Embed Size (px)
Citation preview

1
Documentation
TutorialDefending the Clinical Process
Advanced Institute of Rehab Services
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
1
The Challenge of Documentation
• Historically Documentation has been a struggle for therapists
• Therapists want to treat the patients and can document the progress made but have a hard time justifying their services.

2
“The Ruler”
• We are primarily judged (and denied) not based upon progress, but whether we are really a
necessary part of the process!
• Because our services are quite expensive, reviewers have every right to ask “why are you
still involved with this pt.?” every week we continue to see them.
• The ‘Good News’– we get to design “the ruler” that is used to make this judgment.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
3
How are we accountable?
• We need to demonstrate why we need to intervene?
• Demonstrate a PLOF vs. CLOF on eval
• Propose a cause of that change in function.
• Propose methods of Reintegration (R), Compensating (C) and/or Modification (M) for that change.
• Design a way to measure our progress towards R/C/M of that lost function.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
4

3
When identifying CLOF we do so by
assessing……..
• Functional Deficits (FD) and their correlating…
• Underlying Impairments (UI’s)
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
5
Why you/ Why now?
• Just about anyone can identify functional deficits. (The pt. was probably referred d/t this reason.)
• Use your skill to ID why the FD exists.
• Use your skill to ID the “pathway” to R/C/M for those FD’s.
• When designing the ruler we outline what we work on in Rx to diminish the FD’s as well as incorporate the U.I.’s for those F.D.’s.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
6

4
Designing the Ruler• Picture STG’s on the “Ruler”.
• The top side shows F.D.’s– has noted gaps for progress.
• The bottom has U.I.’s– which can be used for the measurable impacts to achieve the F.D’s (ROM, balance score, or components of swallow.
FD
UI
CG MIN MOD MAX TOTAL
5 4+ 4 4- 3+ 3 3- 2+ 2 2- 1+ 1 1-
FD
UI
REG MECH SOFT PUREE THIN LIQ NPO
AIRWAY AP BOLUS TIMELY ORAL ORAL ATTEND
PROT PROP CONTR SWALL AWARE SENS
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
7
Bottom Line: We need to show impact by:
• Measuring U.I.’s.
• Link them to F.D.’s – so relationship to FUNCTION is obvious.
• Set goals on both.
• Increase L/E strength from 4 to 4+ to improve ability to rise for transfer
• Improve transfer from mod to min assist
• Analyze both in progress updates. cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
8

5
Scope of Practice GridOCCUPATIONAL THERAPY SCOPE OF PRACTICE GRID Place severity rating in box: 1. stand by 2. Mild 3. Mod 4. Severe 5. Profound
Impact Rating on Function
Bath
ing/
S
how
ering
Bed M
obili
ty
Com
munity
A
ctivi
ties
Dre
ssin
g
Em
erg
. R
esp./
Safe
ty P
roc.
Feedin
g
Functional
Com
mun.
Gro
om
ing
/Hygie
ne
Hom
e
Managem
ent
Join
t M
obili
ty
Leis
ure
/ P
roductive
Activ.
Meal P
rep/
Cle
anup
Medic
ation
Routine
Positio
nin
g
Toile
t H
ygie
ne
U
N
D
E
R
L
Y
I
N
G
I
M
P
A
I
R
M
E
N
T
S
1. Sensory
a. sensory awareness
b. sensory processing
(1) tactile
(2) proprioceptive
(3) vestibular
(4) visual
(5) auditory
(6) gustatory
(7) olfactory
c. perceptual processing
(1) stereognosis
(2) kinesthesia
(3) pain response
(4) body scheme
(5) right - left discrimination
(6) form constancy
(7) position in space
(8) visual-closure
(9) figure ground
(10) depth perception
(11) spatial relations
(12) topographical orientation
2. Neuromusculoskeletal
a. reflex
b. range of motion
c. muscle tone
d. strength
e. endurance
f. postural control/balance
g. postural alignment
h. soft tissue integrity
i. gross coordination
j. crossing the midline
k. laterality
l. bilateral integration
m. motor control
n. praxis
o. fine coordination / dexterity
p. visual-motor integration
q. oral-motor control
r. edema
4. Cognitive Integration
a. level of arousal
b. orientation
c. recognition
d. attention span
e. initiation of activity
f. termination of activity
g. memory
h. sequencing
i. categorization
j. concept formation
k. spatial operations
l. problem solving
m. learning
n. generalization
o. safety awareness
5. Psycho/Social/Self-Expression
a. self-concept
b. role performance
c. social conduct
d. interpersonal skills
e. self-expression
f. coping skills
g. time management
h. self-control
6. Cardiorespiratory
a. breathing patterns (diaphr.)
Un
de
rlyin
g Im
pa
irme
nt
Functional Deficits
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
9
Scope of Practice(Use the tools you have)
• Scope of Practice Grids have underlying impairments for all disciplines.
• Draws the line to F.D’s.
• Have tools for OT, PT, ST just need to apply to documentation.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
10

6
Critical Elements of Documentation
• Medical Necessity
• Skilled Service
• Skilled Analysis
• Interfering factors/Prognosis
• Measurable Improvement
• Patient Stimulability
• Frequency/Duration/Intensity
• Pertinent Medical History
Medical Necessity
• What is it?
• Defines the need for skilled intervention…A change function related to recent medical history.
• Describe it?
• Links medical condition change in functional ability
• Justifies need for skilled intervention
• Explains impact to the patient
12
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es

7
Skilled Services
What is it?
• The service that we are qualified to provide because of our specialized training and license…It is our analysis and adjustments
Describe it
The observation, analysis, assessment, that results in the necessary adjustment of treatment goals, approaches and cueing strategies.
13
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
Measurable Improvement
• Deciding the criteria
• Assuring measurable gain
1. Patient potential
2. Intensity of treatment
3. Writing an objective that is attainable - do you need a bridging step?
4. What level is really needed for functional ability
14
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es

8
Measurable Progress
• Are you reporting gains week to week?
• If so, have you upgraded the program to the point that the patient has reached their best ability to function?
• If not, have you documented adjusted treatment techniques and approaches? Or…have you attempted to address a different underlying impairment that may be interfering?
SOAP Element ExampleTo write a good soap note, you need to have a plan! A consistent format reduces time spent in writing and ensures the content is complete. Here is a step
by step process to learn!!!
S. Optional information stated by resident or therapist opinion on patient attending, cooperation, tolerance of treatment etc.
O. Objective data: Initial content needs to be: # of treatment sessions/#
sessions scheduled.
“Skilled intervention included:…..” needs to be next where you
document the skill you used such as: choice of tasks; verbal cues; phonemic
prompts; modeling; analysis of strength, range, and coordination of
exercises; + reinforcement etc. (Don’t make your reviewer have to look for this!!!)
Then give the complete objectives. These need to be written either in
narrative or column style, which gives each objective’s data compared to
baseline or the previous weeks information. I believe the column style is easiest for reviewers and staff to read.
Then be sure to address all the caregiver training you conducted during that week.
A. Analysis and Assessment:
1. Deal with each functional outcome individually. For example: “Bill has
increased the safety of oral intake as evidenced by reduced coughing
and throat clearing at meals. This is due to increased tongue strength and increased ability to form a cohesive bolus” Or: ”Bill has increase
the safety and independence of ambulation as evidenced by using his
w walker as trained throughout the facility.” Or: “Bill has increased the independence of self dressing as evidenced by no longer requiring
assistance to button his shirt.”
2. Talk about the skilled interventions which had the greatest/least
impact: “ Bill’s use of double swallow and chin tuck was more
consistent requiring less verbal cues to initiate.
3. Discuss complicating factors having a negative impact in treatment
that week. (Anything from the flu to death in the family!)

9
SOAP Element Example(continued)P. Prognosis and Plan:
1. Provide a prognostic statement regarding the likelihood of therapy
success. Use you functional outcomes here!!! “Prognosis is good for
increasing the safety of Bill’s swallow due to recency of onset, patient cooperation, and progress to date.”
2. Explain the changes you intend to make to the care plan- whether it is
a change of stimuli, task, response mode or type.
3. Then explain why the skills of a therapist remain critical for this patient’s care: “ The skills of a Speech/Language Pathologist remain necessary to analyze Bill’s swallow, determine safe diet texture
modifications, train nursing on feeding techniques as they change. In addition, SLP will determine best exercises to increase quality of bolus
formation.”
4. The “P” section should also be where you indicate potential discharge time frame.
The above format maintains medical necessity by use of functional outcomes in
the objectives as addressed on the evaluation. It also maintains it by use of functional outcomes within the analysis/assessment portion of the note. Prognostic statements further support this where these are addressed again.
The above format addresses Skilled Intervention for each objective via use of
different conditions, tasks, response requirements, and timelines. This is
elaborated on in the “A” section and the “P” section with changes in the plan being documented.
The frequency and duration are justified because the clinical reasoning within
this type of note is obvious.
The R/C/M Continuum
• For each U.I.– we determine where they fit into the continuum.
• Prevention<>Reintegration<>Compensation<>Modification
Example:
Pain <> Balance/Proprioception <> Strength<> Memory
Prevention<>Restoration<>Compensation<>Adaptation
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
18

10
R/C/M Clinical Judgments(Several variable to consider)
• Consider PMH
• Past intervention they may have had
• Consider any precautions
• Assess cognition
• Consider possible D/C environment
• Consider presence of caregivers to assist in follow-through.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
19
Designing Goals
• Types of Goals
• Duration of Treatment
-Goals focus on active pt. involvement -Goals focus on positive
--Longer durations of Tx and/or on caregiver inv.
-Shorter durations of Rx.
--------------------------------------------------------------------------------
Prevention Restoration Compensation Adaptation
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
20

11
Model of Care—Reintegrate(Aligning U.I’s with sample goals)
REINTEGRATE
Emphasizes restoration
of underlying
components that
impact function
Falls/Balance—sensory
env. Stimulation, COG-sitting,
Ther ex., PREs, ROM, stretching
Improve trunk flexion
ROM for safety during LE
dressing.
Medically complex—
posture, strength, breathing
patterns, activity tolerance and
vitals for activities.
Falls/Balance—sensory
env. Stimulation, closed chain
exercises, gait training, COG
control training, Ther Ex., PREs,
ROM, stretching
Restore dynamic weight
shifting ability.
Medically Complex—
posture, resp. pattern, breath
sounds, activity tolerance, vitals
for tasks (BP, O2 sats, heart rate)
Falls/Balance—Sensory
environment stimulation
Improve problem solving
Medically Complex—
breathing pattern for
speech/swallowing, lung volume
for breath support, swallowing
Language—
receptive/expressive
Cognition—attention,
memory, problem solving,
reasoning, judgment, executive
functions.
Sample Goal
Falls/Balance
Enhance integration of
sensory input as evidenced by a
score of ___sec. on the MSIT to
allow for______.
Enhance ability to improve
COG within BOS as evidenced
by an increased score of
___inches on the Functional
Reach, so pt. can do___ w/o loss
of balance.
Pt. will be able to lock
brakes before standing 5/5 times
by using training technique to
prevent falling within 3 weeks.
Sample Goal
Chronic Disease
Pt will demonstrate
increased activity tolerance as
demonstrated by the ability to
perform lower body dressing
with min asst. and Borg PRE
score of <6/10
Pt will demonstrate
increased activity tolerance as
demonstrated by the ability to
perform a standing activity for 5
min. with a Borg PRE score of
<5/10
To increase phonation,
patient will exhibit improved
breath control as evidenced by
increased VRI score of 2/4.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
21
OT PT ST
Model of Care—Compensate(Aligning U.I.’s with sample goals)
COMPENSATE
Teaches the pt. to
compensate for
deficits. The
treatment focus is on
the functional task, not
on the underlying
component.
Falls/Balance—
Assistive devices for
ADLs.
Teach the pt visual
scanning techniques to
compensate for visual
field cut.
Falls/Balance—
Assistive devices for
ambulation.
Teach the pt. to use
a rolling walker
Assistive devices
for improving cognition—
memory book, cue cards.
Compensatory
techniques for Dysphagia,
swallowing strategies.
Establish consistent
routine appropriate for
cognitive level to
maximize safety.
Sample goal Pt will perform UB
dressing, grooming,
bathing at I level with
compensatory techniques.
Pt will ambulate 75’
with FWW with min. A of
1 to get to and from the
bathroom within 3 weeks.
Pt will use
compensatory strategy of
effortful swallow to
decrease swallow delay to
1.5 sec. and decrease risk
of aspiration 90% of the
time.
Pt will use
compensatory memory
aide to recall hip
precautions 90% of the
time to avoid re-injury.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
22
OT PT ST

12
Model of Care– Modify(aligning U.I.’s with sample goals)
MODIFYThe task and the environment
are the sources of change, not
the patient.
Environmental
modifications—
eliminating barriers—
bedside table when getting
out of bed. Contrasting
colors, lighting.
Alter colors within
bathroom for improved
safety (change-white toilet
on white floor with white
walls)
Train caregivers
Environmental
modifications—striking
colors on w/c brakes to
locate, move bedside table
to decrease risk of falling,
height of bed for transfers,
lighting.
Ask family to
purchase more supportive
shoes.
Train caregivers
Modify diet
Contrasting colors
to find room or locate
other objects in room.
Train caregiver in
how to cue pt.
Train caregivers
Sample Goal Caregiver will stack
clothing in sequence of
donning over 3
consecutive observations
to allow pt. to dress self.
Caregiver will use
designated footwear when
ambulating pt. for cares on
3 consecutive observations
for decrease risk of
falling.
Caregiver will
verbally cue pt. to tuck
chin when swallowing on
3 consecutive observations
for decreased risk of
aspiration.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
23
OT PT ST
Case Study/ Return Demonstrations
• Assessment
• Review Case Study
• Write a sample assessment
• Write sample goals STG’s and LTG’s
• Continuation of Treatment
• Write a sample visit/encounter note
24
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es

13
Quality Review Form HH EvalHOME HEALTH EVAL DOC AUDIT TOOL Therapist: Page 1
Patient: Discipline: PT ⃝ OT ⃝ ST ⃝ SOC:
Evidence of: Y N N/A Comments
Medical Hx/Dx present, supports Intervention ⃝ ⃝ ⃝
Reason for referral evident/ supports Rx ⃝ ⃝ ⃝
PLOF compared to CLOF and justifies Rx ⃝ ⃝ ⃝
Precautions/Contraindications documented ⃝ ⃝ ⃝
Vital Signs (circle) BP - HR - RR ⃝ ⃝ ⃝
Cognition- evidence of fxl deficit ⃝ ⃝ ⃝
(Orient; person, place time,circumstance, STM, LTM, PS, Reasoning, safety)
Pain documented w impact on fx ⃝ ⃝ ⃝
Homebound reason clearly documented ⃝ ⃝ ⃝
Med Changes documented ⃝ ⃝ ⃝
Safety docmented and impact on fx ⃝ ⃝ ⃝
Underlying Impair: Strength, ROM impact on fx ⃝ ⃝ ⃝
Functional Assessment Test documented ⃝ ⃝ ⃝
Skilled Gait Training (Inc. deviations, cues) ⃝ ⃝ ⃝
HEP; response and return demo documented ⃝ ⃝ ⃝
Plan of Care: Freq/Dur. # visits perf. ⃝ ⃝ ⃝
If re-assess; PLOF/CLOF is outlined and r/t fx ⃝ ⃝ ⃝
If POC update has analysis, adjustments, chng ⃝ ⃝ ⃝
If POC Update: indicates prognosis to cont ⃝ ⃝ ⃝
If POC Update: indicates remaining deficits ⃝ ⃝ ⃝
STG specific, measureable, time frame ⃝ ⃝ ⃝
STG show UI's and Fxl Deficits from eval ⃝ ⃝ ⃝
STG's are related to LTG's ⃝ ⃝ ⃝
LTG indicate end of Rx outcome ⃝ ⃝ ⃝
Visits match orders for compliance ⃝ ⃝ ⃝
Caregiver ed. and train documented w return demo ⃝ ⃝ ⃝
Missed Visits w/Document. ⃝ ⃝ ⃝
Extra Visits w/ MD Order(s) ⃝ ⃝ ⃝
Case Conferencing evidence of: ⃝ ⃝ ⃝
PT - PTA - ST - OT - OTA - RN - MSW
MD Called @ SOC ⃝ ⃝ ⃝
D/C ⃝ ⃝ ⃝
# FAT Submitted ⃝ ⃝ ⃝
Each Doc Signed & Title ⃝ ⃝ ⃝
CPT # ⃝ ⃝ ⃝
Agency Branch ⃝ ⃝ ⃝
SV Doc. w/ Conference ⃝ ⃝ ⃝
Revised 4.29.14
DATE: Reviewer: ________________________
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
25
Quality Review Form HH
Progress NoteHOME HEALTH: VISIT DOC AUDIT TOOL Therapist:
Patient: Discipline: PT ⃝ OT ⃝ ST ⃝ SOC: DOS:
Evidence of: Y N N/A Comments
Homebound reason clearly documented ⃝ ⃝ ⃝
Med Changes documented ⃝ ⃝ ⃝
Pain documented w impact on fx ⃝ ⃝ ⃝
Vital Signs (circle) BP - HR - RR ⃝ ⃝ ⃝
Objective Reporting:
Underlying Impair: Strength, ROM impact on fx ⃝ ⃝ ⃝
Missed Visits w/Document. ⃝ ⃝ ⃝
Summary of CLOF/limitations justifies Rx ⃝ ⃝ ⃝
Precautions/Contraindications documented ⃝ ⃝ ⃝
Safety docmented and impact on fx ⃝ ⃝ ⃝
Functional Assessment Test chng documented ⃝ ⃝ ⃝
Skilled Intervention
Underlying Impairments relate to fxl impact ⃝ ⃝ ⃝
Pts. response to treatment noted ⃝ ⃝ ⃝
Doc of skilled therapy; analsysis, adjustment ⃝ ⃝ ⃝
Prognosis/further gains expected and doc ⃝ ⃝ ⃝
HEP: response and return demo documeted ⃝ ⃝ ⃝
Plan of Care: Freq/Dur. # visits perf. ⃝ ⃝ ⃝
Plan changes, adaptations noted ⃝ ⃝ ⃝
Plan justified reason to continue ⃝ ⃝ ⃝
Caregiver ed. and train documented w return demo ⃝ ⃝ ⃝
Extra Visits w/ MD Order(s) ⃝ ⃝ ⃝
Communication documented: ⃝ ⃝ ⃝
PT - PTA - ST - OT - OTA - RN - MSW
Each Doc Signed & Title ⃝ ⃝ ⃝
CPT # ⃝ ⃝ ⃝
Agency Branch ⃝ ⃝ ⃝
SV Doc. w/ Conference ⃝ ⃝ ⃝
Revised 4.29.14
DATE: Reviewer: ____________________
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
26

14
Quality Review Form
SNF audit tool
Quality Review Form
SNF audit tool

15
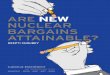
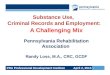
Documentation Cue Cards
(can help outline the clinical process)
• Cue cards for evaluation forms
• PLOF comparing CLOF
• Reason for referral
• Analysis and adjustment
• Prognosis to continue
• Cue cards for progress note
• PLOF comparing CLOF
• Reason for referral
• Analysis and adjustment
• Prognosis to continue
• Documentation Samples
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
29
Documentation Cue Cards--HCcA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
30
16
Documentation Cue Card- HC cont
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
31
Documentation Cue Card SNF
17
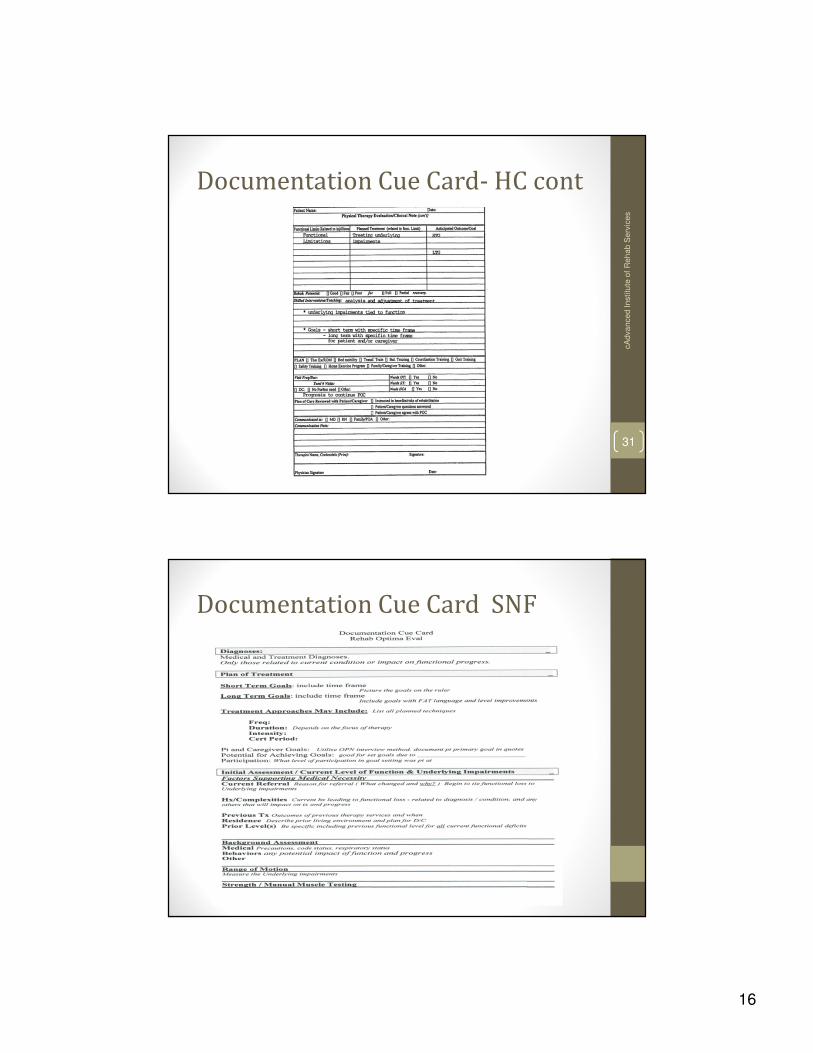
Documentation Cue Card SNF-cont
Peer Review
• Provides clinical reasoning from peer to peer• Provided unbiased review• Can meet regulatory standards• Provides didactic exchange for learning and
clinical decision making
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
34

18
Compliance Review (optional)
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
35
What is Probe Edit? And Why Are We On
It?• Probe Edits and Reviews are part of a larger process that CMS
uses to oversee the Medicare Coverage Process.
• The larger process is called PCA (progressive corrective action).
• PCA is similar to our own clinical process.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
36

19
Clinical Process VS. PCA
Clinical Purpose
Process .Monitor ID triggers that may
indicate a pt. who
needs to be
screened.
Triggers: wt. loss,
falls, poor grooming/
hygiene
____________________________________
PCA Purpose
Process___________________
Probe Edit ID triggers that may
indicate a provider
that needs to be
screened.
Possible Triggers:
ICD codes, CPT
codes, Case mix,
changes in billing
patterns.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
37
Clinical Process VS. PCA cont.
Clinical PurposeProcess .Screen Determine if
triggers are pointing to a legitimate issuethat needs to be investigated further.i.e., Brieflyassess the pt. to see if thewt. loss really indicates a swallowing problemthat may justify Rx.
PCA PurposeProcess___________________Probe Review Determine if triggers
are pointing to a
legitimate issue that
needs to be investigated further.
Possible Triggers:
i.e. Briefly assess the medical records
(via ADR process) to
see if high usage of
key indicators; Alzheimer’s ICD
code, case mix index., that can indicate
over-utilization that
may justify intervention.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
38

20
Clinical Process VS. PCA
Clinical PurposeProcess .Evaluation Intensively assess
the pt. to determine
what needs to be done in order to diminish the issue.
PCA Purpose
Process___________________Targeted Medical Intensively
assess. Reviewthe medicalrecords
(via a focused review of certain types of documentation) to
determine what exactly needs to be done in order to diminish the
issue.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
39
Clinical Process VS. PCA
Clinical PurposeProcess .Therapy ID deficits,
impairments,
and a plan of intervention.
PCA PurposeProcess___________________Corrective ID the provider’s
Action deficits,
Underlying Plan impairments
and a plan of intervention.
____________________________________
Retroactive Penalizing
Refunds, persistent
Stop offenders.
Placements, etc.
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
40

21
Summary
Build the Fire Wall…
Putting out the inferno isn’t fun!
cA
dva
nce
d In
stitu
te o
f R
eh
ab
Se
rvic
es
41