Embed Size (px)
Citation preview

fbm
oUect
Curren
tConcep
ts
CURRENTCONCEPTS
Distal Radius Fractures: Current Concepts
Johannes Schneppendahl, MD, JoachimWindolf, MD, Robert A. Kaufmann, MD
Despite the frequency of distal radius fractures, the optimal treatment remains withoutconsensus opinion. A trend toward increased distal radius fracture open reduction andinternal fixation has been identified, with biomechanical and clinical studies suggestingtreatment advantages of certain fixation methods over others. Well-controlled patient trialsare still missing to lend objective findings to management algorithms. This article reviewsthe literature over the past 5 years to guide our management regarding this commonupper-extremity injury. (J Hand Surg 2012;37A:1718–1725. Copyright © 2012 by theAmerican Society for Surgery of the Hand. All rights reserved.)
Key words Distal, radius, fracture, surgical, fixation.
tamqspmdtmeo$
TREATMENT OVERVIEWThe goal of distal radius fracture treatment is to restorean upper extremity that has both acceptable mobilityand durability. Although these fractures are commonand often reviewed, there remains little evidence insupport of different treatment options. A recent Co-chrane Review1 revealed insufficient literature supportor any one method of surgical fixation; an evidence-ased clinical practice guideline was unable to recom-end one form of treatment over another.2
Despite a lack of consensus, a rise in internal fixationf distal radius fractures has been observed within thenited States. Europe is witnessing a similar trend, as
videnced in a nationwide registry review of all surgi-ally treated distal radius fractures in Finland from 1998o 2008.3 In a country that has universal public health
coverage ensuring insurance-unbiased findings, a dou-bling incidence of surgical treatment for distal radiusfractures and a more than 13-fold increase in the inci-
From the Department of Orthopaedic Surgery, University of Pittsburgh Medical Center, Pittsburgh, PA;and the Department of Trauma and Hand Surgery, University Hospital Duesseldorf, Duesseldorf,Germany.
Received for publication February 23, 2012; accepted in revised form June 3, 2012.
No benefits in any form have been received or will be received related directly or indirectly to thesubject of this article.
Corresponding author: Robert A. Kaufmann, MD, Department of Orthopaedic Surgery, Univer-sity of Pittsburgh Medical Center, Kaufmann Medical Building, 3471 Fifth Avenue, Suite 911, Pitts-burgh, PA 15213; e-mail: [email protected].
0363-5023/12/37A08-0039$36.00/0
http://dx.doi.org/10.1016/j.jhsa.2012.06.0011718 � © ASSH � Published by Elsevier, Inc. All rights reserved.
dence of open reduction and plate fixation were ob-served. The causes of this global increase may be re-lated to greater need or perhaps improved surgicaltraining. Patients treated by members of the AmericanSociety for Surgery of the Hand received internal fix-ation substantially more often than patients treated bysurgeons who were not members (33% vs 16%; P �.001). Factors such as number of years in practice,practice type, and the particular type of training re-ceived contributed most heavily to whether the fracturereceived internal fixation.4
As the incidence of surgical treatment has increased,he cost of different methods has been explored. Toccomplish this, health care intervention cost analysisay be employed that determines a treatment’s cost per
uality-adjusted life-year (QALY) and compares it withocietal norms. The current, widely accepted cost limiter QALY is $50,000, a figure derived from the incre-ental cost-utility ratio of renal transplantation over
ialysis for end-stage renal failure. In patients olderhan age 65, utility values derived from a decision treeodel determined that although casting is the least
xpensive, internal fixation adds an incremental cost ofnly $15,330 per QALY, far less than the limit of50,000, rendering it cost effective for these fractures.5
IMAGINGPlain radiographs remain the mainstay in diagnostics ofdistal radius fractures. The posteroanterior (PA) view
obtained in neutral variance as well as a lateral view
rg/CM
DISTAL RADIUS FRACTURES 1719
CurrentConcepts
with a beam that is inclined 20° will assess ulnar vari-ance and effectively visualize the articular surface. A45° pronated oblique view is helpful in that it profilesthe dorsal ulnar cortex and lends insight into this bio-mechanically important region. At times, improvedfracture visualization through computed tomographyscanning is valuable. This is particularly importantwhen nonoperative treatmentis being considered and itmust be ensured that accept-able articular alignment ispresent. Computed tomogra-phy has demonstrated theability to better characterizewhat radiographically mayappear as an extra-articularinjury. A high percentage ofdistal radius fractures, classi-fied as extra-articular bystandard radiographs, are re-vealed as intra-articular inju-ries. Axial views are helpfulin visualizing the distal ra-dioulnar joint (DRUJ) andcan identify subluxation orfrank dislocation in additionto bony fragments suggestive of radioulnar ligamentavulsions. Magnetic resonance imaging is reserved forcases in which the mere existence of a fracture is calledinto question, and also to help identify concomitant softtissue pathology.
CLASSIFICATIONA multitude of classification systems exist, and a recentevaluation of 5 common systems (Fernandez, AO,Frykman, Melone, and Universal Classification Sys-tems) concluded that all exhibited high interobserverand intra-observer unreliability. A more user-friendlyand reliable method incorporating a 3-dimensional as-sessment was advocated.6 The Melone Classification isclinically useful in that it often influences the operativeapproach. It emphasizes the importance of the radiolu-nate articulation and categorizes fractures into 5 groupsbased on the parts involved: shaft, styloid, dorsal medialfacet, volar medial facet, and severely comminutedfractures. The AO Classification divides intra-articularinvolvement into 3 broad groups that can be subdividedinto 27 distinct fracture patterns. Type A describes anextra-articular fracture, type B involves a partial disrup-tion of the articular surface, and type C represents acomplete separation of multiple articular fragments
EDUCATIONAL OBJEC● State the trend with regard to th
tures.
● Discuss the cost per quality-adjument.
● List the cumulative risk factors ffracture.
● Describe the AO Classification of
● List the advantages and disadvaradius fracture pain.
● Summarize the differences betwpercutaneous pinning versus opplate/screw construct.
Earn up to 2 hours of CME creditarticles and take the online test. Ttest, visit http://www.jhandsurg.o
from the shaft.
JHS �Vol A, A
CLOSED REDUCTION AND IMMOBILIZATIONClosed reduction and immobilization in a plaster castremains an accepted method of treatment for most sta-ble distal radius fractures. A stable fracture is one that isacceptably aligned after reduction effort and where thelikelihood of displacement is small. Cumulative risk
factors for the loss of reduc-tion have been identified asage over 60, greater than 20°dorsal angulation, 5 mm ra-dial shortening, dorsal com-minution, ulna fracture, andintra-articular radiocarpal in-volvement.7 In elderly pa-tients, decreased bone min-eral density may cause distalradius fracture instability, re-sulting in a 30% to 50% riskfor secondary displacementafter closed reduction andsplinting, with redisplace-ment severity correlated withincreasing age.7 If closedtreatment is considered ap-propriate, a splint is usuallyused for the first few days to
accommodate for appropriate swelling. A cast or re-movable splint is worn thereafter. Radiographs obtainedat initial presentation and then at weekly intervals forthe first 3 weeks and at 6 weeks status posttrauma willmonitor fracture alignment.
If the decision for operative intervention is made, amultitude of stabilization options exist. Factors thatmust be considered include the biomechanical charac-teristics of each fixation method, the procedure’s asso-ciated difficulty, and the soft tissue morbidity.
CLOSED REDUCTION AND PINNINGClosed reduction and percutaneous pin fixation are bestsuited for fractures without articular involvement andalso without substantial metaphyseal comminution. Avariety of pinning methods have been described; themost popular is oblique radial styloid to proximal ulnarcortex, as well as placement of the pins through thefracture site. Wires are usually removed 4 weeks afterplacement to minimize the risk of infection. The deci-sion to use percutaneous pin fixation should be consid-ered with care, because a prospective, randomized trialencountered markedly inferior clinical and radiologicalresults for percutaneous pinning compared with lockedvolar plating, even for extra-articular distal radius frac-
ES
ical treatment of distal radius frac-
fe year method of assessing treat-
loss of reduction in a distal radius
radius fractures.
s of dorsal plate fixation for distal
ternal fixation in combination withction and internal fixation using a
S issue when you read the relatedthe $20 fee and take this month’sE/home.
TIV
e surg
sted li
or the
distal
ntage
een exen redu
per JHo pay
tures.8 A new fixation technique that uses threaded
ugust

A pre
1720 DISTAL RADIUS FRACTURES
Curren
tConcep
ts
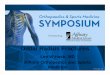
variable-length cannulated pins (T-Pin; Union Surgical,Philadelphia, PA) may improve bony purchase andyield superior clinical results compared with smoothpins (Fig. 1).
EXTERNAL FIXATIONBridging external fracture fixation refers to a surgicaleffort that bridges the radius fracture and gains purchasedistal to the radiocarpal joint. It employs ligamentotaxisto improve the length and alignment of the fracture.Intra-articular displacement may be corrected throughthe placement of percutaneous pins. A prospective,randomized trial compared external fixation in combi-nation with percutaneous pinning to open reduction andinternal fixation (ORIF) using a volar or dorsal plate.There was significantly less pain and disability in theORIF group at early follow-up, with the differencesdiminishing over time. There were no significant dif-ferences in the Disabilities of the Arm, Shoulder, andHand score, and only a trend for better wrist extension,supination, and grip strength in the ORIF group at 3months. There were no significant differences betweeninitial postoperative alignment, except for a slightlygreater restoration of volar tilt in the ORIF group. Theincidence of complications was similar in both groups,although greater tendon complications were seen withinternal fixation and more infections were identified
FIGURE 1: Radiographs of a distal radius fracture
with external fixation.9 These findings are consistent
JHS �Vol A, A
with what other studies have shown. Pin track infectioncoupled with unsightly scars and superficial radialnerve traction that may lead to complex regional painsyndrome contribute to a trend away from its use.
Nonbridging external fixation uses pins in the distalradial fragment and pins proximal to the fracture with-out bridging the radiocarpal joint. In this instance, frag-ments are reduced by direct manipulation. The non-bridging method requires a sizeable extra-articulardistal fracture fragment, yet offers less risk of radialshortening and dorsal angulation compared with bridg-ing external fixation.10
INDIVIDUAL FRAGMENT FIXATIONFracture fragment-specific fixation uses a series of low-profile plates and clips to individually supply rigid,low-profile fixation to fracture fragments. Restorationof radial column integrity is followed by fixation effortsto address additional displaced fragments. The fracturefragment specific plates are sufficiently low-profile soas to allow implant placement to match the individualfracture pattern. The fracture fixation usually beginswith a radial-sided incision through which the radialand volar plates can be applied. Dorsal and sometimesvolar incisions are also required. A prospective cohortstudy reviewed radiograph and clinical outcomes tocompare volar plating with fragment-specific fixation
operatively and B after fixation with threaded pins.
methods. Whereas the radiographic parameters were
ugust

DISTAL RADIUS FRACTURES 1721
CurrentConcepts
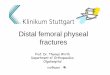
superior with volar locked plating and the complicationrate was higher with fragment-specific fixation, no sig-nificant clinical difference was seen.11 Understandinghow to employ fracture fragment-specific fixationmethods requires considerable expertise and experi-ence, yet proves invaluable when the surgeon is occa-sionally faced with a comminuted fracture for which noother method will suffice (Fig. 2).
DORSAL PLATESRadius fractures with metaphyseal comminution typi-cally collapse in a dorsal direction and a dorsal ap-proach will provide excellent articular surface visual-ization and allow for buttressing of these fragments.Disadvantages are that the plate is placed under theextensor tendons, which may lead to extensor tendonirritation and rupture. Late-generation, low-profileplates that are designed to not cause tendon irritationtackle this major source of complications. Distal frag-
FIGURE 2: A Coronal, B sagittal, and C axial computed tomogE lateral radiographs after fragment-specific fixation.
ments may become devitalized once exposed ade-
JHS �Vol A, A
quately, and achieving adequate purchase is anotherdrawback given that the native volar tilt of 10° maypreclude distal enough placement of the plate in afixed-angle device. Dorsal plates that allow variable-angle screw fixation would not have this problem. Aretrospective study on complications of low-profile dor-sal and volar locked plating did not identify majordifferences in tendon irritation or rupture for either ofthe techniques, and found a higher rate of neuropathiccomplications with the volar approach.12 The use ofdorsal plates may increase if the concern about tendonirritation that plagued previous design generationsproves to be less frequent with newer implants.
VOLAR FIXED-ANGLE PLATESThe volar plate is an evolution of the blade plate as ittransfers forces from the subchondral bone away fromthe dorsal metaphysis and toward the volar cortex. Alongitudinal volar scar and the creation of a rigid bio-
y views of a comminuted distal radius fracture, and D PA and
raphmechanical construct that offers the possibility of near-
ugust

1722 DISTAL RADIUS FRACTURES
Curren
tConcep
ts
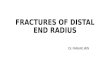
immediate functional wrist loading are considered ben-efits. Depending on the plate design, distal screws canlock at a predetermined angle, facilitating the lift-offtechnique, or can be placed at variable angles relative tothe plate. The lift-off method places the distal screwsfirst and then uses the plate to correct the dorsal mal-alignment of the fracture (Fig. 3). A more traditionalapproach involves proximal plate fixation before thefracture is reduced, and the distal screws are subse-quently placed to maintain the reduction effort. Havingscrews that can be positioned at a variable angle isadvantageous for the latter method. Regardless of tech-nique, the distal screws or pegs are placed immediatelysubchondral, which a 45° pronated oblique view canhelp visualize. Volar fixation leverages the intact exten-sor compartment structural framework that contains andeven reduces dorsal fracture comminution. However,dorsal cortical penetration of the screws may lead toextensor tendon rupture. Because lateral and obliqueradiographic views have a relatively low sensitivity fordetecting dorsal cortical penetration, a study evaluatedthe sensitivity, specificity, and accuracy of the skylineview in detecting penetration by 1 mm compared withstandard radiographs. The skyline view was the most sen-sitive and accurate for detection of dorsal cortical penetra-tion. The sensitivity, specificity, and accuracy of this viewwere all 83%. The pronated oblique and lateral views wereless accurate, registering 77% and 51%, respectively.13
A volar plate has the potential to be subsequently cov-ered by repairing the pronator quadratus, which may re-duce the likelihood of tendon interference. The flexorpollicis longus tendon can be at risk for irritation andpotential rupture, however, and a cadaver model evaluatedthe influence of distal radius plate position on contactpressure between it and the distal edge of the locking plate.Contact pressure considerably increased when the distalplate edge was placed distal to the watershed line.14
The question of whether using pegs or screws results inimportant biomechanical differences has been addressedin a cadaveric study. Although there were no statistically
FIGURE 3: The lift-off technique employs distal fixation intoand B proximal plate fixation.
significant differences in torsional or axial stiffness at the
JHS �Vol A, A
beginning of loading, after 1,000 cycles, pegs failed byloosening, most often at the peg–plate interface. Screwfixation provided a more stable construct.15
Volar plate fixation appears to be used with fewercomplications compared with external fixation. A total of115 patients were reviewed with comminuted intrarticulardistal radius fractures. Of those patients, 59 were treatedwith bridging external fixation, and 56 with volar lockingplate fixation. Volar plate fixation had an overall decreasedincidence of complications and significantly better motioncompared with external fixation. Volar plate fixation alsoresulted in less radial shortening than the external fixationgroup, as well as less pain, improved functional outcomes,and grip strength.16
INTRAMEDULLARY-BASED DEVICESIntramedullary radius fracture fixation using subchon-dral screws that lock to a stem has the theoreticaladvantages of less surgical dissection and decreasedtendon irritation. As one of the available devices, theMicronail (Wright Medical Technology, Inc., Arling-ton, TN) is inserted through a radial styloid portal andcontains 3 fixed-angle distal locking screws and 2 self-tapping, bicortical screws for proximal fixation throughan attached outrigger guide. Use of the implant, indi-cated for extra-articular or simple intra-articular frac-tures, was reported in 29 consecutive patients whosefunctional and radiographic outcomes at 12 monthsdemonstrated 9 good and 20 excellent functional re-sults, according to the Mayo wrist score, with almostcompletely restored range of motion and grip strength.Loss of reduction was seen in 2 patients.17 Althoughclinical reports presenting encouraging results areemerging, larger studies with long-term follow-up arenecessary to support its use.
ARTHROSCOPYMost likely because of its logistical and technical de-mands, arthroscopic assistance during reduction of in-tra-articular radius fractures has not gained widespread
orsally unstable fracture fragment A before fracture reduction
the dacceptance. A stepwise algorithm for dry wrist arthros-
ugust

DISTAL RADIUS FRACTURES 1723
CurrentConcepts
copy presented technical tips on how to handle airflow,suction, and surgical technique. Salient features in-cluded initial fixation of the plate with proximal screws;then, the radius fracture is visualized through a 6Rportal, and reduced. Provisional K-wires are employedto maintain the fracture alignment while the fragmentsare reduced arthroscopically. These fragments are thenheld in proper alignment via screws placed iteratively asthe K-wires are replaced.18
A study comparing arthroscopic to fluoroscopic re-duction for the treatment of AO type C fractures with astepoff greater than 2 mm underscored the value ofdirect fracture visualization. After performing reductionand external fixation of the fracture under fluoroscopy,arthroscopy was performed in 1 group, which mandateda revision pinning effort in 45% of patients. Radio-graphically, the mean stepoff was significantly lowerfor the arthroscopy group compared with those who hadfluoroscopy alone. In the near and midterm follow-up,Mayo wrist scores as well as range of motion weresignificantly better for the arthroscopy group than thecontrol group.19
BRIDGE PLATINGHigh-energy comminuted distal radius fractures repre-sent unique treatment challenges. In particular, 1 groupof patients—those with multiple injuries that requireload bearing through the injured wrist to assist withmobilization—may benefit from bridge plating. Thisdevice acts as an internal fixator and depends on liga-mentotaxis for fracture reduction. The technique maybe performed easily, is associated with few complica-tions, and achieves the goals of fracture reduction main-tenance while allowing weightbearing through the in-jured extremity. The latter attribute places it securely inthe armamentarium of a surgeon treating complex up-per-extremity trauma.
SOFT TISSUE INJURIESWhen treating distal radius fractures, a high level ofsuspicion should be maintained for associated soft tis-sue injuries to the intrinsic wrist ligaments. Preoperativediagnostic studies as well as intraoperative instabilityassessment may be valuable. In younger patients, main-taining a high index of suspicion for scapholunate lig-ament injury is imperative. Prompt diagnosis and treat-ment in the acute setting may achieve primary ligamenthealing and avoid a reconstructive or salvage proce-dure.
DRUJ radioulnar joint instability
Distal radioulnar joint instability is commonly associ-
ated with a radius fracture. It was noted as early asJHS �Vol A, A
1814, when Abraham Colles stated, “If the surgeonproceeds to investigate the nature of this injury, he willfind that the end of the ulna admits of being readilymoved backwards and forwards.” This high associationis likely related to the bony architecture of this joint,which accounts for only 20% of stability, and thusplaces the mechanical integrity burden on the soft tissueattachments. The bony contact between the radius andulna is reduced at the extremes of forearm rotation,further reducing bony constraints, thus increasing therisk of DRUJ injury when the forearm is maximallypronated or supinated. The primary stabilizer of theDRUJ is the triangular fibrocartilage complex (TFCC).Additional stabilizers such as the ulnocarpal ligaments,extensor carpi ulnaris subsheath, and interosseousmembrane have a secondary role.
Studies examining the incidence of TFCC injuriesassociated with distal radius fractures have noted anincidence of 45% to 65%. Radial shortening of 5 to 7mm can stretch the dorsal and palmar radioulnar liga-ments and result in ligament tears. Distal radius fractureangulation also affects the biomechanics of the DRUJ.More than 20° dorsal angulation has also been associ-ated with incongruency of the DRUJ in addition toaltered TFCC kinematics, leading to tearing at its pe-ripheral attachments. As the amount of displacementand angulation increases, secondary constraints to jointstability are injured as well, such as the ulnocarpalligaments, extensor carpi ulnaris subsheath, and in-terosseous membrane.
Prereduction radiographic findings may help to in-crease the surgeon’s suspicion for injury to the DRUJ.Additional findings that may herald problems includean ulnar styloid base fracture, widening of the DRUJinterval on PA radiographs, and dislocation of theDRUJ on lateral radiographs. A computed tomographyscan can provide additional insight. Axial views of theDRUJ can be compared with the contralateral side.Subluxation or frank dislocation may often be identi-fied, in addition to bony fragments suggestive of palmaror dorsal radioulnar ligament avulsions.
Once the radius fracture has been reduced and sta-bilized, the DRUJ may be examined under anesthesiaand compared with the contralateral side. The dorsallunate facet may be fractured, from which the dorsallimb of the radioulnar ligament originates. The mostcommon cause for DRUJ instability is via a fracturethrough the base of the ulnar styloid, and requires thedetermination of instability after radius fracture internalfixation through manual testing. When managing thisfracture, greater than 1 cm of dorsal to palmar transla-
tion mandates instability presumption. Distal radioulnarugust

1724 DISTAL RADIUS FRACTURES
Curren
tConcep
ts
joint instability is then addressed through open reductionand internal fixation of the ulna styloid fracture. A litera-ture review suggests not addressing the ulnar styloid frac-ture if the DRUJ is stable after fixation of the radius, andusing either fixation of the ulnar styloid or reduction andsupination splinting if the DRUJ is unstable.20
A prospective cohort study aimed to identify anassociation between DRUJ instability and potential pre-dictors such as age, gender, dominant hand involve-ment, mechanism of injury, fracture pattern, ulnar sty-loid fracture, and fracture displacement. A total of 163adult patients with unstable distal radius fractures weretreated with volar locking plates and then evaluated bymanual intraoperative examination and repair of theTFCC when needed. The authors found 11 completeradioulnar ligament tears at the fovea of the ulnar head.The only noteworthy independent risk factor was anincrease of DRUJ gap distance by 1 mm on PA radio-graph, which increases by 5-fold the risk of radioulnarligament tear in a patient of average wrist width.21
BONE GRAFTINGWhereas grafting with autologous bone or bone substi-tutes has been described for corrective osteotomies ofmalunited distal radius fractures, some studies recom-mend its use in unstable distal radius fractures as well.Various tricalcium phosphate preparations and rapidlyhardening bone cements have been described for thispurpose. This may not be needed unless the fracture hasbeen approached dorsally, which disrupts the stabilityprovided by the retinacular framework of the extensorcompartments. Substantial physiologic or soft tissuecompromises are additional reasons for its use.
A recent literature review concluded that graftingmay improve radiographic alignment or short-term out-come, but no overall influence on final result wasseen.22 These results resemble those of a CochraneReview that considered 10 trials including 874 patients,all of which presented insufficient evidence to drawconclusions regarding functional outcome and safety.
Given the added cost of allografting and the in-creased morbidity of autografting radius fractures, itsuse should be limited to corrective osteotomy cases anddistal radius fractures that are treated between 3 and 6weeks after injury, unless uncommon extenuating cir-cumstances prevail creating a much compromised heal-ing environment.
MEDIAN NERVE DECOMPRESSIONCarpal tunnel syndrome (CTS) after distal radius frac-ture is common and may occur as a result of the
concussive insult at the time of trauma or extrinsicJHS �Vol A, A
nerve compression, the latter of which may occur inboth an acute and delayed manner.
Causes for nerve compression are numerous and in-clude hematoma, tenosynovitis, forces induced by fracturemanipulation during closed reduction efforts, maintenanceof a flexed wrist posture after reduction, surgical trauma,and excessive fracture callus formation. A case-controlseries reported acute CTS to occur frequently inyoung patients sustaining high-energy trauma, butfound fracture translation to be the only significantrisk factor for its development. A 1% translationwas reported to cause an increment of 0.26 in theodds of developing acute CTS.23
The development of delayed median nerve dysfunc-tion was shown to occur in 24 of 282 patients (8.5%)treated with volar plating efforts. Locking plates had ahigher incidence than nonlocking plates (10.2% vs 3%),which was postulated to be the result of their moredistal placement.24
Given that elevated pressure on the median nervemay lead to permanent dysfunction if not surgicallyrelieved, close monitoring of neurologic function, bothin the acute and later stages of care, is imperative.
MANAGEMENT IN THE ELDERLYTo date, there is no consensus regarding the appropriatetreatment for unstable distal radius fractures in elderlypatients, because only minor differences exist betweenfunctional outcomes and activities of daily living aftersurgical and nonsurgical treatment 1 year after injury.25
Although activities will eventually decrease with ad-vancing age, today’s elderly patients are increasinglyremaining more active. In addition, the potential sepa-ration between actual, physiologic, and perceived ageneeds to be considered when managing distal radiusfractures in this age group.
In low-functioning patients living a sedentary life-style, nonoperative management with avoidance of fin-ger stiffness is appropriate given the realization thatoutcomes are good. Nonoperative treatment, even in thepresence of deformity, makes this cost-effective man-agement worthwhile. If nonoperative treatment is cho-sen, cast disease—namely, atrophy and joint stiffness—must be avoided. Fingers in the elderly may be arthriticand are particularly susceptible to detrimental stiffnessif the joints are not ranged shortly after injury.7
Malunion acceptance may not benefit elderly pa-tients who are more active and place greater functionaldemands on the upper extremity. Increased efforts torestore articular alignment and pre-injury radius anat-omy should be considered. Despite a lack of large-
scale, randomized, controlled trials to clearly positionugust

DISTAL RADIUS FRACTURES 1725
volar plating as superior, its use in the elderly is on therise.7
REFERENCES1. Handoll HH, Huntley JS, Madhok R. Different methods of external
fixation for treating distal radial fractures in adults. Cochrane Data-base Syst Rev 2008:CD006522.
2. The treatment of distal radius fractures: guideline and evidence report.Adopted by the American Academy of Orthopaedic Surgeons Board ofDirectors. 2009. Available at: http://www.aaos.org/research/guidelines/drfguideline.pdf. Accessed January, 2012.
3. Mattila VM, Huttunen TT, Sillanpaa P, Niemi S, Pihlajamaki H,Kannus P. Significant change in the surgical treatment of distalradius fractures: a nationwide study between 1998 and 2008 inFinland. J Trauma 2011;71:939–942.
4. Chung KC, Shauver MJ, Yin H. The relationship between ASSHmembership and the treatment of distal radius fracture in the UnitedStates Medicare population. J Hand Surg 2011;36A:1288–1293.
5. Shauver MJ, Clapham PJ, Chung KC. An economic analysis ofoutcomes and complications of treating distal radius fractures in theelderly. J Hand Surg 2011;36A:1912–1918.
6. Kural C, Sungur I, Kaya I, Ugras A, Erturk A, Cetinus E. Evaluationof the reliability of classification systems used for distal radiusfractures. Orthopedics 2010;33:801.
7. Gehrmann SV, Windolf J, Kaufmann RA. Distal radius fracturemanagement in elderly patients: a literature review. J Hand Surg2008;33A:421–429.
8. McFadyen I, Field J, McCann P, Ward J, Nicol S, Curwen C. Shouldunstable extra-articular distal radial fractures be treated with fixed-angle volar-locked plates or percutaneous Kirschner wires? A pro-spective randomised controlled trial. Injury 2010;42:162–166.
9. Grewal R, MacDermid JC, King GJ, Faber KJ. Open reductioninternal fixation versus percutaneous pinning with external fixationof distal radius fractures: a prospective, randomized clinical trial.J Hand Surg 2011;36A:1899–1906.
10. Hayes AJ, Duffy PJ, McQueen MM. Bridging and non-bridging exter-nal fixation in the treatment of unstable fractures of the distal radius: aretrospective study of 588 patients. Acta Orthop 2008;79:540–547.
11. Sammer DM, Fuller DS, Kim HM, Chung KC. A comparative studyof fragment-specific versus volar plate fixation of distal radius frac-
tures. Plast Reconstr Surg 2008;122:1441–1450.JOURNAL CME QUESTIONS
JHS �Vol A, A
Complications of low-profile dorsal versus volar locking plates in the distalradius: a comparative study. J Hand Surg 2011;36A:1135–1141.
13. Riddick AP, Hickey B, White SP. Accuracy of the skyline view fordetecting dorsal cortical penetration during volar distal radius fixa-tion. J Hand Surg 2012;37E:407–411.
14. Tanaka Y, Aoki M, Izumi T, Fujimiya M, Yamashita T, Imai T.Effect of distal radius volar plate position on contact pressure be-tween the flexor pollicis longus tendon and the distal plate edge.J Hand Surg 2011;36A:1790–1797.
15. Mehling I, Klitscher D, Mehling AP, Nowak TE, Sternstein W, RommensPM, et al. Volar fixed-angle plating of distal radius fractures: screws versuspegs—a biomechanical study in a cadaveric model. J Orthop Trauma 2011.doi:10.1097/BOT.0b013e318225ea46.
16. Richard MJ, Wartinbee DA, Riboh J, Miller M, Leversedge FJ, RuchDS. Analysis of the complications of palmar plating versus externalfixation for fractures of the distal radius. J Hand Surg 2011;36A:1614–1620.
17. Nishiwaki M, Tazaki K, Shimizu H, Ilyas AM. Prospective study ofdistal radial fractures treated with an intramedullary nail. J BoneJoint Surg 2011;93A:1436–1441.
18. Del Pinal F. Technical tips for (dry) arthroscopic reduction andinternal fixation of distal radius fractures. J Hand Surg 2011;36A:1694–1705.
19. Varitimidis SE, Basdekis GK, Dailiana ZH, Hantes ME, BargiotasK, Malizos K. Treatment of intra-articular fractures of the distalradius: fluoroscopic or arthroscopic reduction? J Bone Joint Surg2008;90B:778–785.
20. Wysocki RW, Ruch DS. Ulnar styloid fracture with distal radiusfracture. J Hand Surg 2012;37A:568–569.
21. Fujitani R, Omokawa S, Akahane M, Iida A, Ono H, Tanaka Y.Predictors of distal radioulnar joint instability in distal radius frac-tures. J Hand Surg 2011;36A:1919–1925.
22. Tosti R, Ilyas AM. The role of bone grafting in distal radius frac-tures. J Hand Surg 2010;35A:2082–2084.
23. Dyer G, Lozano-Calderon S, Gannon C, Baratz M, Ring D. Predic-tors of acute carpal tunnel syndrome associated with fracture of thedistal radius. J Hand Surg 2008;33A:1309–1313.
24. Ho AW, Ho ST, Koo SC, Wong KH. Hand numbness and carpaltunnel syndrome after volar plating of distal radius fracture. Hand (NY) 2011;6:34–38.
25. Diaz-Garcia RJ, Oda T, Shauver MJ, Chung KC. A systematic
review of outcomes and complications of treating unstable distal12. Yu YR, Makhni MC, Tabrizi S, Rozental TD, Mundanthanam G, Day CS. radius fractures in the elderly. J Hand Surg 2011;36A:824 – 835.
tConcepts
Distal Radius Fractures: Current Concepts
What x-ray view best visualizes the dorsal ulnarcortex of the distal radius?
a. 45° pronated oblique view
b. 45° supinated oblique view
c. Hyperpronated lateral view
d. Hypersupinated lateral view
What risk factor(s) contribute to the cumulativerisk for loss of reduction following a distal radiusfracture?
a. Age � 50
b. Greater than 10° dorsal angulation
c. 3 mm of radial shortening
d. Dorsal comminution
Curren
e. Anteroposterior view e. All of the aboveTo take the online test and receive CME credit, go to http://www.jhandsurg.org/CME/home.
ugust