Embed Size (px)
Citation preview

Dr lina haffar
Pr of pathology
1

Oral Cavity
Oral Inflammatory Lesions
Leukoplakia
Squamous Cell Carcinoma
Diseases of Salivary Glands
Esophagus
Esophagitis
Eosinophilic Esophagitis
Barrett Esophagus
Esophageal Tumors
Adenocarcinoma
Squamous Cell Carcinoma
Stomach
Gastropathy and Acute Gastritis
Stress-Related Mucosal Disease
Chronic Gastritis
Helicobacter pylori Gastritis
Autoimmune Gastritis
Complications of Chronic Gastritis
Peptic Ulcer Disease
Mucosal Atrophy and Intestinal Metaplasia
Dysplasia
plications of Chronic Gastritis
Gastric Polyps and Tumors
Gastric Polyps
Gastric Adenocarcinoma
Lymphoma
Gastrointestinal Stromal Tumor
Small and Large Intestines
Intestinal Obstruction
Hirschsprung Disease
Ischemic Bowel Disease
Malabsorptive Diarrhea
Infectious Enterocolitis
Inflammatory Intestinal Disease
Sigmoid Diverticulitis
Inflammatory Bowel Disease
Colonic Polyps and Neoplastic Disease
Inflammatory Polyps
Hamartomatous Polyps
Hyperplastic Polyps
Adenomas
Adenocarcinoma
Appendix
Acute Appendicitis
Tumors of the Appendix
2

• Leukoplakia• Leukoplakia is a clinical term used to describe patches of
keratosis.
• it can be premalignant.
• Hyperkeratosis and hyperplasia of the squamous epithelium
• In the UK and USA leukoplakia is associated with heavy cigarette smoking, excessive alcohol consumption and poor dental hygiene.
• The high incidence in India and Sri Lanka is attributed to the habit of chewing betel quids made up of tobacco dust,…..
3

1. Pleomorphic adenoma: a benign mixed tumour
2. Warthin's tumour (adenolymphoma): a benign tumour
3. Muco-epidermoid tumour: benign and malignant
4. Adenoid cystic carcinoma: malignant with tendency for perineural invasion
• Pleomorphic adenoma
• At least two-thirds of all salivary tumours
• Composed of a mixture of stromal and epithelial elements
• The facial nerve is vulnerable during attempts at surgical removal.
• A very small proportion undergo malignant change and are capable of metastasizing
4

The squamous lining of the esophagus consists of a layer of non-keratinizing squamous epithelium
overlying connective tissue papillae containing blood vessels and lymphatics
5
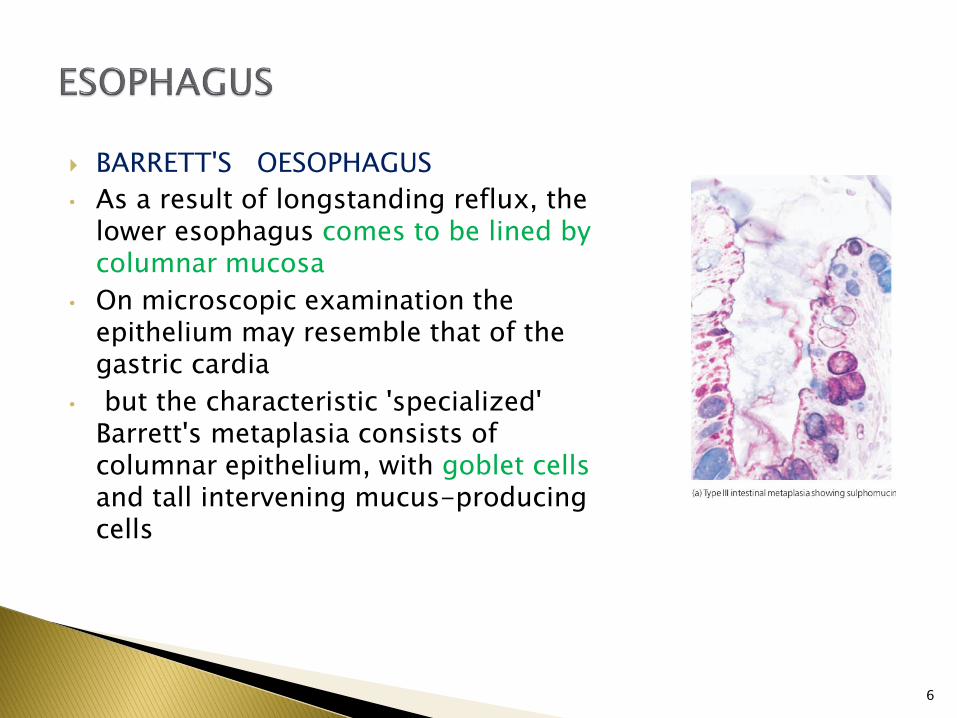
BARRETT'S OESOPHAGUS
• As a result of longstanding reflux, the lower esophagus comes to be lined by columnar mucosa
• On microscopic examination the epithelium may resemble that of the gastric cardia
• but the characteristic 'specialized' Barrett's metaplasia consists of columnar epithelium, with goblet cells and tall intervening mucus-producing cells
6
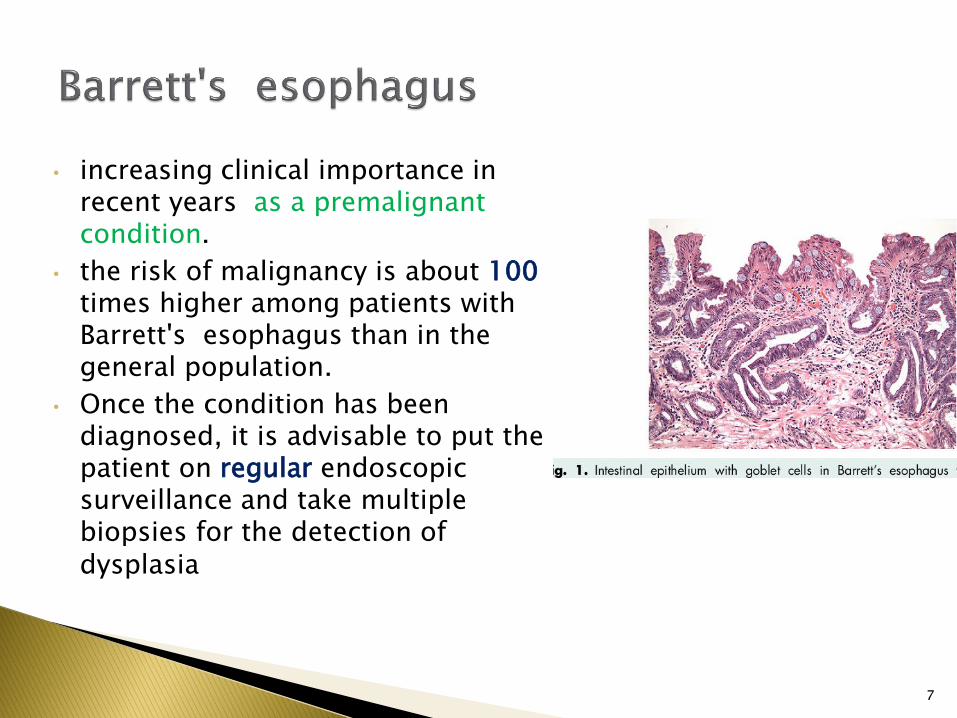
• increasing clinical importance in recent years as a premalignant condition.
• the risk of malignancy is about 100times higher among patients with Barrett's esophagus than in the general population.
• Once the condition has been diagnosed, it is advisable to put the patient on regular endoscopic surveillance and take multiple biopsies for the detection of dysplasia
7

Most malignant tumors are Carcinoma. Two main types :
squamous carcinoma and adenocarcinoma
Most adenocarcinomas arise from metaplastic columnar epithelium (Barrett's esophagus)
Squamous carcinoma is much more common in males than females
8

Squamous Carcinoma : Epidemiological studies in high-incidence areas have
indicated that a high dietary intake of tannic acid, in the form of strong tea or sorghum wheat, or dietary deficiencies of riboflavin, vitamin A and possibly zinc may be important,
In Western countries, cigarette smoking and the drinking of alcoholic spirits are associated with a higher incidence
A factor of current interest is the possible involvement of HPV.
9

Adenocarcinoma• In the lower third of the esophagus
adenocarcinomas are the predominant type
• They almost invariably develop on the basis of a Barrett's esophagus and their incidence has risen dramatically in recent years among white, middle-aged men in European countries and the USA
10

Histologically, the stomach can be divided into three regions-the cardia, body and antrum. The surface of the gastric mucosa and its pits (foveolae) are lined throughout by columnar mucus-secreting epithelium. The mucus forms a viscid gel covering the mucosa-the gastric mucus barrier
11

INFLAMMATORY DISORDERS
• Acute gastritis is commonly due to chemical injury (e.g. alcohol, drugs)
• Commonest form of chronic gastritis results from Helicobacter pylori HP infection
• Chronic gastritis can also result from an autoimmuneprocess, often causing vitamin B12 deficiency
• Chemical (reactive) gastritis is caused by biliary regurgitation or drug-induced damage
12

Acute gastritis
• An acute neutrophilic gastritis is characteristic of the initial response to Helicobacter pylori infection.
• Acute Helicobacter gastritis HP is a transient phase .
• over the course of 3-4 weeks gives way to chronic gastritis.
• In a minority of individuals the infection is spontaneously eradicated and the inflammatory response resolves
13
Chronic gastritis
Autoimmune chronic gastritis :
• A few patients have antibodies in serum directed against gastric parietal cells.
• These patients exhibit hypochlorhydria and a macrocytic anemia resulting from vitamin B12 deficiency;
this association of autoimmune gastritis with macrocytic anemia is called pernicious anemia
Histologically : marked loss of specialized cells (glandular atrophy) and fibrosis with an infiltrate of lymphocytes and plasma cells + intestinal metaplasia (IM),
14

Clinical consequences
Histological findingsPathogenic mechanisms
Etiology
Peptic ulceration (duodenal/gastric ulcer)?Gastric cancer
Active chronic inflammationMultifocal atrophy: antrum > bodyIntestinal metaplasia
CytotoxinsLiberation of chemokinesTissue damage by immune response
Bacterial infection (H. pylori)
Gastric erosionsGastric ulcer
Foveolar hyperplasiaedemaVasodilatationPaucity of inflammatory cells
Direct injuryDisruption of the mucus layerDegranulation of mast cells
Chemical injuryNSAIDsBile reflux?Alcohol
15

• Major sites :
first part of duodenum, junction of antral and body mucosa in stomach, ….
• Main etiological factors:
hyperacidity, Helicobacter gastritis, duodenal reflux, NSAIDs, smoking and genetic factors
• Ulcers may be acute or chronic
• Complications include hemorrhage, penetration of adjacent organs, perforation, anemia, obstruction due to fibrous strictures, and malignancy
• Peptic ulceration is a breach in the mucosa lining the alimentary tract as a result of acid and pepsin attack.
16

17
• Acute ulcers :
Acute peptic ulcers develop as part of an acute gastritis as a complication of a severe stress response as a result of extreme hyperacidity
• Deeper extension of the erosions in acute gastritis resulting from NSAIDsor acute alcohol over dosage can produce frank ulcers
• most ulcers respond initially to anti-acid treatment

• Chronic ulcers :
• Pathogenesis:• For many years peptic ulceration has been attributed to
excessive acid production
• People with gastric ulcers frequently have normal or even subnormal acid production
• Failure of the mucosal defense mechanisms means that ulcers can result from normal or even decreased
quantities of acid.
18

Morphology• Grossly, chronic peptic ulcers are
usually less than 20 mm but they may be larger and can exceed 100 mm .
• The edges are clear-cut and overhang the base
• Microscopically, the base consists of necrotic tissue and polymorph exudate overlying inflamed granulation tissue which merges with mature fibrous (scar) tissue
19

• More immediate complications of peptic ulcers include :
• Perforation, giving rise to spillage of gastric contents into the peritoneal cavity and peritonitis
• Penetration, whereby the ulcer erodes into an adjacent organ such as the liver or pancreas
• Hemorrhage, from eroded vessels in the ulcer base
• Although malignant change is claimed to occur in gastric peptic ulcers
20

• Uncommon in most Western countries
• frequent in Japan and other countries with a high incidence of gastric cancer.
• When polypoid, these tumors have a strong potential for malignant change 40% will be found to contain carcinoma on microscopic examination.
• Flat adenomas with lower malignant potential
21

• In addition to atrophy and intestinal metaplasia in chronic H. pylori gastritis,
• a higher incidence of gastric cancer is seen in patients with pernicious anemia
• Genetic factors are likely to be involved : link with blood group A and the appearance of frequent gastric cancers in certain families at a young age
Gastric cancers are classified as either 'early' or 'advanced' on the basis of direct spread through the stomach wall
Early gastric cancer is confined to either the mucosa (intra-mucosal carcinoma) or submucosa;
advanced tumors extend into or beyond the main muscle coats
22

• Second most common fatal malignancy (after lung cancer)
• H. pylori plays a major role.
• a sequence of events, (chronic gastritis , atrophy and intestinal metaplasia , premalignant dysplasia) precursor to cancer
Several molecular genetic changes have been demonstrated :
• mutations and deletions of tumor suppressor genes, notably p53, K-ras ,.
• Over-expression of oncogenes like c-myc and erbB-2
23

Carcinoma of the stomach• Majority are adenocarcinomas
• Many arise on a background of chronic gastritis and intestinal metaplasia
• Most cases present when clinically advanced
• Early cases (carcinoma confined to mucosa or submucosa) have a good prognosis
• All gastric ulcers must be regarded as potentially malignant
• There is a notably high incidence in Japan, China, Colombia and Finland
24

PROGNOSIS :
Intestinal-type gastric carcinomas carry a better prognosis than the diffuse type
COMPLICATIONS :
Carcinomas spread directly to involve the serosa, which can lead to peritoneal dissemination.
This can result in the formation of a malignant effusion (ascites) or involvement of other organs by transcoelomic spread, of which metastases in the ovaries (Krukenberg tumors) are a classical example
25

26
Gastrointestinal Stromal tumors GIST
Stromal tumors are of unpredictable behavior and it is difficult to distinguish between benign and malignant tumors on histological criteria
Approximately 45% of these are malignant and can give rise to metastases.
• present with symptoms referable to secondary ulceration( hemorrhage, anemia, anorexia and weight loss….

27
Gastrointestinal Stromal tumors GIST
• Endoscopically they protrude into the lumen and often have a central deep ulcer crater.
• Malignancy is recognized by the presence of metastases OR , by increased mitotic activity in tumor tissue
• CONFIRMED DIAGNOSIS BY IHC :
CD117 (Ckit ); POSITIVE .
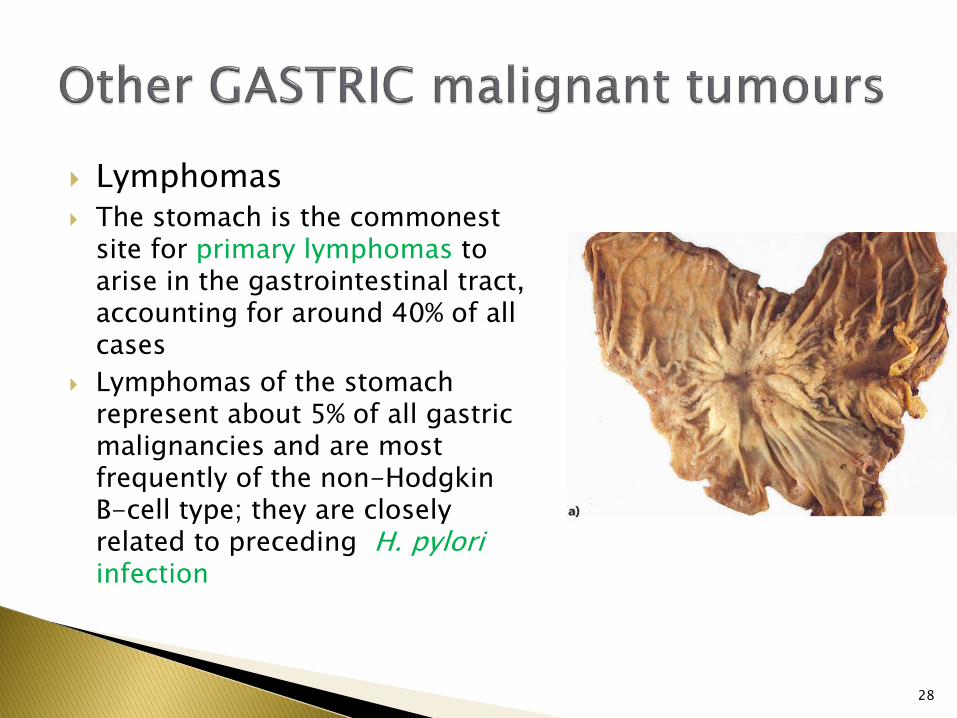
Lymphomas The stomach is the commonest
site for primary lymphomas to arise in the gastrointestinal tract, accounting for around 40% of all cases
Lymphomas of the stomach represent about 5% of all gastric malignancies and are most frequently of the non-Hodgkin B-cell type; they are closely related to preceding H. pyloriinfection
28
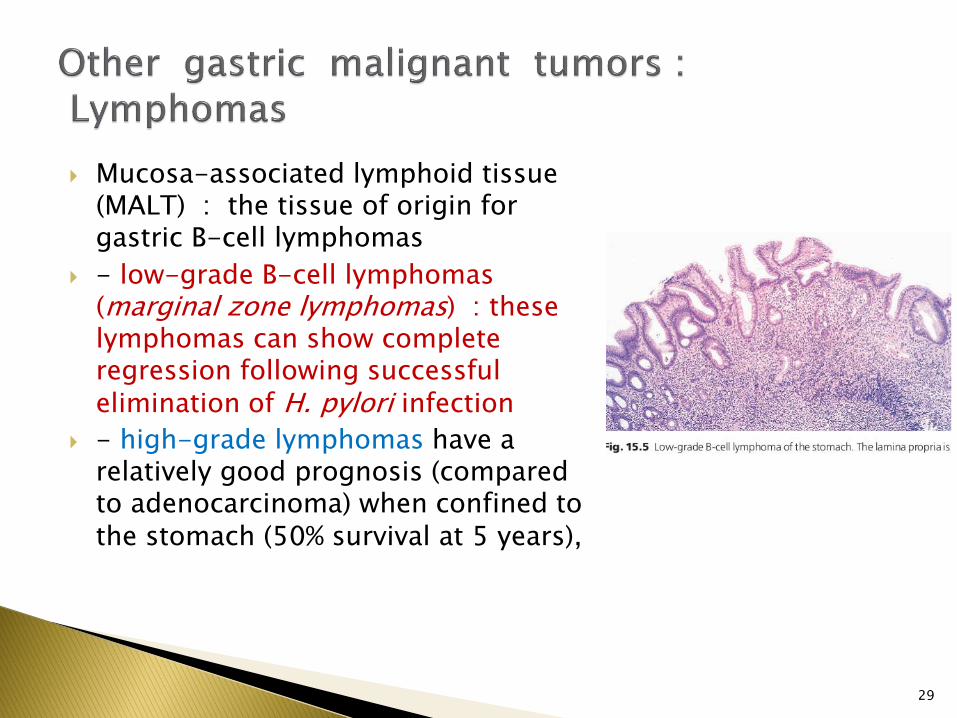
Mucosa-associated lymphoid tissue (MALT) : the tissue of origin for gastric B-cell lymphomas
- low-grade B-cell lymphomas (marginal zone lymphomas) : these lymphomas can show complete regression following successful elimination of H. pylori infection
- high-grade lymphomas have a relatively good prognosis (compared to adenocarcinoma) when confined to the stomach (50% survival at 5 years),
29

MALABSORPTION
Small-intestinal causes include:
• coeliac disease, the major small-intestinal cause of malabsorption in Western countries
• extensive surgical resection, for example in patients with Crohn's disease
• lymphatic obstruction, which gives rise to a protein-losing state
• 'blind loop syndrome', where bacterial overgrowth in partly obstructed or bypassed loops robs the patient of vital nutrients
30
Mild malabsorptionsometimes occurs in
giardiasis

31
• Results from sensitivity to gluten in cereals
• Diagnosis by finding villous atrophy and crypt hyperplasia on duodenal or jejunal biopsy
• Coeliac disease is due to an abnormal reaction to a constituent of wheat flour, gluten, which damages the surface enterocytes of the small intestine and severely reduces their absorptive capacity

• The toxic component of gluten is probably gliadin
• There is an increase in intraepithelial lymphocytes (IELs) in this condition and an increased of T-lymphocytes among the IELs
• Genetic factors are also involved and there is a strong association with HLA-B8:
Morphology
• Shrinkage of villi and reduction in epithelial surface area
• hypercellularity and high mitotic activity of the crypts (crypt hyperplasia
• The degenerate surface epithelium is infiltrated by large numbers of T-lymphocytes (IELs).
32

• This was the form of infection characteristic of bovine tuberculosis
• eliminated from the UK through the introduction of tubercle-free herds of cattle and the pasteurization of milk
• Secondary tuberculous enteritis is a complication of extensive pulmonary tuberculosis which results from the swallowing of infected sputum.
Ileo-caecal tuberculosis is a distinctive form of infection consisting of an ulcerative, granulomatous and fibrotic process occurring around the ileo-caecal valve
33

34
• is a disease of the large intestine resulting from infection with the protozoan Entamoeba histolytica.
• more prevalent in the tropics than in temperate climates.
• Vegetative forms in the large bowel • Contamination of food and water by
human carriers, infected rats, or flies.• Carriers may either be individuals
known to have suffered an attack in the past, or be apparently healthy people, some of whom may have symptomless lesions in the bowel

The term chronic (idiopathic) inflammatory bowel disease‘ IBD
embraces two conditions: Crohn's disease and ulcerative colitis
Crohn's disease• Chronic inflammatory disorder of
unknown etiology • Small bowel most commonly affected, but
any part of the gut may be involved • Characterized by transmural inflammation
with granulomas • Thickened and fissured bowel leads to
intestinal obstruction and fistulation• Etiology and pathogenesis :a higher
prevalence of HLA-DR1 and DQw5 has been found in Crohn's disease.
35
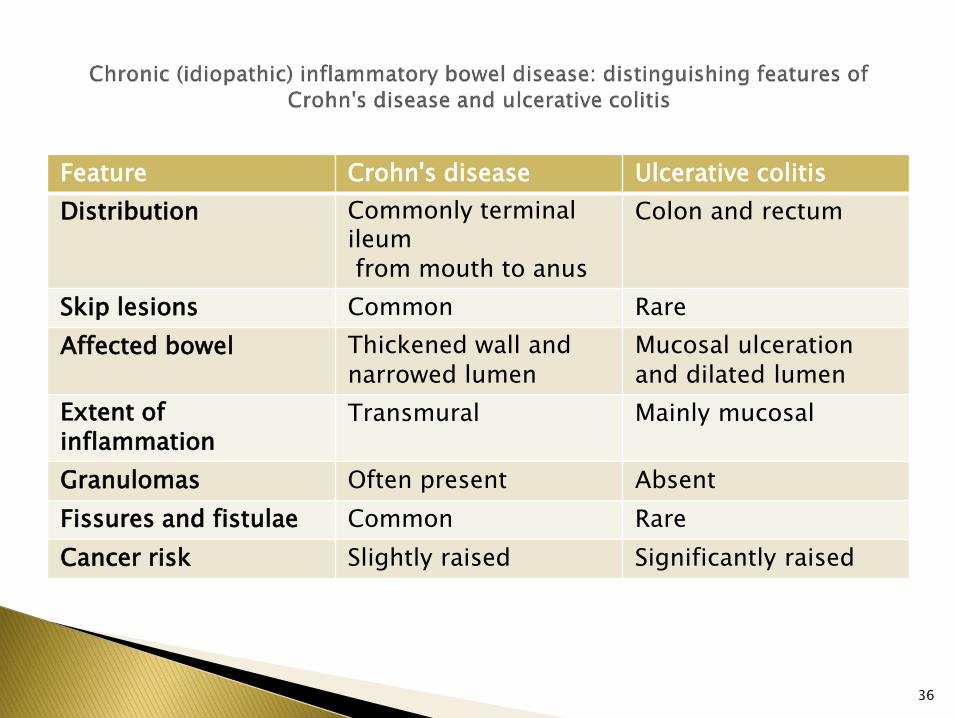
Ulcerative colitisCrohn's diseaseFeature
Colon and rectumCommonly terminal ileum from mouth to anus
Distribution
RareCommonSkip lesions
Mucosal ulceration and dilated lumen
Thickened wall and narrowed lumen
Affected bowel
Mainly mucosalTransmuralExtent of inflammation
AbsentOften presentGranulomas
RareCommonFissures and fistulae
Significantly raisedSlightly raisedCancer risk
36
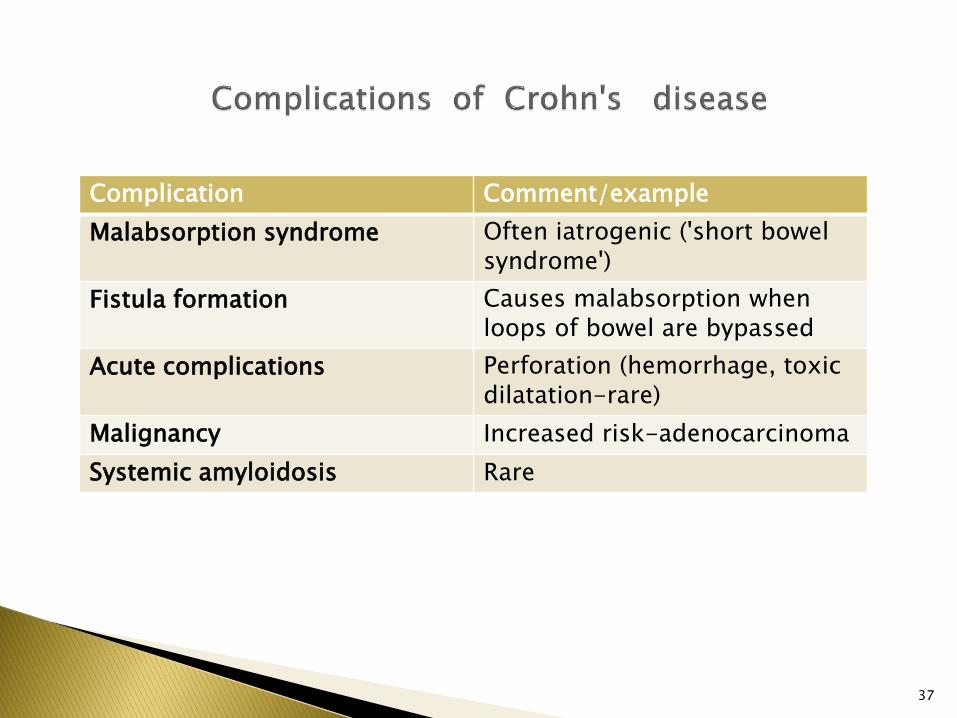
Comment/exampleComplication
Often iatrogenic ('short bowel syndrome')
Malabsorption syndrome
Causes malabsorption when loops of bowel are bypassed
Fistula formation
Perforation (hemorrhage, toxic dilatation-rare)
Acute complications
Increased risk-adenocarcinomaMalignancy
RareSystemic amyloidosis
37

• Chronic relapsing inflammatory disorder, but may have an acute fulminating presentation
• Etiology is unknown
• Affects only colon and rectum, sometimes confined to the latter
• Diffuse superficial inflammation
• Acute complications include toxic dilatation, perforation, hemorrhage and
dehydration;
• the chronic complications are anemia, liver disease and malignant change
38

Malignancy • The incidence of colorectal cancer in
ulcerative colitis is 2%, • rises to about 10% in patients who have
had the disease for 25 years. • The increased risk over that for the
general population warrants colonoscopicsurveillance of longstanding cases.
• The clinical factors apparently associated with a higher cancer risk
are:• onset of the disease in childhood • clinically severe first attack • total involvement of the colon • continuous rather than intermittent
symptoms
39
Typical crypt abscesses

Comment/exampleComplication
May be: acute (hemorrhage) chronic, leading to anemia
Blood loss
May develop insidiouslyToxic dilatation
Overall incidence 2%Colorectal cancer
Fatty change, chronic pericholangitis, sclerosing cholangitis, cirrhosis, hepatitis
Liver involvement
40

41
Diverticular disease Diverticula are herniations of mucosa
into the intestinal wall
• the sigmoid, is by far the commonest site
• The disease is generally acknowledged to result from a deficiency of fibre in the diet.
• abnormally high intra-luminal pressures
• Complications• abdominal pain and altered bowel habit
• the most common being diverticulitis
• can cause a peri-colic abscess and a fistula

42
Polyps A polyp is a protuberant growth The adenoma-carcinoma sequence Adenomas are the precursors of
colorectal cancers
familial adenomatous polyposis(FAP).
• FAP is a rare autosomal dominant disease Both sexes are equally affected
• develop during the second and third decades
• almost inevitable progression to cancer by the age of 35
The oncogenes most frequently altered in colorectal cancer are c-Ki-ras and c-myc

Common malignancy in developed countries • All are adenocarcinomas
• Increased risk in patients with adenomatous polyps and longstanding ulcerative colitis
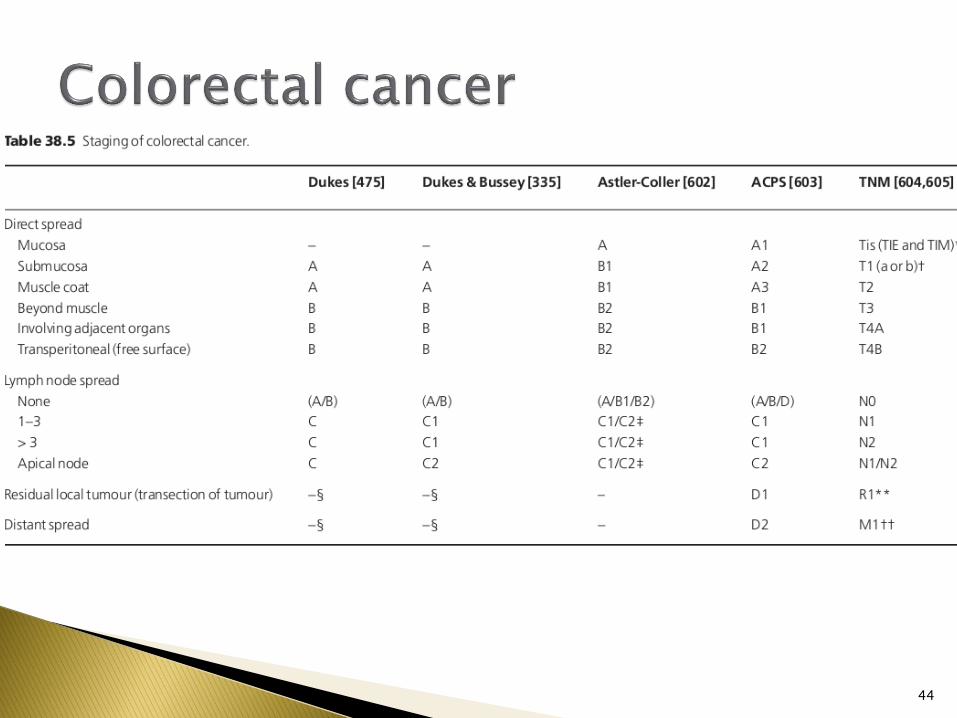
Dukes' staging, based on local extent and metastatic status, is the best guide to prognosis
Clinicopathological features• Approximately 50% of cancers occur in the rectum
• as about 50% of large bowel cancers can be reached with the examining finger and 80% with the sigmoidoscope.
• Microscopically the cancers are Adenocarcinomas
43
44
The appendix can be the site for carcinoid tumors, adenocarcinomas and lymphomas, but these are rare compared with the frequency of non-specific suppurative inflammation
APPENDICITIS
• Common cause of the 'acute abdomen'
• Inflammation often precipitated by obstruction due to faecolith, lymphoid hyperplasia or tumor
• Complications include peritonitis, hepatic abscesses,…
Etiology
• Faecoliths
• and food residues, lymphoid hyperplasia (as occurs in childhood and with some viral infections),
• diverticulosis of the appendix,
• and the presence of a carcinoid tumour
45

46





























