Embed Size (px)
DESCRIPTION
Sanjeet Panesar, Sanjay Chaturvedi, NK Saini, R. Avasthi, Abhishek Singh, Pankaj Chikkara. Do joint national committee VII criteria also need to take non pharmacological measures into consideration? - Empirical evidence from slum resettlement colony from Delhi. IAIM, 2015; 2(1): 15-21.
Citation preview
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol.
Copy right © 2015, IAIM, All Rights Reserved.
Original Research Article
Do joint national committee VII criteria
also need to take non pharmacological
measures into consideration?
evidence from slum resettlement colony
Sanjeet Panesar1, Sanjay Chaturvedi
Abhishek Singh1Senior Resident, Department of Community Medicine, Vardhman Mahavir Medical College and
Safdarjung Hospital, New Delh2Professor, Department of Community Medicine, UCMS, Delhi
3 Assistant Professor, Department of Community Medicine, UCMS, Delhi4 Professor,
5Assistant Professor, Department of Community Medicine
6Assistant Professor, Department of F
*Corresponding author email:
How to cite this article: Sanjeet Panesar, Sanjay Chaturvedi
Pankaj Chikkara. Do joint national committee VII crit
measures into consideration? - Empirical evidence from slum resettlement colony from Delhi
2015; 2(1): 15-21.
Available online at
Received on: 03-12-2014
Abstract
Background: Currently Joint National Committee (JNC) VII criteria are used worldwide to d
hypertension but it does not take non pharmacological measures into consideration. Also, it does
not consider Indian system of medicine.
Objectives: To assess whether JNC
or revision is required especially for Indian communities where such practices are prevalent.
Material and methods: The present community based cross
Nagri, a slum resettlement of East Delhi which comes un
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol. 2, Issue 1, January, 2015.
Rights Reserved.
Do joint national committee VII criteria
also need to take non pharmacological
measures into consideration? - Empirical
evidence from slum resettlement colony
from Delhi
, Sanjay Chaturvedi2, NK Saini
3, R.
Abhishek Singh5*
, Pankaj Chikkara
6
Senior Resident, Department of Community Medicine, Vardhman Mahavir Medical College and
Safdarjung Hospital, New Delhi, India
Department of Community Medicine, UCMS, Delhi, India
, Department of Community Medicine, UCMS, Delhi
Professor, Department of Medicine, UCMS, Delhi, India
Assistant Professor, Department of Community Medicine, SHKM Govt. Medical College, Haryana
India
Assistant Professor, Department of Forensic Medicine, PGIMS, Rohtak, Haryana
*Corresponding author email: [email protected]
Sanjeet Panesar, Sanjay Chaturvedi, NK Saini, R. Avasthi,
Do joint national committee VII criteria also need to take non pharmacological
Empirical evidence from slum resettlement colony from Delhi
Available online at www.iaimjournal.com
2014 Accepted on:
Currently Joint National Committee (JNC) VII criteria are used worldwide to d
not take non pharmacological measures into consideration. Also, it does
not consider Indian system of medicine.
To assess whether JNC VII in its present form is valid to diagnose hypertension correctly
or revision is required especially for Indian communities where such practices are prevalent.
The present community based cross-sectional study was carried out in Na
Nagri, a slum resettlement of East Delhi which comes under field practice area of the D
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 15
Do joint national committee VII criteria
also need to take non pharmacological
Empirical
evidence from slum resettlement colony
, R. Avasthi4,
Senior Resident, Department of Community Medicine, Vardhman Mahavir Medical College and
, India
, Department of Community Medicine, UCMS, Delhi, India
, SHKM Govt. Medical College, Haryana,
, PGIMS, Rohtak, Haryana, India
R. Avasthi, Abhishek Singh,
eria also need to take non pharmacological
Empirical evidence from slum resettlement colony from Delhi. IAIM,
Accepted on: 19-12-2014
Currently Joint National Committee (JNC) VII criteria are used worldwide to diagnose
not take non pharmacological measures into consideration. Also, it does
VII in its present form is valid to diagnose hypertension correctly
or revision is required especially for Indian communities where such practices are prevalent.
sectional study was carried out in Nand
der field practice area of the Department of

JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol.
Copy right © 2015, IAIM, All Rights Reserved.
Community Medicine, UCMS, Delhi from
59 years were selected through multistage systematic random
cut-offs considered in our criteria was similar to the JNC VII cut
≥90 mmHg), the difference was in the last part of JNC VII definition of hypertension i.e. treatment by
anti hypertensive medicines; our criteria comprised of this statement as “any anti hypertensive
measure”. Chi-square (χ²) test was applied
Results: Overall 54 were found to have hypertension by JNC VII criteria whereas 61 by our criteria.
Seven patients who were not hypertensive by JNC VII but hypertensive by our criteria and the
difference was found to be statistically highly significant (p<0.001).
non pharmacological measure adopted by male gender where as in females
most common measure adopted.
Conclusion: Our study emphasized inclusion of non
making diagnosis of hypertension in our setup.
Key words
Treatment, Control, Non pharmacological
Introduction
Non-communicable diseases especially
cardiovascular diseases (CVD) are major causes
of death and disability in low and
countries [1]. Over 80% of CVD deaths occur in
such countries as their populations are more
exposed to risk factors, and have less access to
preventive efforts [2]. By 2020, it is expected
that India will have more than 50% of the CVD
cases in the world. World Health Organization
(WHO) has named hypertension as ‘Silent Killer’
and it has been reported as seventh contributor
to premature death in developing countries
Hypertension is most commonly associated with
cardiovascular diseases worldwide and is the
most important modifiable risk factor for
cardiovascular mortality. According to WHO,
each year at least 7.1 million people die as a
result of hypertension [3]. Despite the high
prevalence; prevention, detection, treatment,
and control of hypertension is suboptimal and
unsatisfactory in developing coun
[4].
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol. 2, Issue 1, January, 2015.
Rights Reserved.
nity Medicine, UCMS, Delhi from August 2010 to February 2012. Total 310
59 years were selected through multistage systematic random sample. Though the blood pressure
offs considered in our criteria was similar to the JNC VII cut-offs (SBP ≥140 mmHg and or DBP
90 mmHg), the difference was in the last part of JNC VII definition of hypertension i.e. treatment by
dicines; our criteria comprised of this statement as “any anti hypertensive
square (χ²) test was applied for analysis.
54 were found to have hypertension by JNC VII criteria whereas 61 by our criteria.
not hypertensive by JNC VII but hypertensive by our criteria and the
difference was found to be statistically highly significant (p<0.001). Exercise was the most common
non pharmacological measure adopted by male gender where as in females, salt restricti
most common measure adopted.
Our study emphasized inclusion of non-drug therapy measures into consideration while
making diagnosis of hypertension in our setup.
n pharmacological interventions, Hypertension.
communicable diseases especially
cardiovascular diseases (CVD) are major causes
and middle income
. Over 80% of CVD deaths occur in
countries as their populations are more
exposed to risk factors, and have less access to
. By 2020, it is expected
that India will have more than 50% of the CVD
World Health Organization
n as ‘Silent Killer’
and it has been reported as seventh contributor
to premature death in developing countries [3].
Hypertension is most commonly associated with
cardiovascular diseases worldwide and is the
most important modifiable risk factor for
ovascular mortality. According to WHO,
each year at least 7.1 million people die as a
. Despite the high
prevalence; prevention, detection, treatment,
and control of hypertension is suboptimal and
unsatisfactory in developing countries like India
It is established fact that non pharmacological
measures also have significant role in treatment
and control of hypertension. Currently JNC VII
criteria are used worldwide to diagnose
hypertension but it does not take non
pharmacological measures into consideration.
Also, it does not consider Indian system of
medicine. Therefore it becomes essential to
assess whether JNC VII in its present form is
valid to diagnose hypertension correctly or
revision is required especially for Indian
communities where such practices are
prevalent.
Material and methods
The present community based cross
study was carried out in Nand
resettlement of East Delhi which comes under
field practice area of the D
Community Medicine, University College of
Medical Sciences (UCMS), Delhi from August
2010 to February 2012. It has a population of
over 50,000 and mostly falling in
low socio-economic status.
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 16
310 subjects aged 20-
Though the blood pressure
140 mmHg and or DBP
90 mmHg), the difference was in the last part of JNC VII definition of hypertension i.e. treatment by
dicines; our criteria comprised of this statement as “any anti hypertensive
54 were found to have hypertension by JNC VII criteria whereas 61 by our criteria.
not hypertensive by JNC VII but hypertensive by our criteria and the
Exercise was the most common
salt restriction was the
herapy measures into consideration while
non pharmacological
measures also have significant role in treatment
and control of hypertension. Currently JNC VII
criteria are used worldwide to diagnose
hypertension but it does not take non
cal measures into consideration.
Also, it does not consider Indian system of
medicine. Therefore it becomes essential to
assess whether JNC VII in its present form is
valid to diagnose hypertension correctly or
revision is required especially for Indian
ommunities where such practices are
The present community based cross-sectional
study was carried out in Nand Nagri, a slum
resettlement of East Delhi which comes under
ractice area of the Department of
dicine, University College of
Medical Sciences (UCMS), Delhi from August
2010 to February 2012. It has a population of
over 50,000 and mostly falling in the category of

JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol.
Copy right © 2015, IAIM, All Rights Reserved.
The sample size was calculated with anticipated
prevalence of hypertension as 27.5%
Absolute precision, 95% Confidence Interval and
10% non response error, as 310 adults over the
age of 20 years. The study subjects were
selected through multistage systematic random
sampling technique. One sub block was
randomly selected from each of the five blocks
of the study area. Sampling unit was a
household; a household was randomly selected
from first 20 households (sampling interval for
5%). Thereafter, starting from that household,
every 20th household was selected
years subjects, residing in the selected
household for 6 months or more, were included
in the study. If there were no eligible subj
the selected household or the house was closed
for 3 consecutive visits, it was replaced by a
contiguous household without disturbing the
allocation of next 20th sampling unit.
Blood pressure of all the subjects was measured
according to JNC VII / American Heart
Association (AHA) recommendations. JNC
guidelines [6, 7] were followed for defining
awareness, treatment and control of
hypertension. Among the hypertensive’s,
subjects with prior diagnosis of hypertension/
high BP were considered as ‘aware’; those with
current anti hypertensive drug therapy as
‘treated’; and subjects showing SBP
DBP <90 mmHg, and taking anti
medication as ‘controlled’. Though the blood
pressure cut-offs considered in our criteria was
similar to the JNC VII cut-offs (SBP
and or DBP ≥90 mmHg), the difference was in
the last part of JNC VII definition
i.e. treatment by anti hypertensive medicines;
our criteria comprised of this statement as “any
anti hypertensive measure”; these measures
taken include anti hypertensive drugs (which
could be allopathic, ayurvedic, homeopathic,
unani, siddha, herbal medicine, indigenous
medicines), non pharmacologic measures like
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol. 2, Issue 1, January, 2015.
Rights Reserved.
The sample size was calculated with anticipated
of hypertension as 27.5% [5], 5%
Absolute precision, 95% Confidence Interval and
10% non response error, as 310 adults over the
age of 20 years. The study subjects were
selected through multistage systematic random
sampling technique. One sub block was
domly selected from each of the five blocks
of the study area. Sampling unit was a
household; a household was randomly selected
from first 20 households (sampling interval for
5%). Thereafter, starting from that household,
household was selected. All the 20-59
years subjects, residing in the selected
household for 6 months or more, were included
in the study. If there were no eligible subject in
or the house was closed
for 3 consecutive visits, it was replaced by a
us household without disturbing the
sampling unit.
Blood pressure of all the subjects was measured
according to JNC VII / American Heart
Association (AHA) recommendations. JNC
were followed for defining
treatment and control of
sion. Among the hypertensive’s,
subjects with prior diagnosis of hypertension/
high BP were considered as ‘aware’; those with
hypertensive drug therapy as
‘treated’; and subjects showing SBP <140 mmHg,
, and taking anti hypertensive
Though the blood
offs considered in our criteria was
offs (SBP ≥140 mmHg
90 mmHg), the difference was in
the last part of JNC VII definition of hypertension
i.e. treatment by anti hypertensive medicines;
our criteria comprised of this statement as “any
anti hypertensive measure”; these measures
taken include anti hypertensive drugs (which
could be allopathic, ayurvedic, homeopathic,
dha, herbal medicine, indigenous
medicines), non pharmacologic measures like
weight reduction, exercise, salt restriction,
smoking cessation, reduction in alcohol intake,
stress management, yoga, meditation, etc.
In depth enquiry was made regarding afore
mentioned non-pharmacological anti
hypertensive measures taken by them. Relevant
socio-demographic data of the individuals was
also recorded. Ethical committee approved the
study. Informed consent was obtained from the
study participants.
The collected data was coded and entered in
Statistical Package for Social Sciences (SPSS),
version 20. The results were expressed as
proportions. Chi-square (χ²) test was applied to
test the difference across the groups and p<0.05
was considered statistically significan
Results
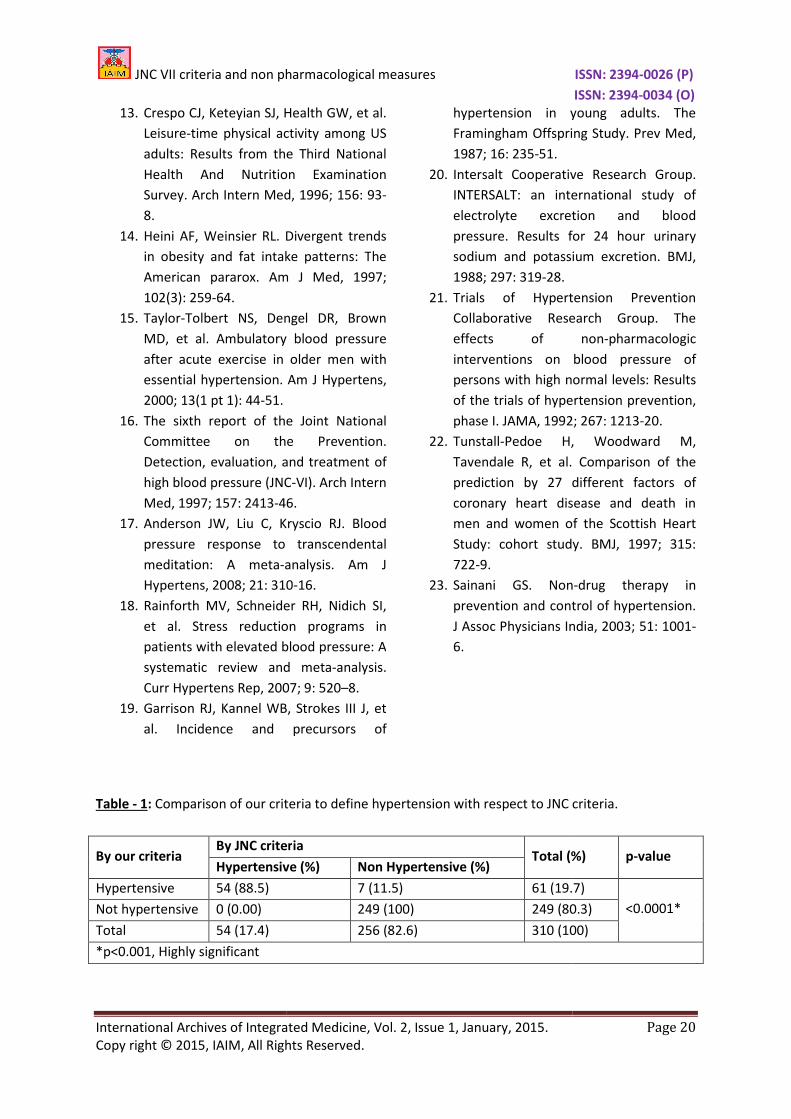
The comparison made between JNC VII and our
criteria to diagnose the hypertension among 310
subjects as per Table - 1. Overall 54 were found
to have hypertension by JNC VII criteria whereas
61 by our criteria. Seven patients who were not
hypertensive by JNC VII but hypertensive by our
criteria and the difference were found to be
statistically highly significant. (p<0.001)
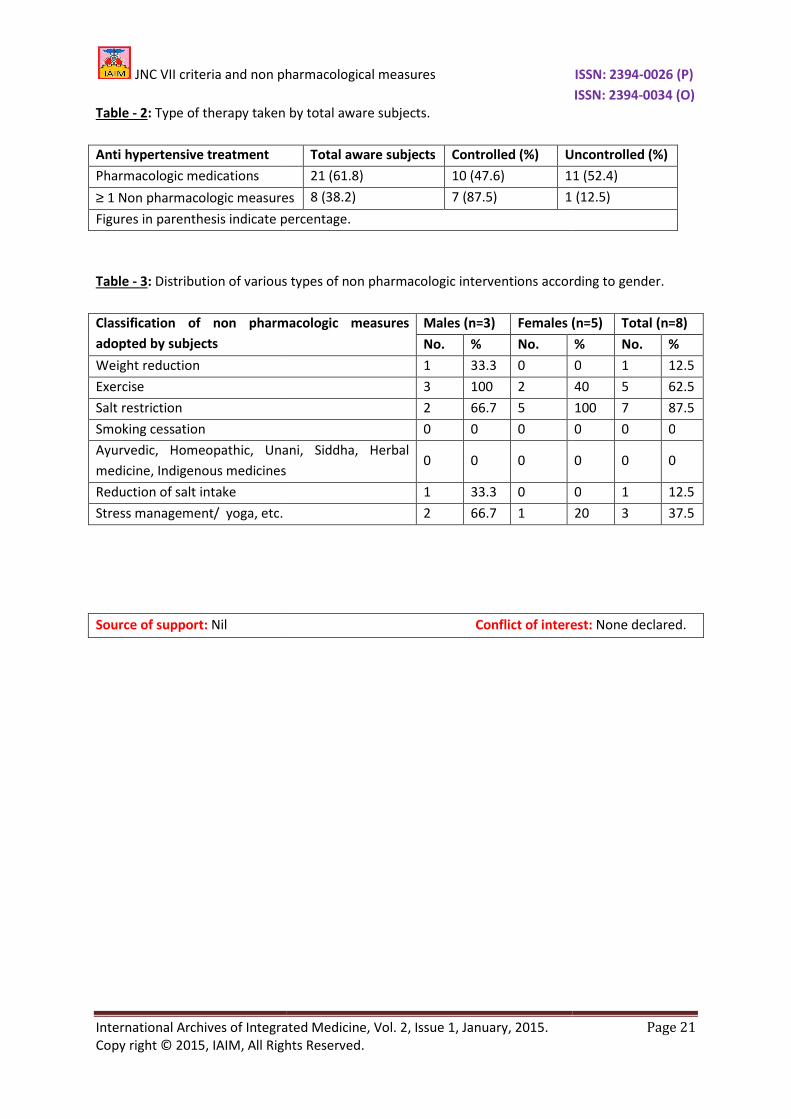
Proportion of aware subjects who controlled
their blood pressure by adopting one
non pharmacologic measure or life style was
calculated. According to it,
non pharmacologic medication to control their
BP of which 7 subjects were able to achieve BP
control. All the 8 subjects who used non
pharmacologic measures w
hypertension as per Table - 2
The most common non pharmacological
measure adopted by the subjects was salt
restriction in diet (87.5%), among males most
common measure was exercise (100%) where as
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 17
weight reduction, exercise, salt restriction,
smoking cessation, reduction in alcohol intake,
stress management, yoga, meditation, etc.
In depth enquiry was made regarding afore
pharmacological anti
hypertensive measures taken by them. Relevant
demographic data of the individuals was
also recorded. Ethical committee approved the
study. Informed consent was obtained from the
ata was coded and entered in
Statistical Package for Social Sciences (SPSS),
version 20. The results were expressed as
square (χ²) test was applied to
test the difference across the groups and p<0.05
was considered statistically significant.
The comparison made between JNC VII and our
criteria to diagnose the hypertension among 310
. Overall 54 were found
to have hypertension by JNC VII criteria whereas
61 by our criteria. Seven patients who were not
rtensive by JNC VII but hypertensive by our
criteria and the difference were found to be
statistically highly significant. (p<0.001)
Proportion of aware subjects who controlled
eir blood pressure by adopting one or more
non pharmacologic measure or life style was
8 subjects adopted
non pharmacologic medication to control their
BP of which 7 subjects were able to achieve BP
control. All the 8 subjects who used non
s were having Grade 1
2.
The most common non pharmacological
measure adopted by the subjects was salt
restriction in diet (87.5%), among males most
common measure was exercise (100%) where as

JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol.
Copy right © 2015, IAIM, All Rights Reserved.
in females salt restriction was the
measure adopted (100%). Any other system of
medicine other than allopathic system
used by study subjects as per Table
Discussion
The successive reports of the Joint National
Committee on prevention, detection, evaluation
and treatment of high blood pressure (HBP), non
drug therapy is recommended as
been considered efficacious [8]
reports on primary prevention of HBP including
the primary prevention
hypertension (report of a WHO s
[9] and National High Blood Pressure Education
Program’s (NHBPEP) working groups report on
primary prevention of hypertension
stressed on the non drug therapy.
The JNC VII criteria to diagnose hypertension
were put forth way back in 2003.
study, we observed that 54 were diagnosed to
have hypertension by JNC VII criteria where
61 by our criteria in a study of mere 310
subjects. Difference between JNC VII and our
criteria was in the last part of JNC VII definition
of hypertension i.e. treatment by anti
hypertensive medicines; our criteria comprised
of this statement as “any an
measure.” Seven patients were non
hypertensive by JNC VII but diagnosed to have
hypertension by our criteria. Issue would look
more relevant and serious when this aspect is
applied to the bigger population of our
communities where they prac
pharmacologic measures to live healthy. It can
be said that we are underestimating the actual
burden of hypertension. How policies can be
made to manage a public health problem
without knowing its actual magnitude!
It was observed in our study that out of 8
subjects who adopted non pharmacologic
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol. 2, Issue 1, January, 2015.
Rights Reserved.
in females salt restriction was the most common
measure adopted (100%). Any other system of
medicine other than allopathic system was not
Table - 3.
The successive reports of the Joint National
detection, evaluation
pressure (HBP), non
drug therapy is recommended as it has long
[8]. In addition,
revention of HBP including
of essential
hypertension (report of a WHO scientific group)
and National High Blood Pressure Education
Program’s (NHBPEP) working groups report on
primary prevention of hypertension [10], have
drug therapy.
The JNC VII criteria to diagnose hypertension
were put forth way back in 2003. In the present
we observed that 54 were diagnosed to
have hypertension by JNC VII criteria where as
61 by our criteria in a study of mere 310
subjects. Difference between JNC VII and our
criteria was in the last part of JNC VII definition
of hypertension i.e. treatment by anti
hypertensive medicines; our criteria comprised
of this statement as “any anti hypertensive
measure.” Seven patients were non
hypertensive by JNC VII but diagnosed to have
hypertension by our criteria. Issue would look
more relevant and serious when this aspect is
applied to the bigger population of our
where they practice non
pharmacologic measures to live healthy. It can
be said that we are underestimating the actual
burden of hypertension. How policies can be
made to manage a public health problem
without knowing its actual magnitude!
It was observed in our study that out of 8
subjects who adopted non pharmacologic
medication to control their BP
practiced ‘Salt restriction’. Cutler
their analysis of 23 randomly controlled trials
showed that 100 mmol/day re
intake was associated with a
mmHg SBP and 2.7 mmHg DBP in hypertensive
subjects and 2.2 mmHg/1.3 mm
normotensives. Others also observed the similar
findings [8, 12].
Physical activity in the form of exercise was
adopted by 5 individuals in our study. Today,
physical exercise is considered as an important
component of the non
hypertension. Physically active persons have
lower blood pressure, reduced risk for
cardiovascular and all cause mortality and l
longer. The benefit of physical activity to the
primary prevention of hypertension has been
documented by both clinical trials and
longitudinal studies [13, 14, 15]
Smoking independently raises BP, although
epidemiologically the relationship between
smoking and hypertension is often confounded
by other factors such as alcohol consumption
and lower consumption of fruits and vegetables
(anti-oxidants) amongst smokers than
smokers [8].
JNC VI report [16] found no support for the use
of relaxation techniques for the prevention of
hypertension. Yoga, meditation (mind
techniques) are widely practiced for stress
reduction in India. In our study also 3 subjects
adopted such techniques to reduce their blood
pressure. BP lowering effect of
meditation has been further supported by two
meta-analyses; each suggesting TM can reduce
both SBP and DBP.
Several clinical studies Viz. Framingham off
spring study [19], INTERSALT study
II [21, 22] have shown direct benefit
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 18
medication to control their BP, 7 of them had
practiced ‘Salt restriction’. Cutler, et al. [11] in
analysis of 23 randomly controlled trials
showed that 100 mmol/day reduction in sodium
intake was associated with a decline of 5.7
Hg DBP in hypertensive
subjects and 2.2 mmHg/1.3 mmHg in
normotensives. Others also observed the similar
Physical activity in the form of exercise was
ed by 5 individuals in our study. Today,
physical exercise is considered as an important
component of the non drug treatment of
hypertension. Physically active persons have
lower blood pressure, reduced risk for
cardiovascular and all cause mortality and live
longer. The benefit of physical activity to the
hypertension has been
documented by both clinical trials and
[13, 14, 15].
Smoking independently raises BP, although
epidemiologically the relationship between
smoking and hypertension is often confounded
factors such as alcohol consumption
of fruits and vegetables
oxidants) amongst smokers than non-
found no support for the use
echniques for the prevention of
Yoga, meditation (mind-body
techniques) are widely practiced for stress
reduction in India. In our study also 3 subjects
adopted such techniques to reduce their blood
lowering effect of transcendental
meditation has been further supported by two
analyses; each suggesting TM can reduce
Several clinical studies Viz. Framingham off-
, INTERSALT study [20], TOPH-I,
have shown direct benefit of weight
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol.
Copy right © 2015, IAIM, All Rights Reserved.
reduction on hypertension. During weight loss, a
rapid reduction in BP is seen over 8
There seems to be a linear relationship between
weight and blood pressure. The BP falls as there
is reduction of weight. With reduction of weight,
one can reduce or even stop the medications
[23].
Conclusion
To conclude, we have accumulated knowledge
and empirical evidences over decades of
research but made poor use of them.
emphasized inclusion of non drug t
measures into consideration while making
diagnosis of hypertension in our setup. Large
scale studies are recommended to support our
findings.
References
1. Gupta R, Guptha S, Joshi R, Xavier D.
Translating evidence into policy for
cardiovascular disease control in India.
Health Res Policy Syst., 2011
2. Gersh B, Mayosi B, Sliwa K, Yusuf S.
epidemic of cardiovascular diseases in
the developing world: Global
implications. Eur Heart J,
648.
3. Deepa R, Shanthirani CS, Pradeepa R,
Mohan V. Is the 'rule of halves' in
hypertension still valid?
the Chennai Urban Population
Assoc Physicians India, 2003
4. Gandhi S, Chaudhari N, Bh
K, Vasava B. Awareness and prevalence
of myocardial infarction and
hypertension in general population of
Surat city. National Journal of
Community Medicine, 2010; 1(2):
42.
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol. 2, Issue 1, January, 2015.
Rights Reserved.
reduction on hypertension. During weight loss, a
rapid reduction in BP is seen over 8-10 weeks.
There seems to be a linear relationship between
weight and blood pressure. The BP falls as there
is reduction of weight. With reduction of weight,
can reduce or even stop the medications
To conclude, we have accumulated knowledge
and empirical evidences over decades of
use of them. Our study
emphasized inclusion of non drug therapy
n while making
diagnosis of hypertension in our setup. Large
scale studies are recommended to support our
S, Joshi R, Xavier D.
Translating evidence into policy for
cardiovascular disease control in India.
, 2011; 9: 8.
Gersh B, Mayosi B, Sliwa K, Yusuf S. The
epidemic of cardiovascular diseases in
the developing world: Global
Eur Heart J, 2010; 31: 642-
Deepa R, Shanthirani CS, Pradeepa R,
Is the 'rule of halves' in
hypertension still valid? - Evidence from
the Chennai Urban Population Study. J
Assoc Physicians India, 2003; 51: 153-7.
Gandhi S, Chaudhari N, Bhuva R, Mallick
K, Vasava B. Awareness and prevalence
of myocardial infarction and
hypertension in general population of
Surat city. National Journal of
, 2010; 1(2): 139-
5. Chaturvedi S, Pant M, Neelam, Yadav G.
Hypertension in Delhi: pr
awareness, treatment and control. Trop
Doct, 2007; 37: 142-
6. Chobanian AV, Bakris GL, Black HR,
Cushman WC, Green LA, Izzo JL Jr, et al.
The Seventh Report of the Joint National
Committee on prevention, detection,
evaluation, and treatment of hi
pressure: The JNC 7 report. JAMA
289: 2560-72.
7. Burt VL, Cutler JA, Higgins M, Horan MJ,
Labarthe D, Whelton P, Brown C,
Roccella EJ. Trends in the prevalence,
awareness, treatment, and control of
hypertension in the ad
Hypertension, 1995; 26: 60
8. Labarthe Darwin,
Drug interventions in hyper
prevention and control. Cardiol Clin
2002; 20: 249-63.
9. World Health Organization
prevention of essential hypertension
report of a WHO Scientific
Geneva, Switzerland: World Health
Organization; Technical Report Series
1982, 678.
10. National High Blood Pressure Education
Program (NHBPEP) Working Group.
National High Blood Pressure Education
Program Working Group report on
primary prevention of hy
Arch Intern Med, 1993;
11. Culter JA, Follmann D, Elliott P,
overview of randomized trials of sodium
reduction and blood pressure.
Hypertension, 1991;
33.
12. Dole PV, Dahl LK, Cotzias GC, Eer HA,
Krebs ME. Dietary treatment of
hypertension: Clinical and metabolic
studies of patients on rice
Clinc Invest, 1950; 29:
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 19
Chaturvedi S, Pant M, Neelam, Yadav G.
Hypertension in Delhi: prevalence,
awareness, treatment and control. Trop
-5.
Chobanian AV, Bakris GL, Black HR,
Cushman WC, Green LA, Izzo JL Jr, et al.
The Seventh Report of the Joint National
Committee on prevention, detection,
atment of high blood
he JNC 7 report. JAMA, 2003;
Burt VL, Cutler JA, Higgins M, Horan MJ,
Labarthe D, Whelton P, Brown C,
Roccella EJ. Trends in the prevalence,
awareness, treatment, and control of
hypertension in the adult US population.
1995; 26: 60-69.
Labarthe Darwin, Ayala Carma. Non
Drug interventions in hyper-tension,
prevention and control. Cardiol Clin,
World Health Organization - Primary
prevention of essential hypertension
report of a WHO Scientific Group.
Geneva, Switzerland: World Health
Organization; Technical Report Series
National High Blood Pressure Education
Program (NHBPEP) Working Group.
National High Blood Pressure Education
Program Working Group report on
primary prevention of hypertension.
1993; 153: 186-208.
r JA, Follmann D, Elliott P, Suhl I. An
overview of randomized trials of sodium
reduction and blood pressure.
1991; 17(suppl. I); 1: 27-
Dahl LK, Cotzias GC, Eer HA,
ary treatment of
linical and metabolic
studies of patients on rice-fruits diet. J
29: 1189-1206.
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol.
Copy right © 2015, IAIM, All Rights Reserved.
13. Crespo CJ, Keteyian SJ, Health GW, et al.
Leisure-time physical activity among US
adults: Results from the Third Nationa
Health And Nutrition Examination
Survey. Arch Intern Med
8.
14. Heini AF, Weinsier RL. Divergent trends
in obesity and fat intake patterns: T
American pararox. Am J Med
102(3): 259-64.
15. Taylor-Tolbert NS, Dengel DR, Brown
MD, et al. Ambulatory blood pressure
after acute exercise in older men with
essential hypertension. Am J Hypertens
2000; 13(1 pt 1): 44-51.
16. The sixth report of the Joint National
Committee on the Prevention.
Detection, evaluation, and treatment of
high blood pressure (JNC
Med, 1997; 157: 2413-46.
17. Anderson JW, Liu C, Kryscio RJ. Blood
pressure response to t
meditation: A meta-analysis. Am J
Hypertens, 2008; 21: 310
18. Rainforth MV, Schneider RH, Nidich SI
et al. Stress reduction programs
patients with elevated blood pressure: A
systematic review and meta
Curr Hypertens Rep, 2007;
19. Garrison RJ, Kannel WB, Strokes III J, et
al. Incidence and precursors of
Table - 1: Comparison of our criteria to define hypertension with respect to JNC criteria
By our criteria By JNC criter
Hypertensive
Hypertensive 54 (88.5)
Not hypertensive 0 (0.00)
Total 54 (17.4)
*p<0.001, Highly significant
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol. 2, Issue 1, January, 2015.
Rights Reserved.
Crespo CJ, Keteyian SJ, Health GW, et al.
ical activity among US
esults from the Third National
Health And Nutrition Examination
Survey. Arch Intern Med, 1996; 156: 93-
Heini AF, Weinsier RL. Divergent trends
esity and fat intake patterns: The
American pararox. Am J Med, 1997;
Tolbert NS, Dengel DR, Brown
bulatory blood pressure
after acute exercise in older men with
essential hypertension. Am J Hypertens,
The sixth report of the Joint National
Committee on the Prevention.
Detection, evaluation, and treatment of
(JNC-VI). Arch Intern
46.
Anderson JW, Liu C, Kryscio RJ. Blood
pressure response to transcendental
analysis. Am J
310-16.
Rainforth MV, Schneider RH, Nidich SI,
et al. Stress reduction programs in
with elevated blood pressure: A
systematic review and meta-analysis.
2007; 9: 520–8.
Garrison RJ, Kannel WB, Strokes III J, et
al. Incidence and precursors of
hypertension in young adults. The
Framingham Offspring Study. Pre
1987; 16: 235-51.
20. Intersalt Cooperative Research Group.
INTERSALT: an international study of
electrolyte excretion and blood
pressure. Results for 24 hour urinary
sodium and potassium excretion. BMJ
1988; 297: 319-28.
21. Trials of Hypertension Prevent
Collaborative Research Group. The
effects of non
interventions on blood pressure of
persons with high n
of the trials of hypertension prevention,
phase I. JAMA, 1992;
22. Tunstall-Pedoe H, Woodward M,
Tavendale R, et al. Comparison of the
prediction by 27 different factors of
coronary heart disease and death in
men and women of the Scottish Heart
Study: cohort study. BMJ
722-9.
23. Sainani GS. Non
prevention and control of hyperte
J Assoc Physicians India, 2003
6.
Comparison of our criteria to define hypertension with respect to JNC criteria
By JNC criteria Total (%)
Hypertensive (%) Non Hypertensive (%)
7 (11.5) 61 (19.7)
249 (100) 249 (80.3)
256 (82.6) 310 (100)
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 20
hypertension in young adults. The
Framingham Offspring Study. Prev Med,
Intersalt Cooperative Research Group.
INTERSALT: an international study of
electrolyte excretion and blood
pressure. Results for 24 hour urinary
sodium and potassium excretion. BMJ,
Trials of Hypertension Prevention
Collaborative Research Group. The
effects of non-pharmacologic
interventions on blood pressure of
persons with high normal levels: Results
of the trials of hypertension prevention,
1992; 267: 1213-20.
Pedoe H, Woodward M,
Tavendale R, et al. Comparison of the
prediction by 27 different factors of
coronary heart disease and death in
men and women of the Scottish Heart
Study: cohort study. BMJ, 1997; 315:
GS. Non-drug therapy in
prevention and control of hypertension.
J Assoc Physicians India, 2003; 51: 1001-
Comparison of our criteria to define hypertension with respect to JNC criteria.
Total (%) p-value
61 (19.7)
<0.0001* 249 (80.3)
310 (100)
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol.
Copy right © 2015, IAIM, All Rights Reserved.
Table - 2: Type of therapy taken by total aware subjects.
Anti hypertensive treatment
Pharmacologic medications
≥ 1 Non pharmacologic measures
Figures in parenthesis indicate percentage.
Table - 3: Distribution of various types of non pharmacologic interventions according to gender.
Classification of non pharmacologic measures
adopted by subjects
Weight reduction
Exercise
Salt restriction
Smoking cessation
Ayurvedic, Homeopathic, Unani, Siddha, Herbal
medicine, Indigenous medicines
Reduction of salt intake
Stress management/ yoga, etc.
Source of support: Nil
JNC VII criteria and non pharmacological measures
International Archives of Integrated Medicine, Vol. 2, Issue 1, January, 2015.
Rights Reserved.
therapy taken by total aware subjects.
Total aware subjects Controlled (%) Uncontrolled (%)
21 (61.8) 10 (47.6) 11
pharmacologic measures 8 (38.2) 7 (87.5) 1
parenthesis indicate percentage.
Distribution of various types of non pharmacologic interventions according to gender.
Classification of non pharmacologic measures Males (n=3) Females (n=5)
No. % No.
1 33.3 0
3 100 2
2 66.7 5
0 0 0
Ayurvedic, Homeopathic, Unani, Siddha, Herbal
0 0 0
1 33.3 0
2 66.7 1
Nil Conflict of interest:
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 21
Uncontrolled (%)
11 (52.4)
(12.5)
Distribution of various types of non pharmacologic interventions according to gender.
(n=5) Total (n=8)
% No. %
0 1 12.5
40 5 62.5
100 7 87.5
0 0 0
0 0 0
0 1 12.5
20 3 37.5
Conflict of interest: None declared.