Embed Size (px)
Citation preview
Do You Think Like the Experts?Refining the Management of Advanced NSCLC With
ALK Rearrangement
Reference SlidesClinical Case Scenario #2

Clincial Case Scenario #2A 37-year-old woman with symptomatic metastatic lung adenocarcinoma (metastases in lung, liver, and left suprarenal gland) started crizotinib under the expanded access program 12 months ago. She tolerated treatment well and became asymptomatic after the first month of therapy. Evaluation after 4 months of therapy showed very good partial remission. The patient had a surveillance brain magnetic resonance image (MRI) performed at 6 months, the results of which were normal. On her 12th month of crizotinib, results from her brain MRI show 3 asymptomatic brain lesions between 0.5 cm to 2.5 cm in size. There is no extracranial progression.

Q1: Which of the following best describes your treatment approach for this patient with asymptomatic brain metastases?
1. Local therapy + continue crizotinib2. Discontinue crizotinib → local therapy →
pemetrexed-based chemotherapy3. Discontinue crizotinib → local therapy → ceritinib4. No local therapy for brain metastases at this time,
discontinue crizotinib and start ceritinib

Q2: What would be your approach if this patient only had extracranial progression and is symptomatic?
1. Continue crizotinib and add chemotherapy2. Stop crizotinib and start cisplatin/pemetrexed
chemotherapy3. Stop crizotinib and start ceritinib4. Rebiopsy for additional mutation testing
Managing Brain Metastasis in Patients With ALK+ NSCLC
• Use stereotatic radiosurgery as opposed to whole-brain radiotherapy
• Discontinue treatment for two days before performing local therapy, and then resumetreatment
• Follow-up best performed by magnetic resonance imaging (MRI)– Imaging every ~4-6 months
• ALK inhibitors do have activity in brain metastasis

Duration of Treatment Before/After Intracranial PD in Patients Randomized to Crizotinib
Treatment Duration, Weeks
0-70-80-90-100 100908070605040302010-60 -50 -40 -30 -20 -10
* *
*
BM at baselineNo BM at baselineRadiotherapy after intracranial PDOn treatment at data cutoffHad intracranial PD in existing lesion
*
Duration of treatment beyond intracranial PDa: Median 20.4 weeks (range: 3.3-84.4) aAmong the 22 patients receiving crizotinib for ≥3 weeks beyond intracranial PDPD, progression of disease; BM, brain metastases
Solomon BJ, et al. Presented at: 16th World Conference on Lung Cancer; September 6-9 2015; Denver, Colorado; Abstract MINI31.04.
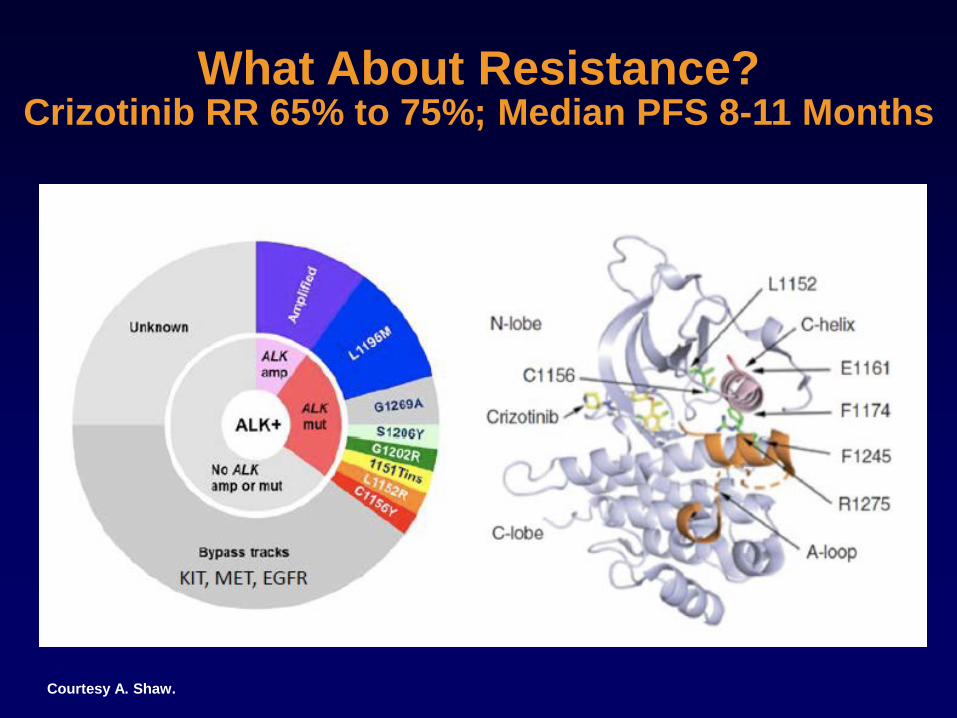
What About Resistance?Crizotinib RR 65% to 75%; Median PFS 8-11 Months
Courtesy A. Shaw.

Rebiopsy• Currently no formal recommendations
– The CAP, IASLC, and AMP guidelines are currently being revised to include the role of rebiopsy and repeat analysis in the setting of post-treatment relapse—the revisions are expected in 2016
• NCCN guidelines state consider rebiopsy if appropriate for metastatic disease
• May have utility in the future in directing treatment decisions
International Association for the Study of Lung Cancer. News: Revisions to molecular testing guideline continues to give hope to lung cancer patients. Available at: www.iaslc.org/news/revisions-molecular-testing-guideline-continues-give-hope-lung-cancer-patients. Accessed 25 October 2015. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Non-Small Cell Lung Cancer. Version 1.2016. Available at www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Accessed 29 October 2015.
AMP, Association for Molecular Pathology; CAP, College of American Pathologists; IASLC, International Association for the Study of Lung Cancer; NCCN, National Comprehensive Cancer Network

Next Generation ALK Inhibitors in Crizotinib Resistance
1. Kim D-W, et al. J Clin Oncol 2014;32(5S): Abstract 8003. 2. Ou S-H, et al. J Clin Oncol 2015;33(Suppl): Abstract 8008. 3. Camidge DR, et al. J Clin Oncol 2015;33(Suppl): Abstract 8062. 4. Shaw AT, et al. J Clin Oncol. 2015;33(Suppl): Abstract 8018.
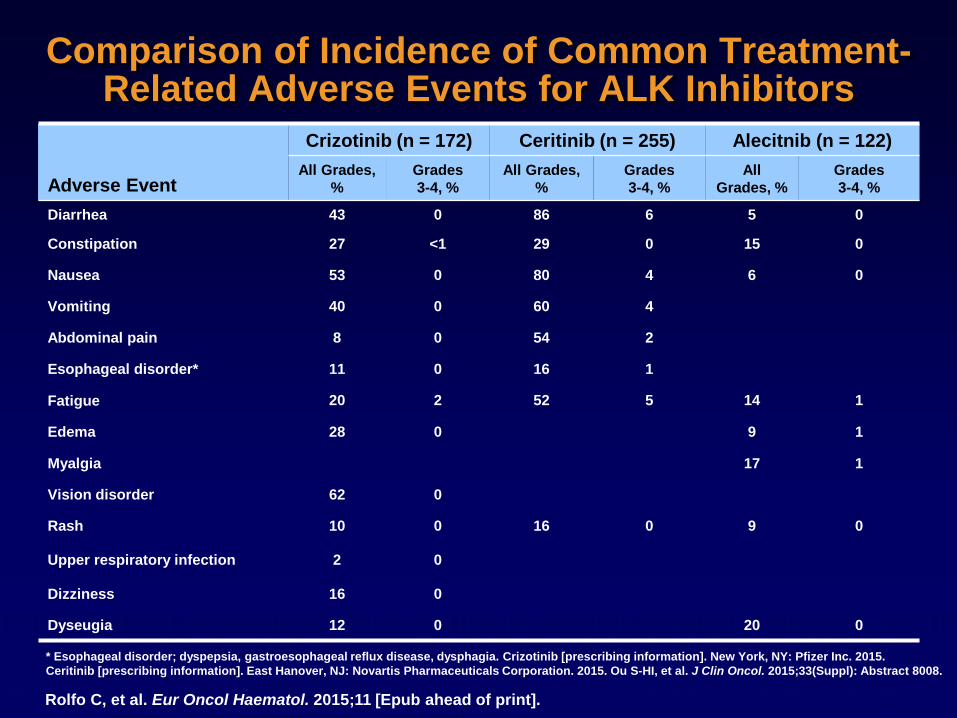
Comparison of Incidence of Common Treatment-Related Adverse Events for ALK Inhibitors
Rolfo C, et al. Eur Oncol Haematol. 2015;11 [Epub ahead of print].
Adverse Event
Crizotinib (n = 172) Ceritinib (n = 255) Alecitnib (n = 122)All Grades,
%Grades3-4, %
All Grades, %
Grades3-4, %
All Grades, %
Grades3-4, %
Diarrhea 43 0 86 6 5 0
Constipation 27 <1 29 0 15 0
Nausea 53 0 80 4 6 0
Vomiting 40 0 60 4
Abdominal pain 8 0 54 2
Esophageal disorder* 11 0 16 1
Fatigue 20 2 52 5 14 1
Edema 28 0 9 1
Myalgia 17 1
Vision disorder 62 0
Rash 10 0 16 0 9 0
Upper respiratory infection 2 0
Dizziness 16 0
Dyseugia 12 0 20 0
* Esophageal disorder; dyspepsia, gastroesophageal reflux disease, dysphagia. Crizotinib [prescribing information]. New York, NY: Pfizer Inc. 2015.Ceritinib [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. 2015. Ou S-HI, et al. J Clin Oncol. 2015;33(Suppl): Abstract 8008.

Recommendations for Management of Ceritinib-Associated Hepatocellular and
Gastrointestinal ToxicitiesLiver• Monitor liver function with monthly
Ceritinib [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. 2015.
• For severe/intolerable nausea, vomiting or diarrhea patients who are not responsive to anti-emetic/anti-diarrheals ceritinib should first be withheld until improvement and then resumed with a 150 mg dose reduction, then dose reduced
Criteria Ceritinib dosing
• ALT or AST elevation >5x ULN with• total bilirubin elevation ≤2x ULN
Withhold until recovery to baseline or less than or equal to 3X ULN, then resume ceritinibwith a 150 mg dose reduction
• ALT or AST elevation >3x ULN with• Total bilirubin elevation >2x ULN in the
absence of cholestasis or hemolysis
Permanently discontinue ceritinib
GI toxicities

Sequential Therapy of Crizotinib Followed by Ceritinib
• Multicenter, retrospective study in 73 ALK-positive patients• Patients received sequential crizotinib and ceritinib between
2008-2014• Primary endpoint of PFS• The Kaplan-Meier method was used to estimate PFS and OS
endpoints• Log-rank test used to compare differences between groups
Gainor JF, et al. Clin Cancer Res. 2015;21(12):2745-2752.

PFS
Gainor JF, et al. Clin Cancer Res. 2015;21(12):2745-2752
Crizotinib Ceritinib Following Crizotinib
• 30.4% of patients had ALK resistance mutations
• No difference seen in PFS with ceritinib between patients with or without an ALK resistance mutation
o mPFS 5.8 months versus 6.5 months, respectively; P = .510)

PFS
Gainor JF, et al. Clin Cancer Res. 2015;21(12):2745-2752.

OS
Gainor JF, et al. Clin Cancer Res. 2015;21(12):2745-2752.
OS From Time of Metastatic Disease for Overall Population
OS of ALK-Positive PatientsTreated With Second-Line Crizotinib*
* OS is measured from the start of crizotinib

Sequencing for Patients With ALK-Positive NSCLC Based on Current Paradigm
Verbal communication Tony Mok. Solomon BJ, et al. N Engl J Med. 2014;371(23):2167-2177. Gainor JF, et al. Clin Cancer Res. 2015;21(12):2745-2752. Friboulet L, et al. Cancer Discov. 2014;4(6):662-667. * Ignatius Ou SH, et al. J Thorac Oncol. 2014;9(4):549-553.
CrizotinibBased on PROFILE 1014 trial
Progression Disease
Second Generation TKI(eg, ceritinib, alectinib)
Chemotherapy?
• ALK G1202R mutation, a new aquired secondary mutation in the ALK gene who is resistant to both ceritinib and alectenib*
1st Line
Rebiopsy
No mutation ALK G1202R mutation*
2nd Line