Embed Size (px)
Citation preview
Prim Care Clin Office Pract
31 (2004) 627–648
Down syndrome, Turner syndrome,and Klinefelter syndrome: primary
care throughout the life span
Carl Tyler, MD, MS*, Jennifer C. Edman, MDCleveland Clinic Foundation Family Practice/Fairview Hospital,
18200 Lorraine Avenue, Cleveland, OH 44111, USA
Down syndrome, Turner syndrome, and Klinefelter syndrome constitutethe three most common chromosomal abnormalities encountered byprimary care physicians. Down syndrome typically is recognized at birth,Turner syndrome often is not recognized until adolescence, and many menwith Klinefelter syndrome are never diagnosed. Although each syndrome iscaused by an abnormal number of chromosomes, or aneuploidy, theyare distinct syndromes with learning disabilities and a predisposition towardautoimmune diseases, endocrinologic disorders, and cancers. Optimalhealth care requires a thorough knowledge of the unique health risks,psychoeducational needs, functional capabilities, and phenotypic variationassociated with each chromosomal condition. Unless otherwise specified,syndrome-specific health care should complement standard preventivehealth care recommendations.
Down syndrome
Etiology and diagnosis
Down syndrome is the most common chromosomal cause of mentalretardation [1], with an incidence of 1 in 800 to 1000 live births [2]. In March1999, the British Medical Journal published a survey conducted by the UKDown’s Syndrome Association, which asserted that 28% of 1509 memberparents surveyed expressed a high level of dissatisfaction with the medicalcare received by their child. In response, the UK Down’s Syndrome
* Corresponding author.
E-mail address: [email protected] (C. Tyler).
0095-4543/04/$ - see front matter � 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.pop.2004.04.006
628 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
Association recommended wider implementation of screening for specificmorbidities in all affected individuals with Down syndrome and createda special 14-page insert to supplement standard child health records [3].There is a critical need for primary care physicians to provide state-of-the-art, syndrome-specific health care in addition to routine, age-appropriatehealth care screening and immunizations across the life span. Medical andsurgical advances ensure an increasingly longer life span for individuals withDown syndrome. Primary care physicians must be prepared to assist thepatient and family with life transitions and offer interventions designed toimprove the functional capacity of the individual with Down syndrome.According to the American Academy of Pediatrics Committee on Genetics,key areas of emphasis throughout childhood include comprehensive medicalmanagement, family support, application for Supplemental Social SecurityIncome benefits and other medical and financial support programs, de-velopmentally appropriate prevention of injury and abuse, education andvocational training, and development of healthy eating habits and activelifestyle to promote and maintain healthy weight [4].
The cause of Down syndrome is trisomy, or presence of three copies ofsome or all of chromosome 21. Down syndrome is caused 95% of the timeby nondisjunction of chromosome 21 during the meiotic formation of thespermatocyte or oocyte. Around 4% of individuals with Down syndromehave the ‘‘extra’’ copy of chromosome 21 attached, or translocated, toanother chromosome; in one third of these cases, this translocation also ispresent in one of the parents. The remainder of individuals with Downsyndrome have mosaicism caused by nondisjunction occurring in the embryoafter conception [4,5].
Karyotyping is indicated for confirmation when the diagnosis of Downsyndrome is suspected. The family should be referred for genetic counselingto learn about the disorder and to determine the family-specific risk ofhaving another child with Down syndrome. This risk depends on the com-bination of karyotype and maternal age. In general, the risk of recurrenceof Down syndrome in a future pregnancy is 1% greater than the baselinerisk established by maternal age [2,4,6]. In the 4% to 5% of cases causedby a translocation, however, the recurrence risk could be 100%.
Prenatal risk assessment and diagnosis is offered as an optional portionof standard prenatal care and offers the parents the opportunity to continueor terminate an affected pregnancy. The risk of having a child with Downsyndrome increases with age of the mother, from 1 in 1351 at age 25, to 1 in384 at age 35, and to 1 in 28 by age 45 [7]. Of infants with Down syndrome,however, 70% are born to women younger than age 35. The maternal serumtriple screen, which is performed during the second trimester at 15 to 18weeks of gestation, can detect 60% of trisomy 21 pregnancies with a 5%false-positive rate. This detection rate is improved with ultrasoundassessment of gestational age. Low levels of maternal serum a-fetoproteinand unconjugated estradiol in combination with a twofold elevation in

629C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
maternal serum human chorionic gonadotropin suggest Down syndromeand are an indication for amniocentesis and karyotyping. The triple test failsto detect 10% to 15% of pregnancies affected by trisomy 21 in women olderthan age 35; amniocentesis or chorionic villus sampling should be offered. Inthe future, first-trimester maternal serum screening with different assays maybecome clinically available.
Increased nuchal fold thickness (translucency) secondary to subcutane-ous edema at the base of the occiput is the most common finding suggestingDown syndrome on prenatal ultrasound examination. Ultrasound assess-ment may assist in predicting the likelihood of Down syndrome in womenconsidered to be at increased risk secondary to either advanced maternal ageor abnormal triple screen result [5].
In a systematic literature review, Mansfield et al [8] cited terminationrates of 92% for fetuses diagnosed prenatally with Down syndrome. Thesehigh rates suggest disinclination toward giving birth to children withgenerally mild-to-moderate cognitive impairments, but they also maysuggest lack of information given to parents regarding the full lives led byindividuals with Down syndrome. Prenatal counseling by a trained pro-fessional is needed after confirmation of a prenatal diagnosis [4,5].
If not established antenatally, the diagnosis of Down syndrome is madeeasily shortly after birth. Features of Down syndrome that are commonlypresent in the neonatal period and facilitate diagnosis include hypotonia,poor Moro reflex, hyperflexibility of joints, excess skin at the back of theneck, flattened facies, upslanted palpebral fissures, anomalous auricles,dysplasia of the pelvis, dysplasia of the midphalanx fifth finger, and a singlepalmar crease [6]. Other presenting physical characteristics include brachy-cephaly, gap between first and second toes, low-set ears, protruding tongue,epicanthal folds, Brushfield spots (ring of iris speckles), short broad hands,high arched narrow palate, congenital cardiac defects (most commonlycomplete atrioventricular canal defects), transient myelodysplasia of thenewborn, and duodenal atresia [2,9]. Not all infants with Down syndromepresent with every feature; the phenotype is variable. Down syndrome alsoshould be suspected in a phenotypically normal infant with a leukemoidreaction [4].
Individuals with Down syndrome usually have mild-to-moderate mentalretardation. Other common associated medical complications includegrowth retardation; congenital heart defects; hearing loss due to chronicotitis media and/or sensorineural defects; ophthalmic disorders, includingcongenital cataracts, glaucoma, and strabismus; epilepsy; gastrointestinalmalformations, including duodenal atresia and Hirschsprung’s disease;hypothyroidism; leukemia; atlantoaxial subluxation with spinal cordcompression; early-onset Alzheimer’s disease; increased susceptibility toinfections, including pneumonia, otitis media, sinusitis, periodontal disease,and pharyngitis; and infertility with anovulation present in 30% of womenand sterility in greater than 99% of men [2,4,6].

630 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
Care in childhood
Children with Down syndrome should have height, weight, and headcircumference plotted on the standard and Down syndrome–specific growthcharts to ensure appropriate evaluation for growth delay [4,10]. (Growthcharts are available at http://www.growthcharts.com or in the article byMyrelid et al [10].) Children with Down syndrome manifesting growth delayon Down syndrome–specific charts must be evaluated for undiagnosedmedical problems, such as congenital heart defect, leukemia, or gastroin-testinal problems such as gastroesophageal reflux disease or celiac disease[10]. Evaluation for onset of hypothyroidism is essential in children showingdecreased growth velocity or unexplained weight gain [2]. Evaluation ofthyroid function should continue throughout the life span.
Of infants with Down syndrome, 40% to 60% have congenital heartdefects, the most prevalent being atrioventricular canal defects, ventricularseptal defect, tetralogy of Fallot, ostium secundum, atrial septal defect, andisolated mitral cleft. It is recommended that all individuals with Downsyndrome, even individuals without a murmur, undergo evaluation bya pediatric cardiologist, including electrocardiogram and echocardiogramby age 3 months to minimize the risk of development of severe pulmonaryhypertension as a compensatory mechanism for undiagnosed congenitalheart defects [4,11].
Celiac disease is found in 4% to 17% of children with Down syndromeand may present as growth failure without accompanying symptoms.Institution of a gluten-free diet in individuals with celiac disease normalizesthe small intestine and prevents anemia. Children with Down syndromepresenting with chronic diarrhea or another gastrointestinal complaintshould be evaluated for possible celiac disease. In addition, Csizmadia et al[12] recommended determining HLA-DQ status on all children with Downsyndrome, then measuring IgA endomesial antibodies in children positive forHLA-DQ alleles associated with celiac disease. Biopsy of the small bowel isindicated if the child tests positive for IgA endomesial antibodies. Treatmentwith a gluten-free diet should be instituted in individuals with villus atrophy.Csizmadia et al [12] recommended periodic serum screening for IgAendomesial antibodies in individuals with HLA DQ alleles associated withceliac disease. Some authorities recommend screening for selective IgAdeficiency to assure IgA endomesial antibody results are not falsely negative.
In addition to cognitive impairment (average IQ reported to be 50, butranging from 30 to 70), individuals with Down syndrome have been des-cribed as having specific impairments in expressive language and auditoryprocessing. Despite weaknesses in communication, individuals with Downsyndrome are described as socially adept and generalized to have a ‘‘happy,good-tempered, affectionate, placid’’ personality [1]. They tend to havelower rates of psychiatric and behavioral health problems than otherindividuals with mental retardation but commonly do have difficulties with
631C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
attention, impulsivity, and hyperactivity. Incidence of anxiety, depression,and withdrawal tends to increase with increasing age [13].
Prompt referral to early intervention programs at birth is indicated due tothe high rate of developmental delay. Children with Down syndromerequire comprehensive developmental assessments throughout childhood toevaluate fine and gross motor skills, speech and language comprehension,cognitive ability, and social and adaptive skills. Comprehensive preschoolprograms designed for children with special needs may minimize develop-mental delay and facilitate later mainstreaming into schools, the workforce,and the community [2,4,13]. The prevalence of abuse is higher in individualswith disabilities, and screening for and counseling about prevention of abuseis important beginning in early childhood [14].
Health care guidelines for children with Down syndrome are availablefrom the American Academy of Pediatrics [4], Down Syndrome MedicalInterest Group (US) [15], and Down Syndrome Medical Interest Group(UK) at http://dsmig.org.uk/pdf/downs6.pdf. Each guideline promotesroutine audiologic, ophthalmologic, and dental evaluation; routine annualthyroid function screening; and close monitoring of developmental andeducational progress. In addition to the screening guidelines outlined earlier,the Down Syndrome Medical Interest Group (US) recommends universalscreening for celiac disease beginning at age 2 years. Primary care clinicianscaring for individuals with Down syndrome are strongly encouraged toinclude copies of one of the guidelines and accompanying flow sheet in thepatient’s medical record.
Care in adulthood
Regular physician contact is particularly important in the early adultyears, when changes in educational/vocational, social, and residentialdomains frequently occur simultaneously. Stress and anxiety over transitionsmay result in physical or psychological symptoms. Obtaining employmentthat the young adult with Down syndrome finds meaningful and challengingbut not overtaxing may be difficult. Inquiry about social and sexualrelationships is important, along with counseling regarding the preventionof violence, sexually transmitted diseases, and pregnancy. No one shouldassume that individuals with Down syndrome are infertile. Although thereare rare reports of males with documented offspring, there are far moredocumented reports of women with Down syndrome bearing children.
As with the general population, individuals who were followed bya pediatrician during childhood should transfer their care to a familyphysician or general internist when they reach adulthood. There is a risk forsocial networks to constrict as formal educational programs are completed;peers and siblings leave the community for advanced education, jobs, andmarriage; and older family members become ill, relocate, or die. Prolongedgrief reactions may result, requiring formal mental health referrals.
632 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
Optimizing health and function of an adult with Down syndromerequires knowledge of how aging progresses differently than in the generalpopulation and differently compared with individuals with mental retar-dation of other etiologies. Adults require continued screening for auditoryimpairments and ophthalmologic diseases. In addition to conductive loss,sensorineural hearing loss can emerge in early adulthood. Glaucoma,keratoconus, and early-onset cataracts occur more commonly in individualswith Down syndrome. Without routine ophthalmologic examinations,visual impairments may progress without detection until they becomesevere and irreversible.
Obstructive sleep apnea, manifested by morning irritability and headache,memory difficulty, daytime somnolence, fatigue, depression, or decline inwork performance, is common in Down syndrome. Individuals reluctantto undergo a full sleep laboratory polysomnography study may accept ascreening overnight continuous nocturnal pulse oximetry study as an initialtest. This two-step screening approach has not yet been studied rigorously inadults with Down syndrome, however. Because physicians have difficultypredicting who would accept treatment of sleep apnea, confirmatory testingshould be conducted in all individuals suspected to have it.
Acquired motor impairments deserve careful evaluation. Ligamentouslaxity in the neck (sometimes accompanied by congenital craniocervicalmalformations) may lead to spinal cord compression, cervical nerve rootcompression, or vertebrobasilar insufficiency. Signs of cervical cord com-pression include muscle weakness, increased muscle tone, and increaseddeep tendon reflexes in the lower extremities; ankle clonus; new-onseturinary incontinence; change in hand preference; or positive Babinski’s sign.Hypotonia may persist, however, and interfere with clinical recognition ofcord compression. Individuals with dementia may have long tract neuro-pathic signs without cord compression. Symptoms of cervical root com-pression include pain in the upper neck and occiput that radiates to the eyes,ears, or throat. Vertebrobasilar insufficiency may cause dizziness, vertigo,diplopia, or syncope. Although torticollis should be considered to be due toatlantoaxial instability until proven otherwise, it also can be caused bycervical osteoarthritis.
Routine screening for ‘‘asymptomatic’’ atlantoaxial instability using cutoffmeasurements of the atlanto-dens distance (required for sports participationin Special Olympics in theUnited States) does not reliably identify individualsat risk for cervical myelopathy. A narrow neural canal width may be a betterpredictor of cord compression [16]. Individuals with symptoms suggestingcervical myelopathy should undergo MRI of the cervical spine.
Other orthopedic issues include patellar instability and hip disease. Downsyndrome is associated with an increased incidence of hip dislocation, hipdysplasia, slipped femoral capital epiphysis, Perthes’disease, and avascularnecrosis. Hip disease may progress rapidly in midlife requiring total hiparthroplasty [17]. Decline in ambulatory capacity should be evaluated
633C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
aggressively with attention to the entire spine and lower extremity joints andnot simply attributed to ‘‘old age’’ or dementia. Individuals with Downsyndrome seem to achieve a lower peak bone mineral density and are at riskfor developing osteoporosis by midlife [18].
Screening for thyroid disorders and for gluten-sensitive enteropathy shouldcontinue in adulthood. It is reasonable to measure thyroid-stimulatinghormone annually. There is no clear-cut recommended frequency ofscreening antiendomysial antibody or tissue transglutaminase level deter-minations. Classic malabsorption symptoms of diarrhea and weight lossmay not occur even in individuals with biopsy-proven, gluten-sensitiveenteropathy. Vitamin B12 deficiency due to autoimmune gastritis mayemerge independent of enteropathy.
Obesity is not an inevitable consequence of Down syndrome [19].Attention to caloric intake, adequate physical activity, and early detectionof hypothyroidism can prevent obesity from emerging in adulthood.Although individuals with Down syndrome may be at less risk for coronaryheart disease, other health consequences of obesity include exacerbation ofgastroesophageal reflux, asthma, arthritis, and sleep apnea; difficulty withpersonal hygiene; and limitations in opportunities for recreation andsocialization.
Although psychiatric conditions are difficult to diagnose in individualswith mental retardation, several studies have reported that psychiatricdisorders affect about one quarter of adults with Down syndrome. Of these,the most common condition is depression [20]. Conduct disorder, obsessive-compulsive disorder, attention-deficit disorder, autism, and dementia alsoare reported. Schizophrenia is rare, but unfamiliar clinicians may mis-interpret the ‘‘self-talk’’ and elaborate storytelling of some individuals withDown syndrome as psychotic in nature.
In the United States, the median age of death of persons with Downsyndrome increased from 25 years in 1983 to 49 years in 1997 [21]. Morethan one quarter of individuals with Down syndrome are alive at age 65 [22].Causes of mortality are different than in the general population. Individualswith Down syndrome have greater risk for leukemia and perhaps testicularcancer, but lower risk for all other solid tumors, including breast and coloncancer. This information should be shared with patients and their familieswhen discussing cancer screening recommendations [23].
Increased mortality also is attributed to dementia, epilepsy, congenitalheart disease, infectious disease, ischemic and other heart disease, andcerebrovascular disease. Excess mortality from infectious disease is primar-ily due to influenza and pneumonia. Annual influenza vaccination isimportant. Many clinicians provide pneumococcal vaccination in earlyadulthood. Pneumonia prevention also requires attention to subtle signs ofdysphagia followed by appropriate evaluation and management.
Nearly all adults with Down syndrome manifest Alzheimer’s-typeneuropathology by age 40 [24]. Prospective studies of cognitive change in

634 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
adults suggest, however, that only a subset of individuals actually developclinically evident dementia. Additional factors thought to be associated withearlier onset of dementia include the apoE 4 allele, estrogen deficiency, andhigh levels of Ab 1–42 peptides [25]. In higher functioning individuals, initialmanifestations of dementia include memory impairment, temporal disorien-tation, and reduced verbal output; apathy, inattention, and decreased socialinteraction are observed initially in individuals who are lower functioning atbaseline. As in the general population, the diagnosis of Alzheimer’s diseaserequires careful evaluation to rule out other causes of functional decline,including visual and hearing impairment, depression and other mental healthdisorders, adverse drug effects, nutritional deficiencies, and sleep disorders.Most individuals with Down syndrome who develop Alzheimer’s diseaseeventually manifest seizures. The use of cognitive-enhancing agents in adultswith Down syndrome and Alzheimer’s disease is being investigated.Reported adverse drug effects of donepezil include agitation, aggression,and urinary incontinence [26]. Serotonin-specific reuptake inhibitors mayameliorate the depression that often precedes or coexists with dementia.
Many adults with Down syndrome outlive their parents. Later lifeconsiderations include long-term residential and financial planning; re-tirement; bereavement over the death of friends and family; advancedirectives, guardianship, and durable power of attorney for health care;and accommodations to declines in health and function. Siblings may neededucation and counseling as they assume responsibilities previously handledby parents. Family and service coordinators should investigate local re-sources for the aged, including adult day care, meals on wheels, and othersocial service programs.
Turner syndrome
Etiology and overview
Turner syndrome is caused by complete or partial X monosomy. Theincidence of Turner syndrome is approximately 1 in 2000 among live femaleinfants. In contrast to Down syndrome, there is no association betweenTurner syndrome and advanced maternal age [27]. Different karyotypes areassociated with varying phenotypic expression. The most prevalent karyo-type in patients with Turner syndrome is 45,X monosomy. The Xqisochromosome is associated with autoimmune disorders but not congenitalabnormalities. Women with the ring X chromosome are less likely to displaycongenital abnormalities but are more likely to have spontaneous mensesand cognitive disability [28]. Women with Turner syndrome also can havea mosaic pattern with additional Y chromosome material (45,X/46,XY).Although this mosaic pattern is uncommon, these women have an increasedrisk for the development of gonadoblastoma, dysgerminoma, and mascu-linization, and prophylactic gonadectomy is warranted [29].
635C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
Characteristic features, common findings, and conditions associated withTurner syndrome are summarized in Box 1 [6,29]. The most consistentlyassociated features include short stature and gonadal dysgenesis [6]. Averagelife span of an individual with Turner syndrome is 69 years according toScandinavian studies [27].
Recognition through the lifespan
Antenatal diagnosis may occur incidentally with chorionic villus sam-pling or amniocentesis performed for other indications, such as advancedmaternal age [30]. Ultrasound findings suggesting Turner syndrome includeincreased nuchal translucency, cystic hygroma, coarctation of the aorta orother left-sided cardiac defect, brachycephaly, renal anomalies, polyhy-dramnios, oligohydramnios, and growth retardation [30]. An abnormalmaternal serum screen (elevated a-fetoprotein, dimeric inhibin A, and free bhuman chorionic gonadotropin) also may suggest Turner syndrome.Ultrasound findings and abnormal maternal serum screen are not sufficientto diagnose Turner syndrome; a karyotype is required for definitivediagnosis. Chromosomes always should be re-evaluated postnatally becauseabnormal prenatal karyotypes may reflect cytogenetic abnormalities foundonly in the placenta, but not in the fetus [31].
During the newborn period, physical features characteristic of Turnersyndrome include lymphedema of the hands and feet, nuchal folds, left-sided cardiac anomalies (coarctation or hypoplastic left heart), webbedneck, and low hairline. During childhood, declining growth velocity withshort stature and elevated levels of follicle-stimulating hormone (FSH)should prompt evaluation for Turner syndrome. In adolescence, absence ofbreast development by age 13, pubertal arrest, amenorrhea with elevatedFSH, or unexplained short stature warrants a karyotype and evaluation forTurner syndrome [32].
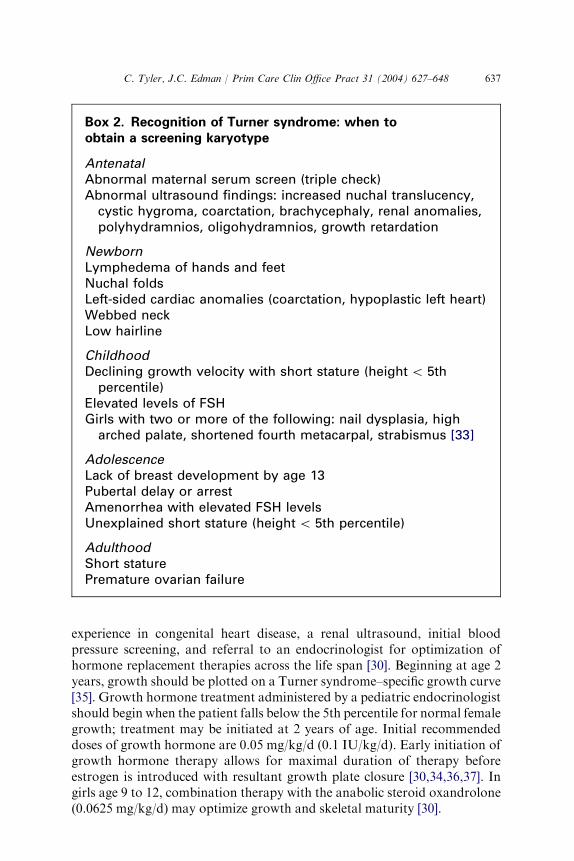
Throughout the life span, the physical signs of Turner syndrome maybe subtle and remain unrecognized by the clinician. Turner syndrome shouldbe considered in any woman with short stature or with premature ovarianfailure. Additionally the phenotypic expression of any X-linked recessivedisorder in a female (eg, hemophilia A, red-green color blindness, orDuchenne muscular dystrophy) might suggest X monosomy [29]. In oneretrospective chart review, two thirds of girls with Turner syndrome notdiagnosed in infancy would have been diagnosed by age 4 had theirphysicians obtained a karyotype when their height fell below the 5thpercentile [33,34]. Box 2 lists indications for obtaining a karyotype to screenfor Turner syndrome [30,32,33,54].
Screening and management of co-morbidities
At the time of diagnosis, all individuals with Turner syndrome, regardlessof age, should have an echocardiogram interpreted by a cardiologist with

636 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
Box 1. Common physical features and associatedconditions in Turner syndrome
Common physical featuresShort stature (reduced final height averaging 143 cm [56 inches])Gonadal failureCubitus valgus (>10( carrying angle between the extended
supinated forearm to the upper arm)Low posterior hairlineHigh-arched palateMultiple pigmented neviWebbed neckLymphedema of hands and feetNail dysplasiaDeep-set hyperconvex nailsShort fourth metacarpalUnusual shape and rotation of earsNarrow maxilla with dental crowdingMicrognathiaBroad shieldlike chest with inverted or hypoplastic nipplesTibial exostosis
Associated conditionsTendency toward obesityRecurrent otitis mediaHearing lossRenal abnormalitiesLeft-sided cardiac anomalies; aortic coarctationStrabismusHypertensionHypothyroidismGlucose intoleranceHyperlipidemiaKyphoscoliosisLordosisOsteoporosisGonadoblastomaInflammatory bowel diseaseColon cancerNeuroblastomaJuvenile rheumatoid arthritisLiver disease
637C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
experience in congenital heart disease, a renal ultrasound, initial bloodpressure screening, and referral to an endocrinologist for optimization ofhormone replacement therapies across the life span [30]. Beginning at age 2years, growth should be plotted on a Turner syndrome–specific growth curve[35]. Growth hormone treatment administered by a pediatric endocrinologistshould begin when the patient falls below the 5th percentile for normal femalegrowth; treatment may be initiated at 2 years of age. Initial recommendeddoses of growth hormone are 0.05 mg/kg/d (0.1 IU/kg/d). Early initiation ofgrowth hormone therapy allows for maximal duration of therapy beforeestrogen is introduced with resultant growth plate closure [30,34,36,37]. Ingirls age 9 to 12, combination therapy with the anabolic steroid oxandrolone(0.0625 mg/kg/d) may optimize growth and skeletal maturity [30].
Box 2. Recognition of Turner syndrome: when toobtain a screening karyotype
AntenatalAbnormal maternal serum screen (triple check)Abnormal ultrasound findings: increased nuchal translucency,cystic hygroma, coarctation, brachycephaly, renal anomalies,polyhydramnios, oligohydramnios, growth retardation
NewbornLymphedema of hands and feetNuchal foldsLeft-sided cardiac anomalies (coarctation, hypoplastic left heart)Webbed neckLow hairline
ChildhoodDeclining growth velocity with short stature (height\ 5thpercentile)
Elevated levels of FSHGirls with two or more of the following: nail dysplasia, higharched palate, shortened fourth metacarpal, strabismus [33]
AdolescenceLack of breast development by age 13Pubertal delay or arrestAmenorrhea with elevated FSH levelsUnexplained short stature (height\ 5th percentile)
AdulthoodShort staturePremature ovarian failure

638 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
Children with Turner syndrome must be monitored for signs ofvirilization. Testing for the presence of Y chromosome mosaicism iswarranted if virilization is present. Prophylactic gonadectomy is advisedif Y chromosome mosaicism is present because of the increased risk forgonadoblastoma or dysgerminoma [29].
Few individuals with Turner syndrome undergo spontaneous puberty (2%to 16%). Pediatric endocrinologists should supervise introduction andtitration of estrogen therapy. Induction of puberty must be balanced withachievement of optimal adult height; introduction of estrogen replacementtherapy should begin after age 12 with a gradual increase in dose to mimicnatural puberty and to facilitate bonematuration [30,32]. Cyclicmenstruationis accomplished with either monthly estrogen withdrawal or progesterone useto prevent endometrial hyperplasia [32]. Women with Turner syndromerequire long-term estrogen and progesterone replacement to help prevent thesequelae of hypoestrogenism, especially low bone mineral density [28].
Except for women with the ring X chromosome karyotype, mentalretardation is not more prevalent in women with Turner syndrome than inthe population at large. They do have lower nonverbal IQ, however, withimpairment in nonverbal visual-spatial organization and nonverbal problemsolving. Other disabilities include impairments in mathematics, memory,ability to formulate goals, and attention span. Attention-deficit disorder ismore common. School-based intervention to facilitate acquisition of lifelongcoping skills should be initiated early because learning disabilities have animpact on vocational success. Girls with Turner syndrome also may showimpaired motor skills and coordination. This impairment may be improvedwith occupational therapy and motor skills training [32,38]. Infants shouldbe referred to early intervention programs when delayed neuromusculardevelopment is detected [29]. It is suggested that some of the aforementioneddeficits may be related to estrogen deficiency and may be reversed partiallywith estrogen supplementation [30,38]. As a group, women with Turnersyndrome are not believed to be at increased risk for mental health problems.
Girls with Turner syndrome consistently and clearly identify with thefemale gender. They are described as having ‘‘high stress tolerance, limitedemotional arousal, high degree of dependence, unassertiveness and over-compliance’’ [32], although these traits are common in all women with shortstature and delayed sexual development. Compared with girls with othercauses of short stature, girls with Turner syndrome often exhibit delayedsocial maturation, impaired social relationships, and lack of self-esteem.Girls must be encouraged to develop and maintain friendships throughinvolvement in formal and informal recreational activities. Parents andteachers must intervene aggressively at the onset of teasing or bullying.Meeting with other children and adults with Turner syndrome and theirfamilies provides invaluable support for affected girls and their parents [38].
Health care of individuals with Turner syndrome involves far more thanrecognition of the disorder and endocrinologic management. Additional

639C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
comorbidities requiring recognition and surveillance, organized by organsystem, are as follows. All infants with Turner syndrome should be checkedcarefully for hip dysplasia. Monitor Children and adolescents should bemonitored for tibial problems and for the development of scoliosis.Beginning in childhood, the importance of optimizing bone density withdietary/supplemental calcium, vitamin D, and weight-bearing exerciseshould be discussed [29]. There is an increased incidence of fractures inTurner syndrome patients older than age 45. It is essential to measure bonemineral density at the initial adult visit and to repeat 2 to 5 years later. Rateof change detected should guide the periodicity of future testing. Osteopo-rosis treatment should be instituted when decreasing bone mass is detected.Oral calcium intake of at least 1200 mg/d is recommended for all womenwith Turner syndrome [28].
Congenital heart defects, most commonly left-sided defects, includingbicuspid aortic valve and coarctation of the aorta, are present in 30% ofpatients with Turner syndrome. Women with Turner syndrome also aremore susceptible to aortic root dilation and rupture. At time of diagnosis,regardless of age, all women with Turner syndrome should be referred toa cardiologist, and a thorough cardiovascular evaluation including echo-cardiogram should be performed [27,30]. Throughout childhood, bloodpressure and peripheral pulses must be monitored closely. Arm and legsystolic blood pressure should be compared with evaluation for possiblecoarctation. Elevated blood pressure must be treated aggressively through-out the life span and a cardiac or renal cause excluded [29]. If cardiacmalformations are present, the patient needs lifelong subacute bacterialendocarditis prophylaxis. Even if initial cardiac evaluation does not revealcongenital defects, an echocardiogram is warranted during adolescence(age 12–15) [29], again at time of transition to an adult provider, thenperiodically throughout adulthood (every 3–5 years) [28,30].
Less than 2% of women with Turner syndrome are able to conceivea child spontaneously [32]. Given the increased cardiac demands ofpregnancy, women with Turner syndrome may have an unacceptable riskfor aortic dissection or rupture. Aortic root dimension must be monitoredby serial echocardiography throughout the pregnancy [30]. Currently, nonational guidelines exist regarding the advisability of pregnancy for womenwith Turner syndrome despite the increasing availability of assisted re-productive technologies. Counseling regarding high rates of maternalmortality must begin early in adolescence and accompany discussion ofassisted reproductive technology [32]. Women with spontaneous mensesmust be educated regarding contraception and prevention of unwantedpregnancy. All women with Turner syndrome need education regardingsexuality and the prevention of sexually transmitted disease.
Congenital renal anomalies, including horseshoe kidney and duplicatecollection system, are present in 30% to 60% of women with Turnersyndrome. At minimum, individuals with urinary tract abnormalities

640 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
require a yearly screening urine culture, serum blood urea nitrogen andcreatinine, and periodic ultrasound evaluation to assess for progression ofthe anomaly [28–30].
Women with Turner syndrome have increased rates of autoimmunedisease, including Hashimoto’s thyroiditis, Graves’ disease, inflammatorybowel disease (ulcerative colitis and Crohn’s disease), myasthenia, IgAdeficiency, celiac disease, juvenile rheumatoid arthritis, and membranopro-liferative glomerulonephritis. Any unexplained diarrhea or bleeding must beevaluated promptly [28,32]. Fifty percent of adults are affected by hypothy-roidism, and if undetected, hypothyroidism increases the individual’s riskfor dyslipidemia and obesity [32]. Routine screening thyroid-stimulatinghormone and free thyroxine levels should be obtained annually beginning atage 4, unless clinical signs warrant evaluation sooner. Thyroid autoantibodiesalso may be evaluated [29]. In addition to the previously described increasedrisk for malignant germ cell tumors (dysgerminomas), women with Turnersyndrome are at a five to six times increased risk for colon cancers independentof the increased relative risk of 2.25 for inflammatory bowel disease [32].
Women with Turner syndrome manifest micrognathia and mild earmalformations. Screening at birth must be done to assess for adequacy ofthe suck and swallow reflex owing to impaired oral motor function.Orthodontic evaluation is recommended between 8 and 10 years of age[29]. Progressive midfrequency sensorineural hearing loss is common inTurner syndrome, affecting children and approximately 40% of women bytheir mid-40s. Hearing should be evaluated at birth, 6 and 12 months of age,and periodically throughout the remainder of childhood and adulthood withprompt referral for hearing aid evaluation if sensorineural hearing loss isdetected [30,39]. Beginning in infancy, children should be evaluated for serousotitis and otitis media at every heath care visit because of eustachian tubedistortion. When these conditions are present, aggressive treatment includingtympanostomy tube placement should be instituted. Strabismus, amblyopia,and ptosis also are common, warranting ophthalmology referral [29].
Beginning with the family in early childhood, a comprehensive programof lifestyle education emphasizing diet and physical activity aimed at theprevention of obesity is desirable for the long-term health of individualswith Turner syndrome. Problems experienced by women with Turnersyndrome, such as glucose intolerance, hypertension, and osteoporosis,are compounded by obesity [28–30]. Although individuals with Turnersyndrome are at increased risk for glucose intolerance, whether or not theyare at increased risk for overt diabetes is controversial [40].
Although multiple pigmented nevi are associated with Turner syndrome,there is not believed to be an increased risk for melanoma. Additionally,keloid formation is common with any dermal procedure in individuals withTurner syndrome and must be discussed before surgery. Experts suggest thatnevi be removed only if necessary, using plastic surgery techniques tominimize scarring [27].
641C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
Support groups for women with Turner syndrome and their families canclarify expectations and help them cope with disease manifestations. LocalTurner syndrome support groups are available, and resources on theInternet include the Turner Syndrome Support Society (http://www.turner-syndrome-us.org/) and the Magic Foundation (http://www.magicfounda-tion.org/).
Klinefelter syndrome
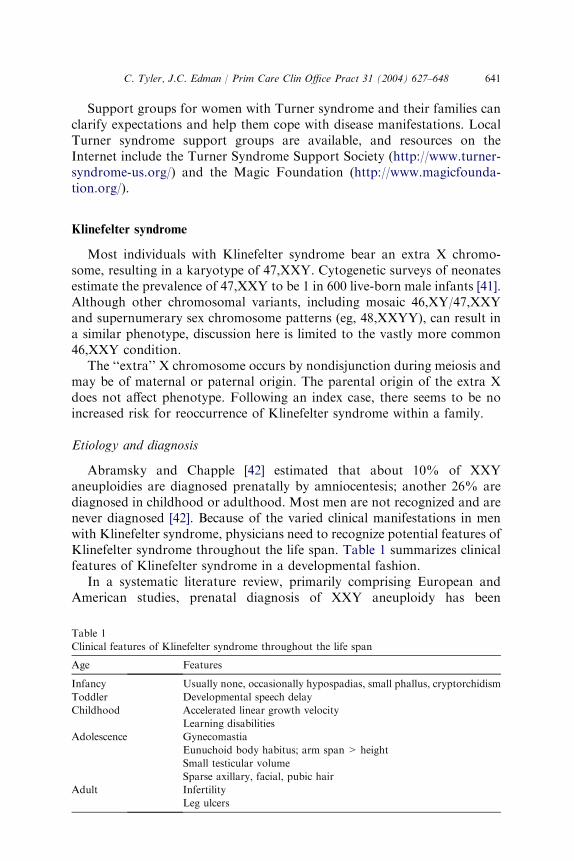
Most individuals with Klinefelter syndrome bear an extra X chromo-some, resulting in a karyotype of 47,XXY. Cytogenetic surveys of neonatesestimate the prevalence of 47,XXY to be 1 in 600 live-born male infants [41].Although other chromosomal variants, including mosaic 46,XY/47,XXYand supernumerary sex chromosome patterns (eg, 48,XXYY), can result ina similar phenotype, discussion here is limited to the vastly more common46,XXY condition.
The ‘‘extra’’ X chromosome occurs by nondisjunction during meiosis andmay be of maternal or paternal origin. The parental origin of the extra Xdoes not affect phenotype. Following an index case, there seems to be noincreased risk for reoccurrence of Klinefelter syndrome within a family.
Etiology and diagnosis
Abramsky and Chapple [42] estimated that about 10% of XXYaneuploidies are diagnosed prenatally by amniocentesis; another 26% arediagnosed in childhood or adulthood. Most men are not recognized and arenever diagnosed [42]. Because of the varied clinical manifestations in menwith Klinefelter syndrome, physicians need to recognize potential features ofKlinefelter syndrome throughout the life span. Table 1 summarizes clinicalfeatures of Klinefelter syndrome in a developmental fashion.
In a systematic literature review, primarily comprising European andAmerican studies, prenatal diagnosis of XXY aneuploidy has been
Table 1
Clinical features of Klinefelter syndrome throughout the life span
Age Features
Infancy Usually none, occasionally hypospadias, small phallus, cryptorchidism
Toddler Developmental speech delay
Childhood Accelerated linear growth velocity
Learning disabilities
Adolescence Gynecomastia
Eunuchoid body habitus; arm span > height
Small testicular volume
Sparse axillary, facial, pubic hair
Adult Infertility
Leg ulcers
642 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
associated with documented pregnancy termination rates of 92% [8].Pregnancy termination rates are lowest when post-test counseling is pro-vided by a geneticist. There is evidence of great variation in health careprofessionals’ knowledge regarding sex chromosome anomalies, such thatsome parents receive outdated and incomplete information [43].
Infancy and childhood
Klinefelter syndrome rarely can be identified in infancy, after karyotyp-ing is performed as part of a routine evaluation for hypospadias, smallphallus, or cryptorchidism. The genitals in infants with Klinefelter syn-drome are usually normal at birth. Affected toddlers often manifest a delayin the first use of words and phrases compared with siblings. Althoughmotor development generally falls within the normal range, some infants areslower to walk and lack coordination due to hypotonia of the lowerextremities and sensorimotor dysfunction.
After age 5, boys with Klinefelter syndrome often show accelerated lineargrowth velocity, owing to excessive leg length. This accelerated growthvelocity is the most uncommon growth abnormality a primary care physicianencounters in practice and always should prompt consideration of obtaininga chromosome analysis to exclude Klinefelter syndrome [44]. Most boys withKlinefelter syndrome manifest learning disabilities. They typically havedifficulty with reading and language arts secondary to poor vocabulary skills,limited abstract reasoning skills, poor auditory memory, and problems withnarrative formation. These speech and language deficits correlate with lowerverbal IQ scores. Although average IQ scoremay be 10 to 15 points below thatof siblings, most individuals with Klinefelter syndrome have average-to-superior intelligence, with less than 20% scoring lower than 90 [45].
Suggested educational accommodations may include the use of visual aids(pictures, diagrams, and graphs), rather than verbal or written directions;computer, typewriter, or tape recorder, rather than written communication;and additional time for written assignments. Speech therapists can helpadvance language development and communication skills. In boys with handtremor and impairments of fine motor coordination, occupational therapymay be beneficial. Obesity may emerge in later childhood. Obesity combinedwith poor coordination and poor muscle development may necessitateadapted physical education [46].
Endocrinologic and reproductive issues
Klinefelter syndrome is the most common congenital abnormalityresponsible for testicular failure in youth. Puberty often occurs at a normalage, but secondary sex changes do not follow typical progression. The testesinitially may enlarge normally, but as the seminiferous tubules fibrose, thetestes involute and become firm. Ultimately the testes are typically less than2.5 cm in greatest dimension with volume of less than 5 cm3. Facial, axillary,

643C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
and pubic hair tends to be sparse. Before adolescence, testosterone levels arewithin the normal range. By early adulthood, testosterone levels decrease tolow or low-normal values. Concomitantly, luteinizing hormone and FSHlevels begin to increase around age 11 or 12 and remain abnormally elevated[47].
More than 50% of adolescents with Klinefelter syndrome developgynecomastia, owing to increased estradiol-to-testosterone ratio; this oftenpersists in adulthood. (Testosterone therapy does not improve or preventgynecomastia.) Eunuchoid proportions become evident, with lower bodysegment (floor to pubis) exceeding upper body segment (pubis to crown) bymore than 2 cm and with arm span typically exceeding height by 7 cm ormore [8]. Males with the XXY karyotype tend to have narrower shouldersand wider hips.
These physical and hormonal characteristics can present significantpsychosocial difficulties for adolescents with Klinefelter syndrome. Thegynecomastia, eunuchoid habitus, and lack of muscle strength, along withdifficulties with academic performance, can lead to low self-esteem, in-security, and withdrawal from peers. Although Klinefelter syndrome is notassociated with homosexuality or gender identity disorders, overall sexualinterest may be diminished. A young man with Klinefelter syndrome mayfind it difficult to individuate and separate from his family [47].
Men with Klinefelter syndrome first may come to diagnosis in the contextof evaluation for infertility. Although men who are mosaic 47,XXY/46,XYmay be fertile, men who are purely 47,XXY are considered infertile. Thereare a few cases of confirmed paternity by men not found to have a mosaicphenotype. Couples may consider assisted reproductive technologies, suchas intracytoplasmic sperm injection, after sperm are extracted throughtesticular biopsy. Although healthy and karyotypically normal infants havebeen born through this technique, there may be an increased risk ofautosomal aneuploidies [48]. Most couples desiring children choose adop-tion or artificial insemination with donor sperm.
Testosterone replacement generally is recommended at around age 11 or12, when gonadotropin levels begin to rise. The dosage should be titratedgradually to provide age-appropriate normal levels of serum testosterone,luteinizing hormone, FSH, and estradiol and to induce gradual virilization.This therapy typically requires consultation with a pediatric endocrinologist.Testosterone replacement in adulthood is less complicated and may be ad-ministered by the primary care clinician.
Associated medical conditions
The physician should be attentive to other medical conditions associatedwith Klinefelter syndrome. Osteoporosis is more common, particularly inpatients who did not receive testosterone replacement during adolescenceand early adulthood. In addition to optimizing calcium, vitamin D, and

644 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
testosterone replacement, patients may benefit from antiresorptive thera-pies. Although autoimmune conditions, including rheumatoid arthritis,systemic lupus erythematosus, and Sjogren’s syndrome, seem to be morecommon in males with Klinefelter syndrome compared with karyotypicallynormal males, the absolute risk for these conditions is unknown. Testos-terone replacement may improve the clinical course of these diseases [49].
Endocrine conditions associated with Klinefelter syndrome include type 2diabetes mellitus and chronic autoimmune thyroiditis. Some authorsrecommend annual thyroid-stimulating hormone testing, beginning inchildhood [50].
Physicians should consider the diagnosis of Klinefelter syndrome inyoung men with recurrent leg ulcers, whether or not obvious venous diseaseis present [51]. Pulmonary conditions associated with Klinefelter syndromeinclude chronic bronchitis, bronchiectasis, and emphysema. Additional in-jury from cigarette use should be avoided.
Men with Klinefelter syndrome bear a risk of breast carcinoma thatapproximates that of similar-aged women. This risk may exceed 20 fold thatof karyotypically normal men [52]. Men should be instructed in breast self-examination, and clinicians should perform annual clinical breast examina-tions. There are no studies to support routine screening mammography orprophylactic mastectomy. Additionally, young adults with Klinefeltersyndrome bear an increased risk, estimated around 1%, for the developmentof mediastinal germ cell tumors [53].
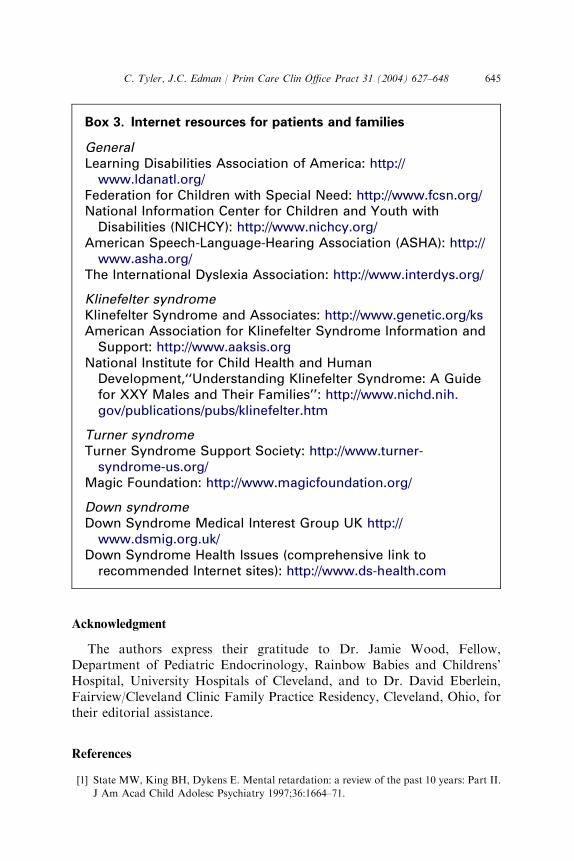
Resources for physicians and families include Klinefelter Syndrome andAssociates (http://www.genetic.org/ks) and the American Association forKlinefelter Syndrome Information and Support (http://www.aaksis.org)(Box 3). The National Institute for Child Health and Human Developmenthas published a booklet entitled ‘‘Understanding Klinefelter Syndrome:A Guide for XXY Males and Their Families,’’ available online at http://www.nichd.nih.gov/publications/pubs/klinefelter.htm.
Summary
Primary care physicians must educate themselves regarding diagnosis andmanagement of common chromosomal aneuploidies. Limited understand-ing of the life experience of persons affected by chromosomal aneuploidiescan lead to inadequate prenatal counseling, resulting in high rates oftermination of affected pregnancies. Throughout the life span, syndrome-specific screening requirements must be integrated into general health careguidelines. Checklists and syndrome-specific growth grids should be usedroutinely. Ongoing communication between specialists and primary carephysicians and between pediatric and adult clinicians is essential. Supportgroups and Internet resources can benefit affected individuals and theirfamilies immensely.
645C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
Acknowledgment
The authors express their gratitude to Dr. Jamie Wood, Fellow,Department of Pediatric Endocrinology, Rainbow Babies and Childrens’Hospital, University Hospitals of Cleveland, and to Dr. David Eberlein,Fairview/Cleveland Clinic Family Practice Residency, Cleveland, Ohio, fortheir editorial assistance.
References
[1] State MW, King BH, Dykens E. Mental retardation: a review of the past 10 years: Part II.
J Am Acad Child Adolesc Psychiatry 1997;36:1664–71.
Box 3. Internet resources for patients and families
GeneralLearning Disabilities Association of America: http://www.ldanatl.org/
Federation for Children with Special Need: http://www.fcsn.org/National Information Center for Children and Youth withDisabilities (NICHCY): http://www.nichcy.org/
American Speech-Language-Hearing Association (ASHA): http://www.asha.org/
The International Dyslexia Association: http://www.interdys.org/
Klinefelter syndromeKlinefelter Syndrome and Associates: http://www.genetic.org/ksAmerican Association for Klinefelter Syndrome Information andSupport: http://www.aaksis.org
National Institute for Child Health and HumanDevelopment,‘‘Understanding Klinefelter Syndrome: A Guidefor XXY Males and Their Families’’: http://www.nichd.nih.gov/publications/pubs/klinefelter.htm
Turner syndromeTurner Syndrome Support Society: http://www.turner-syndrome-us.org/
Magic Foundation: http://www.magicfoundation.org/
Down syndromeDown Syndrome Medical Interest Group UK http://www.dsmig.org.uk/
Down Syndrome Health Issues (comprehensive link torecommended Internet sites): http://www.ds-health.com
646 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
[2] Saenz RB. Primary care of infants and young children with Down syndrome. Am Fam
Physician 1999;59:381–96.
[3] Mayor S. Parents of people with Down’s syndrome report suboptimal care. BMJ 1999;318:
687.
[4] American Academy of Pediatrics. Health supervision for children with Down syndrome.
Pediatrics 2001;107:442–9.
[5] Newberger DS. Down syndrome: prenatal risk assessment and diagnosis. Am Fam
Physician 2000;62:825–38.
[6] Jones KL. Smith’s recognizable patterns of human malformation. 5th edition.
Philadelphia: WB Saunders; 1997.
[7] Morris JK, Wald NJ, Mutton DE, Alberman E. Comparison of models of maternal age-
specific risk for Down syndrome live births. Prenat Diagn 2003;23:252–8.
[8] Mansfield C, Hopfer S, Marteau TM. Termination rates after prenatal diagnosis of Down
syndrome, spina bifida, anencephaly, and Turner and Klinefelter syndromes: a systematic
literature review. European Concerted Action: DADA (Decision-making After the
Diagnosis of a fetal Abnormality). Prenat Diagn 1999;19:808–12.
[9] Hindley D, Medakkar S. Diagnosis of Down’s syndrome in neonates. Arch Dis Child Fetal
Neonatal Educ 2002;87:F220–1.
[10] Myrelid A, Gustafsson J, Ollars B, Anneren G. Growth charts for Down’s syndrome from
birth to 18 years of age. Arch Dis Child 2002;87:97–103.
[11] Jacobs IN, Gray RF, Todd NW. Upper airway obstruction in children with Down
syndrome. Arch Otolaryngol Head Neck Surg 1996;122:945–50.
[12] Csizmadia CG, Mearin ML, Oren A, et al. Accuracy and cost-effectiveness of a new
strategy to screen for celiac disease in children with Down syndrome. J Pediatr 2000;137:
756–61.
[13] Chapman RS, Hesketh LJ. Behavioral phenotype of individuals with Down syndrome.
Ment Retard Dev Disabil Res Rev 2000;6:84–95.
[14] Smith DS. Health care management of adults with Down syndrome. Am Fam Physician
2001;64:1031–8.
[15] Cohen WI. Health care guidelines for individuals with Down syndrome: 1999 revision.
Down Syndrome Quarterly 1999;4:1–15.
[16] White KS, Ball WS, Prenger EC, Patterson BJ, Kirks DR. Evaluation of the craniocervical
junction in Down syndrome: correlation of measurements obtained with radiography and
MR imaging. Radiology 1993;186:377–82.
[17] Kioschos M, Shaw ED, Beals RK. Total hip arthroplasty in patients with Down’s
syndrome. J Bone Joint Surg Br 1999;81:436–9.
[18] Tyler CV, Snyder CW, Zyzanski S. Screening for osteoporosis in community-dwelling
adults with mental retardation. Ment Retard 2000;38:316–21.
[19] Rubin SS, Rimmer JH, Chicoine B, Braddock D, McGuire DE. Overweight prevalence in
persons with Down syndrome. Ment Retard 1998;36:175–81.
[20] Khan S, Osinowo T, Pary RJ. Down syndrome and major depressive disorder: a review.
Mental health aspects of developmental disabilities 2002;5:46–52.
[21] Yang Q, Rasmussen SA, Friedman JM. Mortality associated with Down’s syndrome in the
USA from 1983 to 1997: a population-based study. Lancet 2002;359:1019–25.
[22] Baird PA, Sadovnick AD. Life tables for Down syndrome. Hum Genet 1989;82:291–2.
[23] Satge D, Sasco AJ. Breast screening guidelines should be adapted in Down’s syndrome.
BMJ 2002;324:1155.
[24] Mann DM. Alzheimer’s disease and Down’s syndrome. Histopathology 1988;13:125–37.
[25] Schupf N, Sergievsky GH. Genetic and host factors for dementia in Down’s syndrome.
Br J Psychiatry 2002;180:405–10.
[26] Hemingway-Eltomey JM, Lerner AJ. Adverse effects of donepezil in treating Alzheimer’s
disease associated with Down’s syndrome. Am J Psychiatry 1999;156:1470.
[27] Saenger P. Turner syndrome. N Engl J Med 1996;335:1749–54.
647C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
[28] Elsheikh M, Conway GS, Wass JA. Medical problems in adult women with Turner
syndrome. Ann Med 1999;31:99–105.
[29] Frias JL, Davenport ML. Health supervision for children with Turner syndrome.
Pediatrics 2003;111:692–702.
[30] Saenger P, Wikland KA, Conway GS, et al. Recommendations for the diagnosis and
management of Turner syndrome. J Clin Endocrinol Metab 2001;86:3061–9.
[31] Wenstrom KD, Chu DC, Owen J, Boots L. Maternal serum alpha-fetoprotein and dimeric
inhibin A detect aneuploidies other than Down syndrome. Am J Obstet Gynecol 1998;179:
966–70.
[32] Karnis MF, Reindollar RH. Turner syndrome in adolescence. Obstet Gynecol Clin North
Am 2003;30:303–20.
[33] Savendahl L, Davenport ML. Delayed diagnoses of Turner syndrome: proposed guidelines
for change. J Pediatr 2000;137:455–9.
[34] Rosenfeld RG. Turner syndrome: a growing concern. J Pediatr 2000;137:443–4.
[35] Rongen-Westerlaken C, Corel L, van den Broeck J, et al. Reference values for height,
height velocity and weight in Turner syndrome. Swedish Study Group for GH treatment.
Acta Paediatr 1997;86:937–42.
[36] Saenger P. Growth-promoting strategies in Turner syndrome. J Clin Endocrinol Metab
1999;84:4345–8.
[37] Reiter EO, Blethen SL, Baptista J, Price L. Early initiation of growth hormone treatment
allows age-appropriate estrogen use in Turner syndrome. J Clin Endocrinol Metab 2001;
86:1936–41.
[38] Ross J, Zinn A, McCauley E. Neurodevelopmental and psychosocial aspects of Turner
syndrome. Ment Retard Dev Disabil Res Rev 2000;6:135–41.
[39] Hultcrantz M. Ear and hearing problems in Turner syndrome. Acta Otolaryngol 2003;123:
253–7.
[40] Landin-Wilhelmsen K, Bryman I, Wilhelmsen L. Cardiac malformations and hyperten-
sion, but not metabolic risk factors, are common in Turner syndrome. J Clin Endocrinol
Metab 2001;86:4166–70.
[41] Bojesen A, Juul S, Gravholt CH. Prenatal and postnatal prevalence of Klinefelter
syndrome: a national registry study. J Clin Endocrinol Metab 2003;88:622–6.
[42] Abramsky L, Chapple J. 47, XXY (Klinefelter syndrome) and 47, XYY: estimated rates of
and indication for postnatal diagnosis with implications for prenatal counselling. Prenat
Diagn 1997;17:363–8.
[43] Abramsky L, Hall S, Levitan J, Marteau TM. What parents are told after prenatal
diagnosis of a sex chromosome abnormality: interview and questionnaire study. BMJ 2001;
322:463–6.
[44] Legler JD, Rose LC. Assessment of abnormal growth curves. Am Fam Physician 1998;58:
153–8.
[45] Smyth CM. Diagnosis and treatment of Klinefelter syndrome. Hosp Pract (Office Educ)
1999;34:111–20.
[46] Plumridge D, Bennett R, Dinno N, Branson C. The student with a genetic disorder:
educational implications for special education teachers and for physical therpists,
occupational therapists, and speech pathologists. Springfield (IL): Charles C Thomas;
1993.
[47] Manning MA, Hoyme HE. Diagnosis and management of the adolescent boy with
Klinefelter syndrome. Adolesc Med 2002;13:367–74.
[48] Morel F, Bernicot I, Herry A, Le Bris MJ, Amice V, De Braekeleer M. An increased
incidence of autosomal aneuploidies in spermatozoa from a patient with Klinefelter
syndrome. Fertil Steril 2003;79 (Suppl 3):1644–6.
[49] Bizzarro A, Valentini G, Di Martino G, DaPonte A, De Bellis A, Iacono G. Influence of
testosterone therapy on clinical and immunological features of autoimmune diseases
associated with Klinefelter syndrome. J Clin Endocrinol Metab 1987;64:32–6.
648 C. Tyler, J.C. Edman / Prim Care Clin Office Pract 31 (2004) 627–648
[50] Hsueh WA, Hsu TH, Federman DD. Endocrine features of Klinefelter syndrome.
Medicine (Baltimore) 1978;57:447–61.
[51] Tyler CV Jr, Kungl PA, Green LA. Genetic diagnosis in adulthood: a case report. J Fam
Pract 1998;47:227–30.
[52] Lynch HT, Watson P, Narod SA. The genetic epidemiology of male breast carcinoma.
Cancer 1999;86:744–6.
[53] Hasle H, Mellemgaard A, Nielsen J, Hansen J. Cancer incidence in men with Klinefelter
syndrome. Br J Cancer 1995;71:416–20.
[54] Toth PP, Jogerst GJ. Identification of Turner syndrome in an elderly woman: case report
and review. Arch Fam Med 1996;5:48–51.





























