Embed Size (px)
Citation preview
Diabetes Emergencies
Diabetic Ketoacidosis, Hyperosmolar Hyperglycaemic State, Hypoglycaemia and Feet!
Dr Kath HigginsClinical Lead Inpatient Diabetes, UHL
OverviewDKA, HHS, Hypo’s and Feet
� Background
� Management
� Challenges / controversies
� Case histories
� Key messages
Diabetic Ketoacidosis Acidosis – acute metabolic decompensation
� Case History 1
� 24yr female – abdo pain, vomiting – 24hrs
� Temp 36.4 RR 40 BP 115/50 Pulse 117
� Looks dehydrated, smells of ketones
� Generally tender abdo
� Na 134 K 6.1 Ur 13.7 Cr 159
� pH 6.9 Bic 5.6 pO2 20.16 pCO2 1.19

DKA - introduction
� DKA is a serious and life threatening complication of Type 1 diabetes
� Mortality from DKA has decreased in past 20 yrs from 10% to 2%
Diabetes NSF Standard 7 (2001) – The NHS will develop, implement and
monitor agreed protocols for rapid and effective treatment of diabetic
emergencies
NICE Quality Standard (2011) - Quality Statement 14 - People admitted to
hospital with diabetic ketoacidosis receive educational and psychological support prior to discharge and are followed up by a specialist diabetes
team
JBDS – The Management of Diabetic Ketoacidosis (DKA) in Adults – Sept 2013
DKA• Predominantly in patients with autoimmune type 1
diabetes
• BUT may also occur in those with:
• “ketosis-prone type 2 diabetes”
• Latent autoimmune diabetes of adults (LADA)

What is the physiology?
• absolute (or relative) insulin deficiency which leads to…….
• reduced peripheral uptake of glucose which leads to hyperglycaemia
and….
• lipolysis and increased mobilisation of FFA from adipose tissue to liver –
switch to free fatty acid metabolism
• production and accumulation of acidic ketone bodies
• 3Bhydroxybutyric acid (Optium plus) and acetoacetic acid (Ketostix)
• Early stages ketone production buffered but when capacity to buffer /
extract ketones is exceeded overt ketosis develops and urine becomes
positive.
•Hypergycaemia/osmotic diuresis/serum hyperosmolality and metabolic
acidosis cause severe electrolyte imbalance.
•Total body potassium loss – normal potassium poorly reflects total body
potassium stores.
•Ketones induce nausea and vomiting – worsens fluid depletion
What are the precipitating factors in DKA?
•Poor compliance – commonest
•New presentation of Type 1 diabetes
•Errors in insulin prescription / management
•Infection
•MI

What are the signs and symptoms?
• osmotic symptoms
• weight loss
• SOB – kussmaul breathing
• abdo pain (especially children)
• cramps
• nausea and vomiting
• confusion, drowsiness, coma
• DKA can develop in <24hrs
• need to make a rapid diagnosis and initiate treatment without delay
DKA� What are the 3 key features to make the diagnosis?
� The triad of uncontrolled hyperglycemia, metabolic acidosis, and increased total body ketone concentration characterizes DKA
� significant ketonuria >++ or blood ketone >3mmol/l
� known diabetes or blood glucose >11mmol/l
� bicarbonate <15mmol/l or venous pH <7.3
� Diabetes Medicine 2005 (22) 221 – 50 patients admitted to ED with high
CBG. Assessed using blood ketone meter. 9 had DKA, 8 compensated
metabolic acidosis, 33 not DKA.
� Ketones >3.0mmol/l 100% sensitive for DKA, 86% specific
Consider other causes of acidosis or ketosis?
Ketosis•Ketotic hypoglycaemia•Alcoholic ketosis•Starvation ketosis – pH rarely <7.3 ketones rarely >2.0mmol/l
Acidosis•Lactic acidosis•Hyperchloraemic acidosis•Salycilate poisoning•Uraemic acidosis
Which 2 feature correlate closely with poor prognosis?
• age and conscious level
What is the typical fluid deficit in DKA?
• 6 litres
• Electrolyte deficits – Na 500 – 1000mmol, K 300 – 1000mmol, Cl
350mmol, Ca 50-100 mmol, PO4 50-100mmol, Mg 25-50mmol
Commonest causes of death?
• Precipitating illnes, hypokalaemia, aspiration and cerebral oedema
Core principles in managing DKA
• restore circulating volume – caution in elderly, young and pregnant
• monitor and replace potassium
• commence iv insulin
• aiming to switch off ketone production and correct metabolic disturbance
• avoid complications of treatment
Principles of Management
JBDS Inpatient Care Group : The Management of Diabetic Ketoacidosis in Adults. March 2010 Revised Sept 2013
•Diagnostic requirement - is this DKA?•Investigation•Assessment of severity – do I need to involve ITU?•Immediate management – first 60mins•Recommended area of care – right place and right team•Management guideline for insulin / fluid / potassium •Guidance on clinical and laboratory monitoring – rigorous monitoring•Confirmation of resolution – ketones <0.6mmol/l, pH >7.3•Involvement of the diabetes team - early•Prevention of future episodes – education, ketone meter, sick day rules
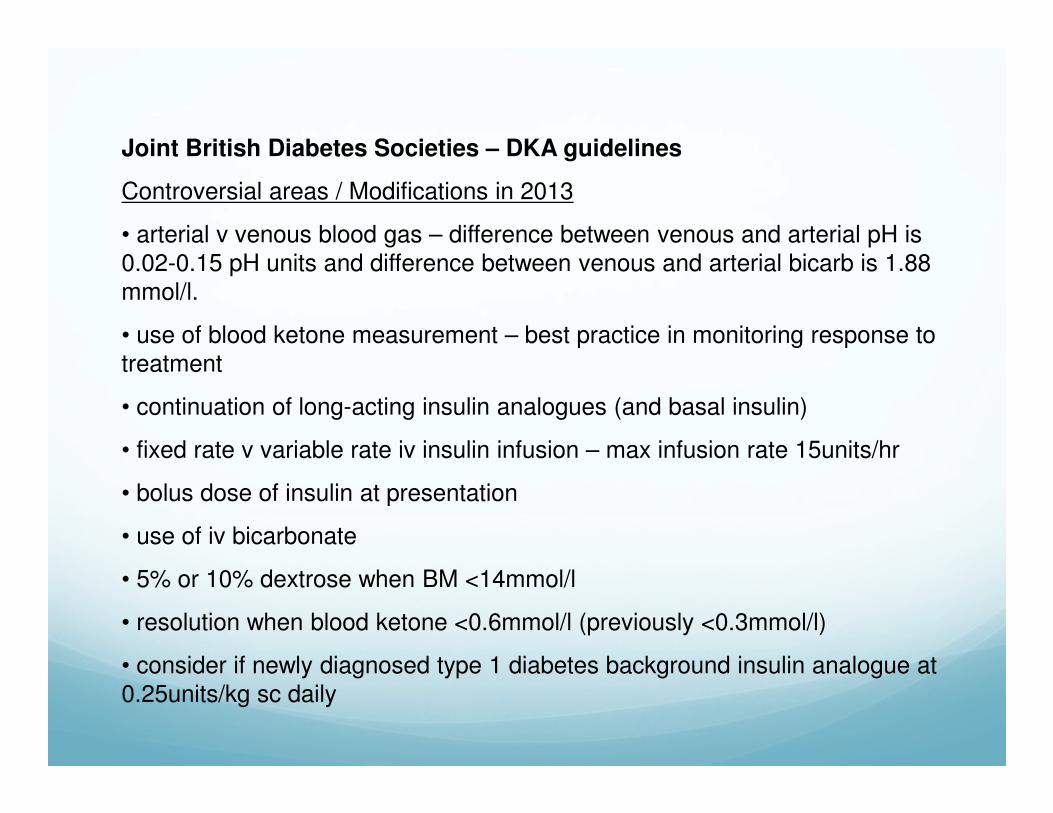
Joint British Diabetes Societies – DKA guidelines
Controversial areas / Modifications in 2013
• arterial v venous blood gas – difference between venous and arterial pH is
0.02-0.15 pH units and difference between venous and arterial bicarb is 1.88
mmol/l.
• use of blood ketone measurement – best practice in monitoring response to
treatment
• continuation of long-acting insulin analogues (and basal insulin)
• fixed rate v variable rate iv insulin infusion – max infusion rate 15units/hr
• bolus dose of insulin at presentation
• use of iv bicarbonate
• 5% or 10% dextrose when BM <14mmol/l
• resolution when blood ketone <0.6mmol/l (previously <0.3mmol/l)
• consider if newly diagnosed type 1 diabetes background insulin analogue at 0.25units/kg sc daily

Regular assessment of clinical and biochemical parameters
Avoid complications of treatment

How well do we do?
National DKA Survey – 2014N=281
Time to N Saline – 41minsTime to iv insulin – 60mins
Resolution at 18hrLOS 2.6 days
Hypoglycaemia – 27%Hypokalaemia – 55%
95% seen by specialist team
Dhatariya KK et al. Diabet Med 2015.

Education and prevention
Discuss precipitating cause and early warning symptoms of DKA
•Sick day rules
•Review of insulin regime
•Provision of blood ketone meter and education on use
Diabetes Medicine 2006 (23) 278 – In 123 young adults and children
with Type 1 diabetes, 62 were taught how to use a blood ketone meter,
61 used urine testing. 50% reduction in days spent in hospital in group
using blood ketone meter
•Education of staff, patient and family
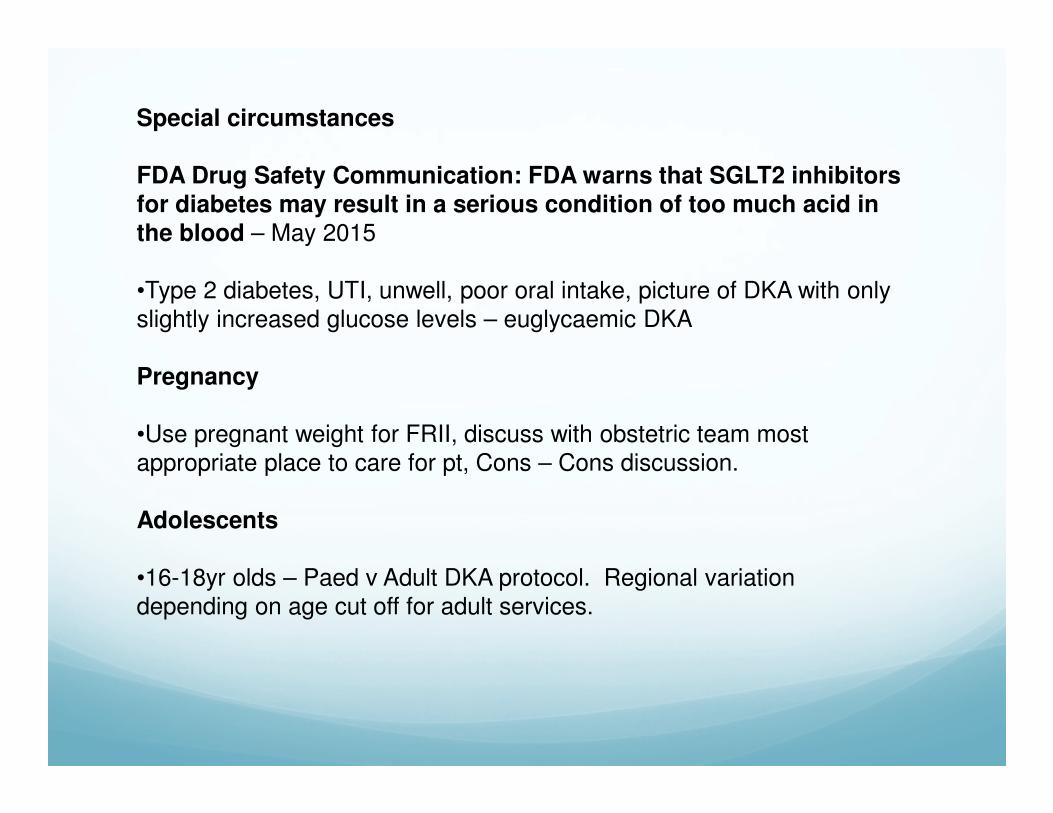
Special circumstances
FDA Drug Safety Communication: FDA warns that SGLT2 inhibitors for diabetes may result in a serious condition of too much acid in the blood – May 2015
•Type 2 diabetes, UTI, unwell, poor oral intake, picture of DKA with only
slightly increased glucose levels – euglycaemic DKA
Pregnancy
•Use pregnant weight for FRII, discuss with obstetric team most
appropriate place to care for pt, Cons – Cons discussion.
Adolescents
•16-18yr olds – Paed v Adult DKA protocol. Regional variation
depending on age cut off for adult services.

Demonstration of the cascade of clinical events and metabolic changes that contribute sequentially to progressive clinical deterioration and development of full-blown episodes of
euDKA.
Julio Rosenstock, and Ele Ferrannini Dia Care 2015;38:1638-1642
©2015 by American Diabetes Association
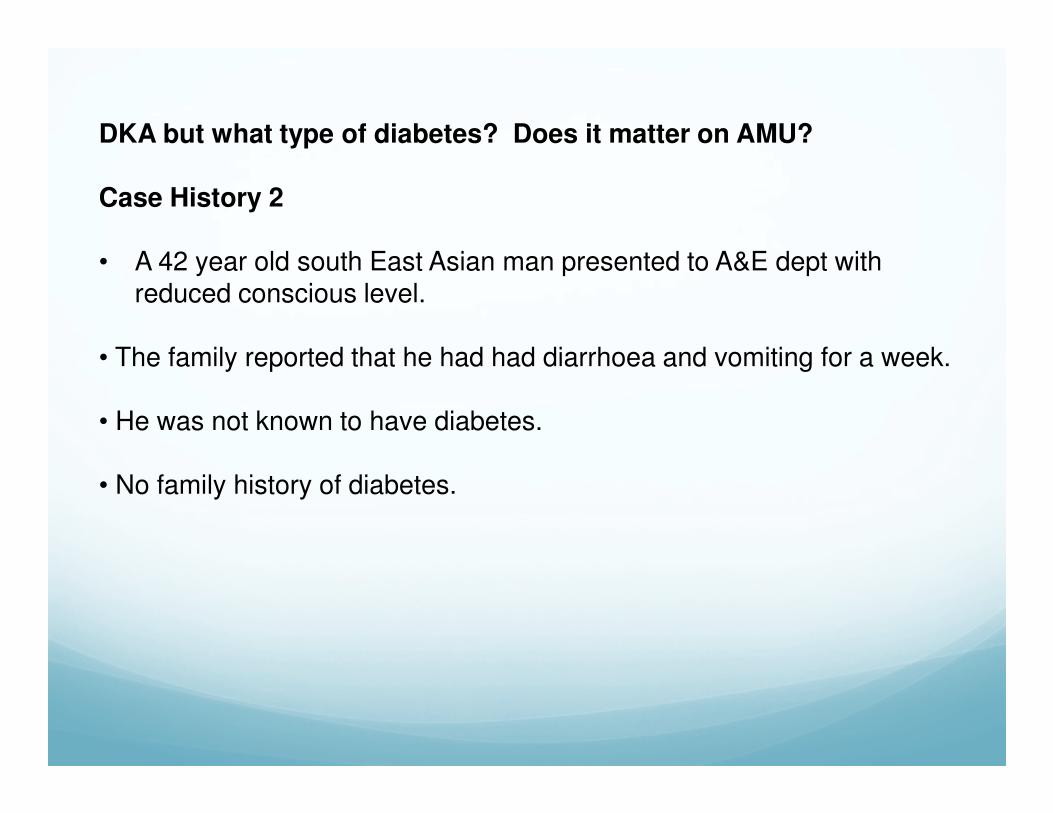
DKA but what type of diabetes? Does it matter on AMU?
Case History 2
• A 42 year old south East Asian man presented to A&E dept with reduced conscious level.
• The family reported that he had had diarrhoea and vomiting for a week.
• He was not known to have diabetes.
• No family history of diabetes.
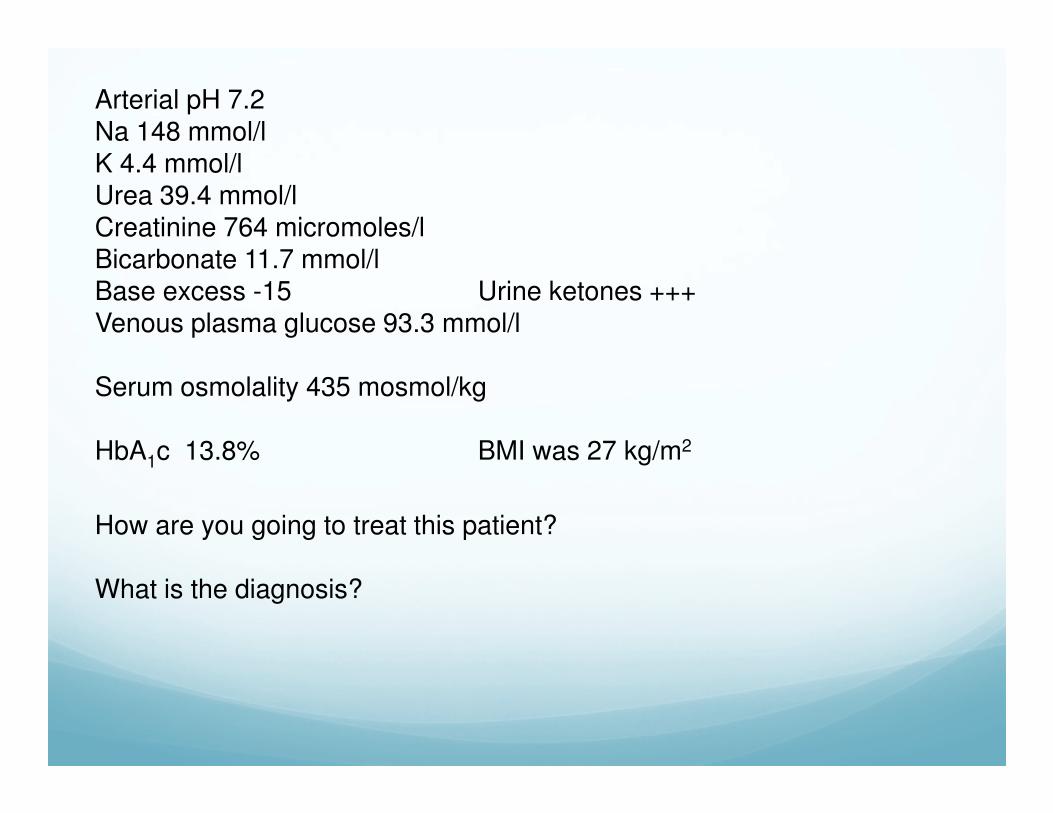
Arterial pH 7.2Na 148 mmol/l K 4.4 mmol/lUrea 39.4 mmol/lCreatinine 764 micromoles/lBicarbonate 11.7 mmol/lBase excess -15 Urine ketones +++Venous plasma glucose 93.3 mmol/l
Serum osmolality 435 mosmol/kg
HbA1c 13.8% BMI was 27 kg/m2
How are you going to treat this patient?
What is the diagnosis?
Diagnosis – Type 1.5 / Type 1B / Atypical DM / Flatbush diabetes
Ketosis Prone Diabetes
Heterogenous group of patients presenting in DKA that do not fit the
traditional autoimmune classification of diabetes
More common in African, African-American and Hispanic people and young “type 2” phenotype pts
Hyperglycaemia _> glucose toxicity which results in acute impairment of B-
cell function which resolves when glucose levels return to normal.
Negative autoantibodies
Improve significantly with return to normoglycaemia and have a temporary
insulin requirement
P Chellmutha et al. Practical Diabetes International 2010; 27(3): 118-119.
Case History 3
• 76-year-old caucasian lady referred with uncontrolled diabetes.
• Diagnosed with type 2 diabetes in 2006.
• Had been controlled on diet alone.
• Over the previous two weeks she had become more and more lethargic with polyuria, polydipsia, loss of appetite and nausea.
• Had lost 1.5 stones over the previous 10 months.

• O/E - Thin lady, weight 45 kg, BMI 17 kg/m2
• Smelled of ketones
• Urinalysis showed 3+ glucose and 3+ ketones.
• Arterial pH 7.241• Bicarbonate 12 mmol/l• Sodium 129 mmol/l• Potassium 4.9 mmol/l• Urea 29.3 mmo/l• Creatinine 213 micromol/l• Blood glucose 59.3 mmol/l
• Treated for diabetic ketoacidosis.
• Made an uneventful recovery.
• Discharged home 5 days later on 16 U of insulin/day.
• Reviewed in the outpatient clinic 2 months later
• Had gained 14 kg. HbA1c was 6.8%.
• Anti-GAD antibody checked - strongly positive.
•What is the diagnosis?

• Diagnosis of latent autoimmune diabetes in adults (LADA) was made.
• Of note is that she had a nephew with type 1 diabetes and her grandfather also had diabetes but she could not ascertain whether it was Type 1 or Type 2.
• Form of Type 1 diabetes which occurs in adults often with slower onset. Despite presence of islet cell antibodies at diagnosis of diabetes, the progression of autoimmune B-cell failure is slow
• It is estimated that 20% of persons diagnosed as having non-obesity-related type 2 diabetes may actually have LADA.
• New onset diabetes in the elderly is not always Type 2
DKA but what type of diabetes? Does it matter on AMU?
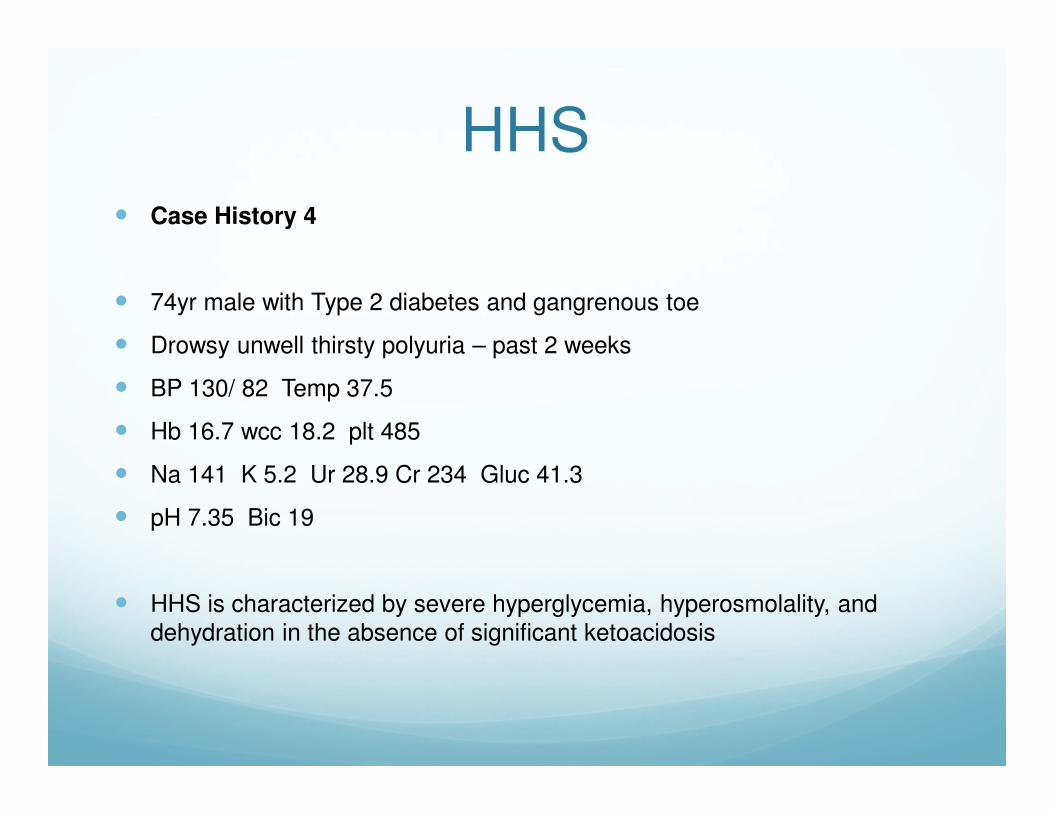
HHS� Case History 4
� 74yr male with Type 2 diabetes and gangrenous toe
� Drowsy unwell thirsty polyuria – past 2 weeks
� BP 130/ 82 Temp 37.5
� Hb 16.7 wcc 18.2 plt 485
� Na 141 K 5.2 Ur 28.9 Cr 234 Gluc 41.3
� pH 7.35 Bic 19
� HHS is characterized by severe hyperglycemia, hyperosmolality, and dehydration in the absence of significant ketoacidosis
• Type 2 diabetes – pathophysiology less well understood
• acute illness with relative insulin deficiency – endogenous insulin secretion is present
• insulin resistance increases with acute illness
• insulin levels in HHS are inadequate to facilitate glucose utilization by insulin
sensitive tissues but adequate to prevent lipolysis and subsequent ketogenesis
• usually associated with an inter-current illness
• Greater degree of dehydration (due to osmotic diuresis) and differences in insulin availability distinguish it from DKA
Ketosis not present as insulin inhibits lipolysis
HHS
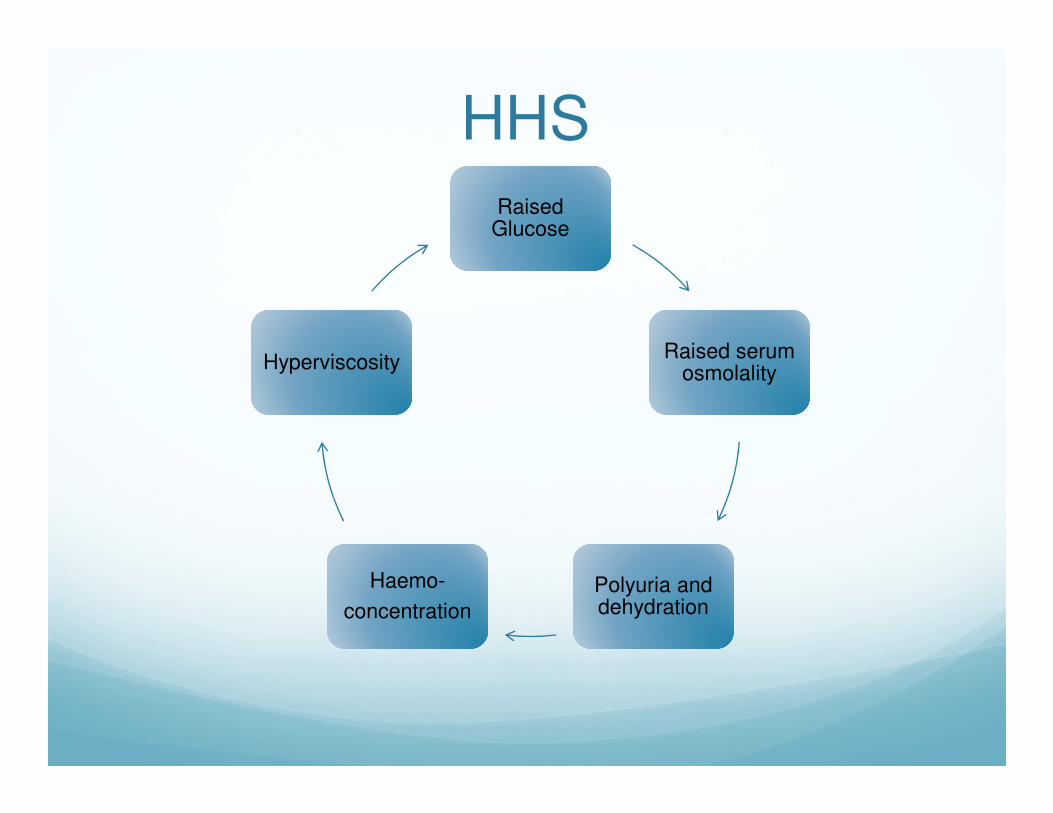
Raised Glucose
Raised serum osmolality
Polyuria and dehydration
Haemo-
concentration
Hyperviscosity
HHS
What features support the diagnosis of HHS?
•BM > 30mmol/l (often >50 mmol/l)
• without significant acidosis or ketonaemia
• serum osmolality >320mmol/l ( 362.6mmol/l)
• osmolality = 2(Na + K) + Ur + Gluc
• 50% of patients are hypernatraemic
What are the signs and symptoms?
• disordered mental functioning
• neurological symptoms
• coma
• renal impairment
• related to precipitating illness
There is usually a precipitating event or inter-current illness
JBDS The Management of the Hyperosmolar Hyperglycaemic state (HHS) in adults with diabetes - 2012
Immediate investigation and prinicples of management
• ABC
• iv cannulation and fluid replacement – review according to change in osmolality
• clinical assessment – consider severity and precipitants
• U&E, Glucose, venous blood gas, urine dip and MSU, blood cultures, ECG,
CXR – calculate osmolality
• pulse oximetry
• iv insulin infusion – low dose 0.05units/kg/hr if blood ketones >1or >++ or if
despite fluid BG falling <5 mmol/hr
• monitor and replace potassium
• consider antibiotics
• stop metformin
• LMWH
• urinary catheter protect heels and daily foot checks Diabetes team
What is the mortality of HHS?
• up to 50%
• consider level 2 environment if indicators of severe episode – osmolality >350mmol/l, Na >160mmol/l, pH <7.1
What is the typical fluid deficit in HHS?
• 10 litres – caution in frail and elderly – may need CVP line
How long does it take for normalisation of physiology?
•Up to 72hrs
What are the commonest causes of death in HHS?
• underlying pathology
• thrombo-embolic complications
• aspiration pneumonia
Controversies and special circumstances
Isotonic v hypotonic fluid replacement
•0.9% saline is principle fluid used. As osmolality falls glucose shifts to intracellular space and Na may rise – not an indication for hypotonic fluid
•If osmolality fails to fall despite adequate 0.9% saline AND adequate fall
in glucose not achieved the 0.45% saline should be substituted
Prophylactic or treatment dose LMWH
•national guidance advises prophylactic dose. Wandsworth et al, BJDVD 2014;14(2):64-66 discuss reviewing on a individual pt basis and using
treatment dose unless high risk of bleeding
Diabetes treatment following recovery
•Majority of pts require insulin on discharge - insulin resistance associated with acute illness can persist for up to 30 days
HHS
A slow and measured approach is required for best outcome
Hypoglycaemia
1 jelly baby = ? g of carbohydrate
What is hypoglycaemia?
•DUK - <4mmol/l•DAFNE - <3.5mmol/ADA - <3.9mmol/l
•DVLA – 4mmol/l or less
Mild Hypoglycaemia – self treated episode
Severe Hypoglycaemia – requiring third party assistance
JBDS – Hospital management of hypoglycaemia in adults with diabetes
Hypoglycaemia

Symptoms of hypoglycaemia
� As plasma glucose levels drop hypoglycaemic symptoms develop:
� Autonomic symptoms: sweating, palpitations, pallor, tremours, nausea, irritability, hunger1,2
� Neuroglycopenic symptoms: inability to concentrate, confusion, drowsiness, personality change, slurred speech, incoordination, weakness, dizziness, vision impairment, headache, seizures, coma1,2
� Generally in diabetic patients autonomic symptoms occur before neuroglycopenic symptoms, but in non-naïve patients the neuroglycopenic symptoms may occur at the same time or perhaps even earlier than the autonomic symptoms1,2
1. Barnett et al. Int J Clin Pract. 20102. McAulay et al. Diabetic Medicine. 2001; 18:690-705
Risk factors for hypoglycaemia – consider when reviewing pt.
•History of previous severe hypoglycaemia
•Duration of diabetes or insulin treatment in Type 2
•Strict control•Impaired awareness of hypoglycaemia•Increased age
•Poor cognitive function
•Poor sleep pattern
•Lipohypertrophy
Common causes of hypoglycaemia•Missed or delayed meal / eating less than planned / fasting•Alcohol
•Unplanned exercise Early pregnancy/breast feeding
•Medication error•Weight loss Food malabsorption
•Hot weather•Changing injection site
Morbidity associated with severe hypoglycaemia
Neurological
• Coma / convulsions
• hemiplegia, TIA, focal lesions• Cognitive impairment
Cardiac• Arrythmias• Myocardial ischaemia / infarction
• Cardiac failure
Accidents• Fractures / joint dislocation, head injuries
• RTA
Hypoglycaemia – the economic cost
•In the UK cost of a severe hypoglycaemic event resulting in admission to
hospital is approx £1,300. If treated by a community based HCP cost is
approx £360.
Hypoglycaemia – the personal cost
•Fear of further events, days off work, injury, loss of driving license
Impaired awareness of hypoglycaemia
� Hypoglycaemia-associated autonomic failure (HAAF) – reduced counter-regulatory response to hypos and reduced hypoawareness
� Acquired syndrome associated with insulin treatment
� Leads to reduction in intensity of warning symptoms of hypoglycaemia
� Altered in nature or lost completely
� Individuals are rendered at risk of progression to severe hypoglycaemia
� Prevalence increases with duration of diabetes and more common in type 1 diabetes than type 2
� Always ask patients regarding presence of symptoms of hypoglycaemia and document
Driving and hypoglycaemia
� Must have adequate awareness of hypoglycaemia
� Must not have had >1 episode of severe hypoglycaemia in preceding 12 months
� Always ask patients regarding presence of symptoms of hypoglycaemia and document
Hypoglycaemia in young pts with Type 1 diabetes -Dead in Bed Syndrome
� Sudden unexplained death of young people with type 1 diabetes
� Accounts for 6% of all deaths in people with type 1 diabetes under age of
40yrs
� Thought to be associated with HAAF
� Data* suggests that the excess mortality attributable to hypoglycaemia
secondary to dysrrhthmias, hyperkalaemia, cardiac ischaemia - “Dead in
Bed” syndrome.
� * The ACCORD Study Grp, NEJM 2008;358:2545-2559.
Risk factor: Age
Hypoglycaemia in the elderly
� Advanced age is a risk factor for hypoglycaemia1
� Symptoms of hypoglycaemia in elderly patients can include neuroglycopenic symptoms, such as weakness, drowsiness, poor concentration, dizziness and confusion and neurological symptoms such as blurred vision, lack of co-ordination and slurred speech2
� Many of the prominent symptoms of hypoglycaemia in elderly people may be misinterpreted as other neurological conditions such as transient cerebral ischaemia, vertebrobasilar insufficiency or vasovagal attacks2
� Elderly people may, in general, have reduced awareness of hypoglycaemia symptoms3
1. Amiel SA et al. Diabet Med. 2008;25(3):245–254
2. McAulay et al. Diabetic Medicine. 2001; 18:690-705
3. Matyka K et al. Diabetes Care. 1997; vol 20;2:135-141
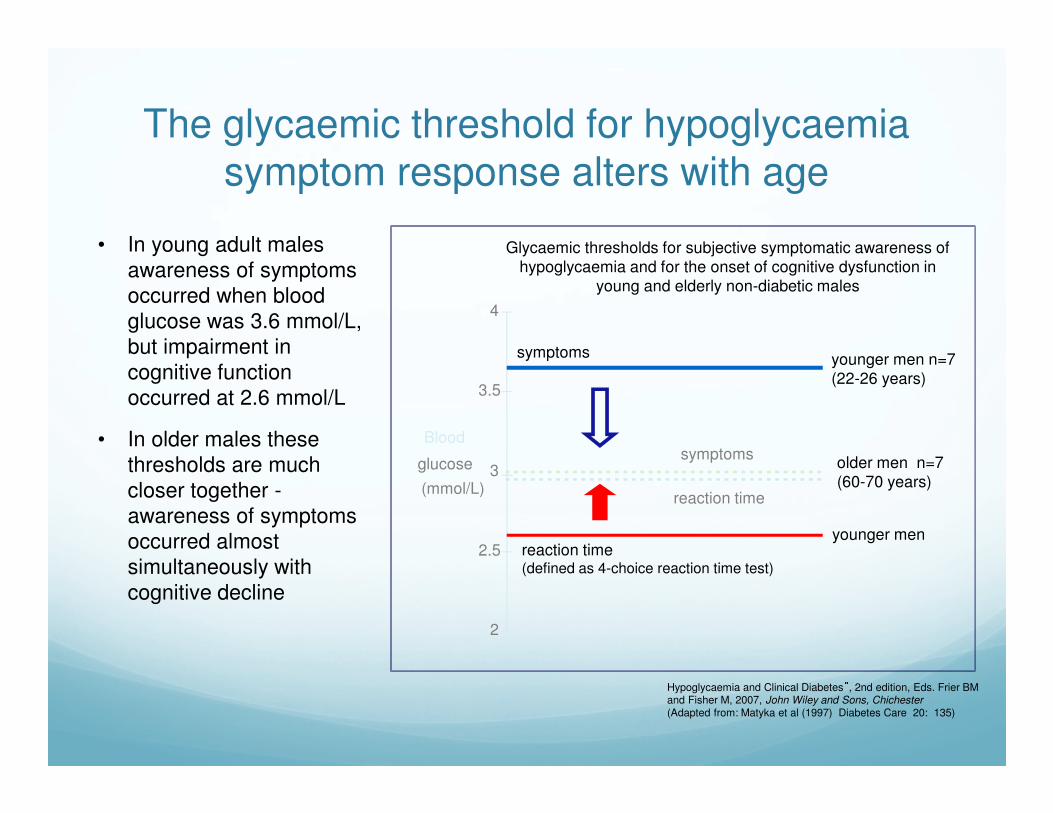
The glycaemic threshold for hypoglycaemia symptom response alters with age
Hypoglycaemia and Clinical Diabetes”, 2nd edition, Eds. Frier BM and Fisher M, 2007, John Wiley and Sons, Chichester (Adapted from: Matyka et al (1997) Diabetes Care 20: 135)
• In young adult males
awareness of symptoms
occurred when blood
glucose was 3.6 mmol/L,
but impairment in
cognitive function
occurred at 2.6 mmol/L
• In older males these
thresholds are much
closer together -
awareness of symptoms
occurred almost
simultaneously with
cognitive decline
2
2.5
3
3.5
4
Blood
glucose
(mmol/L)
symptoms
reaction time(defined as 4-choice reaction time test)
younger men n=7(22-26 years)
older men n=7(60-70 years)
younger men
Glycaemic thresholds for subjective symptomatic awareness of hypoglycaemia and for the onset of cognitive dysfunction in
young and elderly non-diabetic males
symptoms
reaction time
Glycaemic targets in the Elderly
� Functionally independent – 7.0 – 7.5%
� Functionally dependant – 7.0 – 8.0%
� If admitted with hypoglycaemia review HbA1c and medication –avoid further episodes of hypoglycaemia
� End of life care – avoid symptomatic hyperglycaemia – DUK End of Life Diabetes Care – clinical care recommendations
IDF Global Guideline for Managing Older
People with Type 2 Diabetes 2012

Admission avoidance
•EMAS pathway / Ambulance service pathway
•ED / EDU pathway
Hypoglycaemia – severe – when to admit
•poorly responsive to first line treatment•persistent
•insulin overdose
•oral hypoglycaemic agents esp in elderly
•ultra-long acting insulins• with intercurrent illness (CKD, Addisons, liver disease)
Safe discharge and prevention
•Identify any obvious modifiable precipitants - education
•Review and reduce diabetes treatment
•Refer to DSNs to ensure patient contact within 48hrs of discharge

Feet
� Majority of primary diabetes admissions are for foot disease
� Classical “crash landers” to ED or AMU
� 1 in 3 people with diabetes have PAD
� 10% of pts with diabetes will have a foot ulcer in lifetime
� 80% amputations are preceded by an ulcer
� Variation in care is correlated with outcomes

Feet – Management of Diabetic foot
problems – NICE guidance CG19 (2015)
� Every hospital should have a care pathway for pts requiring inpatient care
� Remove shoes, socks and dressings on both feet and examine both feet on admission and daily thereafter
� Refer to member of MDT foot team within 24hrs of initial examination – IMMEDIATELY if limb threatening problem (ulceration with spreading infection/sepsis, deep seated soft tissue or bone infection, critical ischaemia, gangrene or suspicion of acute Charcot arthropathy)
� Every hospital should have agreed antibiotic guidelines
Feet can deteriorate very quickly in hospital - do not delay treatment and ensure preventative measures are in place
OverviewDKA, HHS, Hypoglycaemia and Feet
� Background
� Management
� Challenges / controversies
� Case histories
� Time for your long acting CHO !!
Thank you