Embed Size (px)
Citation preview
Marc S. Levine, MDStephen E. Rubesin, MD
Published online before print10.1148/radiol.2372050199
Radiology 2005; 237:414–427
Abbreviations:AIDS ! acquired immunodeficiency
syndromeCMV ! cytomegalovirusHIV ! human immunodeficiency
virusLPO ! left posterior obliqueRAO ! right anterior oblique
1 From the Department of Radiology,Hospital of the University of Penn-sylvania, 3400 Spruce St, Philadel-phia, PA 19104. Received February 8,2005; revision requested April 7; revi-sion received April 25; accepted June2. Address correspondence to M.S.L.(e-mail: [email protected]).The authors are paid consultants forEZ-Em, Westbury, NY.© RSNA, 2005
Diseases of the Esophagus:Diagnosis withEsophagography1
The barium esophagram is a valuable diagnostic test for evaluating structural andfunctional abnormalities of the esophagus. The study is usually performed as amultiphasic examination that includes upright double-contrast views with a high-density barium suspension, prone single-contrast views with a low-density bariumsuspension, and, not infrequently, mucosal-relief views with either density of bariumsuspension. The double-contrast phase optimizes the ability to detect inflammatoryor neoplastic diseases, whereas the single-contrast phase optimizes the ability todetect hiatal hernias and lower esophageal rings or strictures. Fluoroscopic exami-nation of the esophagus is also important for assessing motility disorders such asachalasia and diffuse esophageal spasm. This article is a review of gastroesophagealreflux disease, other types of esophagitis, benign and malignant esophageal tumors,varices, lower esophageal rings, diverticula, and esophageal motility disorders, all ofwhich can be diagnosed with the aid of esophagography.© RSNA, 2005
Despite the current focus on cross-sectional imaging studies such as those of computedtomography (CT) and magnetic resonance (MR) imaging, the barium examination con-tinues to be the primary radiologic modality for the evaluation of patients with dysphagia,reflux symptoms, or other clinical findings of esophageal disease. Double-contrast esopha-grams are particularly useful for the detection of reflux disease and its complications,infectious esophagitis, esophageal carcinoma, or other structural lesions of the esophagus.The fluoroscopic portion of the examination is also useful for the assessment of esophagealmotility and detection of esophageal motility disorders such as achalasia and diffuseesophageal spasm. The purpose of this article is to review gastroesophageal reflux disease,other types of esophagitis, benign and malignant esophageal tumors, varices, lower esoph-ageal rings, diverticula, and esophageal motility disorders, all of which can be diagnosedwith the aid of esophagography.
TECHNIQUE
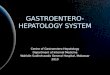
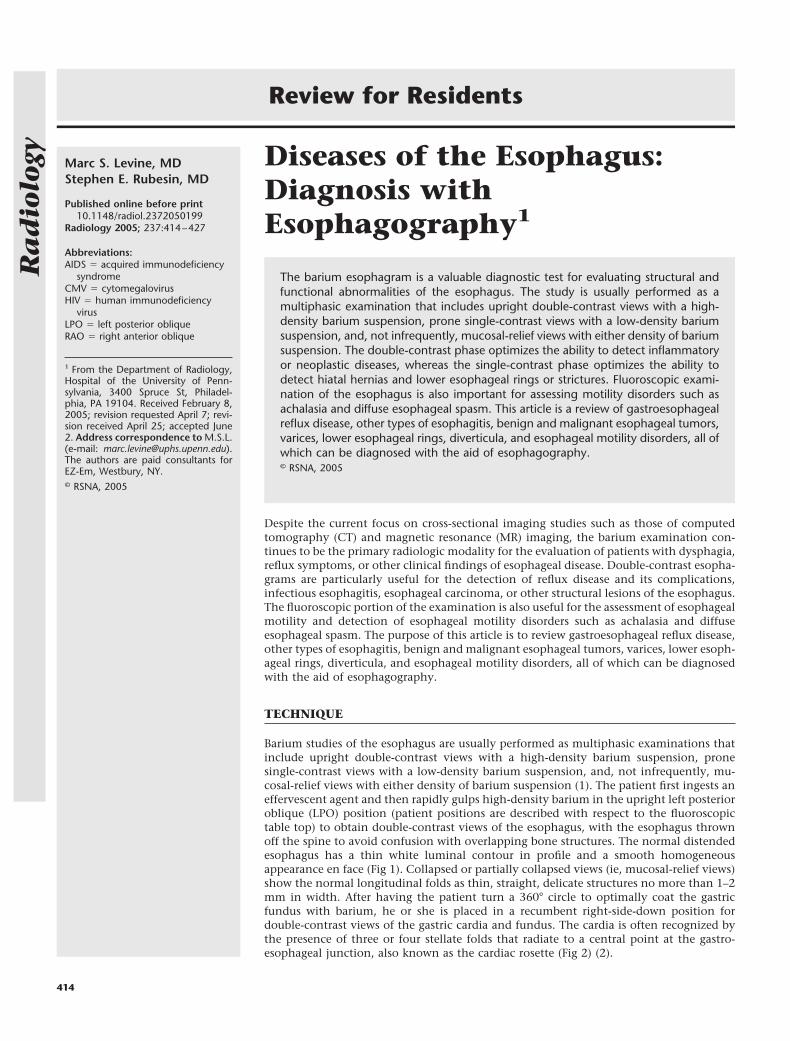
Barium studies of the esophagus are usually performed as multiphasic examinations thatinclude upright double-contrast views with a high-density barium suspension, pronesingle-contrast views with a low-density barium suspension, and, not infrequently, mu-cosal-relief views with either density of barium suspension (1). The patient first ingests aneffervescent agent and then rapidly gulps high-density barium in the upright left posterioroblique (LPO) position (patient positions are described with respect to the fluoroscopictable top) to obtain double-contrast views of the esophagus, with the esophagus thrownoff the spine to avoid confusion with overlapping bone structures. The normal distendedesophagus has a thin white luminal contour in profile and a smooth homogeneousappearance en face (Fig 1). Collapsed or partially collapsed views (ie, mucosal-relief views)show the normal longitudinal folds as thin, straight, delicate structures no more than 1–2mm in width. After having the patient turn a 360° circle to optimally coat the gastricfundus with barium, he or she is placed in a recumbent right-side-down position fordouble-contrast views of the gastric cardia and fundus. The cardia is often recognized bythe presence of three or four stellate folds that radiate to a central point at the gastro-esophageal junction, also known as the cardiac rosette (Fig 2) (2).
Review for Residents
414
Ra
dio
logy
The patient is then placed in a proneright anterior oblique (RAO) position andis asked to take discrete swallows of low-density barium to evaluate esophagealmotility. Esophageal dysmotility is con-sidered to be present when abnormalperistalsis is detected for two or more offive separate swallows (3). The patientnext gulps the low-density barium sus-pension to optimally distend the esoph-agus to show rings, strictures, or hiatalhernias that could be missed on uprightdouble-contrast views. Finally, the pa-tient is turned from a supine to RPO andright-lateral positions to assess for spon-taneous gastroesophageal reflux or for re-flux induced by a Valsalva maneuver toincrease intraabdominal pressure.
GASTROESOPHAGEAL REFLUXDISEASE
The purpose of barium studies in patientswith reflux symptoms is not simply todocument the presence of a hiatal herniaor gastroesophageal reflux but to detectthe morphologic sequelae of reflux, in-cluding reflux esophagitis, peptic stric-tures, Barrett esophagus, and esophagealadenocarcinoma. These conditions arediscussed separately in the following sec-tions.
Reflux Esophagitis
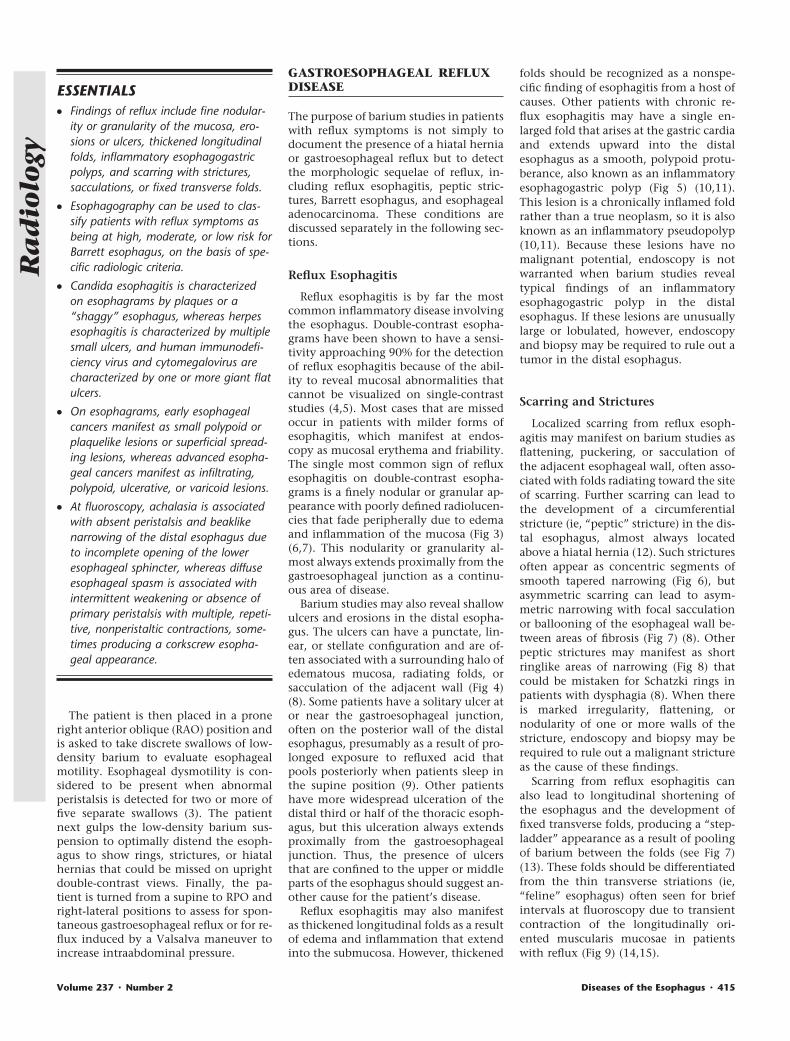
Reflux esophagitis is by far the mostcommon inflammatory disease involvingthe esophagus. Double-contrast esopha-grams have been shown to have a sensi-tivity approaching 90% for the detectionof reflux esophagitis because of the abil-ity to reveal mucosal abnormalities thatcannot be visualized on single-contraststudies (4,5). Most cases that are missedoccur in patients with milder forms ofesophagitis, which manifest at endos-copy as mucosal erythema and friability.The single most common sign of refluxesophagitis on double-contrast esopha-grams is a finely nodular or granular ap-pearance with poorly defined radiolucen-cies that fade peripherally due to edemaand inflammation of the mucosa (Fig 3)(6,7). This nodularity or granularity al-most always extends proximally from thegastroesophageal junction as a continu-ous area of disease.
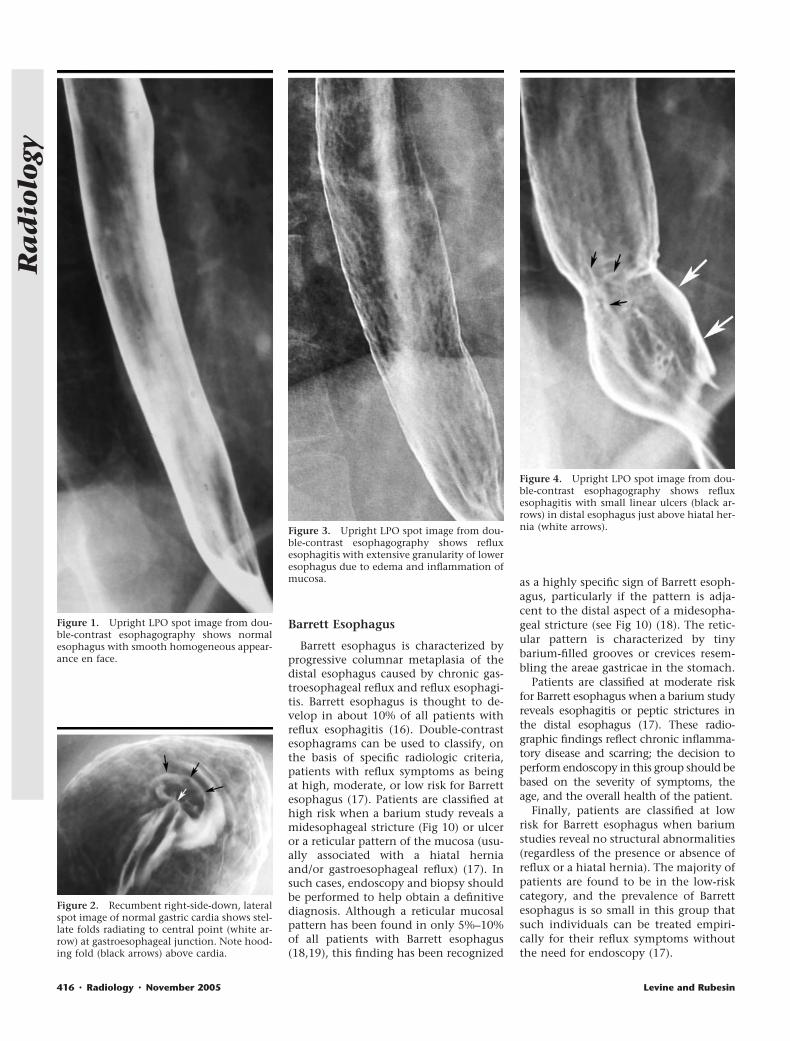
Barium studies may also reveal shallowulcers and erosions in the distal esopha-gus. The ulcers can have a punctate, lin-ear, or stellate configuration and are of-ten associated with a surrounding halo ofedematous mucosa, radiating folds, orsacculation of the adjacent wall (Fig 4)(8). Some patients have a solitary ulcer ator near the gastroesophageal junction,often on the posterior wall of the distalesophagus, presumably as a result of pro-longed exposure to refluxed acid thatpools posteriorly when patients sleep inthe supine position (9). Other patientshave more widespread ulceration of thedistal third or half of the thoracic esoph-agus, but this ulceration always extendsproximally from the gastroesophagealjunction. Thus, the presence of ulcersthat are confined to the upper or middleparts of the esophagus should suggest an-other cause for the patient’s disease.
Reflux esophagitis may also manifestas thickened longitudinal folds as a resultof edema and inflammation that extendinto the submucosa. However, thickened
folds should be recognized as a nonspe-cific finding of esophagitis from a host ofcauses. Other patients with chronic re-flux esophagitis may have a single en-larged fold that arises at the gastric cardiaand extends upward into the distalesophagus as a smooth, polypoid protu-berance, also known as an inflammatoryesophagogastric polyp (Fig 5) (10,11).This lesion is a chronically inflamed foldrather than a true neoplasm, so it is alsoknown as an inflammatory pseudopolyp(10,11). Because these lesions have nomalignant potential, endoscopy is notwarranted when barium studies revealtypical findings of an inflammatoryesophagogastric polyp in the distalesophagus. If these lesions are unusuallylarge or lobulated, however, endoscopyand biopsy may be required to rule out atumor in the distal esophagus.
Scarring and Strictures
Localized scarring from reflux esoph-agitis may manifest on barium studies asflattening, puckering, or sacculation ofthe adjacent esophageal wall, often asso-ciated with folds radiating toward the siteof scarring. Further scarring can lead tothe development of a circumferentialstricture (ie, “peptic” stricture) in the dis-tal esophagus, almost always locatedabove a hiatal hernia (12). Such stricturesoften appear as concentric segments ofsmooth tapered narrowing (Fig 6), butasymmetric scarring can lead to asym-metric narrowing with focal sacculationor ballooning of the esophageal wall be-tween areas of fibrosis (Fig 7) (8). Otherpeptic strictures may manifest as shortringlike areas of narrowing (Fig 8) thatcould be mistaken for Schatzki rings inpatients with dysphagia (8). When thereis marked irregularity, flattening, ornodularity of one or more walls of thestricture, endoscopy and biopsy may berequired to rule out a malignant strictureas the cause of these findings.
Scarring from reflux esophagitis canalso lead to longitudinal shortening ofthe esophagus and the development offixed transverse folds, producing a “step-ladder” appearance as a result of poolingof barium between the folds (see Fig 7)(13). These folds should be differentiatedfrom the thin transverse striations (ie,“feline” esophagus) often seen for briefintervals at fluoroscopy due to transientcontraction of the longitudinally ori-ented muscularis mucosae in patientswith reflux (Fig 9) (14,15).
ESSENTIALS! Findings of reflux include fine nodular-
ity or granularity of the mucosa, ero-sions or ulcers, thickened longitudinalfolds, inflammatory esophagogastricpolyps, and scarring with strictures,sacculations, or fixed transverse folds.
! Esophagography can be used to clas-sify patients with reflux symptoms asbeing at high, moderate, or low risk forBarrett esophagus, on the basis of spe-cific radiologic criteria.
! Candida esophagitis is characterizedon esophagrams by plaques or a“shaggy” esophagus, whereas herpesesophagitis is characterized by multiplesmall ulcers, and human immunodefi-ciency virus and cytomegalovirus arecharacterized by one or more giant flatulcers.
! On esophagrams, early esophagealcancers manifest as small polypoid orplaquelike lesions or superficial spread-ing lesions, whereas advanced esopha-geal cancers manifest as infiltrating,polypoid, ulcerative, or varicoid lesions.
! At fluoroscopy, achalasia is associatedwith absent peristalsis and beaklikenarrowing of the distal esophagus dueto incomplete opening of the loweresophageal sphincter, whereas diffuseesophageal spasm is associated withintermittent weakening or absence ofprimary peristalsis with multiple, repeti-tive, nonperistaltic contractions, some-times producing a corkscrew esopha-geal appearance.
Volume 237 " Number 2 Diseases of the Esophagus " 415
Ra
dio
logy
Barrett Esophagus
Barrett esophagus is characterized byprogressive columnar metaplasia of thedistal esophagus caused by chronic gas-troesophageal reflux and reflux esophagi-tis. Barrett esophagus is thought to de-velop in about 10% of all patients withreflux esophagitis (16). Double-contrastesophagrams can be used to classify, onthe basis of specific radiologic criteria,patients with reflux symptoms as beingat high, moderate, or low risk for Barrettesophagus (17). Patients are classified athigh risk when a barium study reveals amidesophageal stricture (Fig 10) or ulceror a reticular pattern of the mucosa (usu-ally associated with a hiatal herniaand/or gastroesophageal reflux) (17). Insuch cases, endoscopy and biopsy shouldbe performed to help obtain a definitivediagnosis. Although a reticular mucosalpattern has been found in only 5%–10%of all patients with Barrett esophagus(18,19), this finding has been recognized
as a highly specific sign of Barrett esoph-agus, particularly if the pattern is adja-cent to the distal aspect of a midesopha-geal stricture (see Fig 10) (18). The retic-ular pattern is characterized by tinybarium-filled grooves or crevices resem-bling the areae gastricae in the stomach.
Patients are classified at moderate riskfor Barrett esophagus when a barium studyreveals esophagitis or peptic strictures inthe distal esophagus (17). These radio-graphic findings reflect chronic inflamma-tory disease and scarring; the decision toperform endoscopy in this group should bebased on the severity of symptoms, theage, and the overall health of the patient.
Finally, patients are classified at lowrisk for Barrett esophagus when bariumstudies reveal no structural abnormalities(regardless of the presence or absence ofreflux or a hiatal hernia). The majority ofpatients are found to be in the low-riskcategory, and the prevalence of Barrettesophagus is so small in this group thatsuch individuals can be treated empiri-cally for their reflux symptoms withoutthe need for endoscopy (17).
Figure 1. Upright LPO spot image from dou-ble-contrast esophagography shows normalesophagus with smooth homogeneous appear-ance en face.
Figure 2. Recumbent right-side-down, lateralspot image of normal gastric cardia shows stel-late folds radiating to central point (white ar-row) at gastroesophageal junction. Note hood-ing fold (black arrows) above cardia.
Figure 3. Upright LPO spot image from dou-ble-contrast esophagography shows refluxesophagitis with extensive granularity of loweresophagus due to edema and inflammation ofmucosa.
Figure 4. Upright LPO spot image from dou-ble-contrast esophagography shows refluxesophagitis with small linear ulcers (black ar-rows) in distal esophagus just above hiatal her-nia (white arrows).
416 " Radiology " November 2005 Levine and Rubesin
Ra
dio
logy
INFECTIOUS ESOPHAGITIS
Candida Esophagitis
Candida albicans is the most commoncause of infectious esophagitis. It usuallyoccurs as an opportunistic infection inimmunocompromised patients, particu-larly those with acquired immunodefi-ciency syndrome (AIDS), but Candidaesophagitis can also result from localesophageal stasis caused by severe esoph-ageal motility disorders such as achalasiaand scleroderma (20). Only about 50% ofpatients with Candida esophagitis arefound to have thrush, so the absence oforopharyngeal disease in no way ex-cludes this diagnosis.
Candida esophagitis usually manifestson double-contrast studies as discreteplaquelike lesions that are seen as linearor irregular filling defects that tend to beoriented longitudinally and are separatedby normal mucosa (Fig 11) (21). Double-contrast esophagrams have been foundto have a sensitivity of 90% for the detec-tion of Candida esophagitis (21,22), pri-marily because of the ability to showthese plaques.
Glycogenic acanthosis is another com-mon condition affecting elderly people.In glycogenic acanthosis, cytoplasmicglycogen accumulates in the squamousepithelial cell lining of the esophagus,which causes focal plaquelike thickeningof the mucosa (23,24). Glycogenic acan-thosis may manifest on double-contraststudies as multiple small nodules orplaques (Fig 12) (23,24). The major con-sideration in the differential diagnosis isCandida esophagitis. However, the nod-ules of glycogenic acanthosis have amore rounded appearance, whereas theplaques of Candida esophagitis tend tohave a more linear configuration. Also,candidiasis usually occurs in immuno-compromised patients with odynopha-gia, whereas glycogenic acanthosis oc-curs in older individuals with no esoph-ageal symptoms. It therefore is usually
possible to differentiate these conditionson the basis of the clinical and radio-graphic findings.
During the past 2 decades, a muchmore fulminant form of candidiasis hasbeen encountered in patients with AIDS,who may present with a grossly irregularor “shaggy” esophagus caused by innu-merable coalescent pseudomembranesand plaques, with trapping of barium be-tween the lesions (Fig 13) (25). Other pa-tients with achalasia or scleroderma maydevelop a “foamy” esophagus, with innu-merable tiny bubbles layering out in thebarium column; this phenomenon pre-sumably results from the yeast form offungal infection (26). When typical find-ings of Candida esophagitis are encoun-tered on double-contrast esophagrams,patients with these findings can betreated with antifungal agents such asfluconazole, without the need for endos-copy.
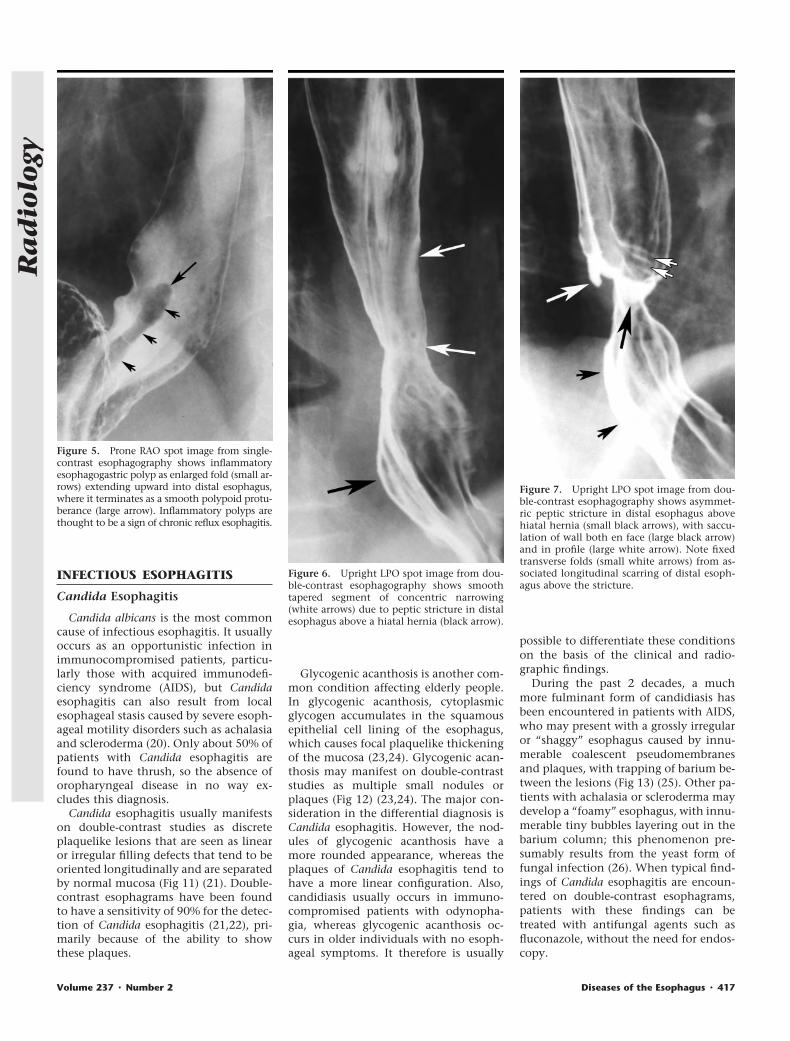
Figure 5. Prone RAO spot image from single-contrast esophagography shows inflammatoryesophagogastric polyp as enlarged fold (small ar-rows) extending upward into distal esophagus,where it terminates as a smooth polypoid protu-berance (large arrow). Inflammatory polyps arethought to be a sign of chronic reflux esophagitis.
Figure 6. Upright LPO spot image from dou-ble-contrast esophagography shows smoothtapered segment of concentric narrowing(white arrows) due to peptic stricture in distalesophagus above a hiatal hernia (black arrow).
Figure 7. Upright LPO spot image from dou-ble-contrast esophagography shows asymmet-ric peptic stricture in distal esophagus abovehiatal hernia (small black arrows), with saccu-lation of wall both en face (large black arrow)and in profile (large white arrow). Note fixedtransverse folds (small white arrows) from as-sociated longitudinal scarring of distal esoph-agus above the stricture.
Volume 237 " Number 2 Diseases of the Esophagus " 417
Ra
dio
logy
Herpes Esophagitis
The herpes simplex virus is another fre-quent cause of infectious esophagitis (27).Most patients with this virus are immuno-compromised, but herpes esophagitis mayoccasionally develop as an acute self-lim-ited disease in immunocompetent individ-uals (28). Herpes esophagitis initially leadsto the development of small mucosal ves-icles that rupture to form discretepunched-out ulcers. As a result, herpesesophagitis may manifest on double-con-trast studies as small superficial ulcersagainst a background of normal mucosa(27,29). The ulcers can have a punctate,stellate, or ringlike configuration and areoften surrounded by radiolucent moundsof edema (Fig 14). In the appropriate clin-ical setting, the presence of small discreteulcers without plaques should be highlysuggestive of herpes esophagitis, becauseulceration in candidiasis almost always oc-curs against a background of diffuse plaqueformation. As the disease progresses, how-ever, herpes esophagitis may manifest as a
combination of ulcers and plaques thatmimic Candida esophagitis (27).
Herpes esophagitis in otherwise healthypatients manifests as innumerable tinyulcers clustered together in themidesophagus below the level of the leftmain bronchus (28). The ulcers are evensmaller than those in immunocompro-mised patients with herpes esophagitis,presumably because these individualshave an intact immune system that pre-vents the ulcers from enlarging.
Cytomegalovirus Esophagitis
Cytomegalovirus (CMV) is anothercause of infectious esophagitis that oc-curs primarily in patients with AIDS.CMV esophagitis may manifest on dou-ble-contrast studies as multiple small ul-cers or, even more commonly, as one ormore giant flat ulcers that are several cen-timeters or more in length (30). The ul-cers may have an ovoid or diamond-shaped configuration and are often sur-rounded by a thin radiolucent rim ofedematous mucosa. Because herpetic ul-cers rarely become this large, the pres-
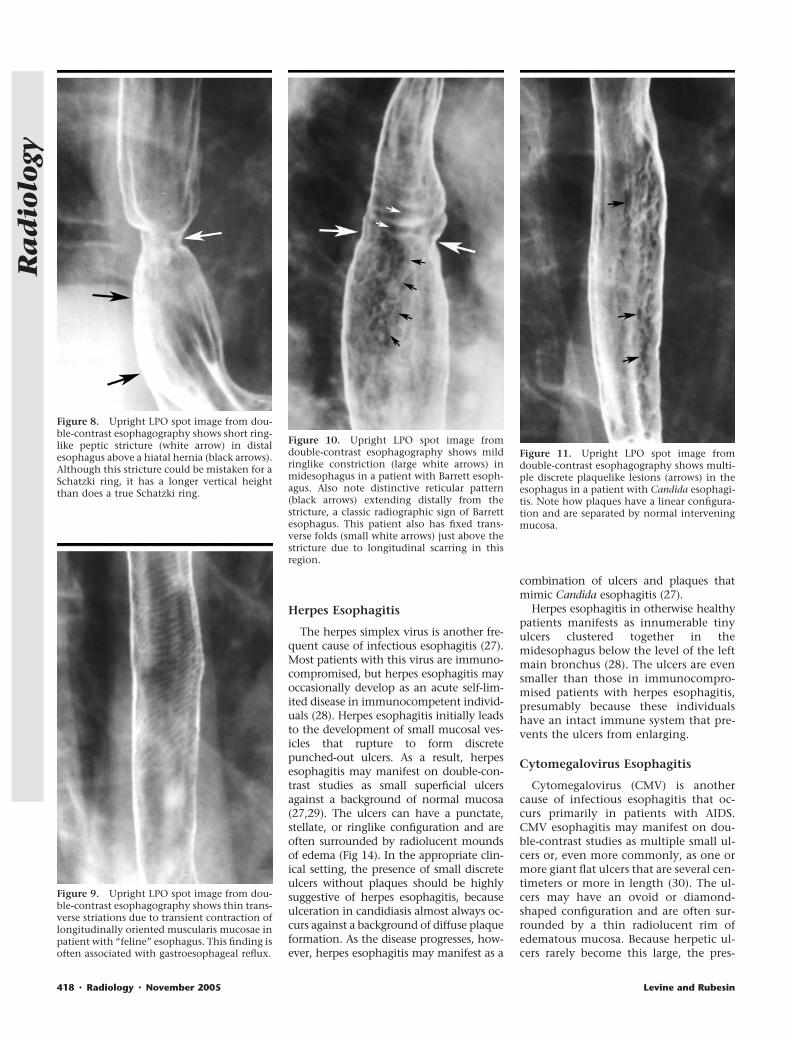
Figure 8. Upright LPO spot image from dou-ble-contrast esophagography shows short ring-like peptic stricture (white arrow) in distalesophagus above a hiatal hernia (black arrows).Although this stricture could be mistaken for aSchatzki ring, it has a longer vertical heightthan does a true Schatzki ring.
Figure 9. Upright LPO spot image from dou-ble-contrast esophagography shows thin trans-verse striations due to transient contraction oflongitudinally oriented muscularis mucosae inpatient with “feline” esophagus. This finding isoften associated with gastroesophageal reflux.
Figure 10. Upright LPO spot image fromdouble-contrast esophagography shows mildringlike constriction (large white arrows) inmidesophagus in a patient with Barrett esoph-agus. Also note distinctive reticular pattern(black arrows) extending distally from thestricture, a classic radiographic sign of Barrettesophagus. This patient also has fixed trans-verse folds (small white arrows) just above thestricture due to longitudinal scarring in thisregion.
Figure 11. Upright LPO spot image fromdouble-contrast esophagography shows multi-ple discrete plaquelike lesions (arrows) in theesophagus in a patient with Candida esophagi-tis. Note how plaques have a linear configura-tion and are separated by normal interveningmucosa.
418 " Radiology " November 2005 Levine and Rubesin
Ra
dio
logy
ence of one or more giant ulcers shouldsuggest the possibility of CMV esophagi-tis in patients with AIDS. However, thedifferential diagnosis also includes gianthuman immunodeficiency virus (HIV)ulcers in the esophagus (see next sec-tion). Because CMV esophagitis is treatedwith relatively toxic antiviral agents suchas ganciclovir, endoscopy (with biopsyspecimens, brushings, or cultures fromthe esophagus) is required to confirm thepresence of CMV infection before thesepatients are treated.
HIV Esophagitis
HIV infection of the esophagus canlead to the development of giant esoph-ageal ulcers indistinguishable from thosecaused by CMV esophagitis. Double-con-trast esophagrams typically reveal one ormore large ovoid or diamond-shaped ul-cers surrounded by a radiolucent rim ofedema (Fig 15), sometimes associatedwith a cluster of small satellite ulcers(31,32). Occasionally, these individualsmay have associated palatal ulcers or acharacteristic maculopapular rash on the
upper body (31,32). The diagnosis is es-tablished by obtaining endoscopic bi-opsy specimens, brushings, or cultures torule out CMV esophagitis as the cause ofthe ulcers. Unlike CMV ulcers, HIV-re-lated esophageal ulcers usually healmarkedly after treatment with oral ste-roids (31,32). Thus, endoscopy is re-quired in HIV-positive patients with gi-ant esophageal ulcers, to differentiateesophagitis caused by HIV and CMV sothat appropriate therapy can be insti-tuted.
DRUG-INDUCED ESOPHAGITIS
Tetracycline and doxycycline are the twoagents most commonly responsible fordrug-induced esophagitis in the UnitedStates, but other causative agents includepotassium chloride, quinidine, aspirin orother nonsteroidal antiinflammatorydrugs, and alendronate sodium (33–35).
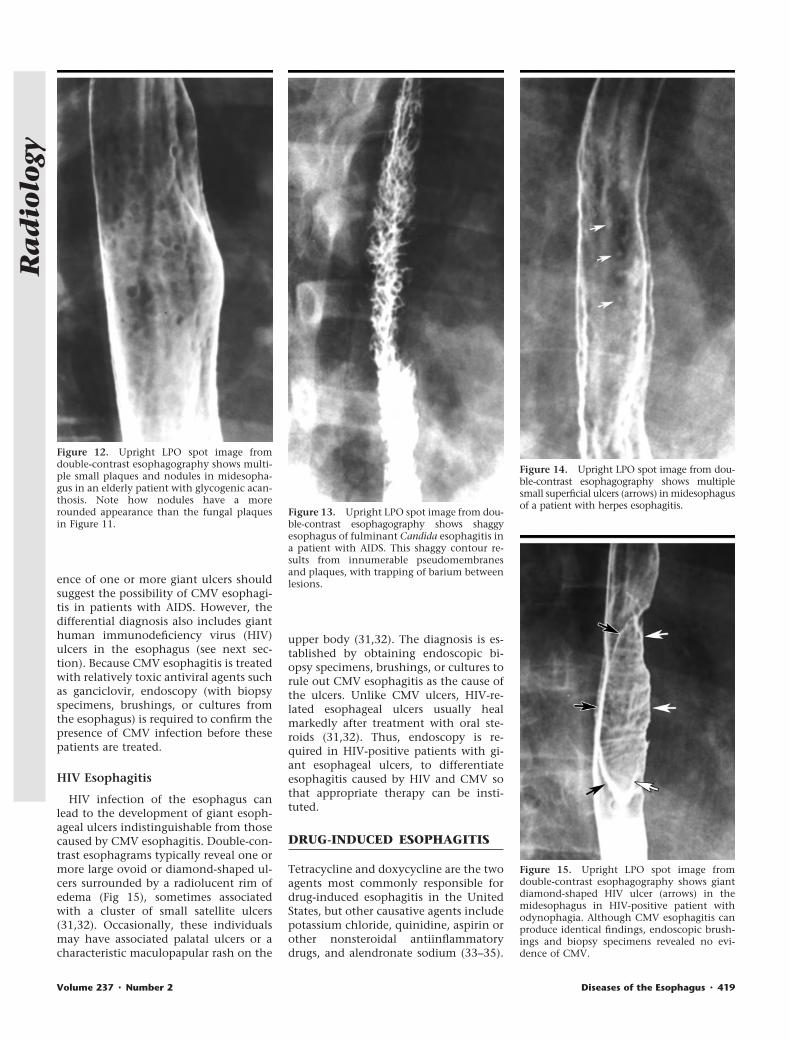
Figure 12. Upright LPO spot image fromdouble-contrast esophagography shows multi-ple small plaques and nodules in midesopha-gus in an elderly patient with glycogenic acan-thosis. Note how nodules have a morerounded appearance than the fungal plaquesin Figure 11.
Figure 13. Upright LPO spot image from dou-ble-contrast esophagography shows shaggyesophagus of fulminant Candida esophagitis ina patient with AIDS. This shaggy contour re-sults from innumerable pseudomembranesand plaques, with trapping of barium betweenlesions.
Figure 14. Upright LPO spot image from dou-ble-contrast esophagography shows multiplesmall superficial ulcers (arrows) in midesophagusof a patient with herpes esophagitis.
Figure 15. Upright LPO spot image fromdouble-contrast esophagography shows giantdiamond-shaped HIV ulcer (arrows) in themidesophagus in HIV-positive patient withodynophagia. Although CMV esophagitis canproduce identical findings, endoscopic brush-ings and biopsy specimens revealed no evi-dence of CMV.
Volume 237 " Number 2 Diseases of the Esophagus " 419
Ra
dio
logy
Affected individuals typically ingest themedication with little or no water imme-diately before going to bed. The capsuleor pill then usually becomes lodged inthe midesophagus, where it is com-pressed by the adjacent aortic arch or leftmain bronchus. Prolonged contact of theesophageal mucosa with these medica-tions presumably causes an irritant con-tact esophagitis. Affected individualsmay present with severe odynophagia,but marked clinical improvement usuallyoccurs after withdrawal of the offendingagent.
The radiographic findings in drug-in-duced esophagitis depend on the natureof the offending medication. Tetracy-cline and doxycycline are associated withthe development of small shallow ulcersin the upper or middle part of the esoph-agus and are indistinguishable fromthose in herpes esophagitis (Fig 16)(36,37). Because of their superficial na-ture, these ulcers almost always healwithout scarring or strictures. In contrast,potassium chloride, quinidine, and non-steroidal antiinflammatory drugs maycause more severe esophageal injury lead-ing to the development of larger ulcersand possible stricture formation (38–40).Alendronate sodium (an inhibitor of os-
teoclast-mediated bone resorption, usedto prevent osteoporosis in postmeno-pausal women) may cause severe esoph-agitis with extensive ulceration and stric-tures that are usually confined to the dis-tal esophagus (41).
RADIATION-INDUCEDESOPHAGITIS
A radiation dose of 5000 cGy or more tothe mediastinum may cause severe in-jury to the esophagus. Acute radiation-induced esophagitis usually occurs 2–4weeks after the initiation of radiationtherapy (42). The mucosa typically hasa granular appearance because of edemaand inflammation of the irradiated seg-
ment (42). Ulceration and decreased lu-minal distensibility are other frequentfindings (42). The extent of disease con-forms to the margins of the radiationportal. Most cases of acute radiationesophagitis are self-limited, but somepatients may have progressive dyspha-gia due to the development of radiationstrictures 4–8 months after completionof radiation therapy (43). Such stric-tures typically appear as smooth ta-pered areas of concentric narrowingwithin a preexisting radiation portal(Fig 17).
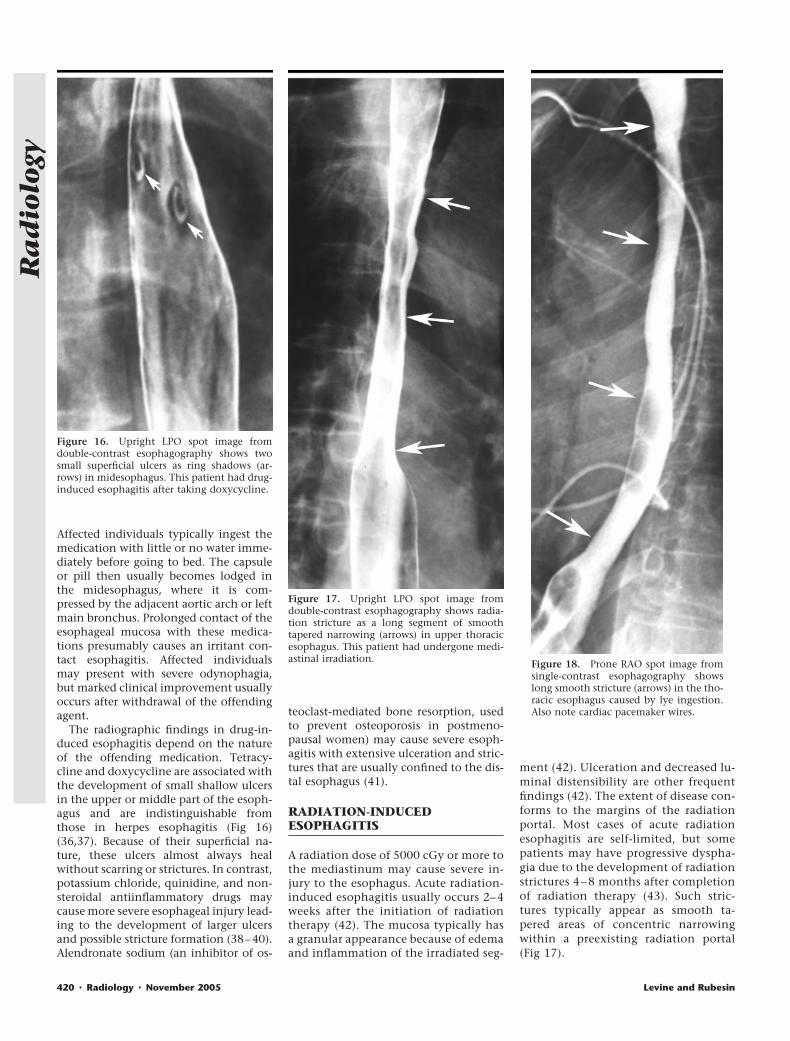
Figure 16. Upright LPO spot image fromdouble-contrast esophagography shows twosmall superficial ulcers as ring shadows (ar-rows) in midesophagus. This patient had drug-induced esophagitis after taking doxycycline.
Figure 17. Upright LPO spot image fromdouble-contrast esophagography shows radia-tion stricture as a long segment of smoothtapered narrowing (arrows) in upper thoracicesophagus. This patient had undergone medi-astinal irradiation. Figure 18. Prone RAO spot image from
single-contrast esophagography showslong smooth stricture (arrows) in the tho-racic esophagus caused by lye ingestion.Also note cardiac pacemaker wires.
420 " Radiology " November 2005 Levine and Rubesin
Ra
dio
logy

CAUSTIC ESOPHAGITIS
Whether accidental or intentional, inges-tion of lye or other caustic agents causesmarked esophagitis, eventually leadingto extensive stricture formation. Liquidlye causes liquefactive necrosis, resultingin the most severe form of caustic injuryto the esophagus (44). Endoscopy is usu-ally performed as the primary diagnostictest to help assess the extent and severityof esophageal injury after ingestion of acaustic agent. If esophageal perforation issuspected, however, a radiographic studywith water-soluble contrast materialshould be performed to document thepresence of a leak. Such studies may alsoreveal marked edema, spasm, and ulcer-ation of the affected esophagus. As theesophagitis heals, follow-up barium stud-ies have a major role in helping deter-mine the length of developing strictures,which typically involve a longer segmentof the esophagus (Fig 18) than does scar-ring from other types of esophagitis (44).Patients with chronic lye strictures alsohave an increased risk of developingsquamous cell carcinoma of the esopha-gus (45), so a new area of mucosal irreg-ularity or nodularity within a preexistinglye stricture on a barium study shouldraise concern about the possibility of asuperimposed carcinoma.
OTHER ESOPHAGITIDES
Alkaline reflux esophagitis is caused byreflux of bile or pancreatic secretions intothe esophagus after partial or total gas-trectomy (46). This form of esophagitis ischaracterized on barium studies by mu-cosal nodularity or ulceration or, in se-vere disease, by distal esophageal stric-tures that often progress rapidly in lengthand severity over a short period of time(46). The risk of developing alkaline re-flux esophagitis can be decreased by per-forming a Roux-en-Y reconstruction tominimize reflux of alkaline secretionsinto the esophagus after partial or totalgastrectomy.
Nasogastric intubation is an uncom-mon cause of esophagitis and strictureformation in the distal esophagus. It hasbeen postulated that the strictures resultfrom severe reflux esophagitis caused byconstant reflux of acid around the tubeinto the distal esophagus (44). Affectedindividuals sometimes develop markedesophageal strictures that show rapidprogression in length and severity on se-rial barium studies (44).
Other uncommon causes of esophagi-
tis include Crohn disease, tuberculosis,eosinophilic esophagitis, chronic graft-versus-host disease, Behcet syndrome,and, rarely, skin disorders involving theesophagus, such as epidermolysis bullosadystrophica and benign mucous mem-brane pemphigoid (44).
BENIGN TUMORS
Benign tumors of the esophagus composeonly about 20% of all esophageal neo-plasms (47). The majority are detected asincidental findings in asymptomatic pa-tients. Squamous papillomas are the mostcommon benign mucosal tumor in theesophagus. These lesions usually appear ondouble-contrast esophagrams as smallsessile polyps with a smooth or slightlylobulated contour (48). Some papillomasmay be difficult to distinguish from smallesophageal cancers on the basis of the ra-diographic findings, so endoscopy is re-quired for a definitive diagnosis.
In contrast, leiomyomas are the mostcommon benign submucosal tumor inthe esophagus. Affected individuals areusually asymptomatic but may occasion-
ally present with dysphagia, dependingon the size of the tumor and how much itencroaches on the lumen. Leiomyomasusually manifest on esophagrams as asmooth submucosal mass etched inwhite, which forms a right or slightlyobtuse angle with the adjacent esopha-geal wall when viewed in profile (Fig 19)(49). As a result, these lesions may beindistinguishable from other mesenchy-mal tumors such as fibromas, neurofibro-mas, and hemangiomas (except thatleiomyomas are more likely on empiricalgrounds).
Fibrovascular polyps are rare benigntumors consisting of varying amounts offibrovascular and adipose tissue coveredby squamous epithelium (50). Fibrovas-cular polyps usually arise near the level ofthe cricopharyngeus muscle, graduallyelongating over a period of years as theyare dragged inferiorly by means of esoph-
Figure 19. Upright LPO spot image fromdouble-contrast esophagography shows leio-myoma as a smooth submucosal mass (blackarrows) in the midesophagus. Note how lesionforms slightly obtuse angles with adjacentesophageal wall. Also note kissing artifact(white arrows) due to apposition of opposingesophageal walls.
Figure 20. Upright LPO spot image fromdouble-contrast esophagography shows giantfibrovascular polyp as smooth sausage-shapedmass (black arrows) expanding the lumen ofthe upper thoracic esophagus. Note polypoiddistal tip (white arrow) of polyp. Fibrovascularpolyps usually arise from the region of thecricopharyngeus muscle. (Reprinted, with per-mission, from reference 50.)
Volume 237 " Number 2 Diseases of the Esophagus " 421
Ra
dio
logy
ageal peristalsis. In rare cases, affected in-dividuals may have a spectacular clinicalpresentation, with regurgitation of afleshy mass into the pharynx or mouthor even asphyxia and sudden death if theregurgitated polyp occludes the larynx(50). Fibrovascular polyps typically ap-
pear on barium studies as smooth, expan-sile, sausage-shaped masses that expandthe lumen of the upper and middle por-tions of the esophagus (Fig 20) (50). Le-sions composed predominantly of adi-pose tissue may appear as fat-attenuationlesions on CT images, whereas lesionscontaining greater amounts of fibrovas-cular tissue may have a heterogeneousappearance with areas of fat juxtaposedwith areas of soft-tissue attenuation (50).
MALIGNANT TUMORS
Esophageal Carcinoma
Esophageal carcinoma constitutes about1% of all cancers in the United States and7% of all gastrointestinal tumors (51). Earlydissemination of tumor occurs because theesophagus lacks a serosa, so there is no
anatomic barrier to prevent these cancersfrom spreading rapidly into the mediasti-num. Patients with esophageal carcinomausually present with dysphagia, but this isa late finding that develops after the tumorhas invaded the esophageal wall, peri-esophageal lymphatics, or other mediasti-nal structures. As a result, most patientshave advanced lesions at the time of diag-nosis, with a 5-year survival rate of lessthan 10% (52). Histologically, 50%–70% ofthese tumors are squamous cell carcino-mas, and the remaining 30%–50% are ad-enocarcinomas (53).
Squamous cell carcinoma most com-monly develops in patients with a long-standing history of alcohol and/or tobaccoconsumption, whereas adenocarcinomavirtually always arises against a back-ground of Barrett mucosa in the esopha-gus. The reported prevalence of adenocar-cinoma in patients with Barrett esophagusis about 10% (54). Because these tumorsdevelop by means of a sequence of progres-sively severe epithelial dysplasia, many in-vestigators advocate endoscopic surveil-lance of patients with known Barrettesophagus to detect dysplastic or early car-cinomatous changes before the develop-ment of an advanced adenocarcinoma(54).
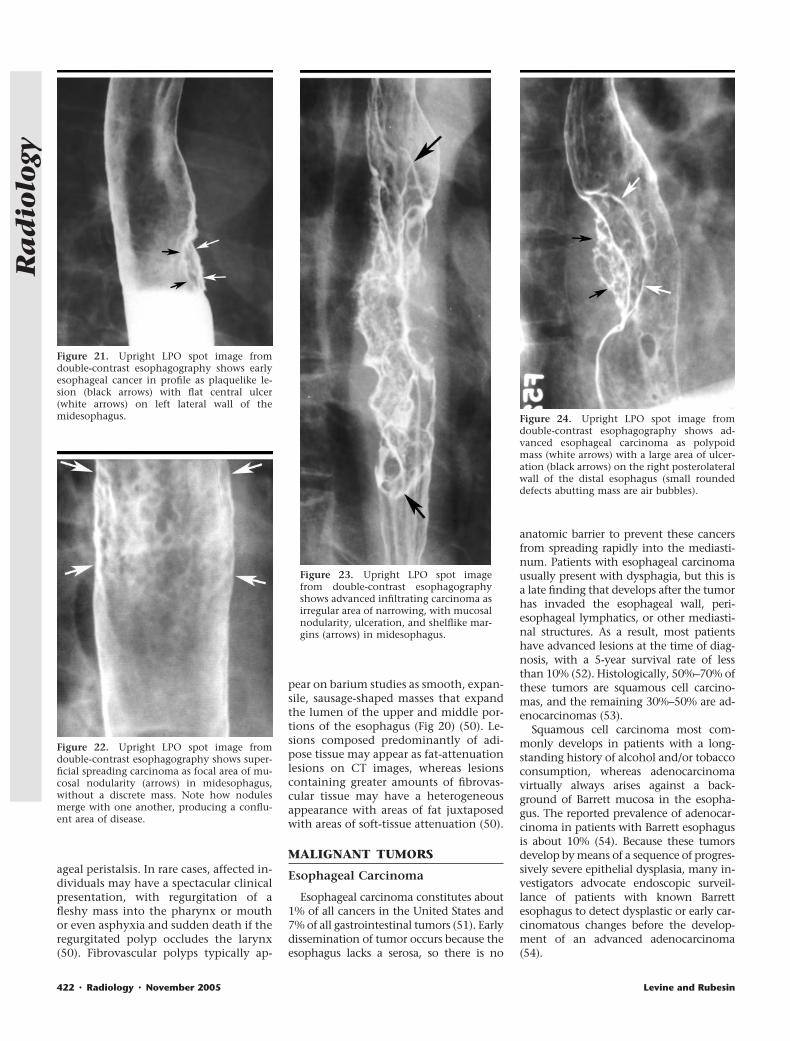
Figure 21. Upright LPO spot image fromdouble-contrast esophagography shows earlyesophageal cancer in profile as plaquelike le-sion (black arrows) with flat central ulcer(white arrows) on left lateral wall of themidesophagus.
Figure 22. Upright LPO spot image fromdouble-contrast esophagography shows super-ficial spreading carcinoma as focal area of mu-cosal nodularity (arrows) in midesophagus,without a discrete mass. Note how nodulesmerge with one another, producing a conflu-ent area of disease.
Figure 23. Upright LPO spot imagefrom double-contrast esophagographyshows advanced infiltrating carcinoma asirregular area of narrowing, with mucosalnodularity, ulceration, and shelflike mar-gins (arrows) in midesophagus.
Figure 24. Upright LPO spot image fromdouble-contrast esophagography shows ad-vanced esophageal carcinoma as polypoidmass (white arrows) with a large area of ulcer-ation (black arrows) on the right posterolateralwall of the distal esophagus (small roundeddefects abutting mass are air bubbles).
422 " Radiology " November 2005 Levine and Rubesin
Ra
dio
logy
Double-contrast esophagography has asensitivity of greater than 95% in the de-tection of esophageal cancer (55), a num-ber comparable to the endoscopic sensi-tivity of 95%–100% when brushings andbiopsy specimens are obtained (53). Earlyesophageal cancers are usually small pro-truded lesions less than 3.5 cm in size.These tumors may manifest on double-contrast studies as plaquelike lesions (of-ten containing flat central ulcers) (Fig21), sessile polyps with a smooth orslightly lobulated contour, or focal irreg-ularities of the esophageal wall (56). Earlyadenocarcinomas may also manifest as alocalized area of wall flattening or irreg-ularity within a preexisting peptic stric-ture (53). Superficial spreading carci-noma is another form of early esophagealcancer characterized by poorly definednodules or plaques that merge with oneanother, producing a confluent area ofdisease (Fig 22) (56,57).
Advanced esophageal carcinomas usu-ally appear on barium studies as infiltrat-ing, polypoid, ulcerative, or, less com-monly, varicoid lesions (53). Infiltratingcarcinomas manifest as irregular luminalnarrowing with mucosal nodularity or ul-ceration and abrupt shelflike borders (Fig23). Polypoid carcinomas appear as lobu-lated intraluminal masses or as polypoidulcerated masses (Fig 24). Primary ulcer-ative carcinomas are seen as giant menis-coid ulcers surrounded by a radiolucentrind of tumor (58). Finally, varicoid car-cinomas are those in which submucosalspread of tumor produces thickened, tor-tuous, longitudinal defects (Fig 25) thatmimic the appearance of varices (59).Varicoid tumors have a fixed configura-tion, however, whereas varices change insize and shape at fluoroscopy. Also, vari-ces rarely cause dysphagia because theyare soft and compressible. Thus, it is usu-ally possible to differentiate these condi-tions on the basis of the clinical and ra-diographic findings.
Squamous cell carcinoma and adenocar-cinoma of the esophagus cannot be reli-ably differentiated on barium studies. Nev-ertheless, squamous cell carcinoma tendsto involve the upper or middle part of theesophagus, whereas adenocarcinoma is lo-cated mainly in the distal esophagus. Un-like squamous cell carcinoma, adenocarci-noma also has a marked tendency to in-vade the gastric cardia or fundus andcomposes as many as 50% of all malignanttumors that involve the gastroesophagealjunction (60,61).
Esophageal carcinomas can metasta-size to other parts of the esophagus via arich network of intramural lymphatic
channels. These satellite metastases mayappear as polypoid, plaquelike, or ulcer-ated lesions separated from the primarytumor by normal mucosa (53). Tumoralso spreads subdiaphragmatically to theproximal stomach via submucosal lym-phatics. Metastases to the gastric cardiaand fundus may appear as large submu-cosal masses that often contain centralulcers (62).
Appropriate treatment strategies foresophageal carcinoma depend on accu-rate staging of the tumor with the aid ofCT, MR imaging, or endoscopic sonogra-phy. Tumor staging is beyond the scopeof this review.
Other Malignant Tumors
Non-Hodgkin lymphoma and, rarely,Hodgkin lymphoma may involve theesophagus. Esophageal lymphoma maymanifest on barium studies as submuco-sal masses, polypoid lesions, enlargedfolds, or strictures (63). Spindle cell car-cinoma (formerly known as carcinosar-coma) is another rare tumor; it is charac-terized by a bulky polypoid intraluminalmass that expands the lumen of theesophagus without causing obstruction(64). Other rare malignant tumors that
involve the esophagus include leiomyo-sarcoma, malignant melanoma, and Ka-posi sarcoma.
VARICES
Uphill Varices
Uphill varices are usually caused byportal hypertension with hepatofugalflow through dilated esophageal collat-eral vessels to the superior vena cava. Up-hill varices may cause marked upper gas-trointestinal tract bleeding. Varices ap-pear on barium studies as serpentinelongitudinal filling defects in the distalhalf of the thoracic portion of the esoph-agus (Fig 26) (65). They are best seen onmucosal-relief views of the collapsedesophagus while the patient is in a proneRAO position, with use of a high-densitybarium suspension or barium paste to in-
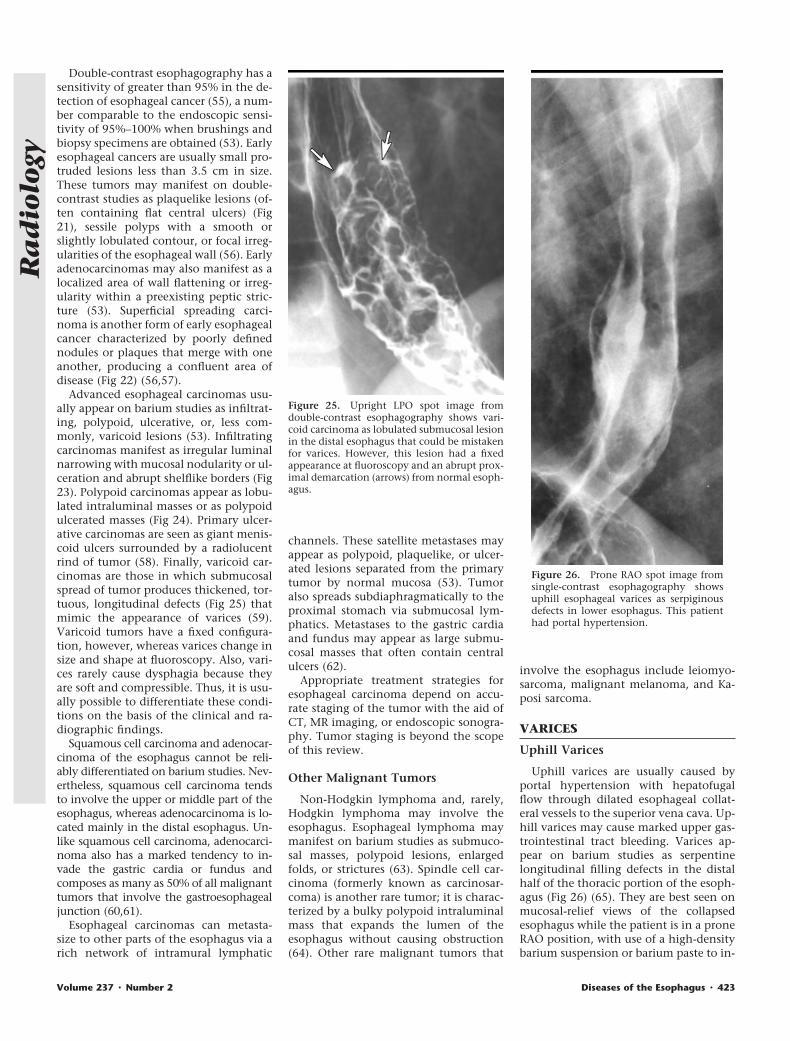
Figure 25. Upright LPO spot image fromdouble-contrast esophagography shows vari-coid carcinoma as lobulated submucosal lesionin the distal esophagus that could be mistakenfor varices. However, this lesion had a fixedappearance at fluoroscopy and an abrupt prox-imal demarcation (arrows) from normal esoph-agus.
Figure 26. Prone RAO spot image fromsingle-contrast esophagography showsuphill esophageal varices as serpiginousdefects in lower esophagus. This patienthad portal hypertension.
Volume 237 " Number 2 Diseases of the Esophagus " 423
Ra
dio
logy
crease mucosal adherence (65). The dif-ferential diagnosis for varices includesvaricoid carcinoma and esophagitis withthickened folds.
Downhill Varices
Downhill varices are caused by supe-rior vena cava obstruction with down-ward flow via dilated esophageal collat-eral vessels to the portal venous systemand the inferior vena cava. Causes ofdownhill varices include central cathe-ter–related thrombosis of the superiorvena cava, bronchogenic carcinoma orother metastatic tumors involving themediastinum, lymphoma, substernal goi-ter, mediastinal radiation, and sclerosingmediastinitis (65). Most patients withdownhill varices have superior vena cavasyndrome at the time of clinical presen-tation. Such varices typically appear asserpentine longitudinal filling defectsthat, unlike uphill esophageal varices, are
confined to the upper or middle part ofthe esophagus (Fig 27). Venography, CT,or MR imaging may be performed to con-firm the presence of superior vena cavaobstruction and to help determine theunderlying cause.
LOWER ESOPHAGEAL RINGS
Lower esophageal rings are a frequentfinding on esophagrams, but only a smallpercentage cause symptoms. The termSchatzki ring is reserved for lower esoph-ageal rings in patients who present withdysphagia. Such rings are almost alwayslocated at the gastroesophageal junction.Histologically, the superior surface of thering is lined by squamous epithelium,and the inferior surface is lined by co-lumnar epithelium. The exact pathogen-esis of Schatzki rings is uncertain, butsome rings are thought to develop as aresult of scarring from reflux esophagitis.
Lower esophageal rings appear on bar-ium studies as smooth-surfaced ringlikeconstrictions 2–3-mm in height at thegastroesophageal junction, almost al-ways located above a hiatal hernia (Fig28a) (66). The rings can be missed if the
distal esophagus is not adequately dis-tended at fluoroscopy (Fig 28b), so it isimportant to obtain prone views of theesophagus during continuous drinking ofa low-density barium suspension (67).Conversely, rings can also be missed ifthe hiatal hernia is overdistended, result-ing in overlap of the distal esophagus andhernia that obscure the ring (68). Ringswith a maximum luminal diameter ofmore than 20 mm rarely cause dyspha-gia, whereas rings with a maximum di-ameter of less than 13 mm almost alwayscause dysphagia (66). Studies have shownthat esophagography is a sensitive tech-nique for the detection of symptomaticlower esophageal rings, sometimes reveal-ing rings that are missed at endoscopy (67).
DIVERTICULA
Pulsion Diverticula
Pulsion diverticula tend to be locatedin the distal esophagus and are often as-sociated with fluoroscopic or manomet-ric evidence of esophageal dysmotility(69). These diverticula are usually de-tected as incidental findings in patientswith no esophageal symptoms. However,
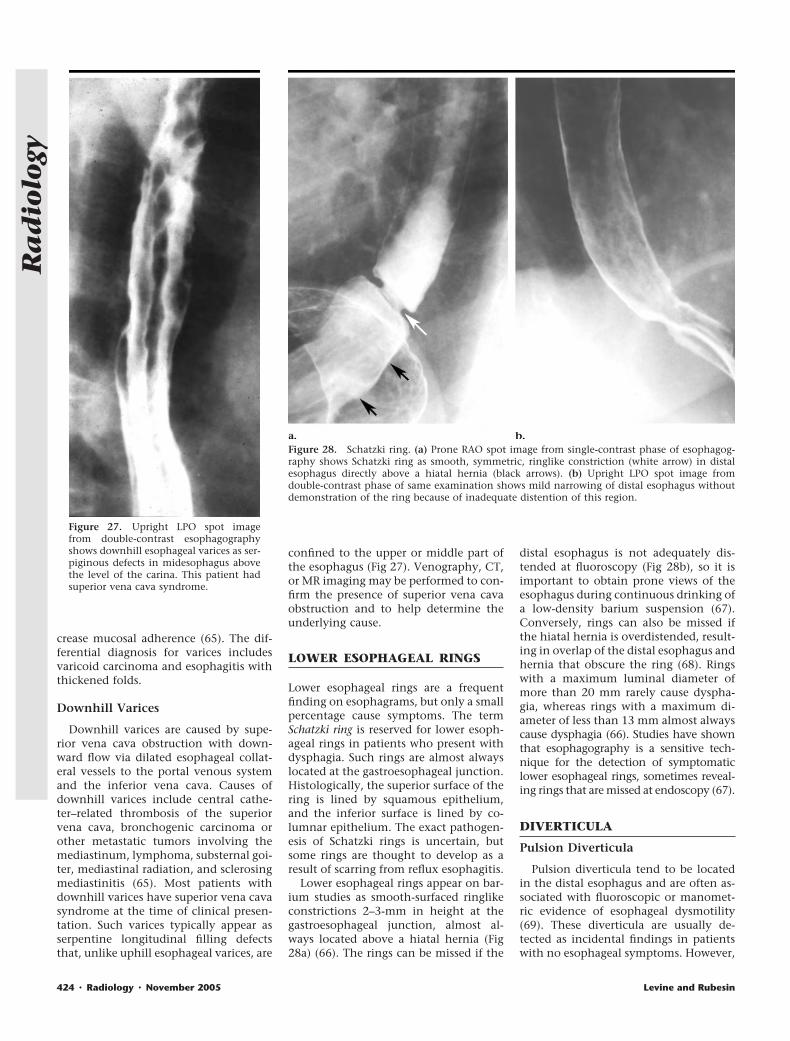
Figure 27. Upright LPO spot imagefrom double-contrast esophagographyshows downhill esophageal varices as ser-piginous defects in midesophagus abovethe level of the carina. This patient hadsuperior vena cava syndrome.
Figure 28. Schatzki ring. (a) Prone RAO spot image from single-contrast phase of esophagog-raphy shows Schatzki ring as smooth, symmetric, ringlike constriction (white arrow) in distalesophagus directly above a hiatal hernia (black arrows). (b) Upright LPO spot image fromdouble-contrast phase of same examination shows mild narrowing of distal esophagus withoutdemonstration of the ring because of inadequate distention of this region.
424 " Radiology " November 2005 Levine and Rubesin
Ra
dio
logy
a large epiphrenic diverticulum adjacentto the gastroesophageal junction may fillwith debris, causing dysphagia, regurgi-tation, or aspiration (70). Pulsion diver-ticula appear on barium studies asrounded wide-necked outpouchings thatfail to empty when the esophagus col-lapses (69).
Traction Diverticula
Traction diverticula occur in themidesophagus and are usually caused byscarring from tuberculosis or histoplas-mosis in perihilar lymph nodes (69). Be-cause traction diverticula contain all lay-ers of the esophageal wall, they maintaintheir elastic recoil and empty their con-tents when the esophagus collapses atfluoroscopy. Traction diverticula oftenhave a triangular or tented appearanceresulting from traction on the diverticu-lum by the fibrotic process in the adja-cent mediastinum (69).
Esophageal IntramuralPseudodiverticula
Esophageal intramural pseudodivertic-ula consist of dilated excretory ducts ofdeep mucous glands in the esophagus. Thepseudodiverticula typically appear onesophagrams as flask-shaped outpouchingsin rows parallel to the longitudinal axis ofthe esophagus (Fig 29) (71). When vieweden face on double-contrast esophagrams,the pseudodiverticula can be mistaken fortiny ulcers. When viewed in profile, how-ever, they often appear to be floating out-side the wall of the esophagus, withoutapparent communication with the lumen(see Fig 29) (72). Many patients have anisolated cluster of pseudodiverticula in thedistal esophagus in the region of a pepticstricture (72). In such cases, the pseudodi-verticula probably occur as a sequela ofscarring from reflux esophagitis. Less fre-quently, the pseudodiverticula have a dif-fuse distribution and are associated with
high esophageal strictures (71), or they oc-cur as an isolated finding. When stricturesare present, these patients may presentwith dysphagia, but the pseudodiverticulathemselves rarely cause symptoms.
ESOPHAGEAL MOTILITYDISORDERS
Achalasia
Primary achalasia is an idiopathic con-dition involving the myenteric plexus ofthe esophagus, whereas secondary acha-lasia is caused by other underlying con-ditions, most commonly a malignant tu-mor involving the gastroesophagealjunction (especially carcinoma of the gas-tric cardia) (73). Primary achalasia ischaracterized by absence of primary peri-stalsis in the esophagus and incompleterelaxation of the lower esophagealsphincter, which manifests on bariumstudies as a tapered beaklike narrowing ofthe distal esophagus adjacent to the gas-troesophageal junction (Fig 30) (73). Inadvanced disease, the esophagus can be-
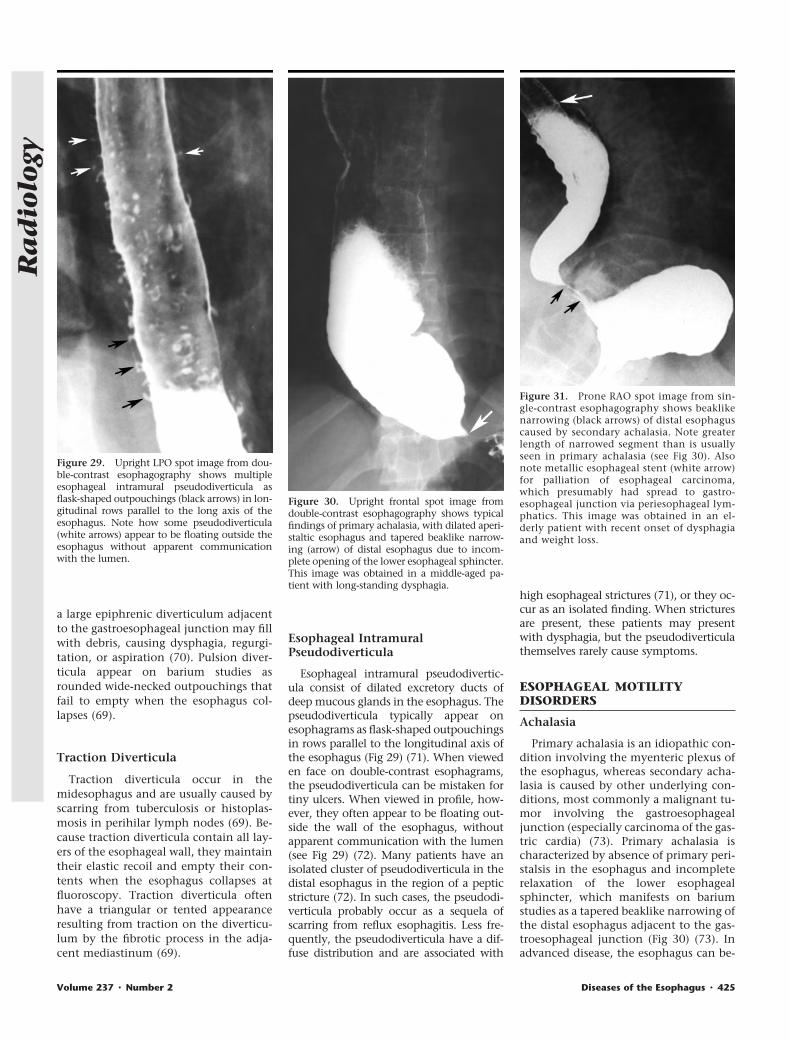
Figure 29. Upright LPO spot image from dou-ble-contrast esophagography shows multipleesophageal intramural pseudodiverticula asflask-shaped outpouchings (black arrows) in lon-gitudinal rows parallel to the long axis of theesophagus. Note how some pseudodiverticula(white arrows) appear to be floating outside theesophagus without apparent communicationwith the lumen.
Figure 30. Upright frontal spot image fromdouble-contrast esophagography shows typicalfindings of primary achalasia, with dilated aperi-staltic esophagus and tapered beaklike narrow-ing (arrow) of distal esophagus due to incom-plete opening of the lower esophageal sphincter.This image was obtained in a middle-aged pa-tient with long-standing dysphagia.
Figure 31. Prone RAO spot image from sin-gle-contrast esophagography shows beaklikenarrowing (black arrows) of distal esophaguscaused by secondary achalasia. Note greaterlength of narrowed segment than is usuallyseen in primary achalasia (see Fig 30). Alsonote metallic esophageal stent (white arrow)for palliation of esophageal carcinoma,which presumably had spread to gastro-esophageal junction via periesophageal lym-phatics. This image was obtained in an el-derly patient with recent onset of dysphagiaand weight loss.
Volume 237 " Number 2 Diseases of the Esophagus " 425
Ra
dio
logy

come massively dilated and tortuous dis-tally (ie, “sigmoid” esophagus). Becauseof the slow progression of symptoms, af-fected individuals typically have long-standing dysphagia when they seek med-ical attention.
Secondary achalasia is also character-ized by absent peristalsis in the esopha-gus and beaklike narrowing near the gas-troesophageal junction (74). In second-ary achalasia caused by tumor at thegastroesophageal junction, however, thelength of the narrowed segment is oftengreater than that in primary achalasia be-cause of spread of tumor into the distalesophagus (Fig 31) (74). The narrowedsegment may also be asymmetric, nodu-lar, or ulcerated because of tumor infil-trating this region. In some cases, bariumstudies may reveal other signs of malig-nancy at the cardia, with distortion orobliteration of the normal cardiac rosette(74). The clinical history also is impor-tant, because patients with primary acha-lasia almost always have long-standingdysphagia, whereas patients with second-ary achalasia are usually older (over age60 years) with recent onset of dysphagia(less than 6 months) and weight loss (75).
Other Esophageal MotilityDisorders
Symptomatic diffuse esophageal spasmmay manifest on barium studies as inter-mittently weakened or absent primaryperistalsis with repetitive, lumen-obliter-ating, nonperistaltic contractions thatproduce a classic “corkscrew” esophagus(76). More commonly, however, thesepatients have multiple nonperistalticcontractions of mild to moderate severitywithout a corkscrew esophagus (77).Older patients may have intermittentweakening of peristalsis in the distalesophagus and multiple nonperistalticcontractions in the absence of esopha-geal symptoms, a relatively commonmanifestation of aging known as presby-esophagus (78).
References1. Levine MS, Rubesin SE, Herlinger H, Laufer
I. Double-contrast upper gastrointestinalexamination: technique and interpreta-tion. Radiology 1988;168:593–602.
2. Herlinger H, Grossman R, Laufer I, KresselHY, Ochs RH. The gastric cardia in double-contrast study: its dynamic image. AJRAm J Roentgenol 1980;135:21–29.
3. Ott DJ, Chen YM, Hewson EG, et al. Esoph-ageal motility: assessment with synchro-nous video tape fluoroscopy and manom-etry. Radiology 1989;173:419–422.
4. Koehler RE, Weyman PJ, Oakley HF. Sin-gle- and double-contrast techniques in
esophagitis. AJR Am J Roentgenol 1980;135:15–19.
5. Creteur V, Thoeni RF, Federle MP, et al.The role of single- and double-contrast ra-diography in the diagnosis of reflux esoph-agitis. Radiology 1983;147:71–75.
6. Graziani L, Bearzi I, Romagnoli A, PesaresiA, Montesi A. Significance of diffuse gran-ularity and nodularity of the esophagealmucosa at double-contrast radiography.Gastrointest Radiol 1985;10:1–6.
7. Dibble C, Levine MS, Rubesin SE, Laufer I,Katzka DA. Detection of reflux esophagitison double-contrast esophagrams and en-doscopy using the histologic findings asthe gold standard. Abdom Imaging 2004;29:421–425.
8. Levine MS. Gastroesophageal reflux disease.In: Gore RM, Levine MS, eds. Textbook ofgastrointestinal radiology. 2nd ed. Philadel-phia, Pa: Saunders, 2000;329–349.
9. Hu C, Levine MS, Laufer I. Solitary ulcersin reflux esophagitis: radiographic find-ings. Abdom Imaging 1997;22:5–7.
10. Bleshman MH, Banner MP, Johnson RC,DeFord JW. The inflammatory esophago-gastric polyp and fold. Radiology 1978;128:589–593.
11. Styles RA, Gibb SP, Tarshis A, SilvermanML, Scholz FJ. Esophagogastric polyps: ra-diographic and endoscopic findings. Radi-ology 1985;154:307–311.
12. Ho CS, Rodrigues PR. Lower esophagealstrictures, benign or malignant? J Can As-soc Radiol 1980;31:110–113.
13. Levine MS, Goldstein HM. Fixed trans-verse folds in the esophagus: a sign of re-flux esophagitis. AJR Am J Roentgenol1984;143:275–278.
14. Gohel VK, Edell SL, Laufer I, Rhodes WH.Transverse folds in the human esophagus.Radiology 1978;128:303–308.
15. Furth EE, Rubesin SE, Rose D. Feline esoph-agus. AJR Am J Roentgenol 1995;164:900.
16. Winters C, Spurling TJ, Chobanian SJ, et al.Barrett’s esophagus: a prevalent, occult com-plication of gastroesophageal reflux disease.Gastroenterology 1987;92:118–124.
17. Gilchrist AM, Levine MS, Carr RF, et al.Barrett’s esophagus: diagnosis by double-contrast esophagography. AJR Am J Roent-genol 1988;150:97–102.
18. Levine MS, Kressel HY, Caroline DF, LauferI, Herlinger H, Thompson JJ. Barrettesophagus: reticular pattern of the mu-cosa. Radiology 1983;147:663–667.
19. Chen YM, Gelfand DW, Ott DJ, Wu WC.Barrett esophagus as an extension of se-vere esophagitis: analysis of radiologicsigns in 29 cases. AJR Am J Roentgenol1985;145:275–281.
20. Gefter WB, Laufer I, Edell S, Gohel VK.Candidiasis in the obstructed esophagus.Radiology 1981;138:25–28.
21. Levine MS, Macones AJ, Laufer I. Candidaesophagitis: accuracy of radiographic diag-nosis. Radiology 1985;154:581–587.
22. Vahey TN, Maglinte DD, Chernish SM.State-of-the-art barium examination in op-portunistic esophagitis. Dig Dis Sci 1986;31:1192–1195.
23. Rose D, Furth EE, Rubesin SE. Glycogenicacanthosis. AJR Am J Roentgenol 1995;164:96.
24. Glick SN, Teplick SK, Goldstein J, Stead JA,Zitomer N. Glycogenic acanthosis of theesophagus. AJR Am J Roentgenol 1982;139:683–688.
25. Levine MS, Woldenberg R, Herlinger H,Laufer I. Opportunistic esophagitis inAIDS: radiographic diagnosis. Radiology1987;165:815–820.
26. Sam JW, Levine MS, Rubesin SE, Laufer I.The “foamy” esophagus: a radiographicsign of Candida esophagitis. AJR Am JRoentgenol 2000;174:999–1002.
27. Levine MS, Laufer I, Kressel HY, FriedmanHM. Herpes esophagitis. AJR Am J Roent-genol 1981;136:863–866.
28. Shortsleeve MJ, Levine MS. Herpes esoph-agitis in otherwise healthy patients: clini-cal and radiographic findings. Radiology1992;182:859–861.
29. Levine MS, Loevner LA, Saul SH, RubesinSE, Herlinger H, Laufer I. Herpes esophagi-tis: sensitivity of double-contrast esopha-gography. AJR Am J Roentgenol 1988;151:57–62.
30. Balthazar EJ, Megibow AJ, Hulnick D, ChoKC, Beranbaum E. Cytomegalovirusesophagitis in AIDS: radiographic featuresin 16 patients. AJR Am J Roentgenol 1987;149:919–923.
31. Levine MS, Loercher G, Katzka DA, Her-linger H, Rubesin SE, Laufer I. Giant, hu-man immunodeficiency virus–related ul-cers in the esophagus. Radiology 1991;180:323–326.
32. Sor S, Levine MS, Kowalski TE, Laufer I,Rubesin SE, Herlinger H. Giant ulcers ofthe esophagus in patients with human im-munodeficiency virus: clinical, radio-graphic, and pathologic findings. Radiol-ogy 1995;194:447–451.
33. Kikendall JW, Friedman AC, Oyewole MA,Fleischer D, Johnson LF. Pill-inducedesophageal injury: case reports and reviewof the medical literature. Dig Dis Sci 1983;28:174–182.
34. Coates AG, Nostrand TT, Wilson JA, EltaGH, Agha FP. Esophagitis caused by non-steroidal anti-inflammatory medication:case reports and review of the literature forpill-induced esophageal injury. South MedJ 1986;79:1094–1097.
35. de Groen PC, Lubbe DF, Hirsch LJ, et al.Esophagitis associated with the use ofalendronate. N Engl J Med 1996;335:1016–1021.
36. Creteur V, Laufer I, Kressel HY, et al. Drug-induced esophagitis detected by double-contrast radiography. Radiology 1983;147:365–368.
37. Bova JG, Dutton NE, Goldstein HM,Hoberman LJ. Medication-induced esoph-agitis: diagnosis by double-contrastesophagography. AJR Am J Roentgenol1987;148:731–732.
38. Teplick JG, Teplick SK, Ominsky SH,Haskin ME. Esophagitis caused by oralmedication. Radiology 1980;134:23–25.
39. Levine MS, Rothstein RD, Laufer I. Giantesophageal ulcer due to Clinoril. AJR Am JRoentgenol 1991;156:955–956.
40. Levine MS, Borislow SM, Rubesin SE,O’Brien C. Esophageal stricture caused bya Motrin tablet (ibuprofen). Abdom Imag-ing 1994;19:6–7.
41. Ryan JM, Kelsey P, Ryan BM, Mueller PR.Alendronate-induced esophagitis: case re-port of a recently recognized form of se-vere esophagitis with esophageal stric-ture—radiographic features. Radiology1998;206:389–391.
42. Collazzo LA, Levine MS, Rubesin SE,Laufer I. Acute radiation esophagitis: ra-
426 " Radiology " November 2005 Levine and Rubesin
Ra
dio
logy

diographic findings. AJR Am J Roentgenol1997;169:1067–1070.
43. Lepke RA, Libshitz HI. Radiation-inducedinjury of the esophagus. Radiology 1983;148:375–378.
44. Levine MS. Other esophagitides. In: GoreRM, Levine MS, eds. Textbook of gastroin-testinal radiology. 2nd ed. Philadelphia,Pa: Saunders, 2000;364–386.
45. Appelqvist P, Salmo M. Lye corrosion car-cinoma of the esophagus: a review of 63cases. Cancer 1980;45:2655–2658.
46. Levine MS, Fisher AR, Rubesin SE, Laufer I,Herlinger H, Rosato EF. Complications af-ter total gastrectomy and esophagojeju-nostomy: radiologic evaluation. AJR Am JRoentgenol 1991;157:1189–1194.
47. Ming SC. Tumors of the esophagus andstomach. In: Atlas of tumor pathology, fas-cicle 7. Washington, DC: Armed Forces In-stitute of Pathology, 1973;16–23.
48. Montesi A, Pesaresi A, Graziani L, Salmis-traro D, Dini L, Bearzi I. Small benign tu-mors of the esophagus: radiological diag-nosis with double-contrast examination.Gastrointest Radiol 1983;8:207–212.
49. Levine MS. Benign tumors of the esophagus.In: Gore RM, Levine MS, eds. Textbook ofgastrointestinal radiology. 2nd ed. Philadel-phia, Pa: Saunders, 2000;387–402.
50. Levine MS, Buck JL, Pantongrag-Brown L,Buetow PC, Hallman JR, Sobin LH. Fibro-vascular polyps of the esophagus: clinical,radiographic, and pathologic findings in16 patients. AJR Am J Roentgenol 1996;166:781–787.
51. Livstone EM, Skinner DB. Tumors of theesophagus. In: Berk JE, ed. Bockus gastro-enterology. 4th ed. Philadelphia, Pa: Saun-ders, 1985;818–840.
52. Silverberg E. Cancer statistics, 1985. CACancer J Clin 1985;35:19–35.
53. Levine MS, Halvorsen RA. Carcinoma ofthe esophagus. In: Gore RM, Levine MS,eds. Textbook of gastrointestinal radiol-ogy. 2nd ed. Philadelphia, Pa: Saunders,2000;403–433.
54. Spechler SJ, Goyal RK. Barrett’s esophagus.N Engl J Med 1986;315:362–371.
55. Levine MS, Chu P, Furth EE, Rubesin SE,Laufer I, Herlinger H. Carcinoma of theesophagus and esophagogastric junction:
sensitivity of radiographic diagnosis. AJRAm J Roentgenol 1997;168:1423–1426.
56. Levine MS, Dillon EC, Saul SH, Laufer I.Early esophageal cancer. AJR Am J Roent-genol 1986;146:507–512.
57. Itai Y, Kogure T, Okuyama Y, Akiyama H.Superficial esophageal carcinoma: radio-logical findings in double-contrast studies.Radiology 1978;126:597–601.
58. Gloyna RE, Zornoza J, Goldstein HM. Pri-mary ulcerative carcinoma of the esopha-gus. AJR Am J Roentgenol 1977;129:599–600.
59. Yates CW, LeVine MA, Jensen KM. Vari-coid carcinoma of the esophagus. Radiol-ogy 1977;122:605–608.
60. Levine MS, Caroline D, Thompson JJ, Kres-sel HY, Laufer I, Herlinger H. Adenocarci-noma of the esophagus: relationship toBarrett mucosa. Radiology 1984;150:305–309.
61. Keen SJ, Dodd GD, Smith JL. Adenocarci-noma arising in Barrett esophagus: patho-logic and radiologic features. Mt SinaiJ Med 1984;51:442–450.
62. Glick SN, Teplick SK, Levine MS, CarolineDF. Gastric cardia metastases in esopha-geal carcinoma. Radiology 1986;160:627–630.
63. Levine MS, Rubesin SE, Pantongrag-BrownL, Buck JL, Herlinger H. Non-Hodgkin’slymphoma of the gastrointestinal tract: ra-diographic findings. AJR Am J Roentgenol1997;168:165–172.
64. Agha FP, Keren DF. Spindle-cell squamouscarcinoma of the esophagus: a tumor withbiphasic morphology. AJR Am J Roentge-nol 1985;145:541–545.
65. Levine MS. Varices. In: Gore RM, LevineMS, eds. Textbook of gastrointestinal radi-ology. 2nd ed. Philadelphia, Pa: Saunders,2000;452–463.
66. Schatzki R. The lower esophageal ring:long term follow-up of symptomatic andasymptomatic rings. Am J Roentgenol Ra-dium Ther Nucl Med 1963;90:805–810.
67. Ott DJ, Chen YM, Wu WC, Gelfand DW,Munitz HA. Radiographic and endoscopicsensitivity in detecting lower esophagealmucosal ring. AJR Am J Roentgenol 1986;147:261–265.
68. Hsu WC, Levine MS, Rubesin SE. Overlapphenomenon: a potential pitfall in the ra-diographic detection of lower esophagealrings. AJR Am J Roentgenol 2003;180:745–747.
69. Levine MS. Miscellaneous abnormalities ofthe esophagus. In: Gore RM, Levine MS,eds. Textbook of gastrointestinal radiol-ogy. 2nd ed. Philadelphia, Pa: Saunders,2000;465–483.
70. Fasano NC, Levine MS, Rubesin SE, Red-fern RO, Laufer I. Epiphrenic diverticulum:clinical and radiographic findings in 27patients. Dysphagia 2003;18:9–15.
71. Cho SR, Sanders MM, Turner MA, Liu CI,Kipreos BE. Esophageal intramural pseudo-diverticulosis. Gastrointest Radiol 1981;6:9–16.
72. Levine MS, Moolten DN, Herlinger H,Laufer I. Esophageal intramural pseudodi-verticulosis: a reevaluation. AJR Am JRoentgenol 1986;147:1165–1170.
73. Ott DJ. Motility disorders of the esophagus.In: Gore RM, Levine MS, eds. Textbook ofgastrointestinal radiology. 2nd ed. Philadel-phia, Pa: Saunders, 2000;316–328.
74. Woodfield CA, Levine MS, Rubesin SE,Langlotz CP, Laufer I. Diagnosis of primaryversus secondary achalasia: reassessmentof clinical and radiographic criteria. AJRAm J Roentgenol 2000;175:727–731.
75. Tucker HJ, Snape WJ, Cohen S. Achalasiasecondary to carcinoma: manometric andclinical features. Ann Intern Med 1978;89:315–318.
76. Chen YM, Ott DJ, Hewson EG, et al. Dif-fuse esophageal spasm: radiographic andmanometric correlation. Radiology 1989;170(3 pt 1):807–810.
77. Prabhakar A, Levine MS, Rubesin S, LauferI, Katzka D. Relationship between diffuseesophageal spasm and lower esophagealsphincter dysfunction on barium studiesand manometry in 14 patients. AJR Am JRoentgenol 2004;183:409–413.
78. Grishaw EK, Ott DJ, Frederick MG, Gel-fand DW, Chen MY. Functional abnormal-ities of the esophagus: a prospective anal-ysis of radiographic findings relative to ageand symptoms. AJR Am J Roentgenol1996;167:719–722.
Volume 237 " Number 2 Diseases of the Esophagus " 427
Ra
dio
logy