Embed Size (px)
Citation preview

!
!
!
A!Balancing!act!DIRECT'ORAL'ANTICOAGUALANTS'(DOACS)'
AND'ANTIPLATELET'THERAPY'IN'ATRIAL'
FIBRILLATION'PATIENTS'UNDERGOING'PCI''
'
September'28,'2018'
Pharmacotherapy'Rounds'
'
Olivia'Collado,'PharmD'
PGY1'Pharmacy'Resident'
Central'Texas'Veterans'Healthcare'System'
' '

9/21/2018
1
A BALANCING ACT:DIRECT ORAL ANTICOAGULANTS (DOACS) AND ANTIPLATELET THERAPY IN ATRIAL FIBRILLATION PATIENTS UNDERGOING PERCUTANEOUS CORONARY INTERVENTION (PCI)Olivia M. Collado
PGY1 Pharmacy ResidentCentral Texas Veterans Healthcare System
September 28, 2018
Disclosures
• No conflicts of interest to disclose.
2
Objectives
1. Explain the challenge of balancing antiplatelet therapy and anticoagulant use in this patient population
2. Review available literature regarding dual and triple therapy with DOACs for antithrombotic strategies
3. Describe current guideline recommendations for specific regimens and duration
3
Patient case
• SH is a 66 yo M that presents with worsening chest pain during a fire drill at Dunder Mifflin Paper Company
• Transferred to emergency department with non-elevated troponin and admitted for NSTEMI and possible PCI
• PMH & Medications • Dyslipidemia: atorvastatin 40 mg daily• HTN (controlled): losartan 100 mg daily, amlodipine 5 mg daily• Diabetes: metformin 1000 mg twice daily, aspirin 81 mg daily • Atrial fibrillation: Dabigatran 150 mg twice daily
4
Patient case• Other pertinent information
⎯ Normal renal and liver function ⎯ No history of bleeding ⎯ No history of stroke/transient ischemic attack (TIA)⎯ Denies alcohol and tobacco use
5
Kahoot Question #1
• What is SH’s CHA2DS2VASc score ?
A. 1
B. 3
C. 2
D. 4
6

9/21/2018
2
Kahoot Question #2
• What is SH’s HAS-BLED score?
A. 1
B. 0
C. 2
D. 3
7
Patient case• SH is taken for cardiac catheterization
⎯ 80% stenosis in mid-LAD and stented with drug-eluting stent (DES)
• How do we manage his antithrombotic therapy?
⎯ Stent thrombosis prevention: antiplatelet therapy⎯ Atrial fibrillation (AF): oral anticoagulation
8
9
Background
9 10
Atrial Fibrillation
10
Atrial fibrillation
⎯ Most common heart arrhythmia
⎯ Affects ~ 7 million US, especially the elderly
⎯ Increase stroke risk by 4-5 X and mortality 2 X
11Andrade J, et al. Circ Res. 2014; 114 (9): 1453-1468.January CT, et al. Jour Am Coll Cardio. 2014; 64 (21): 2246-2280.
CHEST 2018 Guidelines
• Atrial fibrillation (Strong recommendations)
⎯ Oral anticoagulation• CHA2DS2VASc score > 1 male or > 2 female
⎯ HAS-BLED score
⎯ DOACs over vitamin K antagonist (VKA)
⎯ If VKA with time in therapeutic range (TTR) < 65%, switch to DOAC
12Gregory YH, et al. Chest. 2018; (18): 32244

9/21/2018
3
Kahoot Question #3
• What are some advantages of DOACs over warfarin for stroke prevention in non-valvular atrial fibrillation?
A. Standard dosing
B. No need for routine lab monitoring
C. Fewer drug interactions
D. All of the above
13
Chest 2018 Guidelines
14
Dabigatran Rivaroxaban Apixaban EdoxabanMechanism of action
Direct thrombin inhibitor
Factor Xa inhibitor
Factor Xa inhibitor
Factor Xa inhibitor
Approved dose for stroke prevention
150 mg twice daily75 mg twice daily
20 mg/d15 mg/d
5 mg twice daily2.5 mg twice daily
60 mg/d30 mg/d
Major bleedingStroke/SE Non-inferior
Gregory YH, et al. Chest. 2018; (18): 32244
150 mg 60 & 30 mg
150 mg 60 mg
15
Percutaneous coronary intervention (PCI)
15
Percutaneous coronary intervention
• Indicated for ACS or unstable angina
• Types of stents⎯ Bare-metal stents⎯ Drug-eluting stents
• Femoral and radial artery access• Complications
⎯ Stent thrombosis ⎯ Restenosis
16Bokhari S, et al. Cardiac catheterization. 2017
Kahoot Question #4
In general, what is appropriate DAPT therapy for ACS after PCI?
A. Aspirin 81 mg lifelong + warfarin; 12 mo
B. Aspirin 81 mg lifelong + clopidogrel 75 mg daily; 12 mo
C. Aspirin 81 mg lifelong + clopidogrel 75 mg daily; 6 mo
D. Aspirin 81 mg monotherapy lifelong; 6 mo
17
2016 ACC/AHA Dual antiplatelet therapy (DAPT) duration post-PCI
Levine GN, et al. 2016 ACC/AHA Guideline. J Am Coll Cardiol 2016; 68: 1082.
• ACS• Dual antiplatelet therapy after bare metal stent (BMS)/DES• Continue P2Y12 inhibitor for at least 12 mo (Class I)
• Clopidogrel• Prasugrel• Ticagrelor
• Low dose aspirin indefinitely• >12 mo if low bleed risk/ no bleed complication (Class IIb)
• Use DAPT score
18

9/21/2018
4
Antiplatelet agents
19
Aspirin Clopidogrel Prasugrel TicagrelorMOA Irreversible
inhibition of COX 1-2, PGs, TXA2
P2Y12 inhibitor
Dose 75-100 mg/d L: 600 mgM: 75 mg/d
L: 60 mgM: 10 mg/d
L: 180 mgM: 90 mg twice daily
2C19? Y* Y^ NInhibition Irreversible Irreversible Reversible Bleed + ++ ++*= sensitive to polymorphisms and drug interactions^= less sensitive to polymorphisms and drug interactionsCOX: Cyclooxygenase; PGs: prostaglandings; TXA2 : Thromboxane A2
Levine GN, et al. 2016 ACC/AHA Guideline. J Am Coll Cardiol 2016; 68: 1082. 20
AF & ACS Crossover
20
AF & ACS Crossover
21
ACS/Stenting
1-2 million people
Atrial Fibrillation~ 7 million
people
Stent + Afib20-30%
Lip GY, et al. Thromb Haemost. 2010; 103: 13-28.
A Balancing Act
22
Bleeding
Stent thrombosis & thromboembolic event prevention
Anticoagulation + Dual Antiplatelet
Conventional Standard-Triple Therapy
23Hansen MI, et al. Arch Intern Med 2010;170: 1433-1441.
Conventional Standard-Triple Therapy
24Hansen MI, et al. Arch Intern Med 2010;170: 1433-1441.

9/21/2018
5
25
Clinical QuestionAre there alternative treatment options other than triple therapy with warfarin for atrial fibrillation patients requiring oral anticoagulation undergoing PCI?
25 26
Trial Evidence
26
27
Trials
27
Dual and triple therapy with
warfarin
WOEST
ISAR-TRIPLE
Dual and triple therapy with
DOACs
PIONEER AF-PCI
RE-DUAL PCI
28
Use of clopidogrel with or without aspirin in patients taking oral
anticoagulant therapy and undergoing percutaneous coronary intervention: an open-label, randomized, controlled trial
28
WOEST Trial (2013)
Intro Methods Results Conclusion
Dewilde W, et al. Am Heart J. 2009; 158 (5): 713-718.
29
Intro Methods Results Conclusion
• Inclusion criteria⎯ 18-80 yo, indication for OAC and PCI
• Treatment groups⎯ Triple therapy (TT): warfarin, clopidogrel, aspirin ⎯ Dual therapy (DT): warfarin, clopidogrel
• Primary endpoint⎯ Bleeding episode within 1 year of PCI
• Secondary endpoint⎯ Composite of death, myocardial infarction (MI), stroke,
target vessel revascularization (TVR), and stent thrombosis (ST)
Dewilde W, et al. Am Heart J. 2009; 158 (5): 713-718. 30
Primary Endpoint: Bleeding episode within 1 year of PCI
Intro Methods Results Conclusion
Secondary Endpoint: Composite of death, MI, stroke TVR, and ST
HR 0.36 (95% CI 0.26-0.60) p< .0001
HR 0.60 (95% CI 0.38-0.94) p=0.025
Dewilde W, et al. Am Heart J. 2009; 158 (5): 713-718.

9/21/2018
6
31
Authors’ Conclusion
Intro Methods Results Conclusion
• Compared to triple therapy with warfarin:
• Dual therapy with clopidogrel and OAC causes less bleeding
• Dual therapy with clopidogrel and OAC did not increase thrombotic events
Dewilde W, et al. Am Heart J. 2009; 158 (5): 713-718. 32
Trials
Dual and triple therapy with
warfarin
WOEST
ISAR-TRIPLE
Dual and triple therapy with
DOACs
PIONEER AF-PCI
RE-DUAL PCI
33
Duration of Triple Therapy in Patients Requiring Oral Anticoagulation After
Drug-Eluting Stent Implantation
ISAR-TRIPLE (2015)
Intro Methods Results Conclusion
Fiedler KA, et al. J Am Coll Cardiol. 2015; 65 (16): 1619-1629. 34
Intro Methods Results Conclusion
• Inclusion criteria⎯ OAC at least 12 mo. and DES for ACS or stable angina
• Treatment groups⎯ 6 week clopidogrel or 6 mo. clopidogrel
• Primary endpoint⎯ Composite of death, MI, stroke, ST, Thrombolysis in
myocardial infarction (TIMI)-bleeding• Secondary endpoint
⎯ Composite of cardiac death, MI, ST, or ischemic stroke
Fiedler KA, et al. J Am Coll Cardiol. 2015; 65 (16): 1619-1629.
35
Primary Endpoint: Composite of death, MI, stroke, ST, TIMI-bleeding
Intro Methods Results Conclusion
Secondary Endpoint: Composite of cardiac death, MI, ST, or ischemic stroke
HR 1.14 (95% CI 0.68-1.91) p=0.63
HR 0.93 (95% CI 0.43-2.05) p=0.87
Fiedler KA, et al. J Am Coll Cardiol. 2015; 65 (16): 1619-1629. 36
Authors’ Conclusion
Intro Methods Results Conclusion
• Six weeks of clopidogrel not superior to 6 months in patients taking concomitant aspirin and OAC
• Physicians should weigh the ischemic and bleed risk when choosing triple therapy duration
Fiedler KA, et al. J Am Coll Cardiol. 2015; 65 (16): 1619-1629.
9/21/2018
7
37
Trials
Dual and triple therapy with
warfarin
WOEST
ISAR-TRIPLE
Dual and triple therapy with
DOACs
PIONEER AF-PCI
RE-DUAL PCI
38
Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI
PIONEER AF-PCI (2016)
Intro Methods Results Conclusion
Gibson CM, et al. N Engl J Med. 2016; 375 (25): 2423-2434.
39
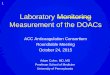
Intro Methods Results Conclusion
• Inclusion criteria⎯ > 18 yo with nonvalvular AF & undergone PCI with stent
• Treatment groups1. Rivaroxaban 15 mg/d + clopidogrel2. Rivaroxaban 2.5 mg/d + clopidogrel+asa3. Warfarin+clopidogrel+asa
• Primary endpoint⎯ Clinically significant bleeding
• Secondary endpoint⎯ Composite death from cardiovascular (CV) causes, MI, stroke
Gibson CM, et al. N Engl J Med. 2016; 375 (25): 2423-2434. 40
Primary Endpoint: Clinically significant bleeding
Intro Methods Results Conclusion
Secondary Endpoint: Composite of death from CV causes, MI, stroke
Group 1 vs 3 HR 0.59 (95% CI 0.47-0.76) p=<0.001
Group 2 vs 3 HR 0.63 (95% CI 0.50-0.80) p=<0.001
Group 1 vs 3 HR 1.08 (95% CI 0.69-1.68) p=0.75
Group 2 vs 3 HR 0.93 (95% CI 0.59-1.48) p=0.76
Gibson CM, et al. N Engl J Med. 2016; 375 (25): 2423-2434.
41
Authors’ Conclusion
Intro Methods Results Conclusion
• Compared to triple therapy with warfarin,
• Both rivaroxaban treatment groups are associated with significant reduction in bleeding
• Both rivaroxaban treatment groups not associated with increased risk of MACE
Gibson CM, et al. N Engl J Med. 2016; 375 (25): 2423-2434.
PIONEER AF-PCI: Pros & Cons
42
Pros Cons• First to compare
DOAC regimen to triple therapy
• Open-label trial; small number of efficacy endpoints
• Lost 0 patients to follow-up
• Very-low-dose rivaroxaban
• Bleeding outcomes consistent across all criteria
• Little ethnic diversity

9/21/2018
8
43
Trials
Dual and triple therapy with
warfarin
WOEST
ISAR-TRIPLE
Dual and triple therapy with
DOACs
PIONEER AF-PCI
RE-DUAL PCI
44
Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation
RE-DUAL PCI (2017)
Intro Methods Results Conclusion
Cannon MD, et al. N Engl J Med. 2016; 375 (25): 2423-2434.
45
Intro Methods Results Conclusion
• Inclusion criteria⎯ > 18 yo with nonvalvular AF & undergone PCI with BMS or DES
• Treatment groups1. Dabigatran 110 mg twice daily + clopidogrel/ticagrelor2. Dabigatran 150 mg twice daily + clopidogrel/ticagrelor3. Warfarin+clopidogrel+asa
• Primary endpoint⎯ ISTH major or clinically relevant non-major bleeding event
• Secondary endpoint⎯ MACE
Cannon MD, et al. N Engl J Med. 2016; 375 (25): 2423-2434.46
Primary Endpoint: International society for thrombosis and hemostasis (ISTH) major or clinically relevant non-major bleeding event
Intro Methods Results Conclusion
Secondary Endpoint: Major adverse cardiac event (MACE)
Dual Therapy 110 mg HR 0.52 (95% CI 0.42-0.63) p=<0.001
Dual Therapy 150 mg HR 0.72 (95% CI 0.58-0.88) p=<0.002
Combined Dabigatran Dual TherapyHR 1.04 (95% CI 0.84-1.29) p=0.005 noninferiority
Cannon MD, et al. N Engl J Med. 2016; 375 (25): 2423-2434.
47
Authors’ Conclusion
Intro Methods Results Conclusion
• Compared to triple therapy with warfarin,
• Dual therapy with dabigatran and a P2Y12inhibitor was associated with significantly lower risk of bleeding events
• Dual therapy with dabigatran and a P2Y12inhibitor was non-inferior regarding thromboembolic events
Cannon MD, et al. N Engl J Med. 2016; 375 (25): 2423-2434.
RE-DUAL PCI: Pros & Cons
48
Pros Cons• Both endpoints met
noninferiority • Open-label
• Study used standard dose for stroke prevention at 150 mg twice daily
• Small number of secondary efficacy endpoints
• Bleeding outcomes consistent across subgroups
• Long follow-up for VKA triple therapy

9/21/2018
9
Dual Therapy vs. Triple Therapy: Meta-Analysis
Overall Hazard Ratio (95% CI)
DAT arm TAT arm
TIMI major/minor bleeding
0.53 (0.36, 0.85) 130/3026 206/229
Stent thrombosis 1.00 (0.32, 2.82) 31/3024 21/2267Stroke 0.94 (0.45, 1.84) 39/3024 30/2267
Golwala HB, et al. Europ Heart Jour. 2018; 39: 1726-1735. 49
WOEST ISAR-TRIPLE
PIONEER AF-PCI
RE-DUAL PCI
Dual Therapy vs. Triple Therapy: Meta-Analysis
• Critique• Caution interpreting efficacy outcomes• Different baseline characteristics• Varying trial designs
• Conclusion
Dual therapy with OAC and a single antiplatelet may be a better option than triple therapy with warfarin and dual antiplatelet in many patients with atrial fibrillation following PCI.
Golwala HB, et al. Europ Heart Jour. 2018; 39: 1726-1735. 50
51
Future DOAC Dual Therapy Trials
DOAC Trials
52
Rivaroxaban(PIONEER AF-
PCI) 2015
Dabigatran(RE-DUAL PCI)
2016
Apixaban (AUGUSTUS) END 12/2018
53
A Study of Apixaban in Patients With Non-valvular Atrial Fibrillation With
High Thrombosis Risk Due to Having Had a Recent Coronary Event, Such as a
Heart Attack or a Procedure to Open the Vessels of the Heart
AUGUSTUS (ongoing)
AUGUSTUS (2018). Clinical Trials (Identification No. NCT02415400). 54
• Inclusion criteria⎯ AF (prior, persistent, >6 hr duration) with ACS and/or PCI with
planned P2Y12 inhibitor for 6 months ⎯ Physician decision that OAC is indicated
• Treatment groups1. Apixaban 5 mg twice daily with aspirin or placebo 2. Warfarin with aspirin or placebo
• Primary endpoint⎯ Major/clinically relevant bleeding (through 6 months)
• Secondary endpoint⎯ Death, MI, stroke, ST
ENTRUST-AF-PCI (2018). Clinical Trials (Identification No. NCT02866175).
AUGUSTUS, continued

9/21/2018
10
DOAC Trials
55
Rivaroxaban(PIONEER AF-PCI)
2015
Dabigatran(RE-DUAL
PCI) 2016
Apixaban (AUGUSTUS)
END 12/2018
Edoxaban(ENTRUST
AF-PCIEND 3/2019
56
Edoxaban Treatment Versus Vitamin K Antagonist in Patients With Atrial
Fibrillation Undergoing PCI
ENTRUST-AF-PCI (ongoing)
ENTRUST-AF-PCI (2018). Clinical Trials (Identification No. NCT02866175).
57
• Inclusion criteria⎯ OAC for AF X 12 mo. and PCI with stent placement
• Treatment groups1. Edoxaban 60 mg daily + P2Y12 antagonist 2. Warfarin + P2Y12 antagonist + asa 1-12 mo.
• Primary endpoint⎯ ISTH major and clinically relevant non-major bleeding
ENTRUST-AF-PCI (2018). Clinical Trials (Identification No. NCT02866175).
ENTRUST AF-PCI, continued
58
Current Guideline Recommendations
59
2018 Guideline Recommendations
EHRACHESTAHA
2018 AHA North American Consensus White PaperManagement of AF patients requiring OAC undergoing PCI
2018 Expert ConsensusChoice of anticoagulant
DOAC preferredIf VKA, INR 2-2.5OAC life-long
Choice of P2Y12inhibitor
Clopidogrel is the P2Y12 inhibitor of choice; ticagrelor if high ischemic/low bleed risk Prefer clopidogrel over aspirin
Strategy (double vs triple)
Dual therapy after hospital discharge Consider triple therapy X 1 mo if high ischemic/low bleed risk
Angiolillo DJ, et al. Circulation (2018). 60

9/21/2018
11
2018 AHA North American Consensus White PaperManagement of AF patients requiring OAC undergoing PCI
Angiolillo DJ, et al. Circulation (2018). 61 62
2018 Guideline Recommendations
EHRACHESTAHA
2018 Updated CHEST Antithrombotic Guidelines
63
AF requiring OAC with ACS undergoing PCI Choice of anticoagulant
VKA TTR > 65-70% (INR 2-3) ORDOAC at stroke prevention dose Less bleeding with DOACs
Choice of P2Y12inhibitor
OAC with:• Low dose aspirin (ASA) + proton pump
inhibitor (PPI)• Clopidogrel preferred P2Y12 inhibitor
Gregory YH, et al. Chest. 2018; (18): 32244
2018 Updated CHEST Antithrombotic Guidelines
Gregory YH, et al. Chest. 2018; (18): 32244
Management of AF patients presenting with ACS requiring OAC undergoing PCI/stenting
(Weak Recommendations)
64
HAS-BLED 0-2 HAS-BLED >3Triple therapy X 6 mo. Triple therapy X 1-3 mo.
Dual therapy up to 12 mo. Dual therapy up to 12 mo.
OAC life-long OAC life-long
Triple therapy: OAC + aspirin/P2Y12-IDual therapy: OAC + P2Y12-I
65
2018 Guideline Recommendations
EHRACHESTAHA
2018 Joint European Consensus
2018 Joint European Consensus. Europace. 2018. 66

9/21/2018
12
67
Key take home points
Key take home points, continued
• Dual therapy with a OAC + P2Y12-I preferred over triple therapy with warfarin in patients with AF + ACS
• Clopidogrel preferred • DOACs preferred over warfarin
• Rivaroxaban 15 mg once daily • Dabigatran 150 mg BID
68
Key take home points, continued
69
1. Triple therapy with aspirin 81mg daily is used until hospital discharge. 2. For bleeding risk use HAS-BLED score: Low risk = 0-2, high risk = 3-4, very high risk >4.3. High atherothrombotic risk: For elective PCI use SYNTAX score; for ACS, GRACE score >140; stenting of the left
main, proximal LAD, proximal bifurcation; recurrent MIs; stent thrombosis etc. 4. DOAC is preferred over warfarin unless CI. Clopidogrel is preferred P2Y12 inhibitor; ticagrelor may be considered
in patients in at high thrombotic and low bleeding risk, avoid prasugrel.
Low Bleed Risk High Bleed Risk Very High Bleed RiskNormal Athero-thromboticRisk
• Triple therapy 1-3 mo. OR
• Dual therapy with OAC + P2Y12-I up to 12 mo.
• OAC lifelong
• Triple therapy 1 mo.• Dual therapy with OAC
+P2Y12-I up to 12 mo.• OAC lifelong
• Dual therapy with OAC + P2Y12-I up to 12 mo.
• OAC lifelong
High Athero-thromboticRisk
• Triple therapy 1-6 mo. • Dual therapy with OAC
+ P2Y12-I up to 12 mo. • OAC lifelong
• Triple therapy 1-3 mo.• Dual therapy with OAC
+ P2Y12-I up to 12 mo.• OAC lifelong
• Triple therapy 1 mo.• Dual therapy with OAC
+ P2Y12-I up to 12 mo.• OAC lifelong
70
Patient Case Recap
Patient Case Recap, continued
71
AF+ NSTEMI
PCIDES Discharge
Kahoot Question #5• At discharge, what medication regimen is most appropriate
for SH, considering bleed and ischemic risk?
A. Warfarin (INR 2-3) + aspirin 81 mg + clopidogrel 75 mg daily; 1 mo
B. Rivaroxaban 20 mg daily + clopidogrel 75 mg daily ; 12 mo
C. Dabigatran 150 mg twice daily + aspirin 81 mg + clopidogrel 75 mg daily; 6 mo
72

9/21/2018
13
Key take home points, continued
73
1. Triple therapy with aspirin 81mg daily is used until hospital discharge. 2. For bleeding risk use HAS-BLED score: Low risk = 0-2, high risk = 3-4, very high risk >4.3. High atherothrombotic risk: For elective PCI use SYNTAX score; for ACS, GRACE score >140; stenting of the left
main, proximal LAD, proximal bifurcation; recurrent MIs; stent thrombosis etc. 4. DOAC is preferred over warfarin unless CI. Clopidogrel is preferred P2Y12 inhibitor; ticagrelor may be considered
in patients in at high thrombotic and low bleeding risk, avoid prasugrel.
Low Bleed Risk High Bleed Risk Very High Bleed RiskNormal Athero-thromboticRisk
• Triple therapy 1-3 mo. OR
• Dual therapy with OAC + P2Y12-I up to 12 mo.
• OAC lifelong
• Triple therapy 1 mo.• Dual therapy with OAC
+P2Y12-I up to 12 mo.• OAC lifelong
• Dual therapy with OAC + P2Y12-I up to 12 mo.
• OAC lifelong
High Athero-thromboticRisk
• Triple therapy 1-6 mo. • Dual therapy with OAC
+ P2Y12-I up to 12 mo. • OAC lifelong
• Triple therapy 1-3 mo.• Dual therapy with OAC
+ P2Y12-I up to 12 mo.• OAC lifelong
• Triple therapy 1 mo.• Dual therapy with OAC
+ P2Y12-I up to 12 mo.• OAC lifelong
Acknowledgements
• Evaluator• Dr. Tamara Knight
• Preceptors
74
75
Questions?

Appendices!!!!
Appendix'A:'Figures'and'Tables'
Appendix'B:'Guideline'definitions'
Appendix'C:'Stroke'and'bleed'assessment'tools''
Appendix'D:'Abbreviations'
! !

Appendix!A.!Figures!and!Tables!
Slide'14:'Chest'2018'Guidelines'
'
!!
Slide'19:'Antiplatelet'agents'
!! !

Slide'23:'Conventional'StandardXTriple'Therapy'(Bleeding'outcomes)'
!
Slide'24:'Conventional'StandardXTriple'Therapy'(Ischemic'outcomes)'
'
'
'

Slide'60:'2018'AHA'North'American'Consensus'White'Paper'
'
Slide'61:'2018'AHA'North'American'Consensus'White'Paper'
'
'
'
'
'
'
'

Slide'63:'2018'Updated'CHEST'Antithrombotic'Guidelines'
!
Slide'64:'2018'Updated'CHEST'Antithrombotic'Guidelines'
'
' '

Slide'66:'2018'Joint'European'Consensus''
'
Slide'69:'Key'take'home'points''
!! !
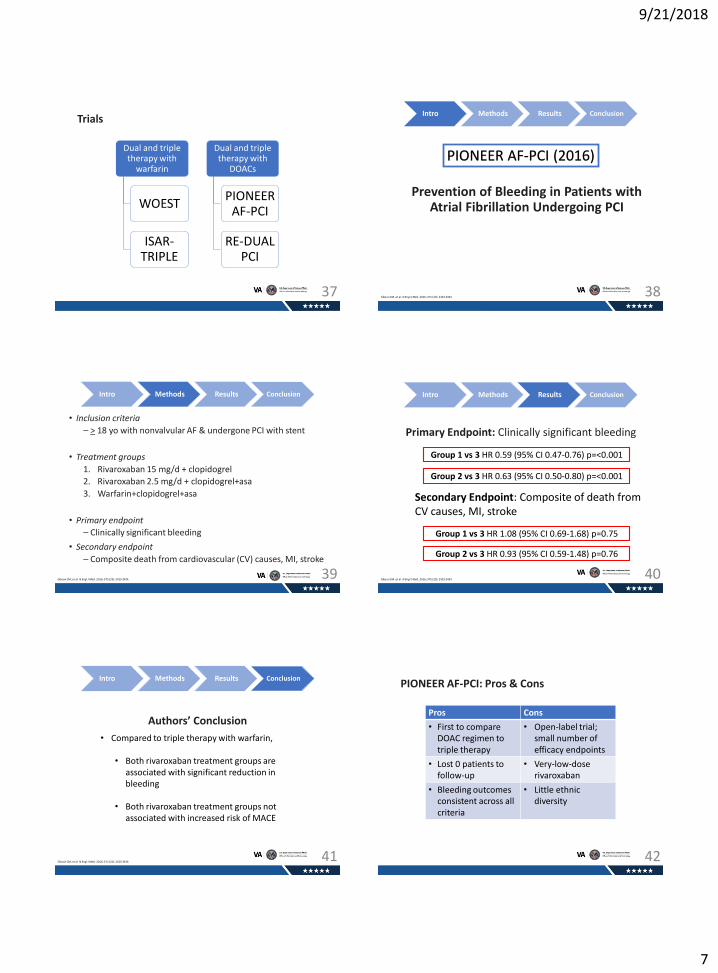
Appendix!B.!Definitions!!'
Classification'of'atrial'fibrillation''
• Paroxysmal:'terminates'spontaneously'or'with'intervention'within'seven'days'of'onset.'
• Persistent:'fails'to'selfXterminate'within'7'days;'often'requiring'pharmacologic'or'electrical'
cardioversion'to'restore'sinus'rhythm.''
• Long0standing:'lasting'for'more'than'12'months.'
• Permanent:'persistent'AF'where'a'joint'decision'by'the'patient'and'clinician'has'been'made'to'no'
longer'pursue'a'rhythm'control'strategy.''
2018'Chest'guideline'definitions'
• Unusually4high4bleed4risk:'patients'with'HASXBLED'>'3'and'recent'acute'bleeding'event.'4• High4thrombotic4risk:'left'main'stent,'multiXvessel'PCI/stenting.'
Bleeding'criteria'definitions'
'
TIMI4criteria''
TIMI!Bleeding!Criteria!Major! ICH;'Hb'drop'>'5'g/d;''Hct'drop'>15%'
Minor! Bleeding;'Hb'drop'>'3'g/d;''Hct'drop'>10%'
No'observed'blood'loss:'Hb'drop'>'4'g/dL;'Hct'drop'>'12%'
Minimal! Any'clinically'overt'sign'of'hemorrhage'associated'with'Hb'drop'<3'g/dL'or'Hct'
drop'<9%'
'
BARC4bleeding4criteria4
BARC!Bleeding!Type!1! Not'actionable,'does'not'cause'unscheduled'studies,'hospitalization,'or'treatment;'may'
include'episodes'leading'to'selfXdiscontinuation'of'medical'therapy'
Type!2! Any'overt,'actionable'sign'of'hemorrhage'that'does'not'fit'the'criteria'for'types'3,4,'or'5'
but'does'meet'>'1'of'the'following'criteria:'(1)'requiring'nonsurgical,'medical'
intervention;'(2)'leading'to'hospitalization'or'increased'level'of'care;'or'(3)'prompting'
evaluation'
Type!3a! Overt'bleeding'+'Hb'drop'3X5'g/dL;'any'transfusion'with'overt'bleeding'
Type!3b! Overt'bleeding'+'Hb'drop'>5'g/dL;'cardiac'tamponade;'bleeding'requiring'surgical'
intervention'or'IV'vasoactive'agents''
Type!3c! ICH'(not'including'microbleeds'or'hemorrhagic'transformation,'does'include'intraspinal)''
Subcategories'confirmed'by'autopsy'or'imaging'or'lumbar'puncture''
Intraocular'bleed'compromising'vision''
Type!4! CABG'bleeding'
Type!5! Fatal'bleeding''
'
'
'

ISTH4
ISTH!Bleeding!Definitions!Major!Bleeding! Fall'in'Hgb'>'2'g/dl,'or'transfusion'of'>'2'units'of'PRBC'or'
whole'blood,'or'that'occurs'in'a'critical'location'i.e.'
intracranial,'or'that'causes'death'
Clinically!Relevant!NonIMajor!Bleeding! Does'not'meet'criteria'for'major'bleeding'that'requires'any'
medical'or'surgical'intervention'to'treat'the'bleeding'
'
GUSTO44
GUSTO!Bleeding!Severe! ICH;'bleeding'that'causes'hemodynamic'compromise'and'requires'intervention'
Moderate! Bleeding'requiring'transfusion'but'does'not'lead'to'hemodynamic'instability''
Mild! Bleeding'that'does'not'meet'criteria'for'severe'or'moderate'bleeding'
'
'
'
'
'
'
'
'
'
'
'
'
'
'
'
'
'
'
'
'
Chesebro'JH,'et'al.'Circulation.'1987;'76:'142X154.''GUSTO'Investigators.'N4Engl4J4Med.'1993;'329:'673X682.''Mehran'R,'et'al.'Circulation.'2011;'123:'2736X2747.''Gregory'LH,'et'al.'Antithrombotic'Therapy'for'Atrial'Fibrillation:'CHEST'guideline'and'Expert'Panel'Report.'2018.'Chest4Journal.'! '

Appendix!C.!Ischemic!or!atherothrombotic!risk!and!bleed!assessment!tools!'
CHA2DS20VASc4score44
Congestive!heat!failure! !sign/symptoms+of+heart+failure+or+objective+evidence+of+reduce+left8ventricular+ejection+fraction++
+1!
Hypertension'Resting+blood+pressure+>+140/90+mmHg+on+at+least+2+occasions+or+current+antihypertensive+treatment++
+1'
Age'>75+
+2'
Diabetes!mellitus!Fasting+glucose+>126+mg/dL+or+treatment+with+oral+hypoglycemic+agent+and/or+insulin+
+1'
Previous!stroke,!transient!ischemic!attack,!or!thromboembolism+ +2'
Age!65I74' +1'
Sex!category!(female)' +1'
'
0='low'
1=lowXmoderate'
>2'='moderateXhigh'
HAS0BLED4
Hypertension!! !uncontrolled,+>160+mmHg+systolic+
+1!
Abnormal!liver!function'Cirrhosis+or+bilirubin+>+2+X+normal+with+AST/ALT/AP+>+3+X+normal+
+1'
Abnormal!renal!function'Dialysis,+transplant,+Cr+>+2.26+mg/dL+or+>+200+umol/L+
+1'
Stroke' +1'
Bleeding!prior+major+bleeding+or+predisposition+to+bleeding+
+1'
Labile!INR'Unstable/high+INR,+time+in+therapeutic+range+<+60%+
+1'
Elderly!>65' +1'
Drugs:!concomitant!antiplatelet!!aspirin,+clopidogrel,+NSAIDS+
+1'
Drugs:!concomitant!excess!alcohol!use!'>+8+drink/+week+
+1'
'
0X2'Lo'bleed'risk'
3X4'High'bleed'risk''
>4'Very'high'bleed'risk''
'
'

DAPT4score4Predicts'patients'that'will'benefit'from'prolonged'DAPT'after'coronary'stent'placement4
Age!>+75++65874+<65+
!I2!I1!0!
Cigarette!smoking+Smoking+within+2+year+prior+to+index+procedure+
+1'
Diabetes!mellitus' +1'
MI!at!presentation+ +1'
Prior!PCI!or!prior!MI+ +1'
PaclitaxelIeluting!stent+ +1'
Stent!diameter!<!3!mm' +1'
CHF!or!LVEF!<!30%' +2'
Vein!graft!stent' +2'
'
X2''''''X1''''''0''''''1''''''2''''''3''''''4''''''5''''''6''''''7''''''8''''''9''
Greater'' ' ' ' ' ' Greater'
Bleed'Risk' ' ' ' ' ' Thrombotic'Risk'
Syntax4Score4Algorithm44Score'complexity'of'CAD4
Dominance!!Number!of!lesions!Segments!involved!per!lesion,!with!lesion!characteristics!!Total!occlusions!with!subtotal!occlusions:'number'of'segments,'age'of'total'
occlusions,'blunt'stumps,'bridging'collaterals,'first'segment'beyond'occlusion'visible'
by'antegrade'or'retrograde'filling,'side'branch'involvement''
Trifurcation,!number!of!segments!diseased!Bifurcation!type!and!angulation!AortoIostial!lesion!Severe!tortuosity!Lesion!length!Heavy!calcification!Thrombus!Diffuse!disease,!with!number!of!segments!!'
4
4
4
4
4

GRACE4Score''Estimates'admissionX6'month'mortality'for'patients'with'acute'coronary'syndrome'4
Age! <40=0'
49X40=18'
59X50=36'
69X60=55'
79X70=73'
>'80='81!!Killip!class! I='0'
II=21'
III=43'
IV=64'
Systolic!blood!pressure! <80=63'
99X30=58'
119X100=47'
139X120=37'
159X140=26'
199X160=11'
>200=0'
Presence!of!ST!segment!deviation!! Yes=30'
Cardiac!arrest!during!presentation! Yes=43'
Serum!creatinine!concentration! 0.0X0.39=2'
0.4X0.79=5'
0.8X1.19=8'
1.2X1.59=11'
1.6X1.99=14'
0.2X3.99=23''
>'4='31'
Presence!of!elevated!serum!cardiac!biomarkers!
Yes=15'
Heart!rate!! <70=0'
89X70=7'
109X90=13'
149X110=23''
199X150=36'
>200=46''
'
'
'
!!!!!Kumar'K,'et'al.'Overview'of'atrial'fibrillation.'In:'Post'T,'ed.'UpToDate.'Waltham,'Mass.:'UpToDate;'2018.'!Assessment'tools.''American4College4of4Cardiology.'Accessed'9/10/18.''

Appendix!D.!Abbreviations!!
ACS:'acute'coronary'syndrome'
AF:'atrial'fibrillation'
BARC:'Bleeding'academic'research'consortium'
BP:'blood'pressure''
CAD:'coronary'artery'disease''
CHF:'congestive'heart'failure''
COX:'cyclooxygenase''
CRNM:'clinically'relevant'nonmajor'bleeding''
DAPT:'dual'antiplatelet'therapy''
DES:'drugXeluting'stent''
DOACs:'DirectXacting'oral'anticoagulants''
ESC:'European'Society'of'Cardiology''
HTN:'hypertension''
INR:'international'normalized'ratio''
ISTH:'International'society'for'thrombosis'and'hemostasis'
MACE:'major'adverse'cardiac'event''
MI:'myocardial'infarction''
NVAF:'nonvalvular'atrial'fibrillation''
OAC:'oral'anticoagulation''
PCI:'percutaneous'coronary'intervention''
PG:'prostaglandins'
PUD:'peptic'ulcer'disease''
SAPT:'single'antiplatelet'therapy''
SE:'systemic'embolism''
SIHD:'stable'ischemic'heart'disease'
TIA:'transient'ischemic'attack''
TIMI:'Thrombolysis'in'Myocardial'Infarction''
TT:'triple'therapy'
TTR:'time'in'therapeutic'range'
TXA2:'Thromboxane'A2'
VKA:'vitamin'K'antagonist''
'