Embed Size (px)
Citation preview

SPECIALCONTRIBUTiON
chronic obstructive pulmonary disease or asthma. Thesepatients are prime candidates for dobutaminestress perfusion imaging.
Other candidates include patients who drank coffee orused medications containing theophyffine (within 12 hr),before a scheduled dipyridamoleor adenosine myocardialperfusion study. Patients who use oral dipyridamole couldattain dangerously high adenosine levels if adenosine isadministered intravenously as a pharmacologic stress;these patients are also candidates for dobutamine stresstesting. In addition, patients with heart failure who arealready receiving low-dose intravenous dobutamine forinotropicsupportare, at times, referredfor stress perfusionimaging. In these patients, it may be more reasonable toperform a dobutamine stress study by simply increasing itsdose rather than a dipyridamole or adenosine perfusionscan.
PROTOCOL
The protocol used in our laboratory(Fig. 1) begins witha low dose of dobutamine, 10 @gfkgiminfor 3 min, and isincreased to a maximum of 40 p@gfkgiminevery 3 mm (4).Thallium-20l is injected 1min afterstartingthe firstdose ofdobutamine, with the infusion maintained for another2 min. Technetium-99m-sestamibi or teboroxime may beused in place of @°‘11.The infusion is stopped andplanarorSPEC!' images are acquired, followed by delayed (or rest)image acquisition to determine radiotracer redistribution.
MECHANISM OF AC11ON
Dobutamine is a predominant beta-l agonist that increases heart rate and myocardiai contractility; at sufficiently high doses, dobutamine also increases systolicblood pressure. The increases in these three parametersresult in increased myocardial oxygen demand. Normalcoronary arteries dilate to increase perfusion in order tomeet the demand; stenotic arteries may not be able toincrease blood flow to the same degree as normal vessels,creating a perfusion defect based on a similar physiologicresponse as that triggered by exercise stress.
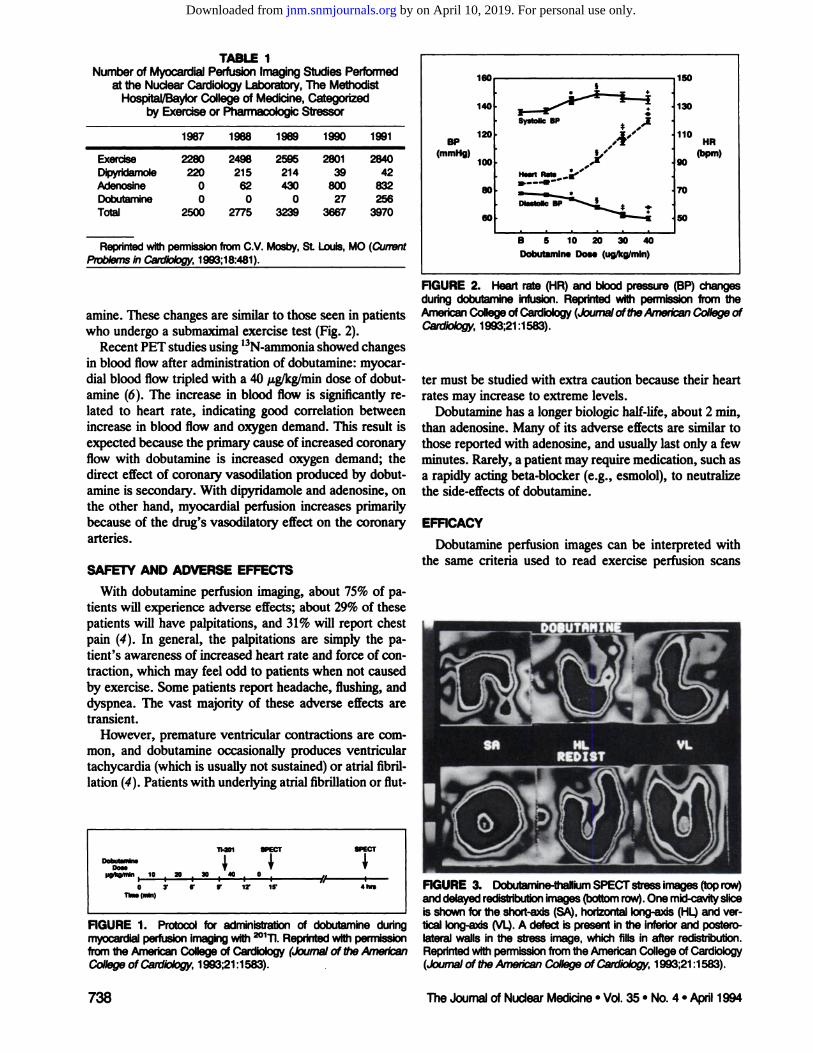
Data from a series of 144 patients indicate that an increase in heart rate is the most consistent effect of dobutamine (4). Systolic blood pressure also increases, peakingaround 20 @gfkgimin;diastolic blood pressure decreasesdue to the peripheral(beta-2) vasodilator effect of dobut
Dobutamine,a pharmacologicstressor,is usefulformyocardialperfusionimaginginpatientswhocannot exercise. Patients withasthma or severe chronic obstructive pulmonary disease whoare at riskfor adverse effectsfromeither dipyridamoleor adenosine are pnme candidatesfor dobutamineperfusionstudies.Dobutamine is a predominant beta-i agonist that increasesheart rate, myocard@cOntractilityand systolicblood pressure.The sensitivityand specificityof dobutaminemyocardialperfusion imaging are comparable, for the most part, to those fromperfusion studies using exercise, dipyndamole or adenosine.
Key Words: myocardial perfusion imaging; pharmacologicstress; dobutamine
J Nuci Med 1994; 35:737-739
ithough most patients undergo exercise stress testingto evaluate myocardial perfusion, the use of drugs thatstress the hearthave become importantin certainpatients,particularlythose who cannot exercise adequately. Thereare three pharmacologicstressors used today in cardiovascular nuclear medicine: dipyridamole (1), adenosine (2,3)and dobutamine (4).
At Baylor College of Medicine/The Methodist Hospitalin Houston, we performed3970myocardialperfusionstudies in 1991 (Table 1) (5). Most patients were stressed byexercise, althoughmore than 800 were stressed with adenosine and 42 with dipyridamoie. (At most institutions, however, dipyridamole is used more often than adenosine because it is commercially available.) Comparingour use ofpharmacologic stressors in 1991 with previous years, thereal growthwas in our use of dobutamine,which was usedfor 256 patients. Since dipyridamole and adenosine workwell and were developed before dobutamine for this indication, one might ask why we need a thirdpharmacologicstress agent.
The patients selected for dobutaminestudies were thosewho could not exercise andwho were not good candidatesfor dipyridamole or adenosine because of a history of
ReceivedJan.3, 1994;revisionacceptedJan. 17,1994.This paper was presented in part at the Annual Meeting of the Society of
NuclearMed@neon June 9, 1993,@ part of a CondrüngMedualEducation.Sen@naror@d bytheCardiovascu@rCoundi.
Forcorrespondenceor repnntscont@ MañoS. Verani,MD,Sedion of Cardk@ogy,Baybr Cdlege of Med@ne, 6536 Fannln F-905, Houston, TX 77030.
737DobutamineMyocardialPerfusionImaging•Verani
Dobutamine Myocardial Perfusion ImagingMario S. Verani
Section of Cardiology, Baylor College ofMedicine, Houston, Texas
by on April 10, 2019. For personal use only. jnm.snmjournals.org Downloaded from
Reprintedwithperm@sionfromCV. Mosby,St. Louis,MO(Ou,rentPmb@msinCairliok;gp;1993;18:481).
amine. These changes are similar to those seen in patientswho undergo a submaximal exercise test (Fig. 2).
Recent PET studies using ‘3N-ammoniashowed changesin blood flow after administrationof dobutamine:myocardial blood flow tripledwith a 40 j@tg/kg/mindose of dobutamine (6). The increase in blood flow in significantly related to heart rate, indicating good correlation betweenincrease in blood flow and oxygen demand. This result inexpected because the primary cause of increased coronaryflow with dobutamine is increased oxygen demand; thedirect effect of coronary vasodilation produced by dobutamine is secondary. With dipyridamole and adenosine, onthe other hand, myocardial perfusion increases primarilybecause of the drug's vasodilatory effect on the coronaryarteries.
SAFETY AND ADVERSE EFFECTS
With dobutamine perfusion imaging, about 75% of patients will experience adverse effects; about 29% of thesepatients will have palpitations, and 31% will report chestpain (4). In general, the palpitations are simply the patient's awareness of increased heart rate and force of contraction, which may feel odd to patients when not causedby exercise. Some patients report headache, flushing, anddyspnea. The vast majority of these adverse effects aretransient.
However, premature ventricular contractions are cornmon, and dobutamine occasionally produces ventriculartachycardia (which is usually not sustained) or atrial fibrillation (4). Patientswith underlyingatrialfibrillationor flut
,p@T
Dossi*kOlnhin,1O,@,X,@1 O@@
0 3@ S. V 12@ 1, 415*Thus(mk@)
FiGURE1. Protocolfor administrationof dobutamineduringmyocardlal perfusion imaging with @°ii.Reprinted with permissionfrom the American College of Cardiology 4kvma! of the Amerk@anCollegeof CaIdk@Iog}';1993;21:1583).
TABLE 1Numberof MyocardialPerfUsionImagingStudies Performed
at the Nudear Cardiology Laboratory, The MethodistHospital/Baylor College of Medicine, Categorized
by Exercise or Pharmacologic StressorSystolic BP
IHssrt RatS
140
120BP
(mmHg)100
60
130
110HR@pm)
60
10
50
1987 1988 1989 1990 1991
Exercise22&l2498259528012840Dipyridamole2202152143942Adenosine062430800832Dobutamine00027256Total25002775323936673970
B 5 10 20 30 40Dobutamins Dos•(ug/kg/mln)
FiGURE2. Heavtrate(HR)and bkod pressure(BP)changesdunng dobutamineinfusion.Reprintedwith permissionfrom theAmedcan College of Cardk@ogy(@kxirna!oftheAmerk@anC@ge ofCardk@k@gy;1993;21:1583).
ter must be studied with extra caution because their heartrates may increase to extreme levels.
Dobutamine has a longer biologic half-life, about 2 mm,than adenosine. Many of its adverse effects are similar tothose reportedwith adenosine, and usually last only a fewminutes. Rarely, a patient may require medication, such asa rapidly acting beta-blocker (e.g., esmolol), to neutralizethe side-effects of dobutarnine.
EFFiCACY
Dobutamine perfusion images can be interpreted withthe same criteria used to read exercise perfusion scans
FiGURE 3. Dobutan@ne-thaIkimSPECT stress images (toprow)and dalayed redistributionimages (bottomrow).One mkI-ca@ñtysliceis shown for the short-ads (SA), horizontal long-ads (HL)and vartical Iong-ads (VL).A defe@ is present in the inferiorand posterolateralwalls Inthe stress image,whichfillsin after redistribution.Reprintedwithpermissionfromthe AmericanCollegeofCardolOgy(Journal of the American College of CaitIioiogj@1993;21 :1583).
738 TheJoumal ofNudearMedicine•Vol.35. No. 4.Aptii 1994
,@, YL•DI$T
,@ c:@f@A@1
by on April 10, 2019. For personal use only. jnm.snmjournals.org Downloaded from

patientswho are not candidates for exercise, dipyridamoleor adenosine imaging.
REFERENCES
1. Borges-Neto5, MahmarianJJ,JamA, RobertsR,VeraniMS.Quantitativethallium-201singlephotonemissioncomputedtomographyafteroraldipyridamole for assessing the presence, anatomic location and severity of coronaly artery disease. lAm Coil Cardiol 1988;11:962-969.
2. VeraniMS, Mahmarianii, Hixson lB. et al. Diagnosisof coronaryarterydisease by controlledcoronaryvasodilationwith adenosineand thallium201scintigraphyinpatientsunableto exercise.Circulation1990;82:80—87.
3. Nishimura5, Mahmarianii, Boyce TM, et al. Quantitativethallium-201single-photon emission computed tomography during maximal pharmacologiccoronary vasodilationwith adenosinefor assessingcoronary arterydisease.JAm CoilCardiol 1991;18:736-745.
4. Hays iT, Mahmarianii, CochranAl, et al. Dobutaminethalhium-201tomography for evaluating patients with suspected coronary artery diseaseunable to undergoexercise or vasodilatorypharmacologictesting.I AmCoil Canliol 199321:1583-1590.
5. VeraniMS.Pharmacologicstressmyocardialperfusionimaging.CurrProbCaniiol 1993;18:481—528.
6. KrivokapichJ, HuangS-C, SchelbertHR. Assessmentof the effectsofdobutamine on myocardial blood flow and oxidative metabolism in normalhuman subjects using nitrogen-13 ammonia and carbon-li acetate. Am ICardiol 1993;71:1351—1356.
7. MabmarianJJ, Boyce TM, GoldbergRK, CocanougherMK, Roberts R,Verani MS. Quantitative exercise thallium-201 single-photon emission cornputed tomography for the enhanced diagnosis of ischemic heart disease. IA,n CoilCardiol1990;15:318—329.
8. PenneliDi, UnderwoodSR. SwantonRH, et al. Dobutaminethalliummyocardial perfusion tomography. JAm Coil Canliol 1991;18:1471—1479.
9. MarwickT, WillemartB, D'HondtAM, et al. Selectionof the optimalnonexercise stress for the evaluation of ischernic regional myocardial dysfunctionand @FcMIBI singlephoton emissioncomputed tomography.Circulation 1993;87:345-354.
10.ForsterT, McNeilAl, SalustriA, et al.Simultaneousdobutaminestressechocardiography and technetium-99rn isonitrile single-photon emissioncomputedtomographyinpatientswithsuspectedcoronaryarterydisease.IA,n Coil Cordial 1993;21:1591—1596.
(Fig. 3). With regard to quantification, it is important todevelop a normal database for dobutamine, just as withexercise, dipyridamole and exercise.
In our own series, the overall sensitivity and specificityfor dobutamine perfusion imaging are 86% and 90%,respectively, for detection of coronary artery disease(CAD) (4). These accuracy measurements are comparable to those reported from our institution for myocardialperfusion imaging with exercise (7), dipyridamole (1) oradenosine (23). Dobutamine perfusion imaging has agood sensitivity (78%)for detection of all severe (>70%)stenoses, whereas the sensitivityinlower (44%)fordetectionofmoderate (50%to 70%)stenoses. Otherinvestigatorshaverecently reported similar accuracies (8—10).
Dobutamine perfusion imaging detects CAD with higheraccuracy in patients with multivessel disease (100%in thosewith triple-vesseldisease) than in patientswith single-vesseldisease (84%) (4). In our institution, the ability to detectCAD in individual vessels with dobutamine perfusion studiesincomparableto thatofmyocardial imagingwithexercise (7)or other pharmacologicstressors (1—3).
Another recent study using dobutarnine-thalliumSPECT in 50 patients reported a sensitivity of 97% and aspecificity of 80% for detecting CAD (8). Two recent studies (9,10) using dobutamine-sestamibiimaging found sensitivities of 80%and 83%and specificities of 74%and 89%,respectively. The same studies reported sensitivities of85%and75%,respectively,forechocardiographywithdobutamine.
CONCLUSION
Myocardial perfusion imaging with dobutamine-inducedstress is a valuable tool for evaluating CAD, especially in
739DobutamineMyocardialPerfusion Imaging•Verani
by on April 10, 2019. For personal use only. jnm.snmjournals.org Downloaded from
1994;35:737-739.J Nucl Med. Mario S. Verani Dobutamine Myocardial Perfusion Imaging
http://jnm.snmjournals.org/content/35/4/737This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1994 SNMMI; all rights reserved.
by on April 10, 2019. For personal use only. jnm.snmjournals.org Downloaded from