Embed Size (px)
Citation preview

Diseases of the Nose & Sinuses
Khalid H. Al-Sebeih, Khalid H. Al-Sebeih, MD, FRCSC, MD, FRCSC, ABOABO
Assistant Professor, Department of Surgery Assistant Professor, Department of Surgery
Faculty of Medicine, Kuwait University.Faculty of Medicine, Kuwait University.
Department of Otolaryngology, Sabah HospitalDepartment of Otolaryngology, Sabah Hospital

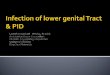
Anatomy Nasal cavity:
Roof: nasal bones, frontal bone, CFP of ethmoid, fovea ethmoidalis, sphenoid.
Septum: PPE, vomer, quadranqular cartilage, memb. septum, columella.
Floor: maxillary & palatine bone.
Lat wall: maxilla, inf. turbinate, ethmoid bone, lacrimal bone, palatine bone.

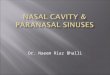
Anatomy1. Maxillary sinus
Largest, 10-20 cc. Med. = lat nasal wall Sup = orbital floor Floor = alveolar
process. Drainage via ostium in
lower infundibulum.
2. Frontal sinus: Absent unilat in 12%,
bilat 5%. Drainage: into frontal
recess posteromedially

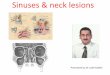
Anatomy3. Ethmoid sinuses:
3-18 air cells Ant & post. Roof = fovea ethmoidalis,
Lat = lamina papyracea, post = sphenoid, optic nerve.
Ant mid meatus, post sup meatus.
Medial wall: uncinate process, ethmoid bulla, in between hiatus semilunaris, infundibulum

Anatomy

Anatomy 4. Sphenoid sinus:
Variable pneumatization
Above: pituitary gland & optic nerve
Lat: carotid, cavernous sinus, orbital apex structures.
Drainage: sphenethmoidal recess

29 years old male Nasal obstruction Runny nose Post-nasal drip Facial fullness

RhinitisRhinitis Classification Inflammatory RhinitisAllergic rhinitis Seasonal allergic rhinitis Perennial allergic rhinitisPerennial nonallergic rhinitis Eosinophilic nasal disease Eosinophilic nonallergic rhinitis (ENR) Nonallergic rhinitis with eosinophilia
syndrome (NARES) Associated with aspirin sensitivity Atrophic rhinitis Primary Acquired Infectious rhinitis Granulomatous rhinitis (noninfectious) Irritant dust, chemical, or fume-induced rhinitis Rhinitis induced by cold, dry air
Noninflammatory Rhinitis
Rhinitis medicamentosa
Topical
Systemic
Hormonal
Idiopathic vasomotor rhinitis
Structurally Related Rhinitis
Septal deviation
Neoplasms
Cerebrospinal fluid rhinorrhea
Miscellaneous

Atrophic Rhinitis nasal mucosal atrophy with crusting and an extremely foul
odor Cuase : uknown
Bacterial: Klebsiella ozaenae, atoxic Corynebacterium diphtheriae, and the Perez-Hofer bacillus
Deficiencies in vitamin A and iron Radical surgery
Sx & Sn: halitosis, nasal obstruction, epistaxis, and headache. Offensive nasal odor, crusting, and turbinate atrophy.\
Tx: reversing nutritional deficiencies, saline irrigations, vitamin A, & systemic or topical antibiotics.
Surgical(faliure of medical therapy): closure of the nostril and nasal vestibuloplasty to narrow the nostrils.

Vasomotor Rhinitis Overactive parasympathetic stimulation of the nasal
mucosa vasodilation, edema, and hypersecretion of mucus
Sx: nasal obstruction, profuse rhinorrhea, infrequent sneezing, stuffiness, and face pressure and headache.
Trigger factors: changes in weather or humidity, the presence of irritating fumes, or air conditioning or stress
Tx: Medical: Systemic decongestants, Antihistamines,
steroids, topical ipratropium bromide. Surgical: many procedures (inf turbinectomy, submucous
resection, Cryotherapy ..etc)

Infectious Rhinitis Rhinoscleroma TB, Syphilis, leprosy. Rhinosporidiosis, histoplasmosis,
aspirgellosis.

Nasal obstruction caused by overuse of topical decongestants or a systemic medications.
Rebound vasodilatation after prolonged vasoconstriction with topical agents
Tx: discontinuation of the offending medication antihistamine-decongestant combinations topical nasal corticosteroids +/- tapering oral
prednisone dosage for 7 to 10 days. gentle submucosal Kenalog-40 injection!!
Rhinitis Medicamentosa

Allergic Rhinosinusitis Type I hypersensitivity reaction.
Occur 2 to 5 minutes of antigen-antibody reaction.
A second (late) phase: result of mediator release from cells (neutrophils, eosinophils) and occurs about 4 to 6 hours after the acute phase.

Sx: tching, sneezing, rhinorrhea, and postnasal drainage (throat-clearing and cough). Seasonal or perennial, & linkage with known exposure to allergens.
Signs: open-mouthed “adenoid facies.”, (“allergic salute”),
“allergic shiners”and puffiness around the eyes. high arched palate, prominent pharyngeal lymphoid
Dx Nasal smears (Hansel’s stain) eosinophils (> 25% of
the cells). total IgE Skin test
Allergic Rhinosinusitis

Management: Level I: Prevention and Control of Symptoms.
Environmental Control First-line Pharmacotherapy:
a) Antihistamines compete with histamine for H1-receptor sites on the target organs during the allergic response
b) Decongestants are sympathomimetic substances that cause vasoconstriction within turbinate stroma, producing shrinkage of congested tissue (Pseudoephedrine & Phenylpropanolamine)
c) Cromolyn nasal spray stabilizes and protects mast cells from degranulation
Level II: Recognition and Management of Complicating Factors Treat other types of rhinitis: vasomotor, medicamentosa…
Allergic Rhinosinusitis

Level III: Corticosteroids for Control of Severe or Chronic Symptoms
Level IV: Immunotherapy symptoms are not controlled with
pharmacotherapy, allergens that cannot be avoided, symptoms span two or more allergy seasons, willing to cooperate in a program of immunotherapy
parenteral administration of antigens formation of allergen-specific IgG-blocking antibodies compete with IgE antibodies for target sites on mast cells or basophils.
Allergic Rhinosinusitis

Paranasal Sinusitis 3 factors essential to normal physiology of the paranasal
sinuses: patency of the ostia, function of the cilia, & quality of the nasal glandular secretions.
Most significant pathophysiology that produces sinusitis: mucosal edema in and around the sinus ostium:
Hypooxygenation of the involved sinus. Ciliary function is disturbed stagnation of the secretion. Local host resistance factors are diminished
darainage & perfect milieu for the growth of bacterial pathogens
Inflammation (e.g. allergic rhinitis, URTI..) increased secretions and edema in the sinonasal mucosa.

Obstruction of the sinus ostium
OO22
Vasodilatation Vasodilatation Ciliary dysfunctionCiliary dysfunction Mucous gland dysfunctionMucous gland dysfunction
TransudationTransudation stagnationstagnation Viscid fluidViscid fluid
Retained secretionsRetained secretions

Classification1. Acute: infectious lasting from 1 day up to 4
weeks. Management is medical, and rarely surgical treatment.
2. Subacute: infection lasts from 4 weeks to 3 months. inflammatory process is still reversible Medical management.
3. Chronic: sinusitis persists longer than 3 months. Results from acute sinusitis that has been either inadequately treated or completely untreated. The process is irreversible surgical treatment is indicated.
Paranasal Sinusitis

Acute sinusitis: Bacterial:
Adults: Streptococcus pneumoniae, Staphylococcus aureus, Streptococcus pyogenes groups ABC, and Haemophilus influenzae (gram-negative).
Children: S. pneumoniae, Branhamella catarrhalis (formerly known as Neisseria catarrhalis), Haemophilus influenzae, Streptococcus pyogenes groups A and C, and Streptococcus pyogenes a-hemolytic type
Paranasal Sinusitis

Management 1. Antibiotics clinical improv. In 2-3 days, Ab should continue for 10-14 days
Penicillin G Amoxicillin Cefaclor Trimethoprim sulfate Erythromycin sulfate Augmentin
2. Analgesics3. Mucolytics4. Saline irrigations5. Topical decongestion edema around the ostia oxygenation and facilitate drainage (reverse the
hypoxia)6. Shrinkage and suction with Argyrol: packing the nose removal of pus & oxygenation7. Surgical management: presence of mucopurulent material in immunosuppressed pt , pt with acute
max. sinusitis, no Improvement or worsening of symptoms.

Complications Mucocele
chronic, cystic lesion of the paranasal sinuses. Expand slowly and concentrically bony erosion & extrasinus expansion.
Most common in the frontal sinus.
Sx: frontal headache and proptosis, displacement of the globe in a downward and outward direction and diplopia but no nasal obstruction and rhinorrhea
Tx: surgery


Complications classification (Chandler):
1. Inflammatory edema — lid edema; no limitation of extraocular movement with normal acuity
2. Orbital cellulitis — diffuse edema of orbital contents; no discrete abscess formation
3. Subperiosteal abscess —purulent collection beneath periosteum of lamina papyracea; displacement of globe downward and laterally
4. Orbital abscess—purulent collection within orbit; proptosis and chemosis with ophthalmoplegia and decreased vision
5. Cavernous sinus thrombosis—bilateral eye findings; prostration; meningismus










Complications Intra-cranial complications
direct extension through a defect in the posterior wall of the frontal sinus
Retrograde thrombophlebitis of the valveless ophthalmic vessels
The subdural space abscess cerebral abscess, seizures, and neurologic deficits. Meningitis (rare). Septic thrombosis of major dural sinuses
Tx: High-dose antibiotic therapy management of increased intracranial pressure, and
prevention of seizures. Surgical drainage

Fungal Rhinosinusitis Classification:
1. Acute invasive fungal sinusitis Life threatining Mucor mycosis, immunocompromised host Tx: radical resection, correct underlying medical problem, systemic
antifungal.
2. Chronic invasive fungal sinusitis Similar to ch. Sinusitis, caused by aspergillus Endemic in hot dry climates e.g. Sudan
3. Mycetoma (fungus ball): concentric hyphae of aspegillus Tx: simple excision.
4. Allergic fungal sinusitis Most common, Demitaceous groub Nasal polyps, +ve skin test, Charcot-Layden crystals Tx: surgery & steroids
5. Saprophytic infection: fungal contamination



Epistaxis
Local SystemicTrauma (facial fractures, Vasculardigital trauma) Blood dyscrasiaInflammatory reactions DrugsAnatomical or structural Systemic toxic (heavy metals)deformities InfectiousForeign bodies CardiovascularToxic chemicalSurgeryIntranasal tumors (benign, malignant)
10% of cases unknown

Epistaxis Osler-Rendu-Weber’s disease (hereditary hemorrhagic
telangiectasia autosomal dominant disease Lack of contractile elements in the vessel walls
arteriovenous fistulae are formed. Precipitating factors include mucosal fragility and trauma.
Blood dyscrasias Identified early in life Most common Factor VIII (80% of cases). Von Willebrand’s: prolonged bleeding time, deficiency in
antihemophilic Factor VIII, and impaired platelet adhesiveness.
Drugs (acetylsalicylic acid, anticoagulants), Systemic toxic agents (phosphorous, mercury), infectious diseases (scarlet fever, smallpox).

Management1. ABC, IV fluid, cross matching.2. Silver Nitrate Cauterization 3. Electrical Cauterization 4. Cryotherapy 5. Nasal Packing
Anterior Nasal Packing Posterior Nasal Packing
6. Greater Palatine Foramen Block 7. Embolization

8. Surgery Septoplasty/Submucous Resection Internal Maxillary Artery Ligation Transantral Sphenopalatine Artery Ligation Anterior and Posterior Ethmoidal Artery Ligation External Carotid Artery Ligation Laser Photocauterization (HHT) Septodermoplasty (HHT) Cutaneous/Myocutaneous Flaps - Microvascular Free
Flaps (HHT)

Epistaxis

Epistaxis

Epistaxis

CSF Leak traumatic 95% (Accidental trauma
80%, iatrogenic 15%) nontraumatic 5% (tumors,
hydrocephalus, congenital anomalies or osteomyelitis
Violation of arachnoid, dura, bone, and mucosa

Cerebrospinal Fluid Leak
Ommaya Classification
CSF Leak
Non-Traumatic 5% Traumatic 95%
High PressureNormal Pressure
congenital, osteomyelitis
Tumors 50%Hydrocephalus
communicationg or obstructive
Accidental 80% Surgical 15%

History

History
Trauma Surgery Sinonasal
disease: sinusitis, Rhinitis, allergy
Symptoms
Symptoms No. of patients
Rhinorrhea 8
Headache 5
Sinus congestion
3
Anosmia 1
Meningitis 1

History
Examination

Cerebrospinal Fluid Leak
Physical examination: Valsalva
maneuver Endonasal scope:
00,300
Collecting CSF

History
Examination
Confirm CSF

Lab. Tests:
Glucose (> 30mg/100ml)
-2 transferrin
Confirm CSF Leak

History
Examination
Confirm CSF Conservative Tx

Medical Management Effective for traumatic leak
Strict bed rest, no straining
Head elevation 300
10 – 14 days
Prophylactic antibiotic (controversial)
L.P
Carbonic-anhydrase inhibitors
(acetazolamide) ??

History
Examination
Confirm CSF Conservative TX
FailureLocalization

Radiology:1. Radionuclide Cisternography: 2. High Resolution CT Scan 3. MRI (+/- FLAIR)
Cerebrospinal Fluid Leak




4. Water-Soluble Contrast CT
Cisternography
5. MRI after intrathecal injection of diluted
Gadolinium (Gd) ( Gd MRI
Cisternography)


History
Examination
Confirm CSF Conservative TX
FailureLocalization
Surgical repair

Surgical management Spontaneous CSF Leak
Unlikely stops with conservative therapy
2 patients responded to medical management
Our experience consistent with Mayo Clinic experienceSurgical intervention
Combined team:
Otolaryngology & neurosurgery

Intracranial Advantage:
ability to achieve a fluid-tight dural closure
repair multiple areas of leakage. Treat associated problems e.g. tumors
Disadvantage: morbidity, mortality prolonged hospitalization period Loss of olfaction
Surgical management

Extracranial (Extranasal & Intranasal) Advantage:
minimal morbidity and mortality while still achieving excellent visualization of the dural defect
Disadvantage: precise, preoperative localization of the
leakage site
Surgical management

Graft selection:a. Connective tissue grafts:
Fascia lata, temporalis fascia, nasal septal cartilage
b. Mucosal grafts: Contralateral inf. turbinate
c. Other grafts: Lyophilized dura, synthetic dura, glass-
ionomer bone cement
Surgical management

Orbit
Dura
Graft
Cerebrum

Orbit
Dura
Graft
Cartilage
Cerebrum

Olfactory Disorders Olfactory bulb lies on top of
the cribriform plate at the base of the brain
Olfactory epithelium: upper septum & lat nasal cavity
Epithelium:1. olfactory receptor (bipolar
neuron) 2. microvillar cell (another
type of olfactory receptor cell)
3. supporting, or sustentacular, cells
4. basal cells (stem cells to replace the dying olfactory receptors)

Causes1. Obstructive Nasal and Sinus Disease 2. Olfactory Loss Following Upper Respiratory Infection
damage to olfactory neurons at the level of the epithelium, the bulb, or the central olfactory tracts
1/3 of patients will regain olfactory ability in 3 to 6 months
3. Head Trauma 5% to 10% of adults who have sustained both major
and minor head trauma shearing of the delicate fila olfactoria nerves as they
pass through the cribriform plate 8% to 39% of the patients recovery of olfactory
function usually within 3 months
Olfactory Disorders

4. Toxins Formalduhyde, benzene, smoking Permenant
5. Aging olfactory loss in old people can occur from
dementia-related diseases two dementia-related diseases: Alzheimer’s
disease and Parkinson’s disease
6. Congenital hypogonadotrophic hypogonadism (Kallmann’s
syndrome
Olfactory Disorders

Midline Nasal Masses
Congenital masses of neuroectodermal origin
Lesion Dural connection Transillumination Furstenberg’s test Meningitis Histology
Glioma None No Negative No Solid mass of glial tissue
with a fibrous stalk
Encephalocele Always Yes Positive YesEpendymal-lined space
that communicates with
the ventricles
Dermoid Rare Rarely Negative Rare Fluctuating cyst with
sinus tract leading to skin

Midline Nasal Masses