Embed Size (px)
Citation preview

DR. JOHARA AL-MUTAWAASST. PROF. & CONSULTANT
OB/GYNE

SPONTANEOUS ABORTION
Definition:Abortion termination of pregnancy before the fetus is sufficiently developed to survive (before 24 wks)Incidence: 15%
It is convenient to consider the clinical aspect of spontaneous abortion under 5 sub groups: 1. Threatened 4. Missed 2. Inevitable 5. Recurrent abortion3. Incomplete 6. Septic Abortion


Threatened Abortion: 25% of pregnancies
This refers only to bleeding from placental site which is not yet severe enough to terminate the pregnancy. In practice any case of bleeding before the 24th wks may be classed as threatened abortion in the absence of any other explanation.

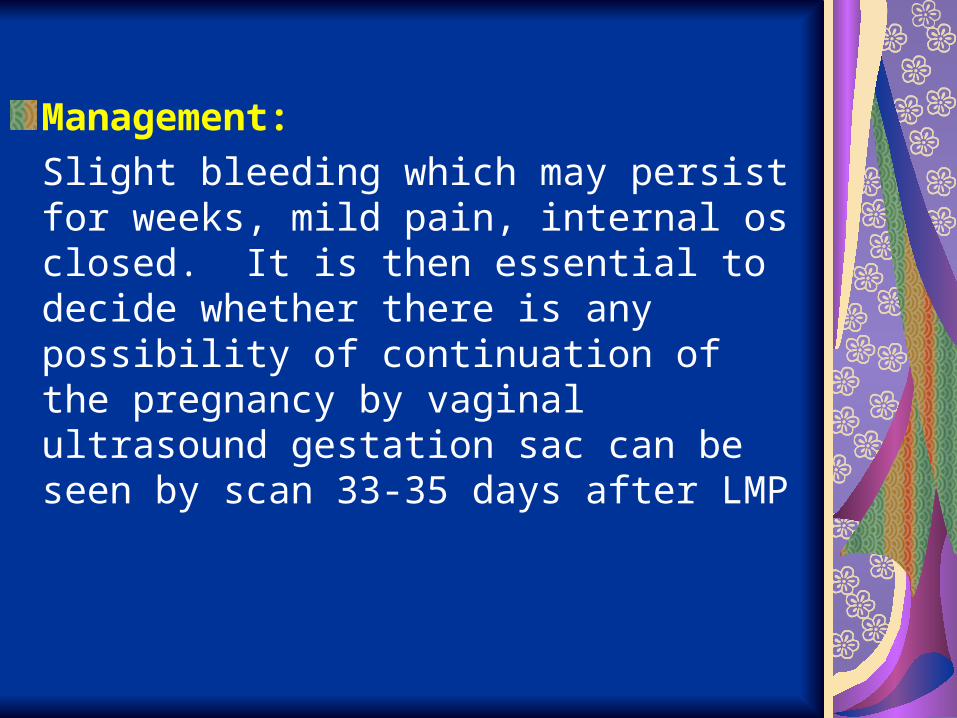
Management:
Slight bleeding which may persist for weeks, mild pain, internal os closed. It is then essential to decide whether there is any possibility of continuation of the pregnancy by vaginal ultrasound gestation sac can be seen by scan 33-35 days after LMP

Serial qualitative HCG level:BHCG level – 1000 miu/mlif gest. Sac seen BHCG less than 1000 unlikely to survive.Qualitative BHG level should ↑ 65% every 48 hours.S. Progesterone levelThe 5 ng/ml associated dead fetus> 25ng/ml associated with alive fetusExpectant observationNo benefit from use of progesterone or bed rest although it is often advised.
Inevitable Abortion
Indicate the pregnancy is doomed to end shortly. Progressive cervical dilation without the passage of tissue. here bleeding is slight but retroplacental fetus is dead. Pain usually more.Dilated internal os. USS – Non viable fetus. P.T. +veEmergency suction: D & C
Complete AbortionDiagnosed if patient passed tissue but now is only slight pain and P/V bleedingExamination confiremd dilated os of Cx.Minimal current bleedingTVU – empty uterusR/O ectopic pregnancy by serial BHCG leveluntil P.T. -veAnti D injection if patients RH – ve to prevent sensitization


Incomplete Abortion
If the internal cervical os is open and patient has passed some tissue.
Management:
Emergency suction and curettage


Missed AbortionIt is defined as retention of dead products of conception in utero for several weeks.Symptoms of early pregnancy disappearUterus not only has ceased to enlarge but also has become smaller.Occasionally serious coagulation defect may develop.Abnormal sonographic finding:
Irregular gest. SacTrophoblastic reactionIrregular and thinYolk sac not seenAbsent embryo or amorrphous

Septic Abortion
Uterine infection at any stage of abortion causes:
Delay in evacuation of uterus Delay seeking advice
Incomplete surgical evacuation followed by infection from vaginal organisms after 48 hours:
– Anaerobic streptococcus– Group B harmolytic streptococcus– Coliform bacilus– Clostridium welchin– Bacterial fragilis

Trauma:Perforation or cervical tearCriminal abortion
Treatment:Should be active to minimize risk of septic shockCervical & HVS, blood cultureBlood spectrum antibioticEvacuation – perforation is commonHystrectomy
Induced AbortionTherapeutic abortion – termination of pregnancy before time of fetal viability for the purpose of safe guarding the health of the mother. Heat disease, invasive Ca of Cx.A certificate of opinion is given by 2 heart consultant obstetrician.Elective (voluntary) abortion is the interruption of pregnancy before viability at request of the women but not for reason of inpaired maternal health or fetal disease.
Cont:
Illegal abortion usually performed in unsterile condition by operators with little or nor medical training.It is often incomplete and complicated by:
Hemorrhage Infection
Infertility tubal occlusionsIntrauterine infection is frequent complication and septic shock and death are the ultimate consequences.

Recurrent Miscarriage
When a woman has had 3 consecutive miscarriage.Risk of abortion for next pregnancy:
1 abortion 15%1 Normal pregnancy 15%1 Abortion1 Normal 25%2 Abortion2 abortion 40%
Etiology and Investigation:1. Genetic factors
Karyotyping of both partners will reveal chromosome anomalies
2. Anatomical factorsUterine anomaliesCervical incompetenceHysteroscopy & HSG – Septum / Fibroid
3. Endocrine problem↑ LH in PCO
4. Immunological factorsRecurrent miscarriage is common in couples with
similar HLA typesCommon in women with antiphopholipid antibodies syndromeAnticardiolipid ant. & Lupus anticoagulant
5. Maternal diseaseSLE, Renal disease
5. Encironmenta factor: Smoking / Alcohol

Abortion Technique: Surgical / Medical
Medical : Oxytocin Prostaglandins Anti progesterone Ru 486
(Mifepristone)Surgical : Suction, D & CProstaglandin vaginal suppressions
applied to Cx. To ripen or soften and dilated cervix before termination by curettage or as adjunct for mifepristone termination


1. Confirm diagnosis – history examination
If sure of date of LMP and /Or regular cycle, i.e.>
6 weeks’gestation, arrangeTV ultrasound and classifyMiscarriage according to
RCOG guidelines
If unsure of date of LMPAnd /or irregular cycle
Take serum hCG
If hCG (?miscarriage/? Early intrauterine/? Ectopic pregnancy
If hCG > 1000,Use protocol for
Suspected ectopicpregnancy
2. If viable pregnancy (threatened miscarriage) Reaasure Check whether pregnancy is wanted or not and give appropriate
written info and arrange follow-up. Offer repeat scan in 2 weeks if further significant bleeding, otherwise offer nuchal thickness scan between 11 and 14 weeks followed by detailed anomaly scan at 20 weeks. Give anti-D if >12 weeks and Rhesus negative
MANAGEMENT OF ABORTION

2. If complete miscarriage (bleeding settled and endometrium <15mm) Reassure and give appropriate written information Give anti-D if> weeks and Rhesus negative Home pregnancy test in 2 weeks
4. Spontaneous incomplete or delayed (missed) or inevitable (cervical os open) miscarriage
A. Exclude Haemodynamically unstable (BP 90/50 mmHg pulse > 100 bpm
Septic (temp >37.50C) Anaemic (Hb <10g/Dl) Significant medical disorder Inform consultant and admit to gynecology ward for surgical management
B. Discuss surgical and conservative treatment and give written information

Conservative managementReview weekly clinically
and serum hCG
Surgical management Organize ERPC
Emergency admission toWard or to DSU
C. Rescan if still bleeding in 2 weeks to confirm complete miscarriage
(endometrium <15mm)
Complete miscarriageHome pregnancy test
2 weeks later
Incomplete miscarriageConsider surgery