Embed Size (px)
Citation preview
Diet – what helps? Lindsey Allan
Macmillan Oncology Dietitian
Royal Surrey County Hospital, Guildford

Diet and cancer…
Diet and cancer…

Nutrition research
Lack of funding
RCTs
Low quality
Small sample sizes
Heterogenous populations
Various treatment types and intent

Dietary management
NOT a cure!
Supportive
Reduce delays in treatment
Dependent on:
Site of tumour
Cancer symptoms
Treatment side effects
Reduced intake
MALNUTRITION

Malnutrition: definition
‘a state of nutrition in which a deficiency or excess (or
imbalance) of energy, protein and other nutrients causes
measurable adverse effects on tissue / body form (body
shape, size and composition) and function and clinical
outcome’.
(BAPEN, 2016)
‘lack of proper nutrition, caused by not having enough to
eat, not eating enough of the right things, or being unable
to use the food that one does eat.’
(Oxford English Dictionary)

Cancer related malnutrition: definition
Reduced intake
Metabolic derangements
Increased resting energy expenditure
Can affect 50% patients
Increased in certain tumour sites
Insulin resistance
Disordered fat and protein breakdown
Associated with inflammation and catabolism
CANCER CACHEXIA
Lack of response to standard nutritional interventions

Dysphagia
Diarrhoea Constipation
Fatigue
Nausea & vomiting
Malabsorption
Surgical interventions
Taste changes
Anorexia
Pain
Medication
Restricted diets
Cancer associated malnutrition: causes
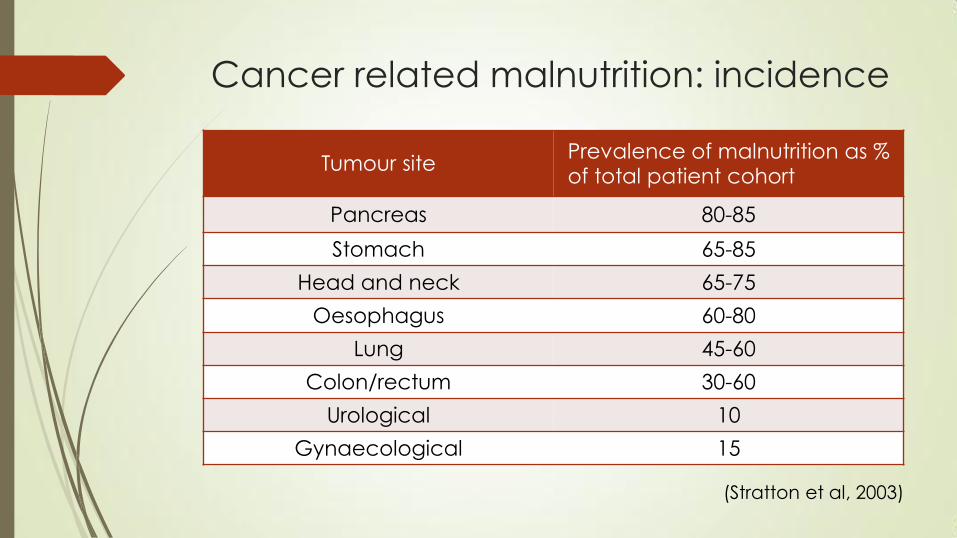
Cancer related malnutrition: incidence
Tumour site Prevalence of malnutrition as % of total patient cohort
Pancreas 80-85
Stomach 65-85
Head and neck 65-75
Oesophagus 60-80
Lung 45-60
Colon/rectum 30-60
Urological 10
Gynaecological 15
(Stratton et al, 2003)
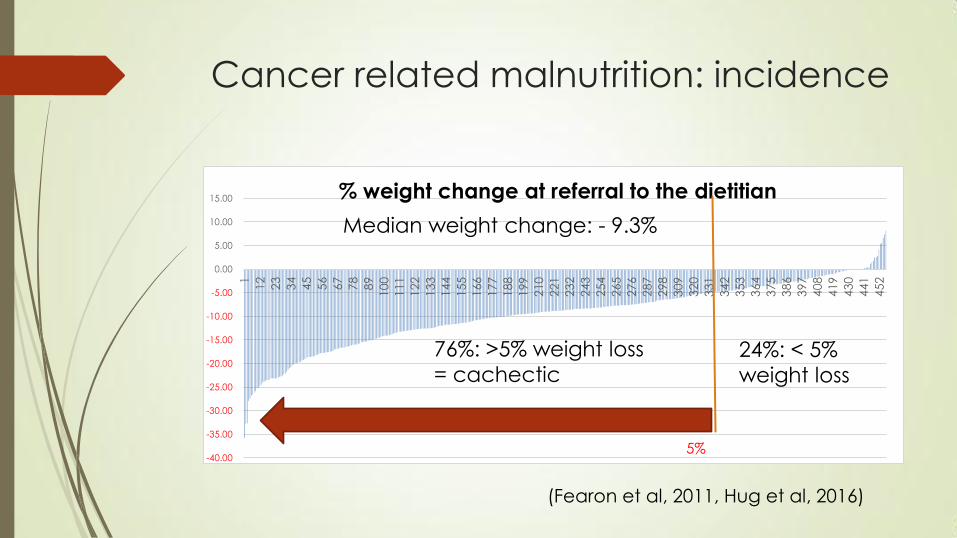
Cancer related malnutrition: incidence
-40.00
-35.00
-30.00
-25.00
-20.00
-15.00
-10.00
-5.00
0.00
5.00
10.00
15.00
1
12
23
34
45
56
67
78
89
100
111
122
133
144
155
166
177
188
199
210
221
232
243
254
265
276
287
298
309
320
331
342
353
364
375
386
397
408
419
430
441
452
% weight change at referral to the dietitian
5%
Median weight change: - 9.3%
76%: >5% weight loss
= cachectic 24%: < 5%
weight loss
(Fearon et al, 2011, Hug et al, 2016)

Cancer related malnutrition:
consequences
Impaired response to chemotherapy
Reduced quality of life
Increased chemotherapy-induced toxicity
Chemotherapy dose reductions
Stop or delay to treatment
Post-operative complications
Shorter overall survival and mortality rates

Cancer related malnutrition:
consequences
-40.00
-35.00
-30.00
-25.00
-20.00
-15.00
-10.00
-5.00
0.00
5.00
10.00
15.00
1
12
23
34
45
56
67
78
89
100
111
122
133
144
155
166
177
188
199
210
221
232
243
254
265
276
287
298
309
320
331
342
353
364
375
386
397
408
419
430
441
452
Weight loss from usual body weight to referral
5%
OS: 299 days OS: 199 days
Unpublished data from RSCH audit

ESPEN Guidelines on nutrition in
cancer patients
Identify, prevent and treat reversible malnutrition in adult
cancer patients
ALL cancers
Nutritional therapy
Physical therapy
Drug management
Strong recommendations
low level of evidence
Areas for future research
(Arends et al, 2016)

Screening
Early identification
Fast, cheap and sensitive
Recommendation
BMI, weight loss history and nutritional intake
Body Mass Index (BMI)
Height to weight ratio
Healthy range: 19.5-25 kg/m2
Lacks sensitivity
Fluid shifts
Obesity and malnutrition
Lung audit: median BMI 23 kg/m2

BMI

Screening
Weight loss history
Major cause of morbidity and mortality (Andreyev et al, 1998)
Accurate indicator of malnutrition
Reliance on personal recall
Nutritional intake
Under / over reporting
Fear of delays
Challenging with treatment cycles

Screening tools
Not mandatory in the UK
No consensus
Most not validated in oncology
MUST
BMI, weight loss, acute disease score
PG-SGA
Validated in oncology outpatients
Weight loss, symptoms AND side effects
No correlation between MUST and PG-SGA

Screening: what works?
Weight loss history
At diagnosis
Repeated during treatment
Subjective assessment
Check symptoms and side effects
Ask questions
Nutrition support: aims
Meet nutritional requirements
Improve nutritional status
When to initiate?
Consensus (Fearon et al, 2011)
On identification
As early as possible post diagnosis
Severe malnutrition / cachexia are irreversible

Nutrition support
Determining route of nutrition:
oral +/- oral nutritional supplements
enteral feeding
parenteral nutrition
Ensuring nutritional needs are met
Food fortification
Texture modification
Timing of meals
Dietary counselling
Treatment of symptoms and side effects

Nutrition support: recommendation
‘nutritional intervention to increase oral intake in cancer patients
who are able to eat but who are malnourished or at risk of
malnutrition. This includes dietary advice, the treatment of
symptoms and derangements impairing food intake (nutrition
impact symptoms) and offering oral nutritional supplements.’
(Arends, 2016)
Start artificial nutrition
No food > 1 week
<60% intake for > 1-2 weeks

Nutrition support
“Can you eat to beat cancer with the best cancer diet
and cancer nutrition?
And is it the sugar-ladened, cheeseburger, cake, biscuits
and milkshake diet that NHS dieticians, Cancer Research
UK and Macmillan suggest?”
Cancer Active

Oral Nutritional Supplements: evidence
Oral nutritional supplements (ONS)
Effective in severe malnutrition only
ONS and enteral feeding
No evidence to improve outcomes
Enteral feedingyyy in head & neck, oesophageal
RCTs are unethical
Observational studies
Reduced weight loss
Delays in treatment
Hospitalization

Parenteral nutrition: evidence
Bowel obstruction / peritoneal carcinomatosis
Expensive
Risks outweigh benefits
Observational study (Fan, 2007)
Malignant GI obstruction, n=115
No oral intake, Home PN
Median survival: 6.5 months
N=11: > 1yr, n=2: > 4 years
Prognosis < 2 months: home PN not recommended
No evidence to improve QoL

Dietary counselling: evidence
Systematic review (Baldwin et al, 2012)
nutritional counselling +/-ONS vs routine care
13 RCTs, n=1414
Mixed results
Increase in body weight, QoL
No impact on overall survival
Dietary counselling: evidence
RCT n=61 (Poulsen et al, 2014)
Intensive counselling by a dietitian vs ad-hoc input from nursing staff
gynaecological, gastric and oesophageal cancer
Weight loss 38% in intervention group, 72% in control
QoL: no difference
RCT n=58 (Uster et al, 2013)
Intensive counselling by a dietitian vs standard care
Increased protein and energy intake
no improvement in QOL, functional status or nutritional status

Dietary counselling: evidence
Systematic review (Lee et al, 2016)
Counselling, ONS and counselling, ONS, tube feeing
11 RCTs, n=1017
Lung, stomach, head & neck, colorectal
Counselling improved energy and protein intake and QoL
No improvements with ONS and tube feeding
No evidence?
Reduction in energy intake or fasting
Ketogenic diets
Cannabis to improve taste changes or appetite
Steroids to increase muscle mass
corticosteroids to aid anorexia
improves dietary intake and quality of life. (Yavuzsen et al, 2005)
No evidence?
Omega-3 fish oils to treat cancer cachexia
weak evidence: fish oil supplements can increase appetite,
energy intake, total body weight and lean muscle mass
(Sanchez-Lara et al, 2014)
Probiotics to reduce the effects radiotherapy-induced
diarrhoea – YET
Inconclusive studies to date
May improve symptoms

Cancer survivors: recommendations
Cancer prevention
1/3 of 13 most common cancers (WCRF)
1 in 10 cancers (Cancer Research UK)
Cancer survivors = cancer prevention (WCRF, Arends et al, 2016)
Healthy body weight with a BMI of 18.5-25 kg/m2
Healthy lifestyle
Physical activity
Healthy diet high in fruit, vegetables, whole grains and low in saturated fat, red meat and alcohol

Cancer survivors: evidence
Lack of evidence
Obesity and metabolic syndrome: independent risk factors of recurrence
breast cancer (Azrad & Demark-Wahnefried, 2014)
gastric cancers post gastrectomy (Kim et al, 2014)
Motivation for behaviour change
Observational study (n=16,282)
cancer survivors: ↑fruit and vegetables, ↓ physical activity (Wang et al, 2014)
Cross-sectional study (n=63,662)
Prostate cancer survivors: ↑fruit and vegetables, → obesity, physical activity (Rogers et al, 2008)

Living with and beyond
Healthy eating, healthy weight
Physical activity
but
Nutrition support
Weight loss
Dysphagia
Enteral feeding
Late effects

Summary
Strong recommendations
Low level evidence
Screening
Early identification
Timely, appropriate nutrition support
Dietary counselling
Meet nutritional requirements
Resolve symptoms and side effects
Prevent deferral of treatment

BUT…..
Cancer is not just physical
Psychological effects
Emotional responses
Reduced food intake is about MORE than just malnutrition
Loss of appetite leads to
loss of control
change in appearance
depression, anxiety
Frailty
Conflict
social isolation
Poor QOL
Remember…
Food is HOPE
Food is CONTROL
What is our responsibility?
Support patients’ beliefs
In spite of lack of evidence
Individualized advice
Address expectations
listen to priorities






























