyard P; Behavioural Weight Management Re-view Group. Effect of behavioural techniques anddelivery mode on effectiveness of weight man-agement: systematic review, meta-analysis andmeta-regression. Obes Rev 2014;15:598–60973. Prestwich A, Kellar I, Parker R, et al. How canself-efficacy be increased? Meta-analysis of die-tary interventions. Health Psychol Rev 2014;8:270–28574. Avery KN, Donovan JL, Horwood J, Lane JA.Behavior theory for dietary interventions for can-cer prevention: a systematic review of utilizationand effectiveness in creating behavior change.Cancer Causes Control 2013;24:409–42075. Bandura A. Social Foundations of Thoughtand Action: A Social Cognitive Theory. Upper Sad-dle River, NJ, Prentice-Hall, 1986
1810 Diet Behavior Change Techniques Diabetes Care Volume 40, December 2017