Embed Size (px)
Citation preview

DOACs in SPECIAL POPULATIONS
Ann K Wittkowsky PharmD, CACP, FASHP, FCCP Clinical Professor
University of Washington School of Pharmacy Director, Anticoagulation Services
UWMedicine Department of Pharmacy Seattle WA USA

CONFLICTS OF INTEREST
Consultant: none Research support: none Speaker’s bureau: none Honoraria: none Ownership interest: none Other: none

OBJECTIVES
Following this presentation, the participant should be able to assess and consider the role of DOACs for treatment of VTE associated with the following conditions: 1. Antiphospholipid syndrome 2. Malignancy

CASE #1
ID: Larry F, a 63 year old male with a history of recurrent VTE in the setting of antiphospholipid syndrome (+ LA) Thrombosis history: 1) LLE DVT 1973: warfarin x 3 months 2) LLE DVT 1981: chronic warfarin, goal INR 2-3 3) RLE DVT 1982: increase goal INR to 2.5-3.5 4) RLE DVT 1990: increase goal INR to 3-4 5) LLE DVT/PE 2001: switched to CFX monitoring 6) LLE DVT 2004: switched to long term LMWH

REVISED CLASSIFICATION CRITERIA FOR ANTIPHOSPHOLIPID SYNDROME APA = at least 1 clinical criterion and 1 laboratory criterion
Miyakis S et al. J Thromb Haemost 2006; 4:295-306
VASCULAR THROMBOSIS
• 1 or more clinical episodes of arterial, venous or small vessel thrombosis
PREGNANCY MORBIDITY
• 1 or more unexplained death of normal fetus > 10 weeks gestation
• 1 or more premature delivery of normal fetus < 34 weeks gestation because of eclampsia or pre-eclampsia, or because of placental insufficiency
• 3 or more unexplained consecutive miscarriages < 10 weeks gestation
LABORATORY CRITERIA
Presence of antiphospholipid antibodies on 2 or more occasions, at least 12 weeks apart and no more than 5 years prior to clinical manifestations
• lupus anticoagulant • anticardiolipin IgG or IgM • anti-B2 glycoprotein IgG or IgM

13th International Congress on Antiphospholipid Antibodies Evidence-based recommendations for secondary thromboprophylaxis
Ruiz-Irastorza G et al. Lupus 2011; 20:206-18
Definite APS and 1st venous thrombosis
VKA with goal INR 2-3 1B
Definite APS and arterial thrombosis
VKA with goal INR > 3 OR VKA with goal INR 2-3 plus antiplatelet therapy
1C
Recurrent thrombosis or fluctuating INRs
LMWH Non-graded
VKA with goal INR > 3 VKA with CFX 35%-25%
Not included

VTE TREATMENT WITH DOACs RANDOMIZED TRIALS
DOAC ACUTE TX TRIAL
Enrolled Unprovoked VTE Known Thrombophilia DOAC Std Tx DOAC Std Tx DOAC Std Tx
Apixaban AMPLIFY 2691 2704 89.8% 89.8% 2.8% 2.2%
Dabigatran RECOVER 1273 1266 NR NR 8.2%
NR
RECOVER II 1280 1288 NR NR NR
Edoxaban HOSUKAI-VTE 4118 4122 65.9% 65.4% NR NR
Rivaroxaban EINSTEIN-DVT 1731 1718 60.9% 63% 6.2% 6.8%
EINSTEIN-PE 2419 2413 64.7% 64.3% 5.7% 5.0%
TOTAL 13,512 > 7,748 > 529
DOAC EXT TX TRIAL Enrolled Unprovoked VTE Known Thrombophilia DOAC Comp DOAC Comp DOAC Comp
Apixaban AMPLIFY-EXT 1653 829 (P) 92% 91.1% (P) NR NR
Dabigatran REMEDY 1430 1426 (W) NR NR 18.3% 18.4% (W)
Rivaroxaban EINSTEIN-EXT 602 594 (P) 73.1% 74.2% (P) 8.1% 8.1% (P)
TOTAL 3,685 > 1,961 > 311

TREATMENT OF VTE WITH DABIGATRAN IN PATIENTS WITH THROMBOPHILIA Post-hoc subgroup analysis of pooled data from RE-COVER, RE-COVER II and RE-MEDY
Goldhaber SZ et al. Vasc Med 2016; 21: 506-514.

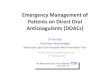
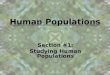
VTE CUMMULATIVE EVENT RATES IN PATIENTS WITH AND WITHOUT THROMBOPHILIA
Goldhaber SZ et al. Vasc Med 2016; 21: 506-514.
RE-COVER + RE-COVER II RE-MEDY
D 1% vs W 3% HR 0.30 95% CI 0.06 -1.51
D 1.5% vs W 2.3% HR 0.64 95% CI 0.18 - 2.27
D 3% vs W 3% HR 0.99 95% CI 0.53 - 1.84
D 2.3% vs W 0.7% HR 3.19 95% CI 0.88 -11.58

DABIGATRAN VS WARFARIN IN APS SUBGROUP Pooled data from patients with APS enrolled in RE-COVER, RE-COVER II and RE-MEDY
Goldhaber SZ et al. Vasc Med 2016; 21: 506-514.
Dabigatran Warfarin HR (95% CI) Number of patients 71 80
VTE and VTE-related deaths
3 (4.2%) 4 (5.0%) 0.43 (0.08, 2.38)
Major bleeding 1/70 (1.4%) 2/77 (2.6%) 0.46 (0.04, 5.43)
Major bleeding and Clinically relevant bleeding
6/70 (8.6%) 14/77 (18.2%) 0.53 (0.20, 1.41)
Any bleeding 14/70 (20%) 31/77 (40.3%) 0.50 (0.26, 0.95)

DOAC USE IN PATIENTS WITH APS – systematic review 6 case reports + 8 case series = 122 APS patients exposed to DOAC (107 = rivaroxaban)
Dufrost V et al Curr Rheumatol Rep 2016; 18:74-81
Patient Characteristics (n=122)
APS without recurrent thrombosis (n=103)
APS with recurrent thrombosis (n=19 [16%])
p value
Number of clinical criteria for APS
1.23 +/- 0.6 1.63 +/- 0.7 0.002
Anticardiolipin Ab 68% 94% 0.06
“triple positive” (LA + aCL+anti-B2-GP1)
22% 50% 0.03
follow-up time (suggestive of time to recurrence)
14.3 +/- 8.5 mo 5.2 +/- 3.2 mo <0.0001

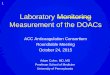
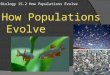
EFFECT OF WARFARIN vs RIVAROXABAN ON THROMBIN GENERATION
Arachchillage DRJ et al. Thromb Res 2015; 135:388-93
1. Thrombin generation curve
a. time to peak thrombin generation – longer for rivaroxaban b. peak thrombin generation - lower for rivaroxaban
2. Endogenous thrombin potential
c. Inhibition of endogenous thrombin potential - relatively less for rivaroxaban

EFFECT OF WARFARIN vs RIVAROXABAN ON THROMBIN GENERATION IN APS N = 116 patients with APS on warfarin (goal INR 2-3) for prior VTE at least 3 months prior Randomized 1:1 to continue warfarin or switch to rivaroxaban 20mg daily Outcome: change in endogenous thrombin potential (ETP) at day 42 Interpretation: rivaroxaban inferior to warfarin in suppressing ETP
Cohen H et al. Lancet 2016; 3:e426-36
Other parameters: time to peak thrombin generation – longer for rivaroxaban peak thrombin generation - lower for rivaroxaban recurrent VTE at day 210 – no events in either group Conclusion: “no increased thrombotic risk” with rivaroxaban

ONGOING CLINICAL TRIALS
www.clinicaltrials.gov
ASTRO-APS Apixaban for secondary prevention of VTE in patients with APS (5mg bid vs warfarin) Intermountain Healthcare/Utah NCT02295475 RAPS Rivaroxaban for APS (20mg daily) St Joseph Healthcare/Hamilton ONT NCT02116036 TRAPS Rivaroxaban for thrombotic APS (20mg daily vs warfarin) University of Pavoda/Italy NCT02157272

AUDIENCE RESPONSE QUESTION #1
Have you prescribed, recommended or managed DOACs in patients with APA? A. YES B. NO C. NOT SURE

AUDIENCE RESPONSE QUESTION #2
Would you recommend a DOAC for this patient? A. YES B. NO C. NOT SURE
ID: Larry F, a 63 year old male with a history of recurrent VTE in the setting of antiphospholipid syndrome (+ LA) Thrombosis history: 1) LLE DVT 1973: warfarin x 3 months 2) LLE DVT 1981: chronic warfarin, goal INR 2-3 3) RLE DVT 1982: increase goal INR to 2.5-3.5 4) RLE DVT 1990: increase goal INR to 3-4 5) LLE DVT/PE 2001: switched to CFX monitoring 6) LLE DVT 2004: switched to long term LMWH

CASE #2
ID: Fred G, a 73 year old male with metastatic prostate cancer, on no active treatment. RLE DVT diagnosed 10/3/16 Treatment history: 1) 10/3/16: started on rivaroxaban 15mg bid by PCP 2) 10/6/16: switched to enoxaparin 1mg/kg SQ q12h 3) 12/1/16: bruising at injection sites. “My stomach looks like a war zone. Get me off this stuff”

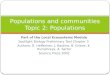
TREATMENT OF CANCER-ASSOCIATED THROMBOSIS Systematic Review and Meta-Analysis
Carrier M et al. Thromb Res 2014; 124:1214-9
Favors LMWH Favors VKA
N = 5 RCTs enrolling 1178 pts with active cancer and acute VTE Randomized to LMWH vs conventional therapy (LMWH/VKA)

Lee AY et al. N Engl J Med. 2003; 349:146-53.
N=672 patients with active cancer and acute VTE Dalteparin 200 U/kg x 1 mo then 150 U/kg daily vs conventional therapy x 6 mo
Recurrent Thrombosis
9.0% of 336
17% of 336
TREATMENT OF CANCER-ASSOCIATED THROMBOSIS The CLOT Trial

TREATMENT OF CANCER-ASSOCIATED THROMBOSIS The CATCH Trial
Lee AYY et al. JAMA 2015; 314:677-686
N=900 patients with active cancer and acute VTE Tinzaparin 175 U/kg q24h vs conventional therapy x 6 mo
7.2% of 449
10.5% of 451


LMHW FOR CANCER-ASSOCIATED VTE
• Expensive
• Burdensome - injection-site pain - injection-site bruising - injection-site hematoma • High discontinuation rates during first 3 months of therapy
Van der Wall SJ et al. J Thromb Haemost 2017; 15:74-9

VTE TREATMENT WITH DOACs RANDOMIZED TRIALS
DOAC ACUTE TX TRIAL
Enrolled Active Cancer DOAC Std Tx DOAC Std Tx
Apixaban AMPLIFY 2691 2704 81 78
Dabigatran RECOVER 1273 1266 64 57
RECOVER II 1280 1288 50 50
Edoxaban HOSUKAI-VTE 4118 4122 109 99
Rivaroxaban EINSTEIN-DVT 1731 1718 118 89
EINSTEIN-PE 2419 2413 114 109
TOTAL 13,512 521
DOAC EXT TX TRIAL Enrolled Active Cancer DOAC Comparison DOAC Comparison
Apixaban AMPLIFY-EXT 1653 829 (P) 24 18 (P)
Dabigatran REMEDY 1430 1426 (W) 60 59 (W)
Rivaroxaban EINSTEIN-EXT 602 594 (P) 28 26 (P)
TOTAL 3,685 112

APIXABAN FOR CANCER-ASSOCIATED THROMBOSIS Subgroup Analysis of AMPLIFY trial
Agnelli G. J Thromb Haemost 2015; 13:2187-91
Apixaban LMWH +VKA
HR (95% CI)
N 81 78 Recurrent VTE 3 (3.7%) 5 (6.4%) 0.56
(0.13-2.37)
Major bleeding 2 (2.3%) 4 (5%) 0.45 (0.08-2.46)
Major + clinically relevant non-major bleeding
11 (12.6%) 18 (22.5%) 0.57 (0.29-1.12)
Mortality 5 (6%) 6 (7.7%)
N = patients with active cancer at baseline

RIVAROXABAN FOR CANCER-ASSOCIATED THROMBOSIS Subgroup Analysis of EINSTEIN DVT/EINSTEIN PE
Prins HM et al. Lancet Haematol 2014; 1:e37-46
Rivaroxaban LMWH +VKA
HR (95% CI)
p value
ITT population 354 301 Safety population 353 298 Recurrent VTE 16 (5%) 20 (7%) 0.67
(0.35 – 1.30) 0.24 Major bleeding 8 (2%) 15 (5%) 0.42
(0.18 – 0.99) 0.047 Major + clinically relevant non-major bleeding
48 (14%) 49 (16%) 0.93 (0.64-1.35) 0.28
Mortality 58 (16%) 53 (18%) 0.54 (0.33-0.90) 0.70
N = patients with active cancer at baseline or diagnosed with cancer during treatment

DOACs FOR CANCER-ASSOCIATED THROMBOSIS Systematic Review and Meta-Analysis N = 1132 pts with active cancer enrolled in 4 RCTs
Carrier M et al. Thromb Res 2014; 124:1214-9
RECURRENT VTE

DOACs FOR CANCER-ASSOCIATED THROMBOSIS Systematic Review and Meta-Analysis N = 1132 pts with active cancer enrolled in 4 RCTs
Carrier M et al. Thromb Res 2014; 124:1214-9
MAJOR BLEEDING


RIVAROXABAN FOR CANCER-ASSOCIATED THROMBOSIS N = 400 consecutive patients with active cancer and acute VTE Treatment a) inpatients (75.5%): LMWH (mean = 5.6 days) then rivaroxaban at discharge b) outpatients (24.5%): rivaroxaban alone
Pignataro BS et al. Clin Appl Thromb Hemost 2016; 14-9
LMWH + rivaroxaban
Rivaroxaban alone
TOTAL
N 302 98 400 Recurrent VTE 3% 4.1% 3.25% Major bleeding 6.3% 3.2% 5.5%

RIVAROXABAN FOR CANCER-ASSOCIATED THROMBOSIS N = 296 consecutive registry patients with acute VTE treated with rivaroxaban Mean Followup = 1.36 +/- 0.5 years Minimum duration of treatment = 3 months
Bott-Kitslaar DM et al. Am J Med 2016; 129:615-9
Active malignancy
No cancer p value
N 118 178 Recurrent VTE 3.3% 2.8% 0.53 Major bleeding 2.5% 0% 0.06 Clinically relevant non-major bleeding
3.4% 0.6% 0.08
Minor bleeding 2.5% 1.7% 0.69 Death (none related to VTE) 22% 0 <0.0001

ONGOING CLINICAL TRIALS
www.clinicaltrials.gov
CANVAS DOACs vs LMWH +/- warfarin for VTE in Cancer Harvard Partners NCT02744092 CONKO-011 Rivaroxaban vs LMWH for cancer-associated VTE Charite University/Berlin and Bayer NCT02583191 COSIMO Rivaroxaban vs LMWH for cancer-associated VTE Bayer/Janssen NCT02742623

AUDIENCE RESPONSE QUESTION #3
Have you prescribed, recommended or managed DOACs during
the first 3-6 months of VTE treatment in patients with malignancy?
A. YES B. NO C. NOT SURE

AUDIENCE RESPONSE QUESTION #4
Would you recommend a DOAC for this patient? A. YES B. NO C. NOT SURE
ID: Fred G, a 73 year old male with metastatic prostate cancer, on no active treatment. RLE DVT diagnosed 10/3/16 Treatment history: 1) 10/3/16: started on rivaroxaban 15mg bid by PCP 2) 10/6/16: switched to enoxaparin 1mg/kg SQ q12h 3) 12/1/16: bruising at injection sites. “My stomach looks like a war zone. Get me off this stuff”

SUMMARY
Following this presentation, the participant should be able to assess and consider the role of DOACs for treatment of VTE associated with the following conditions: 1. Antiphospholipid syndrome 2. Malignancy