Embed Size (px)
Citation preview

Does choice of antiretroviraldrugs matter for inflammation?
Cristina Mussini


Pp prevalence was higher in cases than controls in all age strata (all p-values <0.001)
Pp prevalence seen cases aged 41-50 was similar to that observed among controls
aged 51-60 controls (p=0.282)
Poly-patology prevalence in cases and
controls, stratified by age categories
Pp 3.9% 9.0% 20.0% 46.9% Pp 0.5% 1.9% 6.6% 18.7%
Guaraldi G. et al Clin Infect Dis. 2008 ;47:250-7

HIV: chronic inflammatory disease
• Untreated HIV infection• Inflammation and activation is driven by HIV replication.
• Treated HIV infection• low-level HIV replication
• microbial translocation
• viral coinfections (eg, cytomegalovirus or HCV infection)
• comorbidities
• lifestyle factors (tobacco, alcohol use, low physical activity)

Why is chronic inflammation harmful?

HIV-associated risk factors likely amplify the same
inflammatory pathways associated with CVD in the
general population
Deeks et al NEJM 12

Treated HIV disease associated with increased
aortic inflammation (FDG-PET)
Tissue inflammation predicted by sCD163
Subramanian/Grinspoon, JAMA, 2012
HIV- HIV+

Untreated patients with undetectable viral loads (HIV controllers) had a higher carotid intima-media thickness(IMT) than the HIV-seronegative persons. Carotid IMT was comparable in the HIV controllers and untreatedHIV noncontrollers.
PY Hsue 2009

Will early ART normalize immune
function and health?

Lower But Persistently Abnormal Immune
Activation with Very Early ART (RV254)
• Thai study of HIV+ individuals dx very early during acute HIV infection
• Compared to high-risk HIV- controls and ART-suppressed HIV+ who initiated
during chronic HIV infection
Chronic HIV on ART
HIV-uninfected
Utay, CROI 2015, #47
: 12 days
: 16 days
: 18 days
Estimated Duration
of HIV Infection

10
8
6
4
2
0
Cum
ula
tive P
erc
ent
With E
vent
0 6 12 18 24 30 36 42 48 54 60
Month
Deferred ART
Immediate ART
1.8% vs 4.1% in deferred vs immediate arms experienced serious AIDS or non-
AIDS related event or death: HR = 0.43 (95% CI: 0.30 to 0.62); P < .001

START: No Difference in Cardiovascular Outcomes with Early vs. Delayed ART
START, NEJM, 2015 and Baker, CROI 2016, #41
Cardiovascular
Events(Early vs. Delayed):
HR 0.84 (0.4-1.8)
P=0.65
Small Artery Elasticity
(higher better)
Also no difference in
pulmonary fn. decline
(Base FEV1 96% pred)
(Kunisaki, EACS, 2015)

How can we measure chronicinflammation?

The biomarker most
strongly associated with
mortality risk
was IL-6, despite
HIV suppression in a cohort
of cART-treated men.


CROI 2018

CROI 2018


IL6, D-Dimer or T-cells: which best predict events or explain benefits of early ART?
Abstract 74 CROI 2018




What about antiretroviral drugs



Raltegravir leads to a faster CD4:CD8 ratio normalization


What about new strategies

39978 patients in the ART-CC collaboration followed for 15
years after starting ART

22nd International AIDS Conference; July 23-27, 2018; Amsterdam, the Netherlands


BMC Med. 2018;16:79


The effect was present at 12 months

…maintained at 24 months


Quiros-Roldan et al. BMC Infectious Diseases 2018

Could it be discontinuation of tenofovir?
Quiros-Roldan et al. BMC Infectious Diseases 2018

Maybe it could be different discontinuingabacavir ?
Quiros-Roldan et al. BMC Infectious Diseases 2018

Why does it happen?

A. Chéret Lancet Infect Dis 2015
At month 24, HIV-DNA loads were similar between groups (2·35
[IQR 2·05–2·50] log10 per 106 PBMC in the intensive cART
group vs 2·25 [1·71–2·55] in the standard cART group; p=0·21).

JAC 2010

Fletcher et al., PNAS 2104
Compared with concentrationsin PBMCs, the IC concentration
of TFV-DB, FTC-TP, ATV, DRV and EFV was lower in
the lymphatic tissue (LT) compartment, particularly in the
lymph node.
714 determinations of ARV drug concentrations in plasmaand 592 analyte determinations for IC drug concentrationsin PBMCs and in mononuclear cells (MNCs) from the LN,ileum, and rectum were performed.

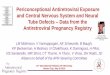
PK of INSTIs in Lymphoid Tissue
In lymph nodes, only EVG/COBI achieved a median IQ > 1
Evaluation of INSTI levels in lymph nodes (LN) in HIV+ participants administered DTG (n=11), EVG/COBI (n=17), or RAL (n=6) with NRTIs
Fletcher C, et al. CROI 2018. Boston, MA. Oral 27
44
Lymph Node Inhibitory Quotient (IQ)
DTG, dolutegravir; EVG/COBI, elvitegravir/cobicistat; pbIC90, protein-binding corrected 90% inhibitory concentration; RAL, raltegravir
1.50
0.430.28
5
4
3
2
1
0LN
In
tra
ce
llula
r C
on
ce
ntr
atio
n:
pbIC
90
Ratio
DTG EVG RAL
‡
• LN and gut-associated lymphoid tissue are the principal sites of HIV replication and where the latent pool of virus is maintained
Further studies are needed to determine whether lower concentrations create conditions that allow persistent viral production
Samples analyzed• DTG: 13/17• EVG/COBI: 19/25• RAL: 4/6

Conclusions
Inflammation is one of the main cause of SNAEs.
Concerning inflammatory biomarkers, CD4:CD8 ratio seems to be the easiest to be performed in clinical practice.
There are not definitive data to indicate that one drug is better than the other.
We still lack a lot of data on what is going on in PLWHIV in tissues different than blood, thus new strategies should be adopted with caution.