Embed Size (px)
DESCRIPTION
Dr Mary Rowlands, Endas. DUAL DIAGNOSIS (CO-MORBIDITY) IN BRIEF. Important reference. Co-existing Problems of Mental Health and Substance Misuse Dual Diagnosis A Review of Relevant Literature College Research Unit Vanessa Crawford Editor Professor Ilana Crome, 2001. - PowerPoint PPT Presentation
Citation preview

Dr Mary Rowlands, Endas
DUAL DIAGNOSIS (CO-MORBIDITY)
IN BRIEF

Important reference
• Co-existing Problems of Mental Health and Substance Misuse
• Dual Diagnosis• A Review of Relevant Literature• College Research Unit• Vanessa Crawford• Editor Professor Ilana Crome, 2001

Aims of today’s course:
• To raise awareness of the nature and prevalence of Dual Diagnosis.
• To enable participants to understand why dual diagnosis is complex.
• To examine brief detection & screening for this client group.

Aims of today’s course:
• Improve knowledge of increased vulnerability in mentally ill to use substances & sub-optimise MH Rx
• To challenge attitudes towards this client group & Mental Health & Addiction Service
response in context that Substance Use is common in UK

Objectives for today’s course:
• To develop your skills in the brief assessment of individuals with a co-morbidity.
• To be able to determine differences and overlap between symptoms of mental health problems and substance misuse.
• For you to feel more confident in being able to manage individuals with complex needs.
• If time Department of Health funded Systematic Review of evidence that cannabis use increases risk of psychotic and affective disorders (June 2005-June 2006)

Definitions of Dual Diagnosis
• “The term dual diagnosis covers a broad spectrum of mental health and substance misuse problems that an individual might experience concurrently. The nature of the relationship between these two conditions is complex………Services need to be clear at the outset which individuals they intend to provide interventions for”
(Department of Health Mental Health Policy Implementation Guide May 2002)

Definitions continued:
• Co-morbidity (Dual Diagnosis) is the co-occurrence of severe mental health problems (and personality disorder) which are caused or complicated by problematic consumption of illicit substances, misuse of prescribed drugs or alcohol.
(Nottingham Dual Diagnosis Team)

Definitions continued:
“The term Dual Diagnosis is not helpful in describing this group. First the term is non-specific and could refer to a whole range of problems.
Secondly low levels of substance misuse
(i.e. not enough to merit a diagnosis of dependence or abuse)
can have a significant effect on those individuals with severe mental health problems and therefore does not warrant the label diagnosis.”
(Graham H et al 2003)

Severe Mental Illness:The DoH sets out 5 defining characteristics:• They are diagnosed (typically with
Schizophrenia or Bipolar affective disorder).• Are substantially disabled due to their illness.• They are currently displaying florid symptoms
as part of an enduring condition.• Have suffered recurring crises resulting in
admissions or interventions.• They may at times pose a significant risk to
themselves or others.

DoH definition examples:Severity of Severity of substance substance misusemisuse
Severity of mental Severity of mental health problemhealth problem
E.g. A man who drinks 2.5 litres of cider per day and experiences increasing anxiety
E.g. A 22 year old man who has a diagnosis of bi-polar disorder who binge drinks and has started experimenting with intravenous drug taking.
E.g. a young woman who takes ecstacy at the weekend and who is now experiencing depression throughout the week
E.g. A woman with schizophrenia who smokes 2-3 joints daily to compensate for social isolation
HIGHHIGHLOWLOW
HIGHIGHH
LOWLOW

Service Models of joint mental health and addiction services
• Consecutive-dangers slip between services• Addiction services deal with mild/moderate
mental illness mainly affective disorder• Parallel-dangers of sub-optimal treatment• Dedicated DD-not cost-effective deskills• Integrated-DOH recommendation
• Low priority with gate-keeping for both services

Prevalence in the UK
• An inner London Study showed that 36% of people with a psychosis had abused substances. (Tyrer et al 1999).
• A recent study conducted in 2 London Boroughs, Nottingham and Sheffield showed that prevalence of drug taking in people with mental health problems had risen to 44%. (Weaver et al 2003)

Client Profile:
• Male (80%)• Between the age of 23 & 35.• Poly-drug user. (55%)• Engaged in experimental & opportunistic
drug taking.• High levels of risk • (40% inject, violence or suicide)

In homeless population
• Higher rates of Substance Misuse• Higher rates of SEMI• Higher rates of DD • Increased risk of sharing injecting equipment • Increased risk of unsafe sexual practices as in
all DD

The drugs that they take:• 49% take stimulants
(amphetamines and cocaine).• Crack smoking is sharply on the
increase.• 27% take heroin.• 37% smoke cannabis and drink
heavily.• 40%+ inject the drugs they take
often straight away and in high risk sites.

Vulnerability to Alcohol Misuse
• Most commonly available and often cheapest drug
• More vulnerability in:– Bipolar and affective disorders– non-compliant, socially isolated

Increased dose recruits additional monoamines
• Dose Low

Cannabinoids neurobiology
• CB1 receptors widely distributed in cortex
• Endogenous cannabinoids (eg anandamide)
• Δ9 THC releases dopamine from nucleus accumbens and prefrontal cortex
• Inhibits GABA & glutamate transmission

Brainstorm.Why might people with severe mental health problems take drugs or alcohol ?

Psychosis is lonely in adolescent development• Substance misuse aetiology as
for general population-fun,escape, relaxation, environmental access
• providing an accepting social in group initially and delays effective early intervention
• Neurodevelopment in brain regions associated with learning for adult roles: motivation,impulsivity also confer addiction learning (Chambers RA, AM J Psych 2003; 160:1041-1052)

?Already primed dopamine reward circuits
• E.g.70% cf 25% smoke before first symptoms of mental illness
• ?common aspects to both conditions of dopamine circuits dysfunction.
• Volkov ND. Cereb Cortex 2000;10:318-325

Pills DD want
• Development of severe mental illness and substance misuse at key stage of teenage autonomy leads to conflict
• Increases hostility• Familial high expressed emotion
worsens• Further alienates support network• Increases vulnerability to
homelessness and coming within the CJ system

versus pills DD don’t want
Non-compliance• &to • addiction treatment

Dual Diagnosis worsens SMI outcomes
– Increases relapse rates–Rehospitalisation
– Increases positive symptoms of psychosis
–Worsens clinical and functional outcomes

Interactive work.What are the differences between symptoms of severe mental health problems and symptoms
relating
to drug taking?
Clue ICD

Psychosis during cannabis intoxication
• Surveys of cannabis users
– 15 % report experiencing brief psychotic symptoms (paranoid beliefs / hearing voices)
• Experimental studies of intravenous THC (DeSouza 2004)
– 22 subjects, randomly given IV THC or placebo
– Highly significant increases in psychotic symptom scores
– Completely resolved within 3 hours, and no effect up to 6 months

Cannabis and psychosis
delusions, hallucinations &thought disorder duringcannabis intoxication
acute & transientpsychotic disorder
schizophreniaother ‘chronic’
psychoses
time
psychotic symptoms not due to
direct biological effects of exogenous
cannabinoids
cannabisuse

Cannabis and psychosis persisting beyond intoxicationeffects
• “Cannabis-induced psychosis”: Numerous case reports
• Typically described as onset of psychotic illness following cannabis use, and resolving usually within 1-2 weeks
• Observe acute & transient psychotic illness
• Assumptive role of cannabis in aetiology….but 10% of young adult population use cannabis regularly

Brief Assessment of Clients With Substance
Misuse Problems.

Three main areas of assessment:
• Detection and Screening.• In depth assessment.• Risk assessment.

Dual diagnosis MHPIG states:
• “Since substance misuse among those with mental health problems is usual rather than exceptional and results in poorer treatment outcomes, it is necessary to consider its presence in all assessments undertaken by mental health services”
• But St Georges School of medicine in London recently found that: 26% of clients who reported substance misuse in their survey had not been assessed by acute in-patient staff as having a drug or alcohol problem.

What have I got to lose except my
• Values • Experience• Taboos
• Fears • Prejudices• For a Motivational
approach

Detection and Screening.
• SuMMBAT (Substance Misuse & Mental health Brief Assessment Tool).
• Self report.• Laboratory tests (including urine, hair & blood
screening).• Other forms of screening (Micro-lines & saliva
swabs).• Records and other collected data.

Why Screen?• It gives an accurate snap shot of drugs taken.• Can help establish if the pattern of drug taking is
linked to changes in MH.• A collection of samples over time give a clear
indication of their pattern of drug taking.• Regular screening can act as a point to reinforce
their motivation.• Clients may not be aware or clear of what they have
taken.• If used in a non punitive way it can become an
objective and therapeutic intervention.• It helps us study mood, behaviours and symptoms
and reflect these to the client.

SuMMBAT:

SuMMBAT guidelines:Which substances do they take?• Does the client know?• Consider other substances e.g. Px, volatile
substances & mushroomsHow much do they spend?• A general indication of level of consumption.Do they inject/smoke etc?• Which area of the body do they inject into?• Where do they get their works?• Do they inject with anything in particular? (e.g.
lemon juice)

SuMMBAT guidelines:How often?• Indicates the main pattern of drug taking e.g
regular or binge.How long for?• Indicates the impact that drug use may have
had on M.H.Ps & lifestyle.• Level of tolerance

SuMMBAT guidelines cont’d:What is their MH diagnosis?• Highlights why a client may be using a
given substance.• Is it directly related to their drug of
choice?What are the positive effects?• Self-medication for illness or Px
medication.• Social inclusion.• Coping mechanisms.• Lifestyle.

What are the negative effects?
•Physical & mental health
•Finances
•Social effect
•Accommodation
•Work or activity
•Offending.Degree of motivation:•Asking the client what they want to achieve. Control or Abstinence?•Even if motivation is low then some interventions are still indicated.

SuMMBAT Guidelines Cont’d:What help does the person want?• Education/information.• Harm-minimisation.• Detox.• Abstinence.• Relapse prevention.Any previous treatment?• Useful to ascertain if they have engaged well,
previous detoxes that worked/failed, notable withdrawal experiences and periods of control/abstinence.

Assessment:
• “Accurate assessment is fundamental to the effective management of people with a dual diagnosis.
• The aim of an assessment is to give the practitioner a clear picture of what is going on for that person and what is contributing to their distress”
(RCP Research Unit, 2002. Co-existing problems of mental disorder and substance misuse (dual diagnosis) an information manual.)

Specialist Assessment.• “Specialist assessments are undertaken to
determine the nature and severity of substance misuse and mental health problems, and to identify corresponding need.
• The more comprehensive and focussed the assessment
• the better the understanding will be of the relationship between the two disorders.”

Risk Assessment:• “Routine risk assessment protocols need to address
specific factors for individuals with a dual diagnosis. • The severity of substance misuse, including the
combination of substances used, is related to the risk of overdose and suicide.
• Exploration of the possible association between substance misuse and increased risk of aggressive or anti-social behaviour
• forms an integral part of the risk assessment, and should be explicitly documented if present.” (DoH Dual Diagnosis MHPIG, 2002).

Risk Assessment cont’d:Other aspects to consider include:• Risk to the client and others due to drug
taking paraphernalia. E.g. the potential for needle stick injuries as a result of improperly discarded needles and syringes.
• Risk due to blood borne infections. E.g. Hepatitis and HIV.
• Risk due to overdose i.e. accidental overdose of illicit substances.

Risk Assessment cont’d:
• Risk of abuse by others. E.g. clients can be dis-empowered or abused by drug pushers who prey on them for money or drug users needing a place to “SCORE”.
• Risk due to violence. Research has shown that this client group is more likely to be unpredictable, aggressive and violent. There is a potential risk to staff due to some of the individuals that a client with a co-morbidity may mix with.
• Risk of relapse as a direct result of their drug or alcohol problem

Harm reduction –CHALLENGES traditional values
Reducing blood borne viral transmission
Reducing quantities of alcohol drunk/drugs used

Recovery Approach in Co-morbidity
• Goal Hierarchy towards abstinence• Personal values & • meaning for life goals• Risk management joint approach with clients and psychiatric & substance misuse services
OpportunityControl
Hope

Other questions you might ask…
• What do they know/understand about the substance and it’s effects?
• What effects do they get from their psychiatric medication?
• What are their social circumstances?• What have they done in the past to help
control or abstain from drug of choice?

Case Study:• Adam is a 34 year old man who has a diagnosis of paranoid
schizophrenia. Until recently he lived at home with his mum and step father. He now lives in a flat in Newtown after being thrown out “For getting lairy” his mum tells you.
• Adam injects around 1 gramme of amphetamines 4 days per week. He also takes heroin which he injects intramuscularly, cocaine which he also injects and occasionally smokes crack. In the past he has drunk heavily and also taken steroids.
• Discuss how you would assess Adam’s needs, what issues you might prioritise and what you would do to try to ensure he receives a comprehensive service.

Stages of treatment:
• Assessment.• Engagement:
Building a therapeutic relationship.Doesn’t necessarily tackle drug and alcohol issues immediately.
• Early empowerment:Gives the client relevant verbal and written information that they may not have had before.

Stages of treatment contd:
• Late empowerment.Helps the client to self monitor using drug/drink diaries.Simple monitoring.Goal setting.
• Action/Active phase.Active detoxification/control of substance taking (based on goals set).Controlled drinking groups.
• Relapse prevention including a relapse prevention plan.

Engagement and risks• UK Mental Health Services• AOT• Early Intervention Services• Substance Misuse can
present in crisis but would normally be excluded from Crisis Team assessment
• Dual diagnosis integrated model with MH Services lead for severe & enduring MI due to limited evidence for dedicated service

• Psychosocial interventions are the evidenced treatments to improve outcomes not substitute medication for stimulant/cannabis abuse
• No evidence of improved outcome by matching MET=CBT=social Network Therapy=12 step for alcohol(1997 Project Match)
• Community reinforcement programmes- eclectic, intensive,repeatedly available to engage, aftercare is evidenced

?

1936 Mythology2006 Limited
Evidence

1936…
“One moment of bliss, a lifetime of regret ....”

2004….
“We and about five other studies have shown that if you start taking cannabis early and heavily you are about seven times more likely to develop schizophrenia”
BBC news 22nd Jan 2004
“Prohibitionists love to claim cannabis causes schizophrenia. Mostly because all their other claims have been proved wrong. Just like this one will soon be.”
The Hempire Aug 2004

ACMD
• Advisory Council on the Misuse of Drugs
– Independent expert body– Remit to review drug situation and advise Government on
prevention / dealing with social problems
• Decision to downgrade based on ACMD report March 2002
• Request by Home Secretary in March 2005 to review evidence
• Department of Health funded Systematic Review of evidence that cannabis use increases risk of psychotic and affective disorders (June 2005-June 2006)

Cannabis and schizophrenia
• Cross-sectional studies show that cannabis use in people with schizophrenia is more common than in general population
• Limitation of cross-sectional studies
– Cannabis increases risk of schizophrenia?
– Schizophrenia increases likelihood of using cannabis?
(self-medication or reverse causation effect)

time
cohort
cannabis
Longitudinal or cohort studies
no cannabis

Systematic review of cannabis use and risk of developing psychoses
• What is the evidence that cannabis use increases risk of developing schizophrenia?
• What is the evidence that cannabis use increases risk of developing other psychoses?
• What is the evidence that cannabis use in people with schizophrenia results in a poorer long-term outcome?

Systematic review of cannabis use and risk of developing psychoses
• Longitudinal (cohort) studies• Reverse causation excluded?• Intoxication effects excluded?• Confounding assessed?
personality traits
cannabis use schizophrenia

Systematic review of cannabis use and risk of developing schizophrenia and other psychoses
• Department of Health funded
• Glyn Lewis• Tess Moore• Anne Lingford-Hughes• Peter Jones• Tom Barnes

Search strategy: databases
• Medline, EMBASE, CINAHL, PsycINFO, ISI Web of Knowledge, ZETOC, BIOSIS, LILACS, MEDCARIB, National Research Register
• Contacting experts: Louise Arsenault IOP, Bovasso, Michael Davidson, Mark Weiser NY/Israel, Louise Degenhardt, William Eaton NY, Robert Ferdinand, David Fergusson (Christchurch), John MacLeod, Robin Murray, George Patton Melbourne, Richie Poulton Dunedin, David Semple, Jim van Os Maastrict, Helene Verdoux Bordeaux

Titles and abstracts possibly relevant N = 169
Papers included Psychosis
n=9 (6 studies)Papers included
Depressionn=19
Titles and abstracts which were very unlikely to be relevant, excluded:
n= 3868
Papers not relevant (full papers or
abstract)n=139
Review flow chart
Total hits 6718(Duplicates 2684)
Reference lists expert knowledge and other
databases = 47 Total N=4037

Summary of studies included
N in cohort
Length of follow-up
N with psychotic outcome
Psychosis type Effect of cannabis on risk
Swedish conscripts (Andreasson 1987) (Zammit 2002)
50,087 27 years 362 (0.7%) schizophrenia
Dunedin (Aresenault 2002)
759 11 years a) 190 (25%)
b) 25 (3.3%)
a) psychotic symptom
b) schizophreniform
NEMESIS
(van Os 2002)
4045 3 years a) 38 (1%)
b) 10 (0.25%)
a) mild symptom
b) moderate symptom
EDSP
(Henquet 2005)
2437 4 years a) 424 (17%)
b) 174 (7%)
a) psychotic symptom
b) 2 symptoms
Christchurch (Fergusson 2005)
1055 2-7 years N/A psychotic symptom
ECA (Tien 1990) 4994 1 year 507 (11%) psychotic symptom

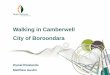
Ever use of cannabis: adjusted results - all psychoses
odds ratio
reduced risk increased risk
.009014 1 110.938
Study odds ratio (95% CI) % Weight
ECA (any Sx) 1.30 ( 0.98, 1.73) 16.1
Christchurch (any Sx) 1.28 ( 1.04, 1.57) 17.6
Munich (any Sx) 1.53 ( 1.13, 2.07) 15.8
Munich (2+ Sx) 2.23 ( 1.52, 3.28) 14.1
Nemesis (any mild Sx) 2.76 ( 1.18, 6.46) 6.8
Nemesis (any mod Sx) 24.17 ( 5.44, 107.42) 2.9
Nemesis ('disorder') 12.01 ( 2.24, 64.36) 2.3
Dunedin 15 (schizophreniform) 3.12 ( 0.73, 13.31) 3.0
Dunedin 18 (schizophreniform) 1.42 ( 0.54, 3.74) 5.7
Swedish (schizophrenia) 1.50 ( 1.11, 2.02) 15.8
Overall 1.83 ( 1.39, 2.40) 100.0
Odds ratio: The ratio of the probability of having a disease in a population exposed to a certain risk factor (e.g. cannabis use) and the probability of having the same disease in a population not exposed.

Ever use of cannabis: adjusted results - psychotic disorders
odds ratio
reduced risk increased risk
.009014 1 110.938
Study
odds ratio
(95% CI) % Weight
Nemesis ('disorder') 12.01 ( 2.24, 64.36) 13.2
Dunedin 15 (schizophreniform) 3.12 ( 0.73, 13.31) 16.2
Dunedin 18 (schizophreniform) 1.42 ( 0.54, 3.74) 25.7
Swedish (schizophrenia) 1.50 ( 1.11, 2.02) 44.8
Overall 2.19 ( 1.07, 4.48) 100.0
% weight: statistically adjusted to take account of
actual or potential confounding factors.

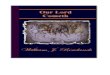
Most frequent use: adjusted results - all psychoses
odds ratio
reduced risk increased risk
.009014 1 110.938
Study
odds ratio
(95% CI) % Weight
Swedish (>50 times) 3.10 ( 1.72, 5.58) 18.6
NEMESIS (>weekly) 6.81 ( 1.79, 25.91) 5.9
EDSP (daily) 2.23 ( 1.30, 3.83) 20.1
ECA (daily) 2.40 ( 1.55, 3.72) 24.0
Christchurch (daily) 1.56 ( 1.20, 2.03) 31.3
Overall 2.31 ( 1.62, 3.29) 100.0

What factors might have lead to studies over-estimating the true association between cannabis
use and psychosis?

cannabis use
well psychosis
sub-clinical symptoms
Reverse causation
prodrome

cannabis use
well psychosis
personality traits, other drugs…
Confounding

cannabis use
well psychosis
continued cannabis use leads to intoxication
symptoms (regular users)
Bias: intoxication effects

Quality assessment of studies included
Reverse causation excluded
Intoxication effects excluded
Number of confounders (% change from crude)
Swedish conscripts (Andreasson 1987)
(Zammit 2002)
++ ++ 11 (30% )
Dunedin
(Aresenault 2002)
- + 4 (no crude results)
NEMESIS
(van Os 2002)
++ + 6 (35% )
EDSP
(Henquet 2005)
- + 9 (15% )
Christchurch
(Fergusson 2005)
+ - 17 (30% )
ECA
(Tien 1990)
++ + 5 (15% )

What factors might have lead to studies under-estimating the true association between cannabis
use and psychosis?

cannabis use
well psychosis
attrition greater in cannabis users who become ill?
Bias: attrition

cannabis use
well psychosis
change in cannabis use over time
Bias: random misclassification
cannabis dose measured inaccurately


Sensitive periods of risk?
• Cerebral development incomplete until late teens
(myelination, synaptogensis..)
• Any evidence for greater risk if use cannabis during early adolescence compared to adulthood?

Age at first use of cannabis
• Dunedin– Age 15 (symptoms) *= 6.6 (4.8, 8.3)– Age 18 (symptoms) risk difference = 1.0 (0.3, 1.8)
– Age 15 (schizophreniform) OR = 3.1 (0.7, 13.3)– Age 18 (schizophreniform) OR = 1.4 (0.5, 3.7)
• Swedish conscripts– Age 15 (schizophrenia) OR = 1.2 (1.0, 1.4)– Age 18 (schizophrenia) OR = 1.2 (1.1, 1.4)
*Multiple logistic regression analyses showed cannabis use by 15 years &18 years had more schizophrenia symptoms than controls at age 26yrs
Cannabis by 15 yrs more than 4 times as likely to have schizophreniform disorder at 26 years than controls.
Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...

Age at first use of cannabis
Risk Difference :
risk in the treated group minus the risk in the control group (confidence intervals).If an experimental intervention has an identical effect to the control, the risk difference will be 0. If it reduces risk, the risk difference will be less than 0; if it increases risk, the risk difference will be bigger than 0.
Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...Risk Difference is the risk in the treated group minus the risk in the control group ...

Summary of findings relevant to clinical practice
• Only one longitudinal study that examines effect of cannabis use on risk of schizophrenia
• Two studies examine other ‘similar’ outcomes:
– Dunedin cohort: 3.5% schizophreniform disorder in 1 year
(200x more than expected 0.015% schizophrenia)
– NEMESIS: ‘needs-based diagnosis’ = most severe symptoms (0.2% in 3 years)

Summary of findings relevant to clinical practice
• Reverse causation unlikely given study designs
• Confounding– Associations all reduced by 15-40% after adjustment– Associations persisted after adjustment– Residual confounding possible
• Intoxication– Unlikely given assessment tools– However, how do you exclude this in regular users?

Support for causality
• Consistency of results– Increased risk of psychoses in all these studies– Not adequately explained by bias, confounding or reverse
causation
• Dose-response effect in all studies that examined this
• Compatible with other sources of knowledge– Cannabis intoxication psychosis– Neurobiology of cannabinoids & abnormalities in schizophrenia
• …There is always room for doubt….

Unanswered questions
• What effect does regular use of cannabis over many years have?
• What about exposure during early teenage years?
• What about use of higher potency forms of cannabis?
• What about risk in those already vulnerable, eg: family history?
• Any other groups where cannabis use may be particularly harmful?– eg: Catechol-O-Methyl Transferase genotype regulates
dopamine metabolism (Caspi et al 2004)
• What about time trends?

Are future studies likely to help?
• Schizophrenia incidence approximately 15/100,000/year
• Cohort study of 10,000 people, followed up for 20 years age 12-32
– Probably about 30 people with schizophrenia…
• More reasonable to study ‘endophenotypes’ of schizophrenia
– eg: specific neuropsychological deficits
• Animal models of endophenotypes may be particular helpful
• Definitive answer not likely in decades to come

What if someone already has schizophrenia?
• Part of current systematic review; not complete as yet
• Clinical experience and evidence from a number of studies suggest that cannabis use:
– Increases relapse rates– Increases positive symptoms of psychosis– Is associated with reduced compliance with medication– Worsens clinical and functional outcomes
• Strength of evidence regarding this unclear
• Future studies feasible, as well as intervention trials for reducing cannabis use in people with schizophrenia

Public health perspective
Does cannabis cause psychotic illnesses?
or..
‘Would reducing cannabis use reduce the incidence of psychotic illnesses?’
• Assuming the strength of association from studies above are correctly estimated and that cannabis use is truly causal...
• Approximately 10-20% of psychosis outcomes in these studies would not have occurred if no-one used cannabis

Individual perspective
• Individual lifetime risk of schizophrenia is 0.7%
• If using cannabis daily increases risk by 2.5 times:
– Lifetime risk of schizophrenia = 0.7% x 2.5 ≈ 2%
• Individual risk relatively low, but may be much higher if heavy or frequent use, if use more potent forms, or use at an early age
• Furthermore, it may be the only modifiable risk factor there is at present

Clinical perspective
• If someone has experienced any psychotic-like phenomena following use of cannabis should be strongly advised about possible risk of developing a severe psychotic illness
• If a patient has a psychotic illness, they should be routinely strongly advised (including written information) that using cannabis may make this worse
• We should actively target family members of patients with schizophrenia to advise about possible risk if use cannabis

Clinical perspective
• Message to public
The evidence supports the view that using cannabis can increase risk of developing a psychotic illness, including chronic and severe psychotic illnesses such as schizophrenia
• Reference• ACMD Further consideration of the classificatioof cannabis
under the Misuse of Drugs Act 1971, HMSO,2006