Embed Size (px)
Citation preview

DM:Practical Point in
Primary Care Setting
Chaicharn Deerochanawong M.D.
Professor of Medicine
Endocrinology Unit, Dept. of Medicine
Rangsit Medical school,
Rajavithi Hospital, Ministry of Public Health

Objectives in the Treatment of
Diabetes Mellitus
• Correct symptoms of hyperglycemia
• Prevent acute complications of
diabetes
• Prevent and delay progression of
chronic complications of diabetes
• Obtain good quality of life

Chronic complications of Diabetes
Retinopathy
Nephropathy
Neuropathy
MICROVASCULAR MACROVASCULAR
Cerebrovascular
disease
CHD
Peripheral
vascular
disease
World Health Organization/International Diabetes Federation, 1999. Diabetes Care 2001; 24 (Suppl 1): S5–20.

Heart Disease
Stroke
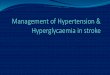
Others
InfectionMalignant
Neoplasms
Diabetes
Thailand Diabetes Registry 2006
Causes of Mortality in PatientsWith Diabetes in Thailand
17%22% 7%14%
20% 20%
J Med Assoc Thai 2010; 93 (Suppl. 3): S12-20

Prevention of Chronic
Vascular Complications in Diabetes
• Holistic approach
• Individualized therapy

Prevention of CVD in Diabetes
Sattar N. Diabetologia 2013;56:686-95

Sattar N. Diabetologia 2013;56:686-95

Prevention and Management of
Diabetic Retinopathy and Nephropathy
• Blood Glucose Control
• BP control
• RAAS blockade
• Other drugs therapy: SGLT2-I,….

0
10
20
30
40
50
60
70
80
G Hb
< 6.5%
Cholesterol <175
mg/dl
Triglycerides <150
mg/dl
Systolic BP <130
mmHg
Diastolic BP <80
mmHg
intensive therapy Conventional therapy
Pa
tien
ts %
P=0.06
P <0.001
P =0.19
P =0.001
P =0.21
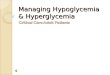
STENO-2: Targeting Multiple CV Risk Factors
in Type 2 Diabetes Improves Outcome
53% reduction in combined
CVD events with intensive
multi-risk factor intervention
Gaede et al. NEJM 2008;358:580–91

Steno-2: 13-year follow-up160 T2DM patients – patterns at 6 years and after
All-cause mortality (%) CV mortality, MI, CVA, CV procedure (%)
8070605040302010
0
8070605040302010
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 1 2 3 4 5 6 7 8 9 10 11 12 13
Cumulative incidence
of death (%)
Cumulative incidence of
any cardiovascular event (%)
Years of follow-upYears of follow-upN at risk
80 78 75 72 65 62 57 39
80 80 77 69 63 51 43 30
N at risk
80 72 65 61 56 50 47 31
80 70 60 46 38 29 25 14
p = 0.02
p < 0.001
Gaede et al. NEJM 2008;358:580–91
Intensive therapy – 2.3% / year
Conventional therapy – 3.8% / year

ABCDES of Diabetes Care2019
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)
C • Cholesterol – LDL < 100 mgl/dL or >30% reduction
D • Drugs to protect the heart
A – ACEi or ARB │ S – Statin │ A – ASA if indicated in very high risk??
E • Exercise / Healthy Eating
S • Smoking cessation
S • Screening for complications
S • Self-management, stress and other barriers

ABCDES of Diabetes Care2019
A • A1C – optimal glycemic control (usually ≤7%)

Impact of Intensive Therapy for Diabetes: Summary of Major Clinical Trials
Study Microvasc CVD Mortality
UKPDS
DCCT / EDIC*
ACCORD ?
ADVANCE
VADT
Long Term Follow-up Initial Trial * in T1DM

Major CV events
Stroke
Myocardial infarction
Favours more
intensive
Favours less
intensive
Meta-analysis of glucose-lowering trials
9% reduction
15% reduction
Turnbull et al. Diabetologia. 2009;52:2288-98.

Possible explanations for the difficulty in
showing that aggressively treating
hyperglycaemia reduces CVD
• No benefits are seen when going below an HbA1c of 7.0%
• The benefits of tight glycaemic control take 5-10 years to
show
• The benefits of lowering blood glucose may be offset by:
– Hypoglycaemia
– Drug side-effects
• Benefits may only be seen in people with relatively early
disease
• Persisting with aggressive therapy in people who don’t
respond may cause harm

Microvascularcomplications
Hypoglycemia
• Newly diagnosed• Long life expectancy
• Young kids• Very elderly• Advanced complications
Benefit and Risk of
Tight Glycemic Control
GOAL A1C < 6.5% or 7%
GOAL A1C 7.5%-9%

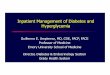
Mechanisms of Hyperglycemia in type 2 diabetes
Adapted from De Fronzo RA. Diabetes 2009;58:773–95.
Hyperglycaemia
Decreasedinsulin
secretion
Increasedglucagonsecretion
Neurotransmitterdysfunction
Decreasedincretin effect
IncreasedHGP
Decreasedglucose uptake
Increasedglucosereabsorption
Increasedlipolysis
Islet-a cell

Adapted from De Fronzo RA. Diabetes 2009;58:773–95.
Hyperglycaemia
Decreasedinsulin
secretion
Increasedglucagonsecretion
Neurotransmitterdysfunction
Decreasedincretin effect
IncreasedHGP
Decreasedglucose uptake
Increasedglucosereabsorption
Increasedlipolysis
Islet-a cell
Insulin,SU,
Glinide
Metformin TZD
TZD
DPP4-I,
GLP1R-A
DPP4-I,
GLP1R-A
SGLT2
inhibitor
GLP1R-A
Therapeutic Implications of Hyperglycemia in type 2 diabetes

THE INFORMATION IN THESE SLIDES IS FOR INTERNAL USE ONLY. NOT TO BE SHARED OR DISTRIBUTED OUTSIDE OF BMS, AMYLIN, OR ASTRAZENECA.
Efficacy Hypo Wt. ASCVD CHF DKD Cost AE
Metfor-min
High No Neutral (loss)
Potential benefit
Neutral Neutral Low GI, potential B12 def
SGLT2i Intermediate
No Loss Benefit (secondaryprevention)
Benefit Benefit High GU inf, DKA,vol dep, amputation, fracture
GLP1-RA
High No Loss Benefit (secondary
prevention)
Neutral Benefit High GI, risk of C cell tumor,pancreatitis?
DPP4i Intermediate
No Neutral Neutral Potentialrisk???? : Saxa, Alo
Neutral High Pancreatitis?Joint pain
TZD High No Gain Potential benefit
Increase Risk
Neutral Low Vol. retention,fracture, Bladder CA??
SU High Yes Gain Neutral Neutral Neutral Low
Insulin Highest Yes Gain Neutral Neutral Neutral Low

INDIVIDUALIZED THERAPY
FACTORS CONSIDERATIONS
• Age
• Weight
• Comorbidities - Coronary artery disease
- Heart Failure
- Chronic kidney disease
- Liver dysfunction
- Hypoglycemia

Age: Older adults
- Reduced life expectancy
- Higher CVD burden
- Reduced GFR
- At risk for adverse events from polypharmacy
- More likely to be compromised from hypoglycemia
Less ambitious targets
HbA1c <7.5–8.0% if tighter targets not easily achieved
Focus on drug safety

Weight
- Majority of T2DM patients overweight / obese
- Intensive lifestyle program
- Metformin
- SGLT-2 inhibitors
- GLP-1 receptor agonists
- Bariatric surgery ( BMI > 35kg/m2)

Comorbidities
- Coronary Disease
- Heart Failure
- Renal disease
- Liver dysfunction
- Hypoglycemia
Avoid hypoglycemia
SGLT2-I : CVD benefit
GLP-1 R agonist : CVD benfit
Metformin: CVD benefit in obese T2DM (UKPDS)
?? Pioglitazone & CVD events
DPP4-I : Safe

Comorbidities
- Coronary Disease
- Heart Failure
- Renal disease
- Liver dysfunction
- Hypoglycemia
Metformin: May use unless condition is unstable or severe
SGLT2-I: Benefit
Avoid TZDs
DPP-4-I safe ( SAXA??)
GLP1-RA safe

Comorbidities
- Coronary Disease
- Heart Failure
- Renal disease
- Liver dysfunction
- Hypoglycemia
Increased risk of hypoglycemia
Metformin & lactic acidosis
half-dose @GFR < 45 & stop @GFR < 30
Caution with SUs (glibenclamide)
DPP-4-i’s – dose adjust for most
Avoid SGLT-2 inhibitors if GFR < 45
Avoid GLP-1 R agonists if GFR < 30

Comorbidities
- Coronary Disease
- Heart Failure
- Renal disease
- Liver dysfunction
- Hypoglycemia
Most drugs not tested in advanced liver disease
Pioglitazone may help steatosis
Insulin best option if disease severe

Comorbidities
- Coronary Disease
- Heart Failure
- Renal disease
- Liver dysfunction
- Hypoglycemia Emerging concerns regarding
association with increased
morbidity / mortality
Proper drug selection is key in the hypoglycemia prone
Avoid SU, insulin (if possible)

Choosing Glucose lowering Drugs in T2DM
Metformin
Is cost is a major issue?
Yes No
SU TZD
insulin

Choosing Glucose lowering Drugs in T2DM
After Metformin, Cost is not a major issue
1. SGLT2-I: CVD, HF, Renal protection2. GLP1-RA : CVD protection, reduce albuminuria
Consider by hierachy….1. SGLT2-I ( if GFR >45) ( may be < 30 in the future)
2. GLP1-RA ( if GFR>30)
Established ASCVD
Yes No

SGLT2-I should not be considered in:
1. GFR < 45 m/min/m2 ( may be 30 in the future )
2. High risk for DKA
- type 1 DM, lean T2DM on insulin Rx????, - on low CHO diet or fasting
3. High risk for hypovolemia
- frail elderly, acute illness
4. High risk for urinary tract infection
- neurogenic bladder, Hx of recurrent UTI
4. High risk for amputation??
- history or presence of amputation, DM foot

Choosing Glucose lowering Drugs in T2DM
After Metformin, Cost is not a major issue
If not candidate for SGLT2-I or GLP1-RA
Established ASCVD
Yes No
Consider: DPP4-I or TZD : before SU or insulin

Choosing Glucose lowering Drugs in T2DMAfter Metformin, Cost is not a major issue
No Established ASCVD
Need to minimize Hypoglycemia
Need to address Weight loss
eGFR< 30 ml/min
SGLT2-I*GLP1-RA DPP4-I
TZD
SGLT2-I* GLP1-RA
DPP4-ITZD?
Glipizide?Insulin* Reduce renal progression and HHF

1. Start with metformin if no contraindication and tolerable and consider SGLT2-I or GLP1-RA if indicated
2. Cost concern?
3. Established ASCVD?
4. Need to minimize hypoglycemia?
5. Need to address weight loss?
6. CKD stage 4-5?
Choosing Glucose lowering Drugs in T2DM

Choosing Glucose lowering Drugs in T2DM
Metformin
Is cost is a major issue?
Yes No
SU TZD
insulin

Choosing Glucose lowering Drugs in T2DM
After Metformin, Cost is not a major issue
1. SGLT2-I: CVD, HF, Renal protection2. GLP1-RA : CVD protection, reduce albuminuria
Consider by hierachy….1. SGLT2-I ( if GFR >45)2. GLP1-RA ( if GFR>30)
Established ASCVD
Yes No

SGLT2-I should not be considered in:
1. GFR < 45 m/min/m2
2. High risk for DKA
3. High risk for hypovolemia
4. High risk for urinary tract infection
5. High risk for amputation

SGLT2-I should not be considered in:
1. GFR < 45 m/min/m2
2. High risk for DKA- type 1 DM, lean T2DM on insulin Rx????, - on low CHO diet or fasting
3. High risk for hypovolemia
- frail elderly, acute illness
4. High risk for urinary tract infection
- neurogenic bladder, Hx of recurrent UTI
4. High risk for amputation
- history or presence of amputation, DM foot, symptomatic PVD????

Choosing Glucose lowering Drugs in T2DM
After Metformin, Cost is not a major issue
If not candidate for SGLT2-I or GLP1-RA
Established ASCVD
Yes No
Consider: DPP4-I or TZD : before SU or insulin

Choosing Glucose lowering Drugs in T2DM
After Metformin, Cost is not a major issue
No Established ASCVD
Need to minimize Hypoglycemia
Need to address Weight loss
eGFR< 30 ml/min
SGLT2-I* DPP4-I
TZD
SGLT2-I* GLP1-RA
DPP4-ITZD
Glipizide?Insulin* Reduce renal progression and HHF

1. Start with metformin if no contraindication and tolerable
2. Cost concern?
3. Established ASCVD?
4. Need to minimize hypoglycemia?
5. Need to address weight loss?
6. CKD stage 4-5?
Choosing Glucose lowering Drugs in T2DM

ABCDES of Diabetes Care2019
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)

in 1148 Type 2 diabetic patients
Effects of tight BP control (BP 144/82 mmHg) vs
less tight BP control (154/87 mmHg)
any diabetes-related endpt. 24% p=0.0046
diabetes-related deaths 32% p=0.019
stroke 44% p=0.013
microvascular disease 37% p=0.0092
heart failure 56% p=0.0043
retinopathy progression 34% p=0.0038
deterioration of vision 47% p=0.0036
UKPDS: Blood Pressure Control Study

Association of Systolic BP and
Cardiovascular Death in Type 2 DM
250
225
200
175
150
125
100
75
50
0
25
< 130 130–139 140–159 160–179 180–199 > 200
Systolic blood pressure (mm Hg)
Cardiovascular
mortality
rate/10,000
person-yr
Nondiabetic
Stamler J et al. Diabetes Care 1993;16:434-444.
Diabetic

RCT Intensive vs Standard BP HT Rx
Clinical Trials Intensive Standard Outcomes
ACCORD-BP SBP<120(achieved119/64)
SBP 130-140(achieved133/70)
-No benefit-Stroke reduce 41%-More AEs: AKI, high K+
ADVANCE-BP achieved 136/73 achieved 142/75 -reduced primary composite endpoints ( micro and macro)
HOT DBP<80 DBP<90 -no benefit the wholegroup, DM subgroup reduced 51% CV events
SPRINT( no DM )
SBP<120(achieved121.4)
SBP<140(achieved136.2)
- Reduced 25% composite CV events- Reduced death 27%- More AEs: AKI, high K+

• For patients with DM and HT, BP should be individualized: CV risk, potential AE and patient preference (C)
• DM with HT and 10 y ASCVD risk >15%, goal of BP may be <130/80 if it can be safely attained (C)
• DM with HT and 10 y ASCVD risk <15%, treat to a BP target of < 140/90 (A)
Blood Pressure Goal in T2DMADA 2019 Recommedation

• Absolute benefit of BP reduction correlated with absolute baseline CV risk in SPRINT and in earlier trials with conducted with higher baseline BP level
• This approach is consistent with guideline of ACC/AHA, which advocate a BP target of <130/80 for all patients with or without DM
Why target of BP < 130/80 in DM with ASCVD risk >15%, if it can be safely achieved?


ABCDES of Diabetes Care2019
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)
C • Cholesterol – LDL < 100 mgl/dL or >30% reduction

1 ผู้ป่วยเบาหวานอายุตัง้แต ่ 40 ปีขึน้ไปให้ ควรเริม่ยา statin โดยมเีป้าหมายคอืระดบั LDL-C < 100 มก/ดล.
หรอื LDL-C ลดลงจากคา่เริม่แรกกอ่นไดร้บัยาอยา่งน้อย
ร้อยละ 30 ยกเว้นผู้ทีม่รีะดบั LDL-C ตัง้แต ่ 190
มก./ดล. ขึน้ไปให้เริม่ statin ทีท่ าให้ระดบั LDL-C <
100 มก/ดล.หรอื LDL-C ลดลงจากคา่เริม่แรกกอ่นไดร้บั
ยาอยา่งน้อยร้อยละ 50 หาก LDL-C ไมล่ดลงตาม
เป้าหมายภายในระยะเวลา 6 เดอืน หรอืมอีาการไมพ่งึประสงคจ์าก statin จงึพจิารณาเพิม่ยากลุม่ non-statin
ไดแ้ก ่ ezetimibe
Thai RCPT Guideline 2016 for Rx dyslipidemia

2. ผู้ป่วยเบาหวานอายุน้อยกวา่ 40 ปีทีม่ปีจัจยัเส่ียงอืน่
ตัง้แต ่ 2 ข้อขึน้ไป ควรไดร้บัค าแนะน าการปรบัเปลีย่น
พฤตกิรรมชวีติ โดยมรีะยะเวลาในการปรบัเปลีย่น
พฤตกิรรมชวีติ 3 – 6 เดอืน และถ้าหลงัการ
ปรบัเปลีย่นพฤตกิรรมชวีติแลว้ ระดบั LDL-C ยงั
>130 มก./ดล. น่าจะพจิารณาให้ยากลุม่ statinโดยมี
เป้าหมายคอืระดบั LDL-C < 100 มก./ดล.
Thai RCPT Guideline 2016 for Rx dyslipidemia

Thai RCPT Guideline 2016 for Rx Dyslipidemia
3 ผู้ป่วยเบาหวานอายุน้อยกวา่ 40 ปีทีไ่มม่ปีจัจยัเส่ียง
อืน่ อาจไมจ่ าเป็นต้องเริม่ยาลดระดบั LDL-C แตต้่อง
เน้นการปรบัเปลีย่นพฤตกิรรมชวีติ โดยมรีะยะเวลาใน
การปรบัเปลีย่นพฤตกิรรม 3 – 6 เดอืน และถ้าหลงั
การปรบัเปลีย่นพฤตกิรรมชวีติแลว้ ระดบั LDL-C >
130 มก./ดล. อาจพจิารณาให้ยากลุม่ statinโดยมี
เป้าหมายคอืระดบั LDL-C < 100 มก./ดล

Thai RCPT Guideline 2016 for Rx Dyslipidemia
4 ผู้ป่วยเบาหวานทีไ่ดร้บั statin แลว้แตร่ะดบั non-
HDL-C ยงัเกนิเป้าหมาย ( < 130 มก./ดล.ในการ
ป้องกนัแบบปฐมภมู,ิ < 100 มก./ดล.ในการป้องกนัแบบ
ทุตยิภูม)ิ น่าพจิารณาเพิม่ intensity ของ statin กอ่น
หาก non-HDL-C ยงัไมไ่ดต้ามเป้าหมาย จงึ
พจิารณาเพิม่ยากลุม่ fibrates


ABCDES of Diabetes Care2019
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)
C • Cholesterol – LDL < 100 mgl/dL or >30% reduction
D • Drugs to protect the heart
A – ACEi or ARB │ S – Statin │ A – ASA if indicated in very high risk??

ACEI (ARB) Therapy in Type 2 Diabetes
• Diabetic nephropathy ( Microalbuminuria, Clinical proteinuria )
• Coronary artery disease
• Hypertension with
- multiple risk factors
- diabetic nephropathy
- cardiovascular disease

ABCDES of Diabetes Care2019
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)
C • Cholesterol – LDL < 100 mgl/dL or >30% reduction
D • Drugs to protect the heart
A – ACEi or ARB │ S – Statin │ A – ASA if indicated in very high risk??



ADA Recommendation 2019
Aspirin for Primary Prevention in DM
• May consider aspirin therapy ( 75-162 mg/day ) as
a primary prevention strategy in patients with
diabetes who increase CV risk after discussion
with the patients on benefit vs increased risk of
bleeding
• Not recommend aspirin for primary prevention in
patients < 50 yrs without other major risk factors.
For patients in these age-groups with multiple
other risk factors, need clinical judgement
Diabetes Care 2019;37(suppl 1):S113

ABCDES of Diabetes Care2019
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)
C • Cholesterol – LDL < 100 mgl/dL or >30% reduction
D • Drugs to protect the heart
A – ACEi or ARB │ S – Statin │ A – ASA if indicated in very high risk??
E • Exercise / Healthy Eating

ABCDES of Diabetes Care2019
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)
C • Cholesterol – LDL < 100 mgl/dL or >30% reduction
D • Drugs to protect the heart
A – ACEi or ARB │ S – Statin │ A – ASA if indicated in very high risk??
E • Exercise / Healthy Eating
S • Smoking cessation

ABCDES of Diabetes Care2019
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)
C • Cholesterol – LDL < 100 mgl/dL or >30% reduction
D • Drugs to protect the heart
A – ACEi or ARB │ S – Statin │ A – ASA if indicated in very high risk??
E • Exercise / Healthy Eating
S • Smoking cessation
S • Screening for complications

Annual Screening for Complications and early treatment is important
• Nephropathy : serum creatinine (eGFR) , spot morning
urine albumin or MAU
• Retinopathy : dilated retina exam every 1-2 year
• Neuropathy : comprehensive, monofilament
• Foot ulcer : identify high risk
• Coronary artery disease : symptoms, EKG???
• Cerebrovascular disease : symptoms, carotid bruit

ABCDES of Diabetes Care2019
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)
C • Cholesterol – LDL < 100 mgl/dL or >30% reduction
D • Drugs to protect the heart
A – ACEi or ARB │ S – Statin │ A – ASA if indicated in very high risk??
E • Exercise / Healthy Eating
S • Smoking cessation
S • Screening for complications
S • Self-management, stress and other barriers

Diabetic Self Management Education
• What is diabetes?• Complications of diabetes• Goals of therapy• Hyperglycemia and Hypoglycemia• Medical nutritional therapy• Exercise• How to use OAD, insulin?• Sick day care• Foot care

ABCDES of Diabetes Care2019( Holistic and Individualized Approach )
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)
C • Cholesterol – LDL < 100 mgl/dL or >30% reduction
D • Drugs to protect the heart
A – ACEi or ARB │ S – Statin │ A – ASA if indicated in very high risk??
E • Exercise / Healthy Eating
S • Smoking cessation
S • Screening for complications
S • Self-management, stress and other barriers

Thank you for your attention