Embed Size (px)
Citation preview
Dissemination of Cancer with Special Emphasis onVascular Spread and Implantation'
W. H. COLE, M.D., S. S. ROBERTS, M.D., R. S. WEBB, JR., M.D.,F. W. STREHm, M.D., G. D. OATES, F.R.C.S.
From the Department of Surgery, University of Illinois College of Medicine,Chicago, Illinois
THERE ARE four known major mechanismsfor the spread of cancer: 1) contiguity, 2)lymphatics, 3) vascular spread and 4) im-plantation. An enormous amount of workhas been done on the spread by contiguity(local invasion) and by the lymphatics. Ac-cordingly, the purpose of this report con-cerns vascular spread and implantation.
Factors Influencing Spread of Cancer
It is well known that some tumors growrapidly whereas others grow slowly. Wecannot explain this difference in growthrate except that it is related to virulence ofthe cancer cell and host resistance. Thelatter is probably more important. Coman 12emphasized the importance of the loss ofcohesiveness of cancer cells in dissemina-tion. He explained that the benign cells aremotile (as are malignant cells) but thatthey are attached so tightly together thatthey rarely break loose and circulate as docancer cells. Coman attributed this loss ofcohesiveness to a deficiency in calcium, al-though certain enzymes (e.g. hyaluroni-dase) may exert an influence on detach-ment of cells.The mitotic time might have a role in the
growth of cancer cells, but since the mitotictime of malignant cells is not shorter thanthat of benign cells this factor probablyhas significance in the uncontrolled growth
of cancer cells. More important is the factthat the benign cell ceases to grow in thereparative process and no overgrowth isencountered. When a tumor develops thecells continue to multiply even though in-creased pressure is developed.
Several authors (Wood,44 Zeidman,47 andCliffton and associates 10) have discussedthe influence of a thrombus at the site oflodgment of cancer cells on their growthand showed that heparin and other anti-coagulants will discourage the growth ofcancer cells.
Vascular Spread of CancerIn 1932 Pool and Dunlop 28 reported the
isolation of cancer cells from the circulatingblood. Since 1955 numerous authors 13,30have corroborated this finding and have re-ported varying percentages of positiveblood samples for various tumors. It is nowagreed that in the early reports these cellswere "overdiagnosed." Numerous bloodcells including granulocytes, monocytes,histiocytes and especially megakaryocyteshave been confused with cancer cells. Someof the difficulty in differentiating thesevarious cells may stem from the possibilitythat the megakaryocytes in patients withcancer have a different histologic appear-ance from those in normal individuals, assuggested by Romsdahl and associates.34Lest the difficulty in positively identifyingcancer cells leads one into thinking thatthe question of cancer cells in the blood is
753
* Presented before the Southern Surgical As-sociation, Dec. 8-10, Boca Raton, Florida.
Aided by NIH Grants 3482 and 9594.
COLE AND OTHERS Annals of SurgeryMay 1965
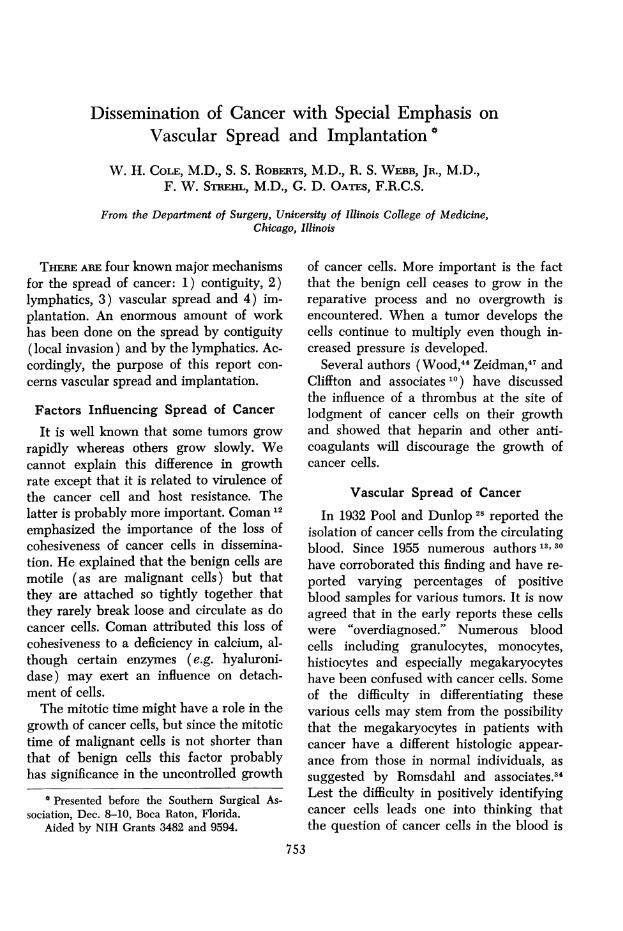
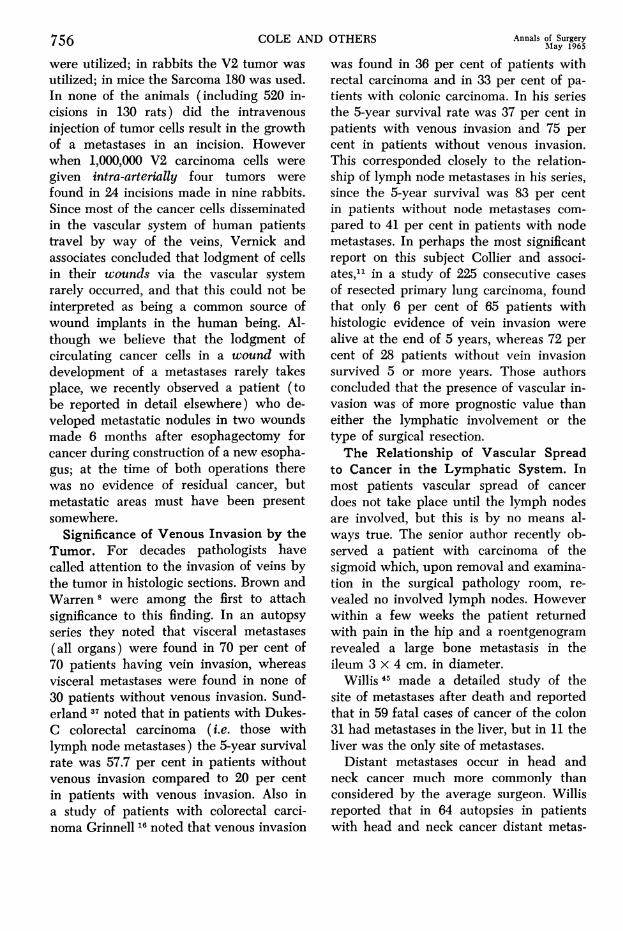
FIG. 1. Carcinoma ofthe kidney, Papanicolaoustain. A. Direct smearof resected tumor. B.Clumps of cancer cellsisolated from blood aspi-rated from the renal veinduring nephrectomy.
not important, we would like to emphasizethat with the exception of head and necktumors, the vascular spread of the tumorrepresents the most important lethal factorin progress of the disease. It is well knownthat metastases develop in certain organsmore readily than in others. This soil hy-pothesis was presented by Paget in 1889.Lucke and associates 22 injected tumor cellsinto the intraportal and pulmonary circula-tions and observed the growth of tumors.They noted that larger tumors were pro-
duced in the liver than in the lungs andthat the total mass of tumor in the lungwas less than that in the liver. It is wellknown that cells and even clumps of cellswill pass through capillaries (Fig. 1).
Prinzmetal and associates 29 have shownthat there are vascular shunts in the lungs,kidney, liver and spleen of dogs and rab-bits with a size many times the diameterof capillaries. These arteriovenous shuntswill explain the transport of cells from one
organ to another without going through thecapillaries. They proved evidence of theseshunts by injection of tiny glass spheres.We would like to add that cancer cells
may gain access to the systemic circulationthrough intravasation, or the passage ofcells from malignant tissue into vascularchannels through anatomic defects, some
of which may be created by trauma.
Number of Cells Required to ProduceGrowth of Tumors. Years ago it was
thought that the escape of a few cancer
cells from the primary growth would pro-
duce metastases with consequent death tothe patient in every instance. HoweverWarren and Gates,4' in 1936, presented evi-dence indicating that the mortality of em-
bolic cancer cells was very high and evi-dence that this hypothesis is valid has beenaccumulating. In 1950 Zeidman and associ-ates 46 reported that in a group of C57 miceinjected with 104,400 Sarcoma-241 cells theaverage number of pulmonary metastaseswas only 11.5. When 5,400 cells were in-jected the average number of pulmonarymetastases was 1.7; when 900 cells were in-jected the average number of pulmonarymetastases was 0.31. Fisher and Fisher 14
noted that when 100 Walker-256 tumor cellswere injected into the portal vein, tumorsdeveloped in only 30 per cent of the rats.If 5,000 cells were injected, 58 per cent ofthe animals developed tumors. Moore andassociates,26 working with the Ehrlich As-cites tumor, noted that when 100,000 cellswere injected intraperitoneally, tumors de-veloped in 28 of 37 animals; when cellswere inoculated subcutaneously, tumors de-veloped in 96 of 102 animals.Time of Disappearance of Cells Follow-
ing Intravenous Inoculation. Madden and
754
DISSEMINATION OF CANCER
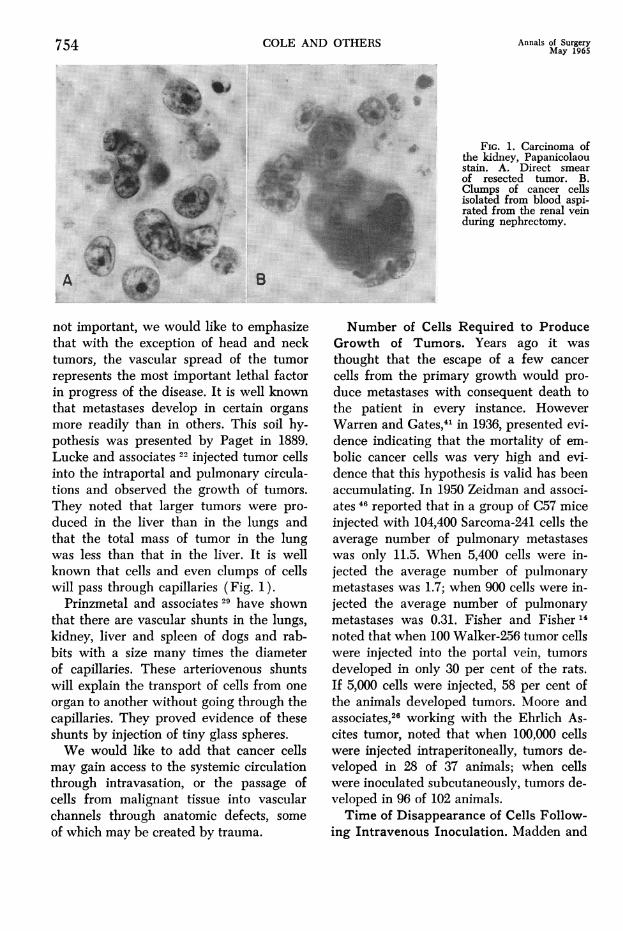
Malmgren 23 injected various numbers ofMPC-3 tumor cells into the tail vein ofBALB/c mice and counted the cells in theblood from the right chamber of the heartat varying intervals after inoculation ofcells. They found that after the inoculationof 50,000 cells, none were found in theblood in the right side of the heart. Afterthe inoculation of 1,000,000 cells, an aver-
age of three cells per 0.5 ml. of blood were
encountered 3 to 5 min. following intra-venous inoculation. Following the injectionof 5,000,000 MPC-3 tumor cells, an average
of 739 cells were found per 0.5 ml. ofblood, but the count dropped sharply toan average of nine at 3 min. and an averageof three at 10 min. Hengesh and associ-ates 19 likewise noted rapid disappearanceof cells from the blood stream after intra-venous inoculation of 4,000,000 EhrlichAscites tumor cells. The cells were injectedinto the tail vein and blood samples ob-tained by direct cardiac puncture at thetime of sacrifice. Although a large numberof cells were found in the blood immedi-ately after injection, at the end of 30 min.no tumor cells could be recovered.
Influence of Trauma and Manipulationof Tumor on Dissemination of Cancer. In1913 Tyzzer inoculated Japanese waltzingmice with tumor cells subcutaneously andmassaged the subsequent tumor to deter-mine the effect on metastases in the lungs.He found that only 9 per cent of controlmice (not subjected to massage) developedpulmonary metastases, whereas 66 per centof 34 mice having massage of their tumordeveloped pulmonary metastases. Roms-dahl 33 of our laboratory recently conductedsimilar experiments with the Walker-256tumor following inoculation of Walker cellsinto the thigh muscles. Twelve to 21 daysafter inoculation, when tumors had de-veloped, the tumors were massaged for 30seconds. Blood was obtained from the vena
cava. Before manipulation no tumor cellswere noted. During manipulation a large
number of tumor cells were found, but atthe end of 15 min. none were demonstrable.Robinson and Hoppe 31 of our laboratory
conducted an experiment to determinewhat effect trauma would have on the de-velopment of metastases following inocula-tion of cells. Under pentobarbital anesthesia1,000,000 cells were inoculated into theaorta and the thigh was subjected to trauma(produced by allowing a 3-pound hammerto fall repeatedly from a height of 3 in. on
the thigh). In half the animals trauma was
applied one minute before cell injectionand in the other half one minute after theinjection. The animals were sacrificed at theend of 20 days. The number of tumornodules developing after inoculation ofcells was five to eight times as high in thetraumatized limb as in the control limb.Alexander and Altmeier 2 conducted some
experiments determining the effect oftrauma on the spleen (produced by injec-tion of nitrogen mustard) in rabbits fol-lowing the inoculation of V2 carcinomacells. They noted that 67 per cent of thetest animals developed metastases to thedamaged spleen whereas metastases were
found in only 8 per cent of the control ani-mals. They also noted that "even intestinaldamage from operative manipulation re-
sulted in an increase in intestinal metas-tases." However these cells were also inocu-lated intra-arterially, which may not allowclinical interpretation because human tu-mor cells (lung cancer excepted) escape
into the veins.There is considerable doubt as to how
often recurrences in a wound made for in-cision of a cancer develop from blood-borne cells and how often they are due toimplantation by cells dislocated at the timeof the operation. To test this hypothesis,Vernick and associates 39 of our laboratorymade several hundred incisions through theskin and muscle in various animals one
hour previous to inoculation of cancer cells.In rats the Walker-256 tumor (25,000 to500,000 cells) and the Guerin uterine tumor
Volume 161Number 5 755
756 COLE AND OTHERS
were utilized; in rabbits the V2 tumor wasutilized; in mice the Sarcoma 180 was used.In none of the animals (including 520 in-cisions in 130 rats) did the intravenousinjection of tumor cells result in the growthof a metastases in an incision. Howeverwhen 1,000,000 V2 carcinoma cells weregiven intra-arterially four tumors werefound in 24 incisions made in nine rabbits.Since most of the cancer cells disseminatedin the vascular system of human patientstravel by way of the veins, Vernick andassociates concluded that lodgment of cellsin their wounds via the vascular systemrarely occurred, and that this could not beinterpreted as being a common source ofwound implants in the human being. Al-though we believe that the lodgment ofcirculating cancer cells in a wound withdevelopment of a metastases rarely takesplace, we recently observed a patient (tobe reported in detail elsewhere) who de-veloped metastatic nodules in two woundsmade 6 months after esophagectomy forcancer during construction of a new esopha-gus; at the time of both operations therewas no evidence of residual cancer, butmetastatic areas must have been presentsomewhere.
Significance of Venous Invasion by theTumor. For decades pathologists havecalled attention to the invasion of veins bythe tumor in histologic sections. Brown andWarren 8 were among the first to attachsignificance to this finding. In an autopsyseries they noted that visceral metastases(all organs) were found in 70 per cent of70 patients having vein invasion, whereasvisceral metastases were found in none of30 patients without venous invasion. Sund-erland 37 noted that in patients with Dukes-C colorectal carcinoma (i.e. those withlymph node metastases) the 5-year survivalrate was 57.7 per cent in patients withoutvenous invasion compared to 20 per centin patients with venous invasion. Also ina study of patients with colorectal carci-noma Grinnell 16 noted that venous invasion
Annals of SurgeryMlay 1965
was found in 36 per cent of patients withrectal carcinoma and in 33 per cent of pa-tients with colonic carcinoma. In his seriesthe 5-year survival rate was 37 per cent inpatients with venous invasion and 75 percent in patients without venous invasion.This corresponded closely to the relation-ship of lymph node metastases in his series,since the 5-year survival was 83 per centin patients without node metastases com-pared to 41 per cent in patients with nodemetastases. In perhaps the most significantreport on this subject Collier and associ-ates,'1 in a study of 225 consecutive casesof resected primary lung carcinoma, foundthat only 6 per cent of 65 patients withhistologic evidence of vein invasion werealive at the end of 5 years, whereas 72 percent of 28 patients without vein invasionsurvived 5 or more years. Those authorsconcluded that the presence of vascular in-vasion was of more prognostic value thaneither the lymphatic involvement or thetype of surgical resection.The Relationship of Vascular Spread
to Cancer in the Lymphatic System. Inmost patients vascular spread of cancerdoes not take place until the lymph nodesare involved, but this is by no means al-ways true. The senior author recently ob-served a patient with carcinoma of thesigmoid which, upon removal and examina-tion in the surgical pathology room, re-vealed no involved lymph nodes. Howeverwithin a few weeks the patient returnedwith pain in the hip and a roentgenogramrevealed a large bone metastasis in theileum 3 x 4 cm. in diameter.
Willis 45 made a detailed study of thesite of metastases after death and reportedthat in 59 fatal cases of cancer of the colon31 had metastases in the liver, but in 11 theliver was the only site of metastases.
Distant metastases occur in head andneck cancer much more commonly thanconsidered by the average surgeon. Willisreported that in 64 autopsies in patientswith head and neck cancer distant metas-
DISSEMINATION OF CANCER
tases were found in 39 per cent of cases.
Most of these were in the lung and liver,although metastases were found in 16 mis-cellaneous sites. Hoye and associates 21 as-
sembled data from ten sources on the in-cidence of distant metastases in head andneck cancer and found a range of 5 to 50per cent and an average of 21 per cent.
Wound Contamination and ImplantationThere is a moderate amount of contro-
versy concerning the origin of recurrentnodules in the wound following a majoroperation for cancer. It is obvious that someof the local recurrences are due to inade-quate removal of the primary tumor. Atthe time of operation the surgeon usuallyknows whether or not he has excised thetumor adequately; if his line of excisionextends close to the tumor, the probabilityof residual tumor is strong.
Excluding the inadequate excision of thetumor, implantation may be spontaneous or
iatrogenic. Spontaneous implantation ofcancer cells is well known, as exemplifiedby the peritoneal metastases so oftenfound at operation for cancer of the gastro-intestinal tract. These metastases are ob-viously spontaneous. On other occasionsthere may be no demonstrable metastasesin the thoracic or peritoneal cavity but ina variable length of time, metastases may
develop; these may have been spontaneousinsofar as cells may have desquamatedfrom the primary tumor before operation,unrelated to the operative manipulation.On other occasions it seems very probablethat there may have been no cells driftingspontaneously from the primary tumor, butthe surgeon may have disseminated thecells by operative manipulations.One of the first surgeons to have called
attention to the danger of disseminationof cancer by operative manipulation was
Gerster (1885). Occasionally thereafter(Lack in 1896 and Ryall in 1907), thisdanger has been re-emphasized. For ex-
ample Ryall reported 25 patients having
recurrence of one type or another in thewound made during the operative pro-
cedure. These local recurrences, secondaryto dissemination by the surgeon, may occur
almost anywhere in the body and underall types of circumstances. Many of themhave been reported in the needle track fol-lowing aspiration of a tumor with a needleand syringe. Some have been in skin graftsand some in the donor site of skin grafts.Occasionally they are found in the drain-age site where the abdominal cavity was
drained following a resection of a carci-noma. Ackerman and Wheat 1 made a spe-
cific study of this complication and reportedlocal recurrences in skin grafts, on the peri-toneum in the abdominal cavity, and in theperitoneal wound following abdominoperi-neal resection. Cancer cells actually havebeen found on the knives used by thesurgeon.One of the most unique examples of im-
plantation is that reported by Beahrs andassociates 6 (reporting on 4 patients) inwhich an adenocarcinoma from a tumorof the rectum or colon had developed inthe scar of a hemorrhoidectomy. These pa-
tients had had a hemorrhoidectomy duringthe time when they actually had a carci-noma of the large bowel from which thecells drifted downward and implanted inthe hemorrhoidectomy wound.About 10 years ago three different groups
became worried about the high incidenceof development of recurrences in the sutureline following resection of the colon forcancer. By utilizing precautions such as
prophylactic irrigation of the bowel lumen,and ligation of the bowel several inchesproximal and distal to the tumor, and ex-
cision of the crushed ends of the bowel be-fore application of sutures, these threegroups reported that local recurrences hadbeen eliminated almost completely; thisrepresents proof, or strong evidence, thatthe recurrences were due to implantationand not to lodgment of circulating tumorcells or new tumors.
Volume 161Number 5 757

COLE AND OTHERS Annals of SurgeryMay 1965
TABLE 1. Local Recurrence in Breast Cancer (after Radical Mastectomy)
Hospital and Source No. Cases % Recurrence Comments
Cleveland Clinic (Robnett, Jones & Hazard32) 203 14.2Presbyterian Hosp. (N.Y.) (Haagensen17) 356 15.2U. of Chicago (Allen & Rigler3) 230 12Mass. Gen. Hosp. (Taylor & Wallace38) 236 11 15%, if biopsied
7.5% if not biopsiedSt. Luke's Hosp. (N.Y.) (Shore35) 116 6.9 if limited to breast
244 21.3 if ax. nodes involvedHenry Ford Hosp. (Hoopes & McGraw20) Plastic 97 6.1 if limited to breast
closure & skin graft 149 20.8 if ax. nodes involvedRoosevelt Hosp. (N.Y.) (White42) 101 10.8 if limited to breast
137 31.5 if ax. nodes involved
As stated above, many surgeons havecalled attention to the probability that can-
cer cells disseminating from the wound atthe time of operation are the cause of a
major portion of the local recurrences.
These cells presumably might escape fromthe severed ends of lymph channels andsmall blood vessels or may have beensqueezed out of the tumor through tissueplanes into the wound.
Local Recurrence. It is our contentionthat residual tumor is too often blamed forthe local recurrence. Although local recur-
rence may occur in any wound followingexcision for cancer it appears to be more
common following radical mastectomy andradical neck dissection. A survey of theliterature reveals a large number of reportswhich give the percentage local recurrence
for these operations. Table 1 shows thatthere is a marked similarity in the variousreports regarding the incidence of localrecurrence in breast cancer. Taylor andWallace 38 reported an incidence of recur-
rence of 7.5 per cent in patients not bi-opsied and 15 per cent in patients havinga biopsy. They stated that of 236 patientshaving radical mastectomy, 116 had a bi-opsy with immediate histologic examina-tion; presumably the remainder did nothave a biopsy. Another significant aspect ofthese data is the marked increase in theincidence when the axillary nodes were in-volved. Likewise, there was close agree-
ment on this incidence in the three reportsproviding that data.The local recurrence rate in the neck fol-
lowing radical neck dissection for cancer ishigher than that following radical mastec-tomy. Many of these recurrences are, ofcourse, due to inadequate excision. How-ever we believe that a major portion are
due to implantation of cells which were
disseminated at operation by mechanismsalready mentioned. The fact that most ofthe primary lesions in this group were
ulcerating in the mouth, and that the neckdissection was often performed in conti-nuity (a desirable and justified procedure),offers an obvious mechanism for dissemina-tion of cells from the primary lesion intothe neck, unless the primary lesion was
completely destroyed by cautery or some
such procedure at the onset of the opera-tion. In a recent study, Beahrs and Barber 7
report local recurrence in 26.5 per cent of616 patients having radical neck dissectionfor cancer of the lip, mouth and larynx andstate that they believed that in 46 per centof the recurrences "seeding" was the causa-
tive mechanism. Local recurrence rates inhead and neck cancer as recorded by nu-
merous authors are listed in Table 2.
Case ReportsCase 1. A 66-year-old man was admitted to
the University of Illinois Hospitals in May, 1962with the chief complaint of a perianal mass of 9
758
Volume 161Number 5
DISSEMINATION OF CANCER 759TABLE 2. Local Recurrence in Head and Neck Cancer (after Radical Neck Dissection)
Hospital Site No. Cases % Recurrence
Memorial Hosp. (N.Y.) (Martin et al.24) Mouth (all sites) 303 33.3Memorial Hosp. (N.Y.) (Harroldl8) Mouth (floor of mouth, gingiva, tongue, 204 43.6
buc. muc.)U. of Colorado (Morfit27) Mouth (8 diff. sites) 58 44Nat. Cancer Inst. (Arons & Smith4) Mouth (11 diff. sites) 72 43Emory Univ. (Wilkins & Vogler43) Gingiva 81 27.1Westminster Hosp. (Cade & Lee9) Tongue 81 19.7Memorial Hosp. (Frazell & Lucas"5) Tongue 227 39Mayo Clinic (Beahrs et al.5) Tongue 217 27Mayo Clinic (Beahrs & Barber7) Lip, mouth, larynx 615 26.5
months duration. At the time the perianal masswas first noted, there were signs of local inflamma-tion. A biopsy revealed no evidence of malignancy.There was evidence of considerable mucous secre-tions from the fistula which failed to heal andcontinued to discharge mucus. There was no priorhistory of an anal fistula.
Four years prior to this illness the patient hadan emergency transverse colostomy followed byanterior resection for adenocarcinoma of the sig-moid colon. At the time of colostomy closure 32years prior to admission, a local recurrence wasfound in the area of the previous anastomosis. Aleft hemicolectomy was then done.
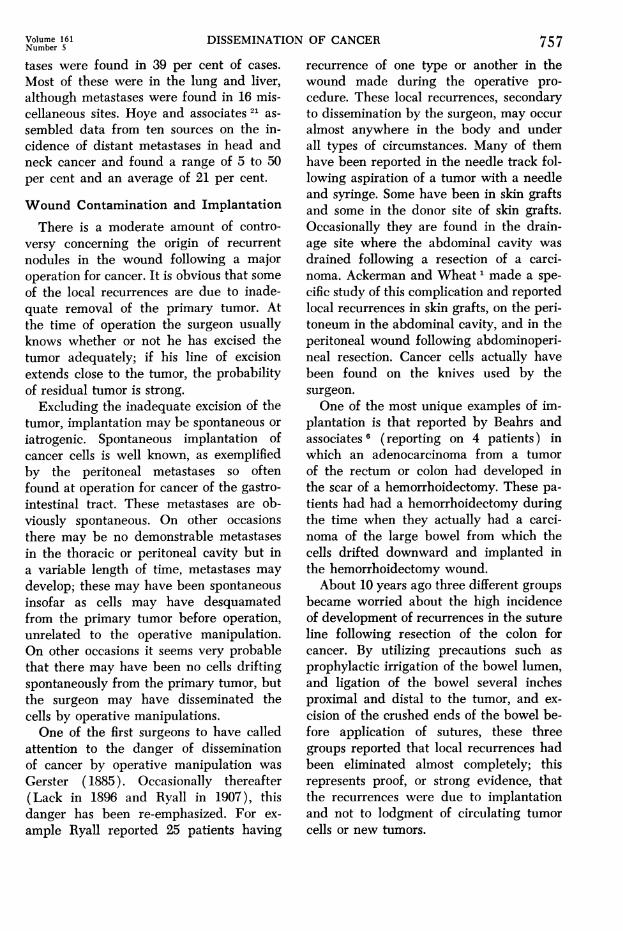
Examination on admission revealed a well cir-cumscribed, elevated, ulcerated mass 3 x 2.5 cm.on the perineal skin just anterior to the anus. Dur-ing rectal examination mucous secretions exudedfrom a single fistulous opening at the margin ofthe tumor mass. A small polyethylene cathetercould be inserted easily into the opening of thefistula and threaded upward until it entered theinternal opening of the anal fistula in an anteriorcrypt of Morgagni (Fig. 2A). No tumor waspalpable or visible within the rectum, and procto-sigmoidoscopy to 22 cm. was negative. A biopsyof the perianal mass revealed this to be a mucous-producing adenocarcinoma. There were no palpa-ble inguinal lymph nodes. Liver function testswere normal.
The patient refused abdominal perineal resec-tion but consented to a local excision. Accordinglyon May 18, 1962 a wide perineal excision wascarried out, including a portion of the externalsphincter and the internal opening of the fistula.The postoperative course was uneventful.
Dissection of the specimen revealed a circum-scribed, lobulated tumor measuring 3 X 2.5 X 2.5cm. (Fig. 2B). Upon opening the fistulous tractfrom the external to the internal opening, it wasfound to be single and lined by rough grayish
FiG. 2. Photographs of patient (Case 1) withimplantation of mucinous carcinoma in a perianalfistula. A. Photograph of lesion on perineum ad-jacent to the base of scrotum. Note polyethylenetube which has been inserted into the singlefistulous tract. B. Gross photograph of resectedspecimen which includes a portion of internalsphincter and mucosa. Tumor is limited to skinand subcutaneous tissue and there is no evidenceof tumor in or near the rectal mucosa.
COLE AND OTHERS Annals of SurgeryMay 1965
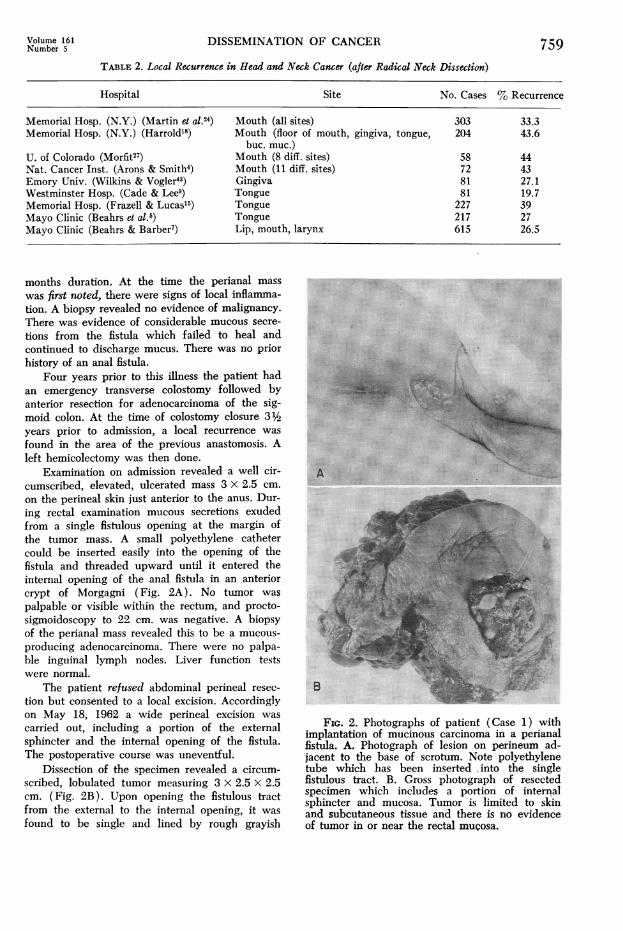
FIG. 2. C. Photomi-crograph showing a mu-cinous adenocarcinoma oflesion shown in B. D.Photomicrograph of colontumor resected 4 yearsprior to the lesion on theperineum. The patholo-gists report this tumor assimilar to the originalcolon tumor removed 4years previously.
tissue. Microscopic examination of the mass showedmucinous adenocarcinoma (Fig. 2C) and a fis-tulous tract lined by gradulation tissue. There was
no evidence of glandular epithelium lining thefistulous tract, and there was no muscularis mucosa.
The microscopic pattern of the mucinous adeno-carcinoma was similar to the original colon tumorremoved 4 years previously (Fig. 2D).
The patient is living and without evidence ofrecuirrence 2 1/_ years later.
Comment. Mucous-producing adenocar-cinoma complicating an anal fistula is ex-
ceedingly rare. We believe this patient pro-
vides a clear example of implantation in thefistula-in-ano from the previous colon tu-mor. However the possibility of colloid car-
cinoma arising in a congenital fistula-in-anomust be excluded. The fistulous tract inthis patient was lined by granulation tissueand not rectal mucosa, thus excluding a col-loid carcinoma arising in a congenital tract.In addition, mucoid carcinoma developingon a long-standing high fistula-in-ano must
760
Volume 161Number 5
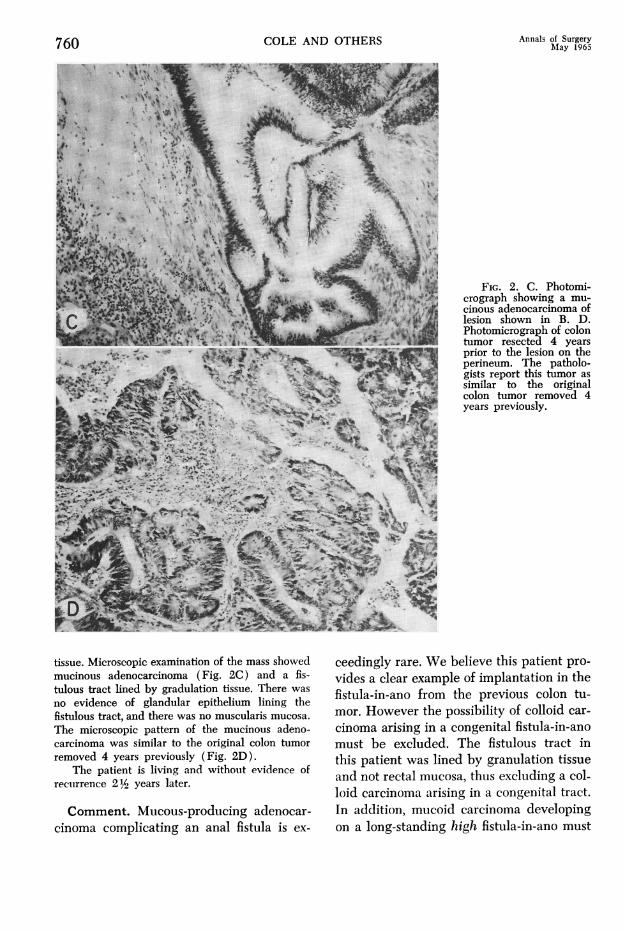
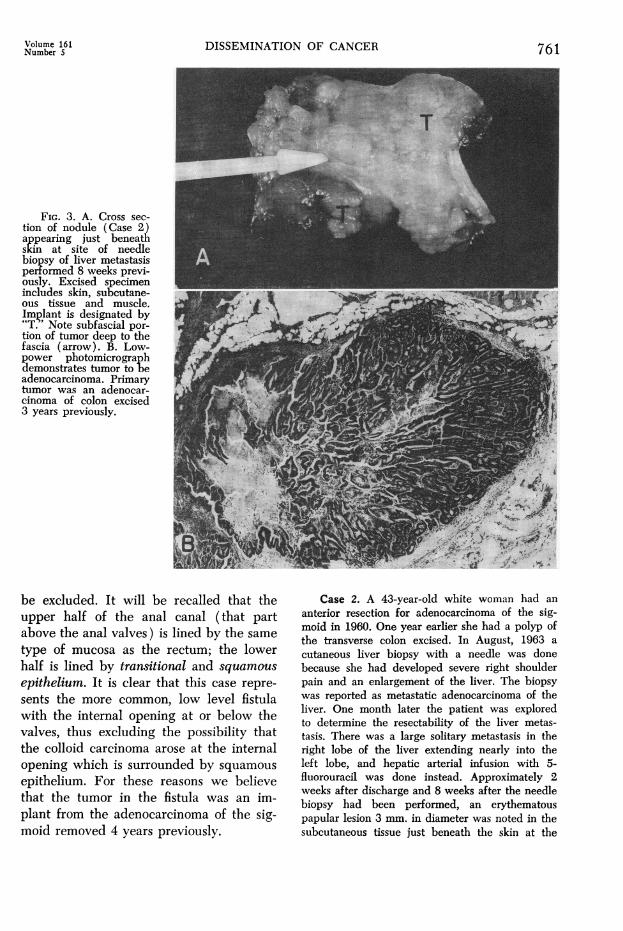
FIG. 3. A. Cross sec-tion of nodule (Case 2)appearing just beneathskin at site of needlebiopsy of liver metastasisperformed 8 weeks previ-ously. Excised specimenincludes skin, subcutane-ous tissue and muscle.Implant is designated by"T.' Note subfascial por-tion of tumor deep to thefascia (arrow). B. Low-power photomicrographdemonstrates tumor to beadenocarcinoma. Primarytumor was an adenocar-cinoma of colon excised3 years previously.
DISSEMINATION OF CANCER
be excluded. It will be recalled that theupper half of the anal canal (that partabove the anal valves) is lined by the same
type of mucosa as the rectum; the lowerhalf is lined by transitional and squamous
epithelium. It is clear that this case repre-
sents the more common, low level fistulawith the internal opening at or below thevalves, thus excluding the possibility thatthe colloid carcinoma arose at the internalopening which is surrounded by squamous
epithelium. For these reasons we believethat the tumor in the fistula was an im-plant from the adenocarcinoma of the sig-moid removed 4 years previously.
Case 2. A 43-year-old white woman had an
anterior resection for adenocarcinoma of the sig-moid in 1960. One year earlier she had a polyp ofthe transverse colon excised. In August, 1963 acutaneous liver biopsy with a needle was donebecause she had developed severe right shoulderpain and an enlargement of the liver. The biopsywas reported as metastatic adenocarcinoma of theliver. One month later the patient was exploredto determine the resectability of the liver metas-tasis. There was a large solitary metastasis in theright lobe of the liver extending nearly into theleft lobe, and hepatic arterial infusion with 5-fluorouracil was done instead. Approximately 2weeks after discharge and 8 weeks after the needlebiopsy had been performed, an erythematouspapular lesion 3 mm. in diameter was noted in thesubcutaneous tissue just beneath the skin at the
761
|3_.Jfi
762
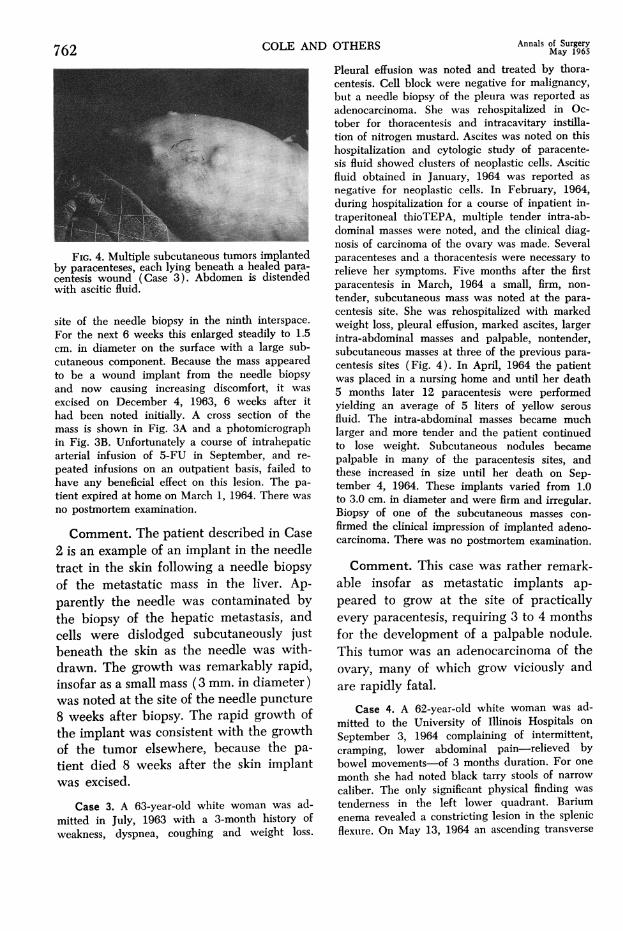
FIG. 4. Multiple subcutaneous tumorsby paracenteses, each lying beneath a hecentesis wound (Case 3). Abdomen iswith ascitic fluid.
site of the needle biopsy in the ninthFor the next 6 weeks this enlarged stealcm. in diameter on the surface with a
cutaneous component. Because the massto be a wound implant from the nee(
and now causing increasing discomfoexcised on December 4, 1963, 6 wee]
had been noted initially. A cross sectimass is shown in Fig. 3A and a photorin Fig. 3B. Unfortunately a course of irarterial infusion of 5-FU in Septembepeated infusions on an outpatient basishave any beneficial effect on this lesiortient expired at home on March 1, 1964.no postmortem examination.
Comment. The patient describe(2 is an example of an implant in tltract in the skin following a needof the metastatic mass in the 1lparently the needle was contamithe biopsy of the hepatic metastcells were dislodged subcutaneobeneath the skin as the needle v
drawn. The growth was remarkalinsofar as a small mass (3 mm. in dwas noted at the site of the needle8 weeks after biopsy. The rapid gthe implant was consistent with tbof the tumor elsewhere, becausetient died 8 weeks after the skirwas excised.
Case 3. A 63-year-old white womamitted in July, 1963 with a 3-monthweakness, dyspnea, coughing and w
COLE AND OTHERS Annals of SurgeryCOLEANDOTHERS ~~~~~~~May1965
Pleural effusion was noted and treated by thora-centesis. Cell block were negative for malignancy,but a needle biopsy of the pleura was reported asadenocarcinoma. She was rehospitalized in Oc-tober for thoracentesis and intracavitary instilla-tion of nitrogen mustard. Ascites was noted on thishospitalization and cytologic study of paracente-sis fluid showed clusters of neoplastic cells. Asciticfluid obtained in January, 1964 was reported asnegative for neoplastic cells. In February, 1964,during hospitalization for a course of inpatient in-traperitoneal thioTEPA, multiple tender intra-ab-dominal masses were noted, and the clinical diag-nosis of carcinoma of the ovary was made. Several
implanted paracenteses and a thoracentesis were necessary to
adedtpara- relieve her symptoms. Five months after the firstdistend-edparacentesis in March, 1964 a small, firm, non-tender, subcutaneous mass was noted at the para-
interspace. centesis site. She was rehospitalized with markedinterspace. weight loss, pleural effusion, marked ascites, largerdily to 1.5 intra-abdominal masses and palpable, nontender,large sub- subcutaneous masses at three of the previous para-
dlappeared centesis sites (Fig. 4). In April, 1964 the patientdle biopsy was placed in a nursing home and until her death
krt, it was 5 months later 12 paracentesis were performedks after it yielding an average of 5 liters of yellow serousion of the fluid. The intra-abdominal masses became muchnicrograph larger and more tender and the patient continuedntrahepatic to lose weight. Subcutaneous nodules becamer, and re- palpable in many of the paracentesis sites, andfailed to these increased in size until her death on Sep-
n. The pa- tember 4, 1964. These implants varied from 1.0There was to 3.0 cm. in diameter and were firm and irregular.
Biopsy of one of the subcutaneous masses con-
d in Case firmed the clinical impression of implanted adeno-heineCae carcinoma. There was no postmortem examination.hie needlele biopsy Comment. This case was rather remark-iver. Ap- able insofar as metastatic implants ap-nated by peared to grow at the site of practicallytasis, and every paracentesis, requiring 3 to 4 months)usly just for the development of a palpable nodule.vas with- This tumor was an adenocarcinoma of the)ly rapid, ovary, many of which grow viciously andliameter) are rapidly fatal.punctureprowth of Case 4. A 62-year-old white woman was ad-' mitted to the University of Illinois Hospitals onie growth September 3, 1964 complaining of intermittent,- the pa- cramping, lower abdominal pain-relieved by1 implant bowel movements-of 3 months duration. For one
month she had noted black tarry stools of narrow
caliber. The only significant physical finding was
in was ad- tenderness in the left lower quadrant. Bariumhistory of enema revealed a constricting lesion in the splenic
reight loss. flexure. On May 13, 1964 an ascending transverse
Volume 161 DISSEMINATION OF CANCERNumber 5
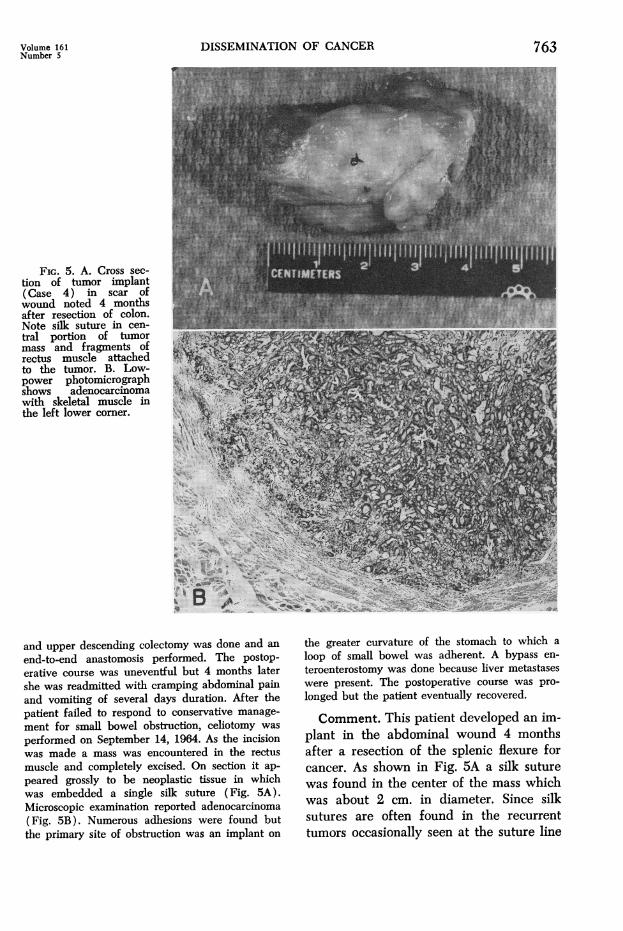
FIG. 5. A. Cross sec-tion of tumor implant(Case 4) in scar ofwound noted 4 monthsafter resection of colon.Note silk suture in cen-tral portion of tumormass and fragments ofrectus muscle attachedto the tumor. B. Low-power photomicrograph
shows adenocarcinoma
with skeletal muscle inthe left lower corner.
A..
; '; 1, 't^ E a-
.,i : .,
db 4X}'^" ''^'; <>,.:.^.
and upper descending colectomy was done and an
end-to-end anastomosis performed. The postop-erative course was uneventful but 4 months latershe was readmitted with cramping abdominal painand vomiting of several days duration. After thepatient failed to respond to conservative manage-
ment for small bowel obstruction, celiotomy was
performed on September 14, 1964. As the incisionwas made a mass was encountered in the rectus
muscle and completely excised. On section it ap-
peared grossly to be neoplastic tissue in whichwas embedded a single silk suture (Fig. 5A).Microscopic examination reported adenocarcinoma(Fig. 5B). Numerous adhesions were found butthe primary site of obstruction was an implant on
the greater curvature of the stomach to which a
loop of small bowel was adherent. A bypass en-
teroenterostomy was done because liver metastaseswere present. The postoperative course was pro-
longed but the patient eventually recovered.
Comment. This patient developed an im-plant in the abdominal wound 4 monthsafter a resection of the splenic flexure forcancer. As shown in Fig. 5A a silk suturewas found in the center of the mass whichwas about 2 cm. in diameter. Since silksutures are often found in the recurrenttumors occasionally seen at the suture line
763
764 COLE AND
following resection of the colon for carci-noma, it appears that the silk suture may
have a causative influence in the develop-ment of the recurrence. If it does, it mightbe assumed that a great majority of cellsdisplaced into the wound during the opera-
tion die, but that if they are displaced intothe tract made by the suture the circum-
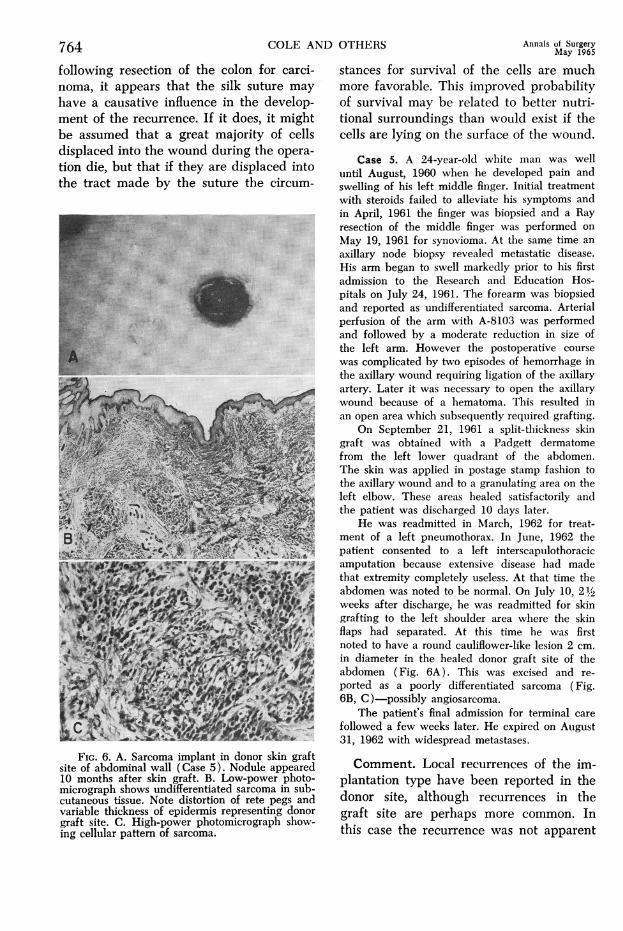
FIG. 6. A. Sarcoma implant in donor skin graftsite of abdominal wall (Case 5). Nodule appeared10 months after skin graft. B. Low-power photo-micrograph shows undifferentiated sarcoma in sub-cutaneous tissue. Note distortion of rete pegs andvariable thickness of epidermis representing donorgraft site. C. High-power photomicrograph show-ing cellular pattern of sarcoma.
OTHERS Annals of SurgeryMay 1965
stances for survival of the cells are muchmore favorable. This improved probabilityof survival may be related to better nutri-tional surroundings than would exist if thecells are lying on the surface of the wound.
Case 5. A 24-year-old white man was welluntil August, 1960 when he developed pain andswelling of his left middle finger. Initial treatmentwith steroids failed to alleviate his symptoms andin April, 1961 the finger was biopsied and a Rayresection of the middle finger was performed onMay 19, 1961 for synovioma. At the same time anaxillary node biopsy revealed metastatic disease.His arm began to swell markedly prior to his firstadmission to the Research and Education Hos-pitals on July 24, 1961. The forearm was biopsiedand reported as undifferentiated sarcoma. Arterialperfusion of the arm with A-8103 was performedand followed by a moderate reduction in size ofthe left arm. However the postoperative coursewas complicated by two episodes of hemorrhage inthe axillary wound requiring ligation of the axillaryartery. Later it was necessary to open the axillarywound because of a hematoma. This resulted inan open area which subsequently required grafting.
On September 21, 1961 a split-thickness skingraft was obtained with a Padgett dermatomefrom the left lower quadrant of the abdomen.The skin was applied in postage stamp fashion tothe axillary wound and to a granulating area on theleft elbow. These areas healed satisfactorily andthe patient was discharged 10 days later.
He was readmitted in March, 1962 for treat-ment of a left pneumothorax. In June, 1962 thepatient consented to a left interscapulothoracicamputation because extensive disease had madethat extremity completely useless. At that time theabdomen was noted to be normal. On July 10, 2½1weeks after discharge, he was readmitted for skingrafting to the left shoulder area where the skinflaps had separated. At this time he was firstnoted to have a round cauliflower-like lesion 2 cm.in diameter in the healed donor graft site of theabdomen (Fig. 6A). This was excised and re-ported as a poorly differentiated sarcoma (Fig.6B, C)-possibly angiosarcoma.
The patient's final admission for terminal carefollowed a few weeks later. He expired on August31, 1962 with widespread metastases.
Comment. Local recurrences of the im-plantation type have been reported in thedonor site, although recurrences in thegraft site are perhaps more common. Inthis case the recurrence was not apparent
DISSEMINATION OF CANCER
until nearly 10 months after the graft; thepatient was seen and examined 9 monthsafter the skin graft at which time therewas no evidence of a recurrence. Sincethere was visible tumor in one or two areas
in the axillary region when the skin graftwas performed there was obviously ampleopportunity for sarcoma cells to contami-nate the surgeons gloves and be implantedinto the donor site. There is, of course, thepossibility that sarcoma cells were circulat-ing in the blood stream and that some ofthem lodged in the traumatized area atthe donor site. However, as stated previ-ously, some experiments performed in our
own laboratory by Vernix and Garside39showed that when the cells were injectedintravenously, not a single implant was
found later in the scar of the incisions, al-though when 1,000,000 V2 cells were in-jected into the aorta of nine rabbits at thetime the incisions were made, a metastasiswas found in four of the 24 incisions.
Irrigation of Wounds withChemical Agents
Cancer Cells in the Wounds of PatientsHaving Operation for Cancer. Smith andassociates 36 were among the first to reportthe discovery of cancer cells in an opera-tive wound. They found cancer cells in 26per cent of 120 wounds and suspicious cellsin an additional 14 per cent. The local re-
currence rate for the patients having cellsin the wound washings was 40 per centcompared to the recurrence rate of 26 percent in patients having negative washings.However when these authors studied thesecases later, they found no relationship ofsurvival of the patients to the presence or
absence of cells in the wound washings.In a recent study, Smith et al.,36 con-
cluded that irrigation with 0.5 per centformaldehyde was effective. For example,21 of 54 patients irrigated with saline de-veloped a recurrence, whereas only 4 of 26patients having their wounds irrigated withformaldehyde developed a recurrence. The
group having their wounds irrigated withformaldehyde also showed a small but con-
sistently greater survival rate.Laboratory Experiments on the Effect
of Various Anticancer Agents in Wounds.Numerous authors have attempted to findchemicals which would destroy cancer cellswhen used to irrigate wounds made for theexcision of cancer. Our own group hastested an enormous number of compounds.Some of those which we thought might beeffective turned out to be ineffective. Theineffective group included phenol, oxytetra-cycline, cholroazodin (Azochloramide) andbenzalkonium (Zephiran chloride). Iodineitself is fairly effective. Clorpactin XCB was
not effective when used in 0.5 per cent solu-tion, which represents a concentration con-
sidered safe by us for human beings. Wefound 0.4 per cent formaldehyde to be rea-
sonably effective but that sodium hypo-chlorite and nitrogen mustard were more
effective. A chlorine compound known as
ACL 60 (sodium dichloroisocyanurate) isalso effective. It has considerable advantageover sodium hypochlorite because it is quitestable; sodium hypochlorite is relativelyunstable and must be buffered with sodiumbicarbonate to a pH of 9.0. In some addi-tional experiments we noted that quinacrine(Atabrine), proflavine hemisulfate, chlor-amine-T, and iodoform were likewise ef-fective.These experiments were performed with
subcutaneous wounds, irrigating thewounds one hour after the cancer cells hadbeen implanted. Knowing that the effect ofthe chemical agents might be different inthe peritoneal cavity because of a differencein the invasive quality and other possiblefactors, we conducted some experimentsinoculating cancer cells in the peritonealcavity and irrigating the cavity one hourlater with various chemicals. We were sur-
prised to find that the use of the chlorinecompounds (ACL 60 and sodium hypo-chlorite) in the peritoneal cavity actuallyincreased the percentage take of the tumor
Volume 161Number 5 765
766 COLE AND OTHERS
cells.25 However thioTEPA and A-8103 usedin the peritoneal cavity were quite effectivein sharply reducing the take of tumor cells.Vernick and associates,40 working in ourlaboratory, noted that when 3 ml. of ir-rigant fluid were instilled in the peritonealcavity one hour after inoculation of cellsthe number of animals developing tumorswas 81.1 per cent in the untreated and 82.4in those receiving physiologic saline. Incontrast the number of animals developingtumors following instillation of A-8103 was2.7, and following thioTEPA it was 3.1 percent. These authors also noted that the in-stillation of chemicals into the peritonealcavity was more effective than irrigation.For example in the animals having theirperitoneal cavity irrigated for 2 min. withthioTEPA the per cent take was 43.4; inanimals having irrigation for 4 min. it was43.4; in animals irrigated for 8 min. itwas 63.3. On the contrary, when an equalamount of thioTEPA was injected into theperitoneal cavity the per cent take was re-duced to 8.0.
Results of these experiments-revealing ahigher per cent "take" in animals inocu-lated with cancer cells in the peritonealcavity, followed by irrigation or instillationof anticancer compounds, than in controlanimals-have been very disturbing. Sincethese findings were unexpected, the experi-ments were repeated several times andunder different circumstances. Howeverwith one or two exceptions, the experimentalways resulted in the same ratio of tumordevelopment, namely about twice as manyin the treated animals as in the controls.Accordingly, if we can draw a conclusionfor human patients from animal data, cer-tain systemically acting drugs like thio-TEPA or A-8103, rather than locally actingdrugs such as ACL 60 or sodium hypo-chlorite, should be used for irrigating theperitoneal cavity to destroy cancer cells.
Annals of SurgeryMay 1965
SummaryOf the four major mechanisms for the
spread of cancer we have been concernedwith vascular spread and implantation. Re-gardless of the frequency with which can-cer cells may be found in the blood streamthe fact remains that in most cancers, par-ticularly those involving the gastrointestinaltract, the vascular spread of the tumor isthe mechanism which kills the patient.
Implantation of cells is a common mecha-nism for the spread of tumor. It may bespontaneous or iatrogenic. We can do littleto prevent the former, except to minimizedelay prior to operating. latrogenic spreadcan and should be prevented, but preven-tion requires more than the usual routineprecautions. Although all possible precau-tions have been utilized, we still encounterinstances of iatrogenic implantation, severalof which are reported.Numerous workers in our department
have conducted animal experiments to findsatisfactory anticancer compounds whichcould be utilized as irrigants to destroyimplanted cancer cells. We found thatsodium hypochlorite (Dakins solution) andnitrogen mustard were quite effective inexperiments with rats. In studies of addi-tional agents and their effects, we notedthat halogenated compounds such as so-dium hypochlorite, sodium dichloro-isocy-anurate (ACL 60) and certain iodophorcompounds actually increase (rather thandecrease) the survival and growth of can-cer cells in the peritoneal cavity, whereasthey were effective in destroying cancercells implanted in subcutaneous wounds.ThioTEPA and a piperazine compound (A-8103) were effective in destroying cancercells in the peritoneal cavity as well assubcutaneous tissue. It appears that thesecompounds might be acceptable for use inthe peritoneal cavity when contaminationwith cancer cells is significant. We haveused sodium hypochlorite as an irrigant inwounds following radical neck dissection
Volume 161 DISSEMINATION OF CANCER 767Number 5
and radical mastectomy for the past 2 to 3years. Inadequate time has elapsed to ar-rive at any conclusion, but preliminary datafrom our series has been disappointing.
References
1. Ackerman, L. V. and M. W. Wheat, Jr.: TheImplantation of Cancer-An Avoidable Sur-gical Risk? Surgery, 37:341, 1955.
2. Alexander, J. W. and W. A. Altemeier: Sus-ceptibility of Injured Tissues to Hematoge-nous Metastases. Ann. Surg., 159:933, 1964.
3. Allen, J. Garrot and S. P. Rigler: End Resultsfrom Radical Mastectomy. Surg. Clin. N.Amer., 42:1467, 1962.
4. Arons, M. S. and R. R. Smith: Distant Metas-tases and Local Recurrence in Head andNeck Cancer. Ann. Surg., 154:235, 1961.
5. Beahrs, 0. H., K. Devine and S. W. Henson:Treatment of Carcinoma of the Tongue:End Results of 168 Cases. Arch. Surg., 79:399, 1959.
6. Beahrs, 0. H., J. W. Phillips and M. B.Dockerty: Implantation of Tumor Cells as aFactor in Recurrence of Carcinoma of theRectosigmoid. Cancer, 8:831, 1953.
7. Beahrs, 0. H. and K. W. Barber: The Valueof a Radical Dissection of Structures of theNeck in the Management of Carcinoma ofthe Lip, Mouth and Larynx. Arch. Surg., 85:49, 1962.
8. Brown, C. E. and S. Warren: Visceral Metas-tases from Rectal Carcinoma. Surg. Gynec.& Obstet., 66:611, 1938.
9. Cade, S. and E. S. Lee: Cancer of the Tongue.Brit. J. Surg., 44:28, 1957.
10. Cliffton, G. G. and D. Agosturo: Factors Af-fecting Development of Metastatic Cancer:Effect of Alteration in Clotting Mechanisms.Cancer, 15:276, 1962.
11. Collier, F. C., W. S. Blakemore, R. H. Kyle,H. T. Enterline, C. K. Kirby and J. Johnson:Carcinoma of the Lung: Factors which In-fluence Five-Year Survival With Special Ref-erence to Blood Vessel Invasion. Ann. Surg.,146:417, 1957.
12. Coman, D. R.: Mechanism Responsible for theOrigin and Distribution of Blood-Borne Tu-mor Metastases: A Review. Cancer Res., 13:397, 1953.
13. Engell, H. C.: Cancer Cells in the CirculatingBlood: Clinical Study of Occurrence of Can-cer Cells in Peripheral Blood and in VenousBlood Draining Tumor Area at Operation.Acta Chir. Scand., (Supp.), 201:1, 1955.
14. Fisher, B. and S. R. Fisher: ExperimentalStudies of Factors Influencing Hepatic Meta-static III Effect of Surgical Trauma WithSpecial Reference to Liver Injury. Ann.Surg., 150:731, 1959.
15. Frazell, E. L. and J. C. Lucas: Cancer of theTongue: Report of the Management of 1554Patients. Cancer, 15:1085, 1962.
16. Grinnell, R. S.: Spread of Carcinoma of theColon and Rectum. Cancer, 3:641, 1950.
17. Haagensen, C. D.: Diseases of the Breast,Philadelphia, W. B. Saunders Co., 1957.
18. Harrold, G. C.: Present Day Methods of Sur-gical Treatment of Intraoral Cancer in Pro-ceedings of the Second National Cancer Con-ference, American Cancer Society, 1952. p.444.
19. Hengesh, J. W., E. H. MlcGrew and S. Nanos:Malignant Cells in the Peripheral Blood ofExperimental Animals. Acta Cytol., 6:143,1962.
20. Hoopes, B. F. and A. B. MIcGraw: The HalstedRadical Mastectomy. Surgery, 12:892, 1942.
21. Hoye, R. C., K. M. Herrold, R. R. Small andL. B. Thomas: A Clinicopathological Studyof Epidermoid Carcinoma of the Head andNeck. Cancer, 15:741, 1962.
22. Lucke, B., C. Breedis, Z. P. Woo, L. Berwickand P. Nowell: Differential Growth of Meta-static Tumors in Liver and Lung. Experi-ments with Rabbit V2 Carcinoma. CancerRes., 12:734, 1952.
23. Madden, R. E. and B. A. Malmgren: Quantita-tive Studies on Circulating Cancer Cells inMouse. Cancer Res., 22:62, 1962.
24. Martin, H., B. Del Valle, H. Ehrlich and XV.G. Cahan: Neck Dissection. Cancer, 4:441,1958.
25. McKibbin, B. and J. C. Gazet: ExperimentalUse of Anti-Cancer Agents in the PeritonealCavity. Brit. J. Surg., 51:693, 1964.
26. Moore, G. E., T. Kondo and R. J. Oliver: Ef-fect of Cortisone in Tumor Transplantation.J. Nat. Cancer Inst., 25:1097, 1960.
27. Morfit, H. H.: End Results in the Combined(Commando) Operation for Mouth Cancer.Surg. Gynec. & Obstet., 108:129, 1959.
28. Pool, E. H. and G. R. Dunlop: Cancer Cellsin Blood Stream. Amer. J. Cancer, 21:99,1934.
29. Prinzmetal, M., E. M. Ornitz, B. Semkin andH. C. Bergman: Arterio-venous Anastomosesin Liver, Spleen and Lungs. Amer. J. Physiol.,152:48, 1948.
30. Roberts, S., A. Watne, R. McGrath, E. Mc-Grew and W. H. Cole: Technique and Re-sults of Isolation of Cancer Cells from theCirculating Blood. Arch. Surg., 75:334, 1958.
30a. Cole, W. H., G. 0. McDonald, S. S. Robertsand H. W. Southwick: Dissemination ofCancer. New York, Appleton-Century-Crofts,Inc., 1961.
31. Robinson, K. P. and E. Hoppe: The Develop-ment of Blood Borne Metastases. Arch.Surg., 85:720, 1962.
32. Robnett, H. H., T. E. Jones and J. B. Hazard:Carcinoma of the Breast. Cancer, 3:757,1950.
33. Romsdahl, M.: Influence of Surgical Proce-dures in Development of Spontaneous LungMetastases. Surg. Res., 4:363, 1964.
34. Romsdahl, M. M., J. Valaitis, R. G. McGrathand E. A. McGrew: Cytological Changes inMegakaryocytes in Patients with Carcinoma,Acta Cytol., 8:343, 1964.
35. Shore, B. R.: Carcinoma of the Breast. Ann.Surg., 116:801, 1942.
36. Smith, R. R. and R. A. Malmgren: Cancer CellWound Seeding in Surgery: A Review. Can-cer, 14:10, 1964; Harris, H. H. and R. R.Smith: Operative Wound Seeding with Tu-mor Cells. Its Role in Recurrence of Headand Neck Cancer. Ann. Surg., 151:330,1960.
768 COLE AND OTHERS Annals of Surgery
37. Sunderland, D. A.: The Significance of VeinInvasion by Cancer of the Rectum and Sig-moid: A Microscopic Study of 210 Cases.Cancer, 2:429, 1949.
38. Taylor, G. W. and R. H. Wallace: Carcinomaof the Breast. New Engl. J. Med., 237:475,1947.
39. Vemick, J., G. Garside and E. Hoppe: TheLack of Growth of Intravenously InoculatedTumor Cells in Peripheral Wounds. CancerRes., 24:1507, 1964.
40. Vernick, J. J., J. Magell and E. T. Hoppe:Alkylating Agents and Iodophor Compoundsfor the Prevention of Local Recurrence ofCancer, Surg. Forum, 15:336, 1964.
41. Warren, S. and 0. Gates: The Fate of Intra-
venously Injected Tumor Cells. Amer. J.Cancer, 27:485, 1936.
42. White, W. C.: Problems of Local RecurrenceAfter Radical Mastectomy for Carcinoma.Surgery, 19:149, 1946.
43. Wilkins, S. A. and W. R. Vogler: Cancer ofthe Gingiva. Surg. Gynec. & Obstet., 105:145, 1959.
44. Wood, S.: Pathogenesis of Metastasis Forma-tion Observed in The Rabbit Ear Chamber.Arch. Path., 66:550, 1958.
45. Willis, R. A.: The Pathology of Tumors, 3rded. London, Butterworth & Co., 1960.
46. Zeidman, I., M. McCutcheon and D. R.Coman: Factors Affecting the Number ofTumor Metastases. Cancer Res., 10:357,1950.
DISCUSSIONDR. BENJAMIN F. BYRD, JR. (Nashville): Dr.
Cole let me see his complete manuscript on thisfascinating continuation of his work on iatrogeniccarcinoma. I think the clinical application of thiscontinued interest of his is something for whichwe are all indebted to Dr. Cole. Certainly the useof irrigating agents for the topical effect of thedrug has been beautifully demonstrated in thiswork which he has shown us here this morning.Of course, it is especially interesting that every-thing that kills cancer cells in the test tube doesnot necessarily kill it in the abdominal cavity, thisfact being shown with the diminished effectiveness,the actual deleterious effects of the halogenatedagents as an irrigating solution as over against thesystematically effective Thiotepa.
I cannot help but believe that the work whichDr. Cole is doing will eventually bring us to areally fruitful solution to the management of meta-static cancer. We are right now beginning to seefollow-up periods on our basic experimental workwhich carries for us individually something thatwe can use in the management of our cancer pa-tients. We all stand to gain from experimentalstudy whenever we are having local recurrencesin cancer of the breast which may be affectedfavorably by the use of systemic cancerocidaldrugs, and whenever we are having 25 to 30%local recurrences in cancers of the head and neckafter radical neck dissections, which we can alterfavorably by the use of one of these drugs.
I would like to speak again for one moment con-ceming Dr. Ochsner's paper. He mentioned in hispresentation one of the possible uses of mammog-raphy. I certainly did not get up here to tell abunch of surgeons that mammograms are satis-factory substitutes for microscopic examination, butI do want to show two instances in which pre-operative mammograms might have favorablyaltered the patients' course.
(Slide) This is a mammogram and here is atumor lying deep within the breast. This patient
was very generously equipped with breast tissueand had in her axilla a mass which was removed.There was no palpable breast mass. The axillarymass was removed, proved to be adenocarcinoma,and then mammograms were done and the tumorfound lying deep within the breast tissue. Thebreast was removed with radical mastectomy in asecond procedure.
(Slide) This patient was an older woman in hersixties, who had an axillary mass, again with nopalpable breast abnormality. This section, on mi-croscopic examination, was diagnosed as malignantmelanoma by the pathologist and by surgicalpathologist as possibly carcinoma but probably amelanotic metastasis. We got a mammogram thefollowing day (slide) which showed this tumorright here, which was not palpable. We took herback to the operating room, did a radical mastec-tomy. She had a carcinoma of the breast, and this,I think, really demonstrates one of the principaluses of mammography, in the evaluation of axillarymasses where there is no palpable abnormality inthe breast itself.We can get something from this and probably
the wealth of material which is being built up bythe radiologists serves to increase their diagnosticacumen.
DR. WALTER J. BURDETTE (Salt Lake City):I would like to discuss Dr. Ochsner's paper. Wehave been interested in the possible usefulness ofmammography at the University of Utah for severalyears as well; and Drs. William Christiansen andCarlisle Smith of the Department of Radiologyhave become very expert at reading mammograms.A few illustrations from the 90 cases having mam-mography and excision of the lesion with histologicstudy may be of interest to the group.
(Slide) This is an example of normal breast, this(slide) of a breast during lactation, and this(slide) is an example of gynecomastia, a lesionwhich is puzzling at times. This roentgen study(slide) shows chronic cystic disease in this area,