Embed Size (px)
Citation preview
Dosage patterns of antipsychotic drugs forthe treatment of schizophrenia in Swedishambulatory clinical practice �/ a highlyindividualized therapyKERSTIN BINGEFORS, DAG ISACSON, EVA LINDSTROM*
Bingefors K, Isacson D, Lindstrom E. Dosage patterns of antipsychotic drugs for the treatmentof schizophrenia in Swedish ambulatory clinical practice �/ a highly individualized therapy. NordJ Psychiatry 2003;57:263�/269. Oslo. ISSN 0803-9488.
Objective: To analyse the dosage pattern of antipsychotic drugs for schizophrenia in ambulatorycare in Sweden. Method: The study was based on a nationwide consecutive weekly randomsample of physicians during the period 1991�/98 comprising 265,331 visits. Results: In 515 visits(0.19%), antipsychotics were prescribed for schizophrenia. More than one antipsychotic (50different combinations) was prescribed in 20% of the visits. Patients received higher total dailydoses when prescribed more than one antipsychotic drug; mean dose in monotherapy was 210.7chlorpromazine equivalents (CPZeq) and in polytherapy 406.8 CPZeq. Conclusion: Antipsy-chotics, in contrast to current recommendations, were prescribed as highly individualizedtherapies in a wide variety of doses and with a high frequency of polypharmacy. Thecombinations used are often unsuitable and may lead to unnecessary adverse effects.� Antipsychotics, Polypharmacy, Pharmacoepidemiology, Prescribing, Schizophrenia.
Kerstin Bingefors, M.Sc., Ph.D., Departments of Neuroscience, Psychiatry, and Pharmacy,Uppsala University, Biomedical Centre, Box 580, SE-751 23 Uppsala, Sweden, E-mail:[email protected]; Accepted 26 March 2002.
Recently, the discussion on antipsychotic drug treat-
ment of schizophrenia in clinical practice has been
intensified in the light of studies showing poor con-
cordance with recommendations for achieving optimal
therapeutic effectiveness with as few adverse effects as
possible (1�/6).
Antipsychotic drug treatment is one of the corner-
stones in the treatment of patients with schizophrenia.
The first report published on the efficacy of neuroleptics
in the schizophrenic syndrome was published by Delay
& Deniker in 1952 (7) and even today, the most effective
treatment for schizophrenia is symptomatic and involves
the use of antipsychotic drugs. The efficacy of anti-
psychotic drugs in treatment of schizophrenia and
schizophrenia-like psychosis is well documented. How-
ever, antipsychotic drugs have also caused serious side-
effects including tardive dyskinesia (8).
Discussions concerning dose regimes have continued
since 1955, when the benefit of high-dose therapy,
‘‘neuroleptization’’ was presented (9). Others considered
that high doses were no more effective than moderate
doses, i.e. daily doses of about 400�/600 mg chlorpro-
mazine (10). The dangers of excessive dosing �/ more
side-effects, sedation and sudden death �/ have been
discussed in the literature since the early 1980s (11�/14).
Higher doses of neuroleptics have also been demon-
strated to worsen cognitive function (15). The majority
of studies with haloperidol show that there is no
advantage in exceeding standard doses (1, 2, 16).
Polypharmacy, i.e. the concomitant use of two or more
antipsychotics, is considered to increase adverse effects
due to higher total doses (17) and/or unpredictable
interaction effects.
Recommended, evidence-based use of antipsychotic
drugs in Sweden today, according to the Swedish
Council on Technology Assessment in Medicine (SBU)
(18), is for patients with severe psychosis only. Moreover,
when prescribing antipsychotic drugs to individuals with
a severe psychotic disorder, monotherapy is strongly
* Declaration of interest: Associate professor EvaLindstrom is the Swedish editor of the Nordic Journal ofPsychiatry.
# 2003 Taylor & Francis DOI: 10.108008039480310002066
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
ifor
nia
Irvi
ne o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

recommended. The dose prescribed should be the lowest
effective dose. The recommendations have been widelycommunicated to physicians.
Costs for antipsychotic treatment are rising with the
introduction of new drugs. In 1991, the total sales of
neuroleptic drugs in Sweden amounted to 178 million
SEK (1 GBP�/15.2 SEK 2001); in 1997, total sales had
increased to 251 million SEK, and in 2000 to 332 million
SEK (19, 20). It has been estimated that only two-thirds
of the sales is spent on antipsychotics prescribed topatients with a psychotic disorder, the rest (one-third) is
spent on antipsychotics given to patients with non-
psychotic disorders (21). Costs for antipsychotics to
psychotic patients in hospital treatment did not increase
during the period. The entire cost increase can be
attributed to sales in ambulatory care.
As mentioned, studies from various countries have
shown that dosage regimens of particularly conventionalantipsychotics often are in excess of guidelines and that
patients receive combination therapy with more than
one antipsychotic (4, 22�/27). However, these studies are
often performed on selected patient groups from hospi-
tals, specified clinics, or insurance populations.
Recommendations are clear, but there are indications
that concordance in clinical practice is low. Therefore,
the aim of the present investigation was to study theprescription pattern of antipsychotic drugs for schizo-
phrenic patients in ambulatory care in Sweden with
respect to daily dose, type of antipsychotic drug, and the
use of monotherapy vs. combined therapies.
Material and MethodsThe Diagnosis and Therapy study is a nationwide study
of prescribing in Sweden (9 million inhabitants). A
consecutive random sample of all doctors each partici-
pate during 1 week. A copy of the prescription form
given to the patient provides information on the drug
prescribed, and certain patient and doctor characteris-tics. The reporting form also requires the physician to
state the diagnosis that led to the prescription. Partici-
pation is voluntary and 65�/70% of selected physicians
participated in the study until 1998; the participation
rate has since decreased considerably. The survey is
carried out in collaborations with the Swedish Medical
Association, the Medical Products Agency, Swedish
Pharmaceutical Data Inc., and the National Corpora-tion of Swedish Pharmacies (28). Due to the decreased
participation rate, the present study used information
collected from 1 April 1991 to 31 March 1998.
In the Diagnosis and Therapy Survey, diagnoses are
classified according to the Swedish version of the
International Classification of Diseases, 9th version
(ICD-9) (29). Medications prescribed are classified
according to the Anatomical-Therapeutical Classifica-tion (ATC) system recommended by the WHO (30). In
Sweden, a prescription can enable the patient to receive
drugs for up to 3 months, with an option to give up to 11repeats (before 1 January 1997) or three repeats (after 1
January 1997) covering drug use for a total of 1 year at
the same visit.
The database is based on individual prescriptions.
Since one patient may get two or more prescriptions in
one visit, we transformed the material into a visit-based
format where all prescriptions issued for antipsychotics
in one visit were summed up. Oral depot neurolepticswere analysed separately since the prescribed dose is not
given in the register. In these cases, the theoretical dose
made available for the patient was calculated from the
amount of drug prescribed. Unfortunately, we were not
able to calculate reliable doses prescribed for injectable
depot neuroleptics.
Statistical methodsAll statistical analyses were performed using the SAS
statistical analysis system (SAS Institute Inc., 1987). The
mean doses for each antipsychotic prescribed was
calculated using the daily dose prescribed by the
physician. The daily doses prescribed were also trans-
formed into chlorpromazine equivalents (CPZeq) (20).
Significance in differences between means was tested
using the t-test; when variances were unequal, theCochran approximation was employed.
ResultsDuring the study period 1990�/98, 265,331 patient-visitswere registered in the Diagnosis-Therapy Study. The
number of visits was higher during the start than during
the end of the study period, a mean of 38,000 visits
approximately the first 2 years compared with a mean of
27,000 visits approximately the last 2 years. At 515 visits
(0.19%), antipsychotic drugs were prescribed to patients
diagnosed as schizophrenics. Thus, the antipsychotic-
treated group consisted of 515 patients, diagnosed asschizophrenics according to ICD-9. The sex and age
distribution is shown in Table 1. The proportion of visits
due to schizophrenia, when antipsychotics were pre-
scribed, decreased during the study period, from 0.22%
in the first half of the study to 0.17% during the second
half of the study.
In total, 653 prescriptions for antipsychotics were
issued for the 515 patients with a diagnosis of schizo-phrenia. The majority of prescriptions for antipsychotics
(82.9%) were issued by psychiatrists. However, 6.4% of
the prescriptions were issued by specialists in internal
medicine, 4.3% by general practitioners (GPs) and 5.2%
by doctors in training (Table 1). The prescription
pattern, with respect to chemical compounds, changed
during the study period. In the first 2 years, 55.3% of the
prescriptions were for phenthiazines, compared with34,3% during the last 2 years. The prescribing of
K BINGEFORS ET AL.
264 NORD J PSYCHIATRY �VOL 57 �NO 4 � 2003
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
ifor
nia
Irvi
ne o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.
butyrophenones and thioxanthenes also decreased, from
10.6% to 4.9% and from 22.1% to 18.3%, respectively.
There was an increase in the prescribing of clozapine,
from 5.5% to 23.0%. Risperidone was prescribed in
13.9% of visits during the last period.
In 421/515 visits, one antipsychotic drug was pre-
scribed; in 81 visits, two different antipsychotics were
prescribed; in 12 visits, three different antipsychotics;
and in one visit, four different antipsychotics. Since it
was not possible to calculate a mean daily dose for
patients on depot medication, these were excluded.
Separate analyses were carried out for antipsychotic
drugs prescribed as monotherapy and for drugs pre-
scribed as combination therapy. After the exclusion of
depot preparations, 353 visits with monotherapy (Table2) and 66 visits with polytherapy (Table 3) remained. In
19 visits with polytherapy, a depot preparation was one
of the drugs prescribed.
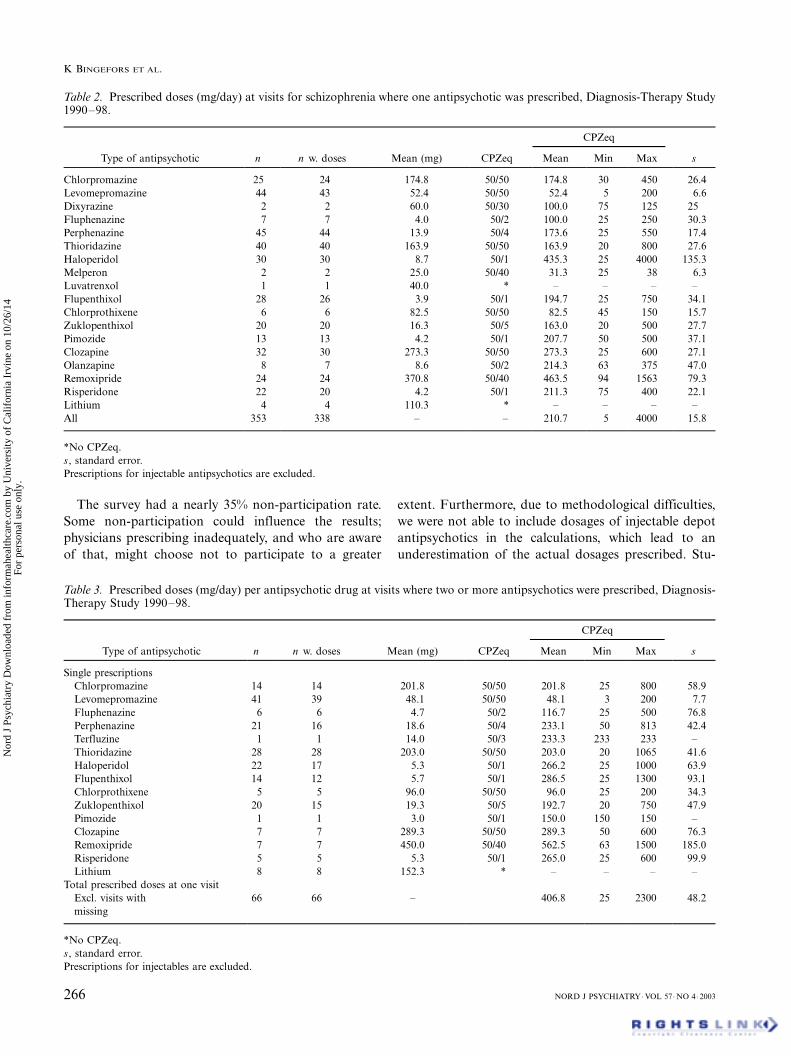
Table 2 shows the mean daily dose (mg/day and
CPZeq) for each drug at visits where monotherapy was
prescribed. There were large variations in dosage be-
tween different drugs; the mean daily dose was 210.7
CPZeq.Table 3 shows the mean daily dose (mg/day for each
substance and CPZeq) for each drug prescribed in visits
where two or more antipsychotic drugs were prescribed
at the same time and to the same patient. There was no
significant difference between the mean dose in patients
with monotherapy or combination therapy with respect
to mean dose for each substance. However, the mean
total daily dose in combination therapy, 406.8 CPZeq,was considerably higher than in monotherapy.
Further linear regression analyses (not shown) showed
that patient gender and age significantly influenced the
dose prescribed. Men received higher average doses (�/
66.5 CPZeq, P�/0.011) and doses decreased by age (�/
2.1 CPZeq/year, P�/0.028).
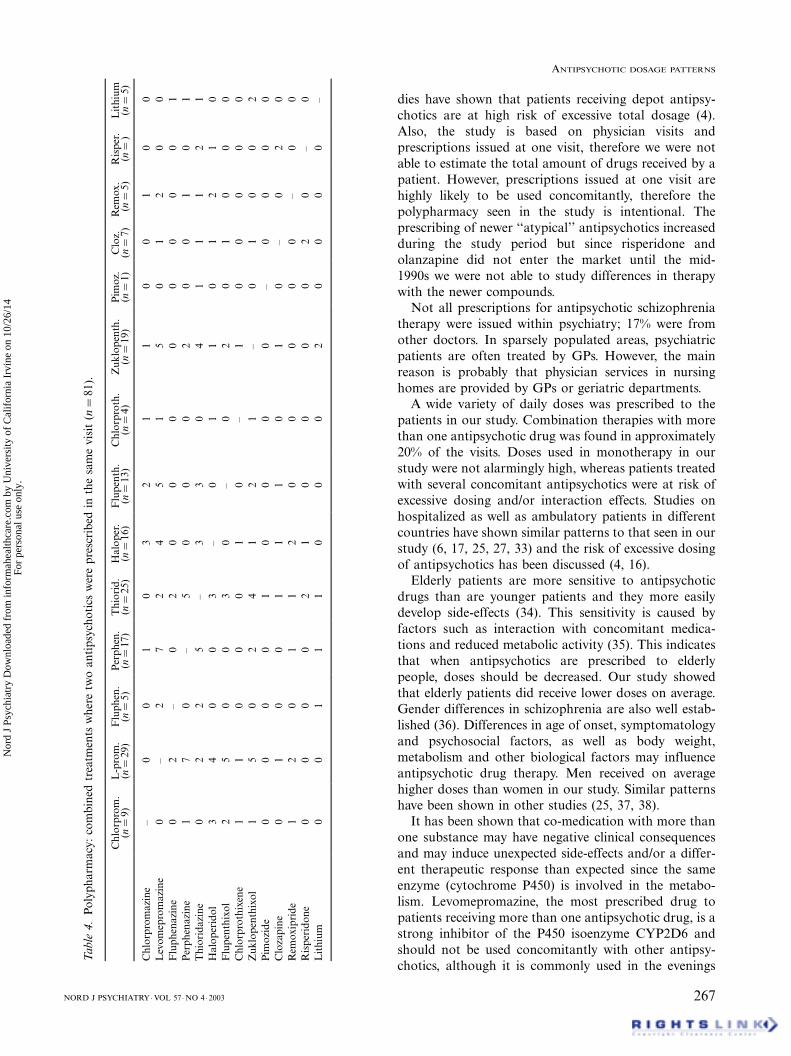
In all, 16 different substances were prescribed in 50
different combinations. At visits when more than oneantipsychotic drug were prescribed, two different anti-
psychotics were prescribed at 81 visits, three different
antipsychotics at 12 visits, and four different antipsy-
chotics at one visit. The combinations used in therapy
with two antipsychotics are shown in Table 4. The most
prescribed antipsychotic drugs in combination therapy
(with another antipsychotic drug) was levomeproma-
zine, 43.6%, followed by thioridazine, 29.8%, haloper-idol, 23.4%, perphenazine, 22.3% and zuklopenthixol,
22.3%.
DiscussionThe present study showed that antipsychotic drugs, in
contrast to current recommendations, are prescribed as
highly individualized therapies in a wide variety of doses
and with a high frequency of polypharmacy in ambula-
tory care in Sweden. In discussing the results, it is
important to emphasize that this study is based on
maintenance treatment in ambulatory care only.The prescription has been called the final common
pathway in therapeutic decision making (31). It has also
been shown that prescribing is influenced by several
non-medical factors, such as physician prescribing
habits, type of practice and patient load (32). The
main advantage of our study is that it covers a
consecutive nationwide sample of prescribers and thus
does not reflect local variations, which are relativelypronounced in Sweden (20).
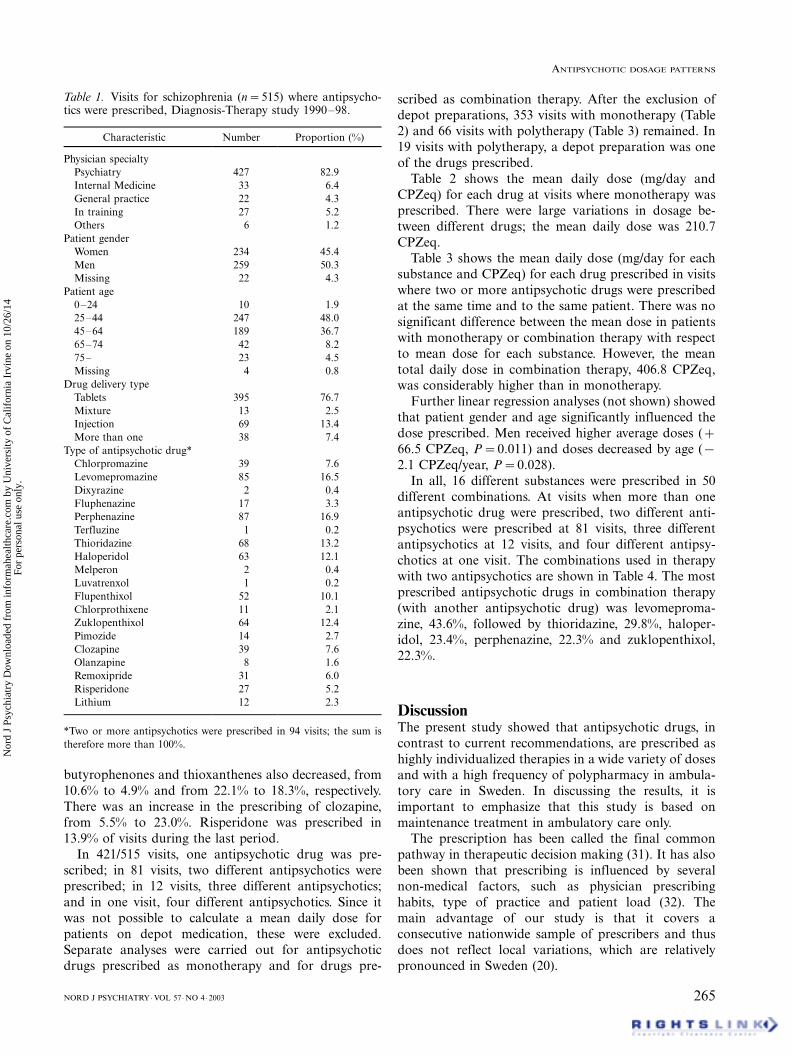
Table 1. Visits for schizophrenia (n�/515) where antipsycho-tics were prescribed, Diagnosis-Therapy study 1990�/98.
Characteristic Number Proportion (%)
Physician specialty
Psychiatry 427 82.9
Internal Medicine 33 6.4
General practice 22 4.3
In training 27 5.2
Others 6 1.2
Patient gender
Women 234 45.4
Men 259 50.3
Missing 22 4.3
Patient age
0�/24 10 1.9
25�/44 247 48.0
45�/64 189 36.7
65�/74 42 8.2
75�/ 23 4.5
Missing 4 0.8
Drug delivery type
Tablets 395 76.7
Mixture 13 2.5
Injection 69 13.4
More than one 38 7.4
Type of antipsychotic drug*
Chlorpromazine 39 7.6
Levomepromazine 85 16.5
Dixyrazine 2 0.4
Fluphenazine 17 3.3
Perphenazine 87 16.9
Terfluzine 1 0.2
Thioridazine 68 13.2
Haloperidol 63 12.1
Melperon 2 0.4
Luvatrenxol 1 0.2
Flupenthixol 52 10.1
Chlorprothixene 11 2.1
Zuklopenthixol 64 12.4
Pimozide 14 2.7
Clozapine 39 7.6
Olanzapine 8 1.6
Remoxipride 31 6.0
Risperidone 27 5.2
Lithium 12 2.3
*Two or more antipsychotics were prescribed in 94 visits; the sum is
therefore more than 100%.
ANTIPSYCHOTIC DOSAGE PATTERNS
NORD J PSYCHIATRY �VOL 57 �NO 4 � 2003 265
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
ifor
nia
Irvi
ne o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.
The survey had a nearly 35% non-participation rate.
Some non-participation could influence the results;
physicians prescribing inadequately, and who are aware
of that, might choose not to participate to a greater
extent. Furthermore, due to methodological difficulties,
we were not able to include dosages of injectable depot
antipsychotics in the calculations, which lead to an
underestimation of the actual dosages prescribed. Stu-
Table 2. Prescribed doses (mg/day) at visits for schizophrenia where one antipsychotic was prescribed, Diagnosis-Therapy Study1990�/98.
CPZeq
Type of antipsychotic n n w. doses Mean (mg) CPZeq Mean Min Max s
Chlorpromazine 25 24 174.8 50/50 174.8 30 450 26.4
Levomepromazine 44 43 52.4 50/50 52.4 5 200 6.6
Dixyrazine 2 2 60.0 50/30 100.0 75 125 25
Fluphenazine 7 7 4.0 50/2 100.0 25 250 30.3
Perphenazine 45 44 13.9 50/4 173.6 25 550 17.4
Thioridazine 40 40 163.9 50/50 163.9 20 800 27.6
Haloperidol 30 30 8.7 50/1 435.3 25 4000 135.3
Melperon 2 2 25.0 50/40 31.3 25 38 6.3
Luvatrenxol 1 1 40.0 * �/ �/ �/ �/
Flupenthixol 28 26 3.9 50/1 194.7 25 750 34.1
Chlorprothixene 6 6 82.5 50/50 82.5 45 150 15.7
Zuklopenthixol 20 20 16.3 50/5 163.0 20 500 27.7
Pimozide 13 13 4.2 50/1 207.7 50 500 37.1
Clozapine 32 30 273.3 50/50 273.3 25 600 27.1
Olanzapine 8 7 8.6 50/2 214.3 63 375 47.0
Remoxipride 24 24 370.8 50/40 463.5 94 1563 79.3
Risperidone 22 20 4.2 50/1 211.3 75 400 22.1
Lithium 4 4 110.3 * �/ �/ �/ �/
All 353 338 �/ �/ 210.7 5 4000 15.8
*No CPZeq.
s, standard error.
Prescriptions for injectable antipsychotics are excluded.
Table 3. Prescribed doses (mg/day) per antipsychotic drug at visits where two or more antipsychotics were prescribed, Diagnosis-Therapy Study 1990�/98.
CPZeq
Type of antipsychotic n n w. doses Mean (mg) CPZeq Mean Min Max s
Single prescriptions
Chlorpromazine 14 14 201.8 50/50 201.8 25 800 58.9
Levomepromazine 41 39 48.1 50/50 48.1 3 200 7.7
Fluphenazine 6 6 4.7 50/2 116.7 25 500 76.8
Perphenazine 21 16 18.6 50/4 233.1 50 813 42.4
Terfluzine 1 1 14.0 50/3 233.3 233 233 �/
Thioridazine 28 28 203.0 50/50 203.0 20 1065 41.6
Haloperidol 22 17 5.3 50/1 266.2 25 1000 63.9
Flupenthixol 14 12 5.7 50/1 286.5 25 1300 93.1
Chlorprothixene 5 5 96.0 50/50 96.0 25 200 34.3
Zuklopenthixol 20 15 19.3 50/5 192.7 20 750 47.9
Pimozide 1 1 3.0 50/1 150.0 150 150 �/
Clozapine 7 7 289.3 50/50 289.3 50 600 76.3
Remoxipride 7 7 450.0 50/40 562.5 63 1500 185.0
Risperidone 5 5 5.3 50/1 265.0 25 600 99.9
Lithium 8 8 152.3 * �/ �/ �/ �/
Total prescribed doses at one visit
Excl. visits with 66 66 �/ 406.8 25 2300 48.2
missing
*No CPZeq.
s, standard error.
Prescriptions for injectables are excluded.
K BINGEFORS ET AL.
266 NORD J PSYCHIATRY �VOL 57 �NO 4 � 2003
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
ifor
nia
Irvi
ne o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.
dies have shown that patients receiving depot antipsy-
chotics are at high risk of excessive total dosage (4).
Also, the study is based on physician visits and
prescriptions issued at one visit, therefore we were not
able to estimate the total amount of drugs received by a
patient. However, prescriptions issued at one visit are
highly likely to be used concomitantly, therefore the
polypharmacy seen in the study is intentional. The
prescribing of newer ‘‘atypical’’ antipsychotics increased
during the study period but since risperidone and
olanzapine did not enter the market until the mid-
1990s we were not able to study differences in therapy
with the newer compounds.
Not all prescriptions for antipsychotic schizophrenia
therapy were issued within psychiatry; 17% were from
other doctors. In sparsely populated areas, psychiatric
patients are often treated by GPs. However, the main
reason is probably that physician services in nursing
homes are provided by GPs or geriatric departments.
A wide variety of daily doses was prescribed to the
patients in our study. Combination therapies with more
than one antipsychotic drug was found in approximately
20% of the visits. Doses used in monotherapy in our
study were not alarmingly high, whereas patients treated
with several concomitant antipsychotics were at risk of
excessive dosing and/or interaction effects. Studies on
hospitalized as well as ambulatory patients in different
countries have shown similar patterns to that seen in our
study (6, 17, 25, 27, 33) and the risk of excessive dosing
of antipsychotics has been discussed (4, 16).
Elderly patients are more sensitive to antipsychotic
drugs than are younger patients and they more easily
develop side-effects (34). This sensitivity is caused by
factors such as interaction with concomitant medica-
tions and reduced metabolic activity (35). This indicates
that when antipsychotics are prescribed to elderly
people, doses should be decreased. Our study showed
that elderly patients did receive lower doses on average.
Gender differences in schizophrenia are also well estab-
lished (36). Differences in age of onset, symptomatology
and psychosocial factors, as well as body weight,
metabolism and other biological factors may influence
antipsychotic drug therapy. Men received on average
higher doses than women in our study. Similar patterns
have been shown in other studies (25, 37, 38).
It has been shown that co-medication with more than
one substance may have negative clinical consequences
and may induce unexpected side-effects and/or a differ-
ent therapeutic response than expected since the same
enzyme (cytochrome P450) is involved in the metabo-
lism. Levomepromazine, the most prescribed drug to
patients receiving more than one antipsychotic drug, is a
strong inhibitor of the P450 isoenzyme CYP2D6 and
should not be used concomitantly with other antipsy-
chotics, although it is commonly used in the evenings
Ta
ble
4.
Po
lyp
ha
rma
cy:
com
bin
edtr
eatm
ents
wh
ere
two
an
tip
sych
oti
csw
ere
pre
scri
bed
inth
esa
me
vis
it(n�
/81
).
Ch
lorp
rom
.L
-pro
m.
Flu
ph
en.
Per
ph
en.
Th
iori
d.
Ha
lop
er.
Flu
pen
th.
Ch
lorp
roth
.Z
uk
lop
enth
.P
imo
z.C
loz.
Rem
ox
.R
isp
er.
Lit
hiu
m(n�
/9)
(n�
/29
)(n�
/5)
(n�
/17
)(n�
/25
)(n�
/16
)(n�
/13
)(n�
/4)
(n�
/19
)(n�
/1)
(n�
/7)
(n�
/5)
(n�
/)(n�
/5)
Ch
lorp
rom
azi
ne
�/0
01
03
21
10
01
00
Lev
om
epro
ma
zin
e0
� /2
72
45
15
01
20
0
Flu
ph
ena
zin
e0
2�/
02
00
00
00
00
1
Per
ph
ena
zin
e1
70
� /5
00
02
00
10
1
Th
iori
dazi
ne
02
25
� /3
30
41
11
21
Ha
lop
erid
ol
34
00
3� /
01
10
12
10
Flu
pen
thix
ol
25
00
30
�/0
20
10
00
Ch
lorp
roth
ixen
e1
10
00
10
� /1
00
00
0
Zu
klo
pen
thix
ol
15
02
41
21
� /0
10
02
Pim
ozi
de
00
00
10
00
0� /
00
00
Clo
zap
ine
01
00
11
10
10
�/0
20
Rem
ox
ipri
de
12
01
12
00
00
0� /
00
Ris
per
ido
ne
00
00
21
00
00
20
�/0
Lit
hiu
m0
01
11
00
02
00
00
�/
ANTIPSYCHOTIC DOSAGE PATTERNS
NORD J PSYCHIATRY �VOL 57 �NO 4 � 2003 267
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
ifor
nia
Irvi
ne o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

due to its sedative effects. Thioridazine, haloperidol,
perphenazine and zuklopenthixol, also commonly pre-scribed during co-medication, are all metabolized by the
same P450 isoenzyme (39).
Polypharmacy in general is associated with a high risk
of hospitalization due to adverse effects of the drug
treatment, particularly among older patients (40) and
has been shown to be associated with reduced survival in
schizophrenia (41). As mentioned earlier, research has
shown that an optimal antipsychotic effect of antipsy-chotics may be achieved at lower doses than earlier
recommended (42). High doses of antipsychotics and/or
interaction effects have been shown to lead to con-
sequences in several areas such as negative subjective
cognitive effects (15), and increased side-effects with
subsequent non-compliance and relapse (43). Sudden
death in connection with high doses of antipsychotics
has been reported repeatedly (5, 13, 16, 44, 45).
ConclusionAntipsychotic treatment of schizophrenia in ambulatory
care is still a highly individualized therapy. The large
variations in prescribing for schizophrenia patients in
ambulatory care, particularly the high frequency of
combination therapies seen in this study, as well as in
others, are causes for concern and are not based on
scientific evidence. In spite of more than a decade ofprofessional debate on high-dose therapy and polyphar-
macy, and widespread communication of the current,
clear guidelines, there seems to be a lack of desired effect
on prescribing in actual clinical practice.
References1. McEvoy J, Haughty G, Steingard S. Optimal dose of neuroleptic in
acute schizophrenia: a controlled study of the neuroleptic thresh-old and higher haloperidol dose. Arch Gen Psychiatry1991;48:739�/45.
2. Muller R, Kissling W, Kockott G. ‘‘Weniger ist mehr’’: Eineretrospektive Untersuchung der Haloperidoldosierungen bei akuterkrankten schizophrenen Patienten. Psychiatr Prax 2000;27:69�/
73.3. Young A, Sullivan G, Burnam M, Brook R. Measuring the quality
of outpatient treatment for schizophrenia. Arch Gen Psychiatry1998;57(Suppl 12B):1�/58.
4. Walkup J, McAlpine D, Olfson M, Labay L, Boyer C, Hansell S.Patients with schizophrenia at risk for excessive antipsychoticdosing. J Clin Psychiatry 2000;61:344�/8.
5. Appleby L, Thomas S, Ferrier N, Lewis G, Shaw J, Amos T.Sudden unexplained death in psychiatric inpatients. Br J Psychiatry2000;176:405�/6.
6. Procyshyn R, Kennedy N, Tse G, Thompson B. Antipsychoticpolypharmacy: a survey of discharge prescriptions from a tertiarycare institution. Can J Psychiatry 2001;46:334�/9.
7. Delay J, Deniker P, Harl J-M. Utilisation en therapeutiquepsychiatrique d?une phenothiazine d?action centrale elective. AnnMed Psychol 1952;110:112�/31.
8. Jeste D, Caliguri M. Tardive dyskinesia. Schizophr Bull1993;19:303�/15.
9. Kinross-Wright J. The intensive chlorpromazine treatment ofschizophrenia. Psychiatry Res 1955;1:53�/62.
10. Ayd FJ. Large doses of chlorpromazine in the treatment ofpsychiatric patients. Dis Nerv Syst 1955;16:146�/9.
11. Bjorndal N, Bjerre M, Gerlach J, Kristjansen P, Mabelund G,Oestrich I, et al. High dosage haloperidol therapy in chronicschizophrenic patients: a double-blind study of clinical response,side effects, serum haloperidol, and serum prolactin. Psychophar-macology 1980;67:17�/23.
12. Browne F, Cooper S, Wilson R, King D. Serum haloperidol levelsand clinical response in chronic, treatment resistant schizophrenicpatients. J Psychopharmacol 1988;2:94�/103.
13. Jusic N, Lader M. Post-mortem antipsychotic drug concentrationsand unexplained deaths. Br J Psychiatry 1994;165:787�/91.
14. Tauscher J, Kapur S. Choosing the right dose of antipsychotics inschizophrenia. CNS Drugs 2001;15:671�/8.
15. Krausz M, Moritz S, Lambert M, Naber D. Dosage of conven-tional neuroleptic medication and subjective cognitive function inschizophrenia. Int Clin Psychopharmacol 2000;15:77�/81.
16. King D. The use of high doses of neuroleptics: the currentsituation. Int Clin Psychopharmacol 1994;9:75�/8.
17. Tognoni G. Pharmacoepidemiology of psychotropic drugs inpatients with severe mental disorders in Italy. Italian CollaborativeStudy Group on the Outcome of Severe Mental Disorders. Eur JClin Pharmacol 1999;55:685�/90.
18. SBU. Treatment with neuroleptic drugs. Stockholm: SBU, TheSwedish Council on Technology Assessment in Health Care; 1997.
19. Apoteksbolaget AB (The National corporation of Swedish phar-macies). Svensk lakemedelsstatistik 1997 (Swedish drug statistics1997). Stockholm: Apoteksbolaget AB; 1997.
20. Lindstrom L. Psykoser (Psychoses). In: Apoteket A, editor.Lakemedelsboken (Drug Treatment Handbook). Stockholm:Apoteket AB; 2001. p. 808�/18.
21. Jonsson D, Marke L. Halsoekonomiska aspekter (Health eco-nomic aspects). In: Treatment with neuroleptics. Stockholm: SBU,The Swedish Council of Technological Assessment in Health Care;1997. p. 155�/67.
22. Remington G, Prendergast P, Bezchlibnyk-Butler K. Dosagingpatterns in schizophrenia with depot, oral and combined neuro-leptic therapy. Can J Psychiatry 1993;38:159�/61.
23. Razali M, Hasanah C. Neuroleptic drug utilization for acuteschizophrenia. Singapore Med J 1996;37:611�/3.
24. Yip K, Ungvari G, Cheung H, Ng F-S, Lau S. A survey ofantipsychotic treatment for schizophrenia in Hong Kong. ChinMed J 1997;110:792�/6.
25. Remington G, Shammi C, Sethna R, Lawrence R. Antipsychoticdosing patterns for schizophrenia in three treatment settings.Psychiatr Serv 2001;52:96�/8.
26. Chen R, Nadkarni P, Levin F, Miller P, Rosenheck R. Using acomputer database to monitor compliance with pharmacother-apeutic guidelines for schizophrenia. Psychiatr Serv 2000;51:791�/
4.27. Valenstein M, Copeland L, Owen R, Blow F, Visnic S. Delays in
adopting evidence-based dosages of conventional antipsychotics.Psychiatr Serv 2001;52:1242�/4.
28. Bingefors K, Isacson D, von Knorring L. Antidepressant dosepatterns in Swedish clinical practice. Int Clin Psychopharmacol1997;12:283�/90.
29. Socialstyrelsen. Classification of Diseases 1987 (in Swedish).Stockholm: Liber/Allmanna Forlaget; 1987.
30. WHO Collaborating Centre for Drug Statistics Methodology.Guidelines for ATC classification and DDD assignment. Oslo:WHO Collaborating Center for Drug Statistics Methodology;1995.
31. Avorn J. The prescription as final common pathway. J TechnolAssess Health Care 1995;11:384�/90.
32. Hartzema A, Christensen D. Nonmedical factors associated withthe prescribing volume among family practitioners in an HMO.Med Care 1983;21:990�/1000.
33. Ito C, Kubota Y, Sato M. A prospective survey on drug choice forprescriptions for admitted patients with schizophrenia. PsychiatryClin Neurosci 1999;53:35�/40.
34. Soares J, Gershon S. Therapeutic targets in late-life psychoses:review of concepts and critical issues. Schizophr Res 1997;27:227�/
39.
K BINGEFORS ET AL.
268 NORD J PSYCHIATRY �VOL 57 �NO 4 � 2003
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
ifor
nia
Irvi
ne o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

35. Baltes P. The ageing mind: potential and limits. Gerontologist1993;33:580�/94.
36. Riecher-Rossler A, Hafner H. Gender aspects in schizophrenia:bridging the border between social and biological psychiatry. ActaPsych Scand 2000;102(Suppl 407):58�/62.
37. Keks N, Altson K, Hope K, Krapvensky N, Culhane C, TanaghowA, et al. Use of antipsychosis and adjunctive medications by aninner urban community psychiatric service. Aust NZ J Psychiatry1999;33:896�/901.
38. Fourrier A, Gasquet I, Allicar M, Bouhassira M, Lepine J, BegaudB. Patterns of neuroleptic drug prescription: a national cross-sectional survey of a random sample of French psychiatrists. Br JClin Pharmacol 2000;49:80�/6.
39. Dahl M-L, Sjoqvist F. Faktorer som paverkar neuroleptikasomsattning i kroppen (Factors influencing the metabolism ofneuroleptics in the body) (in Swedish). In: SBU. Stockholm: TheSwedish Council of Technological Assessment in Health Care;1997. p. 103�/19.
40. Flaherty J, Perry H, Lynchard G, Morley J. Polypharmacy andhospitalization among older home care patients. J Gerontology2000;55A:MS554�/9.
41. Waddington J, Yossef H, Kinsella A. Mortality in schizophrenia.Antipsychotic polypharmacy and absence of adjunctive antic-
holinergics over the course of a 10-year prospective study. Br JPsychiatry 1998;173:325�/9.
42. Nordstrom A. PET evaluation of dopamine hypotheses forantipsychotic drugs and schizophrenia. Stockholm: KarolinskaInstitute; 1993.
43. Lindstrom E, Bingefors K. Patient compliance with drug therapyin schizophrenia. Economic and clinical issues. Pharmacoeco-nomics 2000;18:106�/24.
44. Thompson C. The use of high-dose antipsychotic medication. Br JPsychiatry 1994;164:448�/58.
45. Royal College of Psychiatrists. The association between antipsy-chotic drugs and sudden death. Report of the working group of theRoyal College of Psychiatrists’ Psychopharmacology Sub-Group.London: Royal College of Psychiatrists; 1997. Report No.: CouncilReport CR57.
Kerstin Bingefors, M.Sc., Ph.D., Departments of Neuroscience,Psychiatry, and Pharmacy, Uppsala University, Biomedical Centre,Box 580, SE-751 23 Uppsala, Sweden.Dag Isacson, M.Sc., Ph.D., Department of Pharmacy; UppsalaUniversity, Biomedical Centre, Box 580, SE-751 23 Uppsala, Sweden.Eva Lindstrom, MD, Ph.D., Department of Neuroscience, UppsalaUniversity, Biomedical Centre, Box 580, SE-751 23 Uppsala, Sweden.
ANTIPSYCHOTIC DOSAGE PATTERNS
NORD J PSYCHIATRY �VOL 57 �NO 4 � 2003 269
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
ifor
nia
Irvi
ne o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.